
Quantifying the UK Online Interest in Substances of the EU Watchlist for Water Monitoring: Diclofenac, Estradiol, and the Macrolide Antibiotics




Abstract
:1. Introduction
2. Data and Method
3. Results
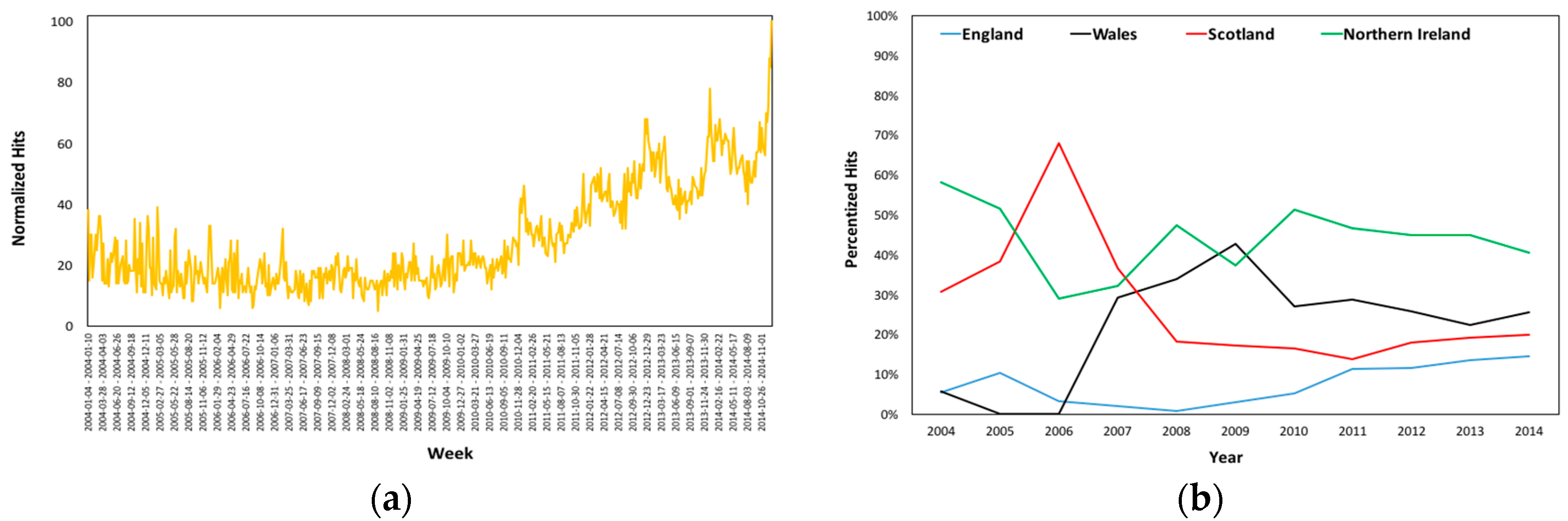
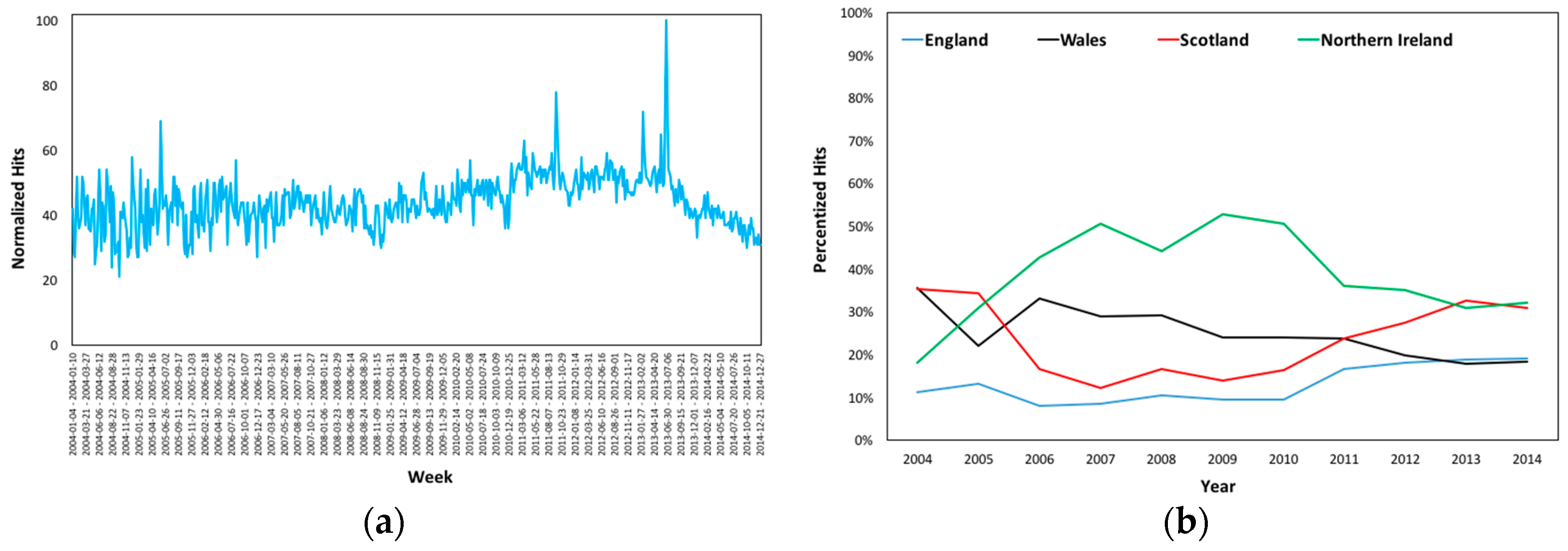
3.1. Worldwide and UK’s Online Interest
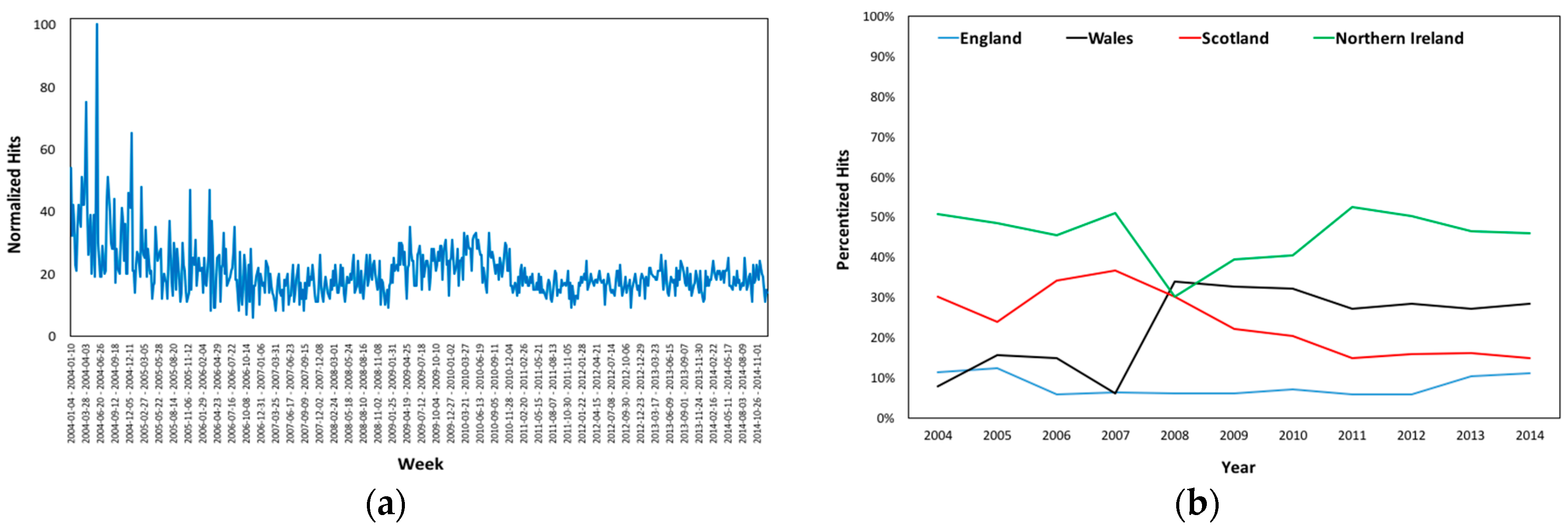
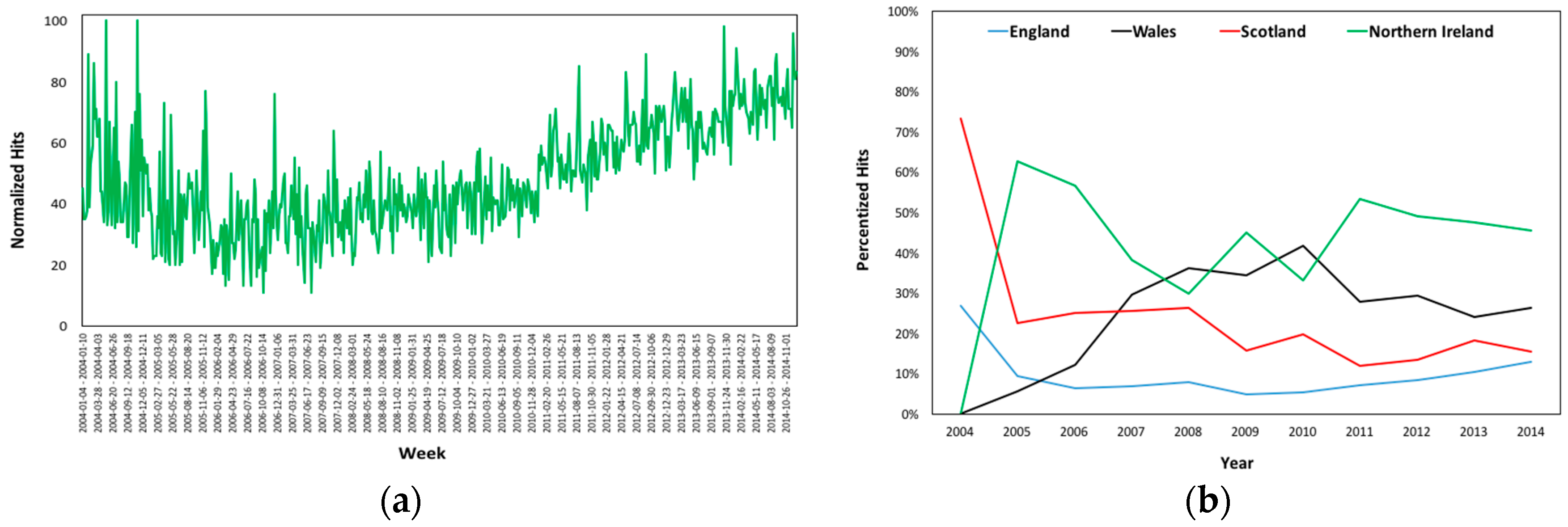
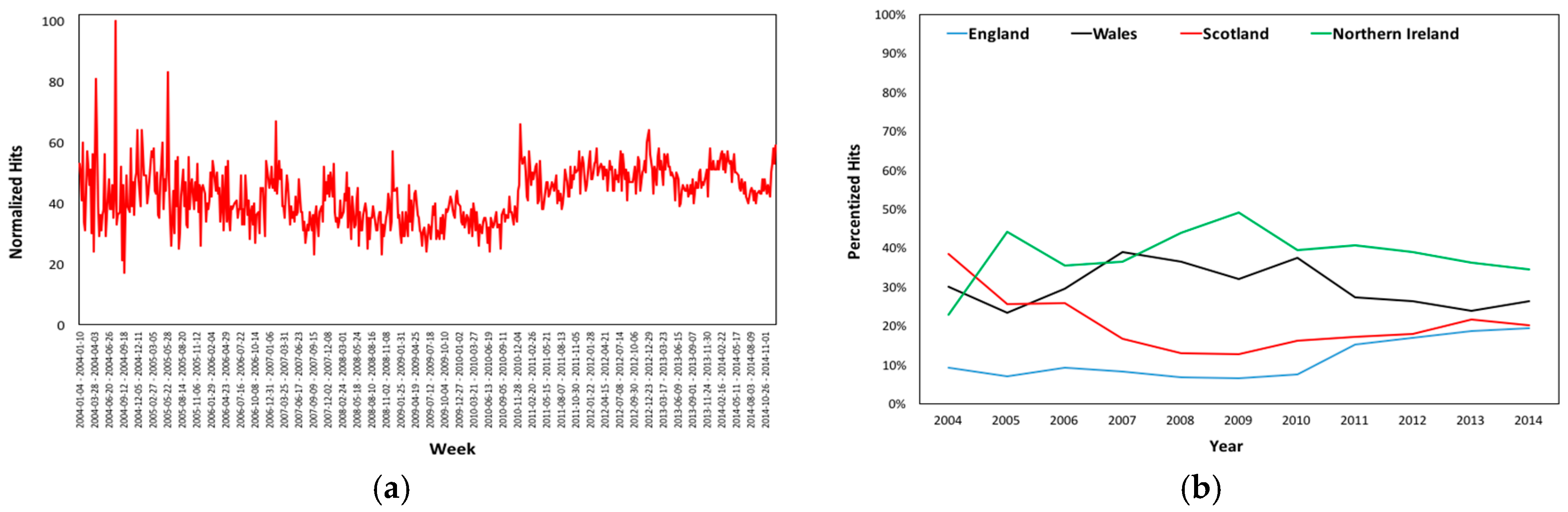
3.2. Regional Online Interest
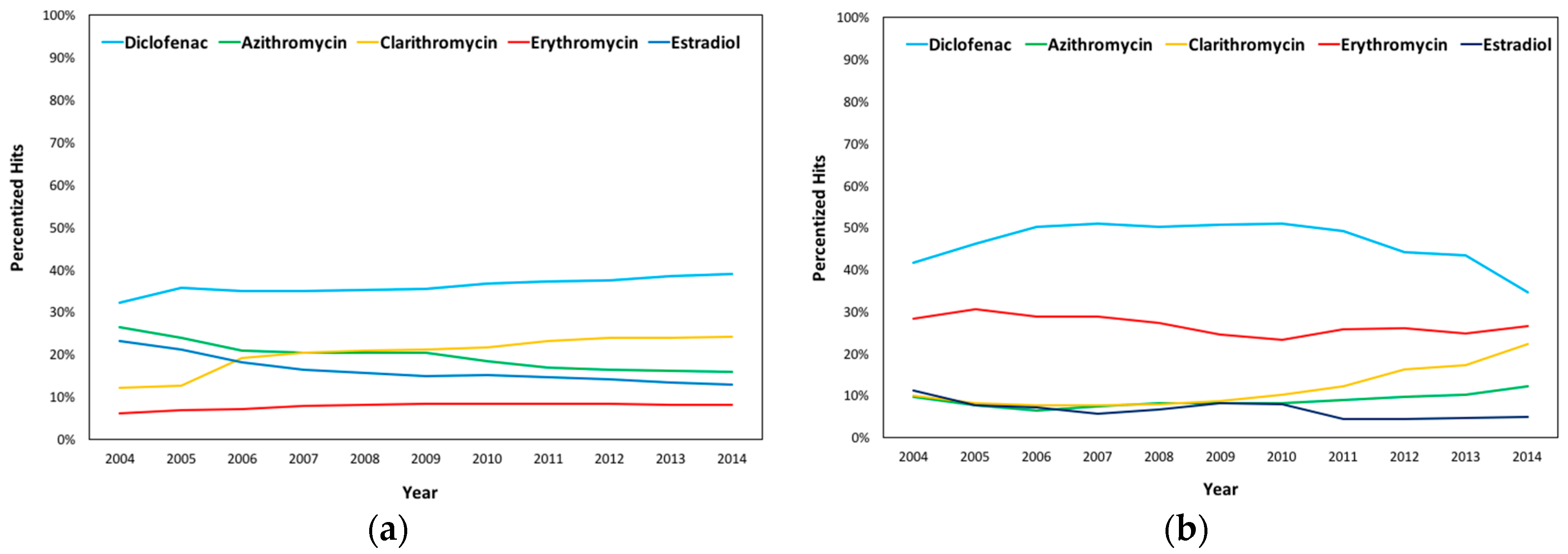
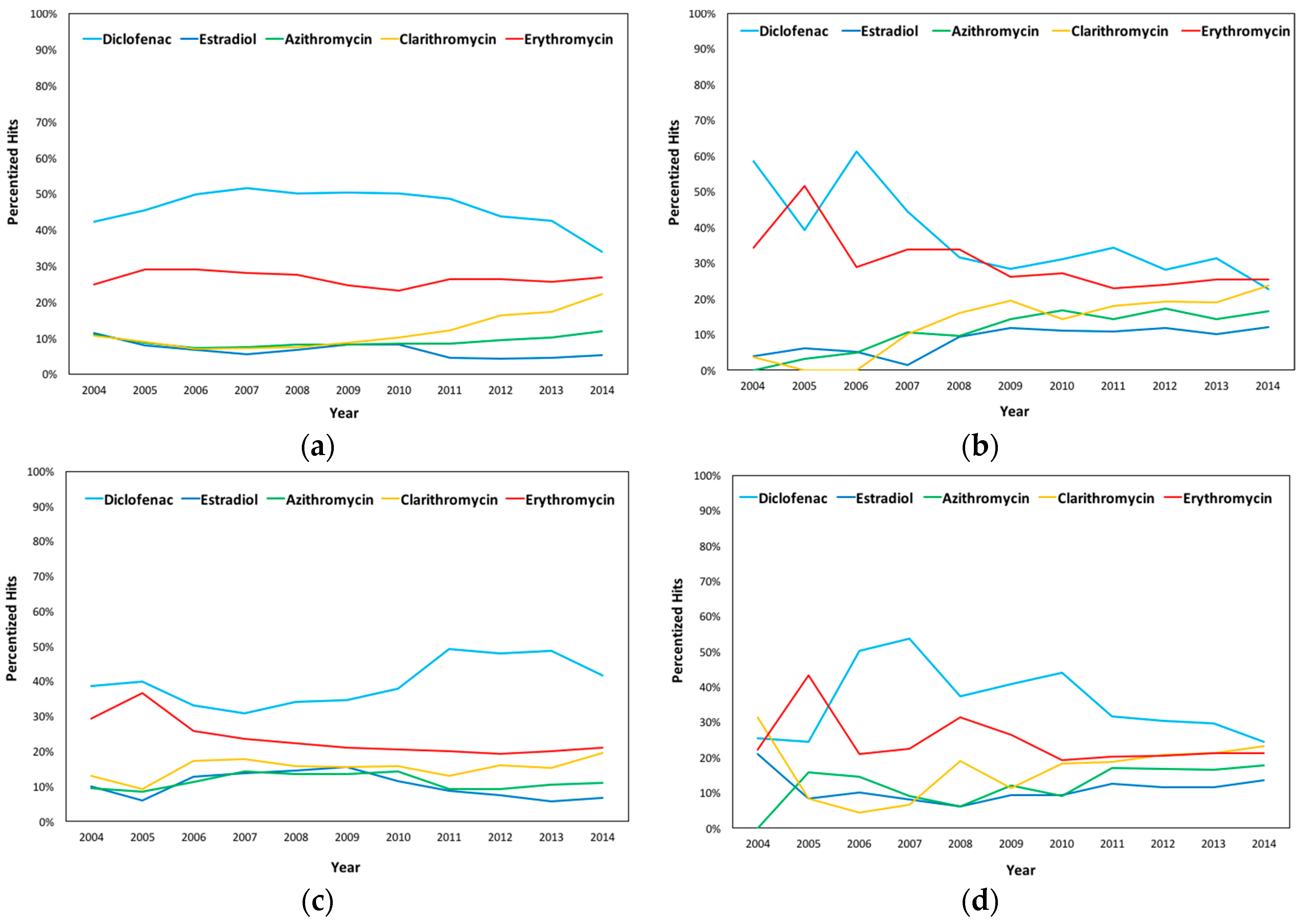
3.3. Online Interest by Substance
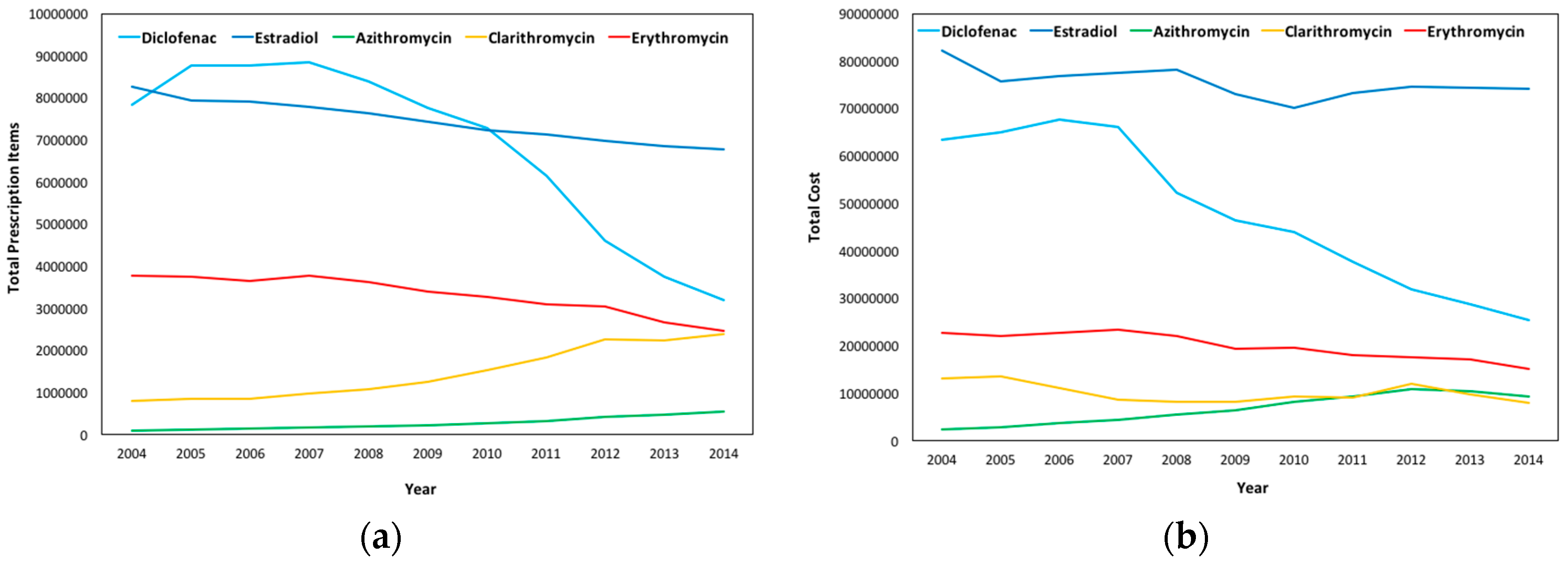
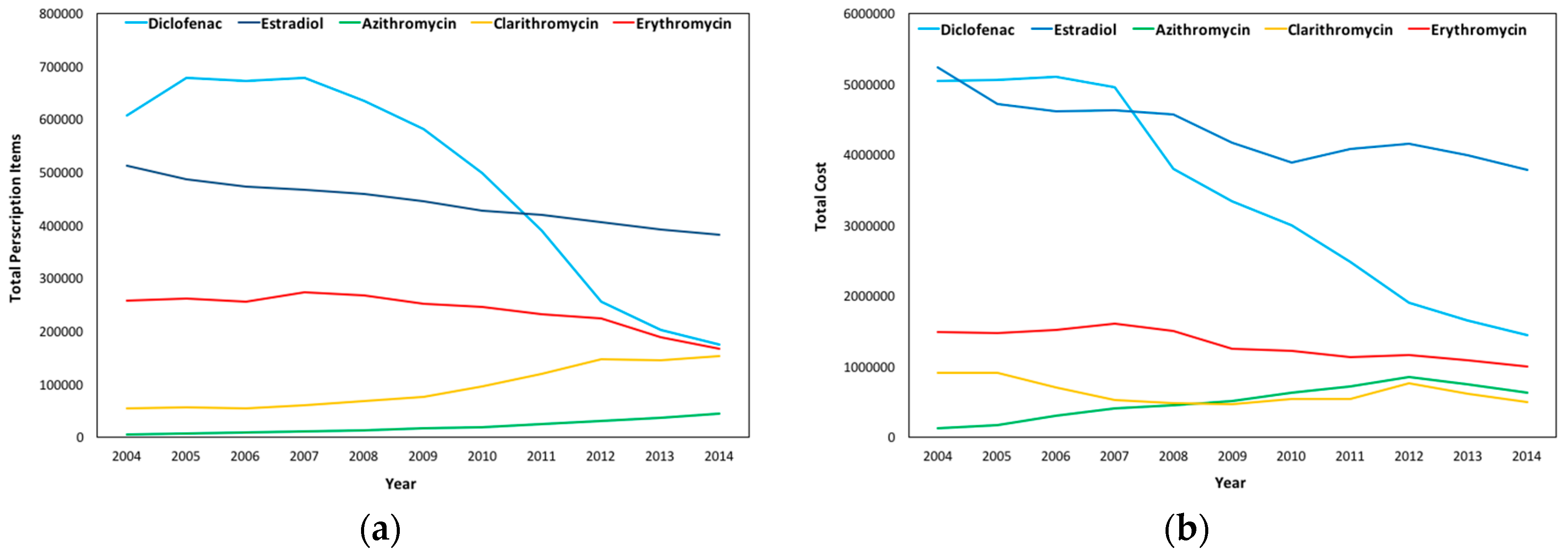
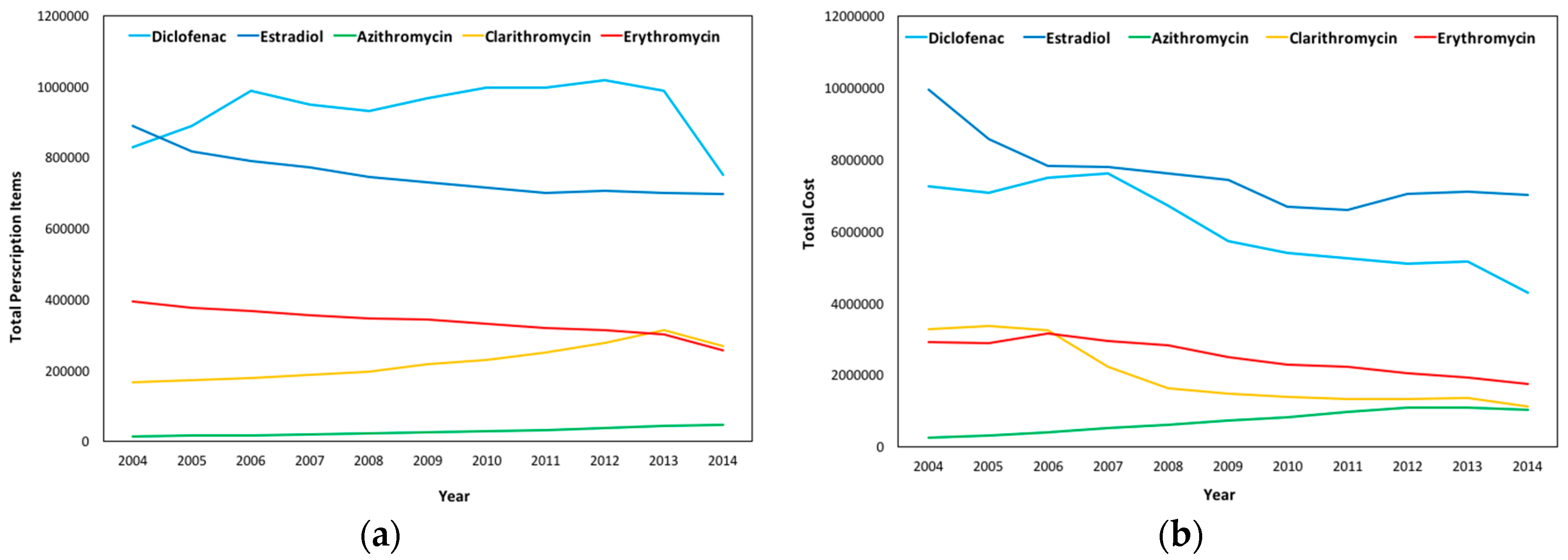
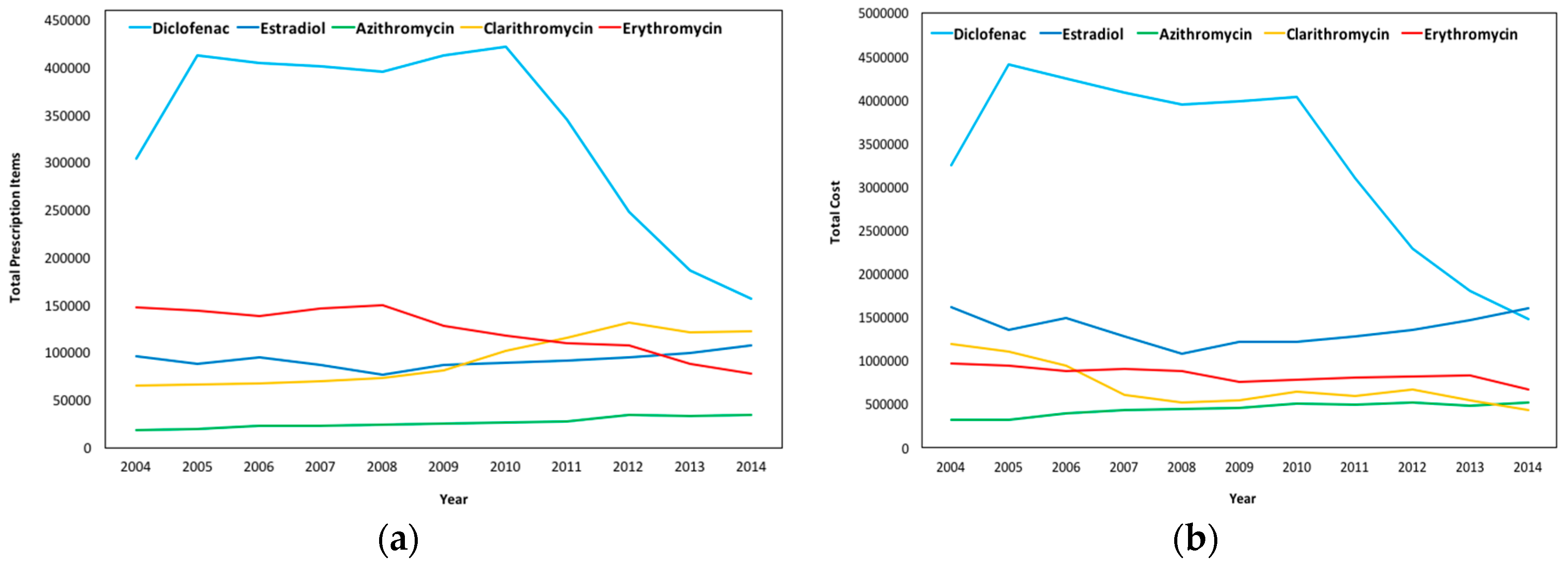
3.4. Total Prescriptions and Costs per Substance
3.5. Research Interest
3.6. Correlations amongst Prescription, Google Hits, and Scientific Papers
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Year | England | Wales | ||||||||
| D | ES | A | C | E | D | ES | A | C | E | |
| 2004 | 42.22% | 11.40% | 10.99% | 10.61% | 24.78% | 58.46% | 3.73% | 0.00% | 3.62% | 34.19% |
| 2005 | 45.53% | 8.03% | 8.67% | 8.82% | 28.95% | 39.26% | 6.03% | 3.09% | 0.00% | 51.62% |
| 2006 | 49.84% | 6.84% | 7.20% | 7.07% | 29.06% | 61.19% | 5.06% | 4.88% | 0.00% | 28.86% |
| 2007 | 51.67% | 5.57% | 7.52% | 7.09% | 28.15% | 44.28% | 1.48% | 10.53% | 10.04% | 33.66% |
| 2008 | 50.09% | 6.68% | 8.19% | 7.55% | 27.49% | 31.47% | 9.21% | 9.51% | 16.08% | 33.74% |
| 2009 | 50.32% | 8.12% | 8.25% | 8.77% | 24.55% | 28.42% | 11.74% | 14.11% | 19.53% | 26.20% |
| 2010 | 50.21% | 8.27% | 8.37% | 10.05% | 23.09% | 30.93% | 10.92% | 16.72% | 14.35% | 27.08% |
| 2011 | 48.70% | 4.48% | 8.54% | 12.00% | 26.28% | 34.21% | 10.85% | 14.30% | 17.88% | 22.77% |
| 2012 | 43.78% | 4.30% | 9.49% | 16.18% | 26.26% | 28.09% | 11.70% | 17.30% | 19.12% | 23.80% |
| 2013 | 42.44% | 4.58% | 10.22% | 17.15% | 25.61% | 31.36% | 10.04% | 14.34% | 19.00% | 25.27% |
| 2014 | 33.93% | 5.16% | 11.84% | 22.17% | 26.90% | 22.53% | 12.12% | 16.55% | 23.55% | 25.26% |
| Year | Scotland | Northern Ireland | ||||||||
| D | ES | A | C | E | D | ES | A | C | E | |
| 2004 | 38.55% | 9.88% | 9.32% | 12.91% | 29.34% | 25.36% | 20.93% | 0.00% | 31.46% | 22.25% |
| 2005 | 40.00% | 5.84% | 8.32% | 9.26% | 36.58% | 24.53% | 8.26% | 15.78% | 8.26% | 43.17% |
| 2006 | 33.02% | 12.69% | 11.26% | 17.21% | 25.82% | 50.27% | 10.11% | 14.55% | 4.23% | 20.83% |
| 2007 | 30.86% | 13.78% | 14.13% | 17.78% | 23.45% | 53.65% | 8.12% | 9.07% | 6.63% | 22.53% |
| 2008 | 34.00% | 14.39% | 13.50% | 15.72% | 22.39% | 37.28% | 6.20% | 6.20% | 19.02% | 31.29% |
| 2009 | 34.53% | 15.47% | 13.52% | 15.44% | 21.05% | 40.78% | 9.41% | 12.11% | 11.25% | 26.45% |
| 2010 | 37.93% | 11.42% | 14.34% | 15.80% | 20.51% | 43.88% | 9.33% | 9.16% | 18.33% | 19.29% |
| 2011 | 49.15% | 8.73% | 9.15% | 13.00% | 19.97% | 31.57% | 12.58% | 17.00% | 18.65% | 20.21% |
| 2012 | 47.97% | 7.56% | 9.21% | 16.02% | 19.25% | 30.48% | 11.52% | 16.67% | 20.76% | 20.57% |
| 2013 | 48.72% | 5.64% | 10.34% | 15.33% | 19.97% | 29.65% | 11.51% | 16.51% | 21.16% | 21.16% |
| 2014 | 41.52% | 6.75% | 11.07% | 19.57% | 21.10% | 24.47% | 13.43% | 17.82% | 23.21% | 21.08% |
Appendix B
| Year | Diclofenac | Estradiol | Azithromycin | Clarithromycin | Erythromycin | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Pxs | Nic | Pxs | Nic | Pxs | Nic | Pxs | Nic | Pxs | Nic | |
| 2004 | 7,835,083 | 63,478,356 | 8,251,847 | 82,173,534 | 103,963 | 2,362,482 | 795,270 | 13,225,502 | 3,766,953 | 22,679,369 |
| 2005 | 8,766,625 | 65,041,774 | 7,941,468 | 75,777,693 | 123,291 | 2,939,084 | 852,806 | 13,603,648 | 3,748,994 | 21,987,699 |
| 2006 | 8,764,671 | 67,572,195 | 7,899,767 | 76,832,218 | 139,963 | 3,652,018 | 853,852 | 11,156,286 | 3,646,943 | 22,700,296 |
| 2007 | 8,851,377 | 66,137,104 | 7,772,486 | 77,574,221 | 164,441 | 4,498,897 | 973,997 | 8,723,270 | 3,763,697 | 23,421,676 |
| 2008 | 8,388,693 | 52,224,959 | 7,642,773 | 78,099,605 | 191,842 | 5,446,935 | 1,077,097 | 8,294,989 | 3,630,628 | 22,108,822 |
| 2009 | 7,748,234 | 46,427,799 | 7,434,276 | 72,950,292 | 225,109 | 6,456,947 | 1,257,967 | 8,242,025 | 3,395,881 | 19,482,448 |
| 2010 | 7,271,070 | 43,885,658 | 7,215,934 | 70,045,022 | 274,706 | 8,203,889 | 1,541,129 | 9,352,900 | 3,279,767 | 19,505,861 |
| 2011 | 6,145,755 | 37,721,617 | 7,129,956 | 73,214,245 | 326,009 | 9,429,128 | 1,823,774 | 9,077,182 | 3,098,773 | 17,956,893 |
| 2012 | 4,595,666 | 31,811,877 | 6,983,092 | 74,604,834 | 410,781 | 10,998,016 | 2,258,788 | 12,040,359 | 3,050,915 | 17,696,503 |
| 2013 | 3,742,673 | 28,798,913 | 6,841,917 | 74,364,235 | 476,529 | 10,369,500 | 2,245,430 | 9,833,664 | 2,673,169 | 17,052,495 |
| 2014 | 3,191,910 | 25,334,219 | 6,767,640 | 74,071,656 | 543,986 | 9,296,368 | 2,397,752 | 8,030,665 | 2,451,888 | 15,181,583 |
| Year | Diclofenac | Estradiol | Azithromycin | Clarithromycin | Erythromycin | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Pxs | Nic | Pxs | Nic | Pxs | Nic | Pxs | Nic | Pxs | Nic | |
| 2004 | 607,248 | 5,042,779 | 511,028 | 5,236,612 | 4568 | 117,091 | 53,652 | 903,849 | 256,824 | 1,481,228 |
| 2005 | 678,484 | 5,046,112 | 485,694 | 4,716,870 | 5699 | 172,899 | 55,902 | 900,822 | 261,533 | 1,469,651 |
| 2006 | 671,812 | 5,093,644 | 472,642 | 4,613,931 | 7941 | 294,818 | 53,439 | 698,619 | 255,790 | 1,519,369 |
| 2007 | 678,105 | 1,067,870 | 466,309 | 4,617,357 | 10,364 | 398,855 | 60,221 | 521,634 | 272,313 | 1,600,360 |
| 2008 | 635,085 | 3,793,644 | 459,422 | 4,569,660 | 12,630 | 455,641 | 67,349 | 478,072 | 266,925 | 1,504,670 |
| 2009 | 580,770 | 3,338,177 | 443,828 | 4,163,532 | 15,805 | 511,380 | 75,638 | 460,939 | 251,236 | 1,249,129 |
| 2010 | 498,367 | 2,989,491 | 427,581 | 3,883,315 | 19,028 | 620,973 | 94,390 | 530,313 | 245,055 | 1,215,885 |
| 2011 | 388,495 | 2,472,713 | 419,273 | 4,080,473 | 24,305 | 719,482 | 119,245 | 539,206 | 230,841 | 1,133,924 |
| 2012 | 254,997 | 1,901,062 | 404,993 | 4,145,176 | 30,320 | 843,584 | 146,134 | 764,544 | 222,667 | 1,159,973 |
| 2013 | 201,798 | 1,647,361 | 390,974 | 3,984,881 | 36,997 | 743,283 | 145,506 | 610,597 | 188,956 | 1,092,414 |
| 2014 | 173,686 | 1,440,695 | 381,413 | 3,781,056 | 44,190 | 633,734 | 153,445 | 495,161 | 166,866 | 994,933 |
| Year | Diclofenac | Estradiol | Azithromycin | Clarithromycin | Erythromycin | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Pxs | Nic | Pxs | Nic | Pxs | Nic | Pxs | Nic | Pxs | Nic | |
| 2004 | 828,315 | 7,240,001 | 888,889 | 9,945,074 | 13,510 | 251,295 | 165,909 | 3,276,480 | 392,270 | 2,895,902 |
| 2005 | 888,239 | 7,064,040 | 816,091 | 8,562,827 | 14,625 | 295,412 | 170,758 | 3,369,381 | 375,763 | 2,872,755 |
| 2006 | 988,181 | 7,488,552 | 790,058 | 7,825,990 | 16,726 | 388,981 | 177,455 | 3,229,276 | 366,113 | 3,149,333 |
| 2007 | 947,237 | 7,598,272 | 769,913 | 7,790,662 | 19,231 | 512,789 | 186,086 | 2,234,031 | 355,662 | 2,932,906 |
| 2008 | 930,227 | 6,706,394 | 743,438 | 7,590,806 | 21,053 | 595,080 | 197,300 | 1,621,024 | 346,642 | 2,821,866 |
| 2009 | 966,564 | 5,709,160 | 729,726 | 7,412,799 | 25,109 | 729,715 | 215,696 | 1,483,031 | 341,418 | 2,483,633 |
| 2010 | 996,611 | 5,400,387 | 712,913 | 6,688,184 | 28,035 | 818,739 | 229,736 | 1,371,893 | 329,611 | 2,278,828 |
| 2011 | 996,967 | 5,231,754 | 698,473 | 6,582,956 | 31,215 | 956,196 | 250,527 | 1,336,948 | 317,831 | 2,223,376 |
| 2012 | 1,016,319 | 5,097,518 | 705,705 | 7,048,774 | 36,229 | 1,098,991 | 275,497 | 1,330,449 | 313,722 | 2,041,729 |
| 2013 | 986,949 | 5,156,256 | 700,361 | 7,092,274 | 41,638 | 1,090,442 | 313,086 | 1,341,904 | 301,406 | 1,937,615 |
| 2014 | 750,888 | 4,298,521 | 694,916 | 7,011,775 | 44,818 | 1,039,360 | 266,637 | 1,121,077 | 255,645 | 1,736,324 |
| Year | Diclofenac | Estradiol | Azithromycin | Clarithromycin | Erythromycin | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Pxs | Nic | Pxs | Nic | Pxs | Nic | Pxs | Nic | Pxs | Nic | |
| 2004 | 303,754 | 3,243,777 | 96,509 | 1,617,714 | 18,353 | 321,834 | 65,089 | 1,197,697 | 147,641 | 969,240 |
| 2005 | 412,903 | 4,402,937 | 88,408 | 1,351,945 | 19,548 | 321,170 | 66,880 | 1,107,689 | 143,967 | 936,716 |
| 2006 | 404,206 | 4,241,150 | 94,915 | 1,491,020 | 22,380 | 392,940 | 67,440 | 940,586 | 137,832 | 874,958 |
| 2007 | 401,661 | 4,081,595 | 86,548 | 1,276,070 | 23,380 | 435,724 | 70,131 | 607,166 | 146,797 | 898,771 |
| 2008 | 394,935 | 3,949,307 | 77,148 | 1,084,687 | 24,536 | 442,670 | 72,918 | 520,957 | 150,073 | 884,860 |
| 2009 | 413,144 | 3,981,120 | 86,468 | 1,219,970 | 25,491 | 460,367 | 81,595 | 541,349 | 128,384 | 754,316 |
| 2010 | 421,552 | 4,036,778 | 89,379 | 1,214,298 | 26,312 | 499,738 | 101,820 | 645,725 | 117,861 | 778,011 |
| 2011 | 345,627 | 3,102,062 | 91,519 | 1,276,442 | 27,760 | 493,735 | 115,077 | 593,917 | 109,444 | 806,347 |
| 2012 | 247,985 | 2,289,123 | 94,837 | 1,349,398 | 34,649 | 522,087 | 131,903 | 667,656 | 107,395 | 814,308 |
| 2013 | 186,076 | 1,799,736 | 99,058 | 1,463,963 | 32,788 | 479,013 | 120,734 | 545,088 | 88,419 | 829,671 |
| 2014 | 156,732 | 1,477,050 | 107,500 | 1,602,230 | 33,831 | 517,421 | 122,544 | 433,467 | 78,104 | 668,663 |
References
- Directive 2000/60/EC of the European Parliament and of the Council of 23 October 2000. Available online: http://ec.europa.eu/health/endocrine_disruptors/docs/wfd_200060ec_directive_en.pdf (accessed on 2 May 2016).
- Directive 2008/105/EC of the European Parliament and of the Council of 16 December 2008. Available online: http://eur-lex.europa.eu/LexUriServ/LexUriServ.do?uri=OJ:L:2008:348:0084:0097:en:PDF (accessed on 2 May 2016).
- Directive 2013/39/EU of the European Parliament and of the Council of 12 August 2013. Available online: http://data.europa.eu/eli/dir/2013/39/oj (accessed on 2 May 2016).
- Decision 2015/495/EU. Available online: http://eur-lex.europa.eu/legal-content/EN/TXT/PDF/?uri=uriserv:OJ.L_.2015.078.01.0040.01.ENG (accessed on 18 July 2016).
- Mayo Clinic. Drugs and Supplements, Diclofenac (Oral Route). Available online: http://www.mayoclinic.org/drugs-supplements/diclofenac-oral-route/description/drg-20069748 (accessed on 18 July 2016).
- Duong, M.; Salvo, F.; Pariente, A.; Abouelfath, A.; Lassalle, R.; Droz, C.; Blin, P.; Moore, N. Usage Patterns of ‘Over-The-Counter’ vs. Prescription-Strength Nonsteroidal Anti-Inflammatory Drugs in France. Br. J. Pharmacol. 2014, 77, 887–895. [Google Scholar] [CrossRef] [PubMed]
- Reddy, K.S.; Roy, A. Cardiovascular Risk of NSAIDs: Time to Translate Knowledge into Practice. PLoS Med. 2013, 10, e1001389. [Google Scholar] [CrossRef] [PubMed]
- Harirforoosh, S.; Asghar, W.; Jamali, F. Adverse Effects of Nonsteroidal Antiinflammatory Drugs: An Update of Gastrointestinal, Cardiovascular and Renal Complications. J. Pharm. Pharm. Sci. 2013, 16, 821–847. [Google Scholar] [CrossRef] [PubMed]
- Medicines and Healthcare products Regulatory Agency (MHRA). Non-Steroidal Anti-Inflammatory Drugs and Cardiovascular Risks in the General Population; MHRA: London, UK, 2010. Available online: http://www.mhra.gov.uk/home/groups/s-par/documents/websiteresources/con068576.pdf (accessed on 6 August 2016).
- Sukkar, E. Risk of Heart Problems Prompts Removal of OTC Diclofenac from UK Pharmacy Selves. Pharm. J. 2015, 294, 7846. [Google Scholar] [CrossRef]
- McGettigan, P.; Henry, D. Use of Non-Steroidal Anti-Inflammatory Drugs that Elevate Cardiovascular Risk: An Examination of Sales and Essential Medicines Lists in Low-, Middle-, and High-Income Countries. PLoS Med. 2013, 10, e1001388. [Google Scholar] [CrossRef] [PubMed]
- European Medicines Agency (EMEA). Diclofenac Summary Report; The European Agency for the Evaluation of Medicinal Products Veterinary Medicines and Inspections: London, UK, 2003. [Google Scholar]
- Pharmaceutical Press. Clarke’s Analysis of Drugs and Poisons; Pharmaceutical Press: London, UK, 2011. [Google Scholar]
- Vieno, N.; Sillanpää, M. Fate of Diclofenac in Municipal Wastewater treatment Plant-A Review. Environ. Int. 2014, 69, 28–39. [Google Scholar] [CrossRef] [PubMed]
- Khetan, S.K.; Collins, T.J. Human Pharmaceuticals in the Aquatic Environment: A Challenge to Green Chemistry. Chem. Rev. 2007, 107, 2319–2364. [Google Scholar] [CrossRef] [PubMed]
- Barbosa, M.O.; Moreira, N.F.F.; Ribeiro, A.R.; Pereira, M.F.R.; Silva, A.M.T. Occurrence and Removal of Organic Micropollutants: An Overview of the Watch List of EU Decision 2015/495. Water Res. 2016, 94, 257–279. [Google Scholar] [CrossRef] [PubMed]
- Huebner, M.; Weber, E.; Niessner, R.; Boujday, S.; Knopp, D. Rapid Analysis of Diclofenac in Freshwater and Wastewater by a Monoclonal Antibody-Based Highly Sensitive ELISA. Anal. Bioanal. Chem. 2015, 407, 8873–8882. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Geißen, S.U.; Gal, C. Carbamazepine and Diclofenac: Removal in Wastewater Treatment Plants and Occurrence in Water Bodies. Chemosphere 2008, 73, 1151–1161. [Google Scholar] [CrossRef] [PubMed]
- Schröder, P.; Helmreich, B.; Škrbić, B.; Carballa, M.; Papa, M.; Pastore, C.; Emre, Z.; Oehmen, A.; Langenhoff, A.; Molinos, M.; et al. Status of Hormones and Painkillers in Wastewater Effluents Across Several European States—Considerations for The EU Watch List Concerning Estradiols and Diclofenac. Environ. Sci. Pollut. Res. 2016, 23, 12835–12866. [Google Scholar] [CrossRef] [PubMed]
- Petrovic, M.; de Alda, M.J.; Diaz-Cruz, S.; Postigo, C.; Radjenovic, J.; Gros, M.; Barcelo, D. Fate and Removal of Pharmaceuticals and Illicit Drugs in Conventional and Membrane Bioreactor Wastewater Treatment Plants and by Riverbank Filtration. Philos. Trans. A Math. Phys. Eng. Sci. 2009, 367, 3979–4003. [Google Scholar] [CrossRef] [PubMed]
- Swan, G.; Naidoo, V.; Cuthbert, R.; Green, R.E.; Pain, D.J.; Swarup, D.; Prakash, V.; Taggart, M.; Bekker, L.; Das, D.; et al. Removing the Threat of Diclofenac to Critically Endangered Asian Vultures. PLoS Biol. 2006, 4, 395–402. [Google Scholar] [CrossRef] [PubMed]
- Brodin, T.; Piovano, S.; Fick, J.; Klaminder, J.; Heynen, M.; Jonsson, M. Ecological Effects of Pharmaceuticals in Aquatic Systems-Impacts through Behavioural Alterations. Philos. Trans. R. Soc. B 2014, 369. [Google Scholar] [CrossRef] [PubMed]
- Yu, H.; Nie, E.; Xu, J.; Yan, S.; Cooper, W.J.; Song, W. Degradation of Diclofenac by Advanced Oxidation and Reduction Processes: Kinetic Studies, Degradation Pathways and Toxicity Assessments. Water Res. 2013, 47, 1909–1918. [Google Scholar] [CrossRef] [PubMed]
- Mehinto, A.C.; Hill, E.M.; Tyler, C.R. Uptake and Biological Effects of Environmentally Relevant Concentrations of the Nonsteroidal Anti-inflammatory Pharmaceutical Diclofenac in Rainbow Trout (Oncorhynchus mykiss). Environ. Sci. Technol. 2010, 44, 2176–2182. [Google Scholar] [CrossRef] [PubMed]
- Xekoukoulotakis, N.P.; Xinidis, N.; Chroni, M.; Mantzavinos, D.; Venieri, D.; Hapeshi, E.; Fatta-Kassinos, D. UV-A/TiO2 Photocatalytic Decomposition of Erythromycin in Water: Factors Affecting Mineralization and Antibiotic Activity. Catal. Today 2010, 151, 29–33. [Google Scholar] [CrossRef]
- Brayfield, A. Martindale: The Complete Drug Reference, 38th ed.; Pharmaceutical Press: London, UK, 2014. [Google Scholar]
- Lange, F.; Cornelissen, S.; Kubac, D.; Sein, M.M.; von Sonntag, J.; Hannich, C.B.; Golloch, A.; Heipieper, H.J.; Möder, M.; von Sonntag, C. Degradation of Macrolide Antibiotics by ozone: A Mechanistic Case Study with Clarithromycin. Chemosphere 2006, 65, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Kanoh, S.; Rubin, B.K. Mechanisms of Action and Clinical Application of Macrolides as Immunomodulatory Medications. Clin. Microbiol. Rev. 2010, 23, 590–615. [Google Scholar] [CrossRef] [PubMed]
- Joint Formulary Committee. British National Formulary, 71st ed.; British National Formulary: London, UK, 2016. [Google Scholar]
- CAP Guideline Working Group. Annotated BTS Guideline for the Management of CAP in Adults 2015; British Thoracic Society: London, UK, 2015. [Google Scholar]
- Rubinstein, E. Comparative Safety of the Different Macrolides. Int. J. Antimicrob. Agents 2001, 18, 71–76. [Google Scholar] [CrossRef]
- Abu-Gharbieh, E.; Vasina, V.; Poluzzi, E.; De Ponti, F. Antibacterial Macrolides: A Drug Class with a Complex Pharmacological Profile. Pharmacol. Res. 2004, 50, 211–222. [Google Scholar] [CrossRef] [PubMed]
- Albert, R.K.; Schuller, J.L. Macrolide Antibiotics and the Risk of Cardiac Arrhythmias. Am. J. Respir. Crit. Care Med. 2014, 189, 1173–1180. [Google Scholar] [CrossRef] [PubMed]
- Le-Minh, N.; Khan, S.J.; Drewes, J.E.; Stuetz, R.M. Fate of Antibiotics during Municipal Water Recycling Treatment Processes. Water Res. 2010, 44, 4295–4323. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, H.; Tamura, I.; Abe, R.; Takanobu, H.; Nakamura, A.; Suzuki, T.; Hirose, A.; Nishimura, T.; Tatarazako, N. Chronic Toxicity of an Environmentally Relevant Mixture of Pharmaceuticals to Three Aquatic Organisms (Alga, Daphnid, and Fish). Environ. Toxicol. Chem. 2016, 35, 996–1006. [Google Scholar] [CrossRef] [PubMed]
- Baumann, M.; Weiss, K.; Maletzki, D.; Schüssler, W.; Schudoma, D.; Kopf, W.; Kühnen, U. Aquatic Toxicity of the Macrolide Antibiotic Clarithromycin and Its Metabolites. Chemosphere 2015, 120, 192–198. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Lu, G.; Xie, Z.; Zhang, Z.; Li, S.; Yan, Z. Occurrence, Bioaccumulation and Risk Assessment of Lipophilic Pharmaceutically Active Compounds in the Downstream Rivers of Sewage Treatment Plants. Sci. Total Environ. 2015, 511, 54–62. [Google Scholar] [CrossRef] [PubMed]
- American Society of Health-System Pharmacists (ASHP). AHFS Clinical Drug Information; ASHP: Bethesda, MD, USA, 2016. [Google Scholar]
- Zhang, C.; Li, Y.; Wang, C.; Niu, L.; Cai, W. Occurrence of Endocrine Disrupting Compounds in Aqueous Environment and their Bacterial Degradation: A Review. Crit. Rev. Environ. Sci. Technol. 2016, 46, 1–59. [Google Scholar] [CrossRef]
- Kostich, M.; Flick, R.; Martinson, J. Comparing Predicted Estrogen Concentrations with Measurements in US Waters. Environ. Pollut. 2013, 178, 271–277. [Google Scholar] [CrossRef] [PubMed]
- Clouzot, L.; Marrot, B.; Doumenq, P.; Roche, N. 17α-Ethinylestradiol: An Endocrine Distrupter of Great Concern. Analytical Methods and Removal Processes Applied to Water Purification. A Review. Environ. Prog. 2008, 27, 383–396. [Google Scholar] [CrossRef]
- Google Trends. Available online: http://www.google.com/trends (accessed on 25 April 2016).
- Jun, S.P.; Park, D.H. Consumer Information Search Behavior and Purchasing Decisions: Empirical Evidence from Korea. Technol. Forecast. Soc. 2016, in press. [Google Scholar] [CrossRef]
- McCallum, M.L.; Bury, G.W. Public Interest in the Environment is Falling: A Response to Ficetola (2013). Biodivers. Conserv. 2014, 23, 1057–1062. [Google Scholar] [CrossRef]
- Vosen, S.; Schmidt, T. Forecasting Private Consumption: Survey-Based Indicators vs. Google Trends. J. Forecast. 2011, 30, 565–578. [Google Scholar] [CrossRef]
- Scharkow, M.; Vogelgesang, J. Measuring the Public Agenda Using Search Engine Queries. Int. J. Public Opin. Res. 2011, 23, 104–113. [Google Scholar] [CrossRef]
- Nuti, S.V.; Wayda, B.; Ranasinghe, I.; Wang, S.; Dreyer, R.P.; Chen, S.I.; Murugiah, K. The Use of Google Trends in Health Care Research: A Systematic Review. PLoS ONE 2014, 9, e109583. [Google Scholar] [CrossRef] [PubMed]
- Zhou, X.; Ye, J.; Feng, Y. Tuberculosis Surveillance by Analyzing Google Trends. IEEE Trans. Biomed. Eng. 2011, 58, 2247–2254. [Google Scholar] [CrossRef] [PubMed]
- Alicino, C.; Bragazzi, N.L.; Faccio, V.; Amicizia, D.; Panatto, D.; Gasparini, R.; Icardi, G.; Orsi, A. Assessing Ebola-Related Web Search Behaviour: Insights and Implications from an Analytical Study of Google Trends-Based Query Volumes. Infect. Dis. Poverty 2015, 4, 54. [Google Scholar] [CrossRef] [PubMed]
- Ingram, D.G.; Matthews, C.K.; Plante, D.T. Seasonal Trends in Sleep-Disordered Breathing: Evidence from Internet Search Engine Query. Sleep Breath. 2015, 19, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Brigo, F.; Lochner, P.; Tezzon, F.; Nardone, R. Web Search Behavior for Multiple Sclerosis: An Infodemiological Study. Mult. Scler. Relat. Disord. 2014, 3, 440–443. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.W.; Chen, D.R.; Yu, H.W.; Chen, Y.M. Forecasting the Incidence of Dementia and Dementia-Related Outpatient Visits with Google Trends: Evidence from Taiwan. J. Med. Internet Res. 2015, 17, e264. [Google Scholar] [CrossRef] [PubMed]
- Brigo, F.; Igwe, S.C.; Ausserer, H.; Nardone, R.; Tezzon, F.; Bongiovanni, L.G.; Trinka, E. Why Do People Google Epilepsy? An Infodemiological Study of Online Behavior for Epilepsy-Related Search Terms. Epilepsy Behav. 2014, 31, 67–70. [Google Scholar] [CrossRef] [PubMed]
- Bragazzi, N.L.; Bacigaluppi, S.; Robba, C.; Nardone, R.; Trinka, E.; Brigo, F. Infodemiology of Status Epilepticus: A Systematic Validation of the Google Trends-Based Search Queries. Epilepsy Behav. 2016, 55, 120–123. [Google Scholar] [CrossRef] [PubMed]
- Linkov, F.; Bovbjerg, D.H.; Freese, K.E.; Ramanathan, R.; Eid, G.M.; Gourash, W. Bariatric Surgery Interest Around the World: What Google Trends Can Teach Us. Surg. Obes. Relat. Dis. 2014, 10, 533–538. [Google Scholar] [CrossRef] [PubMed]
- Rosenkrantz, A.B.; Prabhu, V. Public Interest in Imaging-Based Cancer Screening Examinations in the United States: Analysis Using a Web-Based Search Tool. AJR Am. J. Roentgenol. 2016, 206, 113–118. [Google Scholar] [CrossRef] [PubMed]
- Whitsitt, J.; Karimkhani, C.; Boyers, L.N.; Lott, J.P.; Dellavalle, R.P. Comparing Burden of Dermatologic Disease to Search Interest on Google Trends. Dermatol. Online J. 2015, 21, 25612125. [Google Scholar]
- Ingram, D.G.; Plante, D.T. Seasonal Trends in Restless Legs Symptomatology: Evidence from Internet Search Query Data. J. Clin. Sleep Med. 2013, 14, 1364–1368. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Zheng, X.; Zeng, D.D.; Leischow, S.J. Information Seeking Regarding Tobacco and Lung Cancer: Effects of Seasonality. PLoS ONE 2015, 10, e0117938. [Google Scholar] [CrossRef] [PubMed]
- Cavazos-Rehg, P.A.; Krauss, M.J.; Spitznagel, E.L.; Lowery, A.; Grucza, R.A.; Chaloupka, F.J.; Bierut, L.J. Monitoring of Non-Cigarette Tobacco Use Using Google Trends. Tob. Control 2015, 24, 249–255. [Google Scholar] [CrossRef] [PubMed]
- Davidson, M.W.; Haim, D.A.; Radin, J.M. Using Networks to Combine Big Data and Traditional Surveillance to Improve Influenza Predictions. Sci. Rep. 2015, 5, 8154. [Google Scholar] [CrossRef] [PubMed]
- Dukic, V.; Lopes, H.F.; Polson, N.G. Tracking Epidemics with Google Flu Trends Data and a State-Space SEIR Model. J. Am. Stat. Assoc. 2012, 170, 1410–1426. [Google Scholar] [CrossRef]
- McCallum, M.L.; Bury, G.W. Google Search Patterns Suggest Declining Interest in the Environment. Biodivers. Conserv. 2013, 22, 1355–1367. [Google Scholar] [CrossRef]
- Nijman, V. CITES-listings, EU Eel Trade Bans and the Increase of Export of Tropical Eels out of Indonesia. Mar. Policy 2015, 58, 36–41. [Google Scholar] [CrossRef]
- Schuetz, J.; Soykan, C.U.; Distler, T.; Langham, G. Searching for Backyard Birds in Virtual Words: Internet Queries Mirror Real Species Distributions. Biodivers. Conserv. 2014, 24, 1147–1154. [Google Scholar] [CrossRef]
- Ficetola, G.F. Is Interest Toward the Environment Really Declining? The Complexity of Analyzing Trends Using Internet Search Data. Biodivers. Conserv. 2013, 22, 2983–2988. [Google Scholar] [CrossRef]
- Google Trends. Data Normalization. 2016. Available online: https://support.google.com/trends/answer/4365533 (accessed on 8 February 2016).
- NHS Digital. Available online: http://digital.nhs.uk/ (accessed on 20 July 2016).
- Prescriptions Dispensed in the Community. Available online: http://gov.wales/statistics-and-research/prescriptions-dispensed-community/?lang=en/ (assessed on 24 July 2016).
- Information Services Division. Available online: http://www.isdscotland.org/Health-Topics/Prescribing-and-Medicines/Community-Dispensing/Prescription-Cost-Analysis/ (assessed on 22 July 2016).
- Business Services Organisation. Available online: http://www.hscbusiness.hscni.net/services/1806.htm (assessed on 26 July 2016).
- Diclofenac Tablets Now Only Available as a Prescription Medicine. Available online: https://www.gov.uk/government/news/diclofenac-tablets-now-only-available-as-a-prescription-medicine (accessed on 8 August 2005).
- Scopus. Available online: http://www.scopus.com (accessed on 12 August 2016).
- Medicines and Healthcare products Regulatory Agency (MHRA). New Recommendations after a Europe-Wide Review of Cardiovascular Safety; MHRA: London, UK, 2013.
- Brozinski, J.M.; Lahti, M.; Meierjohann, A.; Oikari, A.; Kronberg, L. The Anti-Inflammatory Drugs Diclofenac, Naproxen and Ibuprofen are found in the Bile of Wild Fish Caught Downstream of a Wastewater Treatment Plant. Environ. Sci. Technol. 2013, 47, 342–348. [Google Scholar] [CrossRef] [PubMed]
- Public Health England. Management of Infection Guidance for Primary Care for Consultation and Local Adaptation; Public Health England: London, UK, 2016.
- Public Health England. Sexually Transmitted Infections and Chlamydia Screening in England, 2015; Public Health England: London, UK, 2016.
- Southern, K.W.; Barker, P.M.; Solis-Moya, A.; Patel, L. Macrolide Antibiotics for Cystic Fibrosis. Cochrane Database Syst. Rev. 2012, 11, CD002203. [Google Scholar] [PubMed]
- National Institute for Health and Care Excellence. Antimicrobial Stewardship: Systems and Processes for Effective Antimicrobial Medicine Use; National Institute for Health and Care Excellence: London, UK, 2015.
- British Poultry Council, 2004. Available online: http://www.britishpoultry.org.uk/areas-of-work/animal-health-and-welfare/antibiotic-use-in-poultry/ (accessed on 4 September 2016).
- NHS-Contraception Guide. Available online: http://www.nhs.uk/conditions/contraception-guide/pages/where-can-i-get-contraception.aspx/ (accessed on 22 September 2016).

| Year | Diclofenac | Estradiol | Azithromycin | Clarithromycin | Erythromycin |
|---|---|---|---|---|---|
| 2004 | 32.19% | 23.08% | 26.39% | 12.19% | 6.15% |
| 2005 | 35.62% | 21.04% | 23.84% | 12.70% | 6.81% |
| 2006 | 34.79% | 18.05% | 20.82% | 19.18% | 7.16% |
| 2007 | 35.01% | 16.40% | 20.43% | 20.35% | 7.80% |
| 2008 | 35.15% | 15.61% | 20.42% | 20.75% | 8.07% |
| 2009 | 35.29% | 14.91% | 20.42% | 21.13% | 8.25% |
| 2010 | 36.63% | 14.98% | 18.33% | 21.71% | 8.34% |
| 2011 | 37.20% | 14.58% | 16.95% | 23.03% | 8.24% |
| 2012 | 37.41% | 14.21% | 16.23% | 23.86% | 8.30% |
| 2013 | 38.44% | 13.46% | 15.99% | 23.95% | 8.16% |
| 2014 | 38.81% | 12.89% | 15.95% | 24.14% | 8.21% |
| Average | 36.05% | 16.29% | 19.61% | 20.27% | 7.77% |
| Year | Diclofenac | Estradiol | Azithromycin | Clarithromycin | Erythromycin |
|---|---|---|---|---|---|
| 2004 | 41.55% | 11.07% | 9.53% | 9.76% | 28.09% |
| 2005 | 46.11% | 7.66% | 7.70% | 8.18% | 30.36% |
| 2006 | 50.00% | 7.06% | 6.42% | 7.69% | 28.82% |
| 2007 | 50.82% | 5.61% | 7.30% | 7.49% | 28.77% |
| 2008 | 50.13% | 6.55% | 8.09% | 7.92% | 27.30% |
| 2009 | 50.60% | 8.05% | 8.19% | 8.69% | 24.47% |
| 2010 | 50.92% | 7.78% | 8.04% | 10.12% | 23.14% |
| 2011 | 48.96% | 4.40% | 8.80% | 12.08% | 25.76% |
| 2012 | 44.10% | 4.33% | 9.53% | 16.03% | 26.01% |
| 2013 | 43.38% | 4.55% | 10.05% | 17.25% | 24.77% |
| 2014 | 34.53% | 4.91% | 12.06% | 22.19% | 26.32% |
| Average | 46.46% | 6.54% | 8.70% | 11.58% | 26.71% |
| Region | Diclofenac | Estradiol | Azithromycin | Clarithromycin | Erythromycin |
|---|---|---|---|---|---|
| England | 46.25% | 6.67% | 9.03% | 11.59% | 26.47% |
| Wales | 37.29% | 8.44% | 11.03% | 13.01% | 30.22% |
| Scotland | 39.66% | 10.19% | 11.29% | 15.28% | 23.58% |
| N. Ireland | 35.63% | 11.04% | 12.26% | 16.63% | 24.44% |
| Region | Diclofenac | Estradiol | Azithromycin | Clarithromycin | Erythromycin |
|---|---|---|---|---|---|
| Worldwide | 20.56% | −44.15% | −39.55% | 98.02% | 33.47% |
| UK | −16.90% | −55.69% | 26.47% | 127.34% | −6.28% |
| England | −19.64% | −54.78% | 7.77% | 109.02% | 8.56% |
| Wales | −61.47% | 224.48% | 435.49% * | 551.03% | −26.13% |
| Scotland | 7.70% | −31.69% | 18.77% | 51.58% | −28.11% |
| N. Ireland | −3.52% | −35.87% | 12.90% * | −26.22% | −5.26% |
| Year | Diclofenac | Estradiol | Azithromycin | Clarithromycin | Erythromycin |
|---|---|---|---|---|---|
| 2004 | 1470 | 4203 | 1259 | 1582 | 2537 |
| 2005 | 1573 | 4342 | 1320 | 1593 | 2554 |
| 2006 | 1561 | 4384 | 1267 | 1445 | 2414 |
| 2007 | 1566 | 4278 | 1282 | 1443 | 2391 |
| 2008 | 1538 | 4453 | 1242 | 1422 | 2429 |
| 2009 | 1659 | 4364 | 1348 | 1493 | 2308 |
| 2010 | 1708 | 4376 | 1332 | 1401 | 2215 |
| 2011 | 1832 | 4447 | 1358 | 1334 | 2126 |
| 2012 | 1896 | 4507 | 1486 | 1356 | 2202 |
| 2013 | 1899 | 4469 | 1700 | 1465 | 2259 |
| 2014 | 1714 | 4316 | 1513 | 1249 | 2005 |
| Total | 18,416 | 48,139 | 15,107 | 15,783 | 25,440 |
| Year | Diclofenac | Estradiol | Azithromycin | Clarithromycin | Erythromycin |
|---|---|---|---|---|---|
| 2004 | 147 | 244 | 96 | 97 | 233 |
| 2005 | 160 | 253 | 105 | 112 | 229 |
| 2006 | 163 | 256 | 93 | 74 | 220 |
| 2007 | 157 | 233 | 83 | 97 | 216 |
| 2008 | 166 | 263 | 92 | 112 | 217 |
| 2009 | 137 | 251 | 108 | 123 | 209 |
| 2010 | 121 | 244 | 132 | 104 | 182 |
| 2011 | 156 | 220 | 107 | 121 | 160 |
| 2012 | 133 | 205 | 116 | 115 | 161 |
| 2013 | 134 | 242 | 147 | 125 | 140 |
| 2014 | 108 | 188 | 129 | 98 | 117 |
| Total | 1582 | 2599 | 1208 | 1178 | 2084 |
| Substance | Pxs-GT (UK) | Pxs-GT (England) | Pxs-GT (Scotland) | Pxs-GT (Wales) | Pxs-GT (N. Ireland) | Scopus-GT (Worldwide) | Scopus-GT (UK) |
|---|---|---|---|---|---|---|---|
| Diclofenac | 0.7814 *** | 0.7903 *** | 0.1358 | 0.6045 ** | 0.5843 * | 0.8637 **** | 0.3067 |
| Estradiol | −0.2775 | −0.3455 | 0.0369 | 0.4974 | 0.5189 | −0.5293 | 0.371 |
| Azithromycin | 0.8287 *** | 0.6395 ** | −0.0642 | 0.7133 ** | 0.5783 * | −0.7569 *** | 0.7778 *** |
| Clarithromycin | 0.9531 **** | 0.9384 **** | 0.4014 | 0.7535 *** | 0.4935 | −0.9129 **** | 0.6631 ** |
| Erythromycin | 0.5677 * | 0.1295 | 0.7795 *** | −0.5847 * | 0.3736 | −0.7933 *** | 0.609 ** |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mavragani, A.; Sypsa, K.; Sampri, A.; Tsagarakis, K.P. Quantifying the UK Online Interest in Substances of the EU Watchlist for Water Monitoring: Diclofenac, Estradiol, and the Macrolide Antibiotics. Water 2016, 8, 542. https://doi.org/10.3390/w8110542
Mavragani A, Sypsa K, Sampri A, Tsagarakis KP. Quantifying the UK Online Interest in Substances of the EU Watchlist for Water Monitoring: Diclofenac, Estradiol, and the Macrolide Antibiotics. Water. 2016; 8(11):542. https://doi.org/10.3390/w8110542
Chicago/Turabian StyleMavragani, Amaryllis, Karla Sypsa, Alexia Sampri, and Konstantinos P. Tsagarakis. 2016. "Quantifying the UK Online Interest in Substances of the EU Watchlist for Water Monitoring: Diclofenac, Estradiol, and the Macrolide Antibiotics" Water 8, no. 11: 542. https://doi.org/10.3390/w8110542
APA StyleMavragani, A., Sypsa, K., Sampri, A., & Tsagarakis, K. P. (2016). Quantifying the UK Online Interest in Substances of the EU Watchlist for Water Monitoring: Diclofenac, Estradiol, and the Macrolide Antibiotics. Water, 8(11), 542. https://doi.org/10.3390/w8110542