
The Design and User Evaluation of Body-Transfer System via Sliding Transfer Approach for Assisting Functionally Impaired People



Abstract
1. Introduction
- 1.
- How can a person be moved from a bed to a wheelchair without altering their posture and angle in the sagittal plane?
- 2.
- How can a physically disabled person attain active assistive living (AAL) using various smart home robotic modules?
- 3.
- How is a human-friendly and intelligent interface developed for a physically disabled person by which activities of daily living can be performed independently?
- 1.
- This research focuses on achieving AAL by utilizing a fully integrated body-transfer system to support the user in transferring from bed to wheelchair.
- 2.
- To mitigate the risk of injuries from a traditional lifting arrangement during the body transfer from a bed to a wheelchair, this is replaced with the sliding transfer approach. Furthermore, the developed system can assist users in the bathroom and toilet.
- 3.
- Furthermore, this study proposes a user-friendly architecture to efficiently manage all the body-transfer smart home assistive devices.
2. State-of-the-Art Assistive Transfer Systems
3. The Body-Transfer Smart Home Design Concept
3.1. Proposed Solution
3.1.1. Design of Body-Transfer Bed
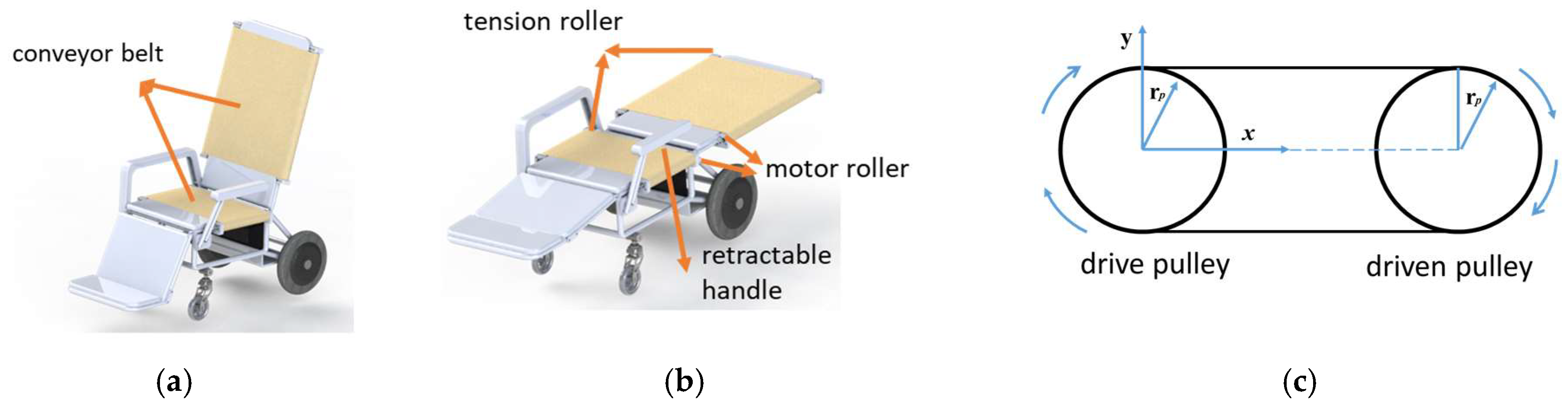
3.1.2. Design of Body-Transfer Wheelchair
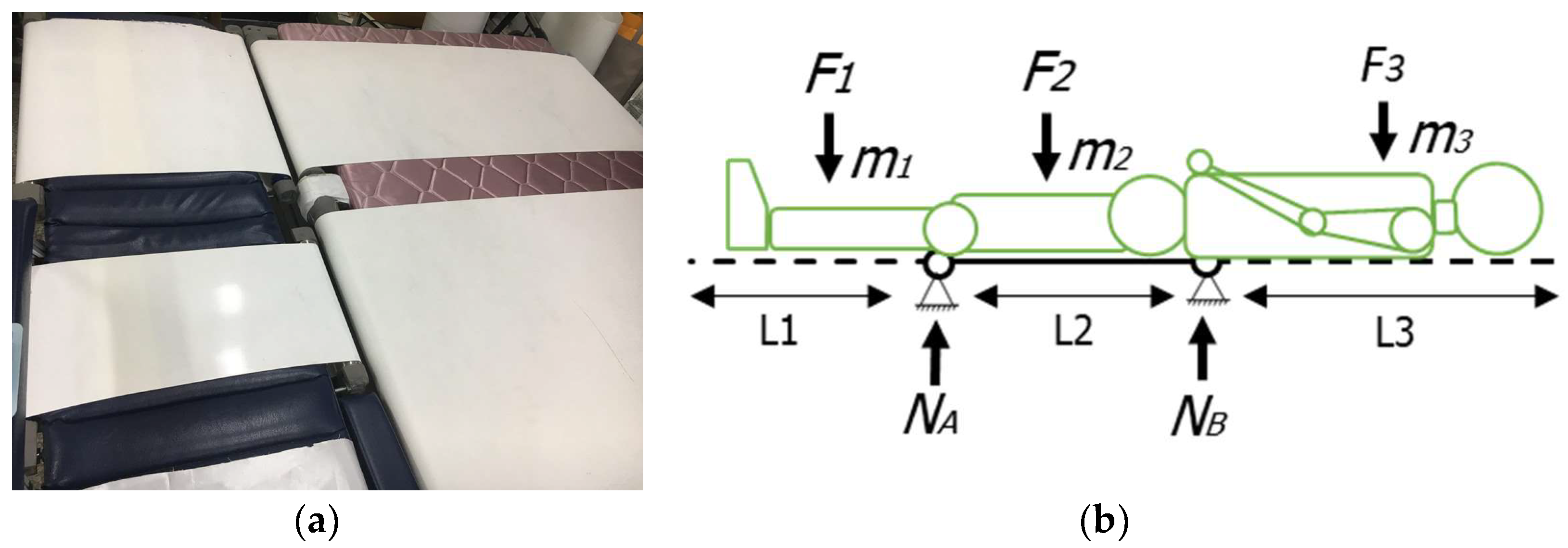
3.1.3. Reclining and Leg-Raising Force Evaluation
3.1.4. Transfer Mechanism
3.1.5. Hand rest Mechanism
3.1.6. Wheelchair Drive Mechanism
3.1.7. Body-Transfer Toilet Wheelchair (BTTW)
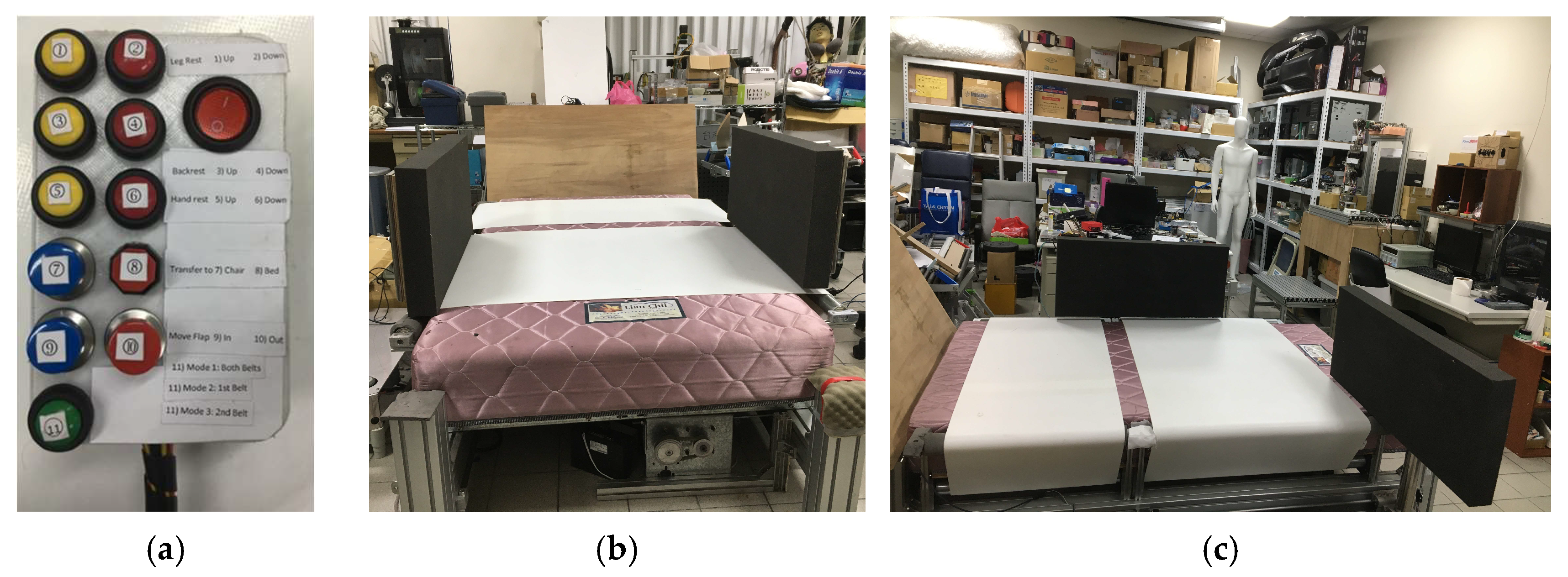
3.1.8. Operational and Control System
3.1.9. Control Architecture of the Transfer System
3.2. Task Scenarios
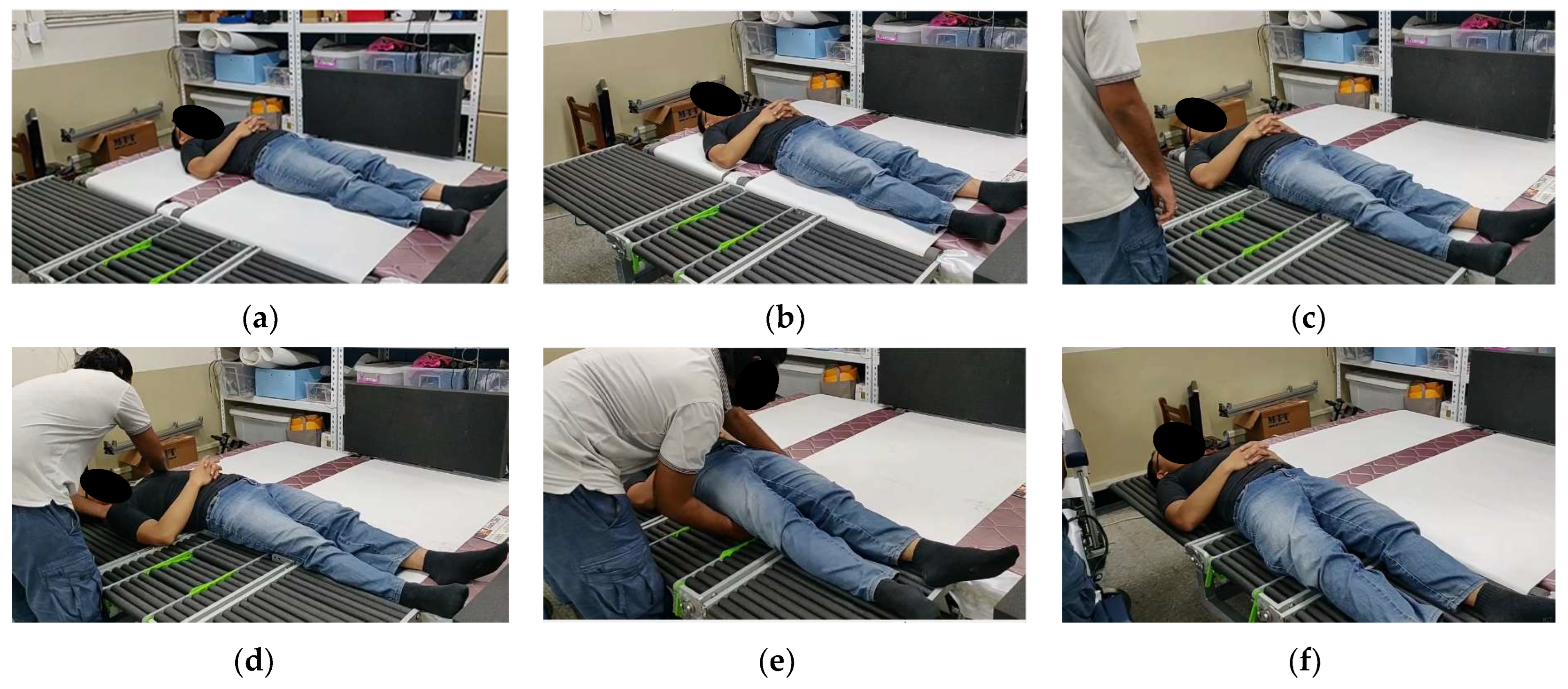
3.2.1. Task Scenario 1: Transfer from Body-Transfer Bed to Body-Transfer Wheelchair and Vice Versa
3.2.2. Task Scenario 2: Transfer from Body-Transfer Wheelchair to Body-Transfer Toilet Wheelchair and Vice Versa
3.2.3. Task Scenario 3: Transfer from Body-Transfer Bed to Body-Transfer Toilet Wheelchair and Vice Versa
4. User Evaluation of the Body-Transfer System
5. Discussion
6. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. World Report on Disability, 1st ed.; World Health Organization: Geneva, Switzerland, 2011; Volume 1, pp. 44–61. [Google Scholar]
- United Nations. Facts on People with Disabilities in China, 1st ed.; International Labour Organization (ILO): Geneva, Switzerland, 2013; Volume 1, pp. 4–5. [Google Scholar]
- Velayutham, B.; Kangusamy, B.; Joshua, V.; Mehendale, S. The prevalence of disability in elderly in India–analysis of 2011 census data. Disabil. Health J. 2016, 9, 584–592. [Google Scholar] [CrossRef]
- Chino, M. Statistical Handbook of Japan 2017, 1st ed.; Statistics Bureau Ministry of Internal Affairs and Communications Japan: Tokyo, Japan, 2017; Volume 1, pp. 9–13. [Google Scholar]
- Yang, C.C.; Chen, S.C. Taiwan Health and Welfare Report 2017; Taiwan Ministry of Health and Welfare (MOHW): Taipei City, Taiwan, 2017; Volume 180, pp. 10–26. [Google Scholar]
- National Development Council. Population Projections for the ROC (Taiwan): 2018–2065. Available online: https://www.ndc.gov.tw/en/cp.aspx?n=2e5dcb04c64512cc (accessed on 5 August 2022).
- Tatsuo, O. Statistics on disabled people in Japan. Aino J. 2010, 8, 3–10. [Google Scholar]
- Cohen-Mansfield, J.; Culpepper, W.J.; Carter, P. Nursing staff back injuries: Prevalence and costs in long term care facilities. Am. Assoc. Occup. Health Nurses J. 1996, 44, 9–17. [Google Scholar] [CrossRef]
- Jiska, C.M. Assessment of agitation. Int. Psychogeriatr. 1996, 8, 233–245. [Google Scholar]
- Guo, H.R.; Tanaka, S.; Cameron, L.L.; Seligman, P.J.; Behrens, V.J.; Ger, J.; Wild, D.K.; Putz-Anderson, V. Back pain among workers in the United States: National estimates and workers at high risk. Am. J. Ind. Med. 1995, 28, 591–602. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.; Haldeman, S.; Lu, M.L.; Baker, D. Low back pain prevalence and related workplace psychosocial risk factors: A study using data from the 2010 national health interview survey. J. Manip. Physiol. Ther. 2016, 39, 459–472. [Google Scholar] [CrossRef] [PubMed]
- Group, P. Panasonic’s Robotic Technology Helps Deliver “A Better Life” to the World of Welfare. Available online: https://www.newswire.co.kr/newsRead.php?no=768853 (accessed on 31 July 2022).
- Kume, Y.; Tsukada, S.; Kawakami, H. Development of safety technology for rise assisting robot Resyone Plus. Dyn. Control. Robot. Mechatron. 2019, 85, 869–889. [Google Scholar] [CrossRef]
- Bakouri, M.; Alsehaimi, M.; Ismail, H.F.; Alshareef, K.; Ganoun, A.; Alqahtani, A.; Alharbi, Y. Steering a robotic wheelchair based on voice recognition system using convolutional neural networks. Electronics 2022, 11, 168–188. [Google Scholar] [CrossRef]
- Sivakanthan, S.; Blaauw, E.; Greenhalgh, M.; Koontz, A.M.; Vegter, R.; Cooper, R.A. Person transfer assist systems: A literature review. Disabil. Rehabil. Assist. Technol. 2021, 16, 270–279. [Google Scholar] [CrossRef]
- Mori, Y.; Sakai, N.; Katsumura, K. Development of a wheelchair with a lifting function. Adv. Mech. Eng. 2012, 4, 489–492. [Google Scholar] [CrossRef]
- Grindle, G.G.; Wang, H.; Jeannis, H.; Teodorski, E.; Cooper, R.A. Design and user evaluation of a wheelchair mounted robotic assisted transfer device. BioMed Res. Int. 2015, 15, 405–423. [Google Scholar] [CrossRef]
- Tian, Y.; Wang, H.; Zhang, Y.; Su, B.; Wang, L.; Wang, X.; Sang, L.; Feng, Y.; Niu, J. Design and evaluation of a novel person transfer assist system. IEEE Access 2021, 9, 14306–14318. [Google Scholar] [CrossRef]
- Mukai, T.; Hirano, S.; Nakashima, H.; Sakaida, Y.; Guo, S. Realization and safety measures of patient transfer by nursing-care assistant robot riba with tactile sensors. J. Robot. Mechatron. 2011, 23, 360–369. [Google Scholar] [CrossRef]
- Bostelman, R.; Ryu, J.C.; Chang, T.; Johnson, J.; Agrawal, S.K. An advanced patient lift and transfer device for the home. J. Med. Devices 2010, 4, 345–365. [Google Scholar] [CrossRef]
- Bostelman, R.; Albus, J. A multipurpose robotic wheelchair and rehabilitation device for the home. In Proceedings of the 2007 IEEE/RSJ International Conference on Intelligent Robots and Systems, San Diego, CA, USA, 29 October–2 November 2007; pp. 3348–3353. [Google Scholar]
- Jung, J.W.; Do, J.H.; Kim, Y.M.; Suh, K.S.; Kim, D.J.; Bien, Z.Z. Advanced robotic residence for the elderly/the handicapped: Realization and user evaluation. In Proceedings of the 9th International Conference on Rehabilitation Robotics (ICORR), Chicago, IL, USA, 28 June–1 July 2005; pp. 492–495. [Google Scholar]
- Park, K.H.; Bien, Z.; Lee, J.J.; Kim, B.K.; Lim, J.T.; Kim, J.O.; Lee, H.; Stefanov, D.H.; Kim, D.J.; Jung, J.W. Robotic smart house to assist people with movement disabilities. Auton. Robot. 2007, 22, 183–198. [Google Scholar] [CrossRef]
- Bien, Z.Z.; Lee, H.E.; Do, J.H.; Kim, Y.H.; Park, K.H.; Yang, S.E. Intelligent interaction for human-friendly service robot in smart house environment. Int. J. Comput. Intell. Syst. 2008, 1, 77–93. [Google Scholar]
- Seo, K.H.; Choi, T.Y.; Oh, C. Development of a robotic system for the bed-ridden. Mechatronics 2011, 21, 227–238. [Google Scholar] [CrossRef]
- Ning, M.; Ren, M.; Fan, Q.; Zhang, L. Mechanism design of a robotic chair/bed system for bedridden aged. Adv. Mech. Eng. 2017, 9, 1–8. [Google Scholar] [CrossRef]
- Kulich, H.R.; Wei, L.; Crytzer, T.M.; Cooper, R.A.; Koontz, A.M. Preliminary evaluation of an automated robotic transfer assist device in the home setting. Disabil. Rehabil. Assist. Technol. 2021, 1, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Sivaprakasam, A.; Cooper, R.; Koontz, A. Evaluation of the Agilelife patient transfer and movement system. In Proceedings of the Rehabilitation Engineering and Assistive Technology Society of North America (RESNA) Annual Conference, New Orleans, LA, USA, 26–30 June 2017; pp. 30–33. [Google Scholar]
- Park, J.; Hong, H.H.; Kim, E.; Shin, G. Redesign process of a semi-powered patient transfer device. In Proceedings of the Human Factors and Ergonomics Society Annual Meeting, Los Angeles, CA, USA, 9–13 October 2017; pp. 1071–1075. [Google Scholar]
- Bruno, S.; José, M.; Filomena, S.; Vítor, C.; Demétrio, M.; Karolina, B. The conceptual design of a mechatronic system to handle bedridden elderly individuals. Sensors 2016, 16, 725–748. [Google Scholar] [CrossRef] [PubMed]
- Collins, D. How to Calculate Motor Drive Torque for Belt and Pulley Systems. Available online: https://www.linearmotiontips.com/how-to-calculate-motor-drive-torque-for-belt-and-pulley-systems/ (accessed on 31 July 2022).
- Knapke, P. Motorized Roller Conveyors: A Better Option for Small and Medium-Sized Businesses. Available online: https://www.pulseroller.com/resources/pulsenews/motorized_roller_conveyors_a_better_option_for_small_and_medium_sized_businesses (accessed on 31 July 2022).
- Lin, C.Y.; Bahrudin; Masroor, S. Efficient body-transfer wheelchair for assisting functionally impaired people. CMC-Comput. Mater. Contin. 2023, 74, 4881–4900. [Google Scholar]
- Meenakshi, R.; Ponnusamy, R.; Alghamdi, S.; Khalaf, O.I.; Alotaibi, Y. Development of mobile app to support the mobility of visually impaired people. CMC-Comput. Mater. Contin. 2022, 73, 3473–3495. [Google Scholar] [CrossRef]
- Weiner, C.; Alperovitch Najenson, D.; Ribak, J.; Kalichman, L. Prevention of nurses’ work-related musculoskeletal disorders resulting from repositioning patients in bed: Comprehensive narrative review. Workplace Health Saf. 2015, 63, 226–233. [Google Scholar] [CrossRef] [PubMed]
- Healey, F.; Oliver, D.; Milne, A.; Connelly, J.B. The effect of bedrails on falls and injury: A systematic review of clinical studies. Age Ageing 2008, 37, 368–378. [Google Scholar] [CrossRef]
- Davis, J.C.; Bryan, S.; Best, J.R.; Li, L.C.; Hsu, C.L.; Gomez, C.; Vertes, K.A.; Liu-Ambrose, T. Mobility predicts change in older adults’ health-related quality of life: Evidence from a vancouver falls prevention prospective cohort study. Health Qual. Life Outcomes 2015, 13, 101–124. [Google Scholar] [CrossRef] [PubMed]
- Alamgir, H.; Li, O.W.; Gorman, E.; Fast, C.; Yu, S.; Kidd, C. Evaluation of ceiling lifts in health care settings: Patient outcome and perceptions. Am. Assoc. Occup. Health Nurses J. 2009, 57, 374–380. [Google Scholar] [CrossRef]
- Darragh, A.R.; Sommerich, C.M.; Lavender, S.A.; Tanner, K.J.; Vogel, K.; Campo, M. Musculoskeletal discomfort, physical demand, and caregiving activities in informal caregivers. J. Appl. Gerontol. 2015, 34, 734–760. [Google Scholar] [CrossRef]
- Pompeii, L.A.; Lipscomb, H.J.; Schoenfisch, A.L.; Dement, J.M. Musculoskeletal injuries resulting from patient handling tasks among hospital workers. Am. J. Ind. Med. 2009, 52, 571–588. [Google Scholar] [CrossRef] [PubMed]
- Karmarkar, A.M.; Dicianno, B.E.; Cooper, R.; Collins, D.M.; Matthews, J.T.; Koontz, A.; Teodorski, E.E.; Cooper, R.A. Demographic Profile of Older Adults Using Wheeled Mobility Devices. J. Aging Res. 2011, 2011, 560358. [Google Scholar] [CrossRef] [PubMed]
- Fong, J.H. Disability incidence and functional decline among older adults with major chronic diseases. BMC Geriatr. 2019, 19, 323–345. [Google Scholar] [CrossRef]
- na Songkhla, T.; Decharat, S.; Inraksa, S. Health risks and safety assessments of the bathrooms for the elderly in Phatthalung province, southern Thailand. In Proceedings of the Conference on Interdisciplinary Approach in Sports in Conjunction with the 4th Yogyakarta International Seminar on Health, Physical Education, and Sport Science (COIS-YISHPESS 2021), Yogyajarta, Indonesia, 13 November 2021; pp. 31–36. [Google Scholar]
- Rajagopal, S.; Thanarajan, T.; Alotaibi, Y.; Alghamdi, S. Brain tumor: Hybrid feature extraction based on UNet and 3DCNN. Comput. Syst. Sci. Eng. 2023, 45, 2093–2109. [Google Scholar] [CrossRef]



















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Name | Year | Transfer Posture | Transfer Mode | Payload (kg) | Assistance in Performing Self-Care Activities | ||
|---|---|---|---|---|---|---|---|
| Transferring from Bed to Wheelchair and Vice Versa | Toileting | Bathing | |||||
| Robotic smart house to assist people with movement disabilities [23] | 2007 | Lifting | Sitting | 90 | √ | √ | x |
| HLPR chair [20,21] | 2010 | Lifting | Sitting | 93 | √ | √ | x |
| RIBA [19] | 2010 | Lifting | Supine | 80 | √ | √ | x |
| Wheelchair with a lifting function [16] | 2012 | Lifting | Sitting | 150 | √ | √ | x |
| Robotic-assistedtransfer device [17] | 2015 | Lifting | Sitting | 117 | √ | √ | x |
| Robotic chair/bed system [26] | 2017 | Lifting | Sitting | 250 | √ | x | x |
| CarryBot [29] | 2017 | Lifting | Sitting | 57 | √ | √ | x |
| Patient Transfer System (PTS) [27,28] | 2021 | Sliding | Supine | 159 | √ | x | x |
| Novel PersonTransfer Assist System [18] | 2021 | Sliding | Supine | 120 | √ | x | x |
| This system | Sliding | Supine | 120 | √ | √ | √ | |
| Rated Power (Watts) | Gear Box Series (Stage) | Rated Speed (RPM) | Allowable Torque (Nm) | Driving Force (N) |
|---|---|---|---|---|
| 40 | 3 | 12.90 | 15 | 1200 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, C.-Y.; Masroor, S.; Bahrudin; Bulut, H. The Design and User Evaluation of Body-Transfer System via Sliding Transfer Approach for Assisting Functionally Impaired People. Machines 2023, 11, 555. https://doi.org/10.3390/machines11050555
Lin C-Y, Masroor S, Bahrudin, Bulut H. The Design and User Evaluation of Body-Transfer System via Sliding Transfer Approach for Assisting Functionally Impaired People. Machines. 2023; 11(5):555. https://doi.org/10.3390/machines11050555
Chicago/Turabian StyleLin, Chyi-Yeu, Salman Masroor, Bahrudin, and Hasan Bulut. 2023. "The Design and User Evaluation of Body-Transfer System via Sliding Transfer Approach for Assisting Functionally Impaired People" Machines 11, no. 5: 555. https://doi.org/10.3390/machines11050555
APA StyleLin, C.-Y., Masroor, S., Bahrudin, & Bulut, H. (2023). The Design and User Evaluation of Body-Transfer System via Sliding Transfer Approach for Assisting Functionally Impaired People. Machines, 11(5), 555. https://doi.org/10.3390/machines11050555