
Impact of Percutaneous Mitral Valve Repair Using the MitraClipTM System on Ventricular Arrhythmias and ICD Therapies

Abstract
1. Introduction
2. Materials and Methods
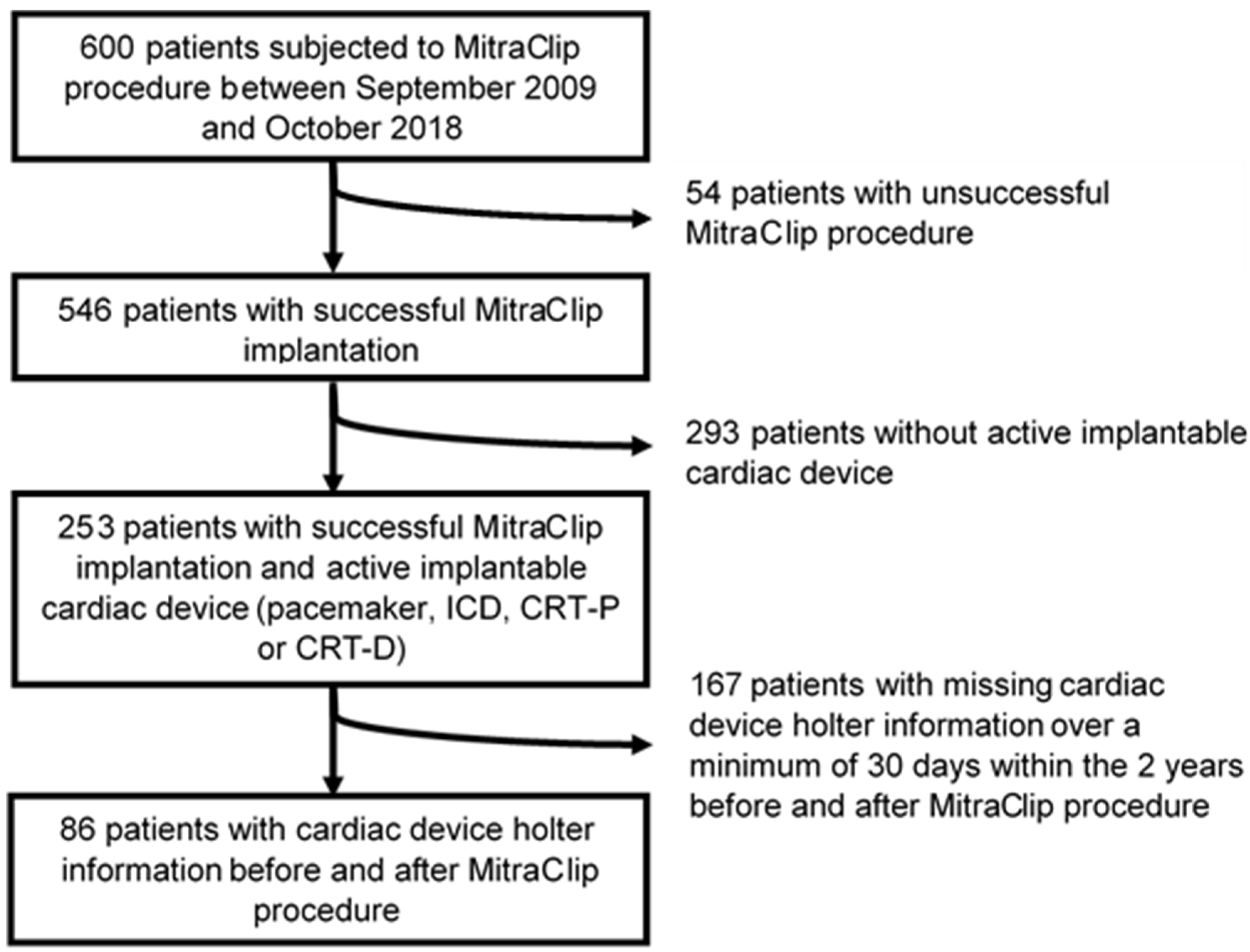
2.1. Patient Population
2.2. MitraClipTM Procedure
2.3. Echocardiographic Assessment
2.4. Arrhythmia Detection
2.5. Statistics
3. Results
3.1. Patient Characteristics
3.2. Procedural Outcome
3.3. Arrhythmic Outcomes
3.4. Ventricular Arrhythmia
3.5. ICD Therapies
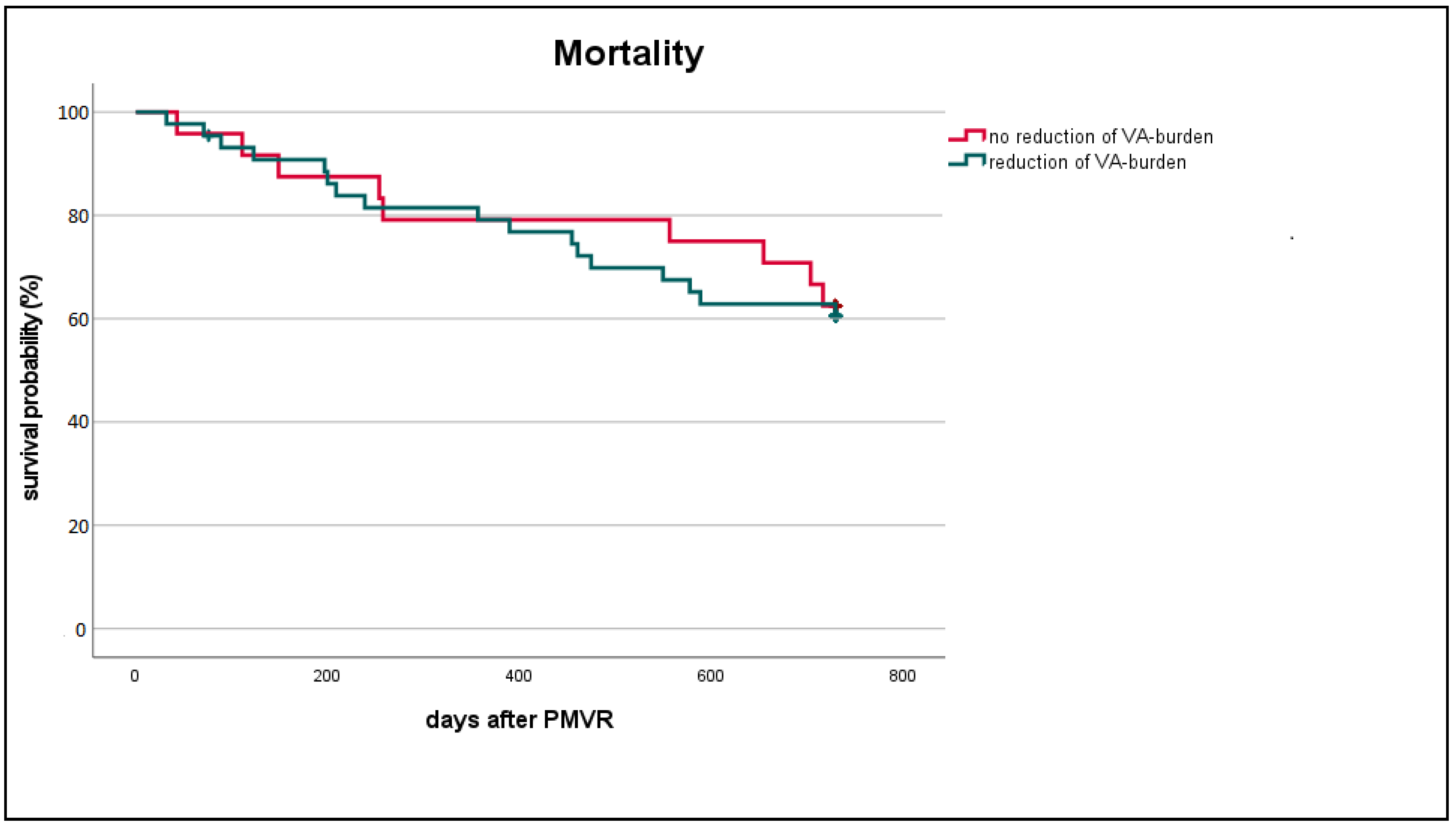
3.6. Characteristics of Patients with Reduced VA Burden Post TEER
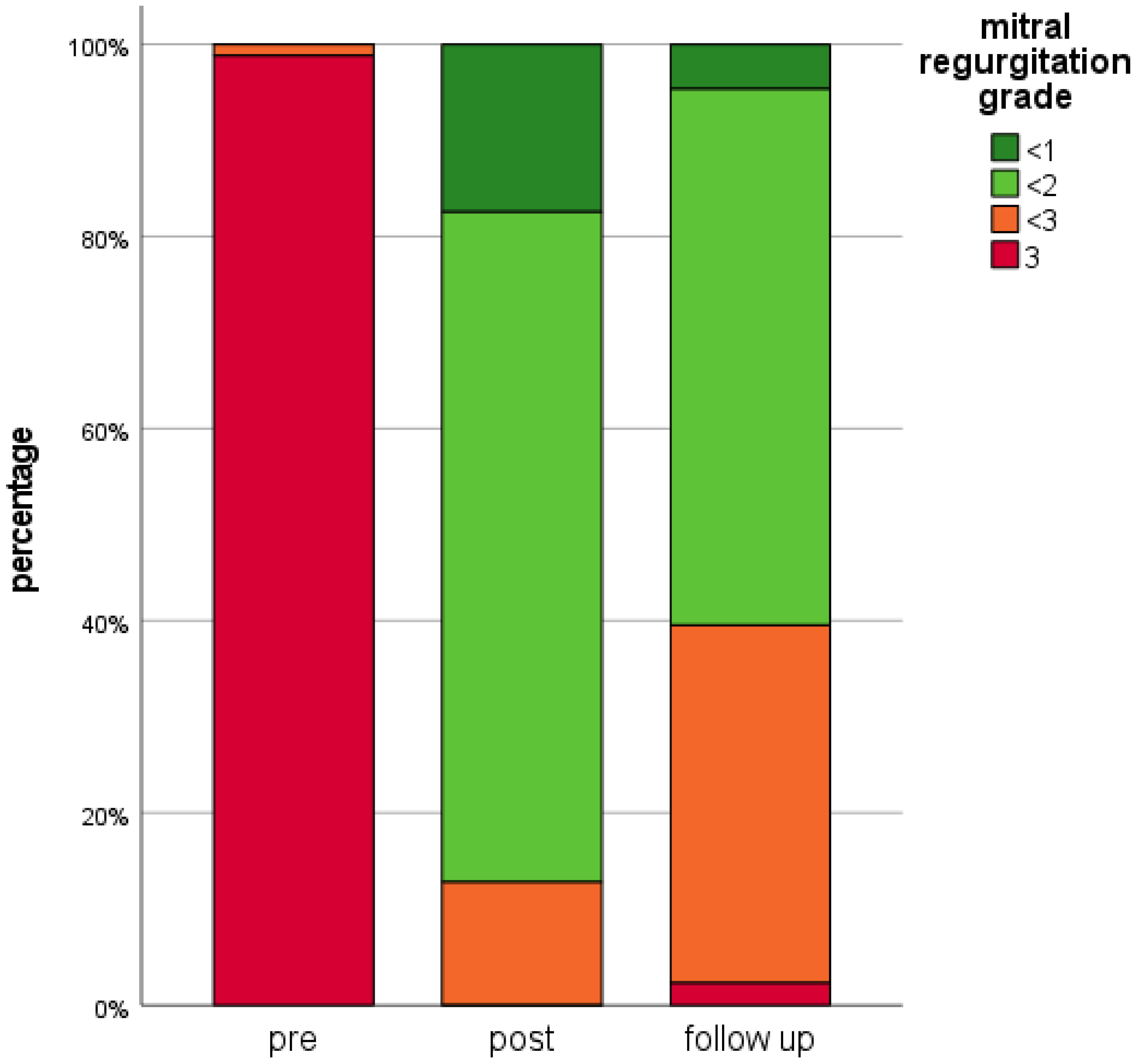
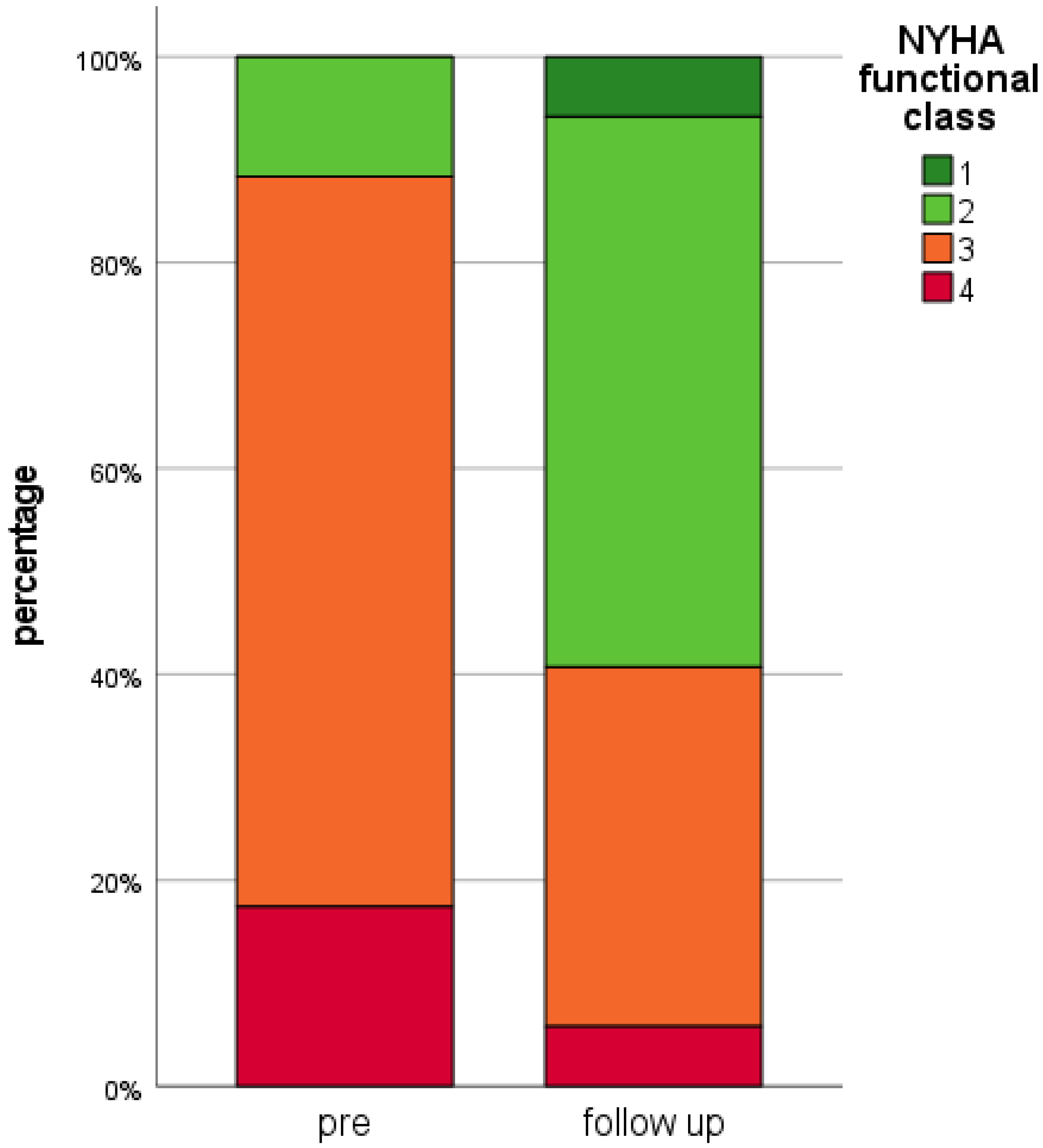
3.7. Echocardiographic and Clinical Outcomes
4. Discussion
Limitations of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ATP | Anti-tachycardia Pacing |
| CI | Confidence Interval |
| CRT | Cardiac Resynchronization Therapy |
| CRT-D | Cardiac Resynchronization Therapy—Defibrillator |
| CRT-P | Cardiac Resynchronization Therapy—Pacemaker |
| DCMP | Dilated Cardiomyopathy |
| GDMT | Guideline-Directed Medical Therapy |
| HF | Heart Failure |
| HFrEF | Heart Failure with reduced Ejection Fraction |
| HR | Hazard Ratio |
| ICD | Implantable Cardioverter Defibrillator |
| LA | Left Atrial |
| LV | Left Ventricular |
| LVEDD | Left Ventricular Enddiastolic Diameter |
| LVESD | Left Ventricular Endsystolic Diameter |
| LVEF | Left Ventricular Ejection Fraction |
| MR | Mitral Regurgitation |
| nsVT | non-sustained Ventricular Tachycardia |
| NT-proBNP | N-terminal prohormone Brain Natriuretic Peptide |
| NYHA | New York Heart Association |
| sVT | sustained Ventricular Tachycardia |
| TEER | Transcatheter Edge-to-Edge Repair |
| VA | Ventricular Arrhythmia |
| VF | Ventricular Fibrillation |
| VT | Ventricular Tachycardia |
References
- Enriquez-Sarano, M.; Akins, C.W.; Vahanian, A. Mitral regurgitation. Lancet 2009, 373, 1382–1394. [Google Scholar] [CrossRef]
- Edwards, N.C.; Moody, W.E.; Yuan, M.; Weale, P.; Neal, D.; Townend, J.N.; Steeds, R.P. Quantification of left ventricular interstitial fibrosis in asymptomatic chronic primary degenerative mitral regurgitation. Circ. Cardiovasc. Imaging 2014, 7, 946–953. [Google Scholar] [CrossRef] [PubMed]
- Rossi, A.; Dini, F.L.; Faggiano, P.; Agricola, E.; Cicoira, M.; Frattini, S.; Simioniuc, A.; Gullace, M.; Ghio, S.; Enriquez-Sarano, M.; et al. Independent prognostic value of functional mitral regurgitation in patients with heart failure. A quantitative analysis of 1256 patients with ischaemic and non-ischaemic dilated cardiomyopathy. Heart 2011, 97, 1675–1680. [Google Scholar] [CrossRef] [PubMed]
- Trichon, B.H.; Felker, G.M.; Shaw, L.K.; Cabell, C.H.; O’Connor, C.M. Relation of frequency and severity of mitral regurgitation to survival among patients with left ventricular systolic dysfunction and heart failure. Am. J. Cardiol. 2003, 91, 538–543. [Google Scholar] [CrossRef]
- Patel, J.B.; Borgeson, D.D.; Barnes, M.E.; Rihal, C.S.; Daly, R.C.; Redfield, M.M. Mitral regurgitation in patients with advanced systolic heart failure. J. Card. Fail. 2004, 10, 285–291. [Google Scholar] [CrossRef]
- Kligfield, P.; Hochreiter, C.; Niles, N.; Devereux, R.B.; Borer, J.S. Relation of sudden death in pure mitral regurgitation, with and without mitral valve prolapse, to repetitive ventricular arrhythmias and right and left ventricular ejection fractions. Am. J. Cardiol. 1987, 60, 397–399. [Google Scholar] [CrossRef]
- Delahaye, J.P.; Gare, J.P.; Viguier, E.; Delahaye, F.; De Gevigney, G.; Milon, H. Natural history of severe mitral regurgitation. Eur. Heart J. 1991, 12 (Suppl. B), 5–9. [Google Scholar] [CrossRef]
- Feldman, T.; Foster, E.; Glower, D.D.; Kar, S.; Rinaldi, M.J.; Fail, P.S.; Smalling, R.W.; Siegel, R.; Rose, G.A.; Engeron, E.; et al. EVEREST II Investigators. Percutaneous repair or surgery for mitral regurgitation. N. Engl. J. Med. 2011, 364, 1395–1406. [Google Scholar] [CrossRef]
- Glower, D.D.; Kar, S.; Trento, A.; Lim, D.S.; Bajwa, T.; Quesada, R.; Whitlow, P.L.; Rinaldi, M.J.; Grayburn, P.; Mack, M.J.; et al. Percutaneous mitral valve repair for mitral regurgitation in high-risk patients: Results of the EVEREST II study. J. Am. Coll. Cardiol. 2014, 64, 172–181. [Google Scholar] [CrossRef]
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; De Bonis, M.; De Paulis, R.; et al. ESC/EACTS Scientific Document Group. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. J. Cardiothorac. Surg. 2021, 60, 727–800. [Google Scholar]
- Pleger, S.T.; Schulz-Schonhagen, M.; Geis, N.; Mereles, D.; Chorianopoulos, E.; Antaredja, M.; Lewening, M.; Katus, H.A.; Bekeredjian, R. One year clinical efficacy and reverse cardiac remodelling in patients with severe mitral regurgitation and reduced ejection fraction after MitraClip(C) implantation. Eur. J. Heart Fail. 2013, 15, 919–927. [Google Scholar] [CrossRef] [PubMed]
- Stone, G.W.; Lindenfeld, J.; Abraham, W.T.; Kar, S.; Lim, D.S.; Mishell, J.M.; Whisenant, B.; Grayburn, P.A.; Rinaldi, M.; Kapadia, S.R.; et al. COAPT Investigators. Transcatheter Mitral-Valve Repair in Patients with Heart Failure. N. Engl. J. Med. 2018, 379, 2307–2318. [Google Scholar] [CrossRef] [PubMed]
- Benito-González, T.; Freixa, X.; Godino, C.; Taramasso, M.; Estévez-Loureiro, R.; Hernandez-Vaquero, D.; Serrador, A.; Nombela-Franco, L.; Grande-Prada, D.; Cruz-González, I.; et al. Ventricular arrhythmias in patients with functional mitral regurgitation and implantable cardiac devices: Implications of mitral valve repair with Mitraclip. Ann. Transl. Med. 2020, 8, 956. [Google Scholar] [CrossRef] [PubMed]
- Ledwoch, J.; Nommensen, A.; Keelani, A.; Meyer-Saraei, R.; Stiermaier, T.; Saad, M.; Pöss, J.; Desch, S.; Tilz, R.; Thiele, H.; et al. Impact of transcatheter mitral valve repair on ventricular arrhythmias. Europace 2019, 21, 1385–1391. [Google Scholar] [CrossRef] [PubMed]
- Benito-González, T.; Estévez-Loureiro, R.; Garrote-Coloma, C.; Arellano-Serrano, C.; Tundidor-Sanz, E.; Fernández-Lozano, I.; Toquero, J.; Pérez de Prado, A.; Goicolea, J.; Fernández-Vázquez, F. Effect of Successful Edge-to-Edge Mitral Valve Repair on Ventricular Arrhythmic Burden in Patients with Functional Mitral Regurgitation and Implantable Cardiac Devices. Am. J. Cardiol. 2019, 124, 1113–1119. [Google Scholar] [CrossRef]
- Feldman, T.; Kar, S.; Elmariah, S.; Smart, S.C.; Trento, A.; Siegel, R.J.; Apruzzese, P.; Fail, P.; Rinaldi, M.J.; Smalling, R.W.; et al. Randomized Comparison of Percutaneous Repair and Surgery for Mitral Regurgitation: 5-Year Results of EVEREST II. J. Am. Coll. Cardiol. 2015, 66, 2844–2854. [Google Scholar] [CrossRef]
- Geis, N.A.; Pleger, S.T.; Chorianopoulos, E.; Müller, O.J.; Katus, H.A.; Bekeredjian, R. Feasibility and clinical benefit of a suture-mediated closure device for femoral vein access after percutaneous edge-to-edge mitral valve repair. EuroIntervention 2015, 10, 1346–1353. [Google Scholar] [CrossRef]
- Geis, N.; Raake, P.; Kiriakou, C.; Mereles, D.; Frankenstein, L.; Abu-Sharar, H.; Chorianopoulos, E.; Katus, H.A.; Bekeredjian, R.; Pleger, S.T. Temporary oral anticoagulation after MitraClip—A strategy to lower the incidence of post-procedural stroke? Acta Cardiol. 2020, 75, 61–67. [Google Scholar] [CrossRef]
- Stone, G.W.; Adams, D.H.; Abraham, W.T.; Kappetein, A.P.; Genereux, P.; Vranckx, P.; Mehran, R.; Kuck, K.H.; Leon, M.B.; Piazza, N.; et al. Mitral Valve Academic Research Consortium. Clinical Trial Design Principles and Endpoint Definitions for Transcatheter Mitral Valve Repair and Replacement: Part 2: Endpoint Definitions: A Consensus Document From the Mitral Valve Academic Research Consortium. J. Am. Coll. Cardiol. 2015, 66, 308–321. [Google Scholar]
- Stone, G.W.; Vahanian, A.S.; Adams, D.H.; Abraham, W.T.; Borer, J.S.; Bax, J.J.; Schofer, J.; Cutlip, D.E.; Krucoff, M.W.; Blackstone, E.H.; et al. Mitral Valve Academic Research Consortium. Clinical Trial Design Principles and Endpoint Definitions for Transcatheter Mitral Valve Repair and Replacement: Part 1: Clinical Trial Design Principles: A Consensus Document From the Mitral Valve Academic Research Consortium. J. Am. Coll. Cardiol. 2015, 66, 278–307. [Google Scholar]
- Geis, N.A.; Pleger, S.T.; Bekeredjian, R.; Chorianopoulos, E.; Kreusser, M.M.; Frankenstein, L.; Ruhparwar, A.; Katus, H.A.; Raake, P.W.J. Haemodynamic effects of percutaneous mitral valve edge-to-edge repair in patients with end-stage heart failure awaiting heart transplantation. ESC Heart Fail. 2018, 5, 892–901. [Google Scholar] [CrossRef] [PubMed]
- Godino, C.; Munafò, A.; Scotti, A.; Estévez-Loureiro, R.; Portolés Hernández, A.; Arzamendi, D.; Fernández Peregrina, E.; Taramasso, M.; Fam, N.P.; Ho, E.C.; et al. MitraClip in secondary mitral regurgitation as a bridge to heart transplantation: 1-year outcomes from the International MitraBridge Registry. J. Heart Lung Transplant. 2020, 39, 1353–1362. [Google Scholar] [CrossRef] [PubMed]
- Geis, N.A.; Puls, M.; Lubos, E.; Zuern, C.S.; Franke, J.; Schueler, R.; von Bardeleben, R.S.; Boekstegers, P.; Ouarrak, T.; Zahn, R.; et al. Safety and efficacy of MitraClip therapy in patients with severely impaired left ventricular ejection fraction: Results from the German transcatheter mitral valve interventions (TRAMI) registry. Eur. J. Heart Fail. 2018, 20, 598–608. [Google Scholar] [CrossRef] [PubMed]
- Obadia, J.F.; Messika-Zeitoun, D.; Leurent, G.; Iung, B.; Bonnet, G.; Piriou, N.; Lefèvre, T.; Piot, C.; Rouleau, F.; Carrié, D.; et al. MITRA-FR Investigators. N. Engl. J. Med. 2018, 379, 2297–2306. [Google Scholar] [CrossRef]
- Kitkungvan, D.; Nabi, F.; Kim, R.J.; Bonow, R.O.; Khan, M.A.; Xu, J.; Little, S.H.; Quinones, M.A.; Lawrie, G.M.; Zoghbi, W.A.; et al. Myocardial Fibrosis in Patients With Primary Mitral Regurgitation With and Without Prolapse. J. Am. Coll. Cardiol. 2018, 72, 823–834. [Google Scholar] [CrossRef]
- Bethge, C.; Motz, W.; von Hehn, A.; Strauer, B.E. Ventricular arrhythmias in hypertensive heart disease with and without heart failure. J. Cardiovasc. Pharmacol. 1987, 10 (Suppl. 6), S119–S128. [Google Scholar] [CrossRef]
- Zeltser, I.; Gaynor, J.W.; Petko, M.; Myung, R.J.; Birbach, M.; Waibel, R.; Ittenbach, R.F.; Tanel, R.E.; Vetter, V.L.; Rhodes, L.A. The roles of chronic pressure and volume overload states in induction of arrhythmias: An animal model of physiologic sequelae after repair of tetralogy of Fallot. J. Thorac. Cardiovasc. Surg. 2005, 130, 1542–1548. [Google Scholar] [CrossRef][Green Version]
- Yokokawa, M.; Tada, H.; Koyama, K.; Ino, T.; Hiramatsu, S.; Kaseno, K.; Naito, S.; Oshima, S.; Taniguchi, K. The characteristics and distribution of the scar tissue predict ventricular tachycardia in patients with advanced heart failure. Pacing Clin. Electrophysiol. 2009, 32, 314–322. [Google Scholar] [CrossRef]
- Basso, C.; Iliceto, S.; Thiene, G.; Perazzolo Marra, M. Mitral Valve Prolapse, Ventricular Arrhythmias, and Sudden Death. Circulation 2019, 140, 952–964. [Google Scholar] [CrossRef]
- Mierke, J.; Loehn, T.; Ende, G.; Jahn, S.; Quick, S.; Speiser, U.; Jellinghaus, S.; Pfluecke, C.; Linke, A.; Ibrahim, K. Percutaneous Left Ventricular Assist Device Leads to Heart Rhythm Stabilisation in Cardiogenic Shock: Results from the Dresden Impella Registry. Heart Lung Circ. 2021, 30, 577–584. [Google Scholar] [CrossRef]
- Kreuz, J.; Balta, O.; Linhart, M.; Fimmers, R.; Lickfett, L.; Mellert, F.; Nickenig, G.; Schwab, J.O. An impaired renal function and advanced heart failure represent independent predictors of the incidence of malignant ventricular arrhythmias in patients with an implantable cardioverter/defibrillator for primary prevention. Europace 2010, 12, 1439–1445. [Google Scholar] [CrossRef] [PubMed]
- Saxon, L.A.; Bristow, M.R.; Boehmer, J.; Krueger, S.; Kass, D.A.; De Marco, T.; Carson, P.; DiCarlo, L.; Feldman, A.M.; Galle, E.; et al. Predictors of sudden cardiac death and appropriate shock in the Comparison of Medical Therapy, Pacing, and Defibrillation in Heart Failure (COMPANION) Trial. Circulation 2006, 114, 2766–2772. [Google Scholar] [CrossRef] [PubMed]
- Berardini, A.; Biagini, E.; Saia, F.; Stolfo, D.; Previtali, M.; Grigioni, F.; Pinamonti, B.; Crimi, G.; Salvi, A.; Ferrario, M.; et al. Percutaneous mitral valve repair: The last chance for symptoms improvement in advanced refractory chronic heart failure? Int. J. Cardiol. 2017, 228, 191–197. [Google Scholar] [CrossRef] [PubMed]
- Pimentel, M.; Zimerman, A.; Chemello, D.; Giaretta, V.; Andrades, M.; Silvello, D.; Zimerman, L.; Rohde, L.E. Predictors of serious arrhythmic events in patients with nonischemic heart failure. J. Interv. Card. Electrophysiol. 2017, 48, 131–139. [Google Scholar] [CrossRef]
- Adelstein, E.C.; Schwartzman, D.; Jain, S.; Bazaz, R.; Wang, N.C.; Saba, S. Left ventricular dimensions predict risk of appropriate shocks but not mortality in cardiac resynchronization therapy-defibrillator recipients with left bundle-branch block and non-ischemic cardiomyopathy. Europace 2017, 19, 1689–1694. [Google Scholar] [CrossRef] [PubMed]
- de Sousa, M.R.; Morillo, C.A.; Rabelo, F.T.; Nogueira Filho, A.M.; Ribeiro, A.L. Non-sustained ventricular tachycardia as a predictor of sudden cardiac death in patients with left ventricular dysfunction: A meta-analysis. Eur. J. Heart. Fail. 2008, 10, 1007–1014. [Google Scholar] [CrossRef]
- Puls, M.; Lubos, E.; Boekstegers, P.; von Bardeleben, R.S.; Ouarrak, T.; Butter, C.; Zuern, C.S.; Bekeredjian, R.; Sievert, H.; Nickenig, G.; et al. One-year outcomes and predictors of mortality after MitraClip therapy in contemporary clinical practice: Results from the German transcatheter mitral valve interventions registry. Eur. Heart J. 2016, 37, 703–712. [Google Scholar] [CrossRef]
- Bedogni, F.; Popolo Rubbio, A.; Grasso, C.; Adamo, M.; Denti, P.; Giordano, A.; Tusa, M.; Bianchi, G.; De Marco, F.; Bartorelli, A.L.; et al. Italian Society of Interventional Cardiology (GIse) registry Of Transcatheter treatment of mitral valve regurgitaTiOn (GIOTTO): Impact of valve disease aetiology and residual mitral regurgitation after MitraClip implantation. Eur. J. Heart Fail. 2021, 23, 1364–1376. [Google Scholar] [CrossRef]
- Maisano, F.; Franzen, O.; Baldus, S.; Schäfer, U.; Hausleiter, J.; Butter, C.; Ussia, G.P.; Sievert, H.; Richardt, G.; Widder, J.D.; et al. Percutaneous mitral valve interventions in the real world: Early and 1-year results from the ACCESS-EU, a prospective, multicenter, nonrandomized post-approval study of the MitraClip therapy in Europe. J. Am. Coll. Cardiol. 2013, 62, 1052–1061. [Google Scholar] [CrossRef]
- Adamo, M.; Grasso, C.; Capodanno, D.; Popolo Rubbio, A.; Scandura, S.; Giannini, C.; Fiorelli, F.; Fiorina, C.; Branca, L.; Brambilla, N.; et al. Five-year clinical outcomes after percutaneous edge-to-edge mitral valve repair: Insights from the multicenter GRASP-IT registry. Am. Heart J. 2019, 217, 32–41. [Google Scholar] [CrossRef]
- Nickenig, G.; Estevez-Loureiro, R.; Franzen, O.; Tamburino, C.; Vanderheyden, M.; Luscher, T.F.; Moat, N.; Price, S.; Dall’Ara, G.; Winter, R.; et al. Percutaneous mitral valve edge-to-edge repair: In-hospital results and 1-year follow-up of 628 patients of the 2011–2012 Pilot European Sentinel Registry. J. Am. Coll. Cardiol. 2014, 64, 875–884. [Google Scholar] [CrossRef]
- Iung, B.; Armoiry, X.; Vahanian, A.; Boutitie, F.; Mewton, N.; Trochu, J.N.; Lefèvre, T.; Messika-Zeitoun, D.; Guerin, P.; Cormier, B.; et al. MITRA-FR Investigators. Percutaneous repair or medical treatment for secondary mitral regurgitation: Outcomes at 2 years. Eur. J. Heart Fail. 2019, 21, 1619–1627. [Google Scholar] [CrossRef] [PubMed]
- Kalbacher, D.; Schäfer, U.; Von Bardeleben, R.S.; Eggrebrecht, H.; Sievert, H.; Nickenig, G.; Butter, C.; May, A.E.; Bekeredjian, R.; Ouarrak, T.; et al. Long-term outcome, survival and predictors of mortality after MitraClip therapy: Results from the German Transcatheter mitral valve interventions (TRAMI) registry. Int. J. Cardiol. 2019, 277, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Mauricio, R.; Kumbhani, D.J. MitraClip: How Do We Reconcile the Inconsistent Findings of MITRA-FR and COAPT? Curr. Cardiol. Rep. 2019, 21, 150. [Google Scholar] [CrossRef] [PubMed]
- Jacq, F.; Foulldrin, G.; Savouré, A.; Anselme, F.; Baguelin-Pinaud, A.; Cribier, A.; Thibaut, F. A comparison of anxiety, depression and quality of life between device shock and nonshock groups in implantable cardioverter defibrillator recipients. Gen. Hosp. Psychiatry 2009, 31, 266–273. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Value | |
|---|---|---|
| Sex (male) | 69/86 (80.2%) | |
| Age (years; median) | 66.5 [58; 76] | |
| mitral regurgitation etiology | degenerative | 6/86 (7.0%) |
| functional | 70/86 (81.4%) | |
| mixed | 10/86 (11.6%) | |
| Left ventricular ejection fraction (%) | 22.1 (±10.3) | |
| Left ventricular ejection fraction ≤ 35% | 78/86 (90.7%) | |
| LA Diameter (mm) | 54.6 (±9.7) | |
| LVESD (mm) | 59.0 (±12.3) | |
| LVEDD (mm) | 68.2 (±11.0) | |
| Systolic PA pressure (TTE; mmHg) | 51 (±13) | |
| hsTNT (pg/mL) | 45.0 (±39.2) | |
| NT-proBNP (median; ng/l) # | 4567 [1957; 10,630] | |
| 6 min walk test distance (m) # | 335 (±126) | |
| NYHA stage (mean) | 3.1 (±0.5) | |
| Stage 1 | 0/86 (0%) | |
| Stage 2 | 10/86 (11.6%) | |
| Stage 3 | 61/86 (70.9%) | |
| Stage 4 | 15/86 (17.4%) | |
| STS Score (median; %) | 5.0 [2.5; 9.7] | |
| EuroScore II (%) | 12.5 (±12.0) | |
| Significant CAD | 63/86 (73.3%) | |
| Prior cardiothoracic surgery | 33/86 (38.4%) | |
| Atrial fibrillation | 56/86 (65.1%) | |
| Prior stroke | 7/86 (8.1%) | |
| Increased retention values (Creatinine ≥ 1.3 mg/dL) | 45/86 (52.3%) | |
| Sleep apnoea syndrome | 6/86 (7.0%) | |
| Pulmonary disease | 16/86 (18.6%) | |
| Diabetes mellitus | 23/86 (26.7%) | |
| Cancer | active | 6/86 (7.0%) |
| state after | 3/86 (3.5%) | |
| Implantable cardioverter defibrillator (ICD) | 42/86 (48.8%) | |
| Cardiac resynchronization therapy—pacemaker (CRT-P) | 1/86 (1.2%) | |
| Cardiac resynchronization therapy—defibrillator (CRT-D) | 39/86 (45.3%) | |
| Pacemaker | 4/86 (4.7%) | |
| Prior ventricular arrhythmia * | nsVT | 50/86 (58.1%) |
| sustained VT | 36/86 (41.9%) | |
| VF | 11/86 (12.8%) | |
| any sustained VA | 40/86 (46.5%) | |
| any VA | 61/86 (70.9%) | |
| Prior Cardiopulmonary Resuscitation Patients enlisted for heart transplantation | 9/86 (11.6%) 18/86 (20.9%) | |
| Ventricular Arrhythmic Event | Before TEER | After TEER | p-Value |
|---|---|---|---|
| Any ventricular arrythmia | 2.24 ± 5.09 | 1.26 ± 3.52 | 0.019 |
| Non-sustained ventricular tachycardia | 1.39 ± 3.31 | 0.83 ± 2.09 | 0.120 |
| Any sustained ventricular arrhythmia | 0.85 ± 3.47 | 0.43 ± 2.03 | 0.010 |
| Sustained ventricular tachycardia | 0.82 ± 3.46 | 0.43 ± 2.03 | 0.014 |
| Ventricular fibrillation | 0.035 ± 0.186 | 0.005 ± 0.033 | 0.056 |
| Any appropriate device-therapy * | 1.00 ± 3.87 | 0.32 ± 1.41 | 0.014 |
| Appropriate antitachycardia pacing * | 0.82 ± 3.56 | 0.28 ± 1.31 | 0.008 |
| Appropriate ICD shocks * | 0.18 ± 0.95 | 0.04 ± 0.12 | 0.052 |
| Left ventricular function | |||
| LVEF (%) | 22.1 ± 10.3 | 23.6 ± 11.9 | 0.161 |
| All Patients (n = 68) | Reduction of Ventricular Arrhythmia Burden (n = 44) | No Reduction of Ventricular Arrhythmia Burden (n = 24) | p-Value | |
|---|---|---|---|---|
| Sex (male) | 56/68 (82.4%) | 39/44 (88.6%) | 17/24 (70.8%) | 0.096 |
| Age (years) | 65.7 ± 12.3 | 68.1 ± 11.7 | 64.2 ± 12.5 | 0.319 |
| Ejection fraction (%) | 21.6 ± 9.7 | 21.3 ± 10.3 | 22.3 ± 8.6 | 0.292 |
| LA Diameter (mm) | 54.8 ± 10.4 | 56.0 ± 11.3 | 52.6 ± 8.4 | 0.452 |
| LVESD (mm) | 59.0 ± 12.0 | 61.1 ± 12.0 | 55.4 ± 11.4 | 0.043 |
| LVEDD (mm) | 68.3 ± 10.8 | 70.3 ± 10.6 | 64.6 ± 10.4 | 0.037 |
| Systolic PA pressure (TTE; mmHg) | 50 ± 13 | 52 ± 13 | 48 ± 13 | 0.306 |
| hsTNT (pg/mL) | 45.1 ± 39.0 | 49.3 ± 44.5 | 37.3 ± 25.1 | 0.390 |
| NT-proBNP (ng/l) | 8559 ± 10,974 | 8455 ± 8339 | 8742 ± 14,708 | 0.305 |
| 6 min walk test distance (m) | 338 ± 121 | 327 ± 127 | 363 ± 103 | 0.340 |
| NYHA stage | 3.1 ± 0.6 | 3.2 ± 0.5 | 2.8 ± 0.6 | 0.004 |
| STS Score (%) | 7.7 ± 7.8 | 7.1 ± 6.9 | 8.9 ± 9.3 | 0.529 |
| EuroScore II (%) | 12.7 ± 12.3 | 13.1 ± 12.9 | 11.9 ± 11.4 | 0.488 |
| Significant CAD | 49/68 (72.1%) | 28/44 (63.6%) | 21/24 (87.5%) | 0.048 |
| Prior cardiothoracic surgery | 26/68 (38.2%) | 16/44 (36.4%) | 10/24 (41.7%) | 0.667 |
| Atrial fibrillation | 43/68 (63.2%) | 27/44 (61.4%) | 16/24 (66.7%) | 0.665 |
| Prior stroke | 6/68 (8.8%) | 3/44 (6.8%) | 3/24 (12.5%) | 0.658 |
| Increased retention values (Creatinine ≥ 1.3 mg/dL) | 36/68 (52.9%) | 24/44 (54.5%) | 12/24 (50.0%) | 0.720 |
| Sleep apnoea syndrome | 6/68 (8.8%) | 2/44 (4.5%) | 4/24 (16.7%) | 0.175 |
| Pulmonary disease | 12/68 (17.6%) | 10/44 (22.7%) | 2/24 (8.3%) | 0.190 |
| Diabetes mellitus | 19/68 (27.9%) | 14/44 (31.8%) | 5/24 (20.8%) | 0.335 |
| Cancer (‘state after’ included) | 5/68 (7.4%) | 2/44 (4.5%) | 3/24 (12.5%) | 0.337 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Geis, N.A.; Göbbel, A.; Kreusser, M.M.; Täger, T.; Katus, H.A.; Frey, N.; Schlegel, P.; Raake, P.W. Impact of Percutaneous Mitral Valve Repair Using the MitraClipTM System on Ventricular Arrhythmias and ICD Therapies. Life 2022, 12, 344. https://doi.org/10.3390/life12030344
Geis NA, Göbbel A, Kreusser MM, Täger T, Katus HA, Frey N, Schlegel P, Raake PW. Impact of Percutaneous Mitral Valve Repair Using the MitraClipTM System on Ventricular Arrhythmias and ICD Therapies. Life. 2022; 12(3):344. https://doi.org/10.3390/life12030344
Chicago/Turabian StyleGeis, Nicolas A., Anna Göbbel, Michael M. Kreusser, Tobias Täger, Hugo A. Katus, Norbert Frey, Philipp Schlegel, and Philip W. Raake. 2022. "Impact of Percutaneous Mitral Valve Repair Using the MitraClipTM System on Ventricular Arrhythmias and ICD Therapies" Life 12, no. 3: 344. https://doi.org/10.3390/life12030344
APA StyleGeis, N. A., Göbbel, A., Kreusser, M. M., Täger, T., Katus, H. A., Frey, N., Schlegel, P., & Raake, P. W. (2022). Impact of Percutaneous Mitral Valve Repair Using the MitraClipTM System on Ventricular Arrhythmias and ICD Therapies. Life, 12(3), 344. https://doi.org/10.3390/life12030344