Abstract
This study examines the effects and durability of postural exercise on gait kinematics in people with intellectual and developmental disabilities (IDDs). Thirty-four men with mild IDDs were assigned to either the training group (n = 19) or the control group (n = 15). The TG performed the intervention over 8 weeks, 3 days/week, 1 h/day. The results indicated that the intervention program had a significant effect on some variables of gait. Additionally, in the TG between post-test and follow-up, there was no significant difference, which indicated that gait variables were maintained by the TG one month after the end of the program. This research demonstrates that postural exercises are a viable intervention for enhancing the gait of people with IDDs.
1. Introduction
Independent and safe movement is essential for functional and social purposes and activities of daily living. Mobility refers to changing body position or location or by transferring from one place to another, and depends on an individual’s body function, structure, gait, and balance capacities [1]. Gait is a complex activity that consists of motor and cognitive activities and relies on constant interaction between the central, peripheral, and musculoskeletal systems [2]. Gait pattern is the result of enhancing force, stability, shock absorption, and energy-saving factors. Therefore, any disturbance in one’s gait pattern can cause instability, pain, and increased energy consumption [3].
Intellectual and developmental disability (IDD) refers to a condition characterized by substantial limitations in both intellectual functioning and adaptive behavior. Adaptive behavior encompasses a range of practical, social, and conceptual skills. These limitations appear before the age of 22 [4]. The classification for subdividing people with IDDs into smaller groups should take into account (a) the intensity of support needs; (b) the extent of limitations in conceptual, social, and practical adaptive skills; and (c) the extent of limitations in intellectual functioning [4].
Postural control is one of the motor abilities that affects motor control, in which persons with IDDs have significant challenges. This is because the central nervous system, which regulates motor and cognitive abilities, often shows some degree of delay in individuals with IDDs [5]. In addition, individuals with IDDs may have several functional disorders of balance [6,7], motor ability [8,9,10], and cognitive ability [9,11]. Delays in motor and cognitive development affect the gait patterns of individuals with IDDs because their efficiency and performance depend on the coordination between these systems [12]. Other factors that may affect gait patterns in these people are weakness in the muscles and joints of the lower extremities, obesity, and the use of multiple medications [3,13].
The functional limitations of individuals with IDDs may be partial or total [14]. As a result, the gait pattern may be observed with impaired sensory integrity and motor development. Shorter stride length, larger stride width, increased double support time, reduced lower limb joint mobility, joint kinetics, and biomechanical changes lead to adopting a “caution in stepping” strategy due to a fear of falling [2,3,15,16]. Enkelaar et al. (2012) discovered that mobility limitations in individuals with IDDs were primarily caused by gait and balance difficulties [17]. Thus, people with IDDs may have frequent falls that lead to injury [18]. The main components of the gait impairment in these individuals are deficits in balance and postural control [17]. Therefore, the optimization of gait is often a rehabilitation goal for individuals with IDDs. Because a relationship between constraints on balance control and gait limitations in IDD has been determined, increased efficiency of postural control may be necessary to facilitate their functional performance.
It was observed that balance, gait, and strength training can increase joint loading and ultimately increase gait and stride length in people with Down syndrome [19]. Gait speed depends on stride length and cadence. People with IDDs tend to walk slower, as they must compensate for sensory impairments. In this way, the individual adopts simpler and slower functional movement strategies, thus compensating for cerebellar changes [20,21].
“The intricacy of managing balance leads to various issues related to balance, gait, and falling, which require a systematic clinical evaluation for effective intervention. Several clinical tests are designed to assess only one specific “balance system”, but since balance control is a complex process that involves multiple underlying systems, a comprehensive evaluation is necessary”.
The development of the Balance Evaluation Systems Test (BESTest) was intended to address this issue by providing a means of evaluating balance [22]. The BESTest can be applied to recognize and classify diverse postural control challenges. Currently, it is considered one of the most all-inclusive, practical, straightforward, and cost-efficient clinical evaluations of balance. The test was initially developed in 2009 [22] and has subsequently undergone validation in several countries, including Iran [6]. The examination evaluates issues related to the operation of equilibrium using six elements: (1) biomechanical constraints; (2) stability limits/verticality; (3) anticipatory postural adjustments; (4) postural responses; (5) sensory orientation; and (6) gait stability. Each system is composed of neurophysiological components that regulate specific elements of postural control.
To direct specific types of treatments, therapists must be able to recognize the disordered system underlying the balance control in their clients [22]. To develop exercise interventions, it is important to thoroughly evaluate the postural control system while taking into account any impacted systems, based on the factors mentioned. Hence, having precise information about these equilibrium systems is crucial [23]. If one or more of these systems are disturbed, it may result in postural instability and a higher likelihood of falling. Therefore, it is important to implement exercise programs based on the BESTest, to influence the different components and subsystems in charge of controlling the balance.
Different studies recommend that evaluation and training protocols for individuals with IDDs should be based on the above-mentioned postural control factors [6,17,22]. To improve the different gait parameters of people with IDDs, it is of vital importance to implement specific education and exercise programs for this particular population. As indicated by Lee et al. (2014, 2016), it is possible to improve balance and gait parameters by implementing a balance exercise program [24,25]. On the other hand, Ahmadi et al. (2020) indicated that lower extremity isokinetic peak torque, static balance, ankle and knee range of motion (ROM), and step length improved after participating in a functional strength training program for people with Down syndrome [26].
To the best of our knowledge, there is a lack of studies examining the effect of exercise on gait patterns in young adults with IDD. Therefore, this study aimed to analyze the impact of postural exercises based on the BESTest program, including the six main sources that affect postural control on the gait kinematics of young adults with IDD. We hypothesized that the exercise program based on BESTest would lead to improvements in gait parameters in individuals with IDDs.
2. Materials and Methods
2.1. Study Design
The present study is a two-armed randomized controlled trial. The study assessed the outcome variables on three occasions: prior to the commencement of the intervention, immediately after the 8-week intervention period, and one month following the conclusion of the intervention. The training protocol was performed at the center that all of the participants attended daily. The training group (TG) completed an 8-week program of selected postural exercises with 3 sessions a week (24 sessions in total). Each session lasted approximately 1 h. In each training session, all aspects of the BESTest system were utilized, encompassing all systems. Table 1 provides an overview of the intervention’s characteristics. The participants of the control group (CG) continued their regular activities at the center.

Table 1.
Characteristics of the study participants.
2.2. Participants
After reviewing previous research [27,28] and utilizing an effect size of d = 0.41 and α < 0.05, and a power (1- β) of 0.80, we concluded that a minimum of 34 participants would be required for this study. The study involved the participation of thirty-four males with mild IDDs who were randomly assigned to either the treatment group (TG; n = 19) or control group (CG; n = 19). Following randomization, four participants in the control group chose to withdraw from the study (CG; n = 15). Table 1 depicts the general characteristics of the participants.
All participants were recruited from one specific center for individuals with IDDs (convenience sample). The intelligence quotient (IQ) of each participant was obtained by an expert using the Wechsler Intelligence Scale—IV. To verify that all participants had a mild IDD, a registered psychologist conducted psychological tests, which included the different domains of adaptive behavior, and an educational test [29].
The inclusion criteria were as follows: being diagnosed with mild IDD (IQ = 50–70 mean and deficits in adaptive behaviors); young individuals with IDDs; the ability to comply with the study’s exercise program and safety protocols; willingness to participate in regular training sessions; and parents/legal guardians and participants agreed to provide written consent. Participants who were involved in rehabilitation and/or occupational therapy activities that could potentially disrupt the training program were excluded from the study; the following reasons were also exclusion criteria: participating in other exercise programs; conditions affecting the vestibular and visual systems that could impact the evaluations; the administration of drugs that could potentially impact motor and/or cognitive functions; inability to provide written informed assent; parents or legal guardians were not willing to give written consent; suffered from neurological disorders; or musculoskeletal conditions prevented them from walking without assistance.
This study complied with the principles of the Declaration of Helsinki (World Medical Association, 2013) and was registered prospectively (trial registration number: IRCT20180203038603N1).
2.3. Procedures
Initially, all subjects were invited to two sessions over two days. The purpose of the first session was to familiarize the participants with the laboratory environment, introduce the tests, have the informed consent forms completed by parents, and measure anthropometric information such as height and weight, as well as the joint width of the knee and ankle of all subjects. Then, in the second session, the subjects performed a gait test and the kinematic data on the gait were collected using a three-dimensional motion capture system (Vicon, Los Angeles, CA, USA). The gait kinematics of the subjects were assessed by two trained raters. The evaluators were not informed about the group allocation of the participants. The tests were performed at baseline, at the end of the program, and one month after the end of the program.
2.4. Postural Exercise Training
Two adapted physical education instructors alternated in delivering the postural exercise training in this study. The training program was conducted three times a week for an hour each time, and it continued for eight weeks. This protocol aimed to create each training session as personalized as possible. As a component of our training program, we utilized the overload principle by enhancing the intensity of exercises, increasing the number of repetitions, and reducing the rest time between workouts.
The program was developed based on the six primary subsystems of the BESTest, which included biomechanical constraints, stability limits/verticality, anticipatory postural adjustments, postural responses, sensory orientation, and gait stability. Each activity outlined in Table 2 encompasses a range of exercises that follow the fundamental principles of the BESTest approach. The training sessions were divided into three parts: the warm-up phase, the main part, and the cool-down phase. These exercises were designed for individuals with IDDs according to their safety and applicability. All workout sessions were conducted in the afternoon (Table 2).
Table 2.
Characteristics of the postural exercise program based on the BESTest system.
2.5. Measurements
Regarding kinematic gait parameters, the gait analysis for all subjects was conducted at the sports science facility in the Guilan University laboratory. For this purpose, each participant performed a gait test in a 10 m corridor in the laboratory, and the kinematic parameters during the test were recorded using a three-dimensional motion analysis system (Cortex v7.0, Motion Analysis Corporation, Santa Rosa, CA, USA) and six Raptor-H cameras (Raptor-H, Motion Analysis Corporation, Santa Rosa, CA, USA).
Before testing, the motion analysis system was calibrated following the manufacturer’s instructions (T-shaped and triangular tools with light-reflecting markers) for a space of 1.5 × 3 × 2 m. This space was located in the middle of a 10 m corridor in the laboratory. After preparing the testing essentials, a single researcher applied 16 25 mm retro-reflective markers manually on both lower limbs using the plugin gait marker to set the model for kinematic measurements during gait tests [24,30]. Then, to define the Plug-In-Gait biomechanical model, each participant stood upright in the calibrated space and placed his upper limb in a 90-degree abduction position so that all markers were visible for about 2 s. Then, participants walked barefoot at their self-selected pace along the laboratory path. Thus, gait kinematic parameters were recorded from three planes (sagittal, frontal, and horizontal) and gait kinematic parameters were extracted such as gait length (cm), step length (cm), gait speed (m/s), gait pace (step/min), setting time (percentage of the gait cycle), swing time (percentage of the gait cycle), and dual support time (percentage of the gait cycle).
All data were extracted using Cortex software (Cortex v7.0, Motion Analysis Corporation, Santa Rosa, CA, USA) and entered into an Excel spreadsheet. The test was repeated three times with a pause of one minute between each repetition. The average of three trials was used for the analysis.
2.6. Statistical Analysis
Descriptive statistics were obtained for age, height, weight, BMI, and gait parameters. Continuous variables were reported as means and standard deviations, while categorical variables were expressed as percentages. The normality of the data was assessed using the Shapiro–Wilk test.
To determine any differences within or between subjects, we employed a repeated measures general linear model. Specifically, we conducted a mixed-factor repeated-measures ANOVA to compare gait kinematics across time points (i.e., pre, post, and follow-up) and between groups (i.e., control group and training group). The time factor was treated as a within-subjects factor, while the group factor was considered as a between-subjects factor. The purpose of this analysis was to examine the main effects (i.e., time and group) and the interaction effect (i.e., time × group) on the dependent variable (gait kinematics). The significant within-group effects were analyzed using paired-sample t-tests. Effect sizes were calculated using Cohen’s d where possible. Effect sizes were classified as small (d ≤ 0.49), medium (d ≥ 0.50; d ≤ 0.79), or large (d ≥ 0.80) [31]. The significance level was set to p ≤ 0.05. The data were analyzed using the Statistical Package for the Social Sciences (IBM SPSS, v 21.0, Chicago, IL, USA).
3. Results
Table 1 depicts the descriptive characteristics of the participants. Both groups had similar age, height, weight, BMI, and IQ (all p < 0.050).
Gait Parameters
At the beginning of the study, there were no differences in the parameters of gait kinematics between the two groups (all p > 0.050).
There were significant group × time interactions for step and stride length (F [2, 32] = 39.41; p < 0.001; η2 = 0.55), cadence (F [2, 32] = 28.83; p < 0.001; η2 = 0.47), gait speed (F [2, 32] = 13.11, p < 0.001; η2 = 0.30), and stance and swing (F [2, 32] = 7.66; p < 0.001; η2 = 0.19). Nevertheless, there was no significant group × time interaction for step width and double support (p > 0.050).
The post hoc analysis revealed that the TG significantly improved their step length in pre–post training (t = −4.85; p < 0.001; d = 0.61) and from pre-training to follow-up (t = −4.41; p < 0.001; d = 0.56).
The TG significantly improved their stride length in pre–post training (t = −4.85; p < 0.001; d = 0.61), and from pre-training to follow-up (t = −4.41; p < 0.001; d = 0.56). However, no significant differences were observed in step length and stride length post training vs. the follow-up period (t = 0.94; p = 0.35).
The TG significantly improved their cadence in pre–post training (t = −5.2; p < 0.001; d = 1.03) and from pre-training to follow-up (t = −3.85; p < 0.001; d = 0.91). However, no significant changes were observed between the post-training vs. follow-up values (t = 1.43; p = 0.43; d = 0.08).
The TG also improved their gait speed in pre–post training (t = −5.52; p < 0.001; d = 0.99) and pre-follow-up (t = −3.41; p < 0.002; d = 0.77), but there were no significant changes post training vs. the follow-up period (t = 1.69; p = 0.10).
The TG group significantly increased their stance in pre–post training (t = 4.14; p < 0.001; d = 0.98) and from pre-training to follow-up (t = 3.45; p < 0.002; d = 0.83), but no significant changes were observed post training vs. the follow-up period (t = −1.3; p = 0.20).
The TG group significantly increased their swing in pre–post training (t = −4.14; p < 0.001; d = 0.98) and from pre-training to follow-up (t = −3.45; p < 0.002; d = 0.83); however, no significant changes were observed between the post-training vs. follow-up values (t = 1.3; p = 0.20). It is noteworthy that the CG was not significantly different in any parameter evaluated between the pre- and post-training or follow-up tests (Table 3) (Figure 1).
Table 3.
Gait parameter outcomes in the pre–post and follow-up assessments for each group of subjects with intellectual and developmental disabilities.
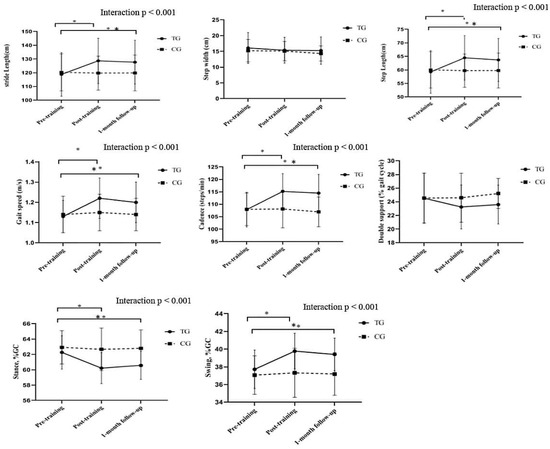
Figure 1.
Pre-, post, and follow-up gait parameters in the training group (TG) and control group (CG). * Post hoc analysis: differences between pre- and post training in the TG vs. CG. ** Post hoc analysis: differences between pre-training and 1-month follow-up in the TG vs. CG.
4. Discussion
This study was conducted to analyze the effects of the BESTest exercise program on kinematic gait parameters in individuals with IDDs. The results showed that 8 weeks of selected exercises led to a significant improvement in gait kinematic parameters, such as step length, stride length, cadence, and speed of gait, stance, and swing. There is limited research on the impact of exercise programs on gait kinematic parameters in individuals with IDDs. Lee et al. (2014) examined the effects of an 8-week balance program on the gait kinematics of people with IDDs. The results showed that balance training programs led to significant improvements in participants’ performance in spatiotemporal gait parameters [24].
Lee et al. (2016), in another study on the effects of 8 weeks of a balance training program on the balance, gait, and muscle strength of adolescents with IDD, with an average age of 14–19 years, reported that balance training did not significantly improve the 10 m gait test, which is not consistent with the present study. Possible reasons for this include the type of exercise program, the age range of the subjects, and the method of measuring the gait variable, or it could be due to a different exercise protocol [25].
Rodenbusch et al. (2013) examined the effect of treadmill inclination exercises on individuals aged 5–11 years with Down syndrome. The results showed that in individuals with Down syndrome, changes in spatiotemporal gait parameters and angular variables were created in the stance phase and plantar flexion reduction before swing [32]. Another study by Vinagre et al. (2016) examined the effect of 10 weeks of Bobath physiotherapy training in individuals with Down syndrome with a mean age of 28 years. They observed enhancements in speed, cadence, step length, stride length, and step width. They also found improvements in stepping angle correction and symmetry [33]. Another study showed that treadmill training could improve gait patterns and increase step and stride length in infants with Down syndrome [34].
Carmeli et al. (2002) examined the effect of 6 months of treadmill training on IDD, and after training, gait and balance also improved significantly [35]. Kubilay et al. (2011) performed 8 weeks of balance training with a Swiss ball in adolescents with IDD. The results indicated a significant improvement in all parameters for the group that received the training [36,37]. Hou TS (2008) examined the effects of 8 weeks of low-intensity jogging and walking exercises in adolescents with IDDs and found significant improvements in gait speed [38].
Previous research has indicated that individuals with IDDs experience greater declines in age, gait ability, and dynamic balance compared to neurotypical individuals [10,36,39]. These studies showed reductions in all gait spatiotemporal parameters and a reduced hip range of motion, affecting step length. In addition, it was observed that the increase in the double support time and step width led to greater instability in individuals with IDDs [25].
The TG in our study was likely to have improved flexibility and muscle strength and this may have reduced the fear of falling due to increased self-confidence. Improving these parameters may lead to improved gait kinematic parameters in individuals with IDDs [40].
For example, the exercise of crossing obstacles leads to an improvement in the stride length and range of motion of the joints. Additionally, walking on a mattress facilitates and integrates the visual and atrial inputs for balance and gait [41]. In addition, balance, gait, and strength training can also increase joint loading and ultimately increase gait and stride length in people with motor disabilities [19].
Individuals with IDDs present an increase in asymmetric movements, especially in their torso and head, which reduces push-off motions and reduces gait speed [42]. Gait function is crucial for performing daily activities independently, and gait speed is a crucial measure of gait disability [15]. On the other hand, reducing the gait speed provides more time for an appropriate response and more balance [43]. In another study by Lee et al. (2014), the balance training program improved gait speed in the experimental group by 31% [24].
Angulo-Barroso et al. (2008) showed that speed gait increased after treadmill training in individuals with IDDs [44]. Verghese et al. (2009) reported that a reduction in speed of 10 cm/s was equivalent to a loss of 10% mobility in daily life, and compared with those in the experimental group, they showed a 30% improvement in gait speed and increased independence in daily life [45]. Additionally, to increase gait speed through cadence, you have to increase the number of steps per minute, which requires more dynamic balance. Therefore, in the training group, better dynamic balance and better cadence led to increased gait speed [39,46]. Therefore, it can be said that an increase in gait speed is due to an increase in cadence, as well as step and stride length [47].
According to different studies, other causes of increased gait speed following a training program are a reduction in double support and increased ankle joint mobility, which is usually reduced in people with IDDs [48]. In other words, increasing the double support phase leads to a decrease in speed and instability in the gait; so, performing balance training and reducing the time of double support indicates an increase in gait stability.
On the other hand, the increased swing phase has a significant effect on the individual’s capacity to maintain a correct posture and facilitate walking [24]. The current study revealed a notable rise in swing time, resulting in an increase in cycle time. As mentioned before, an increased swing time significantly affects the individual’s capacity to maintain an integrated posture and facilitate gait [32]. In general, improving one’s adaptation to everyday obstacles reinforces the idea that selected exercises are a valuable program for people with IDDs.
In justifying the durability of the observed training effects, we can refer to the results of Llorens-Martin et al. (2010), who showed that 7 weeks of voluntary physical training had a significant effect on increasing the process of neuron production in the hippocampus. This effect might have caused improvements in the learning process in our participants because the hippocampus is responsible for motor memory in humans, and the volume of this part of the brain is directly related to learning and motor memory [49]. Increasing the number of cells in this part of the brain indicates an improvement in neural processes that perform motor skills [50]. According to this theory, differences in motor performance between neurologically impaired individuals and the general population are due to the motor control system functioning sub-optimally. The exercise program implemented in our study was probably able to increase the intensity of stimuli that activate motor neurons, producing greater force and thus providing movement patterns comparable to those observed in individuals without disabilities [26,51].
In the present study, the possible effects of movement on the functioning of the neuromuscular system might be attributed to the fact that motor training leads to changes in the transcription process of several known genes associated with neuronal activity, synaptic structure, and the production of neurotransmitters [49]. Exercise may produce adaptations in the hippocampus, which plays an essential role in learning and memory. In this regard, research has shown that physical activity can affect neuroprotective processes and brain flexibility and positively affect cognition and behavior [52].
4.1. Limitations
This study has several limitations that need to be acknowledged. Firstly, the generalizability of our results to individuals with moderate and severe IDDs is limited since we only focused on those with mild IDD. Additionally, caution should be exercised in interpreting our findings as we used a convenience sample. Secondly, our study did not evaluate the balance and risk of falls or injuries of the participants. Thirdly, the duration of our program was only 8 weeks and the follow-up assessment was conducted only 1 month after the end of the study. Therefore, it is recommended to conduct future studies with longer program durations and follow-up assessments at 6 or 12 months to determine whether any changes are sustained over time. Lastly, the authors did not assess the physical activity or sedentary levels of the participants, which could have influenced their gait-related parameters. However, since all participants were from the same center, their physical activity and sedentary levels may be similar.
4.2. Implications and Suggestions for Future Research
According to JudgeRoy et al. (1996), increased strength of the lower extremity muscles may lead to improvements in gait patterns [53]. Thus, future studies should not only evaluate gait kinematics but also assess muscular strength, balance, functional mobility, and quality of life.
More extensive research is needed to analyze gait and kinematic parameters in persons with moderate, severe, and profound IDDs, as well as exercise programs aimed at improving these parameters. Finally, a longer study with extended follow-up would be necessary to gain a better understanding of the effect of BESTest-based postural exercise programs on balance and fall or injury risks in people with IDDs.
Rehabilitation specialists can use basic and specific principles to recommend and implement exercises for young adults with IDDs to maintain and enhance their balance and gait kinematics. The exercise program used in our study can be easily adopted in clinical practice and IDD centers. The implementation of the BESTest program could help to improve the gait performance of people with IDDs and reduce the risk of falls and injuries in this population.
5. Conclusions
The individuals with IDDs who participated in an eight-week BESTest-based postural exercise program showed various improved gait-related parameters and decreased gait pattern abnormalities. The improvements obtained in our study may help to prevent long-term complications, reduce the risk of falls, increase physical performance, and facilitate participation in activities of daily living. We suggest that the exercise program used in this study can be adopted by parents, educators, physiotherapists, healthcare providers, and IDD centers to enhance the quality of life, personal independence, and gait patterns of individuals with IDDs.
Author Contributions
Conceptualization, S.B. and G.R.O.; methodology, E.H.; software, S.B.; validation, G.R.O., S.B. and E.H.; formal analysis, S.B.; investigation, S.B.; resources, E.H.; data curation, G.R.O. and S.B.; writing—original draft preparation, G.R.O.; writing—review and editing, G.R.O.; visualization, E.H.; supervision, S.B.; project administration, S.B.; funding acquisition, S.B. All authors have read and agreed to the published version of the manuscript.
Funding
The study of these results was carried out with funding from the Department of Research and Universities of the Generalitat de Catalunya and the Ramon Llull University (2023-URL-Proj-014).
Informed Consent Statement
All parents/guardians of the participants provided informed consent, and the participants themselves gave verbal assent before being included in the study.
Data Availability Statement
The measurement data used to support the findings of this study are available from the corresponding author upon request.
Acknowledgments
We would like to express our gratitude to the Guilan Intellectual Disabilities Association, especially the parents and individuals with IDs who participated in this study and willingly underwent all of the scheduled evaluations. Special thanks to Rahman Amiri and Hamed Babagoltabar Samakoush for their valuable assistance and contributions to the research program. The study of these results was carried out with funding from the Department of Research and Universities of the Generalitat de Catalunya and the Ramon Llull University (2023-URL-Proj-014).
Conflicts of Interest
The authors declare no conflict of interest.
References
- World Health Organization. International Classification of Functioning, Disability and Health: ICF; World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- Oppewal, A.; Hilgenkamp, T.I. The dual task effect on gait in adults with intellectual disabilities: Is it predictive for falls? Disabil. Rehabil. 2019, 41, 26–32. [Google Scholar] [CrossRef]
- Oppewal, A.; Festen, D.A.; Hilgenkamp, T.I. Gait characteristics of adults with intellectual disability. Am. J. Intellect. Dev. Disabil. 2018, 123, 283–299. [Google Scholar] [CrossRef] [PubMed]
- Schalock, R.L.; Luckasson, R.; Tassé, M.J. An overview of intellectual disability: Definition, diagnosis, classification, and systems of supports. Am. J. Intellect. Dev. Disabil. 2021, 126, 439–442. [Google Scholar] [CrossRef]
- Reguera-García, M.M.; Leirós-Rodríguez, R.; Álvarez-Barrio, L. Reliability and Validity of the Six Spot Step Test in People with Intellectual Disability. Brain Sci. 2021, 11, 201. [Google Scholar] [CrossRef] [PubMed]
- Bahiraei, S.; Daneshmandi, H.; Norasteh, A.A.; Yahya, S. Balance stability in intellectual disability: Introductory evidence for the balance evaluation systems test (BESTest). Life Span Disabil. 2019, 22, 7–28. [Google Scholar]
- Bahiraei, S.; Daneshmandi, H.; Sokhangoei, Y. The Study of Biomechanical Gait Cycle and Balance Characteristics in Intellectual Disabilities: A Systematic Review. Phys. Treat. Specif. Phys. Ther. 2018, 8, 63–76. [Google Scholar] [CrossRef]
- Cleaver, S.; Hunter, D.; Ouellette-Kuntz, H. Physical mobility limitations in adults with intellectual disabilities: A systematic review. J. Intellect. Disabil. Res. 2009, 53, 93–105. [Google Scholar] [CrossRef]
- Galli, M.; Rigoldi, C.; Albertini, G. Postural control in patients with Down syndrome. Disabil. Rehabil. 2008, 30, 1274–1278. [Google Scholar] [CrossRef]
- Giagazoglou, P.; Kokaridas, D.; Neofotistou, K. Effects of a trampoline exercise intervention on motor performance and balance ability of children with intellectual disabilities. Res. Dev. Disabil. 2013, 34, 2701–2707. [Google Scholar] [CrossRef] [PubMed]
- Kachouri, H.; Laatar, R.; Borji, R.; Rebai, H.; Sahli, S. Using a dual-task paradigm to investigate motor and cognitive performance in children with intellectual disability. J. Appl. Res. Intellect. Disabil. 2020, 33, 172–179. [Google Scholar] [CrossRef]
- Lopes Pedralli, M.; Schelle, G.H. Gait evaluation in individuals with Down syndrome. Braz. J. Biomot. 2013, 7, 21–27. [Google Scholar]
- Maas, S.; Festen, D.; Oppewal, A. The association between medication use and gait in adults with intellectual disabilities. J. Intellect. Disabil. Res. 2020, 64, 793–803. [Google Scholar] [CrossRef]
- Lin, L.-P.; Hsia, Y.-C.; Lin, J.-D. Caregivers’ reported functional limitations in activities of daily living among middle-aged adults with intellectual disabilities. Res. Dev. Disabil. 2013, 34, 4559–4564. [Google Scholar] [CrossRef]
- Almuhtaseb, S.; Oppewal, A.; Hilgenkamp, T.I. Gait characteristics in individuals with intellectual disabilities: A literature review. Res. Dev. Disabil. 2014, 35, 2858–2883. [Google Scholar] [CrossRef]
- Cioni, M.; Cocilovo, A.; Valle, M.S. Analysis of ankle kinetics during walking in individuals with Down syndrome. Am. J. Ment. Retard. 2001, 106, 470–478. [Google Scholar] [CrossRef] [PubMed]
- Enkelaar, L.; van Schrojenstein Lantman-de Valk, H.; Weerdesteyn, V. A review of balance and gait capacities in relation to falls in persons with intellectual disability. Res. Dev. Disabil. 2012, 33, 291–306. [Google Scholar] [CrossRef]
- Pal, J.; Hale, L.; Claydon, L. Injuries and falls among adults with intellectual disability: A prospective New Zealand cohort study. J. Intellect. Dev. Disabil. 2014, 39, 35–44. [Google Scholar] [CrossRef]
- Elshemy, S.A. Comparative study: Parameters of gait in Down syndrome versus matched obese and healthy children. Egypt. J. Med. Hum. Genet. 2013, 14, 285–291. [Google Scholar] [CrossRef]
- Smith, B.A.; Ashton-Miller, J.A.; Ulrich, B.D. Gait adaptations in response to perturbations in adults with Down syndrome. Gait Posture 2010, 32, 149–154. [Google Scholar] [CrossRef]
- Smith, B.A.; Ulrich, B.D. Early onset of stabilizing strategies for gait and obstacles: Older adults with Down syndrome. Gait Posture 2008, 28, 448–455. [Google Scholar] [CrossRef] [PubMed]
- Horak, F.B.; Wrisley, D.M.; Frank, J. The balance evaluation systems test (BESTest) to differentiate balance deficits. Phys. Ther. 2009, 89, 484–498. [Google Scholar] [CrossRef] [PubMed]
- Sibley, K.M.; Beauchamp, M.K.; Van Ooteghem, K.; Jaglal, S.B. Using the systems framework for postural control to analyze the components of balance evaluated in standardized balance measures: A scoping review. Arch. Phys. Med. Rehabil. 2015, 96, 122–132.e29. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.J.; Lee, M.M.; Shin, D.C.; Shin, S.H.; Song, C.H. The effects of a balance exercise program for enhancement of gait function on temporal and spatial gait parameters in young people with intellectual disabilities. J. Phys. Ther. Sci. 2014, 26, 513–516. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.; Lee, M.; Song, C. Balance training improves postural balance, gait, and functional strength in adolescents with intellectual disabilities: Single-blinded, randomized clinical trial. Disabil. Health J. 2016, 9, 416–422. [Google Scholar] [CrossRef]
- Ahmadi, N.; Peyk, F.; Garekani, S.H. Effect of functional strength training on gait kinematics, muscle strength and static balance of young adults with Down syndrome. Int. J. Mot. Control Learn. 2020, 2, 1–10. [Google Scholar] [CrossRef]
- Huri, M.; Huri, E.; Altuntas, O. Effects of occupational therapy on quality of life of patients with metastatic prostate cancer: A randomized controlled study. Saudi Med. J. 2015, 36, 954. [Google Scholar] [CrossRef] [PubMed]
- Souza, A.P.S.d.; Silva, L.C.D.; Fayh, A.P.T. Nutritional Intervention Contributes to the Improvement of Symptoms Related to Quality of Life in Breast Cancer Patients Undergoing Neoadjuvant Chemotherapy: A Randomized Clinical Trial. Nutrients 2021, 13, 589. [Google Scholar] [CrossRef]
- Blomqvist, S.; Wester, A.; Sundelin, G.; Rehn, B. Test–retest reliability, smallest real difference and concurrent validity of six different balance tests on young people with mild to moderate intellectual disability. Physiotherapy 2012, 98, 313–319. [Google Scholar] [CrossRef]
- Rigoldi, C.; Galli, M.; Cimolin, V.; Camerota, F.; Celletti, C.; Tenore, N.; Albertini, G. Gait strategy in patients with Ehlers-Danlos syndrome hypermobility type and Down syndrome. Res. Dev. Disabil. 2012, 33, 1437–1442. [Google Scholar] [CrossRef] [PubMed]
- Rosenthal, J.A. Qualitative descriptors of strength of association and effect size. J. Soc. Serv. Res. 1996, 21, 37–59. [Google Scholar] [CrossRef]
- Rodenbusch, T.L.; Ribeiro, T.S.; Simão, C.R.; Britto, H.M.; Tudella, E.; Lindquist, A.R. Effects of treadmill inclination on the gait of children with Down syndrome. Res. Dev. Disabil. 2013, 34, 2185–2190. [Google Scholar] [CrossRef] [PubMed]
- Vinagre, I.N.; Cámara, M.B.; Gadella, J.B. Gait analysis and Bobath physiotherapy in adults with Down syndrome. Int. Med. Rev. Down Syndr. 2016, 20, 8–14. [Google Scholar] [CrossRef]
- Ulrich, D.A.; Ulrich, B.D.; Angulo-Kinzler, R.M.; Yun, J. Treadmill training of infants with Down syndrome: Evidence-based developmental outcomes. Pediatrics 2001, 108, e84. [Google Scholar] [CrossRef]
- Carmeli, E.; Kessel, S.; Coleman, R.; Ayalon, M. Effects of a treadmill walking program on muscle strength and balance in elderly people with Down syndrome. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2002, 57, M106–M110. [Google Scholar] [CrossRef] [PubMed]
- Kubilay, N.S.; Yildirim, Y.; Kara, B.; Harutoglu-Akdur, H. Effect of balance training and posture exercises on functional level in mental retardation. Fiz. Rehabil. 2011, 22, 55–64. [Google Scholar]
- Hartman, E.; Houwen, S.; Scherder, E.; Visscher, C. On the relationship between motor performance and executive functioning in children with intellectual disabilities. J. Intellect. Disabil. Res. 2010, 54, 468–477. [Google Scholar] [CrossRef]
- Ts, H. The effects of run/walk exercise on physical fitness and sport skills on individuals with mental retardation. NCYU Phys. Educ. Health Recreat. J. 2008, 7, 44–58. [Google Scholar]
- Nam, H.-C.; Cha, H.-G.; Kim, M.-K. The effects of exercising on an unstable surface on the gait and balance ability of normal adults. J. Phys. Ther. Sci. 2016, 28, 2102–2104. [Google Scholar] [CrossRef]
- Shashidhara, M. The effect of eight-week yoga exercise on balance and gait in girls with intellectual disability. Int. J. Yoga Allied Sci. 2018, 7, 31–35. [Google Scholar]
- Berg, K.O.; Wood-Dauphinee, S.L.; Williams, J.I.; Maki, B. Measuring balance in the elderly: Validation of an instrument. Can. J. Public Health Rev. Can. Sante Publique 1991, 39, 7–11. [Google Scholar]
- Lipfert, S.W.; Günther, M.; Renjewski, D.; Seyfarth, A. Impulsive ankle push-off powers leg swing in human walking. J. Exp. Biol. 2014, 217, 1218–1228. [Google Scholar] [CrossRef] [PubMed]
- Rosen, S. Kinesiology and sensorimotor function. In Foundations of Orientation and Mobility; American Printing House: Louisville, KY, USA, 1997; pp. 170–199. [Google Scholar]
- Angulo-Barroso, R.M.; Wu, J.; Ulrich, D.A. Long-term effect of different treadmill interventions on gait development in new walkers with Down syndrome. Gait Posture 2008, 27, 231–238. [Google Scholar] [CrossRef] [PubMed]
- Verghese, J.; Holtzer, R.; Lipton, R.B.; Wang, C. Quantitative gait markers and incident fall risk in older adults. J. Gerontol. Ser. A 2009, 64, 896–901. [Google Scholar] [CrossRef] [PubMed]
- Behm, D.G.; Anderson, K.; Curnew, R.S. Muscle force and activation under stable and unstable conditions. J. Strength Cond. Res. 2002, 16, 416–422. [Google Scholar]
- Ardestani, M.M.; Ferrigno, C.; Moazen, M.; Wimmer, M.A. From normal to fast walking: Impact of cadence and stride length on lower extremity joint moments. Gait Posture 2016, 46, 118–125. [Google Scholar] [CrossRef] [PubMed]
- Galli, M.; Rigoldi, C.; Brunner, R.; Virji-Babul, N.; Giorgio, A. Joint stiffness and gait pattern evaluation in children with Down syndrome. Gait Posture 2008, 28, 502–506. [Google Scholar] [CrossRef] [PubMed]
- Long, J.; Feng, Y.; Urbin, M. Motor sequence learning is associated with hippocampal subfield volume in humans with medial temporal lobe epilepsy. Front. Hum. Neurosci. 2018, 12, 367. [Google Scholar] [CrossRef] [PubMed]
- Llorens-Martin, M.; Rueda, N.; Tejeda, G.S.; Flórez, J.; Trejo, J.L.; Martínez-Cué, C. Effects of voluntary physical exercise on adult hippocampal neurogenesis and behavior of Ts65Dn mice, a model of Down syndrome. Neuroscience 2010, 171, 1228–1240. [Google Scholar] [CrossRef] [PubMed]
- Novak, I.; Morgan, C. High-risk follow-up: Early intervention and rehabilitation. In Handbook of Clinical Neurology; Elsevier: Amsterdam, The Netherlands, 2019; Volume 162, pp. 483–510. [Google Scholar]
- Tong, L.; Shen, H.; Perreau, V.M.; Balazs, R.; Cotman, C.W. Effects of exercise on gene-expression profile in the rat hippocampus. Neurobiol. Dis. 2001, 8, 1046–1056. [Google Scholar] [CrossRef]
- JudgeRoy, J.O.; Davis, B., III; Õunpuu, S. Step length reductions in advanced age: The role of ankle and hip kinetics. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 1996, 51, M303–M312. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).