
Construction of Multipollutant Air Quality Health Index and Susceptibility Analysis Based on Mortality Risk in Beijing, China

Abstract
:1. Introduction
2. Methodology
2.1. Data Sources
2.2. Statistical Analysis
2.2.1. Estimating the Associations of Air Pollutants with Mortality
- To control for long-term and seasonal trends in daily deaths, a natural spline (ns) function for dates was incorporated to process nonlinear trends and serial correlations in daily deaths over time.
- The degree of freedom of the time-smooth function determined the degree to which time trends were excluded. The partial autocorrelation function (PACF) was used to guide the selection of the degree of freedom. Through fitting of the GAM and plotting of the PACF graph with a 30-day lag, when the absolute value of the first 2-day lag in the graph was <0.1, the model was regarded as having favorable control of the serial correlation. When more than one parameter satisfied this condition, the parameter with the smallest sum of the 30-day cumulative absolute values was selected. The annual ν for the final fit was 8.
- An indicator variable for the DOW was included in the base model to exclude the natural fluctuations in daily mortality within a given week.
- The mean temperature, relative humidity, and wind velocity were included in the base model to control for the confounding effects of meteorological factors on the association between air pollution and daily mortality. An ns function was adopted to control for the confounding effect of the nonlinear relationship between meteorological factors and mortality; the degree of freedom of the ns function was set to 3 throughout the study. Because of the strong correlation and concurvity of the weather variables between two or more consecutive days, only the confounding effect of the weather on the day of death was controlled [32,33,34].
2.2.2. Construction of the Beijing AQHI
2.2.3. Evaluation of the Validity of the AQHI
3. Results and Discussion
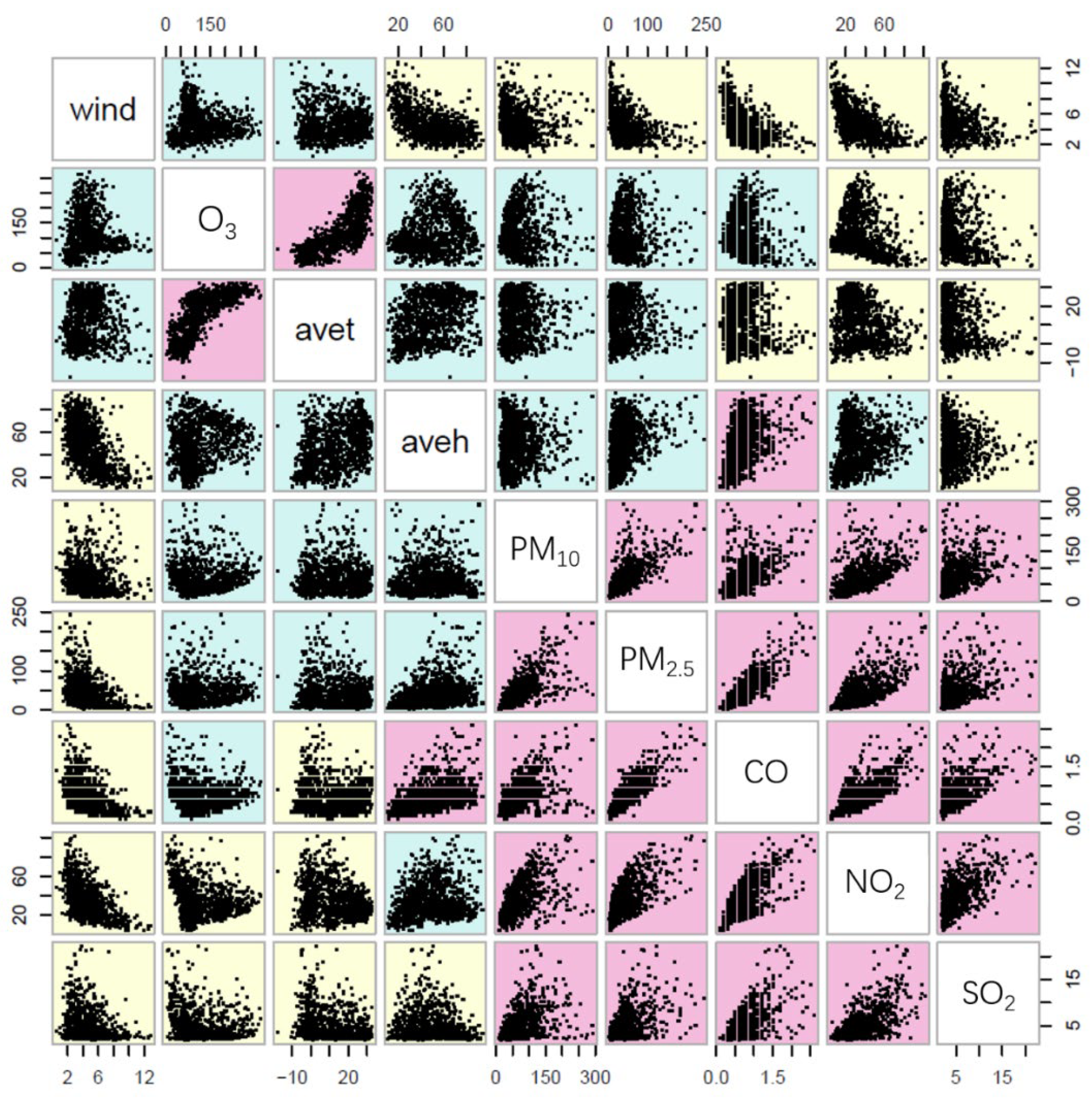
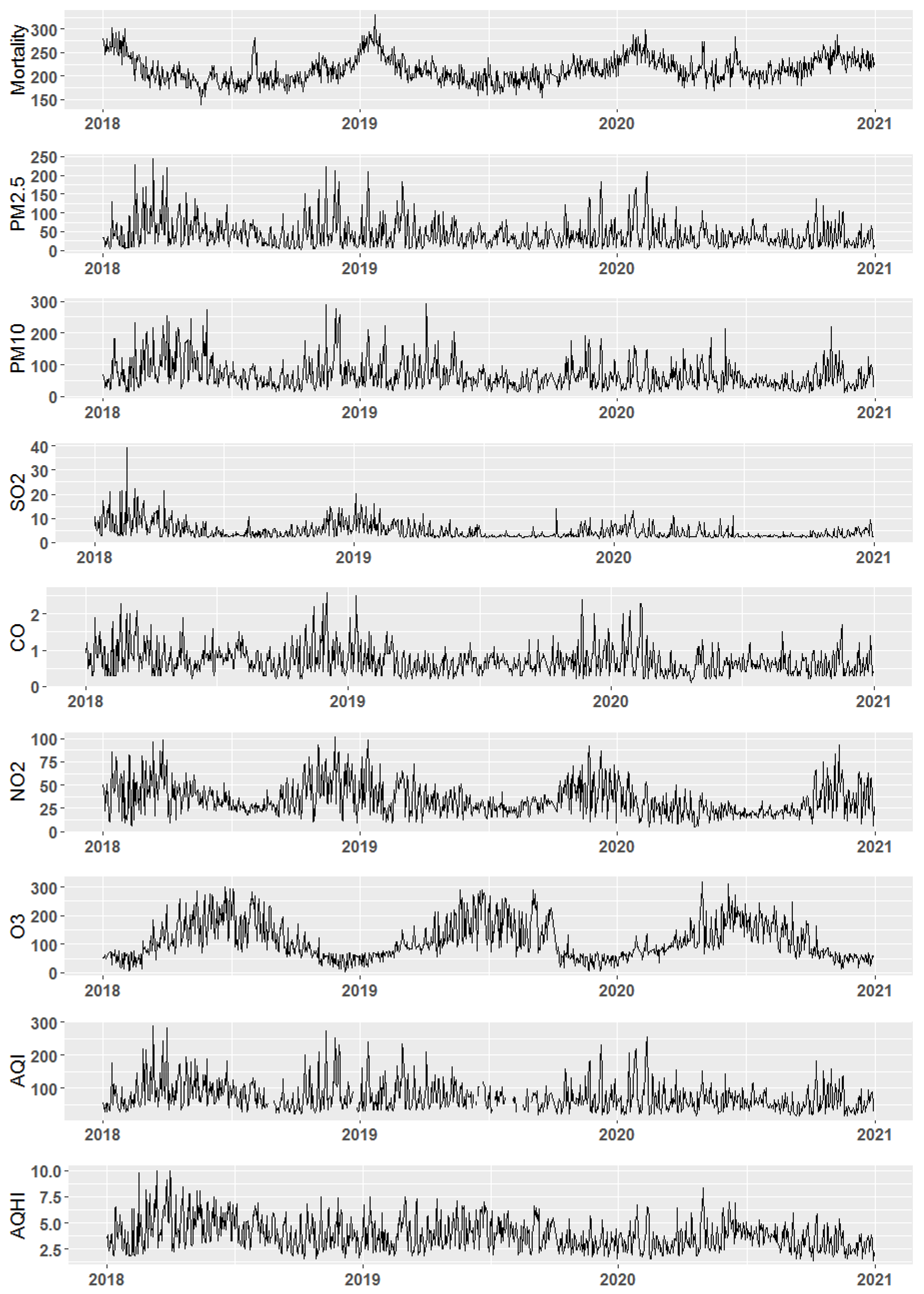
3.1. Analysis of Air Pollution in Beijing
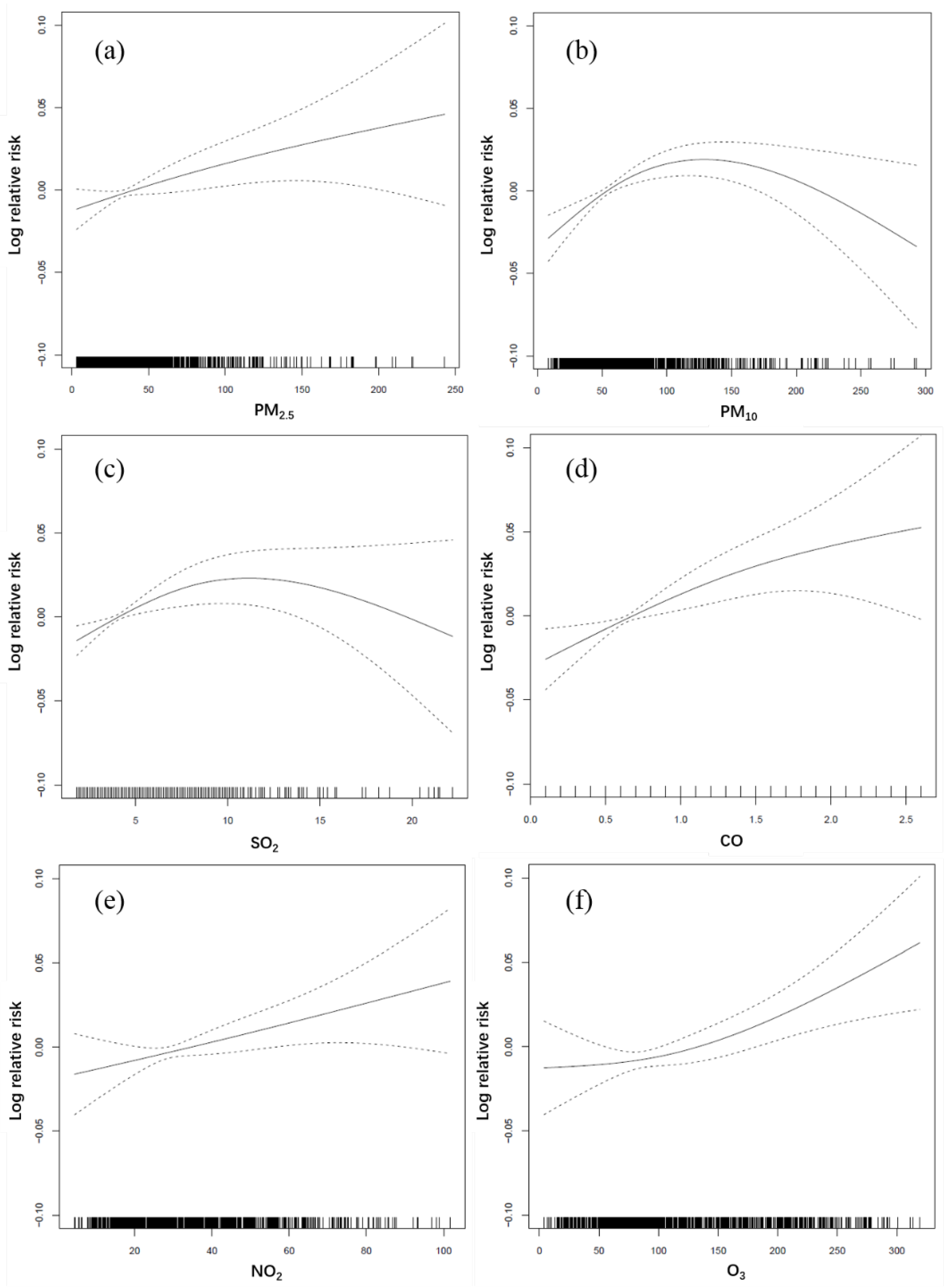
3.2. Health Effects of Air Pollutants in Beijing
3.3. Factors Increasing the Susceptibility of the Population to the Health Effects of Air Pollution
3.4. Construction of the Beijing AQHI
3.4.1. Construction of the AQHI
3.4.2. Construction of the Specific AQHI
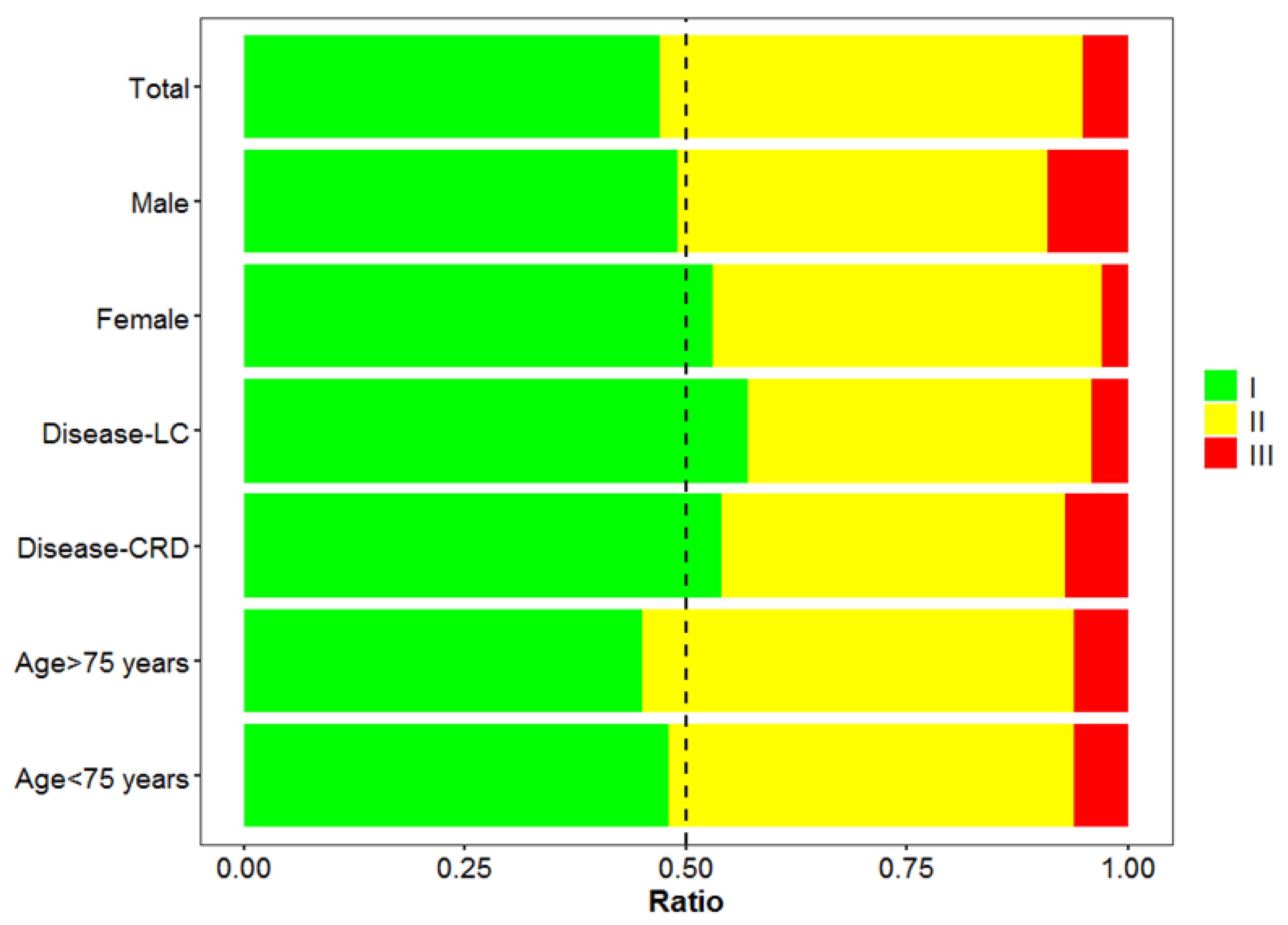
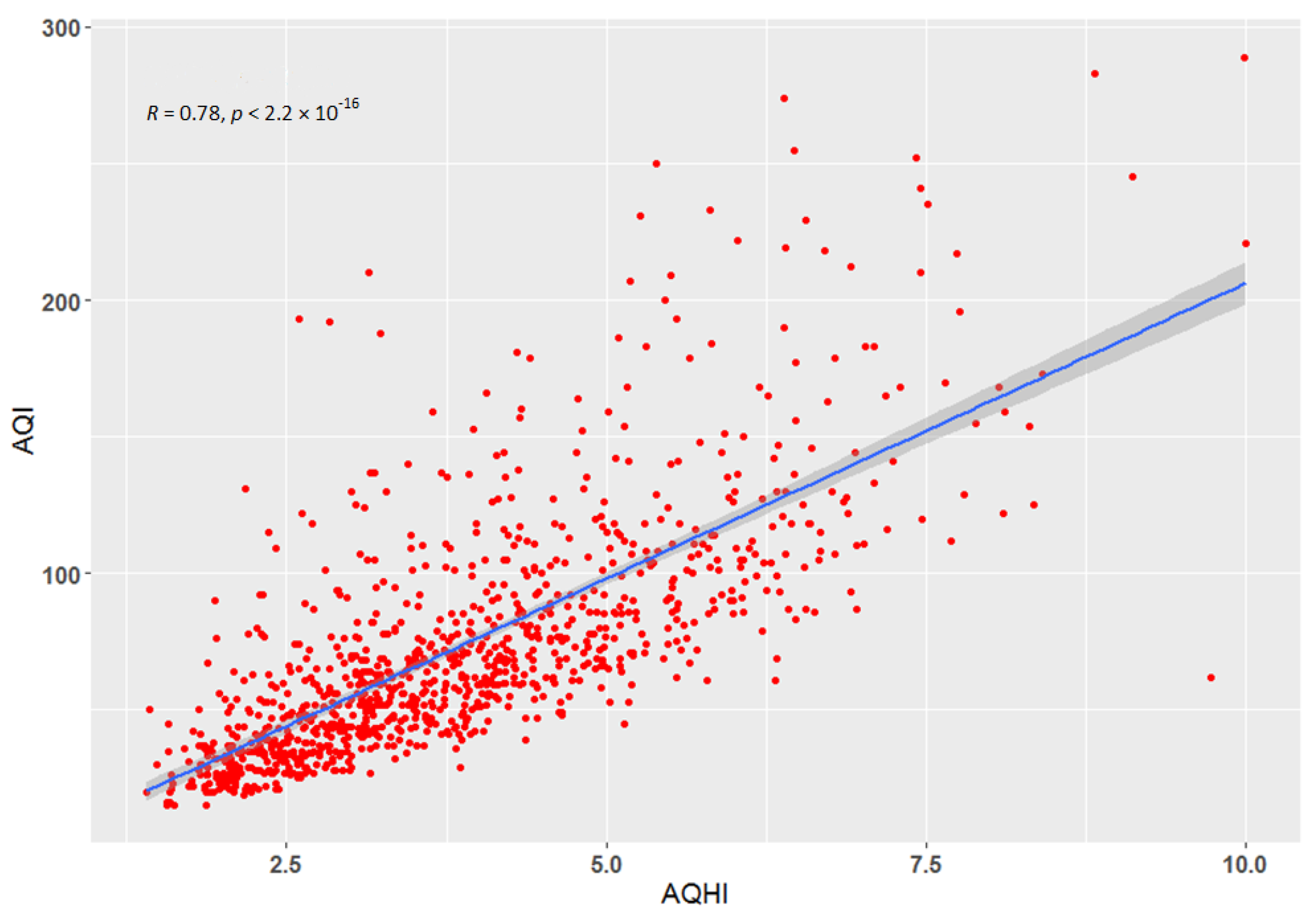
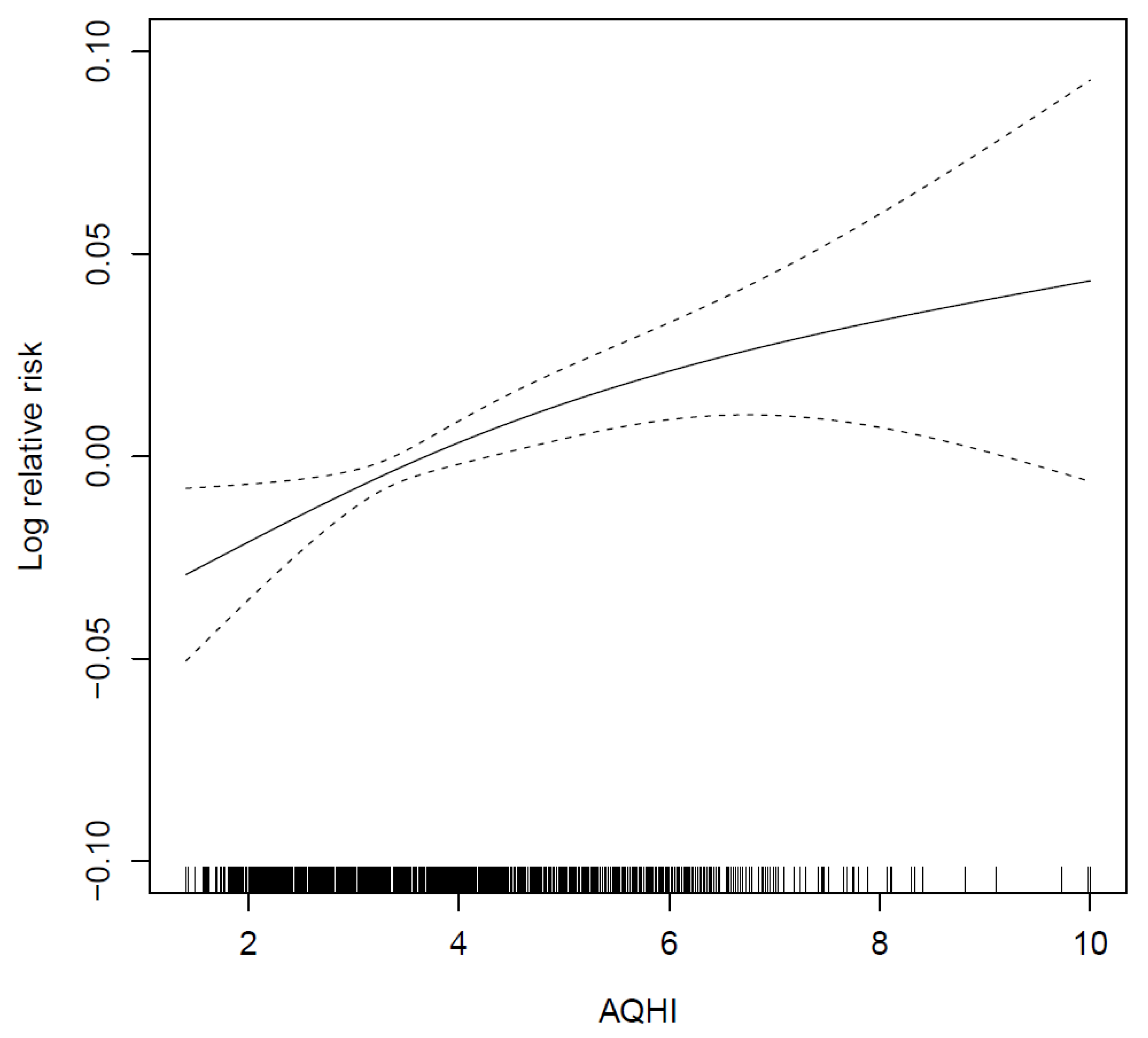
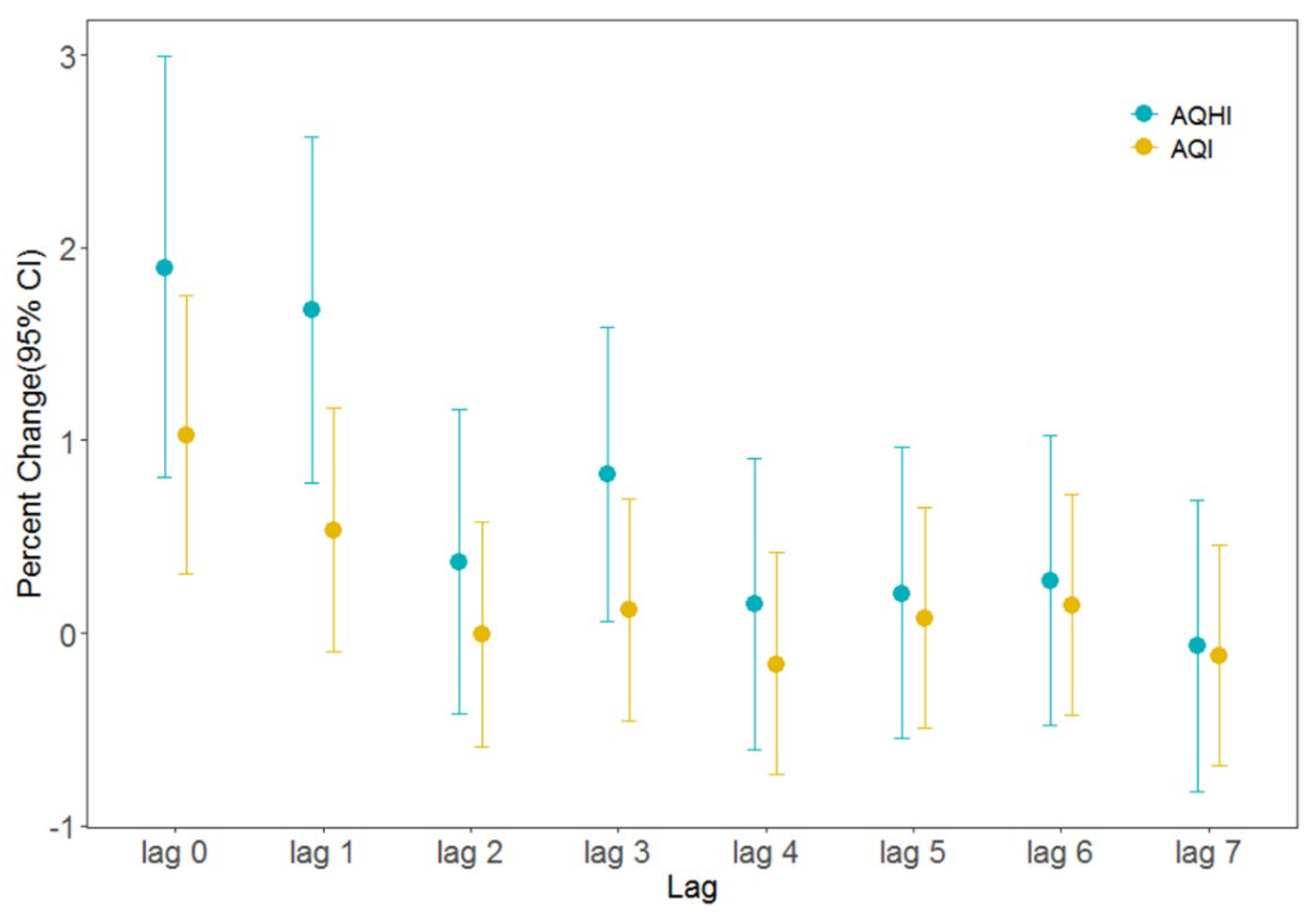
3.5. Validity Analysis of the AQHI
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Evolution of WHO Air Quality Guidelines: Past, Present and Future; World Health Organization: Geneva, Switzerland; Regional Office for Europe: Copenhagen, Denmark, 2017; Available online: https://apps.who.int/iris/handle/10665/341912 (accessed on 21 March 2022).
- World Health Organization. Ambient Air Pollution: A Global Assessment of Exposure and Burden of Disease; World Health Organization: Geneva, Switzerland, 2016; Available online: https://apps.who.int/iris/handle/10665/250141 (accessed on 21 March 2022).
- Babatola, S.S. Global burden of diseases attributable to air pollution. J. Public Health Afr. 2018, 9, 813. [Google Scholar] [CrossRef] [PubMed]
- Mathers, C.; Stevens, G.; Hogan, D.; Mahanani, W.R.; Ho, J. Disease Control Priorities: Improving Health and Reducing Poverty; World Bank: Washington, DC, USA, 2017. [Google Scholar]
- Brunekreef, B.; Holgate, S.T. Air pollution and health. Lancet 2002, 360, 1233–1242. [Google Scholar] [CrossRef]
- He, F.; Shaffer, M.L.; Rodriguez-Colon, S.; Yanosky, J.D.; Bixler, E.; Cascio, W.E.; Liao, D.P. Acute effects of fine particulate air pollution on cardiac arrhythmia: The APACR study. Environ. Health Perspect. 2011, 119, 927–932. [Google Scholar] [CrossRef]
- Hwang, B.F.; Lee, Y.L. Air pollution and prevalence of bronchitic symptoms among children in Taiwan. Chest 2010, 138, 956–964. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.Y.; Yu, Z.B.; Qiu, H.Y.; Wang, J.B.; Chen, X.Y. Association between ambient air pollutants and preterm birth in Ningbo, China: A time-series study. BMC Pediatr. 2018, 18, 305. [Google Scholar] [CrossRef] [PubMed]
- Campbell, L.D.; Pruss, U.A. Climate change, air pollution and noncommunicable diseases. Bull. World Health Organ. 2019, 97, 160–161. [Google Scholar] [CrossRef] [PubMed]
- Stanaway, J.D.; Afshin, A.; Gakidou, E.; Lim, S.S.; Abate, D.; Abate, K.H.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; et al. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for195countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1923–1994. [Google Scholar] [CrossRef]
- Yang, G.; Wang, Y.; Zeng, Y.; Gao, G.F.; Liang, X.; Zhou, M.; Wan, X.; Yu, S.; Jiang, Y.; Naghavi, M. Rapid health transition in China, 1990–2010: Findings from the Global Burden of Disease Study 2010. Lancet 2013, 381, 1987–2015. [Google Scholar] [CrossRef]
- Wu, Y.F.; Jin, A.; Xie, G.Q.; Wang, L.; Liu, K. The 20 most important and most preventable health problems of China: A Delphi consultation of Chinese experts. Am. J. Public Health 2018, 108, 1592–1598. [Google Scholar] [CrossRef]
- World Health Organization. WHO Global Air Quality Guidelines: Particulate Matter (Pm2.5 and Pm10), Ozone, Nitrogen Dioxide, Sulfur Dioxide and Carbon Monoxide; World Health Organization: Geneva, Swtizerland, 2021; Available online: https://apps.who.int/iris/handle/10665/345329 (accessed on 21 March 2022).
- Plaia, A.; Ruggieri, M. Air quality indices: A review. Rev. Environ. Sci. Bio/Technol. 2011, 10, 165–179. [Google Scholar] [CrossRef]
- Stieb, D.M.; Burnett, R.T.; Smith-Doiron, M.; Brion, O.; Shin, H.H.; Economou, V. A new multipollutant, no-threshold air quality health index based on short-term associations observed in daily time-series analyses. J. Air Waste Manag. Assoc. 2008, 58, 435–450. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.J.; Chen, B.H.; Kan, H.D. Air quality health index in China: A pilot study. China Environ. Sci. 2013, 33, 2081–2086. [Google Scholar] [CrossRef]
- Li, X.; Xiao, J.P.; Lin, H.L.; Liu, T.; Qian, Z.M.; Zeng, W.L.; Guo, L.C.; Ma, W.J. The construction and validity analysis of AQHI based on mortality risk: A case study in Guangzhou, China. Environ. Pollut. 2017, 220, 487–494. [Google Scholar] [CrossRef]
- Cairncross, E.K.; John, J.; Zunckel, M. A novel air pollution index based on the relative risk of daily mortality associated with short-term exposure to common air pollutants. Atmos. Environ. 2007, 41, 8442–8454. [Google Scholar] [CrossRef]
- Mason, T.G.; Schooling, C.M.; Chan, K.P.; Tian, L.W. An evaluation of the air quality health index program on respiratory diseases in Hong Kong: An interrupted time series analysis. Atmos. Environ. 2019, 211, 151–158. [Google Scholar] [CrossRef]
- Spurr, K.; Pendergast, N.; MacDonald, S. Assessing the use of the Air Quality Health Index by vulnerable populations in a ‘Lowrisk’ region: A pilot study. Can. J. Respir. Ther. 2014, 50, 45–49. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4456833/ (accessed on 21 March 2022).
- To, T.; Feldman, L.; Simatovic, J.; Gershon, A.S.; Dell, S.; Su, J.D.; Foty, R.; Licskai, C. Health risk of air pollution on people living with major chronic diseases: A Canadian population-based study. BMJ Open 2015, 5, 9075. [Google Scholar] [CrossRef]
- Olstrup, H. An air quality health index (AQHI) with different health outcomes based on the air pollution concentrations in Stockholm during the period of 2015–2017. Atmosphere 2020, 11, 192. [Google Scholar] [CrossRef]
- Fan, L. Preliminary Establishment of an Air Quality Health Index Based on the Relationship between Exposure to Air Pollution and Years of Life Lost; Tianjin Medical University: Tianjin, China, 2019. [Google Scholar]
- Liao, T.T.; Jiang, W.T.; Ouyang, Z.W.; Hu, S.X.; Wu, J.Q.; Zhao, B.; Wang, B.H.; Wang, S.G.; Sun, Y. Evaluation of the health risk of air pollution in major Chinese cities using a risk-based, multi-pollutant air quality health index during 2014–2018. Air Qual. Atmos. Health 2021, 14, 1605–1617. [Google Scholar] [CrossRef]
- Zhang, L.J.; Xu, H.H.; Guo, C.Y.; Chen, J.; Dong, C.Y.; Zhang, J.H.; Shi, Y.W.; Xu, D.; Ling, L.M.; Zhang, B.; et al. Constructing an air quality health index for children: A case study in Shanghai, China. Atmos. Environ. 2021, 267, 118765. [Google Scholar] [CrossRef]
- Huang, W.Z.; He, W.Y.; Knibbs, L.D.; Jalaludin, B.; Guo, Y.M.; Morawska, L.; Heinrich, J.; Chen, D.H.; Yu, Y.J.; Zeng, X.W.; et al. Improved morbidity-based air quality health index development using Bayesian multi-pollutant weighted model. Environ. Res. 2022, 204, 112397. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.J. The Health Effects of Complex Air Pollution in 17 Chinese Cities; Fudan University: Shanghai, China, 2013. [Google Scholar]
- Zhang, J.Y.; Guo, Y.M.; Meng, H.Y.; Jia, Y.P.; Luo, F.J.; Pan, X.C. A time-series study on the relationship between air pollution and citizens’ daily deaths in Chaoyang District, Beijing. Environ. Health. 2010, 27, 797–800. [Google Scholar] [CrossRef]
- Chen, R.J.; Li, Y.; Ma, Y.J.; Pan, G.W.; Zeng, G.; Xu, X.H.; Chen, B.H.; Kan, H.D. Coarse particles and mortality in three Chinese cities: The China Air Pollution and Health Effects Study (CAPES). Sci. Total Environ. 2011, 409, 4934–4938. [Google Scholar] [CrossRef] [PubMed]
- Du, X.H.; Chen, R.J.; Meng, X.; Liu, C.; Niu, Y.; Wang, W.D.; Li, S.Q.; Kan, H.D.; Zhou, M.G. The establishment of National Air Quality Health Index in China. Environ. Int. 2020, 138, 105594. [Google Scholar] [CrossRef]
- Chen, R.J.; Yin, P.; Meng, X.; Wang, L.J.; Liu, C.; Niu, Y.; Lin, Z.J.; Liu, Y.N.; Liu, J.M.; Qi, J.L.; et al. Associations between ambient nitrogen dioxide and daily cause-specific mortality evidence from 272 Chinese cities. Epidemiology 2018, 29, 482–489. [Google Scholar] [CrossRef]
- Qian, Z.; He, Q.; Lin, H.M.; Kong, L.; Liao, D.; Dan, J.; Bentley, C.M.; Wang, B. Association of daily cause-specific mortality with ambient particle air pollution in Wuhan, China. Environ. Res. 2007, 105, 380–389. [Google Scholar] [CrossRef]
- Welty, L.; Zeger, S.L. Are the acute effects of particulate matter on mortality in the National Morbidity, Mortality, and Air Pollution Study the result of inadequate control for weather and season? A sensitivity analysis using flexible distributed lag models. Am. J. Epidemiol. 2005, 162, 80–88. [Google Scholar] [CrossRef]
- Teng, B.; Zhang, X.L.; Yi, C.H.; Zhang, Y.; Ye, S.F.; Wang, Y.F. The association between ambient air pollution and allergic rhinitis: Further epidemiological evidence from Changchun, Northeastern China. Int. J. Environ. Res. Public Health. 2017, 14, 226. [Google Scholar] [CrossRef]
- Pope, C.A.; Burnett, R.T.; Krewski, D.; Jerrett, M.; Shi, Y.; Calle, E.E.; Thun, M.J. Cardiovascular mortality and exposure to airborne fine particulate matter and cigarette smoke shape of the exposure-response relationship. Circulation 2009, 120, 941–948. [Google Scholar] [CrossRef]
- Gu, D.F.; Kelly, T.N.; Wu, X.G.; Chen, J.; Samet, J.M.; Huang, J.F.; Zhu, M.L.; Chen, J.C.; Chen, C.S.; Duan, X.F.; et al. Mortality attributable to smoking in China. N. Engl. J. Med. 2009, 360, 1911. [Google Scholar] [CrossRef]
- Künzli, N.; Jerrett, M.; Mack, W.J.; Beckerman, B.; Labree, L.; Gillil, F.; Thomas, D.; Peters, J.; Hodis, H.N. Ambient air pollution and atherosclerosis in Los Angeles. Environ. Health Perspect. 2005, 113, 201–206. [Google Scholar] [CrossRef] [PubMed]
- Shang, Y.; Sun, Z.W.; Cao, J.J.; Wang, X.M.; Zhong, L.J.; Bi, X.H.; Li, H.; Liu, W.X.; Zhu, T.; Huang, W. Systematic review of Chinese studies of short-term exposure to air pollution and daily mortality. Environ. Int. 2013, 54, 100–111. [Google Scholar] [CrossRef] [PubMed]
- Qian, Z.M.; He, Q.C.; Lin, H.M.; Kong, L.L.; Liao, D.P. Short-term effects of gaseous pollutants on cause-specific mortality in Wuhan, China. J. Air Waste Manag. Assoc. 2007, 57, 785–793. [Google Scholar] [CrossRef] [PubMed]
- Tao, Y.B.; Huang, W.; Huang, X.L.; Zhong, L.J.; Lu, S.E.; Li, Y.; Dai, L.Z.; Zhang, Y.H.; Zhu, J. Estimated acute effects of ambient ozone and nitrogen dioxide on mortality in the Pearl River Delta of Southern China. Environ. Health Perspect. 2012, 120, 393–398. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.; Pan, G.; Kan, H.; Tan, J.; Song, W.; Wu, Z.; Xu, X.; Xu, Q.; Jiang, C.; Chen, B. Ambient air pollution and daily mortality in Anshan, China: A time-stratified case-crossover analysis. Sci. Total Environ. 2010, 408, 6086–6091. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Mean | SD | Min | P25 | Median | P75 | Max | IQR |
|---|---|---|---|---|---|---|---|---|
| PM2.5 (μg/m3) | 42.55 | 36.28 | 3 | 16.75 | 33 | 55.45 | 242.9 | 38.7 |
| PM10 (μg/m3) | 67.87 | 45.2 | 8.4 | 35.55 | 56.1 | 85.05 | 292.9 | 49.5 |
| SO2 (μg/m3) | 4.68 | 3.3 | 1.8 | 2.6 | 3.3 | 5.65 | 39.1 | 3.05 |
| CO (mg/m3) | 0.7 | 0.38 | 0.1 | 0.4 | 0.6 | 0.9 | 2.6 | 0.5 |
| NO2 (μg/m3) | 34.34 | 17.49 | 4.4 | 21.75 | 29.7 | 44.25 | 101.7 | 22.5 |
| O3 (μg/m3) | 112.64 | 66.01 | 3.8 | 63.85 | 91.9 | 158.95 | 319.2 | 95.1 |
| AVET (°C) | 13.71 | 11.43 | −17.8 | 2.6 | 14.3 | 24.6 | 32.4 | 22 |
| Wind (mph) | 4.57 | 1.91 | 0.5 | 3.1 | 4.3 | 5.5 | 12.8 | 2.4 |
| AVEH (%) | 49.08 | 18.71 | 11 | 34 | 49 | 64 | 94 | 30 |
| Mortality | 214 | 28 | 138 | 194 | 210 | 231 | 331 | 37 |
| Population Classification | PM2.5 | SO2 | NO2 | O3 |
|---|---|---|---|---|
| Overall | 0.195 (0.002, 0.387) | 2.133 (0.235, 4.067) | 0.524 (0.037, 1.014) | 0.266 (0.144, 0.389) |
| 75 years and younger | 0.101 (−0.175, 0.378) | 2.045 (−0.530, 4.686) | 0.409 (−0.169, 0.991) | 0.230 (0.058, 0.403) |
| Older than 75 years | 0.215 (−0.028, 0.459) | 2.390 (0.016, 4.820) | 0.537 (−0.080, 1.157) | 0.342 (0.183, 0.500) |
| Men | 0.123 (−0.116, 0.363) | 1.594 (−0.619, 3.855) | 0.265 (−0.341, 0.874) | 0.298 (0.132, 0.464) |
| Women | 0.235 (−0.034, 0.504) | 3.305 (0.657, 6.023) | 0.781 (0.217, 1.347) | 0.305 (0.096, 0.513) |
| Low education level | 0.184 (−0.047, 0.416) | 1.861 (−0.271, 4.038) | 0.448 (−0.034, 0.933) | 0.338 (0.158, 0.517) |
| High education level | 0.142 (−0.154, 0.439) | 2.948 (0.009, 5.973) | 0.794 (0.042, 1.553) | 0.245 (0.059, 0.431) |
| Cardiovascular disease | 0.181 (−0.092, 0.455) | 1.648 (−1.028, 4.397) | 0.505 (−0.190, 1.205) | 0.369 (0.156, 0.583) |
| Lung cancer | 0.461 (0.056, 0.868) | 7.878 (2.148, 13.929) | 0.897 (−0.286, 2.093) | 0.369 (0.025, 0.715) |
| Chronic respiratory disease | 0.591 (−0.050, 1.238) | 4.245 (−1.435, 10.253) | 0.673 (−0.405, 1.761) | 0.723 (0.300, 1.148) |
| AQHI | Health Risk Level | Warning Color | Susceptible Population | General Population |
|---|---|---|---|---|
| 0–3 | Low | Green | Normal outdoor activities | Normal outdoor activities |
| 4–6 | Moderate | Yellow | Reduction in outdoor activities is required | Reduction in daily outdoor activities is not required |
| 7–10 | High | Red | Older adults, children, and the susceptible population must reduce their outdoor activities | Individuals with symptoms such as coughing and sore throat must reduce their outdoor activities |
| >10 | Severe | Brown | Older adults, children, and the susceptible population must avoid outdoor activities | All populations must reduce their outdoor activities |
| Classification | AQHI | S-AQHI |
|---|---|---|
| Overall | 0.938 (0.401, 1.477) | —— |
| Men | 0.850 (0.177, 1.528) | 0.938 (0.388, 1.490) |
| Women | 1.254 (0.511, 2.002) | 1.182 (0.411, 1.958) |
| ≤75 years | 0.730 (0.103, 1.360) | 0.765 (0.130, 1.405) |
| >75 years | 1.196 (0.523, 1.873) | 1.236 (0.563, 1.912) |
| Lung cancer | 1.579 (0.497, 2.674) | 1.557 (0.497, 2.628) |
| Chronic respiratory disease | 1.140 (−0.148, 2.444) | 1.175 (−0.076, 2.442) |
| Index | Mean | SD | Min | P25 | P50 | P75 | Max | IQR |
|---|---|---|---|---|---|---|---|---|
| AQI | 72.75 | 42.75 | 15 | 43 | 63 | 90 | 289 | 47 |
| AQHI | 3.85 | 1.46 | 1.41 | 2.71 | 3.6 | 4.72 | 10 | 2.01 |
| Region | Period | PM10 | PM2.5 | O3 | SO2 | NO2 | Reference |
|---|---|---|---|---|---|---|---|
| Beijing | 2018–2020 | —— | 0.0001945 | 0.000266 | 0.0021108 | 0.0005228 | This research |
| Beijing | 2001–2010 | 0.00026 | 0.00047 | 0.00032 | —— | —— | [27] |
| Beijing | 2004–2008 | 0.00025 | —— | —— | 0.00047 | 0.00055 | [28] |
| Beijing | 2007–2008 | —— | 0.00053 | —— | —— | —— | [29] |
| China | 2013–2015 | —— | 0.000187 | 0.000119 | —— | 0.000675 | [30] |
| China | 2002–2012 | —— | 0.00038 | 0.00048 | —— | —— | [38] |
| China | 2001–2010 | 0.00019 | —— | —— | —— | 0.00061 | [27] |
| Tianjin | 2014–2017 | 0.000185 | 0.000234 | 0.000558 | 0.000740 | 0.000476 | [23] |
| Shanghai | 2001–2010 | 0.00085 | 0.00019 | 0.00031 | —— | —— | [27] |
| Guangzhou | 2012–2015 | —— | 0.000092 | 0.000036 | 0.000251 | 0.000148 | [17] |
| Wuhan | 2000–2004 | —— | —— | 0.00022 | 0.00001 | 0.00143 | [39] |
| Pearl river delta | 2006–2008 | 0.00079 | —— | 0.00081 | —— | 0.00195 | [40] |
| Anshan | 2004–2005 | 0.00024 | —— | —— | 0.00027 | 0.00130 | [41] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, Y.; Ding, D.; Ji, X.; Zhang, X.; Zhou, P.; Dou, Y.; Dan, M.; Shu, M. Construction of Multipollutant Air Quality Health Index and Susceptibility Analysis Based on Mortality Risk in Beijing, China. Atmosphere 2022, 13, 1370. https://doi.org/10.3390/atmos13091370
Wang Y, Ding D, Ji X, Zhang X, Zhou P, Dou Y, Dan M, Shu M. Construction of Multipollutant Air Quality Health Index and Susceptibility Analysis Based on Mortality Risk in Beijing, China. Atmosphere. 2022; 13(9):1370. https://doi.org/10.3390/atmos13091370
Chicago/Turabian StyleWang, Yu, Ding Ding, Xiaohui Ji, Xuelei Zhang, Pengyao Zhou, Yan Dou, Mo Dan, and Mushui Shu. 2022. "Construction of Multipollutant Air Quality Health Index and Susceptibility Analysis Based on Mortality Risk in Beijing, China" Atmosphere 13, no. 9: 1370. https://doi.org/10.3390/atmos13091370
APA StyleWang, Y., Ding, D., Ji, X., Zhang, X., Zhou, P., Dou, Y., Dan, M., & Shu, M. (2022). Construction of Multipollutant Air Quality Health Index and Susceptibility Analysis Based on Mortality Risk in Beijing, China. Atmosphere, 13(9), 1370. https://doi.org/10.3390/atmos13091370