
Immune System Disorders, Cancer and Viral Infections: A New Treatment Opportunity for the Immune Checkpoint Inhibitors


 , , , and
, , , and
Abstract
1. Background
2. Immune Checkpoint Inhibitors
3. Human Papillomavirus Infection
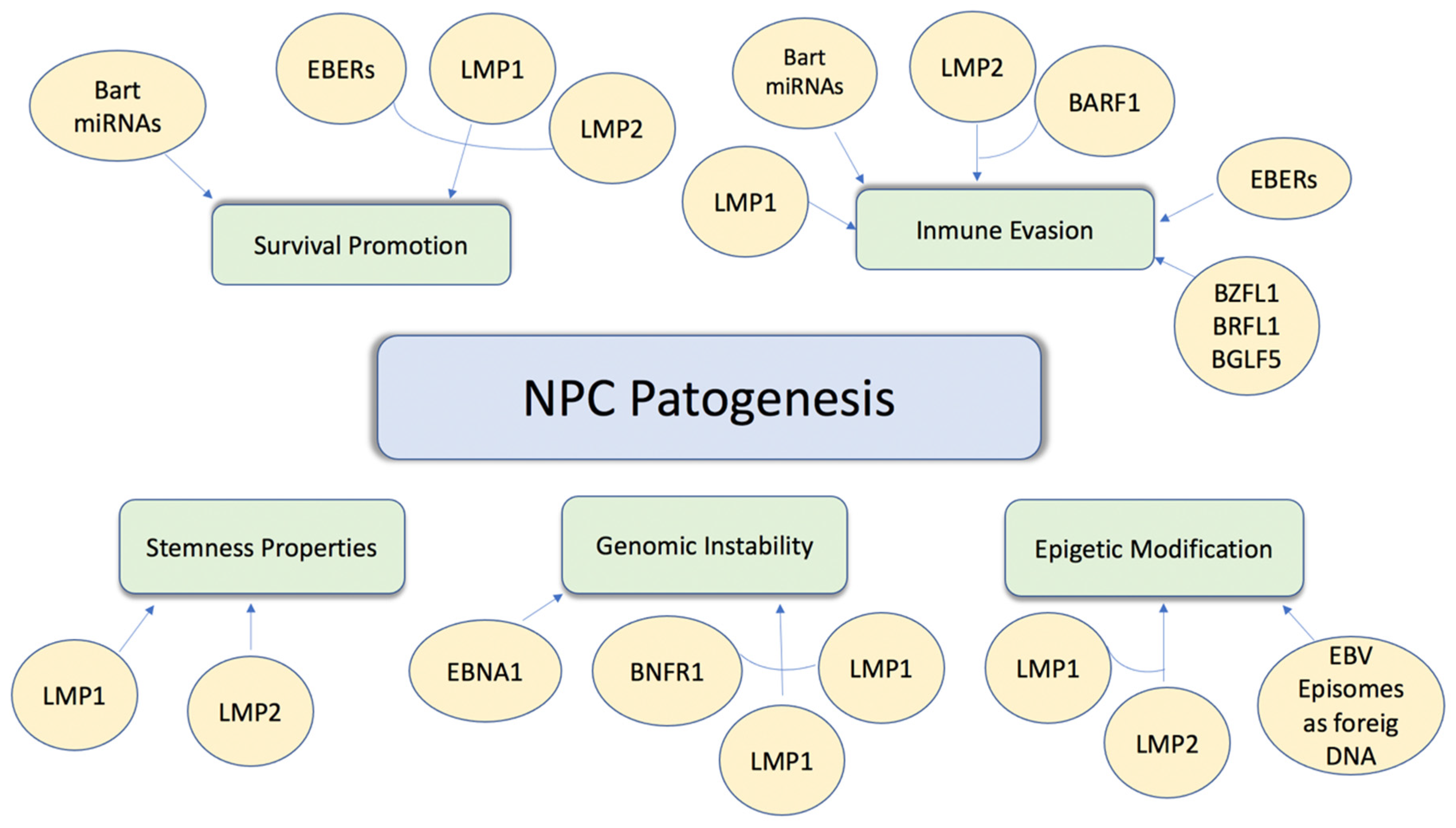
4. Epstein-Barr Virus
5. Hepatitis B and C Viruses
6. Other Viruses
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CPS | combined positive score |
| CTLA-4 | cytotoxic T-lymphocyte antigen 4 |
| EBNA1 | Epstein–Barr nuclear antigen 1 |
| EBV | Epstein–Barr virus |
| EBV-GC | Epstein–Barr virus—gastric cancer |
| ECOG | Eastern Cooperative Oncology Group |
| GC | gastric cancer |
| HBV | hepatitis B virus |
| HCC | hepatocellular carcinoma |
| HCV | hepatitis C virus |
| HHV-8 | human gammaherpesvirus 8 |
| HIV | human immunodeficiency viruses |
| HPV | human papillomavirus |
| HTLV-1 | human T-lymphotropic virus 1 |
| ICIs | immune checkpoint inhibitors |
| LMP1 | latent membrane protein 1 |
| LMP2 | latent membrane protein 2 |
| NPC | nasopharyngeal carcinoma |
| MCPyV | Merkel cell polyomavirus |
| ORR | overall response rate |
| OS | overall survival |
| PD-1 | programmed death 1 |
| PDL-1 | programmed death-ligand 1 |
| PFS | progression free survival |
| R/M | recurrent/metastatic |
| TILs | tumour-infiltrating lymphocytes |
References
- Tashiro, H.; Brenner, M.K. Immunotherapy against cancer-related viruses. Cell Res. 2017, 27, 59–73. [Google Scholar] [CrossRef] [PubMed]
- Morales-Sánchez, A.; Fuentes-Pananá, E.M. Human viruses and cancer. Viruses 2014, 6, 4047–4079. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.J.; You, S.L.; Hsu, W.L.; Yang, H.W.; Lee, M.H.; Chen, H.C.; Chen, Y.Y.; Liu, J.; Hu, H.H.; Lin, Y.J.; et al. Epidemiology of Virus Infection and Human Cancer. Recent Results Cancer Res. 2021, 217, 13–45. [Google Scholar]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Akram, N.; Imran, M.; Noreen, M.; Ahmed, F.; Atif, M.; Fatima, Z.; Bilal Waqar, A. Oncogenic role of tumours viruses in humans. Viral Immunol. 2017, 30, 20–27. [Google Scholar] [CrossRef] [PubMed]
- Kanwal, F.; Kramer, J.R.; Ilyas, J.; Duan, Z.; El-Serag, H.B. HCV genotype 3 is associated with an increased risk of cirrhosis and hepatocellular cancer in a national sample of U.S. Veterans with HCV. Hepatology 2014, 60, 98–105. [Google Scholar] [CrossRef]
- McNally, G.A. HIV and Cancer: An Overview of AIDS-Defining and Non-AIDS-Defining Cancers in Patients with HIV. Clin. J. Oncol. Nurs. 2019, 23, 327–331. [Google Scholar]
- Gao, P.; Lazare, C.; Cao, C.; Meng, Y.; Wu, P.; Zhi, W.; Lin, S.; Wei, J.; Huang, X.; Xi, L.; et al. Immune checkpoint inhibitors in the treatment of virus-associated cancers. J. Hematol. Oncol. 2019, 12, 58. [Google Scholar] [CrossRef]
- Darvin, P.; Toor, S.M.; Nair, V.S.; Elkord, E. Immune checkpoint inhibitors: Recent progress and potential biomarkers. Exp. Mol. Med. 2018, 50, 1–11. [Google Scholar] [CrossRef]
- McCarthy, E.F. The Toxins of William B. Coley and the Treatment of Bone and Soft-Tissue Sarcomas. Iowa Orthop. J. 2006, 26, 154–158. [Google Scholar]
- Lin, Z.; Meng, X.; Wen, J.; Corral, J.M.; Andreev, D.; Kachler, K.; Schett, G.; Chen, X.; Bozec, A. Intratumor Heterogeneity Correlates with Reduced Immune Activity and Worse Survival in Melanoma Patients. Front. Oncol. 2020, 10, 596493. [Google Scholar] [CrossRef]
- Inthagard, J.; Edwards, J.; Roseweir, A.K. Immunotherapy: Enhancing the efficacy of this promising therapeutic in multiple cancers. Clin. Sci. 2019, 133, 181–193. [Google Scholar] [CrossRef]
- Rowshanravan, B.; Halliday, N.; Sansom, D.M. CLTA-4: A moving target in immunotherapy. Blood 2018, 131, 58–67. [Google Scholar] [CrossRef]
- Salmaninejad, A.; Valilou, S.F.; Shabgah, A.G.; Aslani, S.; Alimardani, M.; Pasdar, A.; Sahebkar, A. PD-1/PD-L1 pathway: Basic biology and role in cancer immunotherapy. J. Cell Physiol. 2019, 234, 16824–16837. [Google Scholar] [CrossRef]
- Bai, R.; Lv, Z.; Xu, D.; Cui, J. Predictive biomarkers for cancer immunotherapy with immune checkpoint inhibitors. Biomark. Res. 2020, 26, 34. [Google Scholar] [CrossRef]
- Spencer, K.R.; Wang, J.; Silk, A.W.; Ganesan, S.; Kaufman, H.L.; Mehnert, J.M. Biomarkers for Immunotherapy: Current Developments and Challenges. Am. Soc. Clin. Oncol. Educ. Book 2016, 35, e493–e503. [Google Scholar] [CrossRef]
- Briant, P.; De Flammineis, E.; Mercuri, S.R. Review of HPV-related diseases and cancers. New Microbiol. 2017, 40, 80–85. [Google Scholar]
- Szymonowicz, K.A.; Chen, J. Biological and clinical aspects of HPV-related cancers. Cancer Biol. Med. 2020, 17, 864–878. [Google Scholar] [CrossRef] [PubMed]
- Lei, J.; Ploner, A.; Elfström, K.M.; Wang, J.; Roth, A.; Fang, F.; Sundström, K.; Dillner, J.; Sparén, P. HPV Vaccination and the Risk of Invasive Cervical Cancer. N. Engl. J. Med. 2020, 383, 1340–1348. [Google Scholar] [CrossRef] [PubMed]
- Huibregtse, J.M.; Beaudenon, S.L. Mechanism of HPV E6 proteins in cellular transformation. Semin. Cancer Biol. 1996, 7, 317–326. [Google Scholar] [CrossRef]
- McLaughlin-Drubin, M.E.; Münger, K. The human papillomavirus E7 oncoprotein. Virology 2009, 384, 335–344. [Google Scholar] [CrossRef]
- Elrefaey, S.; Massaro, M.A.; Chiocca, S.; Chiesa, F.; Ansarin, M. HPV in oropharyngeal cancer: The basics to know in clinical practice. Acta Otorhinolaryngol. Ital. 2014, 34, 299–309. [Google Scholar] [PubMed]
- Lechien, J.R.; Seminerio, I.; Descamps, G.; Mat, Q.; Mouawad, F.; Hans, S.; Julieron, M.; Dequanter, D.; Vanderhaegen, T.; Journe, F.; et al. Impact of HPV Infection on the Immune System in Oropharyngeal and Non-Oropharyngeal Squamous Cell Carcinoma: A Systematic Review. Cells 2019, 8, 1061. [Google Scholar] [CrossRef]
- De Felice, F.; Tombolini, V.; Valentini, V.; De Vincentiis, M.; Mezi, S.; Brugnoletti, O.; Polimeni, A. Advances in the Management of HPV-Related Oropharyngeal Cancer. J. Oncol. 2019, 2019, 9163729. [Google Scholar] [CrossRef]
- Baumi, J.M.; Aggarwal, C.; Cohen, R.B. Immunotherapy for head and neck cancer: Where are we now and where are we going? Ann. Transl Med. 2019, 7, S75. [Google Scholar]
- Burtness, B.; Harrington, K.J.; Greil, R.; Souliéres, D.; Tahara, M.; de Castro, G., Jr.; Psyrri, A.; Basté, N.; Neupane, P.; Bratland, Å.; et al. Pembrolizumab alone or with chemotherapy versus cetuximab with chemotherapy for recurrent or metastatic squamous cell carcinoma of the head and neck (KEYNOTE-048): A randomised, open-label, phase 3 study. Lancet 2019, 394, 1915–1928. [Google Scholar] [CrossRef]
- Seiwert, T.Y.; Burtness, B.; Mehra, R.; Weiss, J.; Berger, R.; Eder, J.P.; Heath, K.; McClanahan, T.; Lunceford, J.; Gause, C.; et al. Safety and clinical activity of pembrolizumab for treatment of recurrent or metastatic squamous cell carcinoma of the head and neck (KEYNOTE-012): An open-label, multicentre, phase 1b trial. Lancet Oncol. 2016, 17, 956–965. [Google Scholar] [CrossRef]
- Zandberg, D.P.; Algazi, A.P.; Jimeno, A.; Good, J.S.; Fayette, J.; Bouganim, N.; Ready, N.E.; Clement, P.M.; Even, C.; Jang, R.W.; et al. Durvalumab for recurrent or metastatic head and neck squamous cell carcinoma: Results from a single-arm, phase II study in patients with ≥25% tumour cell PD-L1 expression who have progressed on platinum-based chemotherapy. Eur. J. Cancer 2019, 107, 142–152. [Google Scholar] [CrossRef]
- Patel, J.J.; Levy, D.A.; Nguyen, S.A.; Knochekmann, H.M.; Day, T.A. Impact of PD-L1 expression and human papillomavirus status in anti-PD1/PDL1 immunotherapy for head and neck squamous cell carcinoma-Systematic review and meta-analysis. Head Neck 2020, 42, 774–786. [Google Scholar] [CrossRef] [PubMed]
- Naumann, R.W.; Hollebecque, A.; Meyer, T.; Devlin, M.-J.; Oaknin, A.; Kerger, J.; López-Picazo, J.M.; Machiels, J.-P.; Delord, J.-P.; Evans, T.R.J.; et al. Safety and Efficacy of Nivolumab Monotherapy in Recurrent or Metastatic Cervical, Vaginal, or Vulvar Carcinoma: Results From the Phase I/II CheckMate 358 Trial. J. Clin. Oncol. 2019, 37, 2825–2834. [Google Scholar] [CrossRef] [PubMed]
- Mezache, L.; Paniccia, B.; Nyunawabera, A.; Nuovo, G.J. Enhanced expression of PD L1 in cervical intraepithelial neoplasia and cervical cancers. Mod. Pathol. 2015, 28, 1594–1602. [Google Scholar] [CrossRef]
- Liu, C.; Lu, J.; Tian, H.; Du, W.; Zhao, L.; Feng, J.; Yuan, D.; Li, Z. Increased expression of PD-L1 by the human papillomavirus 16 E7 oncoprotein inhibits anticancer immunity. Mol. Med. Rep. 2017, 15, 1063–1070. [Google Scholar] [CrossRef]
- Usta, C.S.; Altun, E.; Afsar, S.; Bulbul, C.B.; Usta, A.; Adali, E. Overexpression of programmed cell death ligand 1 in patients with CIN and its correlation with human papillomavirus infection and CIN persistence. Infect. Agent Cancer 2020, 17, 47. [Google Scholar] [CrossRef]
- Zacny, V.L.; Gershburg, E.; Davis, M.G.; Biron, K.K.; Pagano, J.S. Inhibition of Epstein-Barr virus replication by a benzimidazole L-riboside: Novel antiviral mechanism of 5, 6-dichloro-2-(isopropylamino)-1-beta-L-ribofuranosyl-1H-benzimidazole. J. Virol. 1999, 73, 7271–7277. [Google Scholar] [CrossRef] [PubMed]
- Odumade, O.A.; Hogquist, K.A.; Balfour, H.H., Jr. Progress and problems in understanding and managing primary Epstein-Barr virus infections. Clin. Microbiol. Rev. 2011, 24, 193–209. [Google Scholar] [CrossRef]
- Thorley-Lawson, D.A.; Gross, A. Persistence of the Epstein-Barr virus and the origins of associated lymphomas. N. Engl. J. Med. 2004, 350, 1328–1337. [Google Scholar] [CrossRef] [PubMed]
- Raghupathy, R.; Hui, E.P.; Chan, A.T. Epstein-Barr virus as a paradigm in nasopharyngeal cancer: From lab to clinic. Am. Soc. Clin. Oncol. Educ. Book 2014, 34, 149–153. [Google Scholar] [CrossRef] [PubMed]
- Tsao, S.W.; Tsang, C.M.; Lo, K.W. Epstein-Barr virus infection and nasopharyngeal carcinoma. Philos. Trans. R. Soc. Lond. B Biol. Sci. 2017, 372, 20160270. [Google Scholar] [CrossRef]
- Hong, M.; Tang, K.; Qian, J.; Deng, H.; Zeng, M.; Zheng, S.; Ding, K.; Du, Y.; Sun, R. Immunotherapy for EBV-associated nasopharyngeal carcinoma. Crit. Rev. Oncog. 2018, 23, 219–234. [Google Scholar] [CrossRef]
- Ma, B.; Lim, W.T.; Goh, B.C.; Hui, E.P.; Lo, K.W.; Pettinger, A.; Foster, N.R.; Riess, J.W.; Agulnik, M.; Chang, A.; et al. Antitumor Activity of Nivolumab in Recurrent and Metastatic Nasopharyngeal Carcinoma: An International, Multicenter Study of the Mayo Clinic Phase 2 Consortium (NCI-9742). J. Clin. Oncol. 2018, 36, 1412–1418. [Google Scholar] [CrossRef]
- Wang, F.H.; Wei, X.L.; Feng, J.; Li, Q.; Xu, N.; Hu, X.C.; Liao, W.; Jiang, Y.; Lin, X.Y.; Zhang, Q.Y.; et al. Efficacy, Safety, and Correlative Biomarkers of Toripalimab in Previously Treated Recurrent or Metastatic Nasopharyngeal Carcinoma: A Phase II Clinical Trial (POLARIS-02). J. Clin. Oncol. 2021, 39, 704–712. [Google Scholar] [CrossRef]
- Boysen, T.; Mohammadi, M.; Melbye, M.; Hamilton-Dutoit, S.; Vainer, B.; Hansen, A.V.; Wohlfahrt, J.; Friborg, J. EBV-associated gastric carcinoma in high- and low-incidence areas for nasopharyngeal carcinoma. Br. J. Cancer 2009, 101, 530–533. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Shinozaki-Ushiku, A.; Kunita, A.; Fukayama, M. Update on Epstein-Barr virus and gastric cancer (review). Int. J. Oncol. 2015, 46, 1421–1434. [Google Scholar] [CrossRef]
- Chang, M.S.; Uozaki, H.; Chong, J.M.; Ushiku, T.; Sakuma, K.; Ishikawa, S.; Hino, R.; Barua, R.R.; Iwasaki, Y.; Arai, K.; et al. CpG island methylation status in gastric carcinoma with and without infection of Epstein-Barr virus. Clin. Cancer Res. 2006, 12, 2995–3002. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Kim, S.H.; Han, S.H.; An, J.S.; Lee, E.S.; Kim, Y.S. Clinicopathological and molecular characteristics of Epstein-Barr virus-associated gastric carcinoma: A meta-analysis. J. Gastroenterol. Hepatol. 2009, 24, 354–365. [Google Scholar] [CrossRef]
- Xie, T.; Liu, Y.; Zhang, Z.; Zhang, X.; Gong, J.; Qi, C.; Li, J.; Shen, L.; Peng, Z. Positive Status of Epstein-Barr Virus as a Biomarker for Gastric Cancer Immunotherapy: A Prospective Observational Study. J. Immunother. 2020, 43, 139–144. [Google Scholar] [CrossRef]
- Kim, S.J.; Hyeon, J.; Cho, I.; Ko, Y.H.; Kim, W.S. Comparison of Efficacy of Pembrolizumab between Epstein-Barr Virus—Positive and—Negative Relapsed or Refractory Non-Hodgkin Lymphomas. Cancer Res. Treat. 2019, 51, 611–622. [Google Scholar] [CrossRef]
- Petrick, J.; McGlynn, K. The changing epidemiology of primary liver cancer. Curr. Epidemiol. Rep. 2019, 6, 104–111. [Google Scholar] [CrossRef] [PubMed]
- Petruzzielo, A. Epidemiology of Hepatitis B Virus (HBV) and Hepatitis C Virus (HCV) Related Hepatocellular Carcinoma. Open Virol. J. 2018, 12, 26–32. [Google Scholar] [CrossRef]
- Kremsdorf, D.; Soussan, P.; Paterlini-Brechot, P.; Brechot, C. Hepatitis B virus-related hepatocellular carcinoma: Paradigms. Oncogene 2006, 25, 3823–3833. [Google Scholar] [CrossRef]
- Lee, A.T.; Lee, C.G. Oncogenesis and transforming viruses: The hepatitis B virus and hepatocellularcarcinoma—the etiopathogenic link. Front. Biosci. 2007, 1, 234–245. [Google Scholar] [CrossRef]
- Goossens, N.; Hoshida, Y. Hepatitis C virus-induced hepatocellular carcinoma. Clin. Mol. Hepatol. 2015, 21, 105–114. [Google Scholar] [CrossRef]
- Pardee, A.D.; Butterfield, L.H. Immunotherapy of hepatocellular. Oncoimmunology 2012, 1, 48–55. [Google Scholar] [CrossRef]
- Sangro, B.; Sarobe, P.; Hervás-Stubbs, S.; Melero, I. Advances in immunotherapy for hepatocellular carcinoma. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 525–543. [Google Scholar] [CrossRef]
- El-Khoueiry, A.B.; Sangro, B.; Yau, T.; Crocenzi, T.S.; Kudo, M.; Hsu, C.; Kim, T.Y.; Choo, S.P.; Trojan, J.; Welling, T.H.; et al. Nivolumab in patients with advanced hepatocellular carcinoma (CheckMate 040): An open-label, non-comparative, phase 1/2 dose escalation and expansion trial. Lancet 2017, 389, 2492–2502. [Google Scholar] [CrossRef]
- Yau, T.; Park, J.W.; Finn, R.S.; Cheng, A.L.; Mathurin, P.; Edeline, J.; Kudo, M.; Han, K.H.; Harding, J.J.; Merle, P.; et al. CheckMate 459: A randomized, multi-center phase III study of nivolumab (NIVO) vs. sorafenib (SOR) as first-line (1L) treatment in patients (pts) with advanced hepatocellular carcinoma (aHCC). Ann. Oncol. 2019, 30, 874–875. [Google Scholar] [CrossRef]
- Finn, R.S.; Ryoo, B.Y.; Merle, P.; Kudo, M.; Bouattour, M.; Lim, H.Y.; Breder, V.; Edeline, J.; Chao, Y.; Ogasawara, S.; et al. Pembrolizumab As Second-Line Therapy in Patients With Advanced Hepatocellular Carcinoma in KEYNOTE-240: A Randomized, Double-Blind, Phase III Trial. J. Clin. Oncol. 2020, 38, 193–202. [Google Scholar] [CrossRef]
- Finn, R.S.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.Y.; Kudo, M.; Breder, V.; Merle, P.; Kaseb, A.O.; et al. Atezolizumab plus Bevacizumab in Unresectable Hepatocellular Carcinoma. N. Engl. J. Med. 2020, 382, 1894–1905. [Google Scholar] [CrossRef] [PubMed]
- D’Angelo, S.P.; Bhatia, S.; Brohl, A.S.; Hamid, O.; Mehnert, J.M.; Terheyden, P.; Shih, K.C.; Brownell, I.; Lebbé, C.; Lewis, K.D.; et al. Avelumab in patients with previously treated metastatic Merkel cell carcinoma: Long-term data and biomarker analyses from the single-arm phase 2 JAVELIN Merkel 200 trial. J. Immunother. Cancer 2020, 8, e000674. [Google Scholar] [CrossRef]
- Marchand, A.; Kervarrec, T.; Bhatia, S.; Samini, M. Pembrolizumab and other immune checkpoint inhibitors in locally advanced or metastatic Merkel Cell Carcinoma: Safety and efficacy. Expert Rev. Anticancer Ther. 2020, 20, 1093–1106. [Google Scholar] [CrossRef]


{kind=link}
| Virus | Cancer | Prevalence in the Tumour |
|---|---|---|
| HPV | Cervix | 100% |
| Penile | 50% | |
| Vaginal | 70% | |
| Anal | 80–90% | |
| Vulvar | 40–50% | |
| Oropharynx | 20–50% | |
| HBV | Liver | 20–60% |
| HCV | Liver | 20–30% |
| EBV | Hodgkin’s lymphoma | 40–90% |
| Burkitt’s lymphoma | 20–100% | |
| Nasopharyngeal carcinoma | 50–100% | |
| MCPyV | Merkel cell carcinoma | 50–80% |
| HHV-8 (KSHV) | Kaposi´s sarcoma | 100% |
| HTLV-1 | Adult T-cell leukaemia and lymphoma | 100% |
| Immune Checkpoint Inhibitors | Immunoglobulin Type | Target Molecule | Treatment of Different Tumours |
|---|---|---|---|
| Ipilimumab (MDX-010) | IgG-1κ | CTLA-4 | Advanced melanoma Advanced renal cancer |
| Pembrolizumab (MK-3475) | IgG-4κ | PD-1 | Advanced melanoma and adjuvant Metastatic non-small cell lung cancer Advanced bladder cancer Advanced head and neck cancer |
| Nivolumab (MDX-1106) | IgG4 | PD-1 | Advanced melanoma and adjuvant Metastatic non-small cell lung cancer Advanced bladder cancer Advanced head and neck cancer Advanced renal cancer |
| Cemiplimab (L01XC33) | IgG4 | PD-1 | Cutaneous Squamous Cell Carcinoma |
| Atezolizumab (MPDL3280A) | IgG1 | PD-L1 | Advanced bladder cancer Metastatic non-small cell lung cancer |
| Durvalumab (MEDI4736) | IgG1 | PD-L1 | Locally advanced unresectable non-small cell lung cancer |
| Avelumab (MSB0010718C) | IgG1 | PD-L1 | Metastatic Merkel cell carcinoma |
| Clinical Trial | Phase | Tumours | Drugs | Relationship between ICIs and Viruses |
|---|---|---|---|---|
| KEYNOTE-012 | 1b | Squamous cell carcinoma of head and neck | Pembrolizumab | Tendency to greater response and survival was observed in HPV+ versus HPV- oropharyngeal tumours. |
| HAWK | 2 | Squamous cell carcinoma of head and neck | Durvalumab | In an ad hoc analysis the percentage of responses was higher in patients with HPV+. |
| CheckMate-358 | 1/2 | Recurrent or metastatic cervical, vaginal, or vulvar carcinoma | Nivolumab | Disease control rate in gynecological tumours VPH+ 70.8%. |
| NCI-9742 | 2 | Recurrent and metastatic nasopharyngeal carcinoma | Nivolumab | No statistical correlation between ORR and plasma EBV DNA clearance |
| POLARIS-02 | 2 | Recurrent or metastatic nasopharyngeal carcinoma | Toripalimab | A reduction of ≥50% in the plasma DNA copy number of EBV at day 28 of treatment was associated with a statistically significantly better ORR |
| Kim et al. (not clinical trial, prospective study) | - | Relapsed or refractory non-Hodgkin lymphomas | Pembrolizumab | Tendency a high expression of PDL-1 in EBV+ tumours. |
| CheckMate-040 | 1/2 | Advanced hepatocellular carcinoma | Nivolumab | Better ORR and disease control in HCV infected versus HBV infected tumours. |
| CheckMate-459 | 3 | Advanced hepatocellular carcinoma | Nivolumab | No differences by subgroups. |
| KEYNOTE-224 | 2 | Advanced hepatocellular carcinoma | Pembrolizumab | No differences by subgroups. |
| KEYNOTE-240 | 3 | Advanced hepatocellular carcinoma | Pembrolizumab | Better OS in HBV+ versus HCV- or not infected. |
| IMbrave 150 | 3 | Advanced hepatocellular carcinoma | Atezolizumab | No differences by subgroups. |
| JAVELIN Merkel 200 | 2 | Metastatic Merkel cell carcinoma | Avelumab | No differences by subgroups. |
| NCT02267603 | 2 | Metastatic Merkel cell carcinoma | Pembrolizumab | High PDL-1 expression in MCPyV+ versus MCPyV- tumours. PDL-1 values did not influence in the response to Pembrolizumab. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Olivares-Hernández, A.; Figuero-Pérez, L.; Miramontes-González, J.P.; López-Gutiérrez, Á.; González-Sarmiento, R.; Cruz-Hernández, J.J.; Fonseca-Sánchez, E. Immune System Disorders, Cancer and Viral Infections: A New Treatment Opportunity for the Immune Checkpoint Inhibitors. Life 2021, 11, 1400. https://doi.org/10.3390/life11121400
Olivares-Hernández A, Figuero-Pérez L, Miramontes-González JP, López-Gutiérrez Á, González-Sarmiento R, Cruz-Hernández JJ, Fonseca-Sánchez E. Immune System Disorders, Cancer and Viral Infections: A New Treatment Opportunity for the Immune Checkpoint Inhibitors. Life. 2021; 11(12):1400. https://doi.org/10.3390/life11121400
Chicago/Turabian StyleOlivares-Hernández, Alejandro, Luis Figuero-Pérez, José Pablo Miramontes-González, Álvaro López-Gutiérrez, Rogelio González-Sarmiento, Juan Jesús Cruz-Hernández, and Emilio Fonseca-Sánchez. 2021. "Immune System Disorders, Cancer and Viral Infections: A New Treatment Opportunity for the Immune Checkpoint Inhibitors" Life 11, no. 12: 1400. https://doi.org/10.3390/life11121400
APA StyleOlivares-Hernández, A., Figuero-Pérez, L., Miramontes-González, J. P., López-Gutiérrez, Á., González-Sarmiento, R., Cruz-Hernández, J. J., & Fonseca-Sánchez, E. (2021). Immune System Disorders, Cancer and Viral Infections: A New Treatment Opportunity for the Immune Checkpoint Inhibitors. Life, 11(12), 1400. https://doi.org/10.3390/life11121400