Electroencephalogram Similarity Analysis Using Temporal and Spectral Dynamics Analysis for Propofol and Desflurane Induced Unconsciousness





Abstract
1. Introduction
2. Materials and Methods
2.1. Ethical Statement
2.2. Patients and Surgeries
2.3. Data Recording
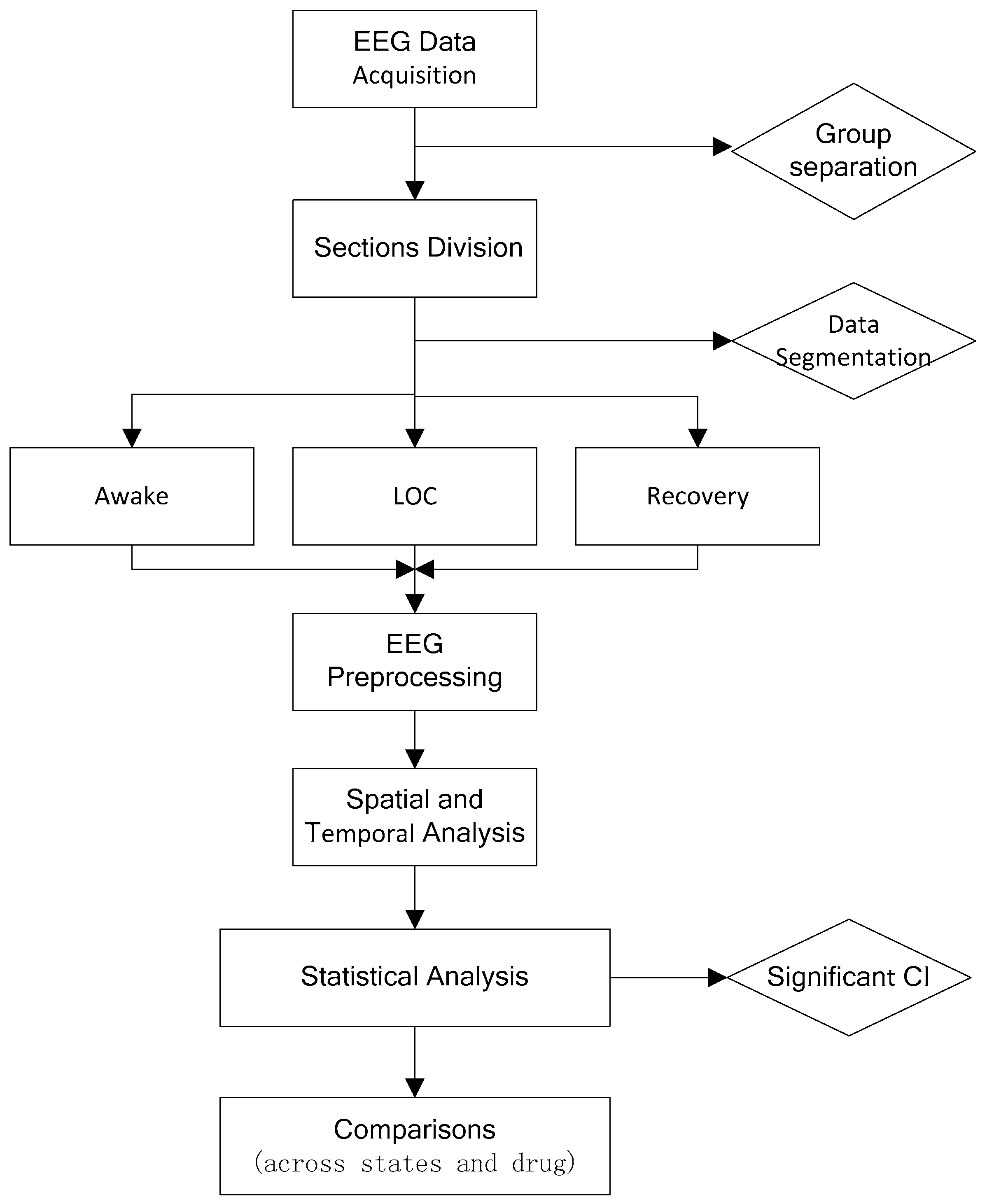
2.4. EEG Data Preprocessing
2.5. Spectral Analysis
2.6. Statistical Analysis
3. Result
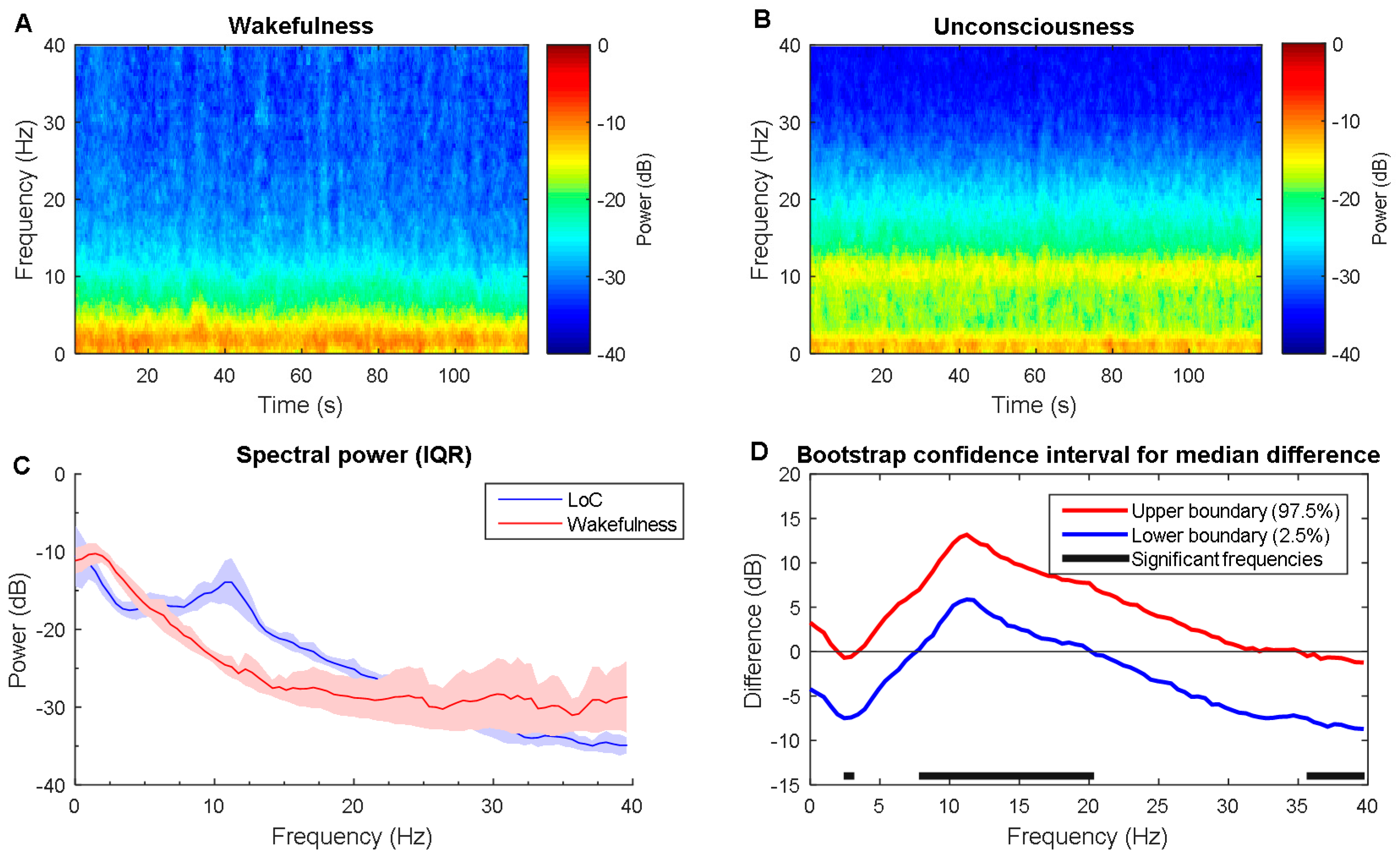
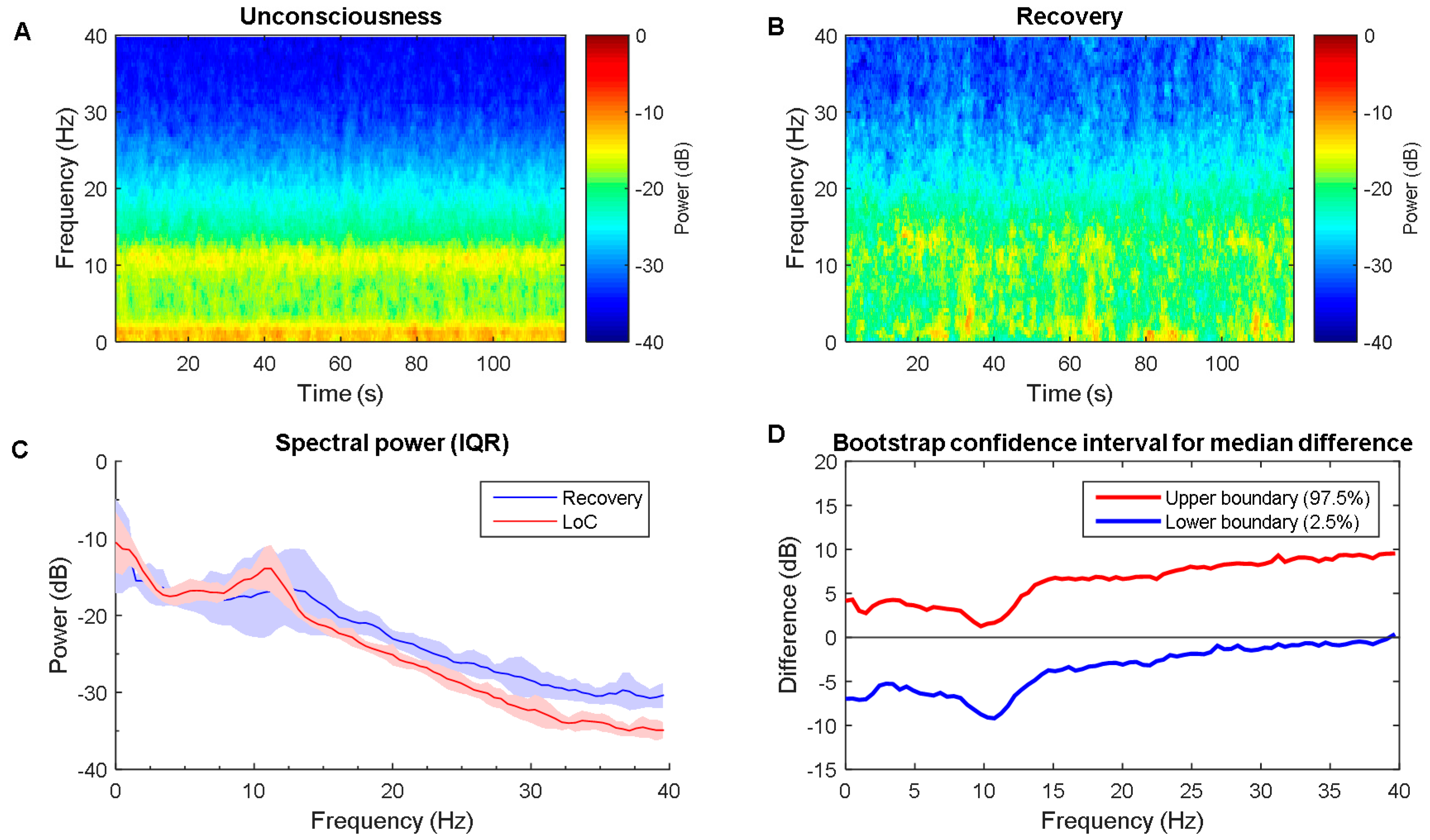
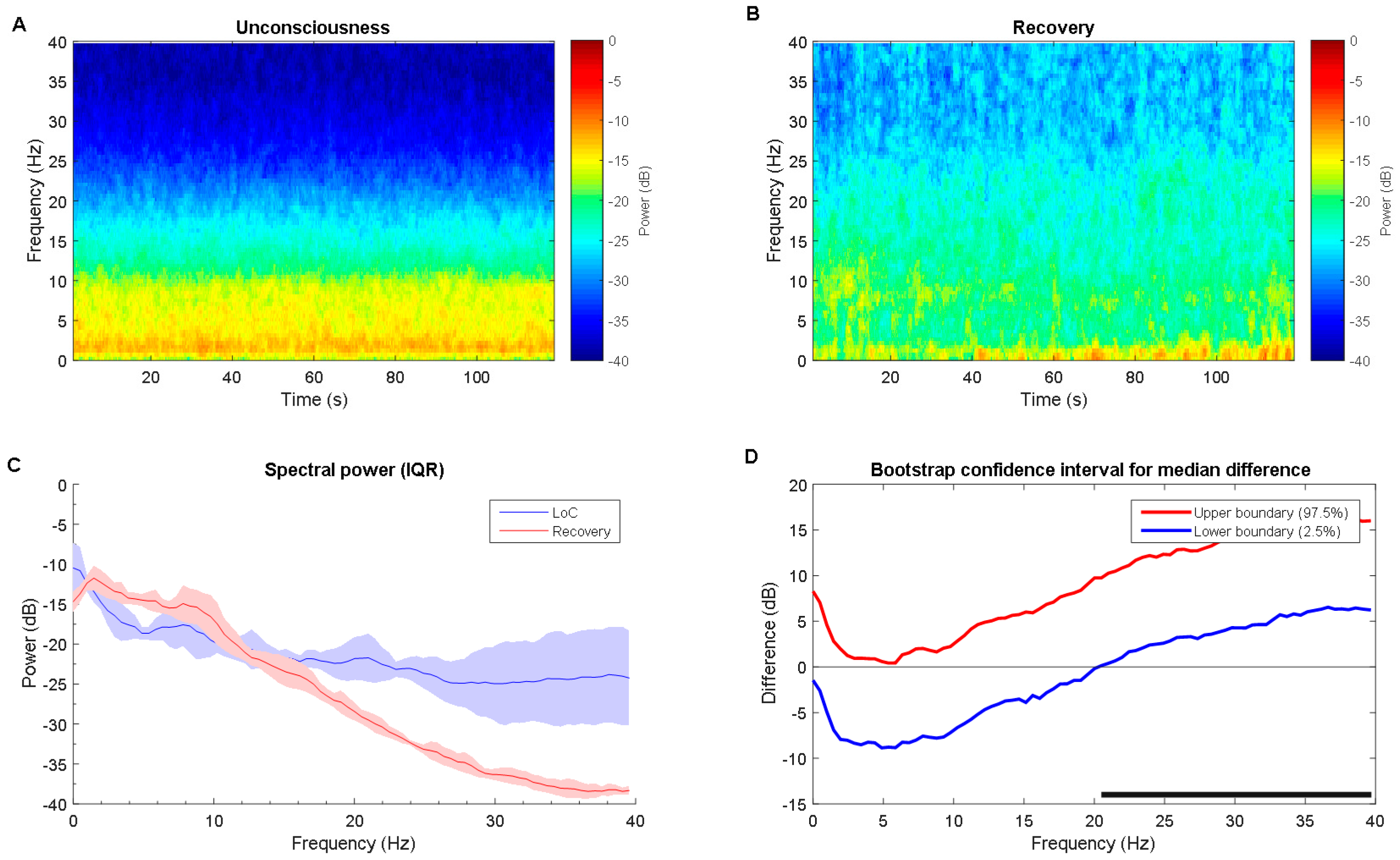
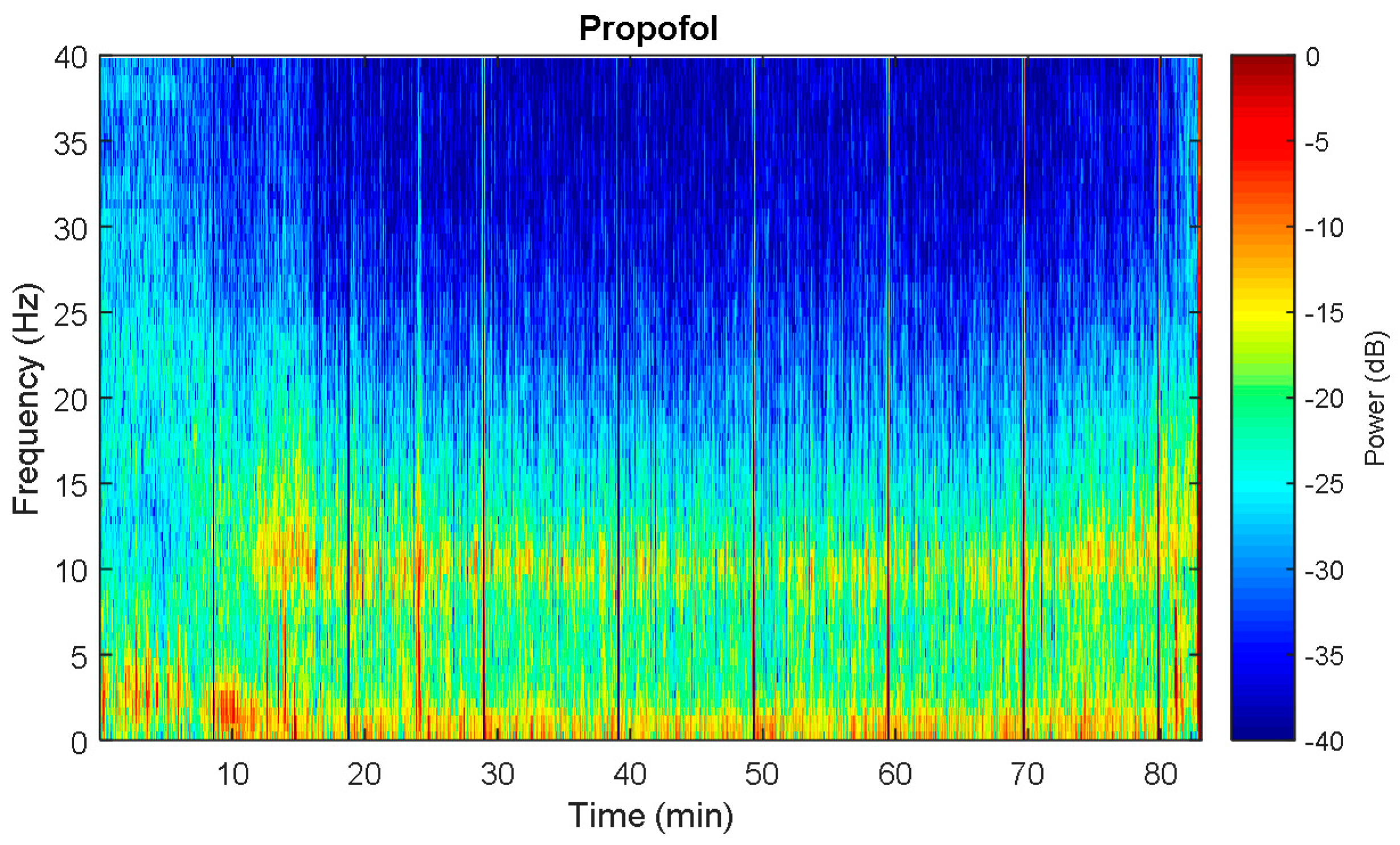
3.1. Propofol Power Spectral Comparisons across Brain States
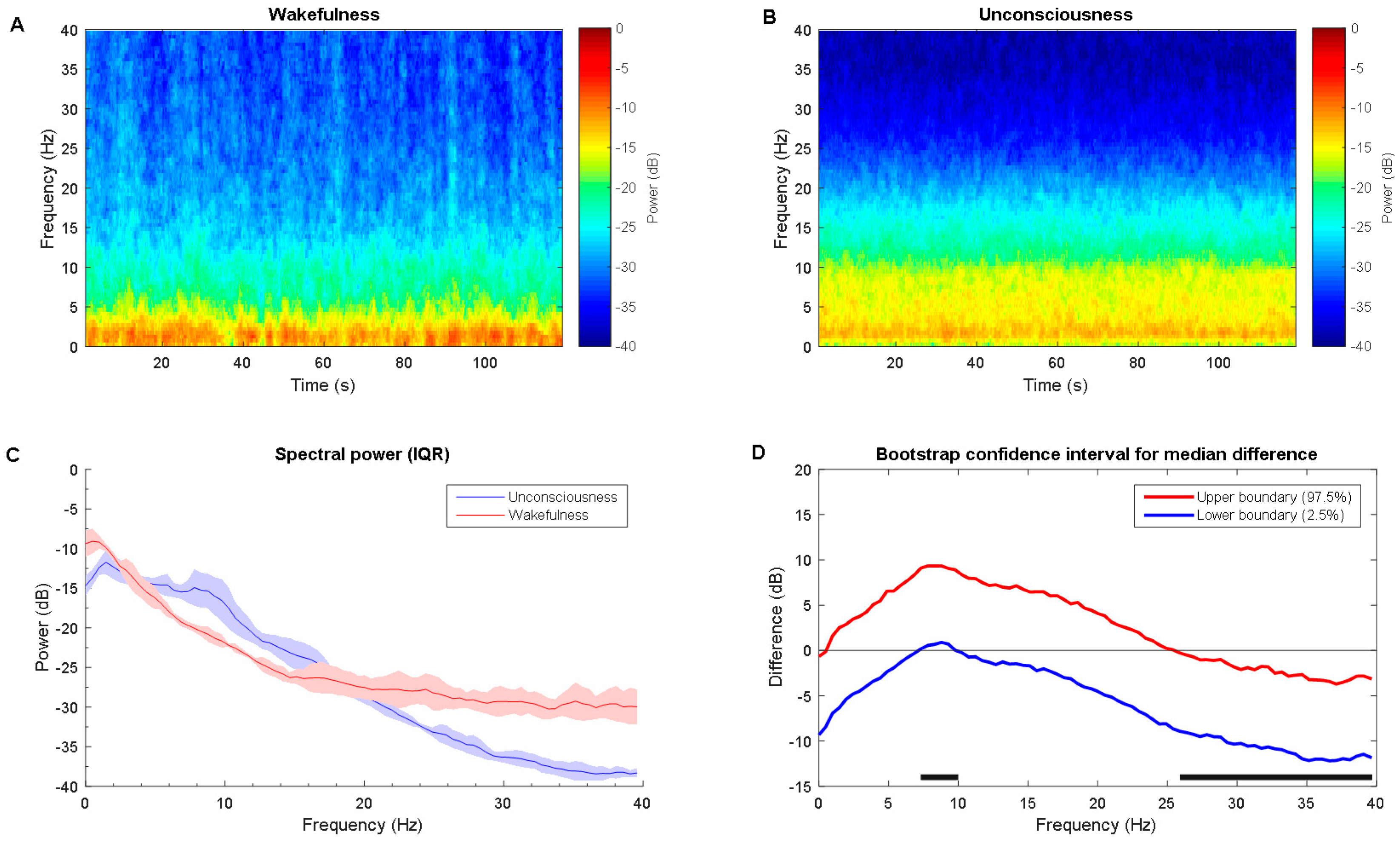
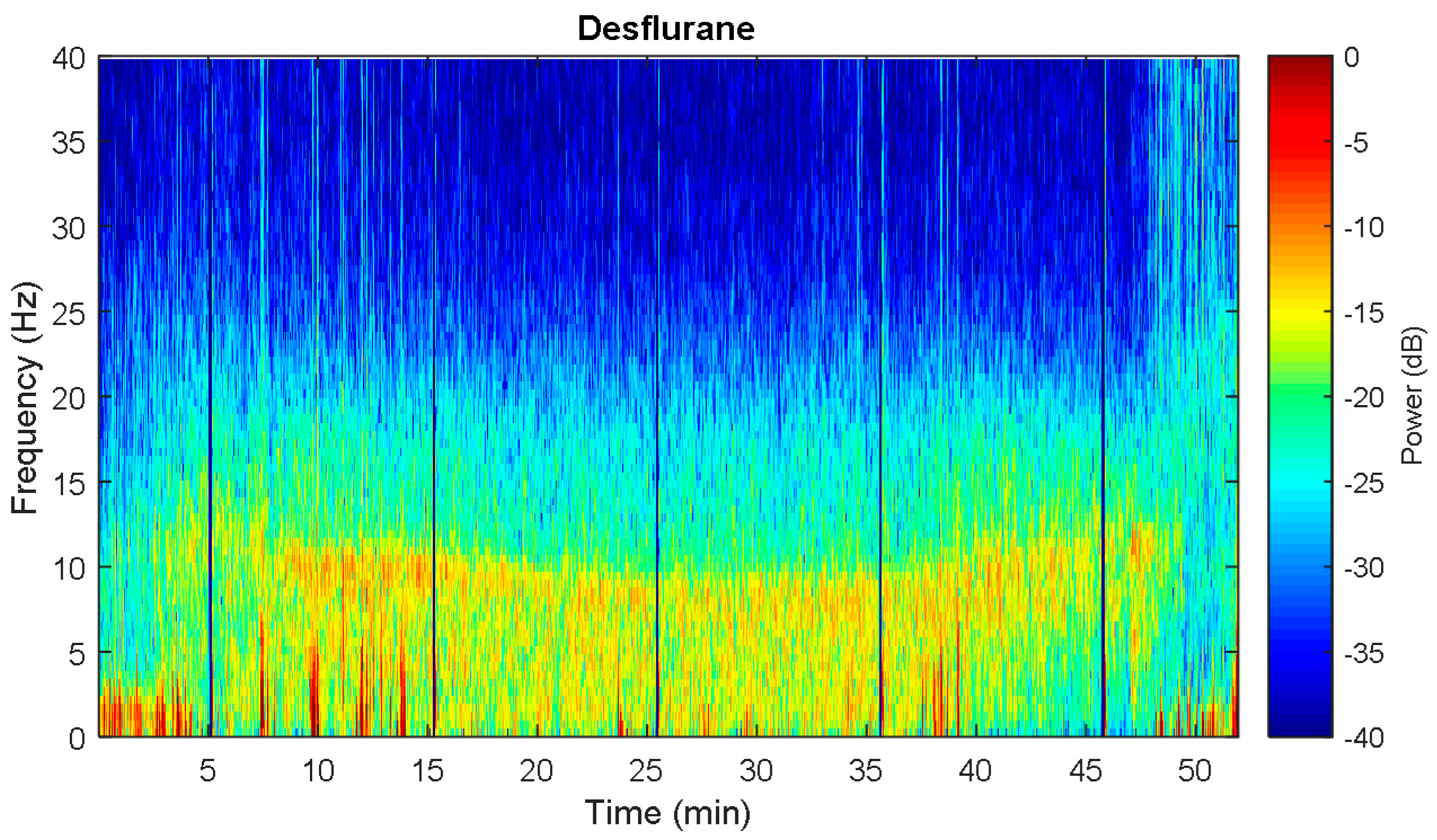
3.2. Desflurane Power Spectral Comparisons across Brain States
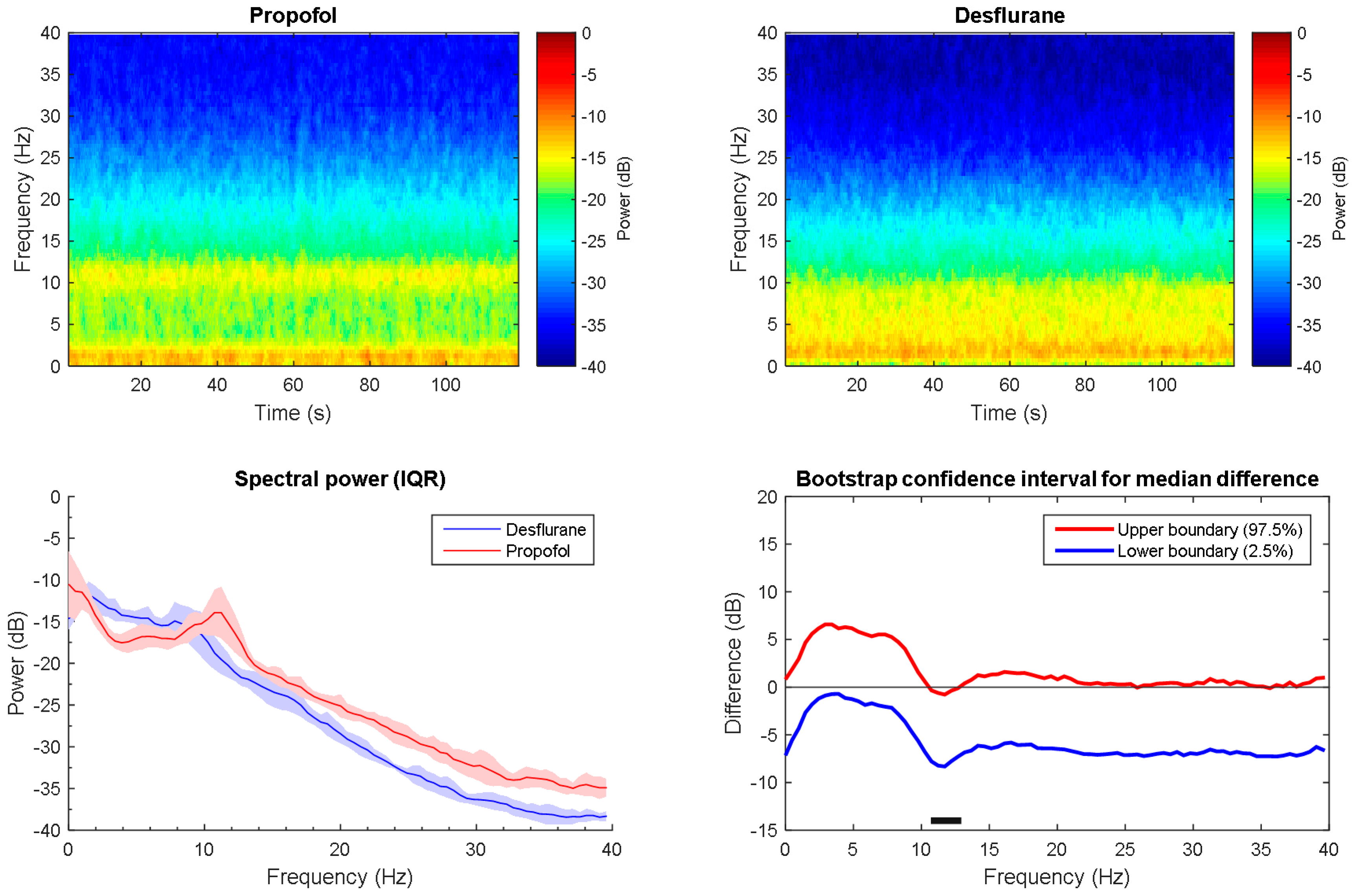
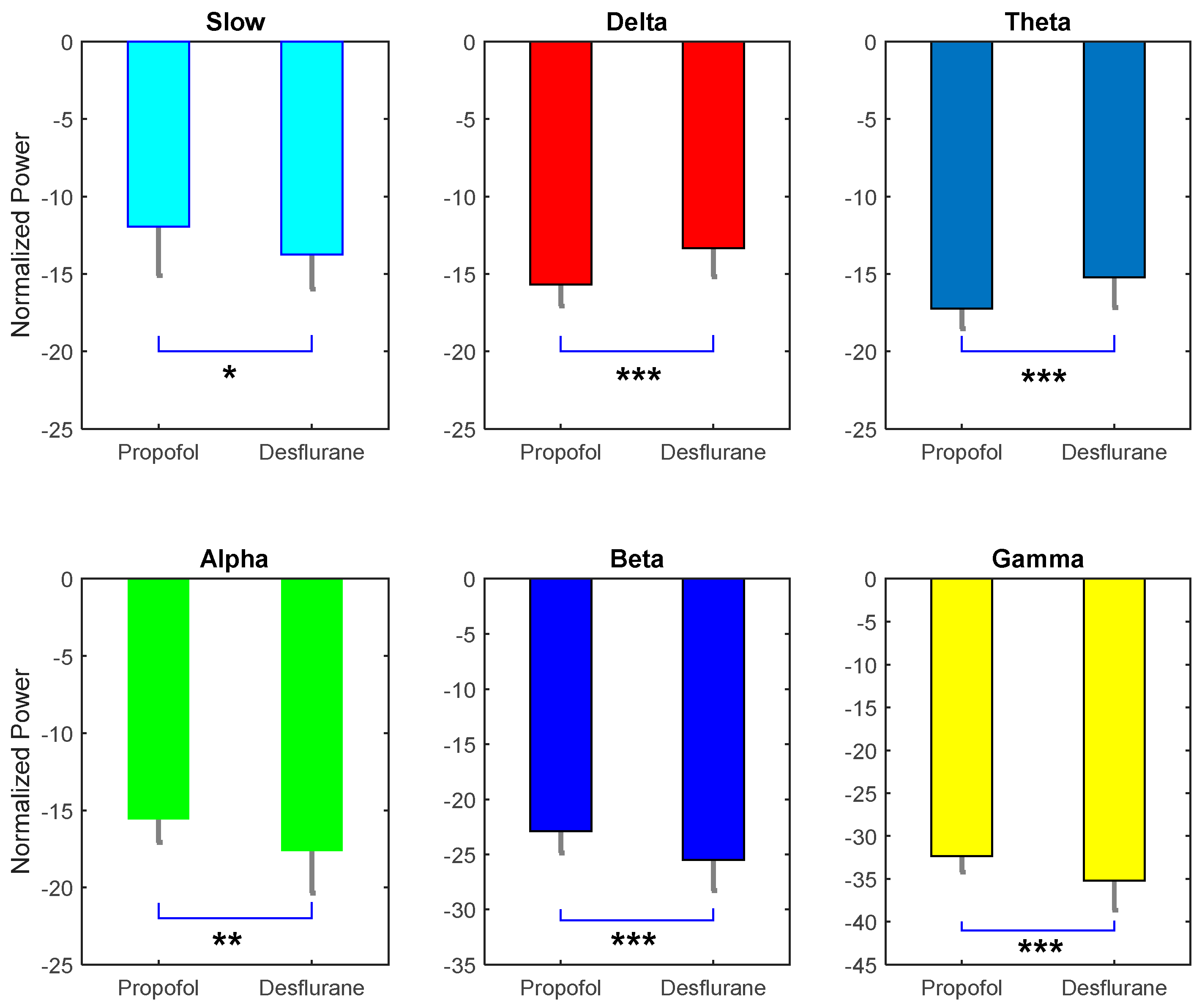
3.3. Propofol versus Desflurane Spectral Dynamics Analysis under Anesthesia
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Brown, E.N.; Lydic, R.; Schiff, N.D. General anesthesia, sleep, and coma. N. Engl. J. Med. 2010, 363, 2638–2650. [Google Scholar] [CrossRef] [PubMed]
- Hutt, A.; Hudetz, A.G. General anesthesia: From theory to experiments. Front. Syst. Neurosci. 2015, 9, 105. [Google Scholar] [CrossRef] [PubMed]
- Pal, D.; Silverstein, B.H.; Lee, H.; Mashour, G.A. Neural correlates of wakefulness, sleep, and general anesthesiaan experimental study in rat. Anesthesiology 2016, 125, 929–942. [Google Scholar] [CrossRef] [PubMed]
- Liu, Q.; Ma, L.; Chiu, R.-C.; Fan, S.-Z.; Abbod, M.F.; Shieh, J.-S. Hrv-derived data similarity and distribution index based on ensemble neural network for measuring depth of anaesthesia. PeerJ 2017, 5, e4067. [Google Scholar] [PubMed]
- Lepouse, C.; Lautner, C.; Liu, L.; Gomis, P.; Leon, A. Emergence delirium in adults in the post-anaesthesia care unit. Br. J. Anaesth. 2006, 96, 747–753. [Google Scholar] [CrossRef] [PubMed]
- Saczynski, J.S.; Marcantonio, E.R.; Quach, L.; Fong, T.G.; Gross, A.; Inouye, S.K.; Jones, R.N. Cognitive trajectories after postoperative delirium. N. Engl. J. Med. 2012, 367, 30–39. [Google Scholar] [CrossRef] [PubMed]
- Arbous, M.S.; Meursing, A.E.; van Kleef, J.W.; de Lange, J.J.; Spoormans, H.H.; Touw, P.; Werner, F.M.; Grobbee, D.E. Impact of anesthesia management characteristics on severe morbidity and mortality. Anesthesiology 2005, 102, 257–268. [Google Scholar] [CrossRef] [PubMed]
- Bainbridge, D.; Martin, J.; Arango, M.; Cheng, D.; Evidence-based Peri-operative Clinical Outcomes Research (EPiCOR) Group. Perioperative and anaesthetic-related mortality in developed and developing countries: A systematic review and meta-analysis. Lancet 2012, 380, 1075–1081. [Google Scholar] [CrossRef]
- Purdon, P.L.; Pierce, E.T.; Mukamel, E.A.; Prerau, M.J.; Walsh, J.L.; Wong, K.F.K.; Salazar-Gomez, A.F.; Harrell, P.G.; Sampson, A.L.; Cimenser, A. Electroencephalogram signatures of loss and recovery of consciousness from propofol. Proc. Natl. Acad. Sci. USA 2013, 110, E1142–E1151. [Google Scholar] [CrossRef] [PubMed]
- Supp, G.G.; Siegel, M.; Hipp, J.F.; Engel, A.K. Cortical hypersynchrony predicts breakdown of sensory processing during loss of consciousness. Curr. Biol. 2011, 21, 1988–1993. [Google Scholar] [CrossRef] [PubMed]
- Brown, E.N.; Purdon, P.L.; Van Dort, C.J. General anesthesia and altered states of arousal: A systems neuroscience analysis. Annu. Rev. Neurosci. 2011, 34, 601–628. [Google Scholar] [CrossRef] [PubMed]
- Ching, S.; Brown, E.N. Modeling the dynamical effects of anesthesia on brain circuits. Curr. Opin. Neurobiol. 2014, 25, 116–122. [Google Scholar] [CrossRef] [PubMed]
- Niedermeyer, E.; da Silva, F.L. Electroencephalography: Basic Principles, Clinical Applications, and Related Fields; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2005. [Google Scholar]
- Kandel, E.R.; Schwartz, J.H.; Jessell, T.M.; Siegelbaum, S.A.; Hudspeth, A.J. Principles of Neural Science; McGraw-Hill: New York, NY, USA, 2000; Volume 4. [Google Scholar]
- Ching, S.; Cimenser, A.; Purdon, P.L.; Brown, E.N.; Kopell, N.J. Thalamocortical model for a propofol-induced α-rhythm associated with loss of consciousness. Proc. Natl. Acad. Sci. USA 2010, 107, 22665–22670. [Google Scholar] [CrossRef] [PubMed]
- Avidan, M.S.; Zhang, L.; Burnside, B.A.; Finkel, K.J.; Searleman, A.C.; Selvidge, J.A.; Saager, L.; Turner, M.S.; Rao, S.; Bottros, M. Anesthesia awareness and the bispectral index. N. Engl. J. Med. 2008, 358, 1097–1108. [Google Scholar] [CrossRef] [PubMed]
- Huang, N.E.; Shen, Z.; Long, S.R.; Wu, M.C.; Shih, H.H.; Zheng, Q.; Yen, N.-C.; Tung, C.C.; Liu, H.H. The Empirical Mode Decomposition and the Hilbert Spectrum for Nonlinear and Non-Stationary Time Series Analysis. Proc. R. Soc. Lond. A 1998, 454, 903–995. [Google Scholar] [CrossRef]
- Gianfelici, F.; Biagetti, G.; Crippa, P.; Turchetti, C. Multicomponent am–fm representations: An asymptotically exact approach. IEEE Trans. Audio Speech Lang. Process. 2007, 15, 823–837. [Google Scholar] [CrossRef]
- Biagetti, G.; Crippa, P.; Curzi, A.; Orcioni, S.; Turchetti, C. Analysis of the emg signal during cyclic movements using multicomponent am–fm decomposition. IEEE J. Biomed. Health Inform. 2015, 19, 1672–1681. [Google Scholar] [CrossRef] [PubMed]
- Pei, S.-C.; Chang, K.-W. The mystery curve: A signal processing point of view [lecture notes]. IEEE Signal Process. Mag. 2017, 34, 158–163. [Google Scholar] [CrossRef]
- Cornelissen, L.; Kim, S.-E.; Purdon, P.L.; Brown, E.N.; Berde, C.B. Age-dependent electroencephalogram (EEG) patterns during sevoflurane general anesthesia in infants. eLife 2015, 4, e06513. [Google Scholar] [CrossRef] [PubMed]
- Rosow, C.; Manberg, P.J. Bispectral index monitoring. Anesthesiol. Clin. N. Am. 2001, 19, 947–966. [Google Scholar] [CrossRef]
- Viertiö-Oja, H.; Maja, V.; Särkelä, M.; Talja, P.; Tenkanen, N.; Tolvanen-Laakso, H.; Paloheimo, M.; Vakkuri, A.; Yli-Hankala, A.; Meriläinen, P. Description of the entropy™ algorithm as applied in the datex-ohmeda s/5™ entropy module. Acta Anaesthesiol. Scand. 2004, 48, 154–161. [Google Scholar] [CrossRef] [PubMed]
- Pavone, K.J.; Akeju, O.; Sampson, A.L.; Ling, K.; Purdon, P.L.; Brown, E.N. Nitrous oxide-induced slow and delta oscillations. Clin. Neurophys. 2016, 127, 556–564. [Google Scholar] [CrossRef] [PubMed]
- Uhrig, L.; Dehaene, S.; Jarraya, B. Cerebral Mechanisms of General Anesthesia. Ann. Fr. Anesth. Reanim. 2014, 33, 72–82. [Google Scholar] [CrossRef] [PubMed]
- Purdon, P.L.; Sampson, A.; Pavone, K.J.; Brown, E.N. Clinical electroencephalography for anesthesiologistspart I: Background and basic signatures. J. Am. Soc. Anesthesiol. 2015, 123, 937–960. [Google Scholar] [CrossRef] [PubMed]
- Kaur, A.; Jain, A.K.; Sehgal, R.; Sood, J. Hemodynamics and early recovery characteristics of desflurane versus sevoflurane in bariatric surgery. J. Anaesthesiol. Clin. Pharmacol. 2013, 29, 36. [Google Scholar] [CrossRef] [PubMed]
- Feshchenko, V.A.; Veselis, R.A.; Reinsel, R.A. Propofol-induced alpha rhythm. Neuropsychobiology 2004, 50, 257–266. [Google Scholar] [CrossRef] [PubMed]
- Bokil, H.; Andrews, P.; Kulkarni, J.E.; Mehta, S.; Mitra, P.P. Chronux: A platform for analyzing neural signals. J. Neurosci. Methods 2010, 192, 146–151. [Google Scholar] [CrossRef] [PubMed]
- Akeju, O.; Westover, M.B.; Pavone, K.J.; Sampson, A.L.; Hartnack, K.E.; Brown, E.N.; Purdon, P.L. Effects of sevoflurane and propofol on frontal electroencephalogram power and coherence. J. Am. Soc. Anesthesiol. 2014, 121, 990–998. [Google Scholar] [CrossRef] [PubMed]
- Akeju, O.; Pavone, K.J.; Westover, M.B.; Vazquez, R.; Prerau, M.J.; Harrell, P.G.; Hartnack, K.E.; Rhee, J.; Sampson, A.L.; Habeeb, K. A comparison of propofol-and dexmedetomidine-induced electroencephalogram dynamics using spectral and coherence analysis. J. Am. Soc. Anesthesiol. 2014, 121, 978–989. [Google Scholar] [CrossRef] [PubMed]
- Neske, G.T. The slow oscillation in cortical and thalamic networks: Mechanisms and functions. Front. Neural Circ. 2016, 9, 88. [Google Scholar] [CrossRef] [PubMed]
- Franks, N.P. General anaesthesia: From molecular targets to neuronal pathways of sleep and arousal. Nat. Rev. Neurosci. 2008, 9, 370–386. [Google Scholar] [CrossRef] [PubMed]
- Akeju, O.; Song, A.H.; Hamilos, A.E.; Pavone, K.J.; Flores, F.J.; Brown, E.N.; Purdon, P.L. Electroencephalogram signatures of ketamine anesthesia-induced unconsciousness. Clin. Neurophysiol. 2016, 127, 2414–2422. [Google Scholar] [CrossRef] [PubMed]
- Poorun, R.; Hartley, C.; Goksan, S.; Worley, A.; Boyd, S.; Cornelissen, L.; Berde, C.; Rogers, R.; Ali, T.; Slater, R. Electroencephalography during general anaesthesia differs between term-born and premature-born children. Clin. Neurophysiol. 2016, 127, 1216–1222. [Google Scholar] [CrossRef] [PubMed]
- Chennu, S.; O’Connor, S.; Adapa, R.; Menon, D.K.; Bekinschtein, T.A. Brain connectivity dissociates responsiveness from drug exposure during propofol-induced transitions of consciousness. PLoS Comput. Biol. 2016, 12, e1004669. [Google Scholar] [CrossRef] [PubMed]
- Akeju, O.; Kim, S.-E.; Vazquez, R.; Rhee, J.; Pavone, K.J.; Hobbs, L.E.; Purdon, P.L.; Brown, E.N. Spatiotemporal dynamics of dexmedetomidine-induced electroencephalogram oscillations. PLoS ONE 2016, 11, e0163431. [Google Scholar] [CrossRef] [PubMed]
- Blain-Moraes, S.; Tarnal, V.; Vanini, G.; Bel-Behar, T.; Janke, E.; Picton, P.; Golmirzaie, G.; Palanca, B.J.; Avidan, M.S.; Kelz, M.B. Network efficiency and posterior alpha patterns are markers of recovery from general anesthesia: A high-density electroencephalography study in healthy volunteers. Front. Hum. Neurosci. 2017, 11, 328. [Google Scholar] [CrossRef] [PubMed]
- Murphy, M.; Bruno, M.-A.; Riedner, B.A.; Boveroux, P.; Noirhomme, Q.; Landsness, E.C.; Brichant, J.-F.; Phillips, C.; Massimini, M.; Laureys, S. Propofol anesthesia and sleep: A high-density EEG study. Sleep 2011, 34, 283–291. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Propofol (n = 28) | Desflurane (n = 23) | |
|---|---|---|
| Age (yr), mean (±SD) | 50.1 (15.0) | 50.7 (12.7) |
| Sex (male), n (%) | 10 (35.7%) | 7 (30.4%) |
| Weight (kg), mean (±SD) | 57.7 (9.7) | 58.5 (11.0) |
| Height (cm), mean (±SD) | 160.1 (7.4) | 162.0 (9.4) |
| BMI (kg/m2), mean (±SD) | 22.5 (3.1) | 22.2 (3.6) |
| Responsiveness | Level |
|---|---|
| Responds readily to name spoken in normal tone | 5 |
| Lethargic response to name spoken in normal tone | 4 |
| Responds only after name is called loudly and/or repeatedly | 3 |
| Responds only after mild prodding or shaking | 2 |
| Responds only after painful trapezius squeeze | 1 |
| Does not respond to painful trapezius squeeze | 0 |
| Frequency Band | Frequency Range (Hz) |
|---|---|
| Slow | <1 |
| Delta | 1–4 |
| Theta | 5–8 |
| Alpha | 9–12 |
| Beta | 13–25 |
| Gamma | 26–40 1 |
| Band | Wakefulness Mean (SD) | Unconsciousness Mean (SD) |
|---|---|---|
| Slow | −11.0 (2.3) | −11.9 (3.2) |
| Delta | −12.2 (1.3) | −15.7 (1.4) |
| Theta | −18.4 (1.6) | −17.2 (1.3) |
| Alpha | −23.1 (2.1) | −15.6 (1.5) |
| Beta | −27.7 (2.7) | −22.8 (1.9) |
| Gamma | −29.4 (4.0) | −32.3 (1.8) |
| Band | Wakefulness Mean (SD) | Unconsciousness Mean (SD) |
|---|---|---|
| Slow | −9.7 (2.2) | −13.7 (2.2) |
| Delta | −12.7 (1.4) | −13.3 (1.8) |
| Theta | −18.3 (1.6) | −15.2 (1.9) |
| Alpha | −21.8 (1.5) | −17.6 (2.7) |
| Beta | −26.4 (1.9) | −25.5 (2.8) |
| Gamma | −29.2 (3.1) | −35.2 (3.4) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, Q.; Ma, L.; Fan, S.-Z.; Abbod, M.F.; Shieh, J.-S. Electroencephalogram Similarity Analysis Using Temporal and Spectral Dynamics Analysis for Propofol and Desflurane Induced Unconsciousness. Symmetry 2018, 10, 15. https://doi.org/10.3390/sym10010015
Liu Q, Ma L, Fan S-Z, Abbod MF, Shieh J-S. Electroencephalogram Similarity Analysis Using Temporal and Spectral Dynamics Analysis for Propofol and Desflurane Induced Unconsciousness. Symmetry. 2018; 10(1):15. https://doi.org/10.3390/sym10010015
Chicago/Turabian StyleLiu, Quan, Li Ma, Shou-Zen Fan, Maysam F. Abbod, and Jiann-Shing Shieh. 2018. "Electroencephalogram Similarity Analysis Using Temporal and Spectral Dynamics Analysis for Propofol and Desflurane Induced Unconsciousness" Symmetry 10, no. 1: 15. https://doi.org/10.3390/sym10010015
APA StyleLiu, Q., Ma, L., Fan, S.-Z., Abbod, M. F., & Shieh, J.-S. (2018). Electroencephalogram Similarity Analysis Using Temporal and Spectral Dynamics Analysis for Propofol and Desflurane Induced Unconsciousness. Symmetry, 10(1), 15. https://doi.org/10.3390/sym10010015