


Early and Direct Endoscopic Stone Removal in the Moderate Grade of Acute Cholangitis with Choledocholithiasis Was Safe and Effective: A Prospective Study

 , , , and
, , , and
Abstract
1. Introduction
2. Patients and Methods
2.1. Study Design
2.2. Research Ethics
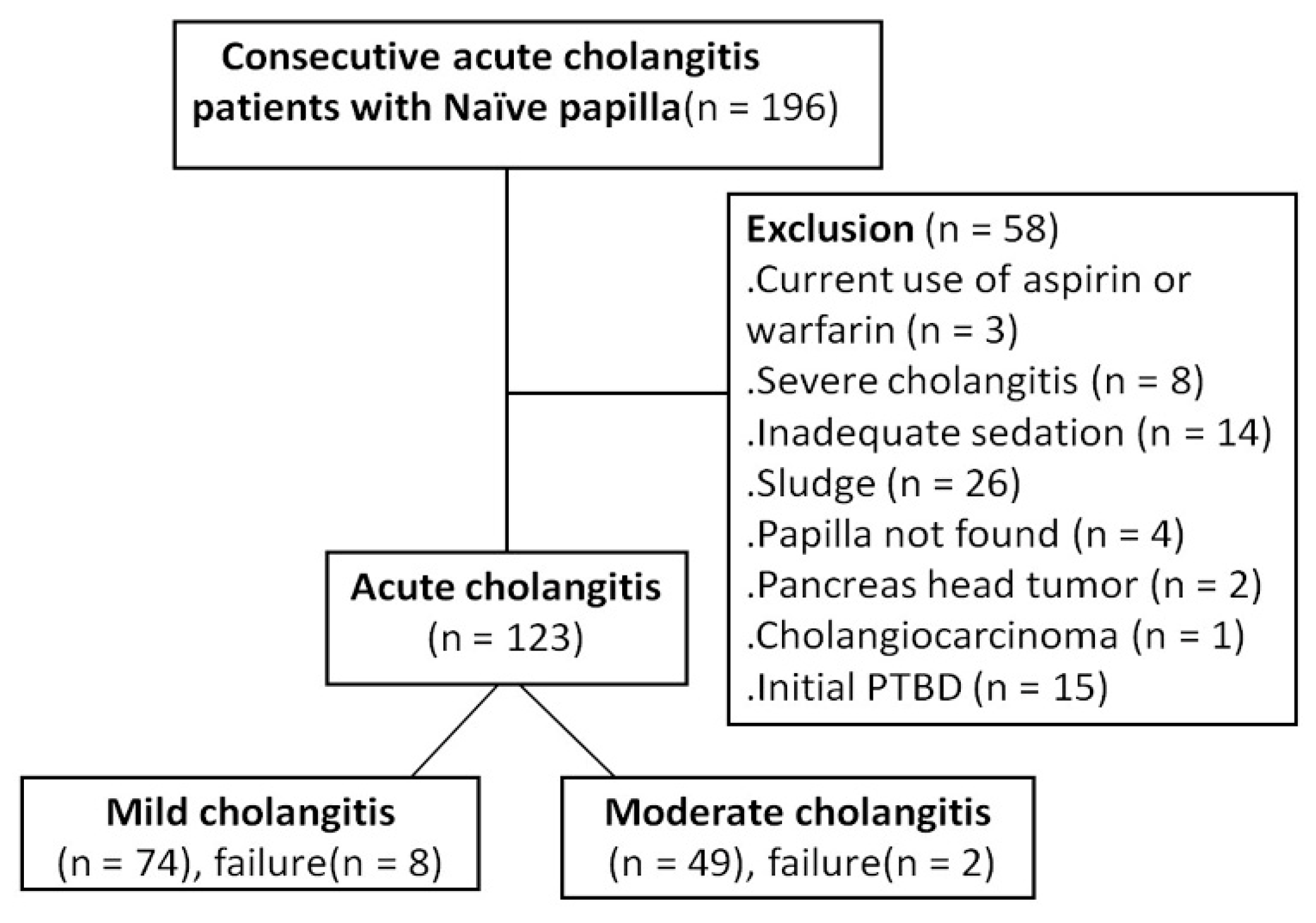
2.3. Inclusion Criteria
2.4. Eligibility Criteria
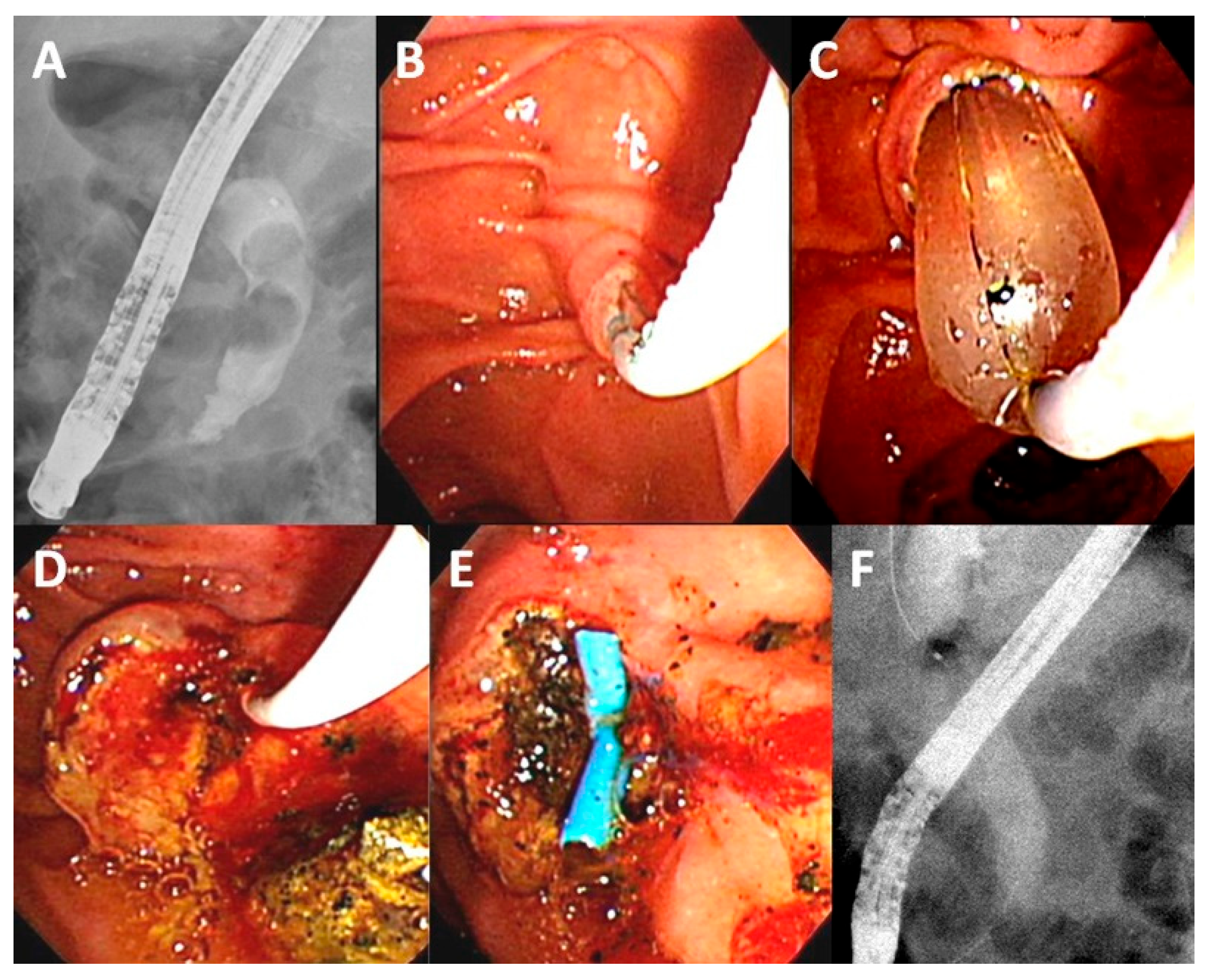
2.5. ERCP Procedure
2.6. Data Records
2.7. Statistical Analysis
2.8. Endpoints
3. Results
3.1. Population Characteristics
3.2. Endoscopic Findings
3.3. Treatment Outcomes and Complications
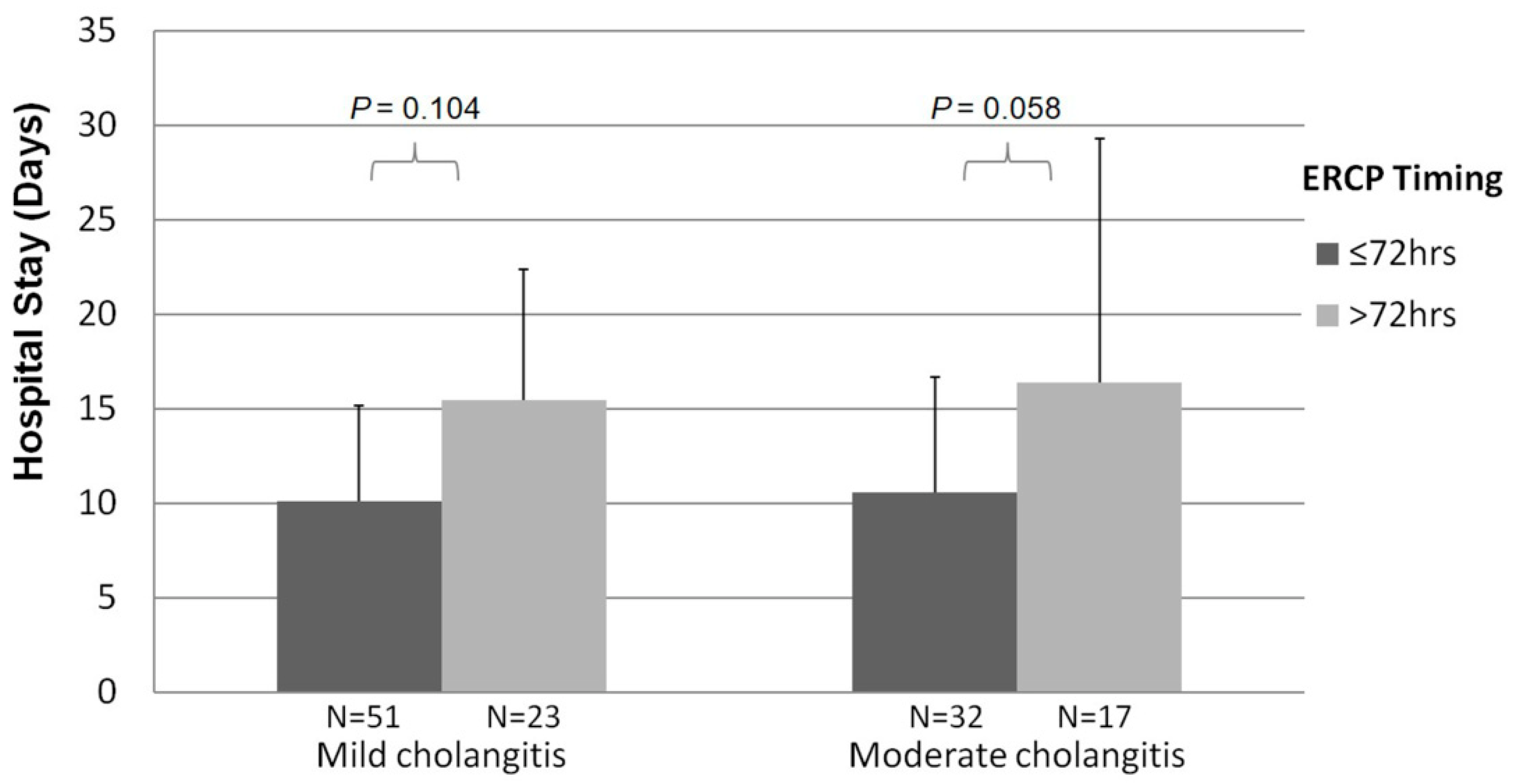
3.4. Timing of Single-Stage Stone Extraction during ERCP
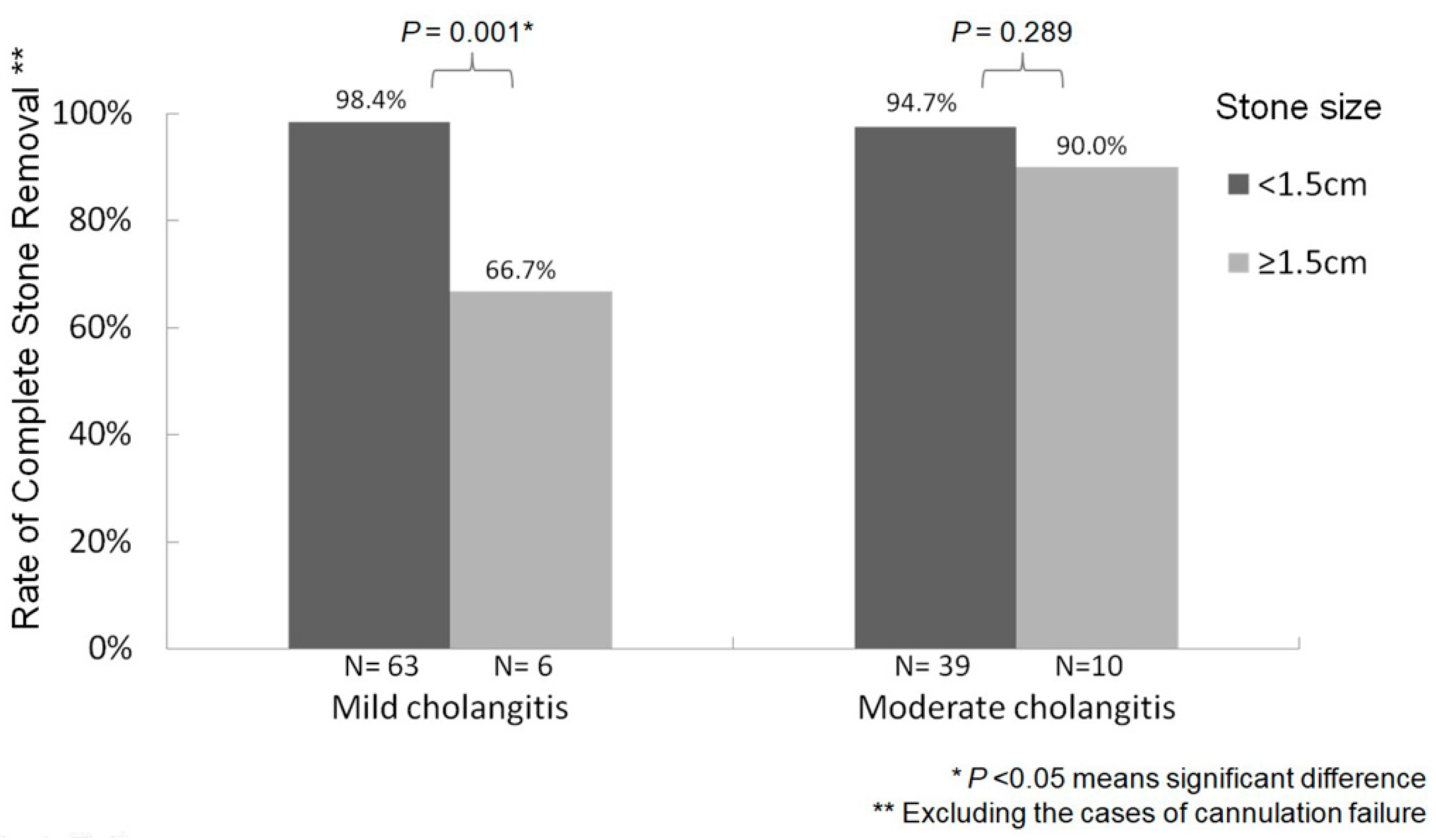
3.5. Stone Size during Single-Stage Stone Extraction by ERCP
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kimura, Y.; Takada, T.; Strasberg, S.M.; Pitt, H.A.; Gouma, D.J.; Garden, O.J.; Büchler, M.W.; Windsor, J.A.; Mayumi, T.; Yoshida, M.; et al. TG13 current terminology, etiology, and epidemi ology of acute cholangitis and cholecystitis. J. Hepato-Biliary-Pancreat. Sci. 2013, 20, 8–23. [Google Scholar] [CrossRef]
- Kinney, T.P. Management of Ascending Cholangitis. Gastrointest. Endosc. Clin. N. Am. 2007, 17, 289–306. [Google Scholar] [CrossRef]
- Chopra, K.B.; Peters, R.A.; O’Toole, P.A.; Williams, S.G.; Gimson, A.E.; Lombard, M.G.; Westaby, D. Randomised study of endoscopic biliary endoprosthesis versus duct clearance for bileduct stones in high-risk patients. Lancet 1996, 348, 791–793. [Google Scholar] [CrossRef]
- Parikh, M.P.; Wadhwa, V.; Thota, P.N.; Lopez, R.; Sanaka, M.R. Outcomes Associated With Timing of ERCP in Acute Cholangitis Secondary to Choledocholithiasis. J. Clin. Gastroenterol. 2018, 52, e97–e102. [Google Scholar] [CrossRef]
- Maple, J.T.; Ben-Menachem, T.; Anderson, M.A.; Appalaneni, V.; Banerjee, S.; Cash, B.D.; Fisher, L.; Harrison, M.E.; Fanelli, R.D.; Fukami, N.; et al. ASGE Standards of Practice Committee: The role of endoscopy in the management of choledocholithiasis. Gastrointest. Endosc. 2011, 74, 731–744. [Google Scholar] [CrossRef]
- Miura, F.; Takada, T.; Strasberg, S.M.; Solomkin, J.; Pitt, H.A.; Gouma, D.J.; Garden, O.J.; Büchler, M.W.; Yoshida, M.; Mayumi, T.; et al. TG13 flowchart for the management of acute cholangitis and cholecystitis. J. Hepato-Biliary-Pancreatic Sci. 2013, 20, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Ito, T.; Sai, J.K.; Okubo, H.; Saito, H.; Ishii, S.; Kanazawa, R.; Tomishima, K.; Watanabe, S.; Shiina, S. Safety of immediate endoscopic sphincterotomy in acute suppurative cholangitis caused by choledocholithiasis. World J. Gastrointest. Endosc. 2016, 8, 180–185. [Google Scholar] [CrossRef] [PubMed]
- Eto, K.; Kawakami, H.; Haba, S.; Yamato, H.; Okuda, T.; Yane, K.; Hayashi, T.; Ehira, N.; Onodera, M.; Matsumoto, R.; et al. Single-stage endoscopic treatment for mild to moderate acute cholangitis associated with choledocholithiasis: A multicenter, non-randomized, open-label and exploratory clinical trial. J. Hepato-Biliary-Pancreatic Sci. 2015, 22, 825–830. [Google Scholar] [CrossRef] [PubMed]
- Jang, S.E.; Park, S.W.; Lee, B.S.; Shin, C.M.; Lee, S.H.; Kim, J.-W.; Jeong, S.-H.; Kim, N.; Lee, D.H.; Park, J.K.; et al. Management for CBD Stone-Related Mild to Moderate Acute Cholangitis: Urgent Versus Elective ERCP. Am. J. Dig. Dis. 2013, 58, 2082–2087. [Google Scholar] [CrossRef]
- Hung, K.; Kuo, C.; Tsai, C.; Chiu, Y.; Lu, L.; Wu, C.; Sou, F.; Huang, P.; Tai, W.; Liang, C.; et al. Single-stage retrograde endoscopic common bile duct stone removal might be sufficient in moderate acute cholangitis with a stone size ≤12 mm: A retrospective cohort study with propensity score matching. Adv. Dig. Med. 2020, 7, 188–194. [Google Scholar] [CrossRef]
- Sato, J.; Nakahara, K.; Morita, R.; Morita, N.; Suetani, K.; Michikawa, Y.; Kobayashi, S.; Itoh, F. Efficacy and Safety of Single-Session Endoscopic Stone Removal for Acute Cholangitis Associated with Choledocholithiasis. Can. J. Gastroenterol. Hepatol. 2018, 2018, 3145107. [Google Scholar] [CrossRef]
- Miura, F.; Okamoto, K.; Takada, T.; Strasberg, S.M.; Asbun, H.J.; Pitt, H.A.; Gomi, H.; Solomkin, J.; Schlossberg, D.; Han, H.-S.; et al. Tokyo Guidelines 2018: Initial management of acute biliary infection and flowchart for acute cholangitis. J. Hepato-Biliary-Pancreatic Sci. 2018, 25, 31–40. [Google Scholar] [CrossRef]
- Kiriyama, S.; Takada, T.; Strasberg, S.M.; Solomkin, J.S.; Mayumi, T.; Pitt, H.A.; Gouma, D.J.; Garden, O.J.; Büchler, M.W.; Yokoe, M.; et al. New diagnostic criteria and severity assessment of acute cholangitis in revised Tokyo guidelines. J. Hepato-Biliary-Pancreatic Sci. 2012, 19, 548–556. [Google Scholar] [CrossRef]
- Kuo, C.M.; Chiu, Y.C.; Changchien, C.S.; Tai, W.C.; Chuah, S.K.; Hu, T.H.; Kuo, Y.H.; Kuo, C.H. Endoscopic papillary balloon dilation for removal of bile duct stones: Evaluation of outcomes and complications in 298 patients. J. Clin. Gastroenterol. 2012, 46, 860–864. [Google Scholar] [CrossRef]
- Kuo, C.-M.; Chiu, Y.-C.; Liang, C.-M.; Lu, L.-S.; Tai, W.-C.; Kuo, Y.-H.; Wu, C.-K.; Chuah, S.-K.; Changchien, C.-S.; Kuo, C.-H. Limited precut sphincterotomy combined with endoscopic papillary balloon dilation for common bile duct stone removal in patients with difficult biliary cannulation. BMC Gastroenterol. 2016, 16, 70. [Google Scholar] [CrossRef][Green Version]
- Dumonceau, J.-M.; Andriulli, A.; Elmunzer, B.J.; Mariani, A.; Meister, T.; Deviere, J.; Marek, T.; Baron, T.H.; Hassan, C.; Testoni, P.A.; et al. Prophylaxis of post-ERCP pancreatitis: European Society of Gastrointestinal Endoscopy (ESGE) Guideline—Updated June 2014. Endoscopy 2014, 46, 799–815. [Google Scholar] [CrossRef]
- Park, C.-H.; Paik, W.H.; Park, E.T.; Shim, C.S.; Lee, T.Y.; Kang, C.; Noh, M.H.; Yi, S.Y.; Lee, J.K.; Hyun, J.J.; et al. Aggressive intravenous hydration with lactated Ringer’s solution for prevention of post-ERCP pancreatitis: A prospective randomized multicenter clinical trial. Endoscopy 2018, 50, 378–385. [Google Scholar] [CrossRef]
- Haraldsson, E.; Lundell, L.; Swahn, F. Results of an inter- and intraobserver agreement study. U Eur. Gastroenterol. J. 2017, 5, 504–510. [Google Scholar] [CrossRef]
- Kuo, C.-M.; Chiu, Y.-C.; Liang, C.-M.; Wu, C.-K.; Lu, L.-S.; Tai, W.-C.; Kuo, Y.-H.; Wu, K.-L.; Chuah, S.-K.; Kuo, C.-H. The efficacy of limited endoscopic sphincterotomy plus endoscopic papillary large balloon dilation for removal of large bile duct stones. BMC Gastroenterol. 2019, 19, 93. [Google Scholar] [CrossRef]
- Tringali, A.; Costa, D.; Fugazza, A.; Colombo, M.; Khalaf, K.; Repici, A.; Anderloni, A. Endoscopic management of difficult common bile duct stones: Where are we now? A comprehensive review. World J. Gastroenterol. 2021, 27, 7597–7611. [Google Scholar] [CrossRef]
- Bursac, Z.; Gauss, C.H.; Williams, D.K.; Hosmer, D.W. Purposeful selection of variables in logistic regression. Source Code Biol. Med. 2008, 3, 17. [Google Scholar] [CrossRef] [PubMed]
- Cotton, P.B.; Eisen, G.M.; Aabakken, L.; Baron, T.H.; Hutter, M.M.; Jacobson, B.C.; Mergener, K.; Nemcek, A., Jr.; Petersen, B.T.; Petrini, J.L.; et al. A lexicon for endoscopic adverse events: Report of an ASGE workshop. Gastrointest. Endosc. 2010, 71, 446–454. [Google Scholar] [CrossRef] [PubMed]
- Freeman, M.L.; Nelson, D.B.; Sherman, S.; Haber, G.B.; Herman, M.E.; Dorsher, P.J.; Moore, J.P.; Fennerty, M.B.; Ryan, M.E.; Shaw, M.J.; et al. Complications of Endoscopic Biliary Sphincterotomy. New Engl. J. Med. 1996, 335, 909–919. [Google Scholar] [CrossRef] [PubMed]
- Liao, W.; Tu, Y.; Wu, M.; Wang, H.; Lin, J.; Leung, J.W.; Chien, K. Balloon Dilation With Adequate Duration Is Safer Than Sphincterotomy for Extracting Bile Duct Stones: A Systematic Review and Meta-analyses. Clin. Gastroenterol. Hepatol. 2012, 10, 1101–1109. [Google Scholar] [CrossRef] [PubMed]
- Sugiyama, M.; Atomi, Y. The benefits of endoscopic nasobiliary drainage without sphincterotomy for acute cholangitis. Am. J. Gastroenterol. 1998, 93, 2065–2068. [Google Scholar] [CrossRef]
- Boender, J.; Nix, G.A.; De Ridder, M.A.; Dees, J.; Schütte, H.E.; Van Buuren, H.R.; Van Blankenstein, M. Endoscopic sphincterotomy and biliary drainage in patients with cholangitis due to common bile duct stones. Am. J. Gastroenterol. 1995, 90, 233–238. [Google Scholar]
- Sawas, T.; Arwani, N.; Al Halabi, S.; Vargo, J. Sphincterotomy with endoscopic biliary drainage for severe acute cholangitis: A meta-analysis. Endosc. Int. Open 2017, 5, E103–E109. [Google Scholar] [CrossRef][Green Version]
- Hung, T.H.; Tseng, C.W.; Chen, Y.C.; Tseng, K.C.; Hsieh, Y.H.; Tsai, C.C. Endoscopic papillary balloon dilation decreases the risk of bleeding in cirrhotic patients compared with endoscopic biliary sphincterotomy: A national population-based study. Medicine 2019, 98, e16529. [Google Scholar] [CrossRef]
- Hui, C.K.; Lai, K.C.; Yuen, M.F.; Ng, M.; Chan, C.K.; Hu, W.; Wong, B.C. Does the addition of endoscopic sphincterotomy to stent insertion improve drainage of the bile duct in acute suppurative cholangitis? Gastrointest. Endosc. 2003, 58, 500–504. [Google Scholar] [CrossRef]
- Wiggins, T.; Markar, S.R.; MacKenzie, H.; Faiz, O.; Mukherjee, D.; Khoo, D.E.; Hanna, G.B. Optimum timing of emergency cholecystectomy for acute cholecystitis in England: Population-based cohort study. Surg. Endosc. 2019, 33, 2495–2502. [Google Scholar] [CrossRef]
- Polo, M.; Duclos, A.; Polazzi, S.; Payet, C.; Lifante, J.C.; Cotte, E.; Barth, X.; Glehen, O.; Passot, G. Acute Cholecystitis—Optimal Timing for Early Cholecystectomy: A French Nationwide Study. J. Gastrointest. Surg. 2015, 19, 2003–2010. [Google Scholar] [CrossRef]
- Zafar, S.N.; Obirieze, A.; Adesibikan, B.; Cornwell, E.E.; Fullum, T.M.; Tran, D.D. Optimal Time for Early Laparoscopic Cholecystectomy for Acute Cholecystitis. JAMA Surg. 2015, 150, 129–136. [Google Scholar] [CrossRef]
- Jansen, B.; Peters, G. Foreign body associated infection. J. Antimicrob. Chemother. 1993, 32, 69–75. [Google Scholar] [CrossRef]
- Navaneethan, U.; Jayanthi, V.; Mohan, P. Pathogenesis of cholangitis in obstructive jaundice-revisited. Minerva Gastroenterol. e Dietol. 2011, 57, 97–104. [Google Scholar]
- Swidsinski, A.; Schlien, P.; Pernthaler, A.; Gottschalk, U.; Bärlehner, E.; Decker, G.; Strassburg, J.; Loening-Baucke, V.; Hoffmann, U.; Seehofer, D.; et al. Bacterial biofilm within diseased pancreatic and biliary tracts. Gut 2005, 54, 388–395. [Google Scholar] [CrossRef]
- Gomi, H.; Solomkin, J.; Schlossberg, D.; Okamoto, K.; Takada, T.; Strasberg, S.M.; Ukai, T.; Endo, I.; Iwashita, Y.; Hibi, T.; et al. Tokyo Guidelines 2018: Antimicrobial therapy for acute cholangitis and cholecystitis. J. Hepato-Biliary-Pancreatic Sci. 2018, 25, 3–16. [Google Scholar] [CrossRef]
- Haal, S.; Wielenga, M.C.B.; Fockens, P.; Leseman, C.A.; Ponsioen, C.Y.; van Soest, E.J.; van Wanrooij, R.L.J.; Sieswerda, E.; Voermans, R.P. Antibiotic Therapy of 3 Days May Be Sufficient After Biliary Drainage for Acute Cholangitis: A Systematic Review. Am. J. Dig. Dis. 2021, 66, 4128–4139. [Google Scholar] [CrossRef]
- Kim, H.J.; Choi, H.S.; Park, J.H.; Park, D.I.; Cho, Y.K.; Sohn, C.I.; Jeon, W.K.; Kim, B.I.; Choi, S.H. Factors influencing the technical difficulty of endoscopic clearance of bile duct stones. Gastrointest. Endosc. 2007, 66, 1154–1160. [Google Scholar] [CrossRef]
- Liang, C.M.; Chiu, Y.C.; Lu, L.S.; Wu, C.K.; Sou, F.M.; Huang, P.Y.; Ma, T.L.; Kuo, C.H.; Chuah, S.K.; Kuo, C.M. Optimal Timing of Single-Stage Retrograde Endoscopic Common Bile Duct Stone Removal in Mild and Moderate Acute Cholangitis: A Prospective Trial. Available online: https://www.researchsquare.com/article/rs-26612/v1 (accessed on 22 June 2020).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Mild Acute Cholangitis n = 74 (*) | Moderate Acute Cholangitis n = 49 (*) | p-Value |
|---|---|---|---|
| Age (year) | 62.9 ± 16.1 | 76.0 ± 11.2 | 0.003 |
| Gender (F) | 33 (44.6) | 18 (36.7) | 0.386 |
| Smoking | 15 (20.3) | 9 (18.4) | 0.794 |
| Alcohol | 13 (17.6) | 8 (16.3) | 0.858 |
| Diabetes Mellitus | 14 (18.9) | 21 (42.9) | 0.004 |
| Hypertension | 37 (50.0) | 35 (71.4) | 0.018 |
| ASA score I/II/II/IV | 31/31/8/4 | 9/21/12/7 | 0.012 |
| Body temperature (°C) | 36.8 ± 0.9 | 37.8 ± 1.4 | <0.001 |
| WBC (×1000/μL) | 10.0 ± 5.4 | 13.7 ± 4.3 | 0.141 |
| Platelet (×1000/μL) | 235.5 ± 91.7 | 194.6 ± 74.2 | 0.102 |
| PT (s) | 10.6 ± 0.8 | 11.7 ± 2.8 | 0.007 |
| APTT (s) | 27.4 ± 3.4 | 29.8 ± 4.9 | 0.038 |
| Albumin (mg/dL) | 3.7 ± 0.4 | 3.3 ± 0.5 | 0.488 |
| eGFR (mL/min/1.732) | 70.5 ± 34.7 | 48.8 ± 25.0 | 0.063 |
| AST (U/L) | 200.8 ± 252.2 | 228.4 ± 192.4 | 0.914 |
| ALT (U/L) | 260.7 ± 209.6 | 243.9 ± 210.7 | 0.583 |
| Bilirubin (total) (mg/dL) | 5.7 ± 4.6 | 5.9 ± 4.4 | 0.265 |
| ALK-P (U/L) | 205.1 ± 133.4 | 231.8 ± 126.3 | 0.845 |
| CRP (U/L) | 45.7 ± 67.9 | 106.7 ± 74.0 | 0.017 |
| Characteristics | Mild Acute Cholangitis n = 74 (*) | Moderate Acute Cholangitis n = 49 (*) | p-Value |
|---|---|---|---|
| Pancreatic duct filling | 2 (2.8) | 3 (6.1) | 0.373 |
| Papilla type(I~IV) | 59/7/5/3 | 38/7/2/2 | 0.803 |
| Periampullary diverticulum | 27 (36.5) | 27 (55.1) | 0.042 |
| EPBD | 68 (91.9) | 44 (89.8) | 0.690 |
| EST | 16 (21.6) | 6 (12.2) | 0.184 |
| Stones size (cm) | 0.9 ± 0.4 | 1.1 ± 0.5 | 0.157 |
| Stone number | 1.8 ± 1.2 | 1.4 ± 1.0 | 0.078 |
| Mean CBD diameter (cm) | 1.3 ± 0.4 | 1.5 ± 0.4 | 0.856 |
| Balloon extraction | 65 (94.2) | 45 (91.8) | 0.614 |
| Basket use | 8 (11.6) | 8 (16.3) | 0.459 |
| ERBD | 16 (21.6) | 15 (30.6) | 0.261 |
| Procedure Time (min) | 24.3 ± 11.4 | 23.8 ± 11.4 | 0.661 |
| Complete stone removal | 66 (89.2) | 47 (95.9) | 0.181 |
| Adverse Events | Mild Acute Cholangitis n = 74 (*) | Moderate Acute Cholangitis n = 49 (*) | p-Value |
|---|---|---|---|
| Hospital stay (days) | 11.8 ± 6.2 | 12.6 ± 9.3 | 0.326 |
| Hospital cost (USD) | 2912.1 ± 1280.7 | 3409.8 ± 2741.9 | 0.026 |
| PEP | 4 (5.4) | 1 (2.0) | 0.355 |
| Bleeding | 1 (1.4) | 0 (0) | 0.414 |
| Perforation | 1 (1.4) | 0 (0) | 0.414 |
| Pneumonia (30 days) | 1 (1.4) | 1 (2.0) | 0.767 |
| Mortality (30 days) | 0 (0) | 0 (0) | - |
| ERCP Timing From ER (Mean ± SD) (h) | Early (≤72 h) (35.2 ± 20.4), n = 83 | Delayed (>72 h) (161.2 ± 85.1), n = 40 | ||||
|---|---|---|---|---|---|---|
| Mild Cholangitis n = 51 (*) | Moderate Cholangitis n = 32 (*) | p-Value | Mild Cholangitis n = 23 (*) | Moderate Cholangitis n = 17 (*) | p-Value | |
| Age (y/o) | 62.0 ± 16.6 | 76.0 ± 10.6 | 0.004 | 65.0 ± 15.2 | 76.0 ± 12.8 | 0.279 |
| CRP (U/L) | 44.8 ± 63.0 | 123.3 ± 70.0 | 0.001 | 47.6 ± 79.0 | 74.3 ± 73.3 | 0.293 |
| Stone ≥ 1.5 cm | 2 (3.9) | 7 (21.2) | 0.010 | 5 (21.7) | 3 (17.6) | 0.749 |
| Complete CBD removal | 48 (94.1) | 30 (93.8) | 0.945 | 18 (78.3) | 17 (100.0) | 0.040 |
| PEP | 3 (5.9) | 1 (3.1) | 0.568 | 1 (4.3) | 0 (0) | 0.384 |
| Bleeding | 1 (2.0) | 0 (0) | 0.425 | 0 (0) | 0 (0) | - |
| Perforation | 0 (0) | 0 (0) | - | 1 (4.3) | 0 (0) | 0.384 |
| ERBD | 13 (25.5) | 14 (43.8) | 0.084 | 3 (13.0) | 1 (5.9) | 0.455 |
| Hospital stay (days) | 10.1 ± 5.1 | 10.6 ± 6.2 | 0.408 | 15.5 ±.6.9 | 16.4 ± 12.9 | 0.196 |
| Hospital cost (USD) | 2806.5 ± 1313.4 | 3076.5 ± 1953.9 | 0.312 | 3175.7 ± 1185.5 | 4037.0 ± 3810.0 | 0.050 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liang, C.-M.; Chiu, Y.-C.; Lu, L.-S.; Wu, C.-K.; Sou, F.-M.; Chiu, S.-M.; Lee, Y.-C.; Huang, P.-Y.; Chuah, S.-K.; Kuo, C.-M. Early and Direct Endoscopic Stone Removal in the Moderate Grade of Acute Cholangitis with Choledocholithiasis Was Safe and Effective: A Prospective Study. Life 2022, 12, 2000. https://doi.org/10.3390/life12122000
Liang C-M, Chiu Y-C, Lu L-S, Wu C-K, Sou F-M, Chiu S-M, Lee Y-C, Huang P-Y, Chuah S-K, Kuo C-M. Early and Direct Endoscopic Stone Removal in the Moderate Grade of Acute Cholangitis with Choledocholithiasis Was Safe and Effective: A Prospective Study. Life. 2022; 12(12):2000. https://doi.org/10.3390/life12122000
Chicago/Turabian StyleLiang, Chih-Ming, Yi-Chun Chiu, Lung-Sheng Lu, Cheng-Kun Wu, Fai-Meng Sou, Shao-Ming Chiu, Yu-Chi Lee, Pao-Yuan Huang, Seng-Kee Chuah, and Chung-Mou Kuo. 2022. "Early and Direct Endoscopic Stone Removal in the Moderate Grade of Acute Cholangitis with Choledocholithiasis Was Safe and Effective: A Prospective Study" Life 12, no. 12: 2000. https://doi.org/10.3390/life12122000
APA StyleLiang, C.-M., Chiu, Y.-C., Lu, L.-S., Wu, C.-K., Sou, F.-M., Chiu, S.-M., Lee, Y.-C., Huang, P.-Y., Chuah, S.-K., & Kuo, C.-M. (2022). Early and Direct Endoscopic Stone Removal in the Moderate Grade of Acute Cholangitis with Choledocholithiasis Was Safe and Effective: A Prospective Study. Life, 12(12), 2000. https://doi.org/10.3390/life12122000