
Impact of Three-Dimensional Strain on Major Adverse Cardiovascular Events after Acute Myocardial Infarction Managed by Primary Percutaneous Coronary Intervention—A Pilot Study

 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
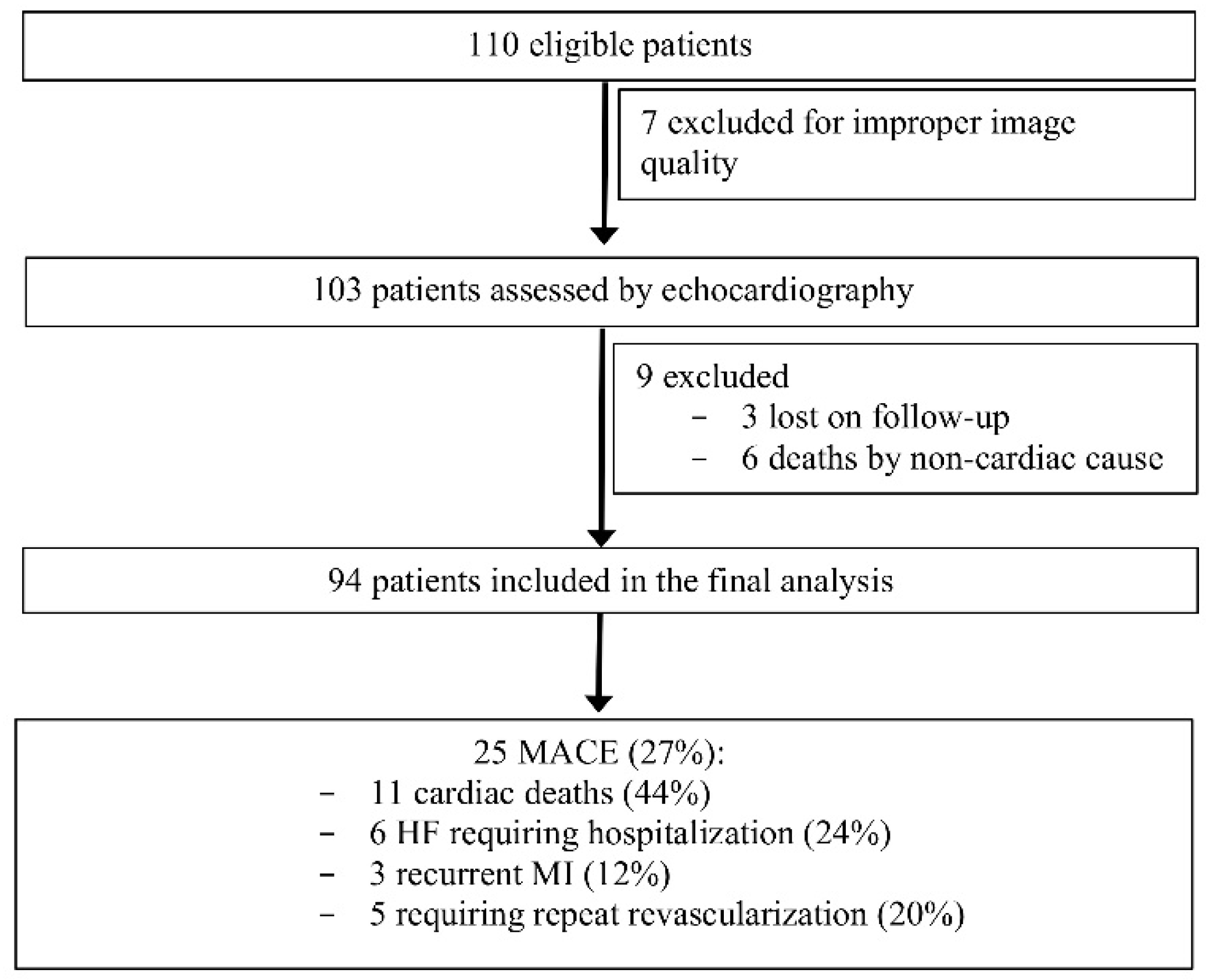
2.1. Study Population
2.2. Echocardiography
2.3. Interobserver Variability
2.4. Follow-Up
2.5. Statistics
3. Results
3.1. Baseline Characteristics
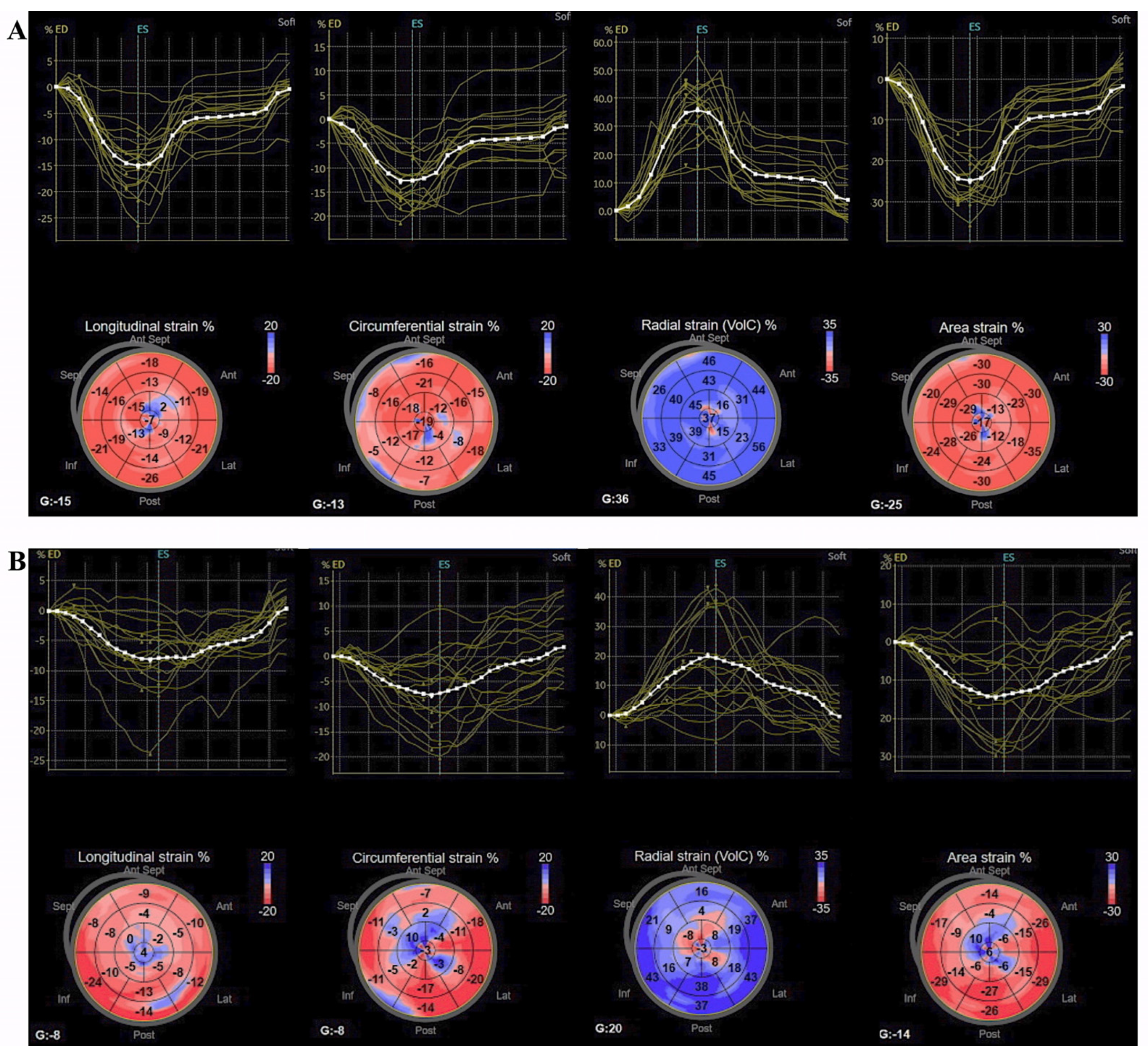
3.2. Standard and 3D Speckle-Tracking Echocardiography Parameters
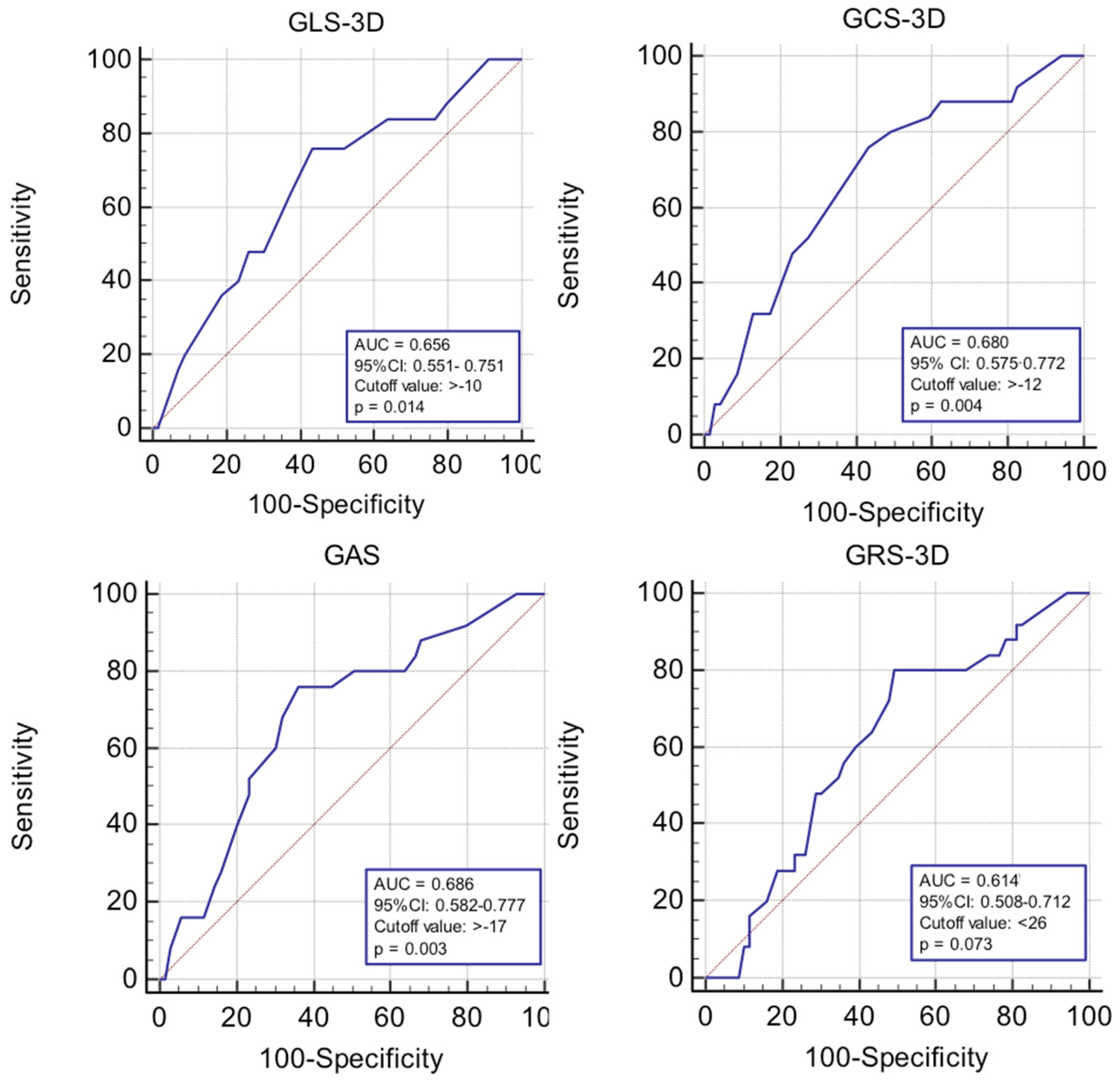
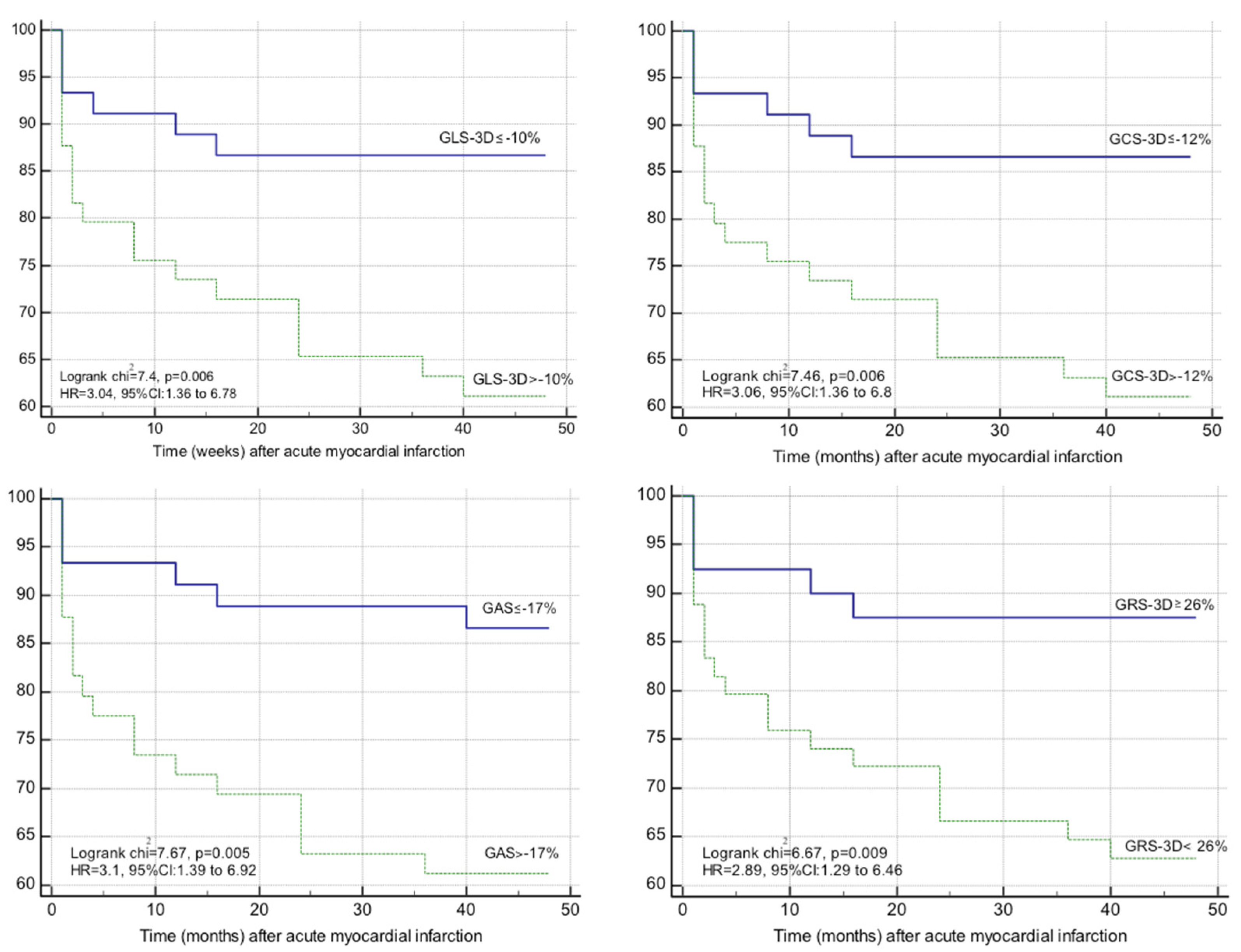
3.3. Impact of 3D Strain on the Occurrence of MACE at 1 Year after Acute Myocardial Infarction
3.4. Interobserver Variability
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ibañez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2018, 39, 119–177. [Google Scholar] [CrossRef] [Green Version]
- Roffi, M.; Patrono, C.; Collet, J.-P.; Mueller, C.; Valgimigli, M.; Andreotti, F.; Bax, J.J.; Borger, M.; Brotons, C.; Chew, D.P.; et al. ESC Scientific Document Group. 2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: Task Force for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2016, 37, 267–315. [Google Scholar] [CrossRef]
- Kalam, K.; Otahal, P.; Marwick, T.H. Prognostic implications of global LV dysfunction: A systematic review and meta-analysis of global longitudinal strain and ejection fraction. Heart 2014, 100, 1673–1680. [Google Scholar] [CrossRef]
- Mor-Avi, V.; Lang, R.M.; Badano, L.P.; Belohlavek, M.; Cardim, N.M.; Derumeaux, G.; Galderisi, M.; Marwick, T.; Nagueh, S.F.; Sengupta, P.P.; et al. Current and evolving echocardiographic techniques for the quantitative evaluation of cardiac mechanics: ASE/ EAE consensus statement on methodology and indications endorsed by the Japanese Society of Echocardiography. Eur. J. Echocardiogr. 2011, 24, 277–313. [Google Scholar] [CrossRef]
- Cimino, S.; Canali, E.; Petronilli, V.; Cicogna, F.; De Luca, L.; Francone, M.; Sardella, G.; Iacoboni, C.; Agati, L. Global and regional longitudinal strain assessed by two-dimensional speckle tracking echocardiography identifies early myocardial dysfunction and transmural extent of myocardial scar in patients with acute ST elevation myocardial infarction and relatively preserved LV function. Eur. Heart J. Cardiovasc. Imaging 2013, 14, 805–811. [Google Scholar] [PubMed]
- Buckberg, G.; Hoffman, J.I.; Mahajan, A.; Saleh, S.; Coghlan, C. Cardiac mechanics revisited: The relationship of cardiac architecture to ventricular function. Circulation 2008, 118, 2571–2587. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hung, C.-L.; Verma, A.; Uno, H.; Shin, S.-H.; Bourgoun, M.; Hassanein, A.H.; Mcmurray, J.; Velazquez, E.J.; Kober, L.; Pfeffer, M.A.; et al. Longitudinal and circumferential strain rate, left ventricular remodeling and prognosis after myocardial infarction. J. Am. Coll. Cardiol. 2010, 22, 1812–1822. [Google Scholar] [CrossRef] [Green Version]
- Antoni, M.L.; Mollema, S.A.; Delgado, V.; Atary, J.Z.; Borleffs, C.J.W.; Boersma, E.; Holman, E.R.; van der Wall, E.E.; Schalij, M.J.; Bax, J.J. Prognostic importance of strain and strain rate after acute myocardial infarction. Eur. Heart J. 2010, 31, 1640–1647. [Google Scholar] [CrossRef] [Green Version]
- Muraru, D.; Niero, A.; Rodriguez-Zanella, H.; Cherata, D.; Badano, L. Three-dimensional speckle-tracking echocardiography: Benefits and limitations of integrating myocardial mechanics with three-dimensional imaging. Cardiovasc. Diagn. Ther. 2018, 8, 101–117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, R.B.; Fedacko, J.; Elkilany, G.; Hristova, K.; Palmiero, P.; Fatima, G.; Pella, D.; Cornelissen, G.; Isaza, A.; Pella, D. 2020 guidelines on pre-heart failure in the light of 2D and 3D speckle tracking echocardiography. A scientific statement of the international college of cardiology. World Heart J. 2020, 12, 51–70. [Google Scholar]
- Shin, S.H.; Suh, Y.J.; Baek, Y.S.; Lee, M.J.; Park, S.D.; Kwon, S.W.; Woo, S.-I.; Kim, D.-H.; Park, K.-S.; Kwan, J. Impact of area strain by 3D speckle tracking on clinical outcome in patients after acute myocardial infarction. Echocardiography 2016, 33, 1854–1859. [Google Scholar] [CrossRef] [Green Version]
- Ali, Y.A.; Alashry, A.M.; Saad, M.T.; Adel, W.; El Fiky, A.A. A Pilot Study to Predict Future Cardiovascular Events by Novel Four-dimensional Echocardiography Global Area Strain in ST-Elevation Myocardial Infarction Patients Managed by Primary Percutaneous Coronary Intervention. J. Cardiovasc. Echogr. 2020, 30, 82–87. [Google Scholar] [CrossRef] [PubMed]
- Iwahashi, N.; Kirigaya, J.; Abe, T.; Horii, M.; Toya, N.; Hanajima, Y.; Takahashi, H.; Akiyama, E.; Okada, K.; Matsuzawa, Y.; et al. Impact of three-dimensional global longitudinal strain for patients with acute myocardial infarction. Eur. Heart J. Cardiovasc. Imaging 2020. [Google Scholar] [CrossRef] [PubMed]
- Cai, W.; Dong, Y.; Tian, L.; Cao, C.X.; Niu, X.L.; Liu, X.L.; Liu, J.-X.; Ji, W.-J.; Zhang, Z.; Zhou, X.; et al. Predictive value of four-dimensional strain echocardiography for adverse cardiovascular outcomes in ST-elevation myocardial infarction patients treated with primary percutaneous coronary intervention. Cardiology 2018, 139, 255–264. [Google Scholar] [CrossRef] [PubMed]
- Anchidin, O.I.; Nemes, A.; Molnar, A.; Rosianu, A.; Rosianu, S.H.; Pop, D. Are cardiovascular rehabilitation programs implemented in young patients with acute coronary syndromes following revascularization procedures? Balneo Res. J. 2020, 1, 133–140. [Google Scholar] [CrossRef]
- Urbano-Moral, J.A.; Godínez, J.A.A.; Ahmad, R.; Malik, R.; Kiernan, M.S.; Denofrio, D.; Pandian, N.G.; Patel, A.R. Evaluation of myocardial mechanics with three-dimensional speckle tracking echocardiography in heart transplant recipients: Comparison with two-dimensional speckle tracking and relationship with clinical variables. Eur. Heart J. Cardiovasc. Imaging 2013, 14, 1167–1173. [Google Scholar] [CrossRef] [Green Version]
- Nagata, Y.; Takeuchi, M.; Wu, V.C.-C.; Izumo, M.; Suzuki, K.; Sato, K.; Seo, Y.; Akashi, Y.; Aonuma, K.; Otsuji, Y. Prognostic value of LV deformation parameters using 2D and 3D speckle-tracking echocardiography in asymptomatic patients with severe aortic stenosis and preserved LV ejection fraction. JACC Cardiovasc. Imaging 2015, 8, 235–245. [Google Scholar] [CrossRef] [Green Version]
- Casas-Rojo, E.; Fernández-Golfin, C.; Moya-Mur, J.L.; González-Gómez, A.; García-Martín, A.; Morán-Fernández, L.; Rodríguez-Muñoz, D.; Jiménez-Nacher, J.J.; Sánchez, D.M.; Gómez, J.L.Z. Area strain from 3D speckle-tracking echocardiography as an independent pre- dictor of early symptoms or ventricular dysfunction in asymptomatic severe mitral regurgitation with preserved ejection fraction. Int. J. Cardiovasc. Imaging 2016, 32, 1189–1198. [Google Scholar] [CrossRef]
- Abate, E.; Hoogslag, G.E.; Antoni, M.L.; Nucifora, G.; Delgado, V.; Holman, E.R.; Schalij, M.J.; Bax, J.J.; Marsan, N.A. Value of three-dimensional speckle-tracking longitudinal strain for predicting improvement of left ventricular function after acute myocardial infarction. Am. J. Cardiol. 2012, 110, 961–967. [Google Scholar] [CrossRef]
- Nabeshima, Y.; Seo, Y.; Takeuchi, M. A review of current trends in three-dimensional analysis of left ventricular myocardial strain. Cardiovasc. Ultrasound 2020, 18, 23. [Google Scholar] [CrossRef]
- Sugano, A.; Seo, Y.; Ishizu, T.; Watabe, H.; Yamamoto, M.; Machino-Ohtsuka, T.; Takaiwa, Y.; Kakefuda, Y.; Aihara, H.; Fumikura, Y.; et al. Value of 3-dimensional speckle tracking echocardiography in the prediction of microvascular obstruction and left ventricular remodeling in patients with ST-elevation myocardial infarction. Circ. J. 2017, 81, 353–360. [Google Scholar] [CrossRef] [Green Version]
- Li, X.-C.; Jin, F.-L.; Jing, C.; Xiao, Q.; Liu, Y.; Ran, Z.-S.; Zhang, J.-J. Predictive value of left ventricular remodeling by area strain based on three-dimensional wall- motion tracking after PCI in patients with recent NSTEMI. Ultrasound Med. Biol. 2012, 38, 1491–1501. [Google Scholar] [CrossRef] [PubMed]
- Zhu, W.; Liu, W.; Tong, Y.; Xiao, J. Three-dimensional speckle tracking echocardiography for the evaluation of the infarct size and segmental transmural involvement in patients with acute myocardial infarction. Echocardiography 2014, 31, 58–66. [Google Scholar] [CrossRef] [PubMed]
- Aly, M.F.A.; Kleijn, S.A.; Menken-Negroiu, R.F.; Robbers, L.F.; Beek, A.M.; Kamp, O. Three-dimensional speckle tracking echocardiography and cardiac magnetic resonance for left ventricular chamber quantification and identification of myocardial transmural scar. Neth. Heart J. 2016, 24, 600–608. [Google Scholar] [CrossRef] [Green Version]
- Lacalzada, J.; de la Rosa, A.; Izquierdo, M.M.; Jiménez, J.J.; Iribarren, J.L.; García-González, M.J.; López, B.M.; Duque, M.A.; Barragán, A.; Hernández, C.; et al. Left ventricular global longitudinal systolic strain predicts adverse remodeling and subsequent cardiac events in patients with acute myocardial infarction treated with primary percutaneous coronary intervention. Int. J. Cardiovasc. Imaging 2015, 31, 575–584. [Google Scholar] [CrossRef] [PubMed]
- Haberka, M.; Liszka, J.; Kozyra, A.; Finik, M.; Gasior, Z. Two-dimensional speckle tracking echocardiography prognostic parameters in patients after acute myocardial infarction. Echocardiography 2015, 32, 454–460. [Google Scholar] [CrossRef] [PubMed]
- Huttin, O.; Zhang, L.; Lemarié, J.; Mandry, D.; Juillière, Y.; Lemoine, S.; Micard, E.; Marie, P.-Y.; Sadoul, N.; Girerd, N.; et al. Global and regional myocardial deformation mechanics of microvascular obstruction in acute myocardial infarction: A three dimensional speckle-tracking imaging study. Int. J. Cardiovasc. Imaging 2015, 31, 1337–1346. [Google Scholar] [CrossRef] [PubMed]
- Tsai, I.-T.; Wang, C.-P.; Lu, Y.-C.; Hung, W.-C.; Wu, C.-C.; Lu, L.-F.; Chung, F.-M.; Hsu, C.-C.; Lee, Y.-J.; Yu, T.-H. The burden of major adverse cardiac events in patients with coronary artery disease. BMC Cardiovasc. Disord. 2017, 17, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, C.H.; Cho, G.Y.; Yoon, Y.E.; Park, J.J.; Youn, T.J.; Chae, I.H. 3D myocardial strain measurement after reperfusion therapy is useful to predict future clinical events in patients with ST-segment elevation myocardial infarction. Eur. Heart J. 2015, 36, 43. [Google Scholar]
- Sun, Y.; Feng, L.; Li, X.; Gao, R.; Wu, Y. The sex difference in 6-month MACEs and its explaining variables in acute myocardial infarction survivors: Data from CPACS-3 study. Int. J. Cardiol. 2020, 311, 1–6. [Google Scholar] [CrossRef]
- Gul, B.; Kozuma, K.; Haimi, I.; Zhao, W.; Simonton, C.; Ying, S.-W.; Buda, A.; Mehta, S.; Baumbach, A.; Lansky, A. Sex disparities in acute myocardial infarction care and outcomes. Catheter. Cardiovasc. Interv. 2018, 92, E341–E347. [Google Scholar] [CrossRef] [PubMed]
- Ioacara, S.; Popescu, A.C.; Tenenbaum, J.; Dimulescu, D.R.; Popescu, M.R.; Sirbu, A.; Fica, S. Acute Myocardial Infarction Mortality Rates and Trends in Romania between 1994 and 2017. Int. J. Environ. Res. Public Health 2019, 17, 285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jasaityte, R.; Heyde, B.; D’hooge, J. Current state of three-dimensional myocardial strain estimation using echocardiography. J. Am. Soc. Echocardiogr. 2013, 26, 15–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Badano, L.P.; Cucchini, U.; Muraru, D.; Al Nono, O.; Sarais, C.; Iliceto, S. Use of three- dimensional speckle tracking to assess left ventricular myocardial mechanics: Inter-vendor consistency and reproducibility of strain measurements. Eur. Heart J. Cardiovasc. Imaging 2013, 14, 285–293. [Google Scholar] [CrossRef]
- Yuda, S.; Sato, Y.; Abe, K.; Kawamukai, M.; Kouzu, H.; Muranaka, A.; Kokubu, N.; Hashimoto, A.; Tsuchihashi, K.; Watanabe, N.; et al. Inter-vendor variability of left ventricular volumes and strains determined by three-dimensional speckle tracking echocardiography. Echocardiography 2014, 31, 597–604. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Patients (n = 94) | MACE− (n = 69) | MACE+ (n = 25) | p | |
|---|---|---|---|---|
| Clinical characteristics | ||||
| Age, mean (SD), years | 66 (13) | 66 (13) | 69 (13.5) | NS |
| Male gender, n (%) | 53 (56) | 42 (60) | 11 (44) | <0.001 |
| BMI, kg/m2 | 29 (5) | 29 (4.8) | 29 (5.8) | NS |
| Current smoking, n (%) | 38 (40) | 30 (43) | 8 (32) | NS |
| Diabetes mellitus, n (%) | 33 (35) | 24 (33) | 7 (28) | NS |
| Hypertension, n (%) | 73 (77) | 53 (77) | 20 (80) | NS |
| Dyslipidaemia, n (%) | 26 (28) | 17 (25) | 9 (35) | NS |
| Heart rate, mean (SD), bpm | 79 (18) | 78 (17) | 80 (21) | NS |
| Systolic blood pressure, mean (SD), mmHg | 132 (26) | 135 (24) | 124 (29) | NS |
| Diastolic blood pressure, mean (SD), mmHg | 76 (15) | 77 (14) | 72 (16) | NS |
| STEMI/NSTEMI, n (%) | 65 (69)/29 (31) | 46 (66)/23 (44) | 19 (76)/6 (24) | 0.009 |
| Biomarker levels | ||||
| Troponin T, median (IQR), ng/mL | 0.29 (0.11–1.02) | 0.30 (0.09–0.93) | 0.28 (0.11–1.66) | NS |
| eGFR, mean (SD), mL/min/1.73 m2 | 91 (40) | 97 (35) | 75 (48) | 0.02 |
| Glucose, mean (SD), mg/dL | 136 (49) | 133 (44) | 145 (60) | NS |
| Total cholesterol, mean (SD), mg/dL | 184 (52) | 187 (53) | 178 (49) | NS |
| High-density lipoprotein, mean (SD), mg/dL | 43 (12) | 43 (11) | 43 (13) | NS |
| Low-density lipoprotein, mean (SD), mg/dL | 111 (46) | 111 (47) | 108 (46) | NS |
| Triglycerides, mean (SD), mg/dL | 155 (81) | 157 (78) | 150 (92) | NS |
| Coronary artery characteristics | ||||
| Infarct related artery, n (%) | ||||
| LAD | 49 (52) | 34 (49) | 15 (60) | NS |
| CX | 14 (15) | 13 (17) | 1 (4) | |
| RCA | 31 (33) | 22 (32) | 9 (36) | |
| Coronary artery disease, n (%) | ||||
| 1-vessel | 43 (46) | 38 (55) | 5 (20) | 0.017 |
| 2-vessel | 27 (29) | 15 (22) | 12 (48) | |
| 3-vessel | 24 (25) | 16 (23) | 8 (32) | |
| Echocardiography | ||||
| LV EDV, mean (SD), mL | 117 (38) | 110 (32) | 134 (47) | 0.006 |
| LV ESV, mean (SD), mL | 67 (13.3) | 60 (29) | 84 (43) | 0.002 |
| LV mass, mean (SD), g | 104 (13.5) | 103 (13.6) | 108 (13) | NS |
| LVEF, mean (SD), % | 45 (12) | 45 (11) | 38 (10) | 0.007 |
| E/e’, mean (SD) | 11 (6) | 10.4 (5) | 11.6(8) | NS |
| LAVi, mean(SD), mL/m2 | 29.4 (7) | 30 (7) | 30 (7) | NS |
| vmaxTR, mean (SD), m/s | 2.4 (0.9) | 2.4 (0.9) | 2.5 (0.8) | NS |
| GLS-3D, mean (SD), % | −9.5 (4.4) | −10.1 (4.4) | −7.8 (4) | 0.02 |
| GCS-3D, mean (SD), % | −11.7 (5.1) | −12.5 (5.2) | −9.5 (4.5) | 0.009 |
| GAS, mean (SD), % | −17.7 (7.4) | −19 (7.4) | −14.2 (6.4) | 0.006 |
| GRS-3D, mean (SD), % | 26.8 (16) | 28.6 (17) | 21 (12.4) | 0.04 |
| Parameter | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| Unadjusted HR (95% CI) | p | Adjusted HR (95% CI) | p | |
| GLS-3D, % | 1.11 (1.01–1.23) | 0.02 | 1.13 (1.03–1.26) | 0.02 |
| GCS-3D, % | 1.11 (1.02–1.21) | 0.01 | 1.13 (1.03–1.23) | 0.01 |
| GAS, % | 1.08 (1.02–1.14) | 0.007 | 1.1 (1.03–1.16) | 0.005 |
| GRS-3D, % | 0.97 (0.94–1) | 0.09 | ||
| Age, years | 1.01 (0.99–1.04) | 0.27 | ||
| Male gender | 0.56 (0.25–1.24) | 0.17 | ||
| BMI, kg/m2 | 1 (0.93–1.09) | 0.9 | ||
| SBP, mmHg | 1 (0.98–1) | 0.07 | ||
| eGFR, mL/min/1.73 m2 | 0.98 (0.97–1) | 0.01 | ||
| STEMI/NSTEMI | 0.66 (0.26–1.65) | 0.37 | ||
| Number of vessels | 1.68 (1.07–2.6) | 0.02 | ||
| LV mass, g | 1.02 (0.99–1.05) | 0.14 | ||
| LVEF, % | 0.95 (0.96–0.99) | 0.006 | ||
| E/e’, | 1.03 (0.97–1.1) | 0.32 | ||
| LAVi, mL/m2 | 1.03 (0.97–1.1) | 0.32 | ||
| Vmax TR, m/s | 1.12 (0.78–1.62) | 0.54 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tomoaia, R.; Beyer, R.Ș.; Zdrenghea, D.; Dădârlat-Pop, A.; Popescu, M.I.; Cismaru, G.; Gușetu, G.; Șerban, A.M.; Simu, G.R.; Minciună, I.A.; et al. Impact of Three-Dimensional Strain on Major Adverse Cardiovascular Events after Acute Myocardial Infarction Managed by Primary Percutaneous Coronary Intervention—A Pilot Study. Life 2021, 11, 930. https://doi.org/10.3390/life11090930
Tomoaia R, Beyer RȘ, Zdrenghea D, Dădârlat-Pop A, Popescu MI, Cismaru G, Gușetu G, Șerban AM, Simu GR, Minciună IA, et al. Impact of Three-Dimensional Strain on Major Adverse Cardiovascular Events after Acute Myocardial Infarction Managed by Primary Percutaneous Coronary Intervention—A Pilot Study. Life. 2021; 11(9):930. https://doi.org/10.3390/life11090930
Chicago/Turabian StyleTomoaia, Raluca, Ruxandra Ștefana Beyer, Dumitru Zdrenghea, Alexandra Dădârlat-Pop, Mircea Ioachim Popescu, Gabriel Cismaru, Gabriel Gușetu, Adela Mihaela Șerban, Gelu Radu Simu, Ioan Alexandru Minciună, and et al. 2021. "Impact of Three-Dimensional Strain on Major Adverse Cardiovascular Events after Acute Myocardial Infarction Managed by Primary Percutaneous Coronary Intervention—A Pilot Study" Life 11, no. 9: 930. https://doi.org/10.3390/life11090930
APA StyleTomoaia, R., Beyer, R. Ș., Zdrenghea, D., Dădârlat-Pop, A., Popescu, M. I., Cismaru, G., Gușetu, G., Șerban, A. M., Simu, G. R., Minciună, I. A., Caloian, B., Roșu, R., Chețan, M. I., & Pop, D. (2021). Impact of Three-Dimensional Strain on Major Adverse Cardiovascular Events after Acute Myocardial Infarction Managed by Primary Percutaneous Coronary Intervention—A Pilot Study. Life, 11(9), 930. https://doi.org/10.3390/life11090930