1. Introduction
Health has always been one of the most important human concerns from the past, and there has been a lot of efforts to create stable health in communities. Today, with an increase in life expectancy and a decline in birth rates in most societies, we are seeing a rise in the average age of the population, which has imposed a lot of costs on health systems around the world, and a significant share of a country’s budget is spent on health care [
1].
In the current situation, creating a plan to use the resources optimally seems to be necessary due to resource limitations. For example, human resource shortages and shortage of hospitals are a limiting factor in health services. On the other hand, one can also see an individual life pattern of elderly people in the developed and developing countries that makes it necessary to focus on this group of individuals. Developing a framework for offering health care to individuals at their home effectively could be a good solution to this problem. In this context, home health care (HHC) companies are usually faced with conflicts in their targets such as maximizing the offering service level and minimizing the operating costs, which usually should be simultaneously optimized. With the attendance of various companies in this field, new angles of existing costs have been clarified, which have encouraged researchers to use optimization techniques in this field. One of the most related issues for companies consists in finding an optimal plan for offering services. This problem is called the home health care routing and scheduling problem (HHCRSP), which has attracted a lot of attention recently among researchers [
2].
In the HHCRSP, there are a set of patients in different geographical regions who need a diverse range of health care services at their home. These service requirements should be handled by some specialized companies and their highly skilled nurses. In this context, most researchers assume that each nurse’s route is started from and ended in the depot. The word depot is used to indicate the starting or ending point of the routes, which is usually the HHC company’s office. Active organizations in this field should make a tradeoff between reducing their operational costs and providing high quality services to customers. Therefore, the HHCRSP focuses on planning a set of routes to deliver the scheduled care services within a planning horizon, which minimizes a criterion such as cost or maximizes the service quality by taking into account a number of constraints [
3].
Fernandez, Gregory, Hindle, and Lee [
4] were the first to study routing and scheduling in the HHC context. They investigated a working day of community nurses in their research. Their plan divides the county into a number of nursing districts. Then, they estimated the number of calls that can be made on average to measure the effectiveness of the proposed plan on the community. Hindle, Hindle, and Spollen [
5] and Hindle, Hindle, and Spollen [
6] extended the problem of Fernandez et al. [
4] by considering resource allocations and travel cost estimation aspects. Decision support systems (DSSs) in this context were first considered by Bertels and Fahle [
7] and Eveborn, Flisberg, and Rönnqvist [
8]. This problem was developed as an extension of the vehicle routing problem by Akjiratikarl, Yenradee, and Drake [
9] and solved by using a particle swarm optimization (PSO) algorithm.
In recent years, the HHCRSP has attracted the attention of many researchers, and various studies have been implemented in this field. Recent research in this field can be classified into two categories: deterministic and uncertain studies. In the category of recent deterministic studies, Mankowska, Meisel, and Bierwirth [
10] provided a daily planning with regard to the specific needs of each patient, the particular skills of each nurse, as well as the relationships between different services. They developed a new heuristic to handle such requirements. Their solutions indicated that the method can achieve a fair distribution of inevitable tardiness, low average waiting times for the patients, and low traveling costs for the nurses. Liu et al. [
11] applied the research of Mankowska et al. [
10] to the logistics domain of home health care. They noted that nurses may need to transfer medicines and medical supplies from the company center to the patients’ home and return the laboratory samples, unused drugs, and medical equipment to the center. Liu et al. [
11] extended the problem of the multiperiod vehicle routing problem with time windows (PVRPTWs) to three different patient demand types. They proposed a Tabu Search method combined with different local search schemes including both feasible and infeasible local searches. Their experiments showed that the proposed approach balances better the workloads of vehicles and reduces the total cost.
Decerle, Grunder, El Hassani, and Barakat [
12] addressed the problem of home health care by considering a few objectives simultaneously and focusing on the applicability of the planning. They employed a memetic algorithm to solve this problem. They conducted several experiments and showed that the developed methods had a good performance for small-sized instances. However, Simulated Annealing (SA) was slightly better than Tabu Search (TS) for large-sized problems. Fathollahi-Fard, Hajiaghaei-Keshteli, and Tavakkoli-Moghaddam [
13] presented a biobjective green home health care problem that considers environmental pollution. They developed a new modified multiobjective version of a social engineering optimizer (SEO) by using an adaptive memory strategy, so-called AMSEO. Based on their analyses, AMSEO performs significantly better than SEO, NSGA-II, and SA when all methods were tuned by the response surface methodology (RSM) and compared across four popular evaluation metrics. The conventional HHCRSP is extended to demand and capacity management by Nasir and Dang [
14]. A mixed integer programming (MIP) model is suggested by considering workload balancing. To solve this model, some heuristics, including a variable neighborhood search (VNS) algorithm, were applied. They compared the results obtained by VNS with a CPLEX-based solution. Performing the model on different datasets showed the efficiency and effectiveness of the solution methods to handle the considered problem. Nasir, Hussain, and Dang [
15] developed a mathematical model to consider group-based and telehealth-based care services. Three different goals were considered in their model to achieve this target. The first goal was to select an optimal location for the HHC centers, staff and group patient centers considering the required specifications. The second goal of their study was to schedule the group patient sessions in specific time windows by pairing each nurse with a telephone service staff. Finally, as their third goal, the violation from good quality services and the dissatisfaction of the patients were considered. They employed Fuzzy c-means in order to validate the effectiveness of the proposed integration approach. Then, a sensitivity analysis was conducted to explore the model behavior against the variation in the values. The detailed analysis of the results showed the effectiveness of the proposed model and its behavior with respect to different types of cost.
Fikar and Hirsch [
16] introduced the concept of car and trip sharing within home health care nurses. They also considered the option that the nurses are allowed to walk to the patient’s home. They investigated different geographic distributions to identify beneficial settings for a successful implementation considering various goals of the decision makers. Their evaluation showed that trip sharing performs best if long service durations exist and long delays for parking occur and in areas where clients are both geographically distributed randomly and in clusters. Lin, Hung, Liu, and Tsai [
17] presented a modified harmony search (MHS) algorithm that considers the three problems of nurse rostering, nurse routing, and nurse rerostering simultaneously. They specified that past studies had considered the issues of the nurse rostering problem (NRP) and VRPTWs independently; in this study, it was investigated at the same time. Then, they formulated the model by MIP and solved it by the commercial solver CPLEX. They also adopted a real dataset extracted from an existing HHC institution. The numerical results showed an efficient computing performance for an optimal solution of small, medium, and large sizes.
The home health care problem in Chinese communities was considered by Zhang, Yang, Chen, Bai, and Chen [
18]. These communities have an intense distribution of patients. They formulated the problem by MIP and considered three main factors, including match qualities, uncertain service times, and time windows. Therefore, they applied a modified ant colony optimization and analyzed it in four instances. Liu, Yang, Su, and Xu [
19] developed a biobjective model with the objective to minimize the costs of the company and to improve patient satisfaction. In their study, multiple weeks of planning and medical teams were considered. To solve such a problem, the epsilon-constraint method was used to obtain the Pareto fronts of the problem. They conducted computational experiments, and the results showed the efficiency of the approaches.
Shanejat-Bushehri, Tavakkoli-Moghaddam, Momen, Gasemkhani, and Tavakkoli-Moghaddam [
20] considered the HHCRSP problem with temporarily precedence and synchronization constraints as well as limited allowable times for transferring the collected biological samples to the laboratory. The goal was to minimize the cost related to the transportation and the idle time of the nurses. They presented a mathematical model and applied Simulated Annealing and Tabu Search in two phases. They performed several comparative experiments and showed that the developed methods had a good performance for small-sized instances. However, SA was slightly better than TS for large-sized problems. Grenouilleau, Legrain, Lahrichi, and Rousseau [
21] presented a method for the HHCRSP problem, which is based on a set partitioning formulation as well as a variable neighborhood search framework. Their algorithm solved first a linear relaxation, and then a constructive heuristic was applied to generate an integer solution. They applied the algorithm to real instances and showed that the proposed method is able to provide an increase of more than 16% in the continuity of care and a reduction in travel times by 37%. Euchi, Zidi, and Laouamer [
22] presented a distributed optimization approach for the HHCRSP problem, which used artificial intelligence techniques. They integrated automatic learning and search techniques to optimize the assignment of nurses to patients. Their results proved the efficiency of the proposed approach, which can offer a decision support for medical executives of HHC. Khodabandeh, Kayvanfar, Rafiee, and Werner [
3] included downgrading aspects into the classical HHCRSP problem. They considered the additional goal to minimize also the difference between the actual and the potential skills of the nurses. To solve the derived biobjective model, the authors used the epsilon-constraint method. They also performed a sensitivity analysis on the epsilon parameter. Ghiasi, Yazdani, Vahdani, and Kazemi [
23] considered the HHCRSP problem with two transportation modes, namely public and private modes under the multidepot version. The objective was the minimization of the sum of the travel distance and overtime costs. After presenting a mixed integer programming model, three metaheuristic algorithms including Invasive Weed Optimization (IWO), Grasshopper Optimization Algorithm (GOA), and Simulated Annealing (SA) were given for solving large instances. Their computational results showed that the suggested IWO performed better than the other algorithms. Xiang, Li, and Szeot [
24] considered the HHCRSP problem by minimizing total costs and maximizing patient preference satisfaction. They formulated a biobjective mixed integer linear programming model. For solving this problem, a local search algorithm was embedded into the basic framework of a nondominated sorting genetic algorithm. The algorithm obtained approximate Pareto-optimal solutions for small instances in a shorter computation time than the epsilon-constraint method.
In the category of recent uncertain studies, Yuan, Liu, and Jiang [
25] addressed the HHCRSP with stochastic service times. The problem was modeled in the form of a stochastic programming problem with recourse in which the expected value of late arrivals of the nurses was considered. Then, the branch and price (B&P) method was used to solve this problem. They validated the effectiveness of their proposed algorithm through numerical experiments. In Liu, Yuan, and Jiang [
26], stochastic service and travel times were considered in their problem. They employed a chance constraint in order to guarantee the probability of on-time services. In their study, a route-based mathematical model was developed, and the branch and cut (B&C) algorithm was used with the discrete estimation method to solve it. Moreover, labeling algorithms and acceleration methods were also employed for solving the proposed model. The performance of the proposed B&P algorithm was validated on test instances and demonstrated the necessity of considering the stochasticity of the travel times of the nurses and the service times. Lanzarone and Matta [
27] presented a robust strategy for home health care, in which random patient requests were considered, and the nurse allocation to the patients was investigated as well. The policy of this paper is compared to other previously developed approaches and applied to a relevant real case. Rodriguez, Garaix, Xie, and Augusto [
28] modeled the HHC problem considering a stochastic demand for patients and handled it through stochastic programming. Then, the B&C method was used to solve their proposed model. The analysis of their computational experiments showed that routing evaluation can help to obtain a more precise working time, especially in geographical areas assuming rural or semi-urban patterns. Their solutions and the computed Pareto optimal sets indicate that their approach can help the decision maker before opening a HHC service or before hiring an employee. Shi, Boudouh, and Grunder [
29] addressed the HHC problem with a fuzzy demand for the patients. They employed a fuzzy chance constraint method as well as a hybrid genetic algorithm (GA) for the solution of the model. Their experiments on the fuzzy version model were undertaken by considering a variable value of the Dispatcher Preference Index (DPI) parameter between [0, 1]. Finally, the influence of DPI on the final objective and the indicators of the problem were discussed using stochastic simulation, and the best value of DPI was obtained. Shi, Boudouh, Grunder, and Wang [
30] investigated the HHC problem considering stochastic travel and service times through stochastic programming with recourse. Then, they applied a simulated annealing (SA) algorithm to obtain the solutions of the problem. Comparisons between the solutions obtained by the stochastic model and the deterministic one have validated the advantages and robustness of considering stochastic travel and service times. Issabakhsh, Hosseini-Motlagh, Pishvaee, and Saghafi Nia [
31] presented a robust optimization model for patients in need of dialysis in which the travel times of nurses are uncertain. Their results showed that the proposed method has less than a 30% variation in the results at the maximum uncertainty level, and, in comparison to the deterministic model, the costs increased only by 1.2%. An innovative approach to accept or reject new patients by a nurse was recently investigated in Demirbilek, Branke, and Strauss [
32]. The objective was to maximize the average number of daily visits for a single nurse. They proposed a new heuristic-based approach, and then, random scenarios were created to present this simple and fast method. Their approach was compared with two greedy heuristics from the literature and showed that it achieves significantly better results compared to other methods. Carello, Lanzarone, and Mattia [
33] proposed a multicriteria optimization approach to consider different goals of the stakeholders with regard to the need for continuity of the care and considering certain and uncertain patient demands. The three stakeholder perspectives were modeled as alternative objective functions of an integer linear programming (ILP) model, and a threshold method to include all of them is proposed. The approach was then validated on real-life instances, and they considered both deterministic and uncertain patient demands. Khodaparasti, Bruni, Beraldi, Maleki, and Jahedi [
34] presented a multiperiod allocation method through a robust approach in which the patient demand was considered to be uncertain. The problem was formulated as a covering model in which the capacity of the facilities as well as the demand elasticity were considered. Then, they applied the proposed model to a real case study.
Bazirha, Kadrani, and Benmansour [
35] dealt with the HHCRSP problem with stochastic travel and care times and the goal to minimize the transportation costs of the nurses and the expected value of recourse caused by delayed services and the overtime of the nurses. The performance of the developed genetic algorithm with an embedded Monte Carlo simulation was discussed. Later in an extended paper, Bazirha, Kadrani, and Benmansour [
36] proposed a stochastic programming model with recourse for solving the HHCRSP problem, where the goal was the minimization of the transportation costs and the expected value of recourse, and also multiple services and their synchronization were considered. While the underlying deterministic problem was solved by CPLEX, a genetic algorithm and a general variable neighborhood search heuristic, the stochastic problem was solved by Monte Carlo simulation embedded into their genetic algorithm. Recently, Bazirha [
37] applied a similar approach to the HHCRSP problem with additional hard/fixed time windows and the objective to minimize the traveling costs of the nurses and the average number of unvisited patients. Very recently, Di Mascolo, Martinze, and Espinouse [
38] presented a survey of the relevant literature and a bibliometric analysis in the field of home health care. They reviewed and analyzed the current state-of-the-art with a focus particularly on uncertain and dynamic aspects.
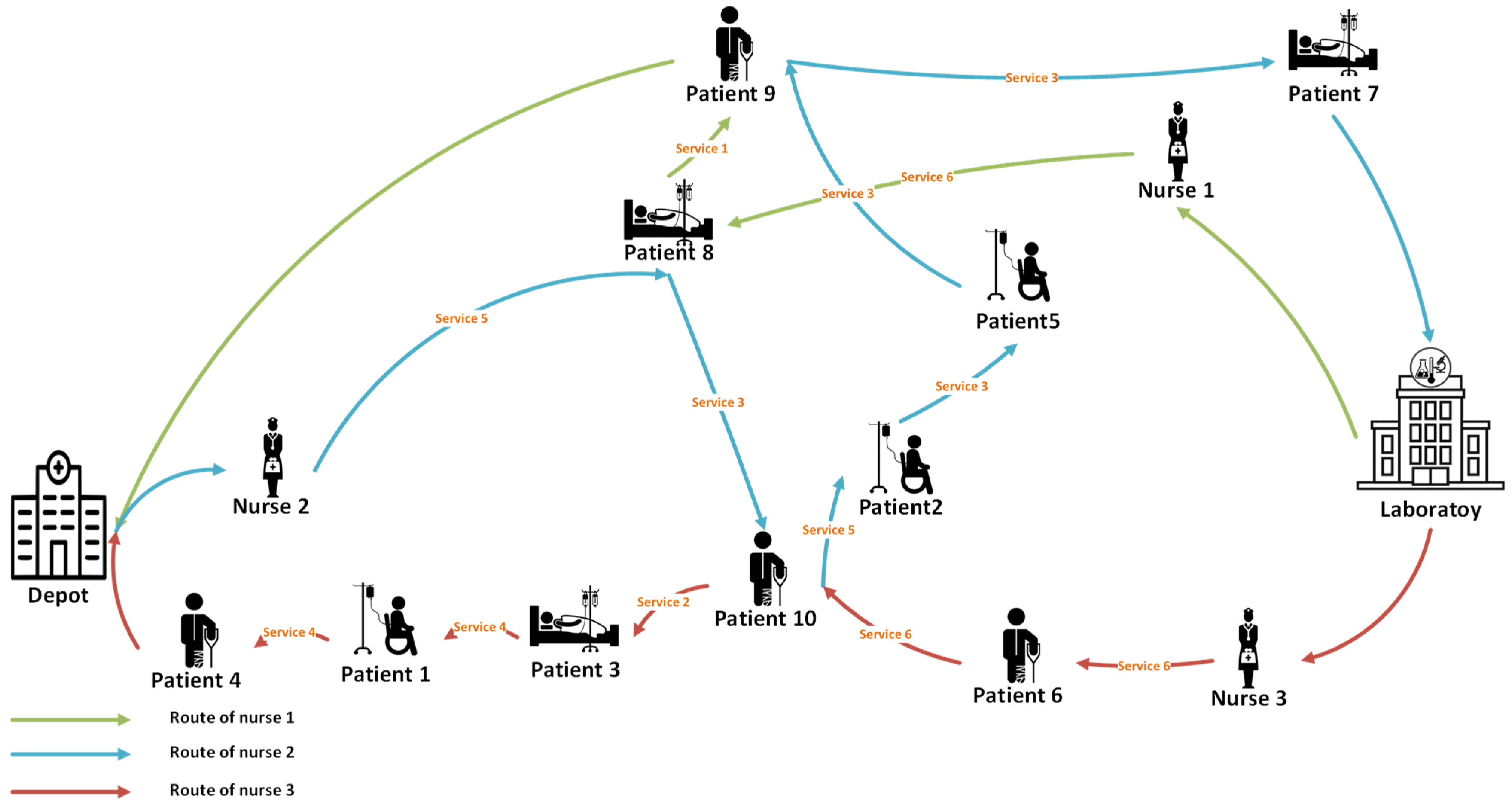
To the best of the authors’ knowledge and as it can be seen from the discussed literature, most of the studies assumed that each nurse should start her/his journey from the depot and end it at the laboratory. In home health care’s real world, there are some services, which need special instruments and force the nurse to start her/his route from the laboratory. On the other hand, if a nurse has to take a biological test or a blood test, she/he should end her/his route at the laboratory instead of the depot [
11]. Such requirements inspired us to develop conventional models to a more flexible model, which can consider different options for the origin and the destination of nurse routes.
The rest of the paper is organized as follows. The description of the problem and the mathematical model are given in
Section 2. The methodological background of the paper is stated in
Section 3.
Section 4 discusses the computational experiments. The results of a sensitivity analysis are explained in
Section 5.
Section 6 offers some managerial insights, and, finally, study limitations, conclusions, and future studies are presented in
Section 7.
7. Study Limitations, Conclusions, and Future Studies
In the real world of home health care context, there are a lot of hard constraints that cannot be considered as soft constraints with some penalties. One of the limitations of this study is the high number of hard constraints that must be satisfied. Constraints, such as special patient needs in a tight and short acceptable time window, the variety of service types that need different nurse qualifications and certificates, and also some service features and instrument requirements that forced some routes to be started from a special place complicate the problem and make the feasible region smaller. Therefore, modeling the real world of this problem was difficult, and also finding a real-world optimal solution with exact algorithms in a small feasible region was complex and needed a high computational effort. On the other hand, due to the high level of complexity in this study, uncertainties were not considered.
Nowadays, an effective management of health care systems is one of the most important concerns of policy makers. These systems can constrain high costs to the communities and have an impressive impact on the public health of the societies. At present, the correct management of health system capacities has received much attention. Giving service to patients in their homes is one of the recent methods to provide suitable health care services. The most important issue that is addressed at the operational level of this problem by the researchers is the routing and scheduling of home health care. In order to improve the quality of the services and reduce the operational costs, it is important to find an optimal solution for the planning (including routing and scheduling) of the home health care problem. This problem is actually an extension of the famous vehicle routing problem (VRP) considering additional features required by health care. This study presents a mathematical model to consider flexibility in the starting and ending points of the nurses due to different real-world service features. These real-world service features can affect the whole optimal planning of the nurses. In this regard, various constraints of home health care problems were taken into account, such as patients time windows, appropriate sequence of services, necessity of responding to all patient needs, and matching the nurse skills with the required services by the patients.
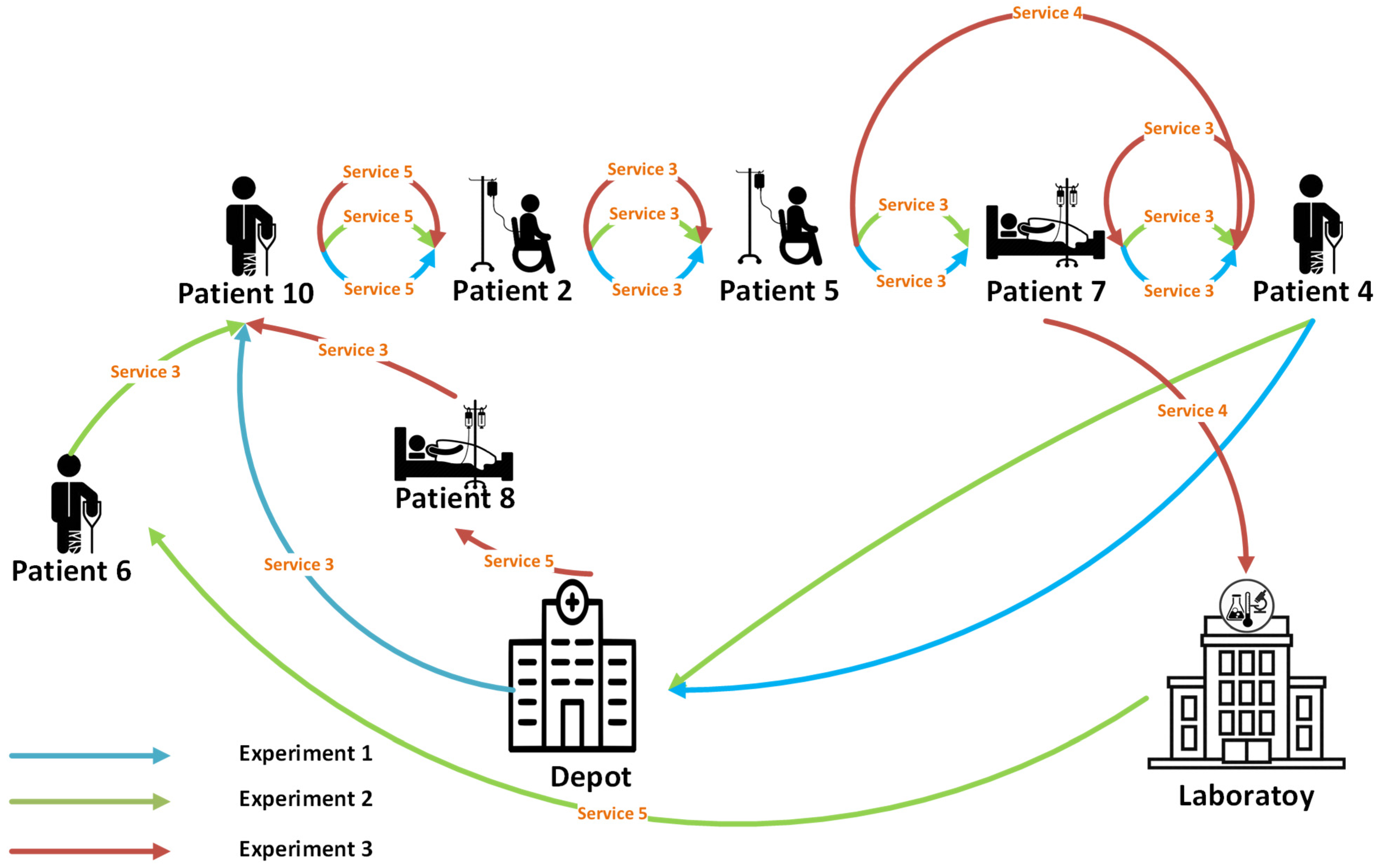
In order to demonstrate the applicability of the suggested model, a small example was first run to demonstrate the validity of the model. In addition, the interpretation of the results showed the importance of the proposed model. Several sets of problems including large-, medium-, and small-sized instances were used to show the efficiency of the new model for problems of various sizes. Moreover, to analyze the effect of important parameters of the problem, a sensitivity analysis was executed on the parameter of the required features for the services. Finally, to help the decision makers handle their limited resources more effectively, some managerial insights were presented.
As a direction for future research, considering the problem in stochastic situations could be an attractive idea. Employing improved exact techniques, such as Benders Relaxation method, could be another direction to solve the suggested model. Moreover, when exact approaches cannot be applied to large-sized problems, using metaheuristic and heuristic approaches could be worthwhile. By considering various existing stakeholder proposals, the home health care problem could be viewed from various perspectives. Thus, multiobjective optimization approaches can be applied to cover different objectives simultaneously. Finally, developing the model using time-dependent traveling times and incorporating nursing education times in the planning could be other streams.





{kind=link}
{kind=link}
{kind=link}