
Long-Term Exposure to PM10 Air Pollution Exaggerates Progression of Coronary Artery Disease

 , ,
, ,  , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
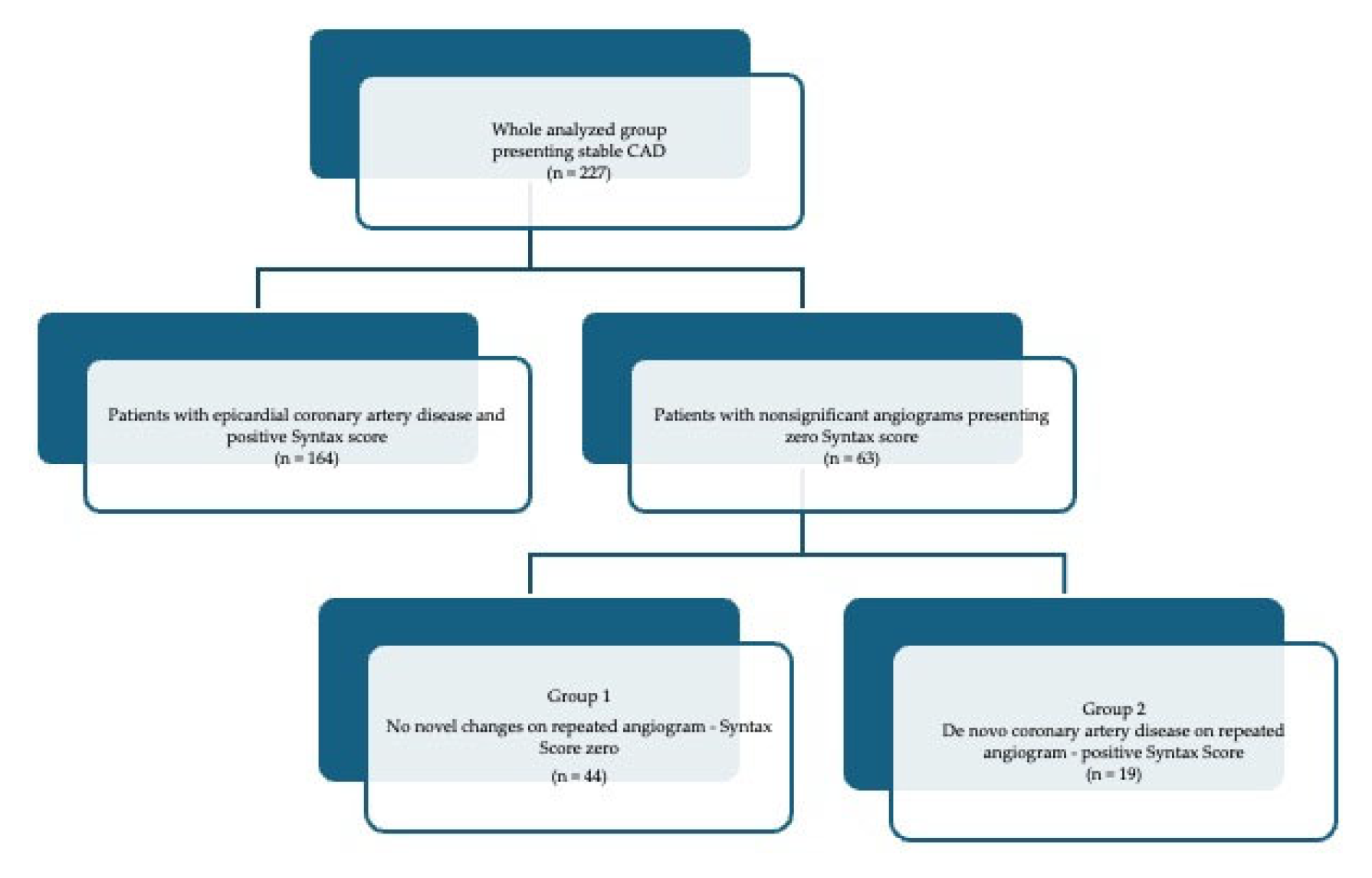
2.1. Patients’ Study Group
2.2. Air Pollution Exposure
2.3. Statistical Analysis
3. Results
3.1. Angiographic and Laboratory Results on Readmission
3.2. Angiographic Results
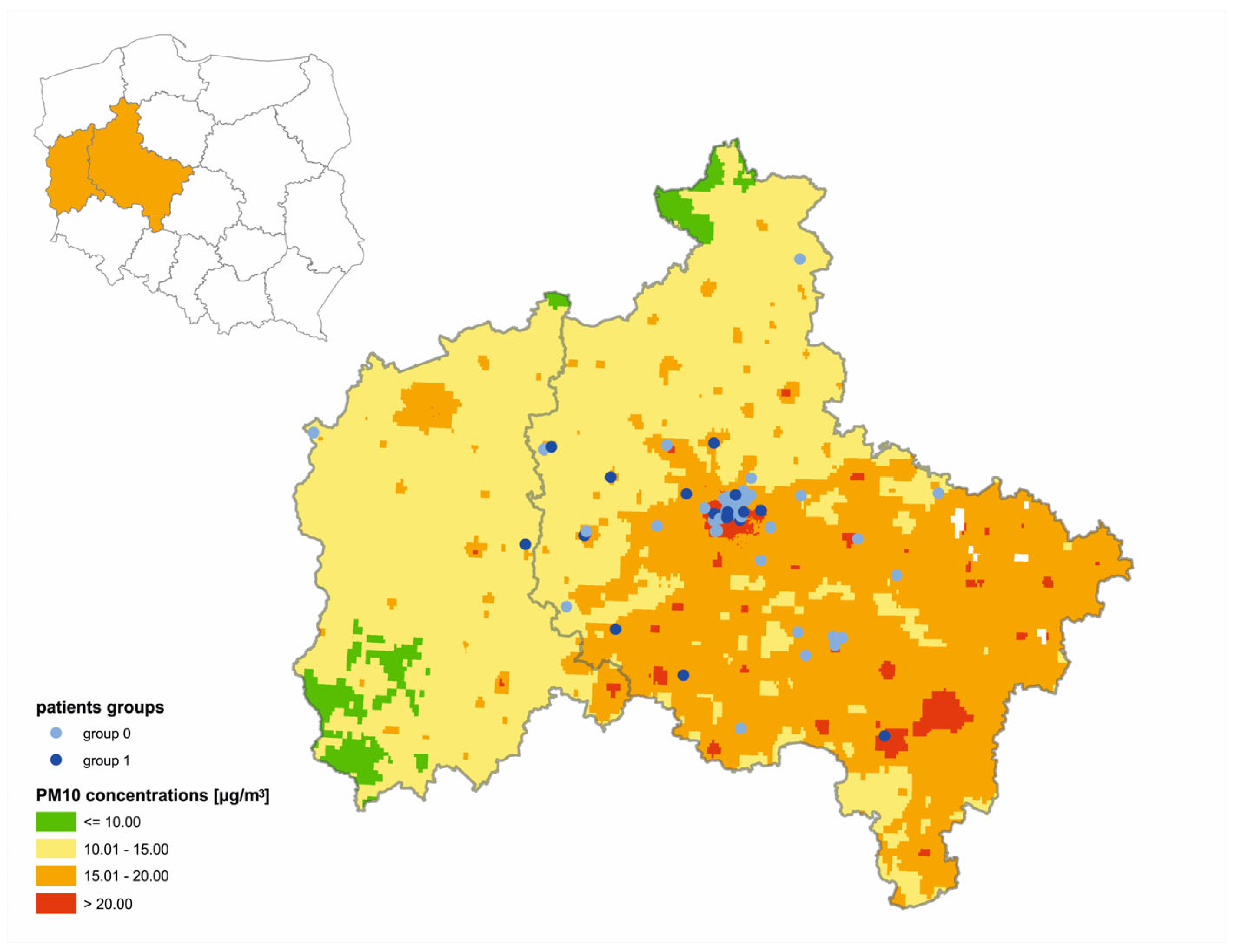
3.3. Air Pollution Exposure
3.4. Correlations
3.4.1. Demographical and Clinical Factors Significant for Atherosclerotic Lesion Development
3.4.2. PM10 Air Pollution Exposure as a Potential Risk Factor for Atherosclerotic Lesion Development
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wang, Y.; Qiu, X.; Wei, Y.; Schwartz, J.D. Long-Term Exposure to Ambient PM2.5 and Hospitalizations for Myocardial Infarction Among US Residents: A Difference-in-Differences Analysis. J. Am. Heart Assoc. 2023, 2023, e029428. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Qian, Z.M.; Chen, L.; Zhao, X.; Cai, M.; Wang, C.; Zou, H.; Wu, Y.; Zhang, Z.; Li, H.; et al. Exposure to Air Pollution during Pre-Hypertension and Subsequent Hypertension, Cardiovascular Disease, and Death: A Trajectory Analysis of the UK Biobank Cohort. Environ. Health Perspect. 2023, 131, 17008–17018. [Google Scholar] [CrossRef] [PubMed]
- Zindel, J.; Kubes, P. DAMPs, PAMPs, and LAMPs in Immunity and Sterile Inflammation. Annu. Rev. Pathol. 2020, 15, 493–518. [Google Scholar] [CrossRef]
- Nogueira, J.B. Air pollution and cardiovascular disease. Rev. Port. Cardiol. 2009, 40, 715–733. [Google Scholar]
- Bhatnagar, A. Cardiovascular Effects of Particulate Air Pollution. Annu. Rev. Med. 2022, 73, 393–406. [Google Scholar] [CrossRef]
- Bourdrel, T.; Bind, M.A.; Béjot, Y.; Morel, O.; Argacha, J.F. Cardiovascular effects of air pollution. Arch. Cardiovasc. Dis. 2017, 110, 634–642. [Google Scholar] [CrossRef]
- Pope, C.A., 3rd; Bhatnagar, A.; McCracken, J.P.; Abplanalp, W.; Conklin, D.J.; O’Toole, T. Exposure to Fine Particulate Air Pollution Is Associated With Endothelial Injury and Systemic Inflammation. Circ. Res. 2016, 119, 1204–1214. [Google Scholar] [CrossRef]
- Hayes, R.B.; Lim, C.; Zhang, Y.; Cromar, K.; Shao, Y.; Reynolds, H.R.; Silverman, D.T.; Jones, R.R.; Park, Y.; Jerrett, M.; et al. PM2.5 air pollution and cause-specific cardiovascular disease mortality. Int. J. Epidemiol. 2020, 49, 25–35. [Google Scholar] [CrossRef]
- Krittanawong, C.; Qadeer, Y.K.; Hayes, R.B.; Wang, Z.; Virani, S.; Thurston, G.D.; Lavie, C.J. PM2.5 and Cardiovascular Health Risks. Curr. Probl. Cardiol. 2023, 48, 101670. [Google Scholar] [CrossRef]
- Wu, K.; Ho, H.C.; Su, H.; Huang, C.; Zheng, H.; Zhang, W.; Tao, J.; Hossain, M.Z.; Zhang, Y.; Hu, K.; et al. A systematic review and meta-analysis of intraday effects of ambient air pollution and temperature on cardiorespiratory morbidities: First few hours of exposure matters to life. EBioMedicine 2022, 86, 104327–104340. [Google Scholar] [CrossRef]
- Donaldson, K.; Stone, V.; Seaton, A.; MacNee, W. Ambient particle inhalation and the cardiovascular system: Potential mechanisms. Environ. Health Perspect. 2001, 109, 523–527. [Google Scholar]
- Stone, V.; Brown, D.M.; Watt, N.; Wilson, M.; Donaldson, K.; Ritchie, H.; MacNee, W. Ultrafine Particle-Mediated Activation of Macrophages: Intracellular Calcium Signaling and Oxidative Stress. Inhal. Toxicol. 2000, 12, 345–351. [Google Scholar] [CrossRef]
- Brown, D.M.; Donaldson, K.; Stone, V. Effects of PM10 in human peripheral blood monocytes and J774 macrophages. Respir. Res. 2004, 5, 29–41. [Google Scholar] [CrossRef] [PubMed]
- Gaio, V.; Roquette, R.; Monteiro, A.; Ferreira, J.; Lopes, D.; Dias, C.M.; Nunes, B. PM10 exposure interacts with abdominal obesity to increase blood triglycerides: A cross-sectional linkage study. Eur. J. Public Health 2022, 32, 281–288. [Google Scholar] [CrossRef] [PubMed]
- Marín-Palma, D.; Tabares-Guevara, J.H.; Zapata-Cardona, M.I.; Zapata-Builes, W.; Taborda, N.; Rµgeles, M.T.; Hernandez, J.C. PM10 promotes an inflammatory cytokine response that may impact SARS-CoV-2 replication in vitro. Front. Immunol. 2023, 14, 1161135–1161147. [Google Scholar] [CrossRef] [PubMed]
- Cen, J.; Jia, Z.L.; Zhu, C.Y.; Wang, X.F.; Zhang, F.; Chen, W.Y.; Liu, K.C.; Li, S.Y.; Zhang, Y. Particulate matter (PM10) induces cardiovascular developmental toxicity in zebrafish embryos and larvae via the ERS, Nrf2 and Wnt pathways. Chemosphere 2020, 250, 126288–126299. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.; Jiang, Y.; Hu, J.; Chen, H.; Li, H.; Meng, X.; Ji, J.S.; Gao, Y.; Wang, W.; Liu, C.; et al. Hourly Air Pollutants and Acute Coronary Syndrome Onset in 1.29 Million Patients. Circulation 2022, 145, 1749–1760. [Google Scholar] [CrossRef] [PubMed]
- Serruys, P.W.; Onuma, Y.; Garg, S.; Sarno, G.; Van den Brand, M.; Kappetein, A.P.; Van Dyck, N.; Mack, M.; Holmes, D.; Feldman, T.; et al. Assessment of the SYNTAX score in the Syntax study. EuroIntervention 2009, 5, 50–56. [Google Scholar] [CrossRef]
- Mapa Wykonana w Oparciu o Modelowanie Matematyczne Przygotowane Przez Instytut Ochrony Środowiska—Państwowy Instytut Badawczy Oraz Metodę Obiektywnego Szacowania. PM10 (Śr. Roczna)—Rozkład Przestrzenny Średniego Rocznego Stężenia PM10 [µg/m3]. Available online: https://powietrze.gios.gov.pl/pjp/maps/modeling (accessed on 10 December 2023).
- Tagaris, E.; Sotiropoulou, R.E.P.; Gounaris, N.; Andronopoulos, S.; Vlachogiannis, D. Effect of the Standard Nomenclature for Air Pollution (SNAP) categories on air quality over Europe. Atmosphere 2015, 6, 1119–1128. [Google Scholar] [CrossRef]
- European Air Quality, Copernicus, Atmosphere Monitoring Service. Available online: https://www.regional.atmosphere.copernicus.eu/ (accessed on 27 December 2022).
- Kaminski, J.W.; Neary, L.; Struzewska, J.; McConnell, J.C.; Lupu, A.; Jarosz, J.; Toyota, K.; Gong, S.L.; Côté, J.; Liu, X. GEM-AQ, an online global multiscale chemical weather modelling system: Model description and evaluation of gas phase chemistry processes. Atmos. Chem. Phys. 2008, 8, 3255–3281. [Google Scholar] [CrossRef]
- Markevych, I.; Orlov, N.; Grellier, J.; Kaczmarek-Majer, K.; Lipowska, M.; Sitnik-Warchulska, K.; Mysak, Y.; Baumbach, C.; Wierzba-Łukaszyk, M.; Hussain Soomro, M.; et al. NeuroSmog: Determining the impact of air pollution on the developing brain: Project protocol. Int. J. Environ. Res. Public Health 2022, 19, 310. [Google Scholar] [CrossRef]
- Fraszczyk, M.; Kaczmarek-Majer, K.; Hryniewicz, O.; Skotak, K.; Degórska, A. Expert-in-the-loop Stepwise Regression and its Application in Air Pollution Modeling. In Proceedings of the 2022 IEEE 11th International Conference on Intelligent Systems (IS), Warsaw, Poland, 12–14 October 2022; pp. 1–7. [Google Scholar]
- The European Union (EU) has Developed an Extensive Body of Legislation Which Establishes Standards and Objectives for a Number of Pollutants in Air. Available online: https://www.eea.europa.eu/themes/air/air-quality-concentrations/air-quality-standards (accessed on 27 December 2022).
- WHO Air Quality Guidelines. Available online: https://www.c40knowledgehub.org/s/article/WHO-Air-Quality-Guidelines?language=en_US (accessed on 27 December 2022).
- Iriti, M.; Piscitelli, P.; Missoni, E.; Miani, A. Air Pollution and Health: The Need for a Medical Reading of Environmental Monitoring Data. Int. J. Environ. Res. Public. Health 2020, 17, 2174. [Google Scholar] [CrossRef]
- Shamsa, E.H.; Song, Z.; Kim, H.; Shamsa, F.; Hazlett, L.D.; Zhang, K. The links of fine airborne particulate matter exposure to occurrence of cardiovascular and metabolic diseases in Michigan, USA. PLoS Glob. Public Health 2022, 2, e0000707. [Google Scholar] [CrossRef]
- Gao, Y.; Sheng, W.; Yang, Y. Air pollution and coronary heart disease-related hospital visits in Beijing, China: Time-series analysis using a generalized additive model. Environ. Sci. Pollut. Res. Int. 2023, 30, 36938–36951. [Google Scholar] [CrossRef] [PubMed]
- Macchi, C.; Sirtori, C.R.; Corsini, A.; Mannuccio Mannucci, P.; Ruscica, M. Pollution from fine particulate matter and atherosclerosis: A narrative review. Environ. Int. 2023, 175, 107923. [Google Scholar] [CrossRef] [PubMed]
- You, X.; Cao, X.; Guo, Y.; Wang, D.; Qiu, W.; Zhou, C.; Zhou, M.; Chen, W.; Zhang, X. Associations between short-term PM2.5 exposure and daily hospital admissions for circulatory system diseases in Ganzhou, China: A time series study. Front. Public Health 2023, 11, 1134516–1134527. [Google Scholar] [CrossRef] [PubMed]
- Soleimanifar, N.; Assadiasl, S.; Kalateh, E.; Hassanvand, M.S.; Sadr, M.; Mojtahedi, H.; Nadafi, K.; Nicknam, M.H.; Edalatifard, M. Circulating Exosomes and Ambient Air Pollution Exposure in COPD. Chronic Obstr. Pulm. Dis. 2023, 10, 412. [Google Scholar] [CrossRef] [PubMed]
- Feizi, A.; Shahraki, P.K.; Najafabadi, A.M.; Iraj, B.; Abyar, M.; Amini, M.; Meamar, R.; Aminorroaya, A. The association of exposure to air pollution with changes in plasma glucose indices, and incidence of diabetes and prediabetes: A prospective cohort of first-degree relatives of patients with type 2 diabetes. J. Res. Med. Sci. 2023, 28, 21–30. [Google Scholar] [PubMed]
- Liu, J.; Zhao, K.; Qian, T.; Li, X.; Yi, W.; Pan, R.; Huang, Y.; Ji, Y.; Su, H. Association between ambient air pollution and thyroid hormones levels: A systematic review and meta-analysis. Sci. Total Environ. 2023, 904, 166780–166796. [Google Scholar] [CrossRef] [PubMed]
- Pallikadavath, S.; Vali, Z.; Patel, R.; Mavilakandy, A.; Peckham, N.; Clegg, M.; Sandilands, A.J.; Ng, G.A. The Influence of Environmental Air Pollution on Ventricular Arrhythmias: A Scoping Review. Curr. Cardiol. Rev. 2022, 18, e160422203685. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Hoek, G. Long-term exposure to PM and all-cause and cause-specific mortality: A systematic review and meta-analysis. Environ. Int. 2020, 143, 105974–105997. [Google Scholar] [CrossRef]
- Han, X.; Guo, B.; Wang, L.; Chen, K.; Zhou, H.; Huang, S.; Xu, H.; Pan, X.; Chen, J.; Gao, X.; et al. The mediation role of blood lipids on the path from air pollution exposure to MAFLD: A longitudinal cohort study. Sci. Total Environ. 2023, 904, 166347–166351. [Google Scholar] [CrossRef]
- Montone, R.A.; Camilli, M.; Russo, M.; Termite, C.; La Vecchia, G.; Iannaccone, G.; Rinaldi, R.; Gurgoglione, F.; Del Buono, M.G.; Sanna, T.; et al. Air Pollution and Coronary Plaque Vulnerability and Instability: An Optical Coherence Tomography Study. JACC Cardiovasc. Imaging 2022, 15, 325–342. [Google Scholar] [CrossRef] [PubMed]
- Luo, M.; Xie, X.; Wu, J.; Zhang, L.; Zheng, X.; Xie, M.; Lin, N.; Xiao, H.; Zeng, J.; Lan, G.; et al. Association of ambient PM10 and PM2.5 with coronary stenosis measured using selective coronary angiography. Ecotoxicol. Environ. Saf. 2023, 262, 115338. [Google Scholar] [CrossRef] [PubMed]
- Terashima, T.; Wiggs, B.; English, D.; Hogg, J.C.; Van Eeden, S.F. Phagocytosis of small carbon particles (PM10) by alveolar macrophages stimulates the release of polymorphonuclear leukocytes from bone marrow. Am. J. Respir. Crit. Care Med. 1997, 155, 1441–1447. [Google Scholar] [CrossRef] [PubMed]
- Goto, Y.; Ishii, H.; Hogg, J.C.; Shih, C.H.; Yatera, K.; Vincent, R.; Van Eeden, S.F. Particulate matter air pollution stimulates monocyte release from the bone marrow. Am. J. Respir. Crit. Care Med. 2004, 170, 891–897. [Google Scholar] [CrossRef]
- Valderrama, A.; Ortiz-Hernández, P.; Agraz-Cibrián, J.M.; Tabares-Guevara, J.H.; Gómez, D.M.; Zambrano-Zaragoza, J.F.; Taborda, N.A.; Hernandez, J.C. Particulate matter (PM10) induces in vitro activation of human neutrophils, and lung histopathological alterations in a mouse model. Sci. Rep. 2022, 12, 7581–7597. [Google Scholar] [CrossRef]
- Suwa, T.; Hogg, J.C.; Quinlan, K.B.; Ohgami, A.; Vincent, R.; Van Eeden, S.F. Particulate air pollution induces progression of atherosclerosis. J. Am. Coll. Cardiol. 2002, 39, 935–942. [Google Scholar] [CrossRef]
- Urbanowicz, T.; Michalak, M.; Komosa, A.; Olasińska-Wiśniewska, A.; Filipiak, K.J.; Tykarski, A.; Jemielity, M. Predictive value of systemic inflammatory response index (SIRI) for complex coronary artery disease occurrence in patients presenting with angina equivalent symptoms. Cardiol. J. 2023, 6, 1–13. [Google Scholar] [CrossRef]
- Urbanowicz, T.; Michalak, M.; Olasińska-Wiśniewska, A.; Rodzki, M.; Witkowska, A.; Gąsecka, A.; Buczkowski, P.; Perek, B.; Jemielity, M. Neutrophil Counts, Neutrophil-to-Lymphocyte Ratio, and Systemic Inflammatory Response Index (SIRI) Predict Mortality after Off-Pump Coronary Artery Bypass Surgery. Cells 2022, 11, 1124. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.W.; Shen, T.J.; Chen, P.Y.; Chen, T.C.; Yeh, J.H.; Tsou, S.C.; Lai, C.Y.; Chen, C.H.; Chang, Y.Y. Particulate matter 2.5 exposure induces epithelial-mesenchymal transition via PI3K/AKT/mTOR pathway in human retinal pigment epithelial ARPE-19 cells. Biochem. Biophys. Res. Commun. 2022, 617, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Dawson, L.P.; Lum, M.; Nerleker, N.; Nicholls, S.J.; Layland, J. Coronary Atherosclerotic Plaque Regression: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2022, 79, 66–82. [Google Scholar] [CrossRef] [PubMed]
- Adriaenssens, T.; Allard-Ratick, M.P.; Thondapu, V.; Sµgiyama, T.; Raffel, O.C.; Barlis, P.; Poon, E.K.W.; Araki, M.; Nakajima, A.; Minami, Y.; et al. Optical Coherence Tomography of Coronary Plaque Progression and Destabilization: JACC Focus Seminar Part 3/3. J. Am. Coll. Cardiol. 2021, 78, 1275–1287. [Google Scholar] [CrossRef] [PubMed]
- Van Driest, F.Y.; Bijns, C.M.; Van der Geest, R.J.; Broersen, A.; Dijkstra, J.; Scholte, A.J.H.A.; Jukema, J.W. Utilizing (serial) coronary computed tomography angiography (CCTA) to predict plaque progression and major adverse cardiac events (MACE): Results, merits and challenges. Eur. Radiol. 2022, 32, 3408–3422. [Google Scholar] [CrossRef]
- Yoon, Y.E.; Baskaran, L.; Lee, B.C.; Pandey, M.K.; Goebel, B.; Lee, S.E.; Sung, J.M.; Andreini, D.; Al-Mallah, M.H.; Budoff, M.J.; et al. Differential progression of coronary atherosclerosis according to plaque composition: A cluster analysis of PARADIGM registry data. Sci. Rep. 2021, 11, 17121–17122. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.E.; Sung, J.M.; Andreini, D.; Al-Mallah, M.H.; Budoff, M.J.; Cademartiri, F.; Chinnaiyan, K.; Choi, J.H.; Chun, E.J.; Conte, E.; et al. Association Between Changes in Perivascular Adipose Tissue Density and Plaque Progression. JACC Cardiovasc. Imaging 2022, 15, 1760–1767. [Google Scholar] [CrossRef] [PubMed]
- Van Rosendael, A.R.; Van den Hoogen, I.J.; Gianni, U.; Ma, X.; Tantawy, S.W.; Bax, A.M.; Lu, Y.; Andreini, D.; Al-Mallah, M.H.; Budoff, M.J.; et al. Association of Statin Treatment With Progression of Coronary Atherosclerotic Plaque Composition. JAMA Cardiol. 2021, 6, 1257–1266. [Google Scholar] [CrossRef] [PubMed]
- Jimenez-Torres, J.; Alcalá-Diaz, J.F.; Torres-Peña, J.D.; Gutierrez-Mariscal, F.M.; Leon-Acuña, A.; Gómez-Luna, P.; Fernández-Gandara, C.; Quintana-Navarro, G.M.; Fernandez-Garcia, J.C.; Perez-Martinez, P.; et al. Mediterranean Diet Reduces Atherosclerosis Progression in Coronary Heart Disease: An Analysis of the CORDIOPREV Randomized Controlled Trial. Stroke 2021, 52, 3440–3449. [Google Scholar] [CrossRef]
- Teo, K.K.; Rafiq, T. Cardiovascular Risk Factors and Prevention: A Perspective From Developing Countries. Can. J. Cardiol. 2021, 37, 733–743. [Google Scholar] [CrossRef]
- Bhatnagar, A. Environmental Determinants of Cardiovascular Disease. Circ. Res. 2017, 121, 162–180. [Google Scholar] [CrossRef]
- Urbanowicz, T.; Skotak, K.; Filipiak, K.J.; Olasińska-Wiśniewska, A.; Szczepański, K.; Wyrwa, M.; Sikora, J.; Tykarski, A.; Jemielity, M. Long-Term Exposure of Nitrogen Oxides Air Pollution (NO2) Impact for Coronary Artery Lesion Progression—Pilot Study. J. Pers. Med. 2023, 13, 1376. [Google Scholar] [CrossRef] [PubMed]
- Chaus, A.; Uretsky, B.F. SYNTAX Score for Clinical Decision-Making: Necessity, Nicety, or Neither? Cardiovasc. Revasc. Med. 2022, 37, 90–91. [Google Scholar] [CrossRef] [PubMed]
- Banning, A.P.; Serruys, P.; De Maria, G.L.; Ryan, N.; Walsh, S.; Gonzalo, N.; Jan van Geuns, R.; Onuma, Y.; Sabate, M.; Davies, J.; et al. Five-year outcomes after state-of-the-art percutaneous coronary revascularization in patients with de novo three-vessel disease: Final results of the SYNTAX II study. Eur. Heart J. 2022, 43, 1307–1316. [Google Scholar] [CrossRef] [PubMed]
- Waheed, N.; Elias-Smale, S.; Malas, W.; Maas, A.H.; Sedlak, T.L.; Tremmel, J.; Mehta, P.K. Sex differences in non-obstructive coronary artery disease. Cardiovasc. Res. 2020, 116, 829–840. [Google Scholar] [CrossRef] [PubMed]
- Asleh, R. Persistent sex differences in outcomes after coronary heart disease: Time to move from observation to action. Heart 2022, 108, 4–6. [Google Scholar] [CrossRef] [PubMed]
- Sato, Y.; Kawakami, R.; Sakamoto, A.; Cornelissen, A.; Mori, M.; Kawai, K.; Ghosh, S.; Romero, M.E.; Kolodgie, F.D.; Finn, A.V.; et al. Sex Differences in Coronary Atherosclerosis. Curr. Atheroscler. Rep. 2022, 24, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Urbanowicz, T.; Michalak, M.; Olasińska-Wiśniewska, A.; Haneya, A.; Straburzyńska-Migaj, E.; Bociański, M.; Jemielity, M. Gender differences in coronary artery diameters and survival results after off-pump coronary artery bypass (OPCAB) procedures. J. Thorac. Dis. 2021, 13, 2867–2873. [Google Scholar] [CrossRef]
- Sram, R.J. Impact of Air Pollution on the Health of the Population in Parts of the Czech Republic. Int. J. Environ. Res. Public Health 2020, 17, 6454. [Google Scholar] [CrossRef]
- Shen, L.J.; Wang, H.L.; Sun, J.J.; Liu, S.Y.; Liu, H.W.; Zhao, T.L. Pollution Characteristics of Carbonaceous Components in PM10 and PM2.5 of Road Dust Fall and Soil Dust in Xi’an. Huan Jing Ke Xue 2023, 44, 4843–4852. [Google Scholar]

{kind=link}
{kind=link}
| Parameters | Group 1 n = 44 | Group 2 n = 19 | p |
|---|---|---|---|
| Age (years; median, Q1–Q3) | 69 (64–74) | 68 (60–72) | 0.505 |
| Male sex (n, %) | 23 (52) | 15 (79) | 0.047 * |
| Interval in days between baseline and repeated exam (median, Q1–Q3) | 1699 (1310–1863) | 1881 (1407–2210) | 0.087 |
| Co-morbidities: | |||
| HA (n, %) | 27 (61) | 14 (74) | 0.401 |
| DM (n, %) | 10 (23) | 3 (16) | 0.738 |
| Hyperlipidemia (n, %) | 24 (55) | 6 (32) | 0.050 * |
| Thyroid disease (n, %) | 1 (2) | 1 (5) | 1.000 |
| COPD (n,%) | 1 (2) | 0 (0) | 1.000 |
| Kidney dysfunction (n, %) | 2 (5) | 0 (0) | 1.000 |
| AF (n,%) | 3 (7) | 0 (0) | 0.544 |
| Nicotine (n, %) | 2 (5) | 1 (5) | 1.000 |
| Stroke (n, %) | 1 (2) | 0 (0) | 1.000 |
| PAD (n, %) | 7 (16) | 0 (0) | 0.083 |
| Laboratory results (median, Q1–Q3) | |||
| WBC [× 109/L] | 7.69 (5.99–7.92) | 6.41 (5.40–7.85) | 0.540 |
| Hb [mmol/L] | 8.90 (8.10–9.20) | 8.85 (8.58–9.35) | 0.539 |
| Neutrophil count [× 109/L] | 4.91 (3.62–5.40) | 4.18 (3.42–4.98) | 0.476 |
| Lymphocyte count [× 109/L] | 1.73 (1.41–1.87) | 1.61 (1.14–2.10) | 0.704 |
| Plt count [× 109/L] | 242 (242–275) | 184 (154–258) | 0.268 |
| Hct [%] | 42 (40–43) | 43.5 (43–44) | 0.215 |
| Creatinine [umol/L] | 73 (66–84) | 81 (69–88) | 0.263 |
| LDL [mmol/L] | 2.4 (1.8–3.7) | 1.9 (1.6–2.7) | 0.007 * |
| HLD [mmol/L] | 1.3 (1.1–1.5) | 1.3 (1.0–1.6) | 0.651 |
| Triglycerides [mmol/L] | 1.3 (1.0–1.7) | 1.3 (0.9–1.6) | 0.909 |
| Labolatory Results | Group 1 n = 44 | Group 2 n = 19 | p (Mann–Whitney) |
|---|---|---|---|
| Laboratory results (median, Q1–Q3) | |||
| WBC [× 109/L] | 6.39 (5.84–6.96) | 6.35 (6.12–6.47) | 0.885 |
| Hb [mmol/L] | 8.45 (8.35–8.90) | 8.50 (8.45–8.60) | 0.942 |
| Neutrophil count [× 109/L] | 4.01 (3.15–4.66) | 3.00 (2.94–3.52) | 0.247 |
| Lymphocyte count [× 109/L] | 1.67 (1.18–1.89) | 2.11 (1.86–2.22) | 0.311 |
| Plt count [× 109/L] | 202 (155–256) | 156 (154–323) | 0.988 |
| Hct [%] | 40 (39–42) | 40 (39–41) | 0.883 |
| Creatinine [umol/L] | 92 (84–103) | 94 (78–112) | 0.885 |
| LDL [mmol/L] | 1.61 (1.29–1.89) | 1.74 (1.46–1.89) | 0.686 |
| HDL [mmol/L] | 1.17 (1.03–1.42) | 1.23 (0.98–1.5) | 0.893 |
| Triglicerydes [mmol/L] | 1.44 (0.99–1.65) | 1.30 (1.0–1.71) | 0.941 |
| CRP protein [mg/L] | 1.40 (1.30–1.85) | 1.80 0(1.60–1.95) | 0.653 |
| Hb1Ac (%) | 5.80 (5.8–6.1) | 6.4 (5.8–6.8) | 0.744 |
| Parameters | Group 1 n = 44 | Group 2 n = 19 |
|---|---|---|
| Interval in days (median (Q1–Q3) | 1699 (1310–1863) | 1881 (1407–2210) |
| Syntax score in de novo lesions | 0 (0) | 7 (4–9.5) |
| (median (Q1–Q3) | ||
| Coronary angiography results: | ||
| LMCA | ||
| Stenosis > 30% (n, %) | 1 (2) | 0 (0) |
| Stenosis > 50% (n, %) | 0 (0) | 0 (0) |
| Occluded (n, %) | 0 (0) | 0 (0) |
| LAD | ||
| Stenosis > 50% (n, %) | 0 (0) | 16.(84) |
| Stenosis > 70% (n, %) | 0 (0) | 7 (37) |
| Occluded (n, %) | 0 (0) | 1 (5) |
| Dg | ||
| Stenosis > 50% (n, %) | 0 (0) | 4 (21) |
| Stenosis > 70% (n, %) | 0 (0) | 2 (11) |
| Occluded (n, %) | 0 (0) | 0 (0) |
| Cx | ||
| Stenosis > 50% (n, %) | 0 (0) | 13 (68) |
| Stenosis > 70% (n, %) | 0 (0) | 4 (21) |
| Occluded (n, %) | 0 (0) | 0 (0) |
| RCA | ||
| Stenosis > 50% (n, %) | 0 (0) | 18 (95) |
| Stenosis > 70% (n, %) | 0 (0) | 6 (26) |
| Occluded (n, %) | 0 (0) | 2 (11) |
| Air Pollutants Annual Concentration [µg/m3] | 0 n = 44 | 1 n = 19 | p |
|---|---|---|---|
| PM 2.5 | |||
| median overall exposure (Q1–Q3) | 15.3 (13.9–16.9) | 17.2 (14.7–19.0) | 0.054 |
| median 2019 exposure (Q1–Q3) | 17 (16.1–18.6) | 18.5 (15.5–18.9) | 0.635 |
| median 2020 exposure (Q1–Q3) | 13.8 (10.6–16.0) | 15.1 (13.0–19.9) | 0.020 |
| median 2021 exposure (Q1–Q3) | 15.6 (13.9–17.7) | 17.2 (15.2–19.5) | 0.040 |
| median 2022 exposure (Q1–Q3) | 15.4 (13.7–17.3) | 16.9 (15.7–18.8) | 0.093 |
| PM 10 | |||
| median overall exposure (Q1–Q3) | 21.7 (19.9–23.4) | 28.4 (27.1–30.1) | <0.001 * |
| median 2019 exposure (Q1–Q3) | 22.4 (20.9–24.7) | 29.2 (28.5–29.9) | <0.001 * |
| median 2020 exposure (Q1–Q3) | 19.6 (17.5–21.5) | 26.7 (24.9–29.4) | <0.001 * |
| median 2021 exposure (Q1–Q3) | 22.5 (21.7–24.5) | 29.5 (28.2–30.6) | <0.001 * |
| median 2022 exposure (Q1–Q3) | 21.4 (19.7–23.5) | 27.8 (25.8–30.3) | <0.001 * |
| NO2 | |||
| median overall exposure (Q1–Q3) | 13.3 (10.1–17.6) | 15.7 (10.7–22.8) | 0.637 |
| median 2019 exposure (Q1–Q3) | 13.7 (10.5–21.9) | 14.6 (10.5–17.3) | 0.611 |
| median 2020 exposure (Q1–Q3) | 12.7 (9.8–16.6) | 14.9 (12.7–18.9) | 0.680 |
| median 2021 exposure (Q1–Q3) | 14 (12.0–17.1) | 14.9 (12.7–18.9) | 0.520 |
| median 2022 exposure (Q1–Q3) | 11.9 (9.6–17.4) | 13.6 (9.7–19.5) | 0.510 |
| PM10 [µg/m3] | Group 0 n = 44 | Group 1 n = 19 | p |
|---|---|---|---|
| pts exposed to PM10 > 10 (n, %) | 44 (100) | 19 (100) | 0.508 |
| pts exposed to PM10 > 15 ** (n, %) | 43 (98) | 19 (100) | 0.011 * |
| pts exposed to PM10 > 20 *** (n, %) | 32 (73) | 19 (100) | <0.001 * |
| pts exposed to PM10 > 25 (n, %) | 2 (5) | 16 (84) | <0.001 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Urbanowicz, T.; Skotak, K.; Olasińska-Wiśniewska, A.; Filipiak, K.J.; Bratkowski, J.; Wyrwa, M.; Sikora, J.; Tyburski, P.; Krasińska, B.; Krasiński, Z.; et al. Long-Term Exposure to PM10 Air Pollution Exaggerates Progression of Coronary Artery Disease. Atmosphere 2024, 15, 216. https://doi.org/10.3390/atmos15020216
Urbanowicz T, Skotak K, Olasińska-Wiśniewska A, Filipiak KJ, Bratkowski J, Wyrwa M, Sikora J, Tyburski P, Krasińska B, Krasiński Z, et al. Long-Term Exposure to PM10 Air Pollution Exaggerates Progression of Coronary Artery Disease. Atmosphere. 2024; 15(2):216. https://doi.org/10.3390/atmos15020216
Chicago/Turabian StyleUrbanowicz, Tomasz, Krzysztof Skotak, Anna Olasińska-Wiśniewska, Krzysztof J. Filipiak, Jakub Bratkowski, Michał Wyrwa, Jędrzej Sikora, Piotr Tyburski, Beata Krasińska, Zbigniew Krasiński, and et al. 2024. "Long-Term Exposure to PM10 Air Pollution Exaggerates Progression of Coronary Artery Disease" Atmosphere 15, no. 2: 216. https://doi.org/10.3390/atmos15020216
APA StyleUrbanowicz, T., Skotak, K., Olasińska-Wiśniewska, A., Filipiak, K. J., Bratkowski, J., Wyrwa, M., Sikora, J., Tyburski, P., Krasińska, B., Krasiński, Z., Tykarski, A., & Jemielity, M. (2024). Long-Term Exposure to PM10 Air Pollution Exaggerates Progression of Coronary Artery Disease. Atmosphere, 15(2), 216. https://doi.org/10.3390/atmos15020216