

A Pathophysiological Approach to Reduce Peritumoral Edema with Gamma Knife Radiosurgery for Large Incidental Meningiomas

 , and
, and
Abstract
1. Introduction
2. Methods
2.1. Study Design and Population
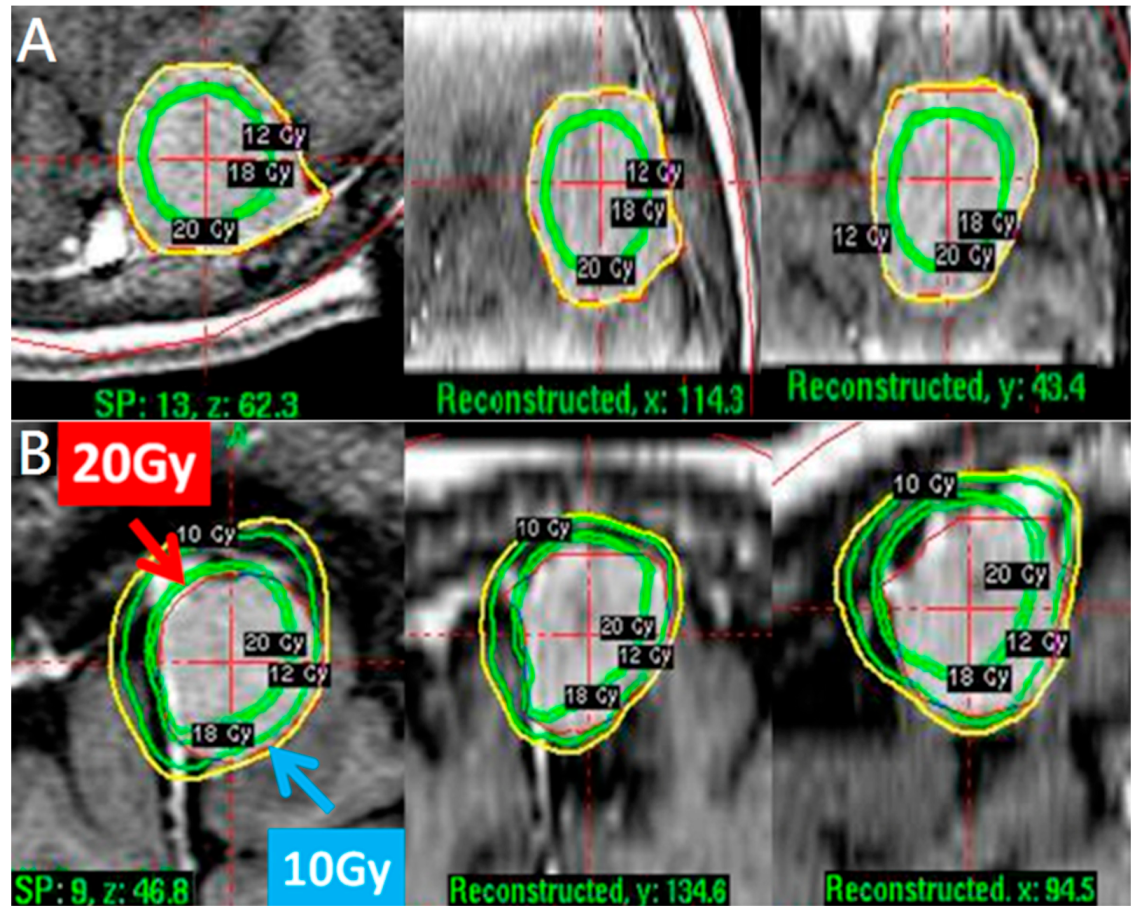
2.2. Treatment Approach and Exposure Variable
2.3. Outcomes and Follow-Up Duration
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
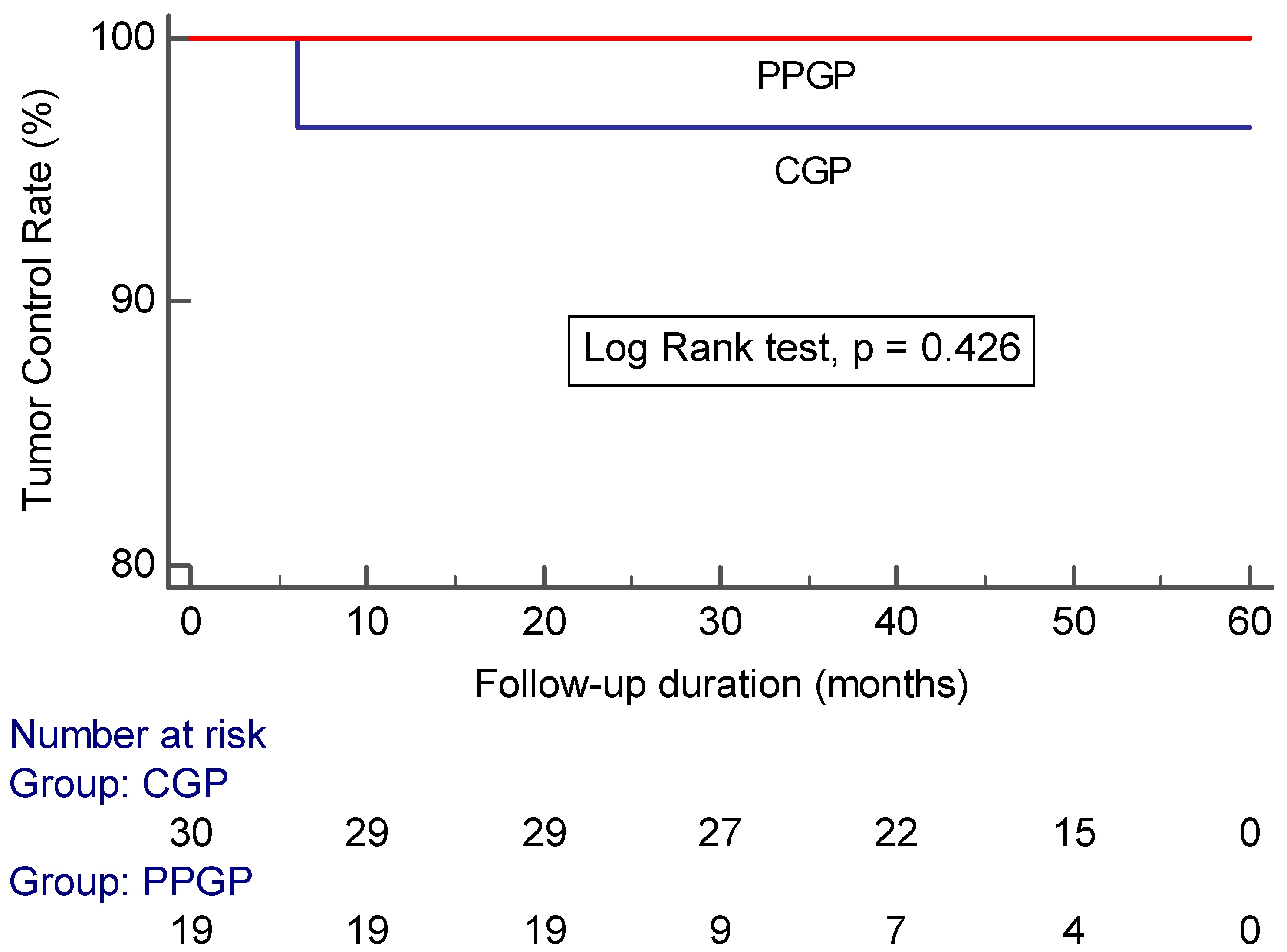
3.2. Outcome
4. Discussion
4.1. Tumor Control of Incidental Meningiomas with Stereotactic Radiosurgery
4.2. Peritumor Edema Following GKRS
4.3. Rationale of Pathophysiological Approach for Relative Large Incidental Meningioma Treated by Stereotactic Radiosurgery
4.4. Limitation and Extension of GKRS for Incidental Meningiomas
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hashiba, T.; Hashimoto, N.; Izumoto, S.; Suzuki, T.; Kagawa, N.; Maruno, M.; Kato, A.; Yoshimine, T. Serial volumetric assessment of the natural history and growth pattern of incidentally discovered meningiomas. J. Neurosurg. 2009, 110, 675–684. [Google Scholar] [CrossRef] [PubMed]
- Jo, K.W.; Kim, C.H.; Kong, D.S.; Seol, H.J.; Nam, D.H.; Park, K.; Kim, J.H.; Lee, J.I. Treatment modalities and outcomes for asymptomatic meningiomas. Acta Neurochir. 2011, 153, 62–67. [Google Scholar] [CrossRef]
- Reinert, M.; Babey, M.; Curschmann, J.; Vajtai, I.; Seiler, R.W.; Mariani, L. Morbidity in 201 patients with small sized meningioma treated by microsurgery. Acta Neurochir. 2006, 148, 1257–1265. [Google Scholar] [CrossRef] [PubMed]
- Cai, R.; Barnett, G.H.; Novak, E.; Chao, S.T.; Suh, J.H. Principal risk of peritumoral edema after stereotactic radiosurgery for intracranial meningioma is tumor-brain contact interface area. Neurosurgery 2010, 66, 513–522. [Google Scholar] [CrossRef] [PubMed]
- Kondziolka, D.; Patel, A.D.; Kano, H.; Flickinger, J.C.; Lunsford, L.D. Long-term outcomes after Gamma Knife radiosurgery for meningiomas. Am. J. Clin. Oncol. 2016, 39, 453–457. [Google Scholar] [CrossRef]
- Pollock, B.E.; Stafford, S.L.; Link, M.J.; Brown, P.D.; Garces, Y.I.; Foote, R.L. Single-fraction radiosurgery of benign intracranial meningiomas. Neurosurgery 2012, 71, 604–612. [Google Scholar] [CrossRef]
- Chang, J.H.; Chang, J.W.; Choi, J.Y.; Park, Y.G.; Chung, S.S. Complications after gamma knife radiosurgery for benign meningiomas. J. Neurol. Neurosurg. Psychiatry 2003, 74, 226–230. [Google Scholar] [CrossRef]
- Hoe, Y.; Choi, Y.J.; Kim, J.H.; Kwon, D.H.; Kim, C.J.; Cho, Y.H. Peritumoral Brain Edema after Stereotactic Radiosurgery for Asymptomatic Intracranial Meningiomas: Risks and Pattern of Evolution. J. Korean Neurosurg. Soc. 2015, 58, 379–384. [Google Scholar] [CrossRef]
- Kim, K.H.; Kang, J.; Choi, W.; Kong, S.; Seol, J.; Nam, H.; Lee, J.I. Clinical and radiological outcomes of proactive Gamma Knife surgery for asymptomatic meningiomas compared with the natural course without intervention. J. Neurosurg. 2019, 130, 1740–1749. [Google Scholar] [CrossRef]
- Kuhn, E.N.; Taksler, G.B.; Dayton, O.; Loganathan, A.; Bourland, D.; Tatter, S.B.; Laxton, A.W.; Chan, M.D. Is there a tumor volume threshold for postradiosurgical symptoms? A single-institution analysis. Neurosurgery 2014, 75, 536–545. [Google Scholar] [CrossRef]
- Novotný, J., Jr.; Kollová, A.; Liscák, R. Prediction of intracranial edema after radiosurgery of meningiomas. J. Neurosurg. 2006, 105, 120–126. [Google Scholar] [CrossRef]
- Sheehan, J.P.; Lee, C.C.; Xu, Z.; Przybylowski, C.J.; Melmer, P.D.; Schlesinger, D. Edema following Gamma Knife radiosurgery for parasagittal and parafalcine meningiomas. J. Neurosurg. 2015, 123, 1287–1293. [Google Scholar] [CrossRef] [PubMed]
- Unger, K.R.; Lominska, C.E.; Chanyasulkit, J.; Randolph-Jackson, P.; White, R.L.; Aulisi, E.; Jacobson, J.; Jean, W.; Gagnon, G.J. Risk factors for posttreatment edema in patients treated with stereotactic radiosurgery for meningiomas. Neurosurgery 2012, 70, 639–645. [Google Scholar] [CrossRef] [PubMed]
- Haselsberger, K.; Maier, T.; Dominikus, K.; Holl, E.; Kurschel, S.; Ofner-Kopeinig, P.; Unger, F. Staged gamma knife radiosurgery for large critically located benign meningiomas: Evaluation of a series comprising 20 patients. J. Neurol. Neurosurg. Psychiatry 2009, 80, 1172–1175. [Google Scholar] [CrossRef] [PubMed]
- Ide, M.; Jimbo, M.; Kubo, O.; Yamamoto, M.; Takeyama, E.; Imanaga, H. Peritumoral brain edema and cortical damage by meningioma. Acta Neurochir. Suppl. 1994, 60, 369–372. [Google Scholar]
- Stevens, J.M.; Ruiz, J.S.; Kendall, B.E. Observations on peritumoral oedema in meningioma. Part II: Mechanisms of oedema production. Neuroradiology 1983, 25, 125–131. [Google Scholar] [CrossRef]
- Islim, A.; Mohan, M.; Moon, R.; Srikandarajah, N.; Mills, S.J.; Brodbelt, R.; Jenkinson, M.D. Incidental intracranial meningiomas: A systematic review and metaanalysis of prognostic factors and outcomes. J. Neuro-Oncol. 2019, 142, 211–221. [Google Scholar] [CrossRef]
- Gupta, A.; Xu, Z.; Cohen-Inbar, O.; Snyder, M.H.; Hobbs, L.K.; Li, C.; Nguyen, Q.T.; Sheehan, J.P. Treatment of Asymptomatic Meningioma with Gamma Knife Radiosurgery: Long-Term Follow-up with Volumetric Assessment and Clinical Outcome. Neurosurgery 2019, 85, E889–E899. [Google Scholar] [CrossRef]
- Salvetti, D.J.; Nagaraja, T.G.; Levy, C.; Xu, Z.; Sheehan, J. Gamma Knife surgery for the treatment of patients with asymptomatic meningiomas. J. Neurosurg. 2013, 119, 487–493. [Google Scholar] [CrossRef]
- Pendl, G.; Unger, F.; Papaefthymiou, G.; Eustacchio, S. Staged radiosurgical treatment for large benign cerebral lesions. J. Neurosurg. 2000, 93, 107–112. [Google Scholar] [CrossRef]
- Yano, S.; Kuratsu, J. Indications for surgery in patients with asymptomatic meningiomas based on an extensive experience. J. Neurosurg. 2006, 105, 538–543. [Google Scholar] [CrossRef] [PubMed]
- Lou, E.; Sumrall, A.L.; Turner, S.; Peters, K.B.; Desjardins, A.; Vredenburgh, J.J.; McLendon, R.E.; Herndon, J.E.; McSherry, F.; Norfleet, J.; et al. Bevacizumab therapy for adults with recurrent/progressive meningioma: A retrospective series. J. Neurooncol. 2012, 109, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Levin, V.A.; Bidaut, L.; Hou, P.; Kumar, A.J.; Wefel, J.S.; Bekele, B.N.; Prabhu, S.; Loghin, M.; Gilbert, M.R.; Jackson, E.F. Randomized double-blind placebo-controlled trial of bevacizumab therapy for radiation necrosis of the central nervous system. Int. J. Radiat. Oncol. Biol. Phys. 2011, 79, 1487–1495. [Google Scholar] [CrossRef] [PubMed]
- Meling, T.R.; Da Broi, M.; Scheie, D.; Helseth, E. Meningiomas: Skull base versus non-skull base. Neurosurg. Rev. 2019, 42, 163–173. [Google Scholar] [CrossRef] [PubMed]
- Biswas, T.; Sandhu, A.P.; Singh, D.P.; Schell, M.C.; Maciunas, R.J.; Bakos, R.S.; Muhs, A.G.; Okunieff, P. Low-dose radiosurgery for benign intracranial lesions. Am. J. Clin. Oncol. 2003, 26, 325–331. [Google Scholar]
- Ganz, J.C.; Backlund, E.O.; Thorsen, F.A. The results of gamma knife surgery of meningiomas, related to size of tumor and dose. Stereotact. Funct. Neurosurg. 1993, 61, 23–29. [Google Scholar] [CrossRef]
- Iwai, Y.; Yamanaka, K.; Nakajima, H. Two-staged gamma knife radiosurgery for the treatment of large petroclival and cavernous sinus meningiomas. Surg. Neurol. 2001, 56, 308–314. [Google Scholar] [CrossRef]
- Nakaya, K.; Hayashi, M.; Nakamura, S.; Atsuchi, S.; Sato, H.; Ochial, T.; Yamamoto, M.; Izawa, M.; Hori, T.; Takakura, K. Low-dose radiosurgery for meningiomas. Stereotact. Funct. Neurosurg. 1999, 72, 67–72. [Google Scholar] [CrossRef]
- Pan, D.H.; Guo, W.Y.; Chang, Y.C.; Chung, W.Y.; Shiau, C.Y.; Wang, L.W.; Wu, S.M. The effectiveness and factors related to treatment results of gamma knife radiosurgery for meningiomas. Stereotact. Funct. Neurosurg. 1998, 70, 19–32. [Google Scholar] [CrossRef]
- Tsuzuki, T.; Tsunoda, S.; Sakaki, T.; Konishi, N.; Hiasa, Y.; Nakamura, M.; Yoshino, E. Tumor cell proliferation and apoptosis associated with the Gamma Knife effect. Stereotact. Funct. Neurosurg. 1996, 66, 39–48. [Google Scholar] [CrossRef]
- Iwai, Y.; Yamanaka, K.; Ikeda, H. Gamma Knife radiosurgery for skull base meningioma: Long-term results of low-dose treatment. J. Neurosurg. 2008, 109, 804–810. [Google Scholar] [CrossRef]
- Su, C.F.; Liu, D.W.; Lee, C.C.; Chiu, T.L. Volume-staged gamma knife surgery for the treatment of large skull base meningioma surrounding the optical apparatus: A snowman-shape design. Chin. Med. Assoc. 2017, 80, 697–704. [Google Scholar] [CrossRef]
- Okunieff, P.; Dols, S.; Lee, J.; Singer, S.; Vaupel, P.; Neuringer, L.J.; Beshah, K. Angiogenesis determines blood flow, metabolism, growth rate, and ATPase kinetics of tumors growing in an irradiated bed: 31P and 2H nuclear magnetic resonance studies. Cancer Res. 1991, 51, 3289–3295. [Google Scholar]
- Seo, Y.; Fukuoka, S.; Nakagawara, J.; Takanashi, M.; Takahashi, S.; Suematsu, K.; Nakamura, J. Effect of gamma knife radiosurgery on acoustic neurinomas. Assessment by 99mTcDTPA-human serum albumin and 201T1C1-single photon emission computed tomography. Stereotact. Funct. Neurosurg. 1996, 66, 93–102. [Google Scholar] [CrossRef]
- Liu, A.; Wang, J.M.; Li, G.L.; Sun, Y.L.; Sun, S.B.; Luo, B.; Wang, M.H. Clinical and pathological analysis of benign brain tumors resected after Gamma Knife surgery. JNS 2014, 121, 179–187. [Google Scholar] [CrossRef]
- Saraf, S.; McCarthy, B.J.; Villano, J.L. Update on meningiomas. Oncologist 2011, 16, 1604–1613. [Google Scholar] [CrossRef]
- Perry, A.; Stafford, S.L.; Scheithauer, B.W.; Suman, V.J.; Lohse, C.M. Meningioma grading: An analysis of histologic parameters. Am. J. Surg. Pathol. 1997, 21, 1455–1465. [Google Scholar] [CrossRef]
- Kshettry, V.R.; Ostrom, Q.T.; Kruchko, C.; Al-Mefty, O.; Barnett, G.H.; Barnholtz-Sloan, J.S. Descriptive epidemiology of World Health Organization grades II and III intracranial meningiomas in the United States. Neuro Oncol. 2015, 17, 1166–1173. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Tumors (n = 53) | Pathophysiological Approach (n = 23) | Conventional Approach (n = 30) | p-Value | |
|---|---|---|---|---|
| Patient age (years) | 64 (33–87) | 68 (45–87) | 61 (33–78) | 0.12 |
| Female/Male | 46 (86.8%)/7 (13.2%) | 18 (78.3%)/5 (21.7%) | 28 (93.3%)/2 (6.7%) | 0.22 |
| Volume (mL) b | 3.5 (2–27.2) | 5.3 (2.2–27.2) | 3.2 (2–15) | 0.02 |
| Location | 0.003 | |||
| Hemispheric | 37 (69.8%) | 21 (91.3%) | 16 (53.3%) | |
| Skull base | 16 (30.2%) | 2 (8.7%) | 14 (46.7%) | |
| Marginal Dose (Gy) b | 12 (9–16) | 10 (10–14) | 12 (9–16) | 0.01 |
| All Tumors (n = 53) | Pathophysiological Approach (n = 23) | Conventional Approach (n = 30) | p-Value | |
|---|---|---|---|---|
| Follow-up (years) | 3.5 (1–5) | 3 (1–5) | 3.6 (1–5) | 0.33 |
| Tumor control | 52 (98.1%) | 23 (100%) | 29 (96.7%) | 1.00 |
| Volume change | 0.82 | |||
| >75% decrease | 1 (1.9%) | 1 (4.3%) | 0 (0%) | |
| 50–75% decrease | 15 (28.3%) | 7 (30.4%) | 8 (26.7%) | |
| 15–49% decrease | 13 (24.5%) | 5 (21.7%) | 8 (26.7%) | |
| <15% change | 23 (43.4%) | 10 (43.5%) | 13 (43.3%) | |
| >15% increase | 1 (1.9%) | 0 (0%) | 1 (3.3%) | |
| Peritumoral edema | 7 (13.5%) | 0 (0%) | 7 (24.1%) | 0.01 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, C.-S.; Huang, C.-W.; Chou, H.-H.; Tu, H.-T.; Lee, M.-T.; Huang, C.-F. A Pathophysiological Approach to Reduce Peritumoral Edema with Gamma Knife Radiosurgery for Large Incidental Meningiomas. Life 2022, 12, 1683. https://doi.org/10.3390/life12111683
Chang C-S, Huang C-W, Chou H-H, Tu H-T, Lee M-T, Huang C-F. A Pathophysiological Approach to Reduce Peritumoral Edema with Gamma Knife Radiosurgery for Large Incidental Meningiomas. Life. 2022; 12(11):1683. https://doi.org/10.3390/life12111683
Chicago/Turabian StyleChang, Cheng-Siu, Cheng-Wei Huang, Hsi-Hsien Chou, Hsien-Tang Tu, Ming-Tsung Lee, and Chuan-Fu Huang. 2022. "A Pathophysiological Approach to Reduce Peritumoral Edema with Gamma Knife Radiosurgery for Large Incidental Meningiomas" Life 12, no. 11: 1683. https://doi.org/10.3390/life12111683
APA StyleChang, C.-S., Huang, C.-W., Chou, H.-H., Tu, H.-T., Lee, M.-T., & Huang, C.-F. (2022). A Pathophysiological Approach to Reduce Peritumoral Edema with Gamma Knife Radiosurgery for Large Incidental Meningiomas. Life, 12(11), 1683. https://doi.org/10.3390/life12111683