

A Guiding and Positioning Motion Strategy Based on a New Conical Virtual Fixture for Robot-Assisted Oral Surgery

 ,
,
Abstract
1. Introduction
1.1. Background and Task
1.2. Related Work
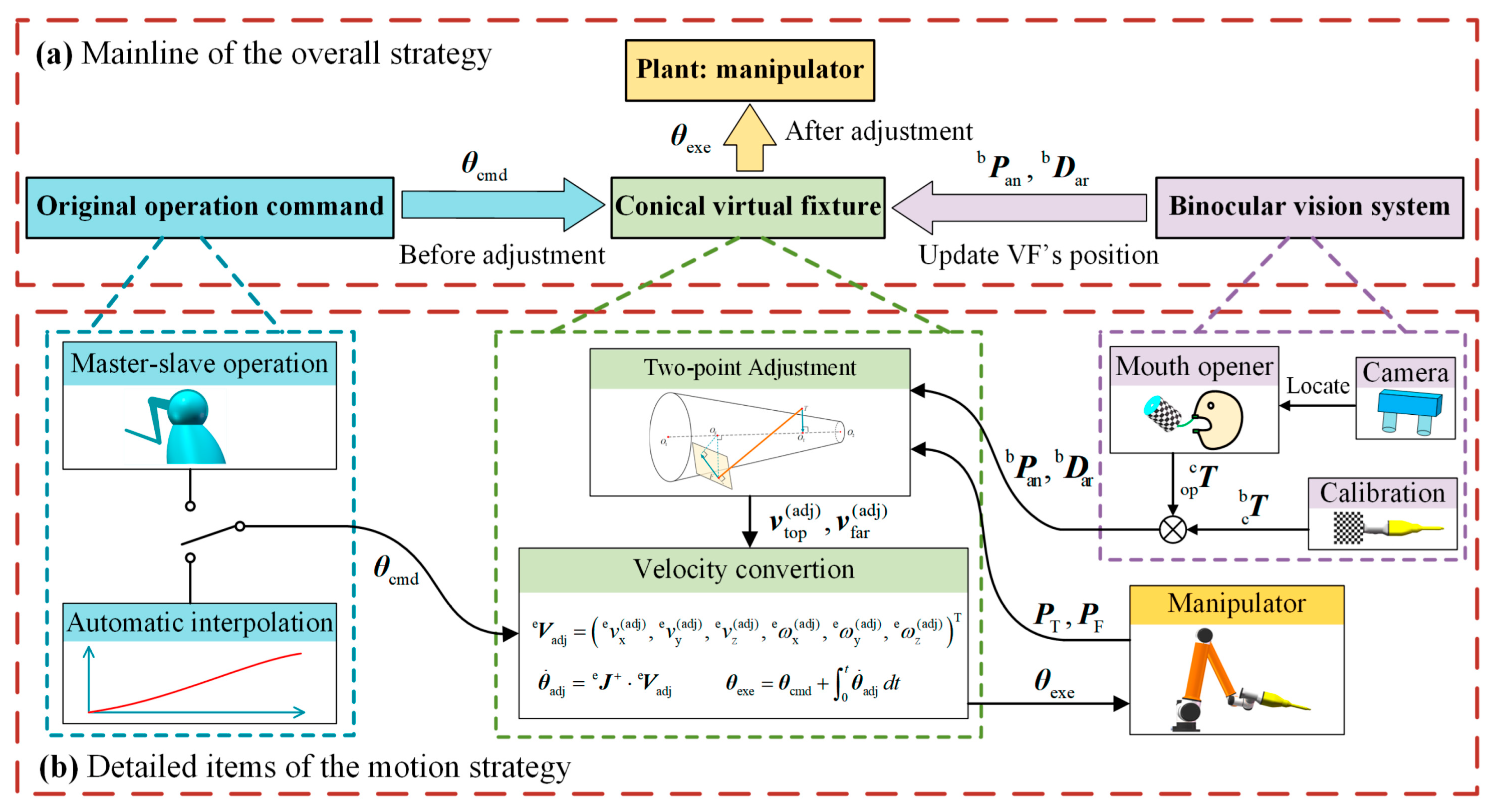
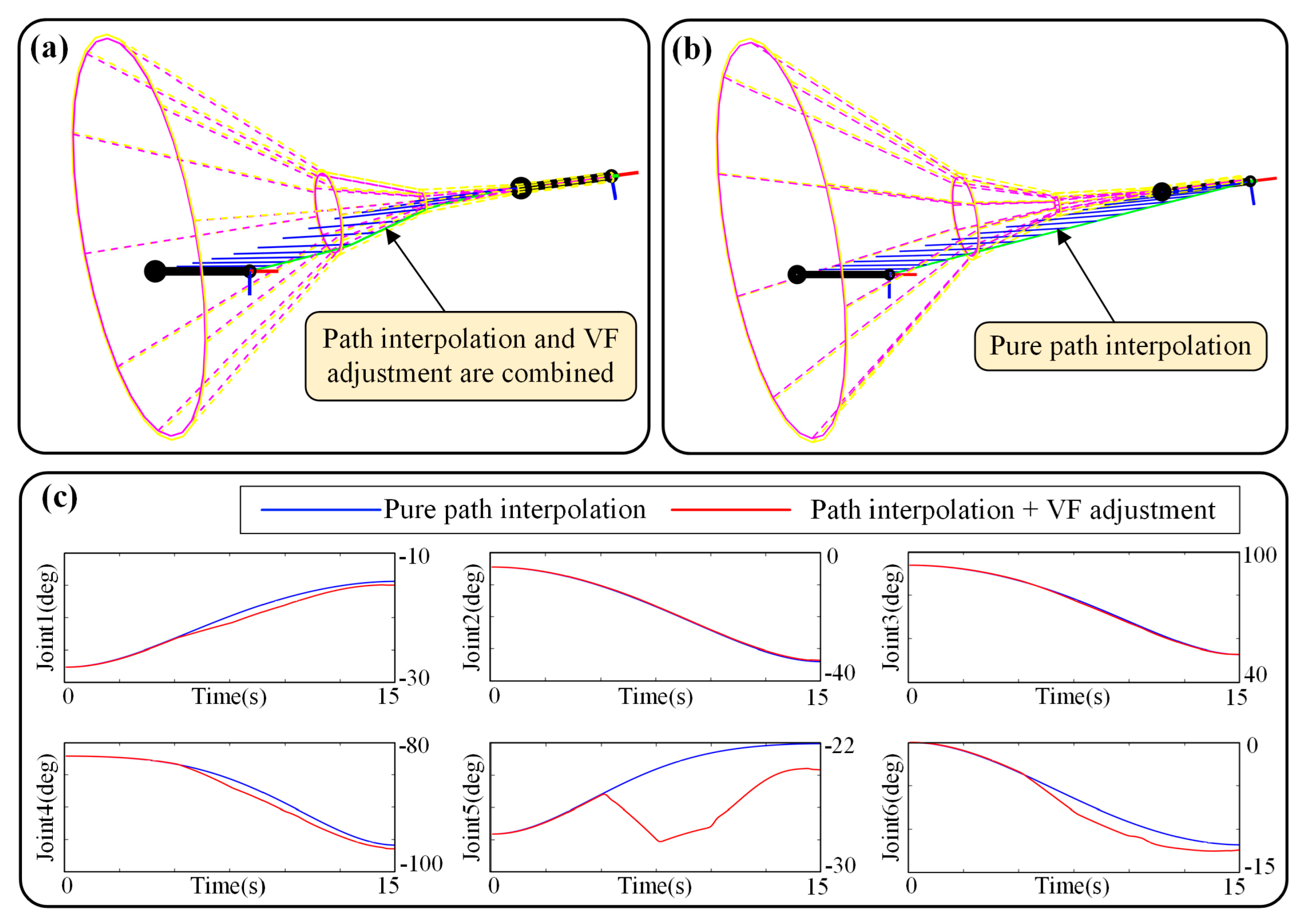
- A new conical virtual fixture is proposed for surgical operation with the master–slave mapping built. In the virtual fixture, a flared guiding cone is designed in accordance with the geometric configuration of oral surgery.
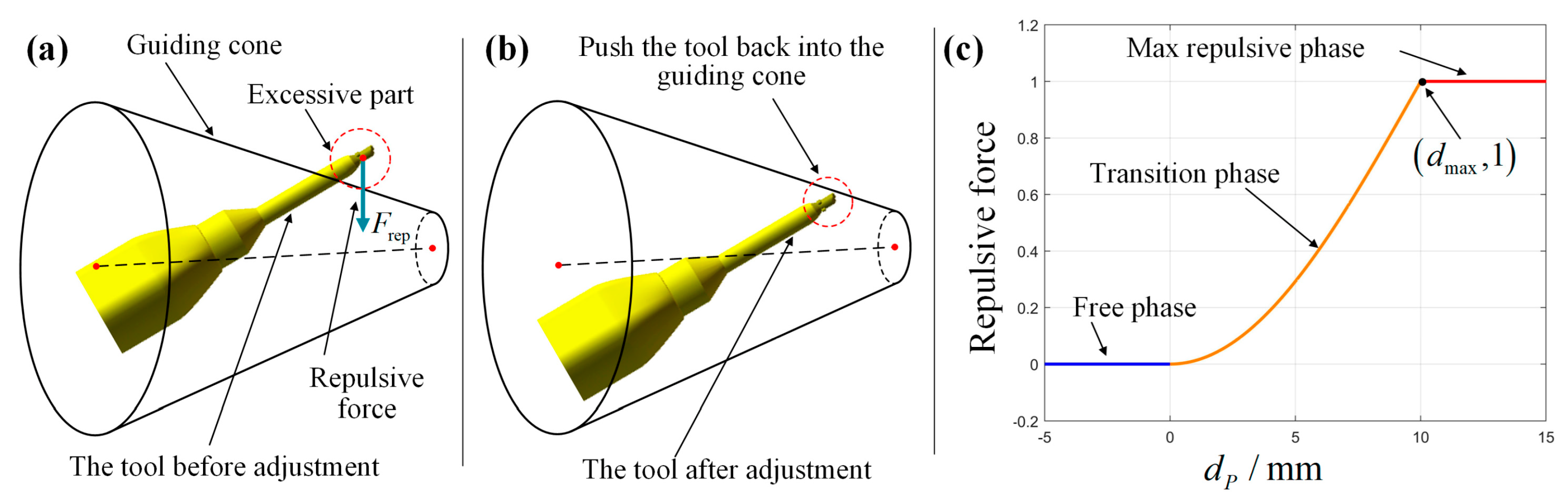
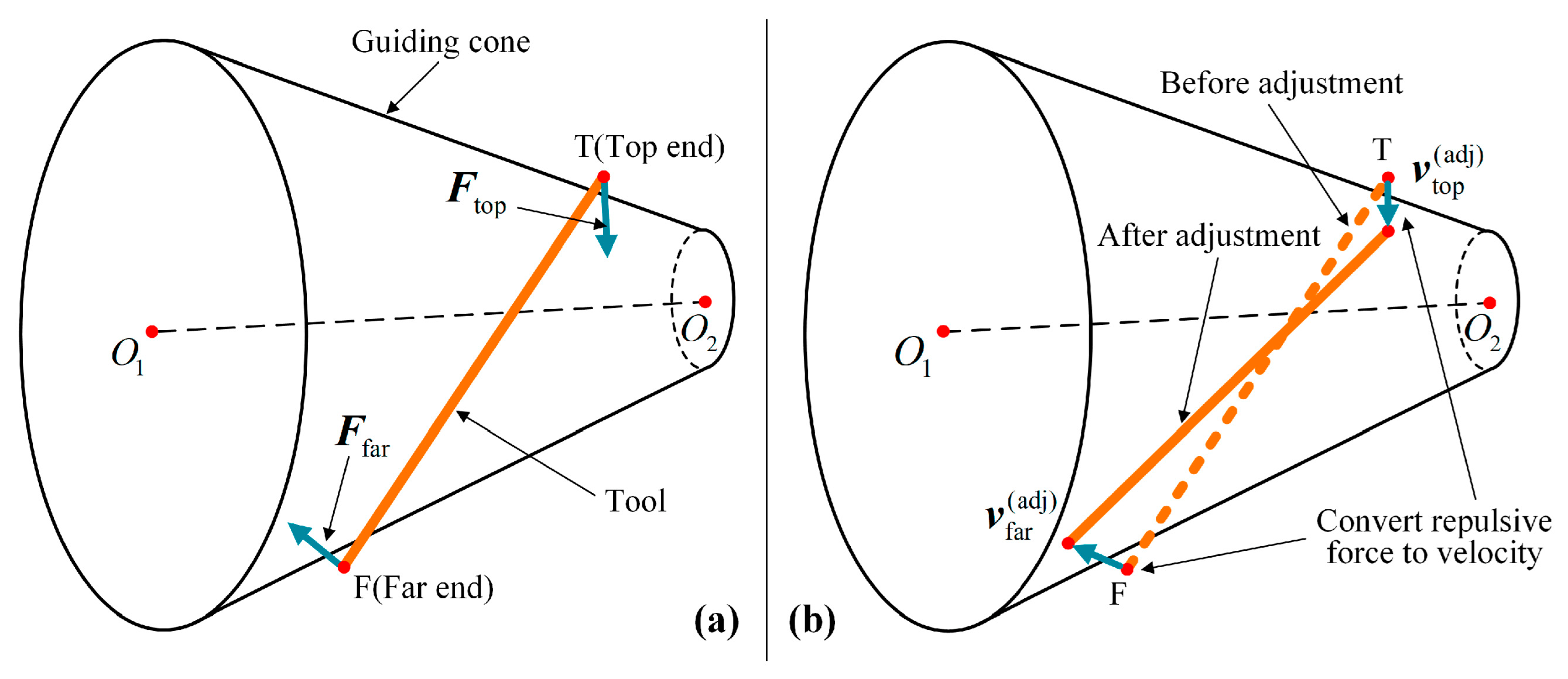
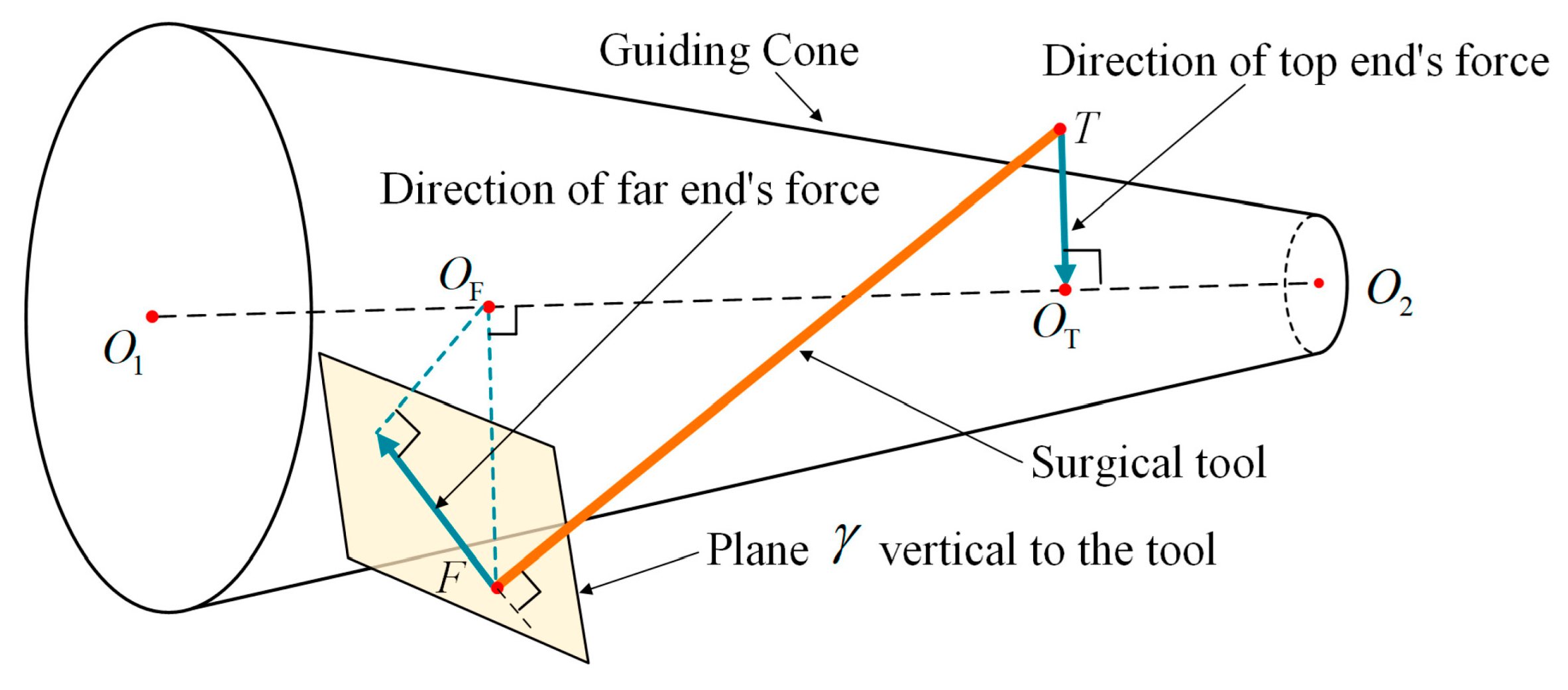
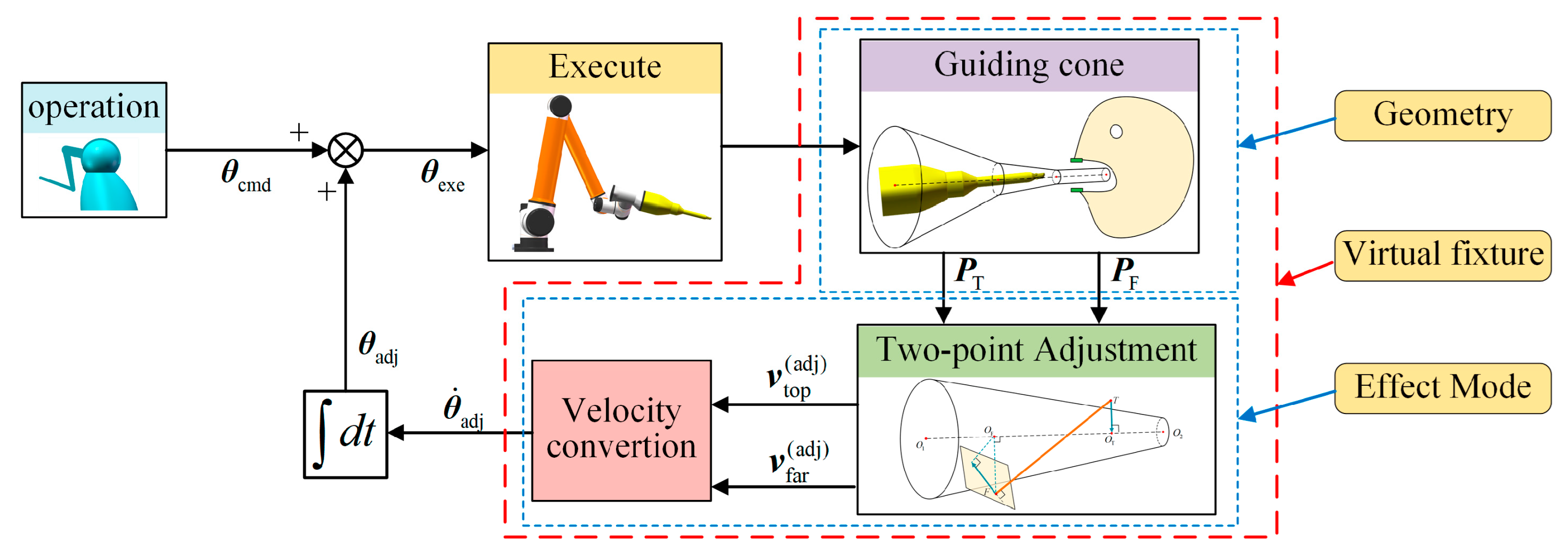
- Two-point adjustment model and velocity conversion are proposed to be the effect of the VF, which can simultaneously adjust the position and orientation of the tool.
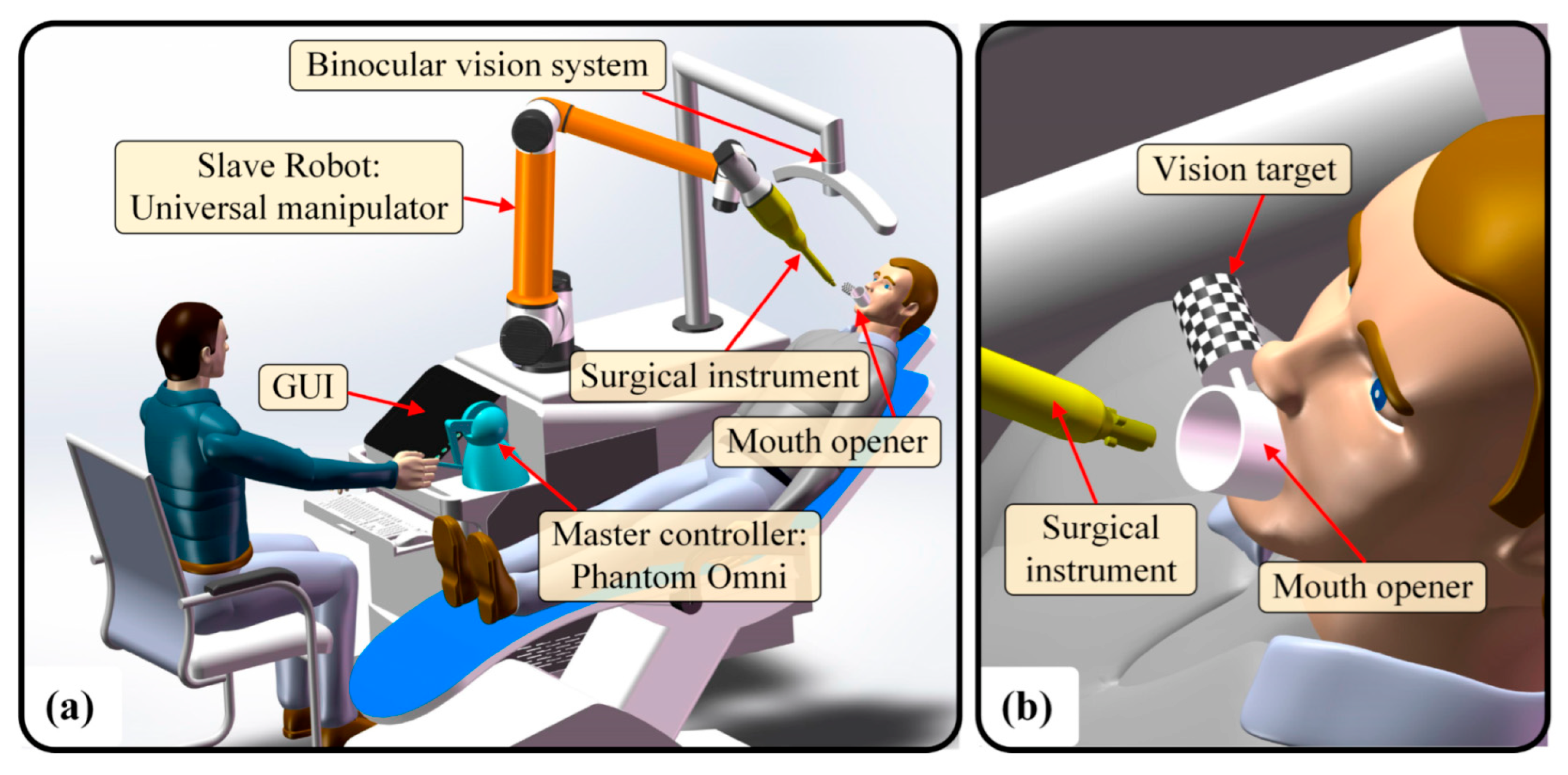
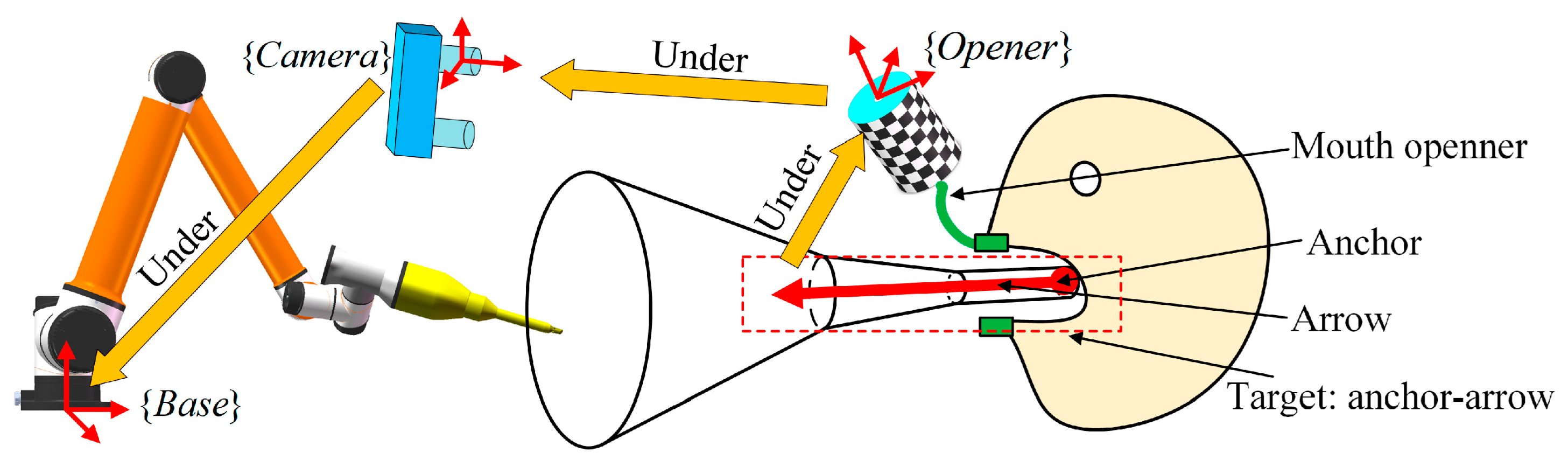
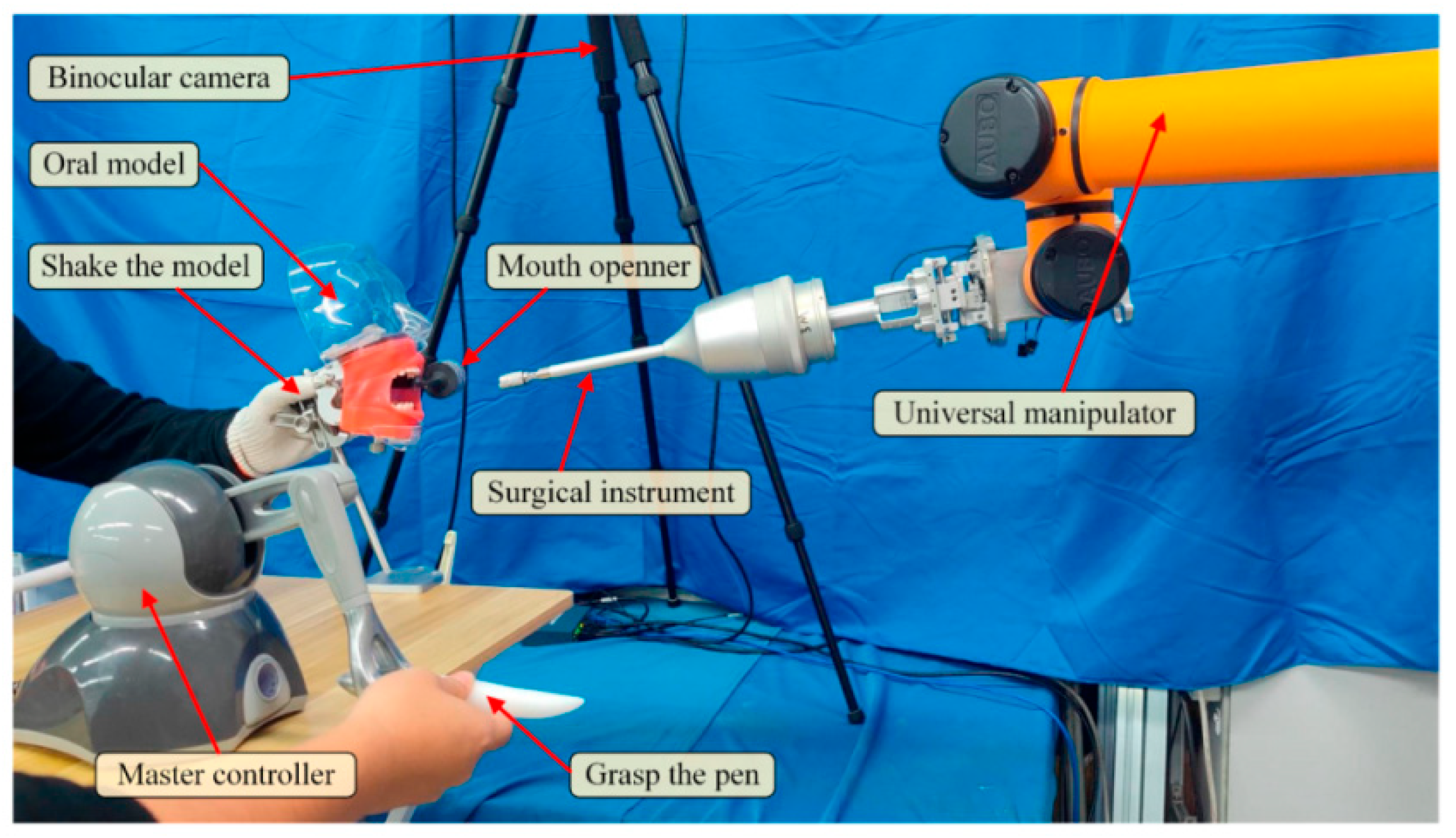
- A new mouth opener is used as a marker for the vision system to locate the oral cavity. The guiding cone is corrected in real-time to compensate for the random disturbance of the patient’s head and realize the feeding to the dynamic target.
- The new VF and vision system are integrated into a full guiding and positioning strategy. This strategy serves as a novel active adjustment framework that not only assists safe and accurate feeding, but also provides an automatic mode to choose.
2. Oral Surgery Robot System (OSRS)
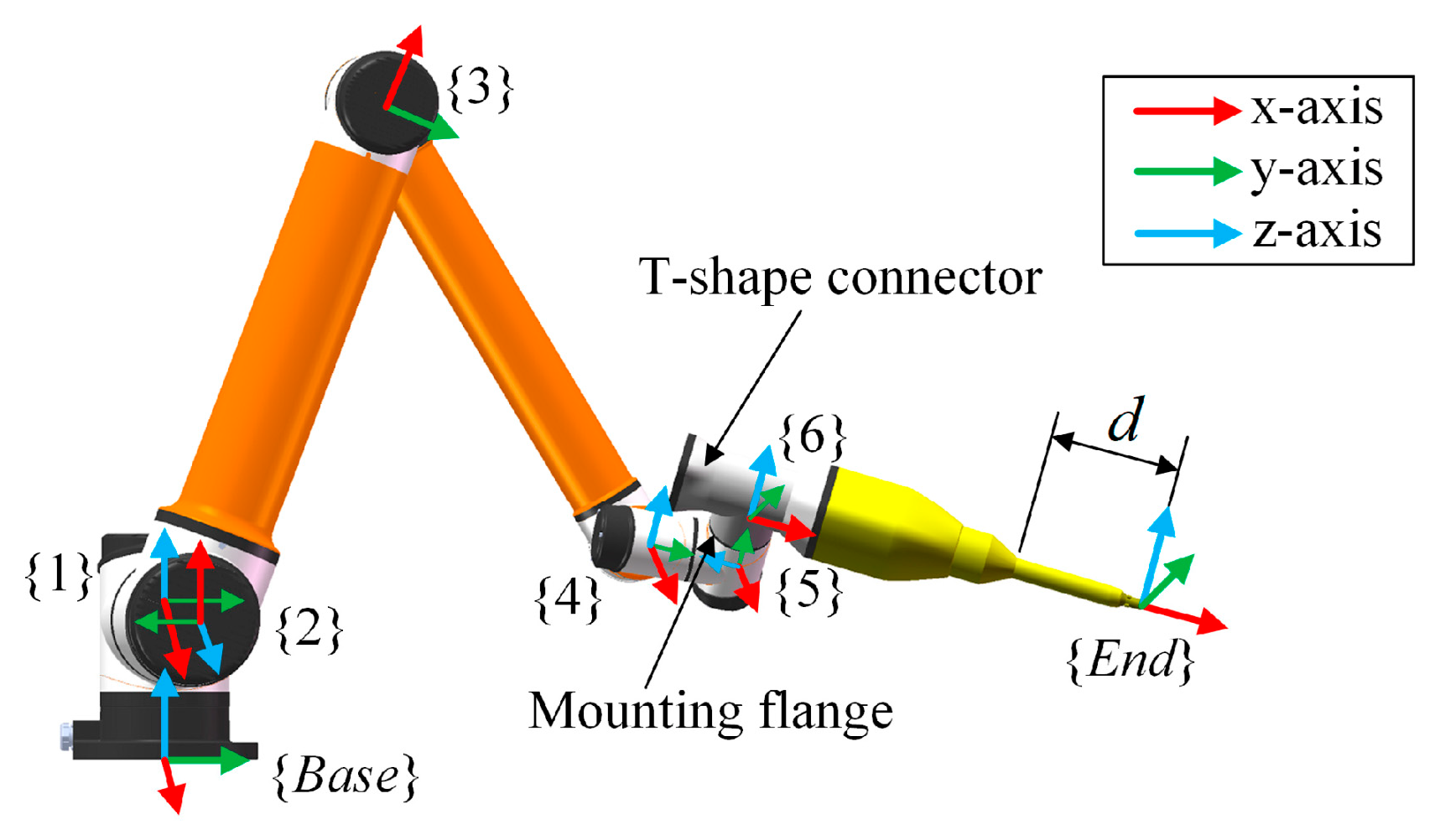
2.1. Hardware Constitution
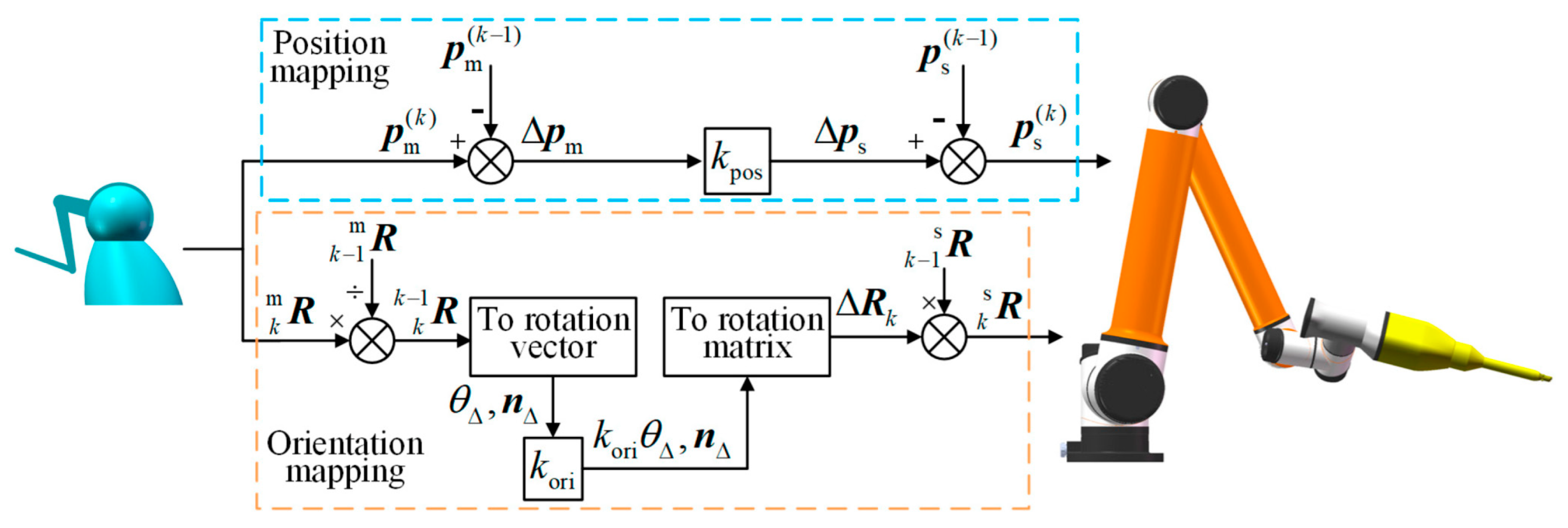
2.2. Master–Slave Mapping
3. Concept of Conical Virtual Fixture
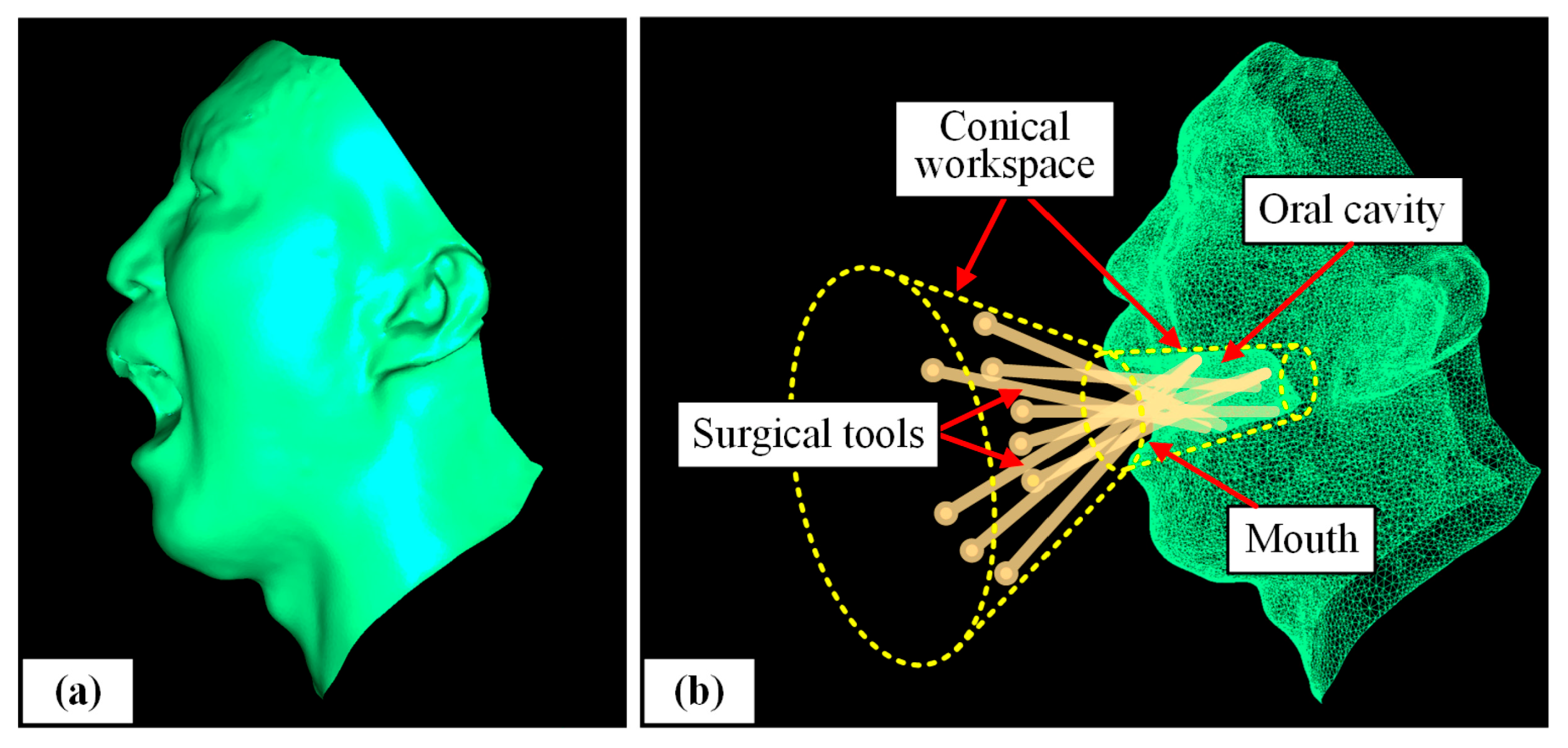
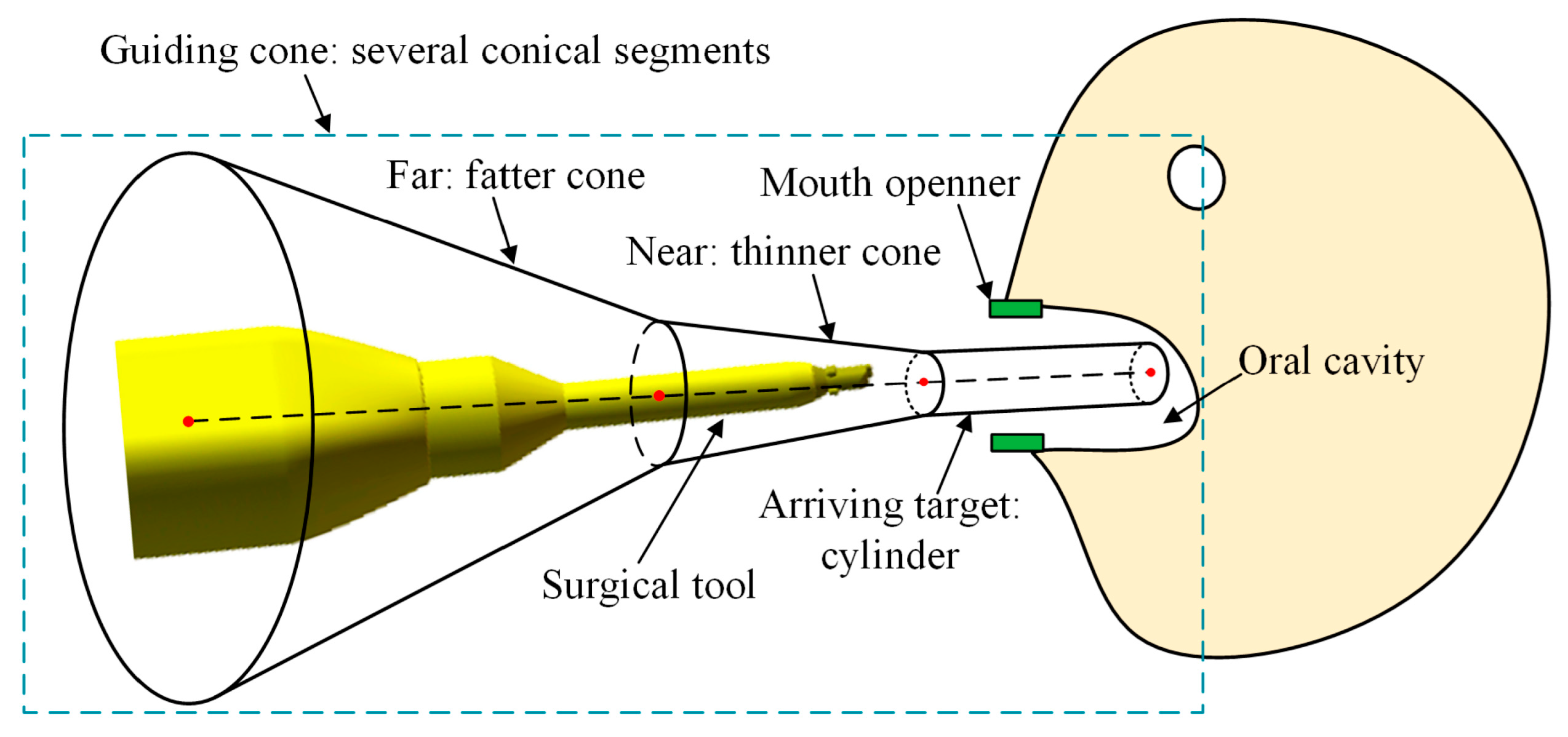
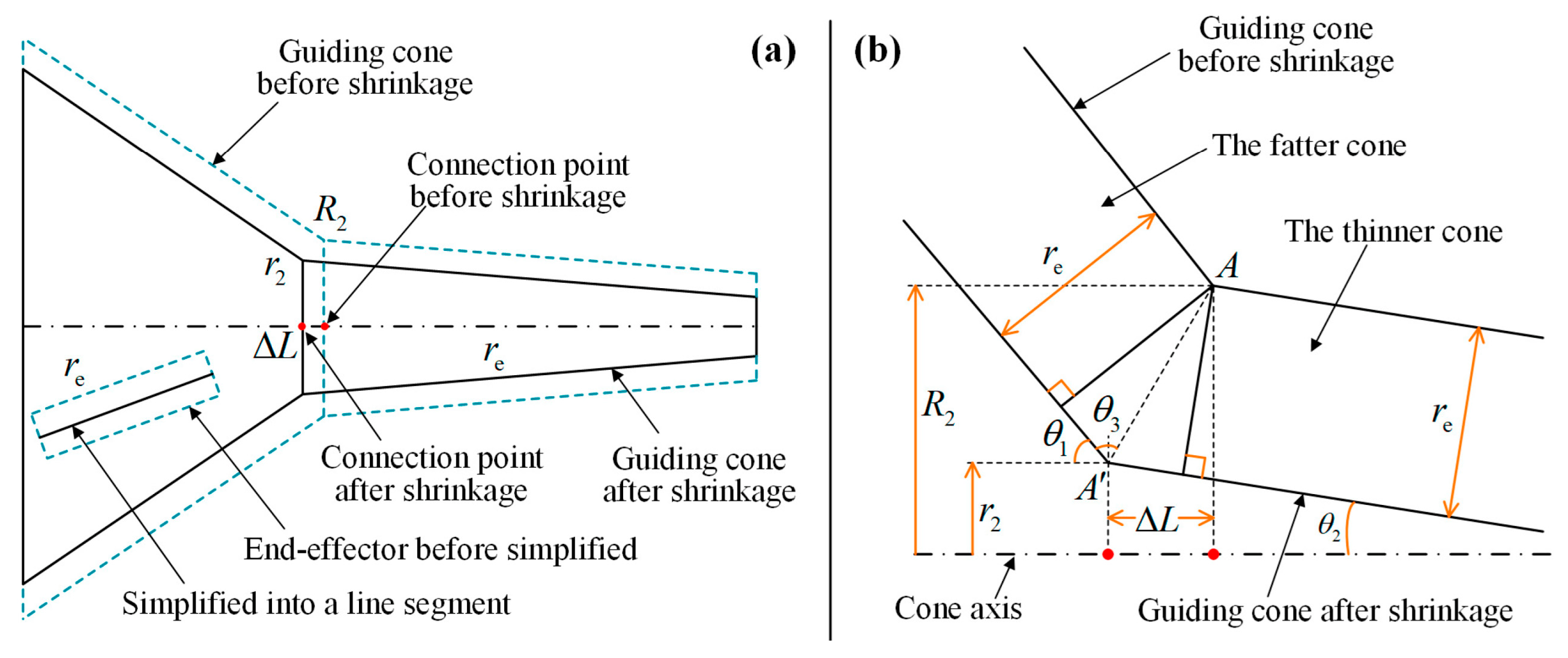
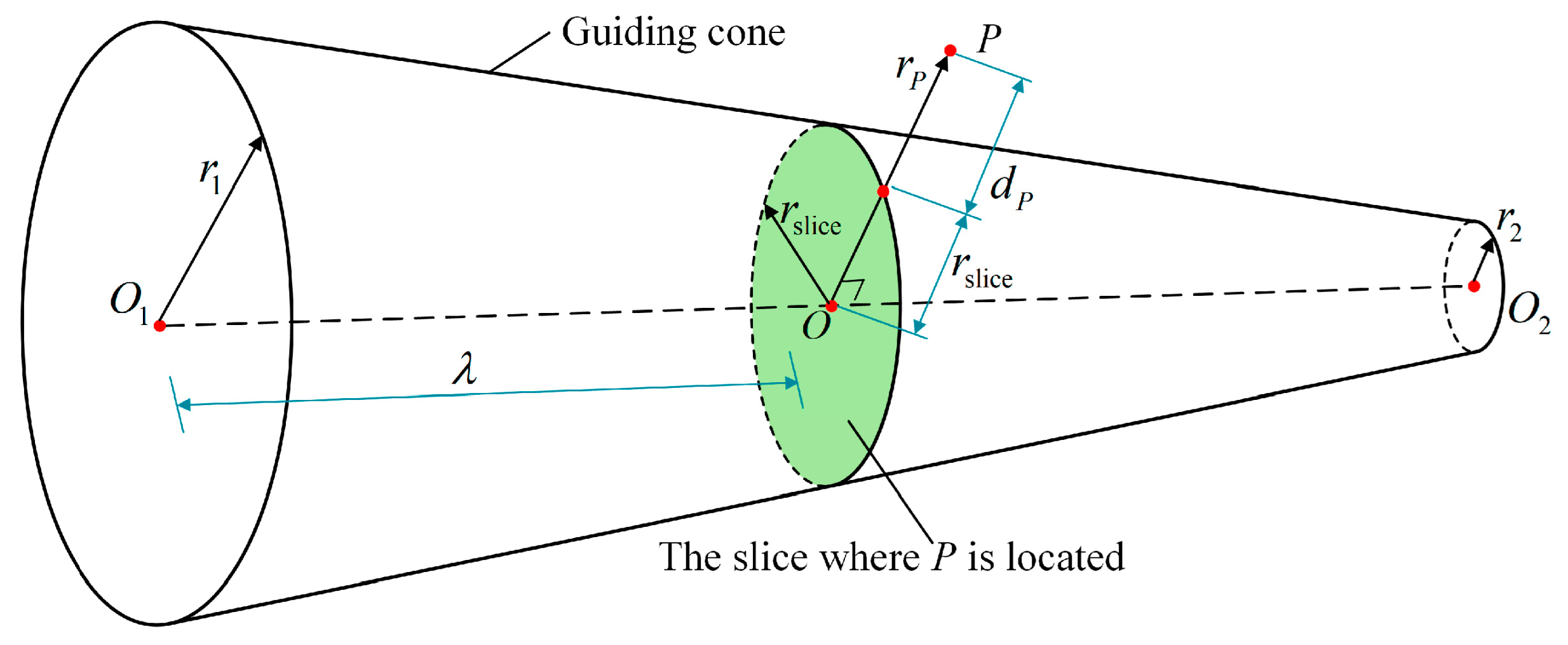
3.1. Geometry of Guiding Cone
3.2. Distance and Repulsive Force
4. Effect of Guiding Cone
4.1. Two-Point Adjustment Model
4.2. Velocity Conversion
5. System Integration of Guiding Cone
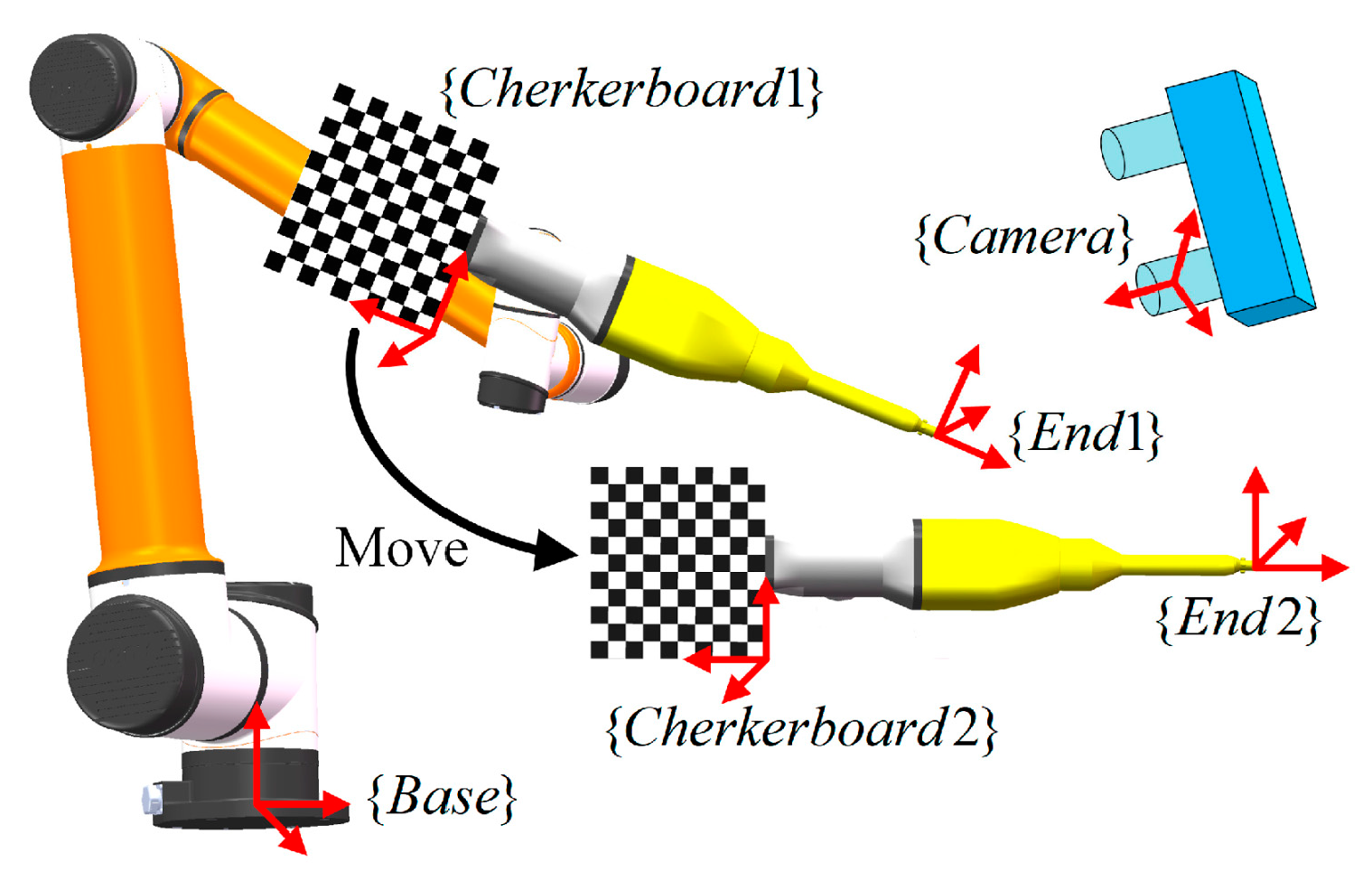
5.1. Calibration and Correction
5.2. Automatic Feeding Mode
6. Simulations, Experiments, and Discussion
6.1. Simulations
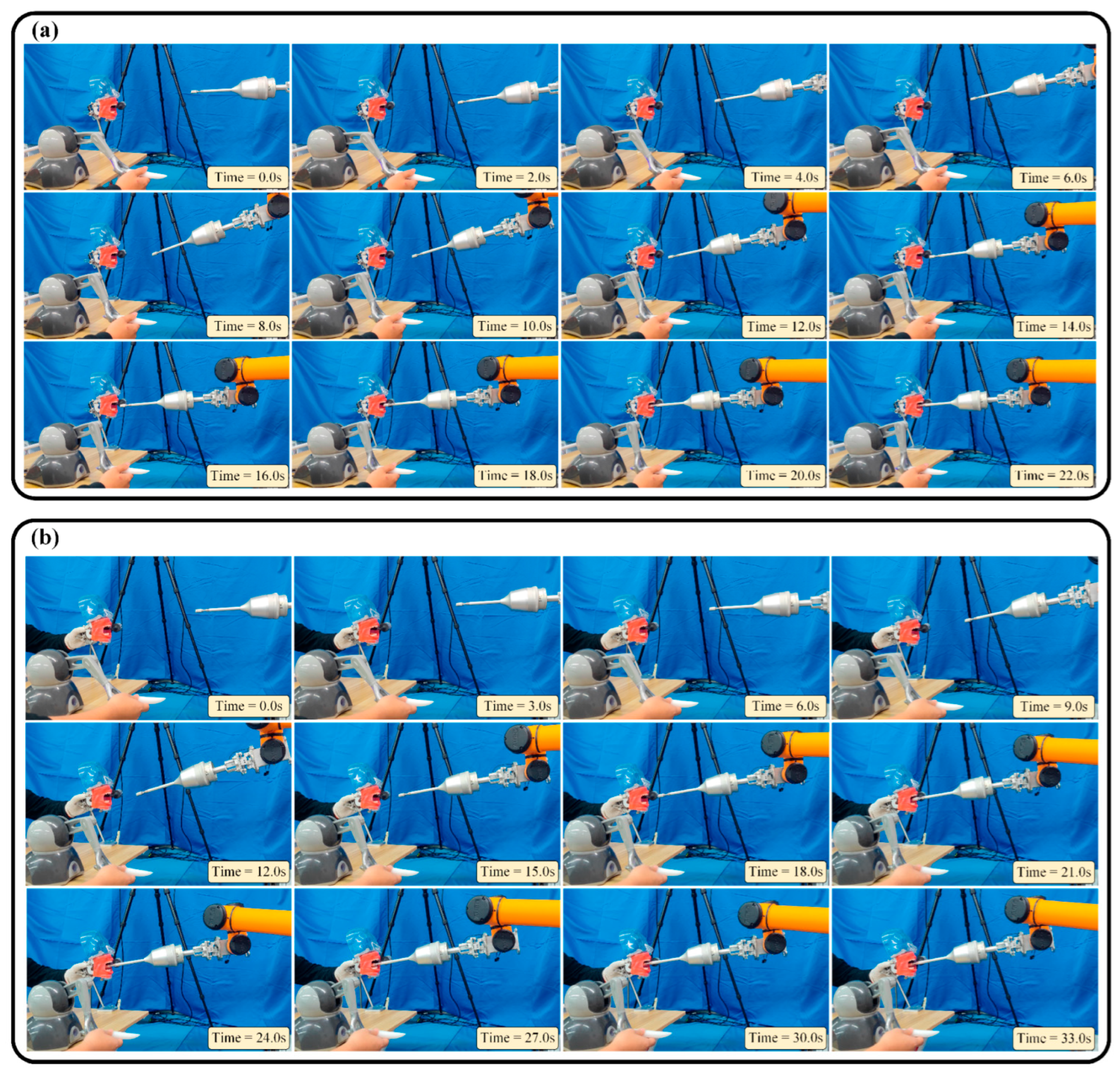
6.2. Experiments
6.3. Discussion
7. Conclusions and Future Work
- A new conical virtual fixture, also called the guiding cone, is designed according to the structure of the oral cavity, making it suitable for robot-assisted oral surgery.
- The effect mode of the virtual fixture is established through two-point adjustment and velocity conversion, which can actively adjust the position and orientation of the surgical tool simultaneously.
- The virtual fixture is integrated with a vision system to compensate for the disturbance of the oral cavity. The system calibration is done, the master–slave mapping is combined, and an automatic mode is adopted, forming a complete motion strategy.
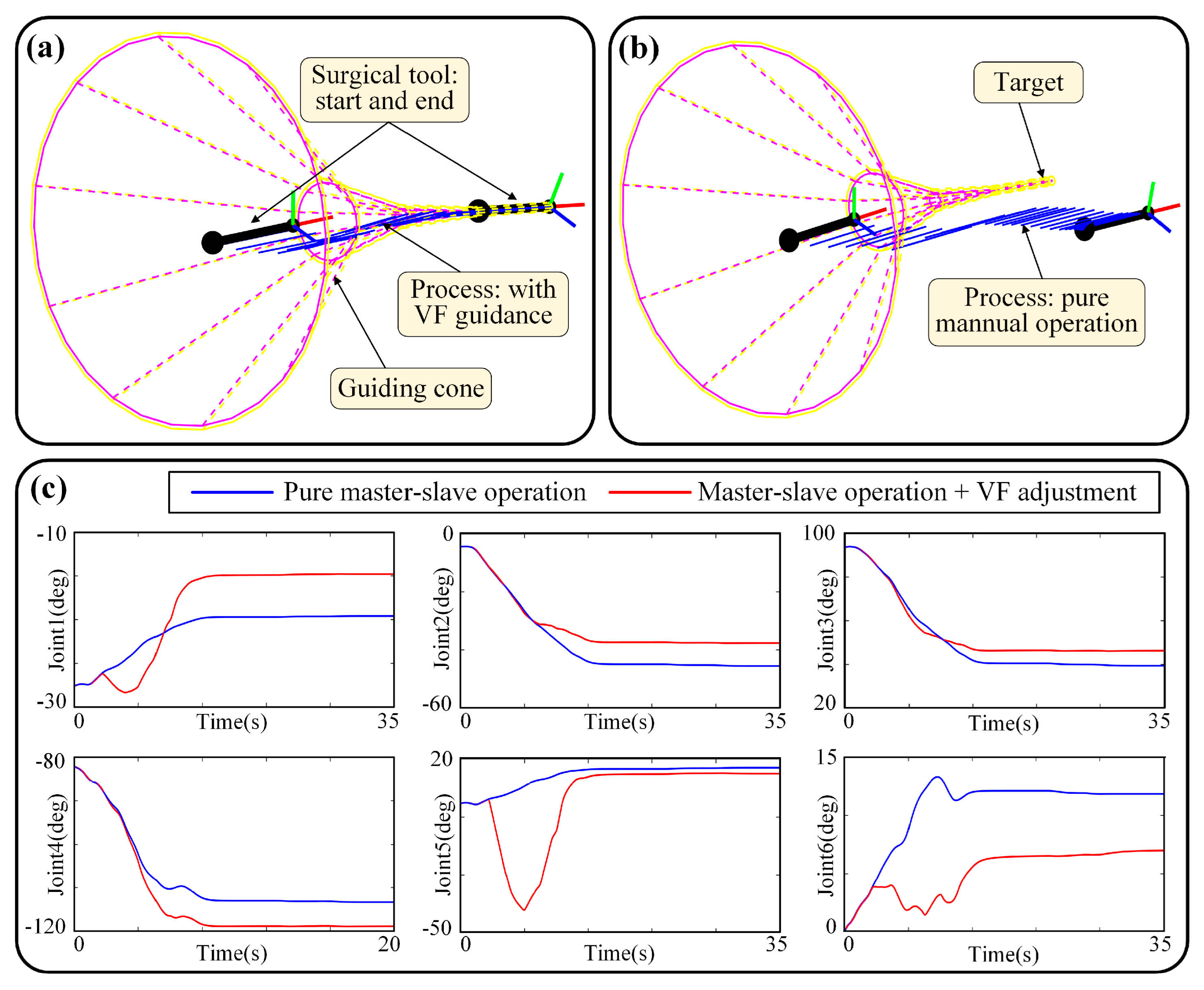
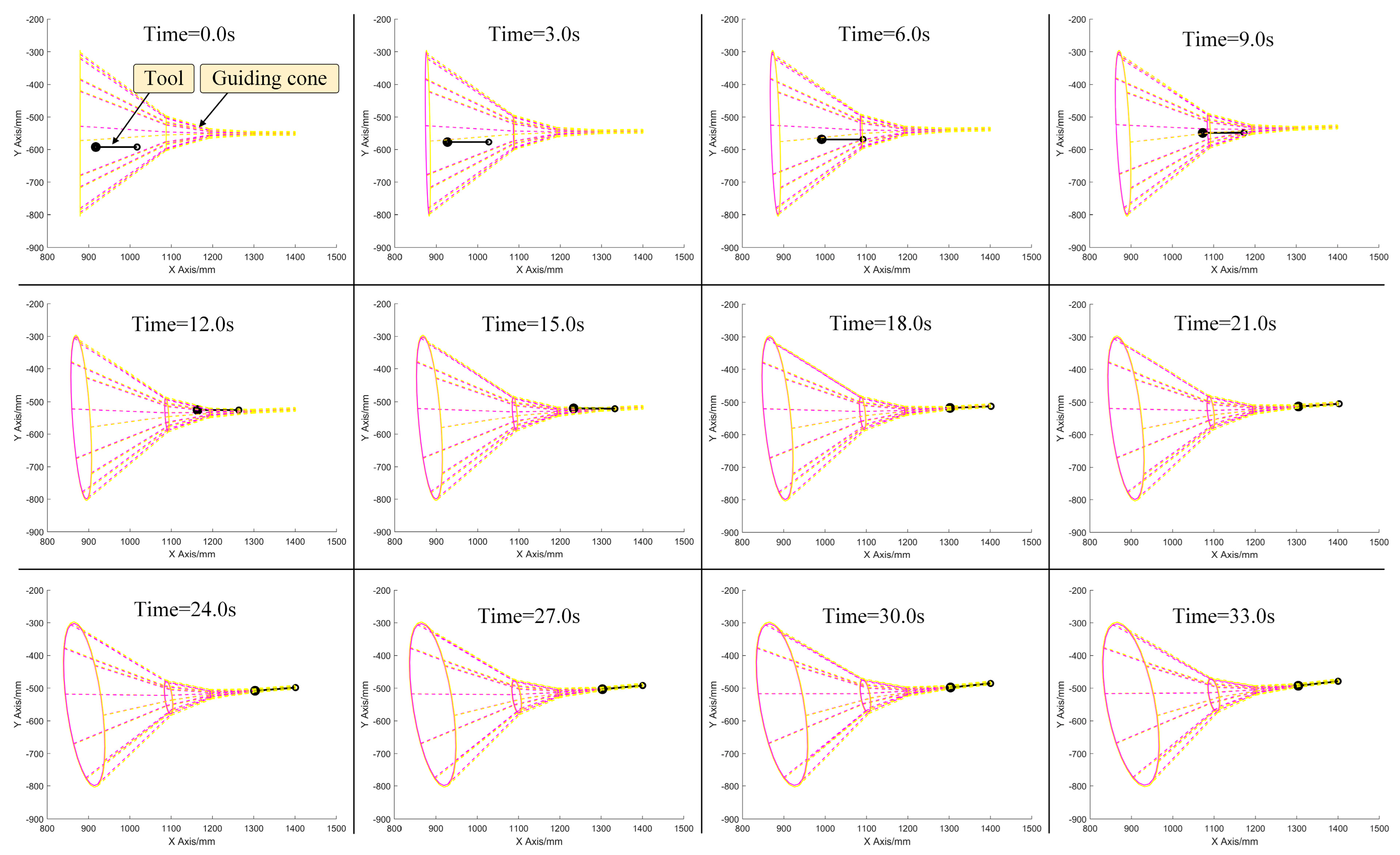
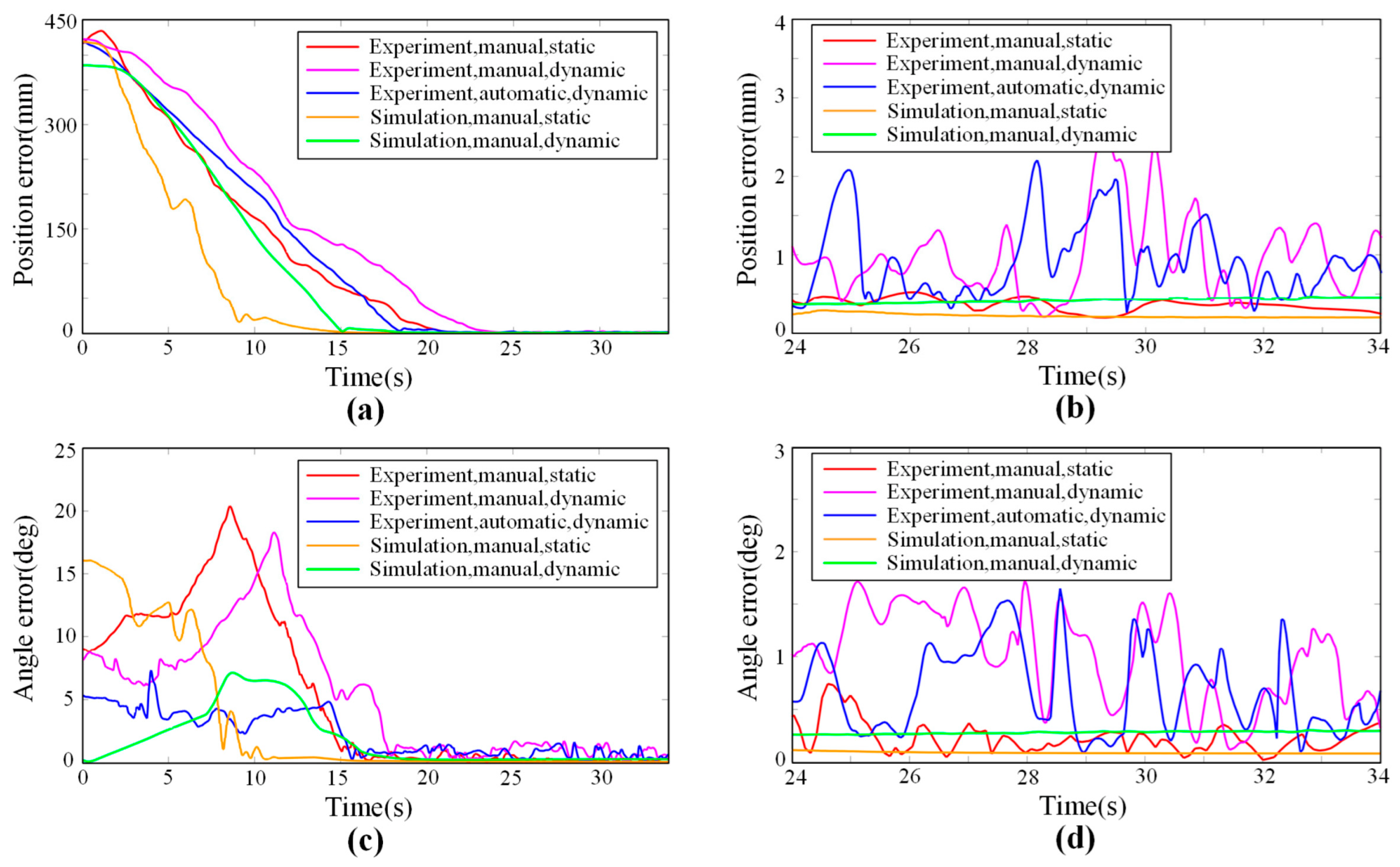
- Simulations and experiments are carried out in the work, the targets are reached, and the errors are quantitatively estimated. In simulations, the estimated positioning errors are 0.202 mm and 0.082 deg for a static target, and 0.439 mm and 0.289 deg for a dynamic target, representing the theoretical ability of VF to adjust the surgical tool. In experiments, the estimated positioning errors are 0.366 mm and 0.227 deg for a static target and 0.977 mm and 1.017 deg for a dynamic target. Despite a few errors, the results suggest the effectiveness of the proposed VF and the motion strategy, which can help the operator keep a relatively high level of accuracy during the manipulating process.
- Safety, accuracy, and dynamic adaptability are three features of the proposed method, making it a palatable auxiliary framework to assist oral surgery operations.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Shanti, R.M.; O’Malley, B.W. Surgical Management of Oral Cancer. Dent. Clin. N. Am. 2018, 62, 77–86. [Google Scholar] [CrossRef] [PubMed]
- Johnston, L.; Warrilow, L.; Fullwood, I.; Tanday, A. Fifteen-minute consultation: Oral ulceration in children. Arch. Dis. Chidhood-Educ. Pract. Ed. 2021, 107, 257–264. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, R.; Botelho, J.; Machado, V.; Mascarenhas, P.; Alcoforado, G.; Mendes, J.; Chambrone, L. Predictors of tooth loss during long-term periodontal maintenance: An updated systematic review. J. Clin. Periodontol. 2021, 48, 1019–1036. [Google Scholar] [CrossRef] [PubMed]
- Kudsi, Z.; Fenlon, M.; Johal, A.; Baysan, A. Assessment of Psychological Disturbance in Patients with Tooth Loss: A Systematic Review of Assessment Tools. J. Prosthodont. Implant Esthet. Reconstr. Dent. 2020, 29, 193–200. [Google Scholar] [CrossRef] [PubMed]
- Hosadurga, R.; Soe, H.; Lim, A.; Adl, A.; Mathew, M. Association between tooth loss and hypertension: A cross-sectional study. J. Fam. Med. Prim. Care 2020, 9, 925–932. [Google Scholar] [CrossRef]
- McMahon, J.; Steele, P.; Kyzas, P.; Pollard, C.; Jampana, R.; MacIver, C.; Subramaniam, S.; Devine, J.; Wales, C.; McCaul, J. Operative tactics in floor of mouth and tongue cancer resection—The importance of imaging and planning. Br. J. Oral Maxillofac. Surg. 2021, 59, 5–15. [Google Scholar] [CrossRef]
- Flanagan, D. Rationale for Mini Dental Implant Treatment. J. Oral Implantol. 2021, 47, 437–444. [Google Scholar] [CrossRef]
- Hupp, J. Robotics and Oral-Maxillofacial Surgery. J. Oral Maxillofac. Surg. 2020, 78, 493–495. [Google Scholar] [CrossRef]
- Yee, S. Transoral Robotic Surgery. Aorn J. 2017, 105, 73–81. [Google Scholar] [CrossRef]
- Ahmad, P.; Alam, M.K.; Aldajani, A.; Alahmari, A.; Alanazi, A.; Stoddart, M.; Sghaireen, M.G. Dental Robotics: A Disruptive Technology. Sensors 2021, 21, 3308. [Google Scholar] [CrossRef]
- Zhang, J.; Wang, W.; Cai, Y.; Li, J.; Zeng, Y.; Chen, L.; Yuan, F.; Ji, Z.; Wang, Y.; Wyrwa, J. A Novel Single-Arm Stapling Robot for Oral and Maxillofacial Surgery-Design and Verification. IEEE Robot. Autom. Lett. 2022, 7, 1348–1355. [Google Scholar] [CrossRef]
- Yuan, F.; Liang., S.; Lyu., P. A Novel Method for Adjusting the Taper and Adaption of Automatic Tooth Preparations with a High-Power Femtosecond Laser. J. Clin. Med. 2021, 10, 3389. [Google Scholar] [CrossRef]
- Gao, Z.; Zhu, M.; Yu, J. A Novel Camera Calibration Pattern Robust to Incomplete Pattern Projection. IEEE Sens. J. 2021, 21, 10051–10060. [Google Scholar] [CrossRef]
- Veras, L.; Medeiros, F.; Guimaraes, L. Rapidly exploring Random Tree* with a sampling method based on Sukharev grids and convex vertices of safety hulls of obstacles. Int. J. Adv. Robot. Syst. 2019, 16, 1729881419825941. [Google Scholar] [CrossRef]
- Machmudah, A.; Parman, S.; Zainuddin, A.; Chacko, S. Polynomial joint angle arm robot motion planning in complex geometrical obstacles. Appl. Soft Comput. 2013, 13, 1099–1109. [Google Scholar] [CrossRef]
- Kim, J.H.; Kim, K.B.; Kim, S.H.; Kim, W.C.; Kim., H.Y.; Kim, J.H. Quantitative evaluation of common errors in digital impression obtained by using an LED blue light in-office CAD/CAM system. Quintessence Int. 2015, 46, 401–407. [Google Scholar] [CrossRef]
- Chen, Z.; Su, W.; Li, B.; Deng, B.; Wu, H.; Liu, B. An intermediate point obstacle avoidance algorithm for serial robot. Adv. Mech. Eng. 2018, 10, 1687814018774627. [Google Scholar] [CrossRef]
- Ma, Q.; Kobayashi, E.; Suenaga, H.; Hara, K.; Wang, J.; Nakagawa, K.; Sakuma, I.; Masamune, K. Autonomous Surgical Robot With Camera-Based Markerless Navigation for Oral and Maxillofacial Surgery. IEEE-ASME Trans. Mechatron. 2020, 25, 1084–1094. [Google Scholar] [CrossRef]
- Hu, Y.; Li, J.; Chen, Y.; Wang, Q.; Chi, C.; Zhang, H.; Gao, Q.; Lan, Y.; Li, Z.; Mu, Z.; et al. Design and Control of a Highly Redundant Rigid-flexible Coupling Robot to Assist the COVID-19 Oropharyngeal-Swab Sampling. IEEE Robot. Autom. Lett. 2022, 7, 1856–1863. [Google Scholar] [CrossRef]
- Cheng, K.; Kan, T.; Liu, Y.; Zhu, W.; Zhu, F.; Wang, W.; Jiang, X.; Dong, X. Accuracy of dental implant surgery with robotic position feedback and registration algorithm: An in-vitro study. Comput. Biol. Med. 2021, 129, 104153. [Google Scholar] [CrossRef]
- Toosi, A.; Arbabtafti, M.; Richardson, B. Virtual Reality Haptic Simulation of Root Canal Therapy. Appl. Mech. Mater. 2014, 66, 388–392. [Google Scholar] [CrossRef]
- Kasahara, Y.; Kawana, H.; Usuda, S.; Ohnishi, K. Telerobotic-assisted bone-drilling system using bilateral control with feed operation scaling and cutting force scaling. Int. J. Med. Robot. Comput. Assist. Surg. 2012, 8, 221–229. [Google Scholar] [CrossRef] [PubMed]
- Iijima, T.; Matsunaga, T.; Shimono, T.; Ohnishi, K.; Usuda, S.; Kawana, H. Development of a Multi DOF Haptic Robot for Dentistry and Oral Surgery. In Proceedings of the 2020 IEEE/SICE International Symposium on System Integration, Honolulu, HI, USA, 12–15 January 2020; pp. 52–57. [Google Scholar]
- Li, J.; Lam, W.; Hsung, R.; Pow, E.; Wu, C.; Wang, Z. Control and Motion Scaling of a Compact Cable-driven Dental Robotic Manipulator. In Proceedings of the 2019 IEEE/ASME International Conference on Advanced Intelligent Mechatronics, Hong Kong, China, 8–12 July 2019; pp. 1002–1007. [Google Scholar]
- Kwon, Y.; Tae, K.; Yi, B. Suspension laryngoscopy using a curved-frame trans-oral robotic system. Int. J. Comput. Assist. Radiol. Surg. 2014, 9, 535–540. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, L. Virtual fixtures: Perceptual tools for telerobotic manipulation. In Proceedings of the IEEE Virtual Reality Annual International Symposium, Seattle, WA, USA, 18–22 September 1993; pp. 76–82. [Google Scholar]
- Abbott, J.; Marayong, P.; Okamura, A. Haptic virtual fixtures for robot-assisted manipulation. In Proceedings of the 12th International Symposium on Robotics Research, San Francisco, CA, USA, 12–15 October 2005; pp. 49–64. [Google Scholar]
- Abbott, J.; Okamura, A. Stable forbidden-region virtual fixtures for bilateral telemanipulation. J. Dyn. Syst. Meas. Control-Trans. ASME 2006, 128, 53–64. [Google Scholar] [CrossRef]
- Bettini, A.; Marayong, P.; Lang, S.; Okamura, A.; Hager, G. Vision-assisted control for manipulation using virtual fixtures. IEEE Trans. Robot. Autom. 2004, 20, 953–966. [Google Scholar] [CrossRef]
- Abbott, J.; Okamura, A. Pseudo-admittance bilateral telemanipulation with guidance virtual fixtures. Int. J. Robot. Res. 2007, 26, 865–884. [Google Scholar] [CrossRef]
- Kikuuwe, R.; Takesue, N.; Fujimoto, H. A control framework to generate nonenergy-storing virtual fixtures: Use of simulated plasticity. IEEE Trans. Robot. 2008, 24, 781–793. [Google Scholar] [CrossRef]
- Lin, A.; Tang, Y.; Gan, M.; Huang, L.; Kuang, S.; Sun, L. A Virtual Fixtures Control Method of Surgical Robot Based on Human Arm Kinematics Model. IEEE Access 2019, 7, 135656–135664. [Google Scholar] [CrossRef]
- Bazzi, D.; Roveda, F.; Zanchettin, A.; Rocco, P. A Unified Approach for Virtual Fixtures and Goal-Driven Variable Admittance Control in Manual Guidance Applications. IEEE Robot. Autom. Lett. 2021, 6, 6378–6385. [Google Scholar] [CrossRef]
- Tang, A.; Cao, Q.; Pan, T. Spatial motion constraints for a minimally invasive surgical robot using customizable virtual fixtures. Int. J. Med. Robot. Comput. Assist. Surg. 2014, 10, 447–460. [Google Scholar] [CrossRef]
- Pruks, V.; Farkhatdinov, I.; Ryu, J. Preliminary Study on Real-Time Interactive Virtual Fixture Generation Method for Shared Teleoperation in Unstructured Environments. In Proceedings of the 11th International Conference on Haptics—Science, Technology, and Applications, Pisa, Italy, 13–16 June 2018; pp. 648–659. [Google Scholar]
- Marinho, M.; Adorno, B.; Harada, K.; Mitsuishi, M. Dynamic Active Constraints for Surgical Robots Using Vector-Field Inequalities. IEEE Trans. Robot. 2019, 35, 1166–1185. [Google Scholar] [CrossRef]
- Xu, C.; Lin, L.; Aung, Z.; Chai, G.; Xie, L. Research on spatial motion safety constraints and cooperative control of robot-assisted craniotomy: Beagle model experiment verification. Int. J. Med. Robot. Comput. Assist. Surg. 2021, 17, e2231. [Google Scholar] [CrossRef]
- Li, M.; Ishii, M.; Taylor, R. Spatial Motion Constraints Using Virtual Fixtures Generated by Anatomy. IEEE Trans. Robot. 2007, 17, 4–19. [Google Scholar] [CrossRef]
- Ren, J.; Patel, R.; McIsaac, K.; Guiraudon, G.; Peters, T. Dynamic 3-D virtual fixtures for minimally invasive beating heart procedures. IEEE Trans. Med. Imaging 2008, 27, 1061–1070. [Google Scholar] [CrossRef]
- He, C.; Yang, E.; McIsaac, K.; Patel, N.; Ebrahimi, A.; Shahbazi, M.; Gehlbach, P.; Iordachita, I. Automatic Light Pipe Actuating System for Bimanual Robot-Assisted Retinal Surgery. IEEE Trans. Mechatron. 2020, 25, 2846–2857. [Google Scholar] [CrossRef]
- Valdenebro, A. Visualizing rotations and composition of rotations with the Rodrigues vector. Eur. J. Phys. 2016, 37, 065001. [Google Scholar] [CrossRef]
- Shi, H.; Liu, Q.; Mei, X. Visualizing rotations and composition of rotations with the Rodrigues vector. Machines 2021, 9, 213. [Google Scholar] [CrossRef]























{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cone | ||||||
|---|---|---|---|---|---|---|
| 1 | (900, −550, 620) | (1100, −520, 570) | 250 mm | 50 mm | 150 | 5 mm |
| 2 | (1100, −520, 570) | (1200, −505, 545) | 50 mm | 10 mm | 150 | 5 mm |
| 3 | (1200, −505, 545) | (1300, −490, 520) | 10 mm | 1 mm | 150 | 5 mm |
| 4 | (1300, −490, 520) | (1400, −475, 495) | 1 mm | 1 mm | 150 | 5 mm |
| Type | Operation | Target | Average Positioning Error |
|---|---|---|---|
| Experiment | Manual | Static | 0.366 mm and 0.227 deg |
| Experiment | Manual | Dynamic | 0.977 mm and 1.017 deg |
| Experiment | Automatic | Dynamic | 0.912 mm and 0.677 deg |
| Simulation | Manual | Static | 0.202 mm and 0.082 deg |
| Simulation | Manual | Dynamic | 0.439 mm and 0.289 deg |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, Y.; Wang, W.; Cai, Y.; Zhao, Q.; Wang, Y.; Hu, Y.; Wang, S. A Guiding and Positioning Motion Strategy Based on a New Conical Virtual Fixture for Robot-Assisted Oral Surgery. Machines 2023, 11, 3. https://doi.org/10.3390/machines11010003
Wang Y, Wang W, Cai Y, Zhao Q, Wang Y, Hu Y, Wang S. A Guiding and Positioning Motion Strategy Based on a New Conical Virtual Fixture for Robot-Assisted Oral Surgery. Machines. 2023; 11(1):3. https://doi.org/10.3390/machines11010003
Chicago/Turabian StyleWang, Yan, Wei Wang, Yueri Cai, Qiming Zhao, Yuyang Wang, Yaoqing Hu, and Shaoan Wang. 2023. "A Guiding and Positioning Motion Strategy Based on a New Conical Virtual Fixture for Robot-Assisted Oral Surgery" Machines 11, no. 1: 3. https://doi.org/10.3390/machines11010003
APA StyleWang, Y., Wang, W., Cai, Y., Zhao, Q., Wang, Y., Hu, Y., & Wang, S. (2023). A Guiding and Positioning Motion Strategy Based on a New Conical Virtual Fixture for Robot-Assisted Oral Surgery. Machines, 11(1), 3. https://doi.org/10.3390/machines11010003