
The Burden of Cerebral Venous Thrombosis in a Romanian Population across a 5-Year Period

 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Study Population
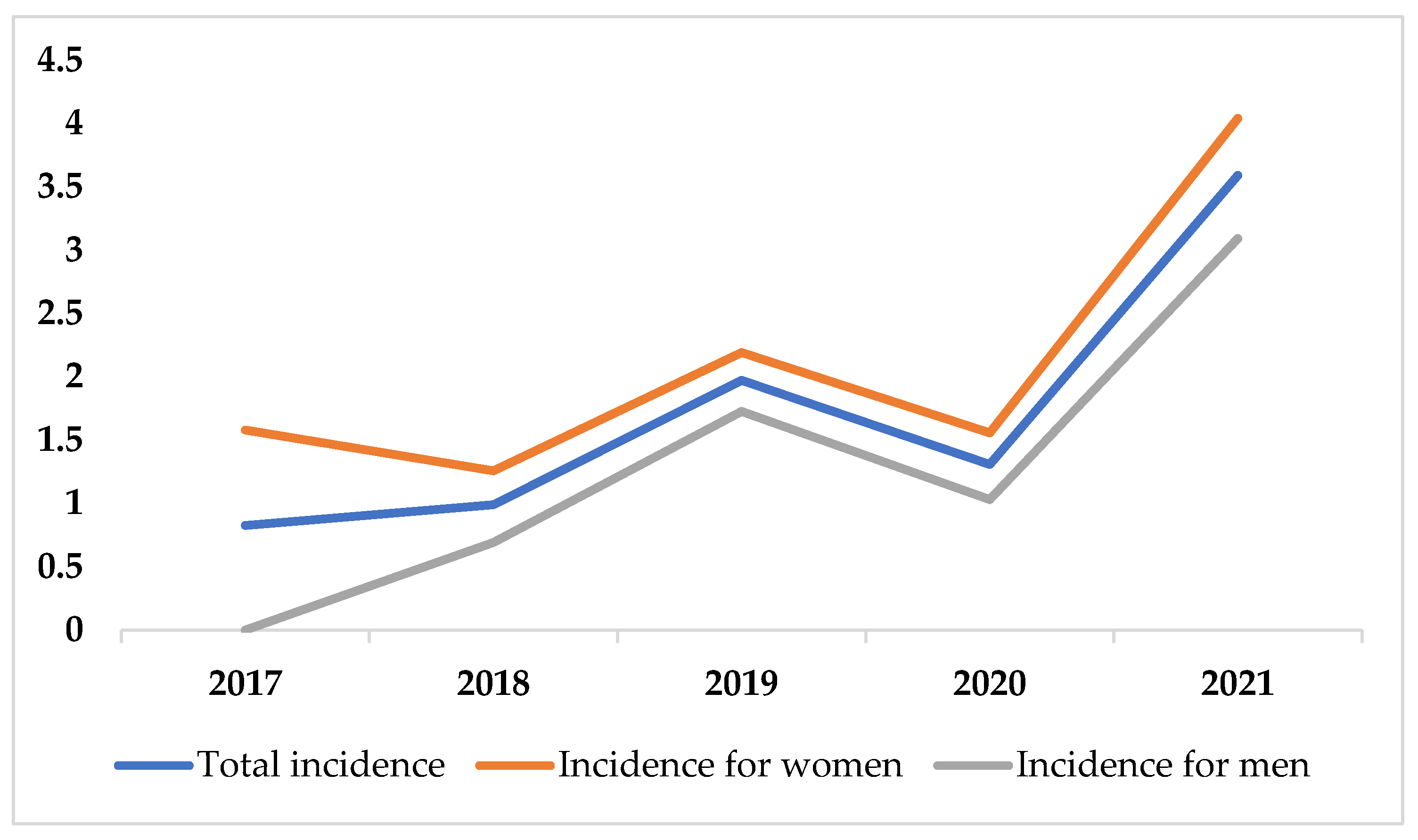
3.2. The Incidence of CVT
3.3. The Burden of CVT
4. Discussion
4.1. The Incidence of CVT
4.2. The Burden of CVT
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ferro, J.M.; Canhão, P.; Stam, J.; Bousser, M.-G.; Barinagarrementeria, F.; ISCVT Investigators. Prognosis of Cerebral Vein and Dural Sinus Thrombosis: Results of the International Study on Cerebral Vein and Dural Sinus Thrombosis (ISCVT). Stroke 2004, 35, 664–670. [Google Scholar] [CrossRef] [PubMed]
- Coutinho, J.M.; Ferro, J.M.; Canhão, P.; Barinagarrementeria, F.; Cantú, C.; Bousser, M.-G.; Stam, J. Cerebral Venous and Sinus Thrombosis in Women. Stroke 2009, 40, 2356–2361. [Google Scholar] [CrossRef] [PubMed]
- Silvis, S.M.; de Sousa, D.A.; Ferro, J.M.; Coutinho, J.M. Cerebral Venous Thrombosis. Nat. Rev. Neurol. 2017, 13, 555–565. [Google Scholar] [CrossRef] [PubMed]
- Stam, J. Thrombosis of the Cerebral Veins and Sinuses. N. Engl. J. Med. 2005, 352, 1791–1798. [Google Scholar] [CrossRef]
- Bousser, M.-G.; Ferro, J.M. Cerebral Venous Thrombosis: An Update. Lancet Neurol. 2007, 6, 162–170. [Google Scholar] [CrossRef]
- Devasagayam, S.; Wyatt, B.; Leyden, J.; Kleinig, T. Cerebral Venous Sinus Thrombosis Incidence Is Higher Than Previously Thought. Stroke 2016, 47, 2180–2182. [Google Scholar] [CrossRef]
- Coutinho, J.M.; Zuurbier, S.M.; Aramideh, M.; Stam, J. The Incidence of Cerebral Venous Thrombosis: A Cross-Sectional Study. Stroke 2012, 43, 3375–3377. [Google Scholar] [CrossRef]
- Kalbag, R.; Woolf, A. Cerebral Venous Thrombosis; Oxford University Press: London, UK, 1967. [Google Scholar]
- Kristoffersen, E.S.; Harper, C.E.; Vetvik, K.G.; Zarnovicky, S.; Hansen, J.M.; Faiz, K.W. Incidence and Mortality of Cerebral Venous Thrombosis in a Norwegian Population. Stroke 2020, 51, 3023–3029. [Google Scholar] [CrossRef]
- Triquenot Bagan, A.; Crassard, I.; Drouet, L.; Barbieux-Guillot, M.; Marlu, R.; Robinet-Borgomino, E.; Morange, P.-E.; Wolff, V.; Grunebaum, L.; Klapczynski, F.; et al. Cerebral Venous Thrombosis: Clinical, Radiological, Biological, and Etiological Characteristics of a French Prospective Cohort (FPCCVT)—Comparison with ISCVT Cohort. Front. Neurol. 2021, 12, 753110. [Google Scholar] [CrossRef]
- Bălaşa, R.; Daboczi, M.; Costache, O.; Maier, S.; Bajko, Z.; Moțățaianu, A.; Bălașa, A. Risk factors and diagnosis of cerebral venous thrombosis: Data from a cohort of 45 Romanian patients. Acta Marisiensis-Ser. Med. 2014, 60, 207–214. [Google Scholar] [CrossRef][Green Version]
- Foschi, M.; Pavolucci, L.; Rondelli, F.; Amore, G.; Spinardi, L.; Rinaldi, R.; Favaretto, E.; Favero, L.; Russo, M.; Pensato, U.; et al. Clinicoradiological Profile and Functional Outcome of Acute Cerebral Venous Thrombosis: A Hospital-Based Cohort Study. Cureus 2021, 13, e17898. [Google Scholar] [CrossRef] [PubMed]
- Coutinho, J.M.; Zuurbier, S.M.; Stam, J. Declining Mortality in Cerebral Venous Thrombosis: A Systematic Review. Stroke 2014, 45, 1338–1341. [Google Scholar] [CrossRef] [PubMed]
- Duman, T.; Uluduz, D.; Midi, I.; Bektas, H.; Kablan, Y.; Goksel, B.K.; Milanlioglu, A.; Necioglu Orken, D.; Aluclu, U.; VENOST Study Group. A Multicenter Study of 1144 Patients with Cerebral Venous Thrombosis: The VENOST Study. J. Stroke Cerebrovasc. Dis. 2017, 26, 1848–1857. [Google Scholar] [CrossRef] [PubMed]
- Ferro, J.M.; Correia, M.; Pontes, C.; Baptista, M.V.; Pita, F.; Cerebral Venous Thrombosis Portuguese Collaborative Study Group (Venoport). Cerebral Vein and Dural Sinus Thrombosis in Portugal: 1980–1998. Cerebrovasc. Dis. 2001, 11, 177–182. [Google Scholar] [CrossRef] [PubMed]
- Mak, W.; Mok, K.Y.; Tsoi, T.H.; Cheung, R.T.; Ho, S.L.; Chang, C.M. Cerebral Venous Thrombosis in Hong Kong. Cerebrovasc. Dis. 2001, 11, 282–283. [Google Scholar] [CrossRef] [PubMed]
- TEMPO Online. Available online: http://statistici.insse.ro:8077/tempo-online/#/pages/tables/insse-table (accessed on 30 September 2022).
- Feng, C.; Wang, H.; Lu, N.; Chen, T.; He, H.; Lu, Y.; Tu, X.M. Log-Transformation and Its Implications for Data Analysis. Shanghai Arch. Psychiatry 2014, 26, 105–109. [Google Scholar] [CrossRef] [PubMed]
- World Bank Open Data|Data. Available online: https://data.worldbank.org/ (accessed on 1 October 2022).
- Rodríguez-Rubio, L.R.; Medina-Córdova, L.L.; Andrade-Ramos, M.A.; González-Padilla, C.; Bañuelos-Becerra, L.J.; Chiquete, E.; Coronado-Magaña, H.; Pérez-Flores, G.; Rojas-Andrews, A.; González-Cornejo, S.; et al. Cerebral venous thrombosis at the Hospital Civil de Guadalajara “Fray Antonio Alcalde”. Rev. Mex. Neurocienc. 2009, 10, 177–183. [Google Scholar]
- Janghorbani, M.; Zare, M.; Saadatnia, M.; Mousavi, S.A.; Mojarrad, M.; Asgari, E. Cerebral Vein and Dural Sinus Thrombosis in Adults in Isfahan, Iran: Frequency and Seasonal Variation. Acta Neurol. Scand. 2008, 117, 117–121. [Google Scholar] [CrossRef]
- Siegal, D.M.; Eikelboom, J.W.; Lee, S.F.; Rangarajan, S.; Bosch, J.; Zhu, J.; Yusuf, S.; the Venous Thromboembolism Collaboration. Variations in Incidence of Venous Thromboembolism in Low-, Middle-, and High-Income Countries. Cardiovasc. Res. 2021, 117, 576–584. [Google Scholar] [CrossRef]
- Swartz, R.H.; Cayley, M.L.; Foley, N.; Ladhani, N.N.N.; Leffert, L.; Bushnell, C.; McClure, J.A.; Lindsay, M.P. The Incidence of Pregnancy-Related Stroke: A Systematic Review and Meta-Analysis. Int. J. Stroke 2017, 12, 687–697. [Google Scholar] [CrossRef]
- Christin-Maitre, S. History of Oral Contraceptive Drugs and Their Use Worldwide. Best Pract. Res. Clin. Endocrinol. Metab. 2013, 27, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Farca, A.; Popa, A.D.; Mardale, S.; Leucu, D.-C.; Mogo, C. Counselling, Knowledge and Attitudes towards Combined Oral Contraceptives: A Cross-sectional Survey among Romanian Women. Farmacia 2017, 65, 954–961. [Google Scholar]
- Axelerad, A.D.; Zlotea, L.A.; Sirbu, C.A.; Stroe, A.Z.; Axelerad, S.D.; Cambrea, S.C.; Muja, L.F. Case Reports of Pregnancy-Related Cerebral Venous Thrombosis in the Neurology Department of the Emergency Clinical Hospital in Constanta. Life 2022, 12, 90. [Google Scholar] [CrossRef] [PubMed]
- Zuurbier, S.M.; Hiltunen, S.; Lindgren, E.; Silvis, S.M.; Jood, K.; Devasagayam, S.; Kleinig, T.J.; Silver, F.L.; Mandell, D.M.; Putaala, J.; et al. Cerebral Venous Thrombosis in Older Patients. Stroke 2018, 49, 197–200. [Google Scholar] [CrossRef]
- Dentali, F.; Poli, D.; Scoditti, U.; Di Minno, M.N.D.; De Stefano, V.; Stefano, V.D.; Siragusa, S.; Kostal, M.; Palareti, G.; Sartori, M.T.; et al. Long-Term Outcomes of Patients with Cerebral Vein Thrombosis: A Multicenter Study. J. Thromb. Haemost. 2012, 10, 1297–1302. [Google Scholar] [CrossRef] [PubMed]
- Ferro, J.M.; Canhão, P.; Bousser, M.-G.; Stam, J.; Barinagarrementeria, F.; ISCVT Investigators. Cerebral Vein and Dural Sinus Thrombosis in Elderly Patients. Stroke 2005, 36, 1927–1932. [Google Scholar] [CrossRef]
- Holcombe, A.; Mohr, N.; Farooqui, M.; Dandapat, S.; Dai, B.; Zevallos, C.B.; Quispe-Orozco, D.; Siddiqui, F.; Ortega-Gutierrez, S. Patterns of Care and Clinical Outcomes in Patients with Cerebral Sinus Venous Thrombosis. J. Stroke Cerebrovasc. Dis. 2020, 29, 105313. [Google Scholar] [CrossRef]
- Birnbaum, J.A.; Labagnara, K.F.; Unda, S.R.; Altschul, D.J. Analyzing the Effect of Weekend and July Admission on Patient Outcomes Following Non-Pyogenic Intracranial Venous Thrombosis. Interdiscip. Neurosurg. 2020, 22, 100797. [Google Scholar] [CrossRef]
- Bousser, M.-G. Cerebral Venous Thrombosis. Stroke 1999, 30, 481–483. [Google Scholar] [CrossRef]
- Coutinho, J.; de Bruijn, S.F.; Deveber, G.; Stam, J. Anticoagulation for Cerebral Venous Sinus Thrombosis. Cochrane Database Syst. Rev. 2011, CD002005. [Google Scholar] [CrossRef]
- Ferro, J.M.; Crassard, I.; Coutinho, J.M.; Canhão, P.; Barinagarrementeria, F.; Cucchiara, B.; Derex, L.; Lichy, C.; Masjuan, J.; Massaro, A.; et al. Decompressive Surgery in Cerebrovenous Thrombosis: A Multicenter Registry and a Systematic Review of Individual Patient Data. Stroke 2011, 42, 2825–2831. [Google Scholar] [CrossRef] [PubMed]
- Nasr, D.M.; Brinjikji, W.; Cloft, H.J.; Saposnik, G.; Rabinstein, A.A. Mortality in Cerebral Venous Thrombosis: Results from the National Inpatient Sample Database. Cerebrovasc. Dis. 2013, 35, 40–44. [Google Scholar] [CrossRef] [PubMed]
- Tu, T.M.; Goh, C.; Tan, Y.K.; Leow, A.S.; Pang, Y.Z.; Chien, J.; Shafi, H.; Chan, B.P.; Hui, A.; Koh, J.; et al. Cerebral Venous Thrombosis in Patients with COVID-19 Infection: A Case Series and Systematic Review. J. Stroke Cerebrovasc. Dis. 2020, 29, 105379. [Google Scholar] [CrossRef]
- Hameed, S.; Wasay, M.; Soomro, B.A.; Mansour, O.; Abd-Allah, F.; Tu, T.; Farhat, R.; Shahbaz, N.; Hashim, H.; Alamgir, W.; et al. Cerebral Venous Thrombosis Associated with COVID-19 Infection: An Observational, Multicenter Study. Cerebrovasc. Dis. Extra 2021, 11, 55–60. [Google Scholar] [CrossRef] [PubMed]
- Al-Mufti, F.; Amuluru, K.; Sahni, R.; Bekelis, K.; Karimi, R.; Ogulnick, J.; Cooper, J.; Overby, P.; Nuoman, R.; Tiwari, A.; et al. Cerebral Venous Thrombosis in COVID-19: A New York Metropolitan Cohort Study. AJNR Am. J. Neuroradiol. 2021, 42, 1196–1200. [Google Scholar] [CrossRef]
- Tu, T.M.; Yi, S.J.; Koh, J.S.; Saffari, S.E.; Hoe, R.H.M.; Chen, G.J.; Chiew, H.J.; Tham, C.H.; Seet, C.Y.H.; Yong, M.H.; et al. Incidence of Cerebral Venous Thrombosis Following SARS-CoV-2 Infection vs MRNA SARS-CoV-2 Vaccination in Singapore. JAMA Netw. Open 2022, 5, e222940. [Google Scholar] [CrossRef] [PubMed]
- See, I.; Su, J.R.; Lale, A.; Woo, E.J.; Guh, A.Y.; Shimabukuro, T.T.; Streiff, M.B.; Rao, A.K.; Wheeler, A.P.; Beavers, S.F.; et al. US Case Reports of Cerebral Venous Sinus Thrombosis with Thrombocytopenia After Ad26.COV2.S Vaccination, 2 March to 21 April 2021. JAMA 2021, 325, 2448–2456. [Google Scholar] [CrossRef]
- Pottegård, A.; Lund, L.C.; Karlstad, Ø.; Dahl, J.; Andersen, M.; Hallas, J.; Lidegaard, Ø.; Tapia, G.; Gulseth, H.L.; Ruiz, P.L.-D.; et al. Arterial Events, Venous Thromboembolism, Thrombocytopenia, and Bleeding after Vaccination with Oxford-AstraZeneca ChAdOx1-S in Denmark and Norway: Population Based Cohort Study. BMJ 2021, 373, n1114. [Google Scholar] [CrossRef]
- Muir, K.-L.; Kallam, A.; Koepsell, S.A.; Gundabolu, K. Thrombotic Thrombocytopenia after Ad26.COV2.S Vaccination. N. Engl. J. Med. 2021, 384, 1964–1965. [Google Scholar] [CrossRef]
- Greinacher, A.; Thiele, T.; Warkentin, T.E.; Weisser, K.; Kyrle, P.A.; Eichinger, S. Thrombotic Thrombocytopenia after ChAdOx1 NCov-19 Vaccination. N. Engl. J. Med. 2021, 384, 2092–2101. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Patient Characteristics | Total, N = 53 | Female, N = 34, 64.2% | Male, N = 19, 35.8% |
|---|---|---|---|
| Median age (interquartile range), years | 45 (29) | 45 (22) | 44 (40) |
| Type of onset, N (%) | |||
| Acute | 32 (60.4%) | 20 (58.8%) | 12 (63.2%) |
| Subacute | 16 (30.2%) | 10 (29.4%) | 6 (31.6%) |
| Chronic | 5 (9.4%) | 4 (11.8%) | 1 (5.2%) |
| Clinical presentation, N (%) | |||
| Headache | 31 (58.5%) | 22 (64.7%) | 9 (47.4%) |
| Nausea/vomiting | 10 (18.9%) | 6 (17.6%) | 4 (21.1%) |
| Motor weakness | 19 (35.8%) | 14 (41.2%) | 5 (26.3%) |
| Seizures | 14 (26.4%) | 6 (17.6%) | 8 (42.1%) |
| Coma | 9 (17%) | 6 (17.6%) | 3 (15.8%) |
| Speech disturbances | 6 (11.3%) | 6 (17.6%) | 0 |
| Cranial nerve palsies | 5 (9.43%) | 2 (5.8%) | 3 (15.8%) |
| Cerebellar signs | 4 (7.5%) | 4 (11.8%) | 0 |
| Sinus/vein involved, N (%) | |||
| Transverse sinus | 8 (15.1%) | 6 (17.6%) | 2 (10.5%) |
| Superior sagittal sinus | 5 (9.4%) | 2 (5.9%) | 3 (15.8%) |
| Cavernous sinus | 3 (5.7%) | 0 | 3 (15.8%) |
| Cortical veins | 3 (5.7%) | 3 (8.8%) | 0 |
| Two or more sinuses/veins involved | 34 (64.1%) | 23 (67.7%) | 11 (57.9%) |
| Transient risk factors, N (%) | |||
| Pregnancy and puerperium | 4 (7.5%) | 4 (11.8%) | 0 |
| Oral contraceptives | 4 (7.5%) | 4 (11.8%) | 0 |
| Head trauma | 6 (11.3%) | 3 (8.8%) | 3 (15.8%) |
| Local infections | 4 (7.5%) | 2 (5.9%) | 2 (10.5%) |
| SARS-CoV-2 infection | 1 (1.88%) | 1 (2.94%) | 0 |
| Adenoviral-vector-based SARS-CoV-2 vaccination | 1 (1.88%) | 0 | 1 (5.2%) |
| Two or more transient risk factors | 2 (3.8%) | 2 (5.9%) | 0 |
| Persistent risk factors, N (%) | |||
| Prior thromboembolism | 3 (5.7%) | 2 (5.9%) | 1 (5.3%) |
| Thrombophilia | 13 (24.5%) | 7 (20.6%) | 6 (31.6%) |
| Neoplasia | 4 (7.5%) | 4 (11.7%) | 0 |
| Two or more persistent risk factors | 7 (13.2%) | 5 (14.7%) | 2 (10.5%) |
| Without transient or persistent risk factors, N (%) | 13 (24.52%) | 7 (20.56%) | 6 (31.6%) |
| Complications, N (%) | |||
| Venous infarct | 9 (17%) | 7 (20.6%) | 2 (10.5%) |
| Subarachnoid hemorrhage | 3 (5.7%) | 2 (5.9%) | 1 (5.3%) |
| Parenchymal hemorrhage | 3 (5.7%) | 0 | 3 (15.7%) |
| Two or more complications | 10 (18.8%) | 9 (26.4%) | 1 (5.3%) |
| Without complications | 28 (52.8%) | 16 (47.1%) | 12 (63.2%) |
| 2017 | 2018 | 2019 | 2020 | 2021 | Overall Incidence | |
|---|---|---|---|---|---|---|
| Incidence/year | 0.82 (0.26–1.92) | 0.98 (0.36–2.15) | 1.97 (1.09–3.44) | 1.30 (0.56–2.57) | 3.59 (2.25–5.43) | 1.74 (1.30–2.27) |
| Women | 1.57 (0.51–3.68) | 1.25 (0.34–3.22) | 2.19 (0.88–4.51) | 1.55 (0.50–3.63) | 4.04 (2.12–6.91) | 2.13 (1.47–2.97) |
| Men | 0 | 0.69 (0.08–2.50) | 1.72 (0.56–4.03) | 1.03 (0.21–3.01) | 3.09 (1.41–5.87) | 1.31 (0.79–2.04) |
| Incidence/18–49 y | 0.86 (0.17–2.52) | 1.75 (0.64–3.81) | 1.77 (0.65–3.85) | 0.59 (0.07–2.15) | 3.89 (2.07–6.66) | 1.76 (1.19–2.53) |
| Women | 1.72 (0.35–5.04) | 2.32 (0.63–5.95) | 1.76 (0.36–5.15) | 0.59 (0.01–3.29) | 5.36 (2.45–10.1) | 2.43 (1.43–3.62) |
| Men | 0 | 1.17 (0.01–4.23) | 1.77 (0.03–5.19) | 0.59 (0.01–3.33) | 2.41 (0.06–6.17) | 1.18 (0.05–2.17) |
| Incidence/50–69 y | 0.57 (0.01–3.20) | 0 | 2.18 (0.05–5.58) | 2.67 (0.08–6.25) | 3.71 (1.49–7.64) | 1.86 (1.08–2.08) |
| Women | 1.09 (0.02–6.07) | 0 | 2.07 (0.02–7.47) | 4.07 (1.11–10.4) | 2.01 (0.02–7.29) | 1.87 (0.08–3.56) |
| Men | 0 | 0 | 2.30 (0.02–8.32) | 1.13 (0.02–6.29) | 5.58 (1.82–13.0) | 1.85 (0.80–3.65) |
| Incidence/>70 y | 1.18 (0.03–6.61) | 0 | 2.31 (0.28–8.34) | 1.12 (0.28–6.26) | 2.20 (0.26–7.98) | 1.37 (0.50–2.99) |
| Women | 1.95 (0.49–10.8) | 0 | 3.80 (0.46–13.7) | 0 | 3.64 (0.44–13.1) | 1.89 (0.61–4.44) |
| Men | 0 | 0 | 0 | 2.85 (0.72–15.8) | 0 | 0.58 (0.14–3.25) |
| ISCVT [1] | High-Income Countries | Upper-Middle-Income Countries | Lower-Middle-Income Countries | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Country | 21 Countries | Portugal [15] | Hong Kong [16] | Australia [6] | Netherlands [7] | France [10] | Norway [9] | Italy [12] | Mexico [20] | VENOST [14], Turkey | Romania (Our Study) | Iran [21] |
| Time interval | 1998–2002 | 1980–1998 | 1995–1998 | 2005–2011 | 2008–2010 | 2011–2016 | 2011–2017 | 2012–2019 | 1999–2008 | 2000–2015 | 2017–2021 | 2001–2004 |
| Sample size | 624 | 142 | 13 | 105 | 94 | 194 | 62 | 32 | 24 | 1144 | 53 | 122 |
| Incidence per 100,000 | NR | 0.22 | 0.34 | 1.57 | 1.32 | NR | 1.75 | 1.6 | NR | NR | 1.74 | 1.23 |
| Median age | 37 (16–86) | 35 | 30 | 49 | 41 | 40 | 46 | 41 | 30 | 40 | 45 | 26 |
| Women, % | 74.5% | 72% | 77% | 52% | 72% | 68.4% | 53% | 75% | 83% | 67.9% | 64.2% | 79% |
| LHS, median | 17 | NR | NR | NR | NR | 10 | NR | 20 | 22 | NR | 10 | NR |
| Discharge mortality | 4.3% | 6% | 8% | 9% | 1% | 2.9% | 3% | 0% | 8% | NR | 5.7% | NR |
| Mortality at follow up | 8.3% | NR | NR | 12% | 3% | 3.4% | 3% | 0% | NR | NR | 7.5% | NR |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stan, A.; Ilut, S.; Dragos, H.M.; Bota, C.; Hanghicel, P.N.; Cristian, A.; Vlad, I.; Mocanu, D.; Strilciuc, S.; Panaitescu, P.S.; et al. The Burden of Cerebral Venous Thrombosis in a Romanian Population across a 5-Year Period. Life 2022, 12, 1825. https://doi.org/10.3390/life12111825
Stan A, Ilut S, Dragos HM, Bota C, Hanghicel PN, Cristian A, Vlad I, Mocanu D, Strilciuc S, Panaitescu PS, et al. The Burden of Cerebral Venous Thrombosis in a Romanian Population across a 5-Year Period. Life. 2022; 12(11):1825. https://doi.org/10.3390/life12111825
Chicago/Turabian StyleStan, Adina, Silvina Ilut, Hanna Maria Dragos, Claudia Bota, Patricia Nicoleta Hanghicel, Alexander Cristian, Irina Vlad, Diana Mocanu, Stefan Strilciuc, Paul Stefan Panaitescu, and et al. 2022. "The Burden of Cerebral Venous Thrombosis in a Romanian Population across a 5-Year Period" Life 12, no. 11: 1825. https://doi.org/10.3390/life12111825
APA StyleStan, A., Ilut, S., Dragos, H. M., Bota, C., Hanghicel, P. N., Cristian, A., Vlad, I., Mocanu, D., Strilciuc, S., Panaitescu, P. S., Stan, H., & Muresanu, D. F. (2022). The Burden of Cerebral Venous Thrombosis in a Romanian Population across a 5-Year Period. Life, 12(11), 1825. https://doi.org/10.3390/life12111825