
Aphasic Syndromes in Cerebral Venous and Dural Sinuses Thrombosis—A Review of the Literature

 ,
, 
Abstract
1. Introduction
1.1. Definition of Aphasia
1.2. Language Localization
- Broca’s area—the posterior part of the left third frontal gyrus (F3)—Brodmann areas 44 and 45;
- Left insula’s cortex and the underlying white matter;
- Left Rolandic operculum—the lower part of the motor area (Fa);
- Left premotor and prefrontal areas (forward and superior of Broca’s area);
- The supplementary motor area;
- Wernicke’s area: the posterior part of the first two temporal gyri-T1/T2 (Brodmann area 22);
- The inferior parietal lobes: the angular gyrus (Brodmann area 39), and the supramarginal gyrus (Brodmann area 40);
- The anterior part of the temporal lobe.
1.3. Types of Aphasic Syndromes
- Broca’s aphasia (10–15%);
- Wernicke’s aphasia (15%);
- Conduction aphasia (15%);
- Transcortical aphasias:
- Transcortical motor aphasia (15–20%);
- Transcortical sensory aphasia;
- Mixed transcortical aphasia.
- Global aphasias (24–38%);
- Anomic plus aphasias (20%);
- Atypical aphasias: mixed aphasias, thalamic aphasias, and capsulo-striatal aphasias (10%).
1.4. Etiology of Aphasia
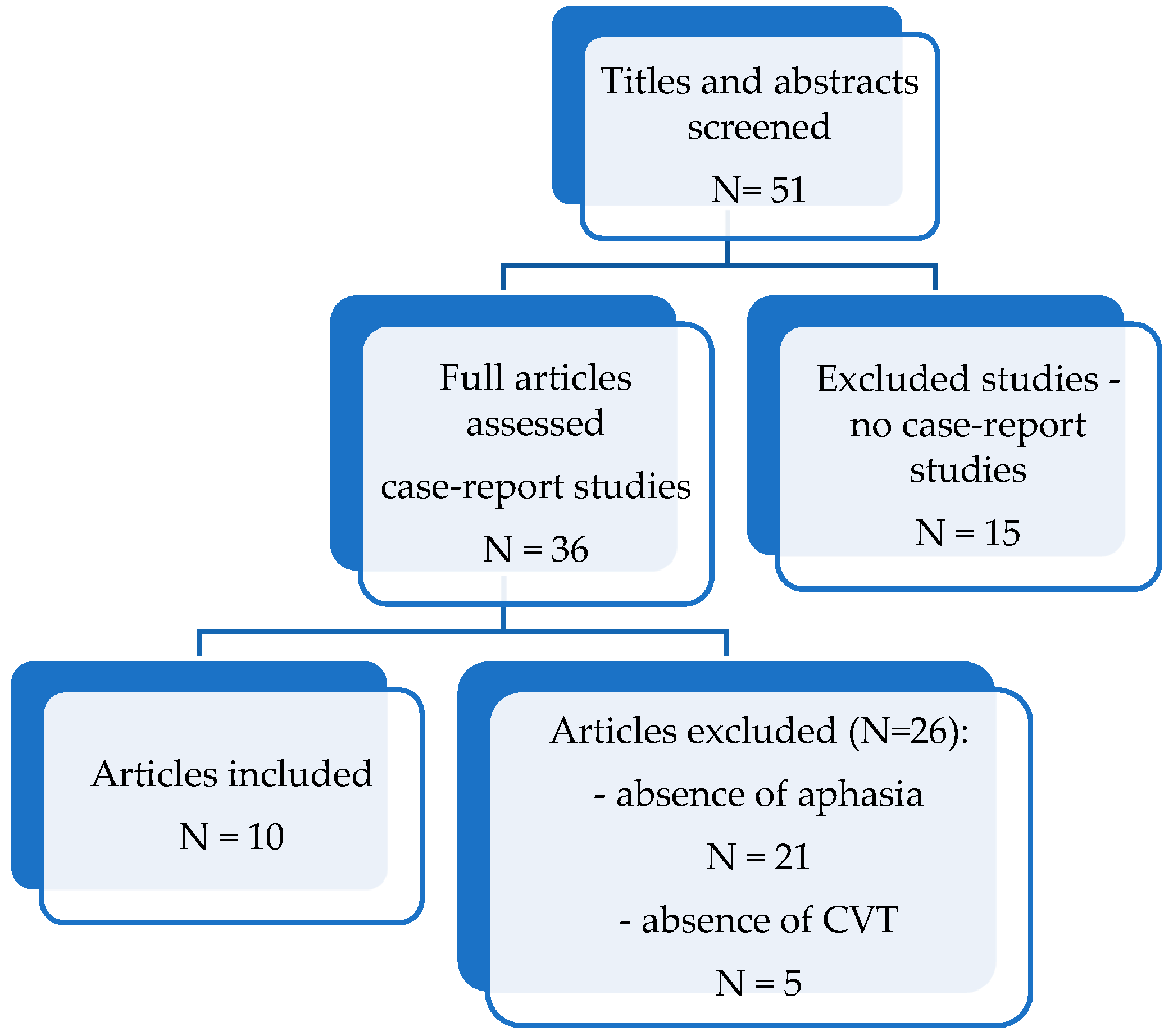
2. Materials and Methods
- (1)
- Presence of language disturbances (aphasia, dysphasia) and description of aphasia ‘s type or characteristics;
- (2)
- Case-report studies published between 2012–2022;
- (3)
- Adult human studies;
- (4)
- Articles written in English;
- (5)
- The patients included in the study were diagnosed based on an imaging examination: computed tomography (CT), computed tomography venography (CTV), magnetic resonance imaging (MRI), magnetic resonance venography (MRV), intra-arterial angiography (Digital Substraction Angiography—DSA);
- (6)
- Detailed, reliable medical history, physical examination, results of laboratory and imaging examinations were required.
3. Results
4. Discussion
- Superior Sagittal Sinus (SSS) Thrombosis
- 2.
- Lateral Sinus (LS) Thrombosis
- 3.
- Isolated Cortical Veins Thrombosis
- 4.
- Deep Cerebral Veins Thrombosis
- -
- aphasia is commonly the consequence of concomitant left transverse sinus thrombosis with left cortical temporal veins, followed by the superior sagittal sinus thrombosis with extension into tributary fronto-parietal cortical veins;
- -
- depending on the site and the size of the brain damage (cerebral vasogenic/cytotoxic edema, venous infarction, intracranial hypertension), the most frequent types of aphasias are: non-fluent aphasias-Broca’s aphasia and anomic plus aphasia (if the lesions are situated in the anterior language areas), fluent aphasias-Wernicke’s aphasia, transcortical sensory aphasia (if the lesions are situated in the posterior language areas), mixed or global aphasias (in the cases of larger lesions);
- -
- in LS sinus thrombosis (the transversal portion) associated with left cortical temporal veins thrombosis, the most common type of aphasia is Wernicke’s aphasia (40%) [16];
- -
- in many cases, the LS thrombosis spreads to the SSS, symptoms and signs of SSS thrombosis depending on the involvement of cerebral veins and other dural sinuses. The most often involved are the superior cerebral veins (Rolandic, parieto-occipital and posterior temporal) which empty into the SSS. If the thrombosis spreads to the deep veins system, altering the Ascending Reticular Activating System (ARAS), awakening alteration may occur;
- -
- the clinical picture depends on the location and the dimensions of cerebral lesion: extensive lesions can determine global aphasia, or mixed transcortical aphasias; meanwhile smaller lesions might determine Wernicke’s aphasia, transcortical sensory aphasia, Broca aphasia or anomic aphasia.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ferro, J.M.; Canhaão, P.; Stam, J.; Bousser, M.-G.; Barinagarrementeria, F. Prognosis of cerebral vein and dural sinus thrombosis: Results of the International Study on Cerebral Vein and Dural Sinus Thrombosis (ISCVT). Stroke 2004, 35, 664–670. [Google Scholar] [CrossRef]
- Sparaco, M.; Feleppa, M.; Bigal, M.E. Cerebral Venous Thrombosis and Headache-A Case-Series. Headache 2015, 55, 806–814. [Google Scholar] [CrossRef] [PubMed]
- Jianu, D.C.; Jianu, S.N.; Munteanu, G.; Dan, F.T.; Bârsan, C. Cerebral Vein and Dural Sinus Thrombosis. In Ischemic Stroke of Brain; Intech Open: London, UK, 2018; Chapter 3. [Google Scholar] [CrossRef]
- Bousser, M.-G.; Ferro, J.M. Cerebral venous thrombosis: An update. Lancet Neurol. 2007, 6, 162–170. [Google Scholar] [CrossRef]
- Devasagayam, S.; Wyatt, B.; Leyden, J.; Kleinig, T. Cerebral Venous Sinus Thrombosis Incidence Is Higher Than Previously Thought: A retrospective population-based study. Stroke 2016, 47, 2180–2182. [Google Scholar] [CrossRef] [PubMed]
- Damak, M.; Crassard, I.; Wolff, V.; Bousser, M.-G. Isolated Lateral Sinus Thrombosis: A series of 62 patients. Stroke 2009, 40, 476–481. [Google Scholar] [CrossRef]
- Ferro, J.; Lopes, M.G.; Rosas, M.; Ferro, M.; Fontes, J. Long-Term Prognosis of Cerebral Vein and Dural Sinus Thrombosis: Results of the VENOPORT study. Cerebrovasc. Dis. 2002, 13, 272–278. [Google Scholar] [CrossRef]
- Jianu, D.C.; Jianu, S.N.; Petrica, L.; Dan, T.F.; Munteanu, G. Vascular Aphasias. In Ischemic Stroke; Sanchetee, P., Ed.; Intech Open: London, UK, 2021; Chapter 3; pp. 37–59. [Google Scholar]
- Abou Zeki, D.; Hillis, A. Acquired Disorders of Language and Speech. In Oxford Textbook of Cognitive Neurology and Dementia; Masud, H., Schott, J.M., Eds.; Oxford University Press: Oxford, UK, 2016; Chapter 12; pp. 123–133. [Google Scholar]
- Croquelois, A.; Godefroy, O. Vascular Aphasias. In The Behavioral and Cognitive Neurology of Stroke, 2nd ed.; Godefroy, O., Ed.; Cambridge University Press: Cambridge, UK, 2013; Chapter 7; pp. 65–75/. [Google Scholar]
- Goodglass, H.; Kaplan, E. (Eds.) The Assessment of Aphasia and Related Disorder, 2nd ed.; Lea and Febiger: Philadelphia, PA, USA, 1983. [Google Scholar]
- Swanberg, M.M.; Nasreddine, Z.S.; Mendez, M.F.; Cummings, J.L. Speech and Language. In Goetz, Textbook of Clinical Neurology, 3rd ed.; Christopher, G., Ed.; W.B. Saunders: Philadelphia, PA, USA, 2007; pp. 79–98. Available online: https://www.sciencedirect.com/science/article/pii/B9781416036180100062 (accessed on 1 April 2022)ISBN 9781416036180. [CrossRef]
- Ferro, J.M.; Canhão, P. Cerebral Venous Thrombosis. In Stroke (Pathophysiology, Diagnosis, and Management), 6th ed.; Grotta, J.C., Albers, G.W., Broderick, J.P., Kasner, S.E., Lo, E.H., Mendelow, A.D., Sacco, R.L., Wong, L.K.S., Eds.; Elsevier: Beijing, China, 2016; Chapter 45; pp. 716–730. [Google Scholar]
- Einhäupl, K.; Bousser, M.G.; de Bruijn, S.F.; Ferro, M.; Martinelli, I.; Masuhr, F.; Stam, J. FEFNS guideline on the treatment of cerebral venous sinus thrombosis. Eur. J. Neurol. 2006, 13, 553–559. [Google Scholar] [CrossRef] [PubMed]
- Ayele, B.A.; Abdella, R.I.; Wachamo, L.Z. Reversible anomia and cerebral venous thrombosis: A case report and review of the literature. J. Med. Case Rep. 2022, 16, 56. [Google Scholar] [CrossRef] [PubMed]
- Jianu, D.; Jianu, S.; Dan, T.; Iacob, N.; Munteanu, G.; Motoc, A.; Băloi, A.; Hodorogea, D.; Axelerad, A.; Pleș, H.; et al. Diagnosis and Management of Mixed Transcortical Aphasia Due to Multiple Predisposing Factors, including Postpartum and Severe Inherited Thrombophilia, Affecting Multiple Cerebral Venous and Dural Sinus Thrombosis: Case Report and Literature Review. Diagnostics 2021, 11, 1425. [Google Scholar] [CrossRef]
- Das, S.; Dubey, S.; Pandit, A.; Ray, B.K. Bilateral thalamic lesion presenting as Broca’s type subcortical aphasia in cerebral venous thrombosis: Index case report. BMJ Case Rep. 2021, 14, e240196. [Google Scholar] [CrossRef] [PubMed]
- Ennis, G.; Domingues, N.; Marques, J.S.; Ribeiro, P.; Andrade, C. Cerebral Venous Thrombosis and Its Clinical Diversity. Cureus 2021, 13, e14750. [Google Scholar] [CrossRef]
- Hwang, S.R.; Wang, Y.; Weil, E.L.; Padmanabhan, A.; Warkentin, T.E.; Pruthi, R.K. Cerebral venous sinus thrombosis associated with spontaneous heparin-induced thrombocytopenia syndrome after total knee arthroplasty. Platelets 2021, 32, 936–940. [Google Scholar] [CrossRef] [PubMed]
- Engelmann, A.; DiPastina, K.; Liu, T. The ugly duckling of aphasia: Cerebral venous sinus thrombosis as a mimic of TIA and stroke. J. Community Hosp. Intern. Med. Perspect. 2021, 11, 156–157. [Google Scholar] [CrossRef] [PubMed]
- Lan, R.; Ma, Y.Z.; Shen, X.M.; Wu, J.T.; Gu, C.Q.; Zhang, Y. Bilateral corpus callosum and corona radiata infarction due to cerebral venous sinus thrombosis presenting as headache and acute reversible aphasia: A rare case report. BMC Neurol. 2020, 20, 249. [Google Scholar] [CrossRef] [PubMed]
- Croci, D.M.; Michael, D.; Kahles, T.; Fathi, A.R.; Fandino, J.; Marbacher, S. Ipsilateral Dural Thickening and Enhancement: A Sign of Isolated Cortical Vein Thrombosis? A Case Report and Review of the Literature. World Neurosurg. 2016, 90, 706.e11–706.e14. [Google Scholar] [CrossRef] [PubMed]
- Kuan, W.S. Anomia and Mild Headache: A Subtle Presentation of Cerebral Venous Thrombosis. Hong Kong J. Emerg. Med. 2014, 21, 172–175. [Google Scholar] [CrossRef]
- Tuncel, T.; Ozgun, A.; Emirzeoğlu, L.; Celiïk, S.; Demiïr, S.; Bilgi, O.; Karagoz, B. Broca’s aphasia due to cerebral venous sinus thrombosis following chemotherapy for small cell lung cancer: A case report and review of literature. Oncol. Lett. 2014, 9, 937–939. [Google Scholar] [CrossRef]
- Jianu, D.C.; Jianu, S.N.; Dan, T.F.; Munteanu, G.; Copil, A.; Birdac, C.D.; Motoc, A.G.M.; Axelerad, A.D.; Petrica, L.; Arnautu, S.F.; et al. An Integrated Approach on the Diagnosis of Cerebral Veins and Dural Sinuses Thrombosis (a Narrative Review). Life 2022, 12, 717. [Google Scholar] [CrossRef]
- Ulivi, L.; Squitieri, M.; Cohen, H.; Cowley, P.; Werring, D.J. Cerebral venous thrombosis: A practical guide. Pract. Neurol. 2020, 20, 356–367. [Google Scholar] [CrossRef]
- Bousser, M.G.; Barnett, H.J.M. Cerebral Venous Thrombosis. In Stroke (Pathophysiology, Diagnosis, and Management), 4th ed.; Mohr, J.P., Choi, D.W., Grotta, J.C., Weir, B., Wolf, P.A., Eds.; Churchill Livingstone: Philadelphia, PA, USA, 2004; Chapter 12; pp. 301–325. [Google Scholar]
- Duman, T.; Uluduz, D.; Midi, I.; Bektas, H.; Kablan, Y.; Goksel, B.K.; Milanlioglu, A.; Orken, D.N.; Aluclu, U.; Colakoglu, S.; et al. A Multicenter Study of 1144 Patients with Cerebral Venous Thrombosis: The VENOST Study. J. Stroke Cerebrovasc. Dis. 2017, 26, 1848–1857. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Study | First Author and Year of Publication | Age | Gender | Associated Pathologies | Site of CVT | Type of Aphasia |
|---|---|---|---|---|---|---|
| Reversible anomia and cerebral venous thrombosis: A case report and review of the literature | Biniyam A. Ayele et al. (2022) [15] | 30 | F | two months after dead fetus birth | left transverse, sigmoid sinus (lateral sinus), corresponding cortical veins. | non-fluent aphasia, anomic aphasia |
| Diagnosis and Management of Mixed Transcortical Aphasia Due to Multiple Predisposing Factors, including Postpartum and Severe Inherited Thrombophilia, Affecting Multiple Cerebral Venous and Dural Sinus Thrombosis: Case Report and Literature Review | Dragos, Catalin Jianu et al. (2021) [16] | 38 | F | inherited thrombophilia 18 days postpartum | superior sagittal sinus, the straight sinus, the vein of Galen, the deep venous system on the left, the lateral sinus left internal jugular vein | mixed transcortical aphasia (isolation aphasia) |
| Bilateral thalamic lesion presenting as Broca’s type subcortical aphasia in cerebral venous thrombosis: Index case report | Shambaditya Das et al. (2021) [17] | 35 | M | multiple substances abuse (alcohol, tobacco, and cannabis), thrombophilia—decreased levels of protein C, protein S and antithrombin III | superior sagittal sinus bilateral transverse sinus (lateral sinus) | non-fluent aphasia–Broca‘s aphasia |
| Cerebral Venous Thrombosis and Its Clinical Diversity | Giovana Ennis et al. (2021) [18] | 75 | F | immune thrombocytopenic purpura, arterial hypertension, and pulmonary embolism | superior sagittal sinus the left lateral sinus | global aphasia |
| Cerebral venous sinus thrombosis associated with spontaneous heparin-induced thrombocytopenia syndrome after total knee arthroplasty | Steven R Hwang et al. (2020) [19] | 56 | F | hypertension degenerative osteoarthritis | left transverse and sigmoid sinuses (lateral sinus) left internal jugular vein | unspecified type |
| The ugly duckling of aphasia: cerebral venous sinus thrombosis as a mimic of TIA and stroke | Alexander Engelmann et al. (2020) [20] | 86 | M | colon adenocarcinoma (status post resection); recent surgery for right sphenoid wing meningioma | left transverse (lateral) sinus | fluent aphasia |
| Bilateral corpus callosum and corona radiata infarction due to cerebral venous sinus thrombosis presenting as headache and acute reversible aphasia: A rare case report | Rui Lan et al. (2020) [21] | 30 | F | 20 days post-partum | superior sagittal sinus the left transverse (lateral) sinus | non-fluent aphasia–Broca‘s aphasia |
| Ipsilateral Dural Thickening and Enhancement: A Sign of Isolated Cortical Vein Thrombosis? A Case Report and Review of the Literature | Davide Marco Croci et al. (2016) [22] | 30 | F | 14 days postpartum | left cortical veins thrombosis | global aphasia |
| Anomia and mild headache: A subtle presentation of cerebral venous thrombosis | WS Kuan (2014) [23] | 52 | F | thrombophilia: low levels of protein C activity of 64% expected range 70–130%), protein S activity of 50% (expected range 55–140%) and anti-thrombin III level of 62% (expected range 80–120) | left transverse and sigmoid (lateral) sinuses, the left internal jugular vein | non-fluent aphasia, anomic aphasia |
| Broca‘s aphasia due to cerebral venous sinus thrombosis following chemotherapy for small cell lung cancer: A case report and review of literature | Tolga Tuncel et al. (2014) [24] | 27 | M | advanced-stage small cell lung cancer cisplatin-based chemotherapy | left transverse (lateral) sinus thrombosis | non-fluent aphasia, anomic aphasia |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Munteanu, G.; Motoc, A.G.M.; Dan, T.F.; Gogu, A.E.; Jianu, D.C. Aphasic Syndromes in Cerebral Venous and Dural Sinuses Thrombosis—A Review of the Literature. Life 2022, 12, 1684. https://doi.org/10.3390/life12111684
Munteanu G, Motoc AGM, Dan TF, Gogu AE, Jianu DC. Aphasic Syndromes in Cerebral Venous and Dural Sinuses Thrombosis—A Review of the Literature. Life. 2022; 12(11):1684. https://doi.org/10.3390/life12111684
Chicago/Turabian StyleMunteanu, Georgiana, Andrei Gheorghe Marius Motoc, Traian Flavius Dan, Anca Elena Gogu, and Dragos Catalin Jianu. 2022. "Aphasic Syndromes in Cerebral Venous and Dural Sinuses Thrombosis—A Review of the Literature" Life 12, no. 11: 1684. https://doi.org/10.3390/life12111684
APA StyleMunteanu, G., Motoc, A. G. M., Dan, T. F., Gogu, A. E., & Jianu, D. C. (2022). Aphasic Syndromes in Cerebral Venous and Dural Sinuses Thrombosis—A Review of the Literature. Life, 12(11), 1684. https://doi.org/10.3390/life12111684