
How Nanoparticle Aerosols Transport through Multi-Stenosis Sections of Upper Airways: A CFD-DPM Modelling

 , ,
, ,  , ,
, ,  ,
, 

Abstract
:1. Introduction
2. Methods
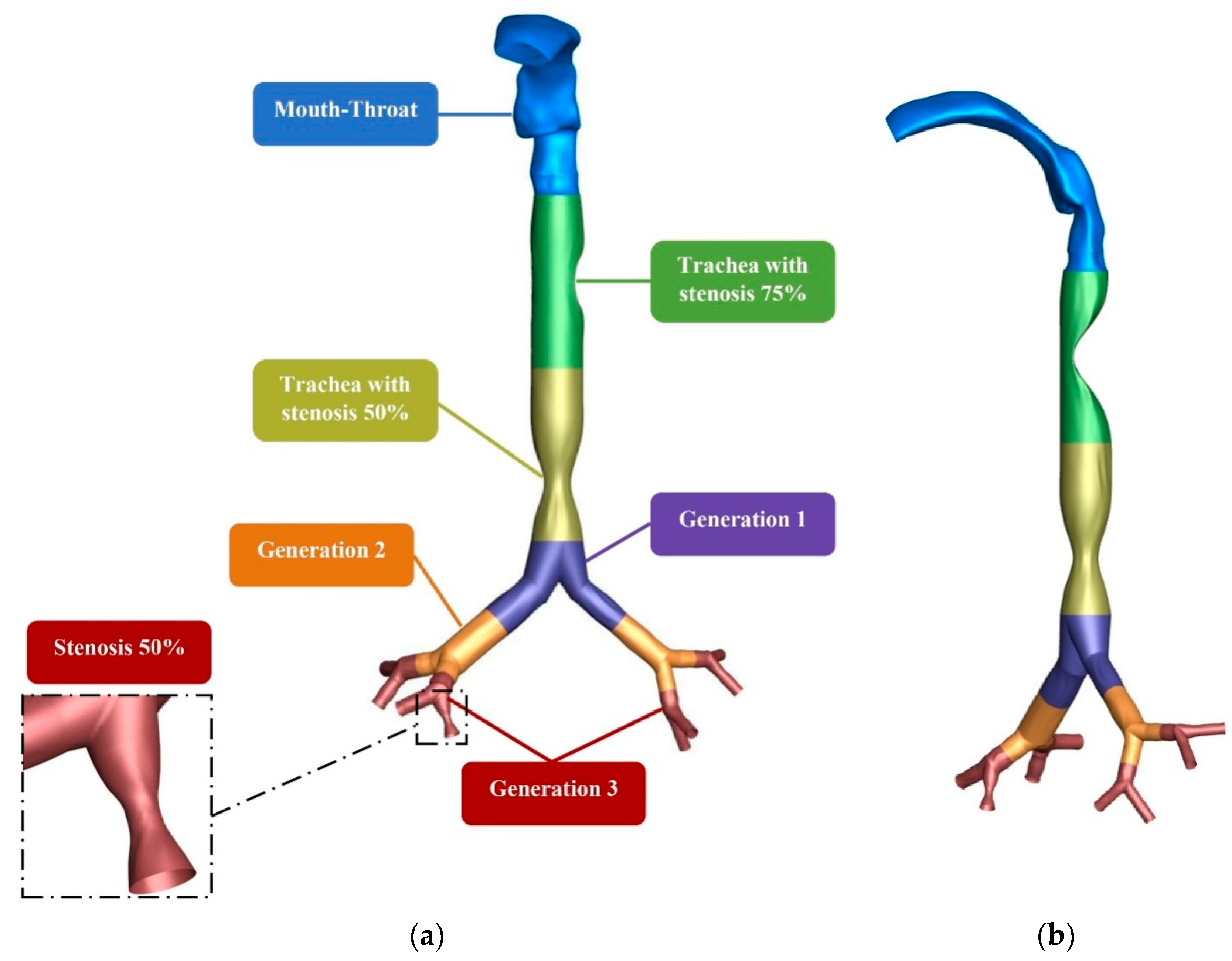
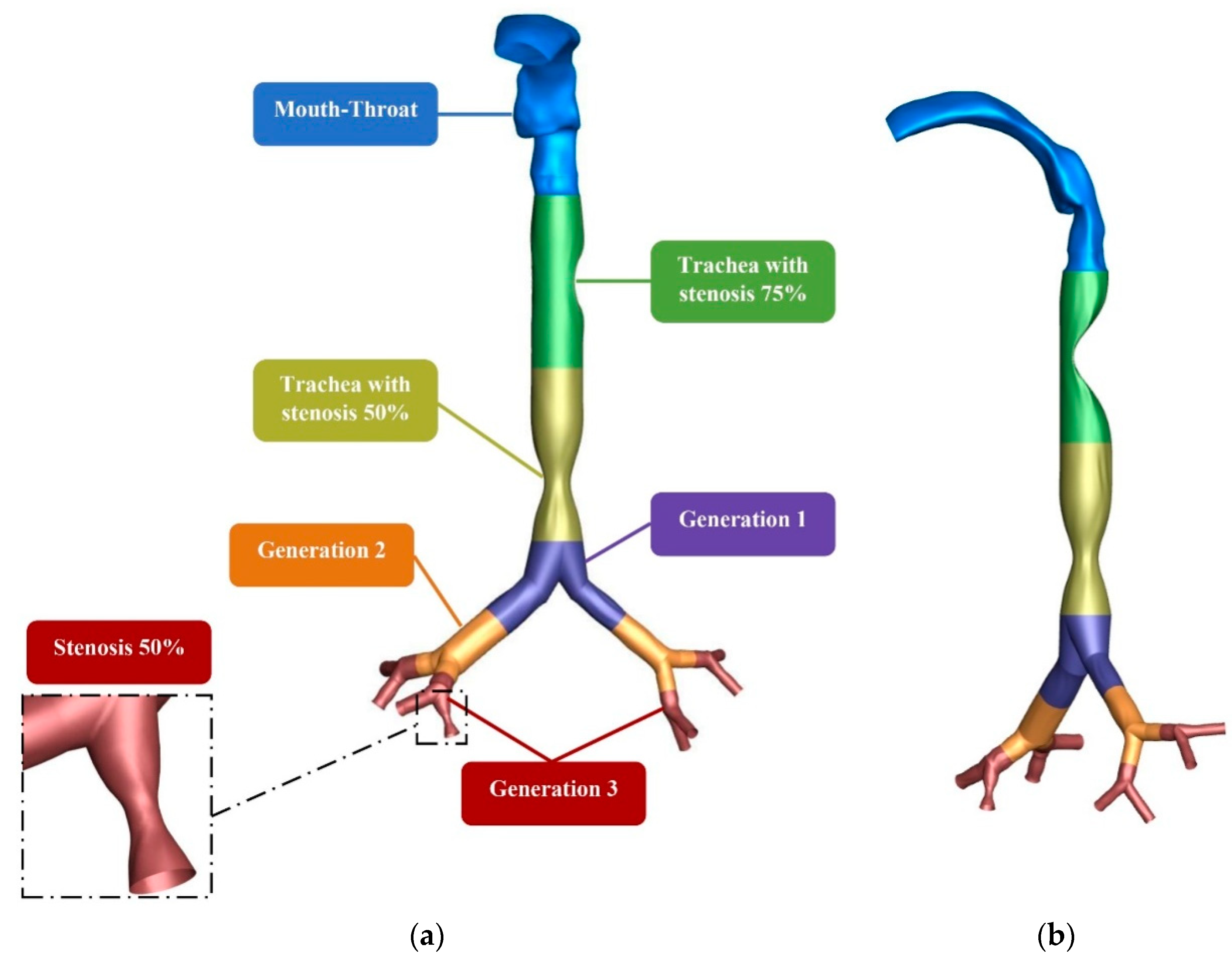
2.1. Geometrical Development
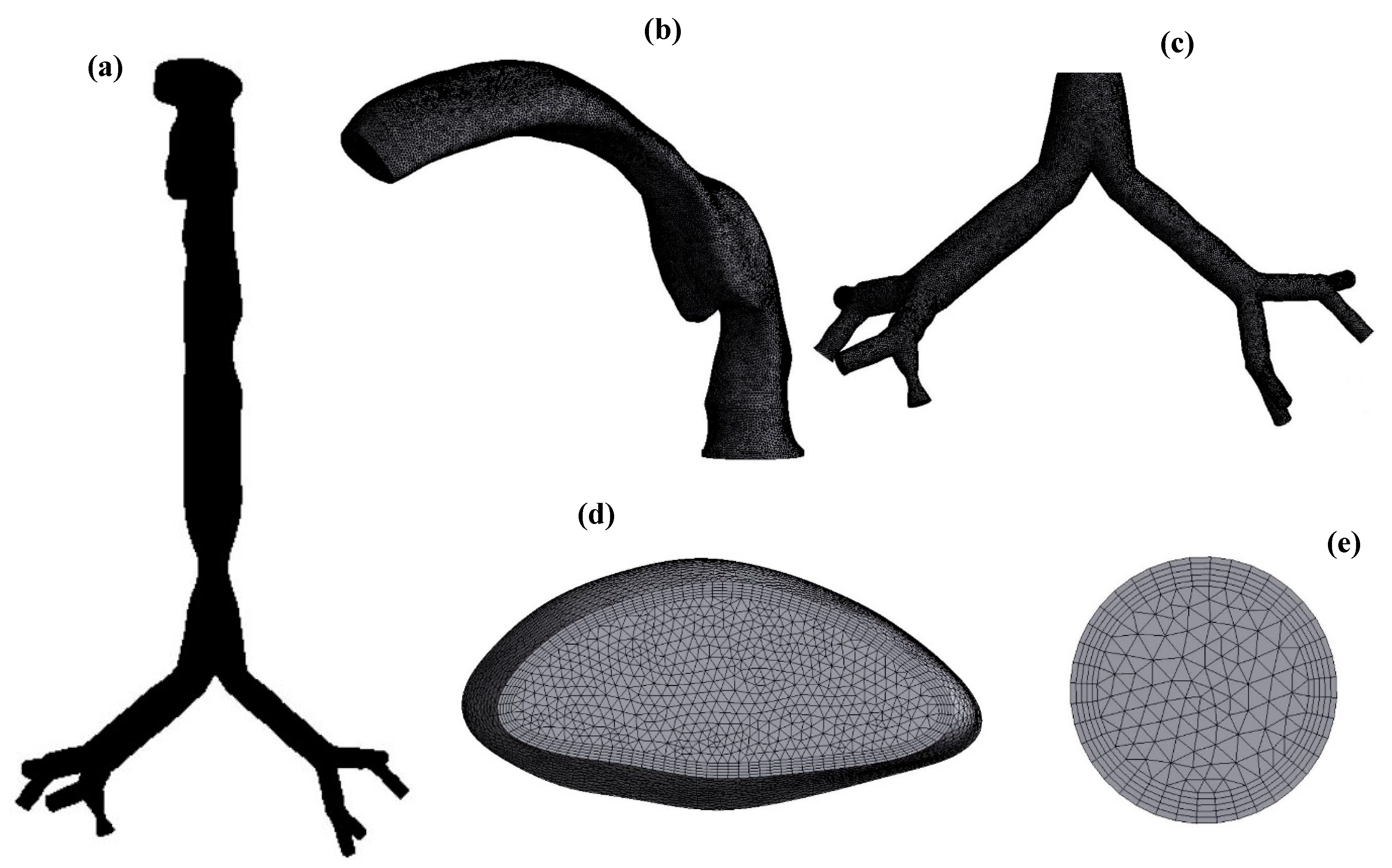
2.2. Mesh Generation and Validation
2.3. Numerical Methods
3. Result and Discussion
3.1. Velocity Analysis
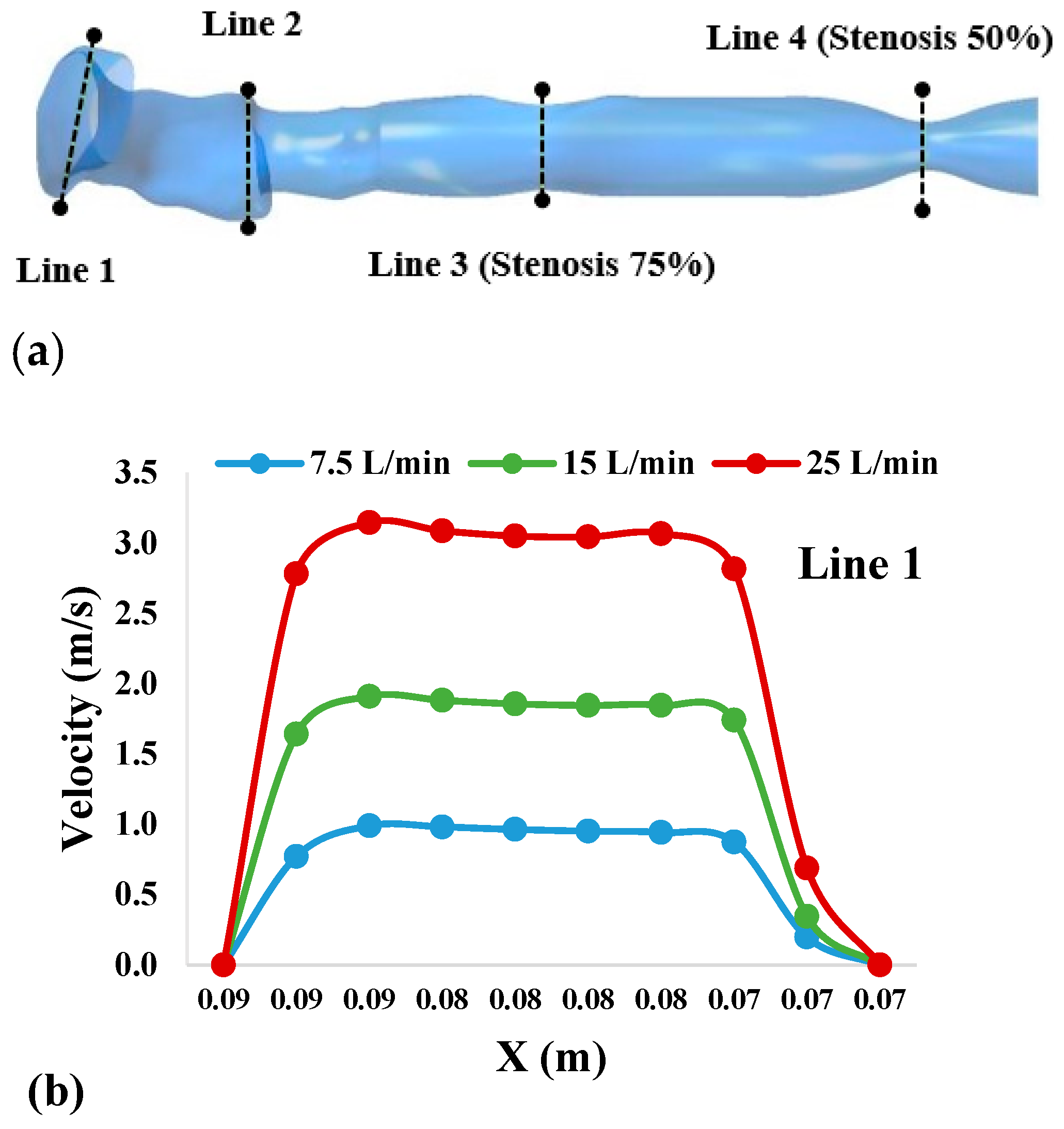
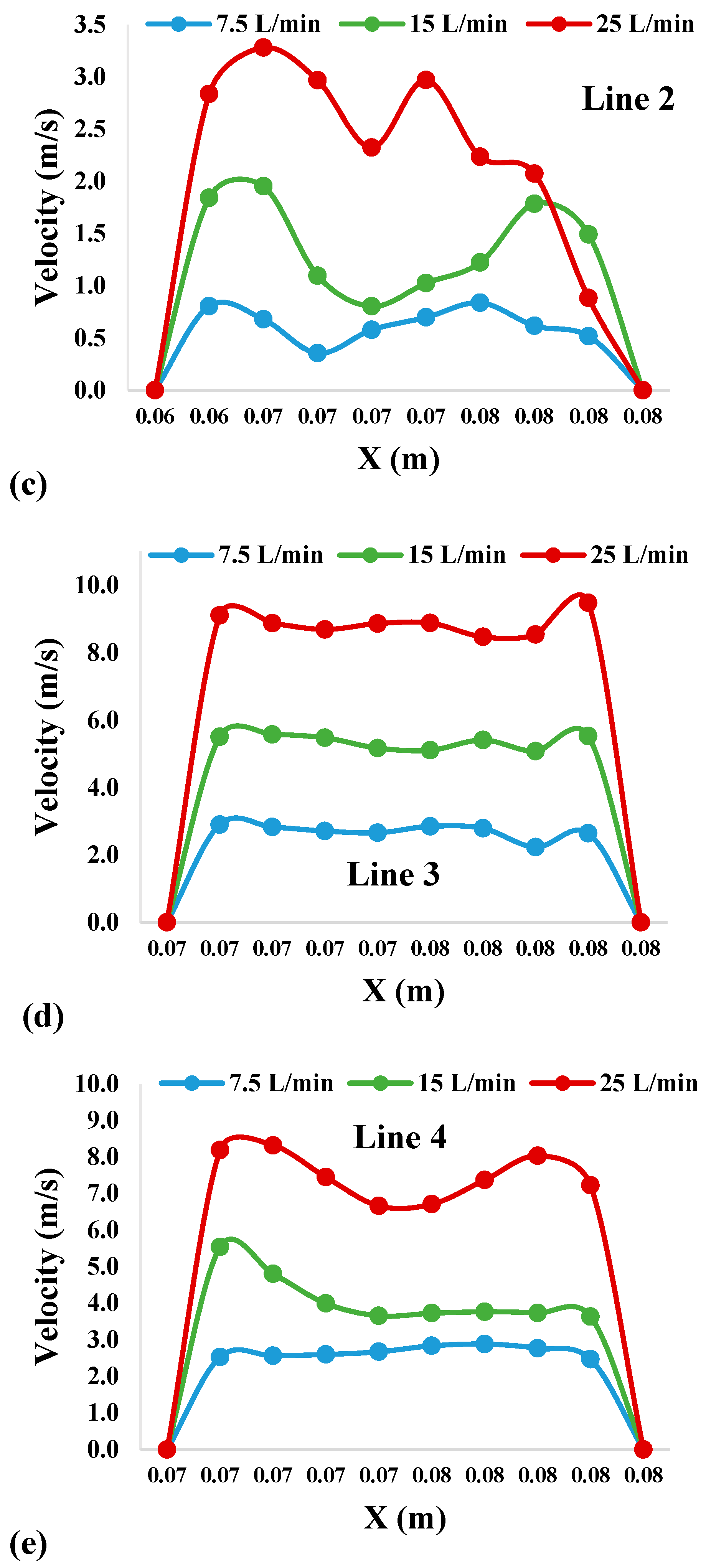
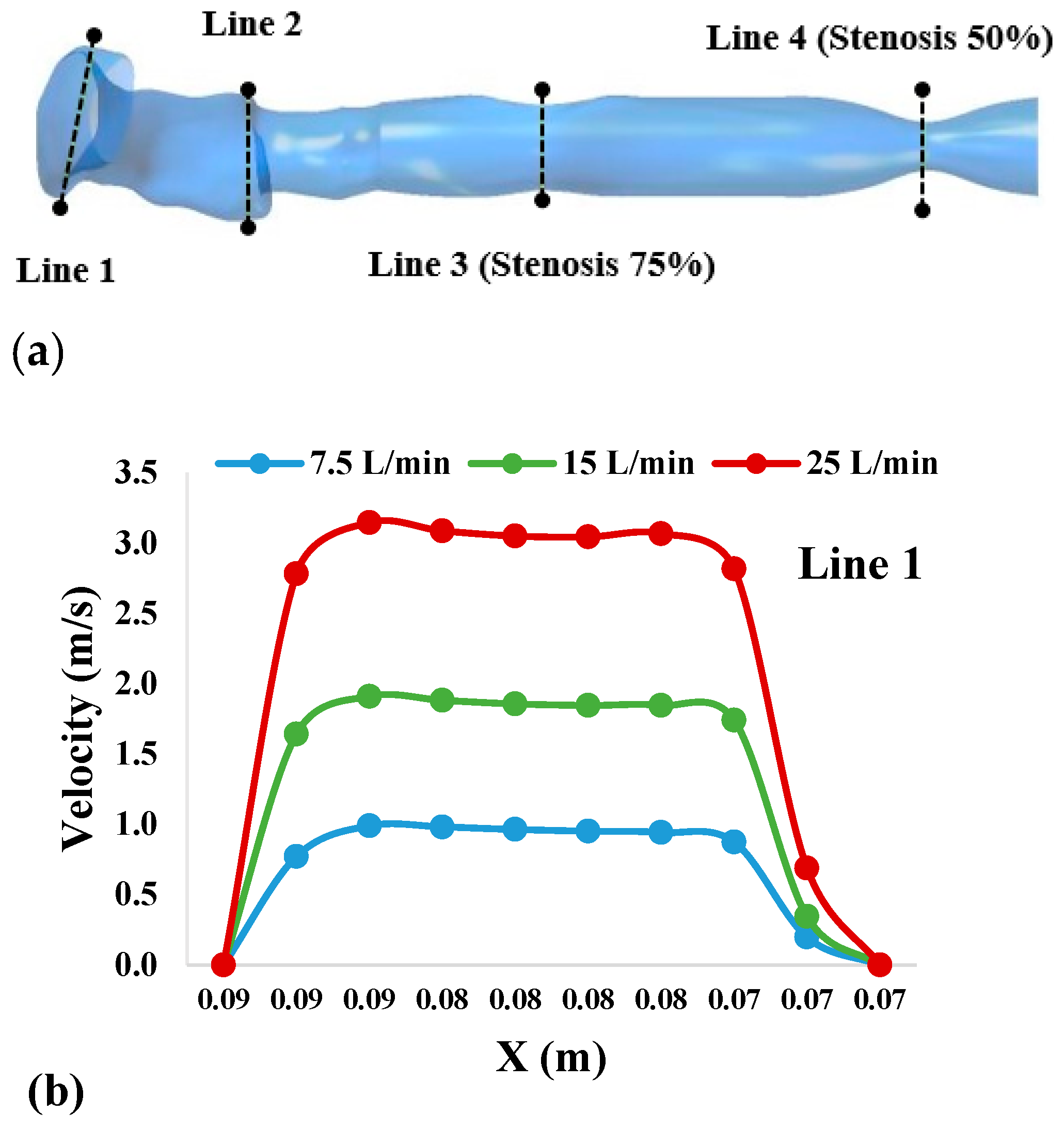
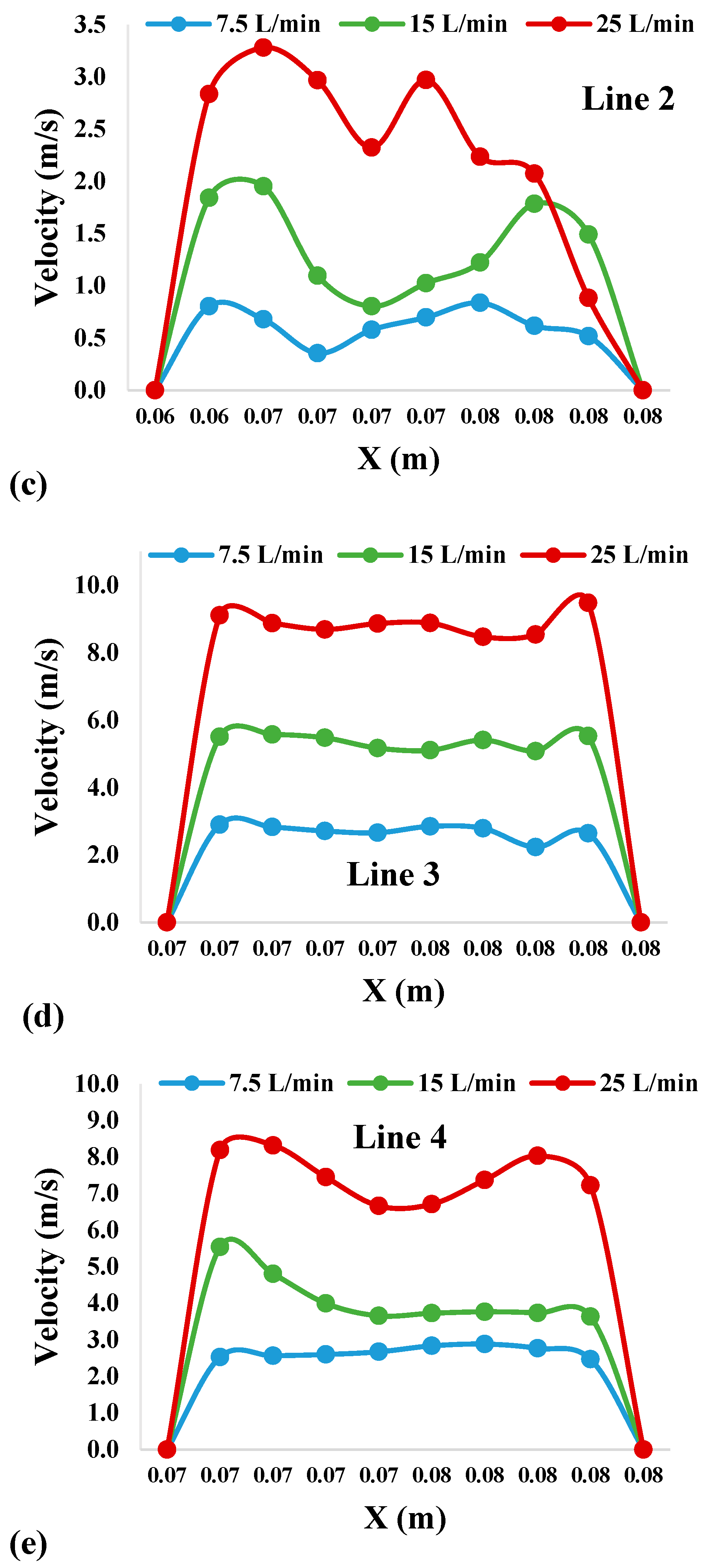
3.1.1. Velocity Profiles
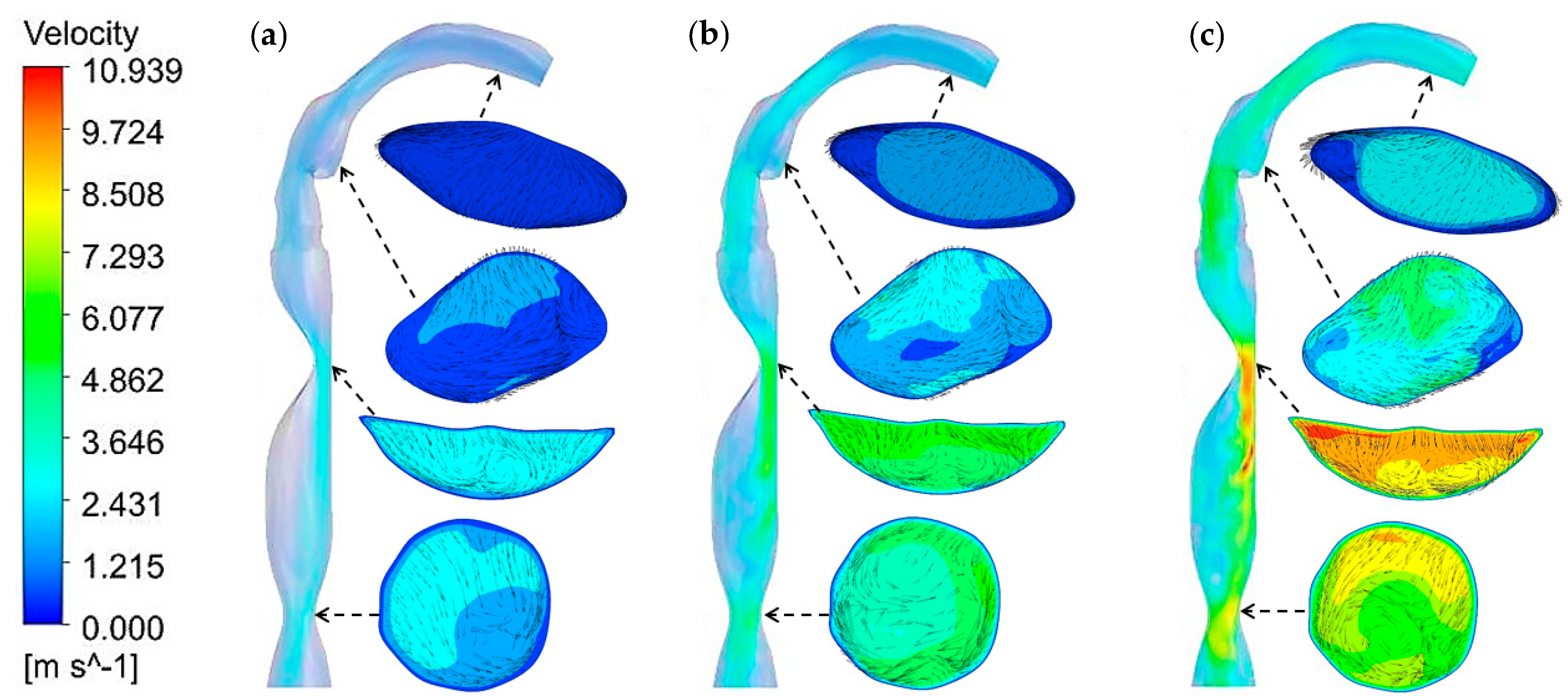
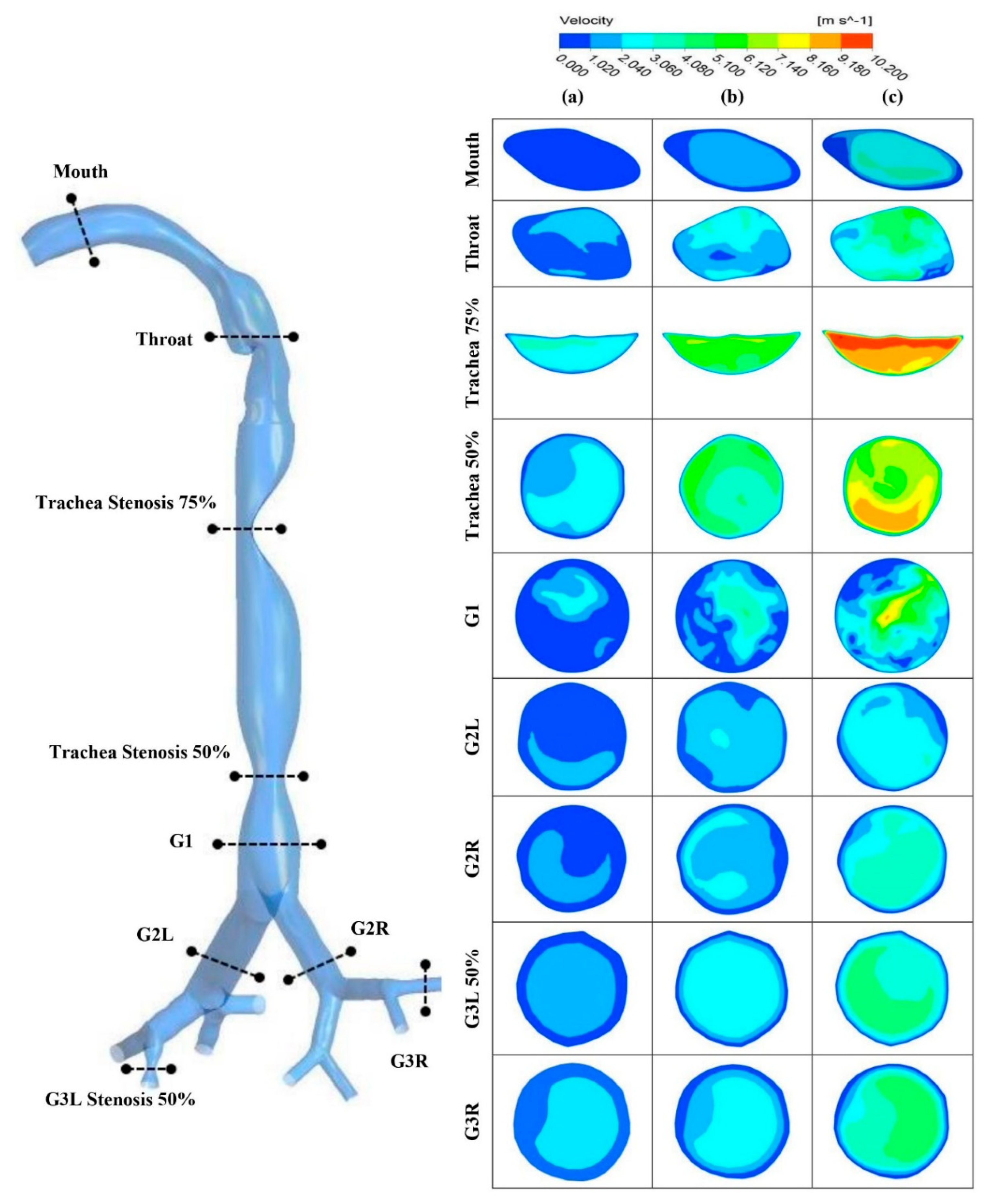
3.1.2. Velocity Contours
3.2. Pressure Analysis
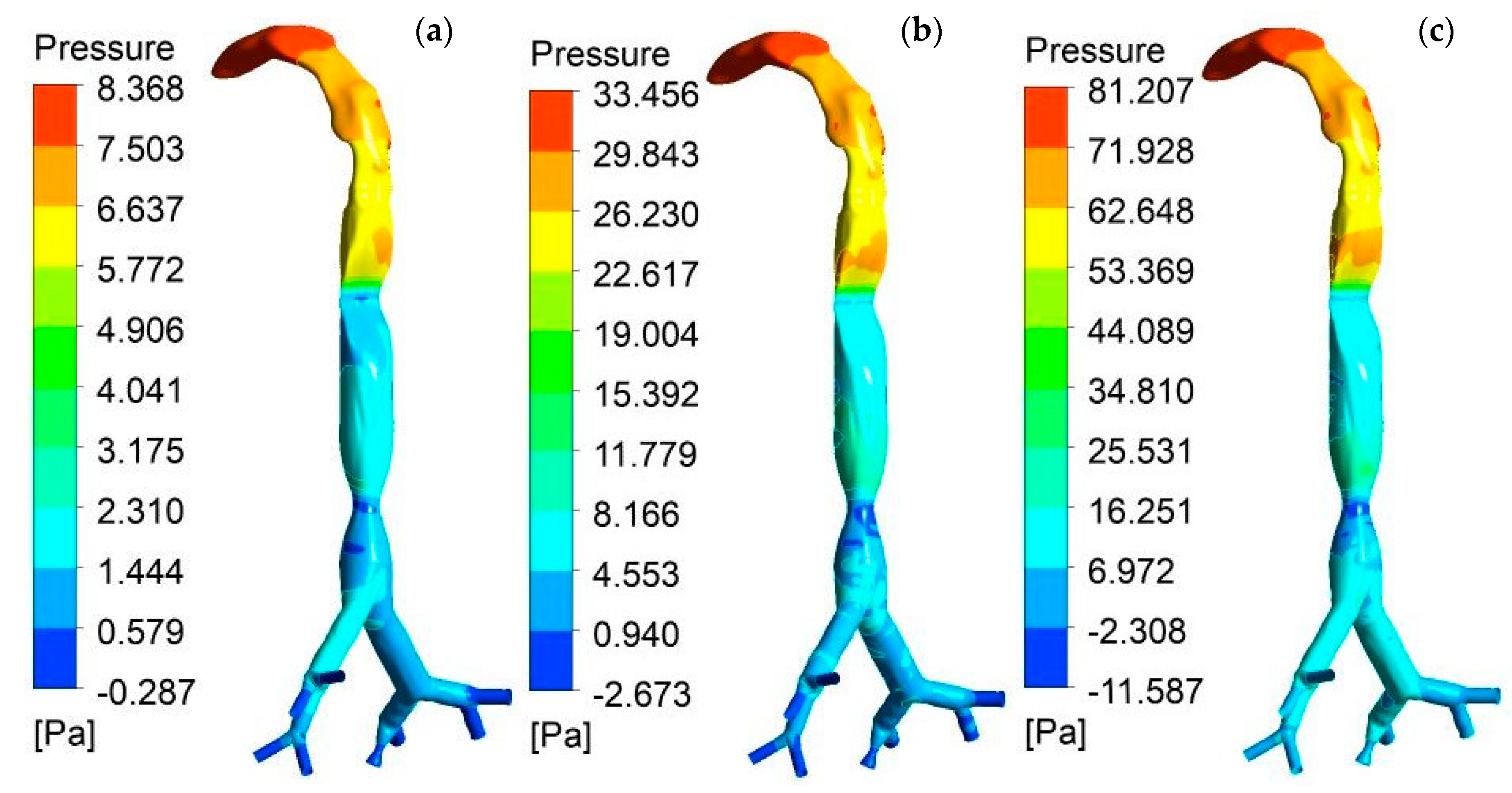
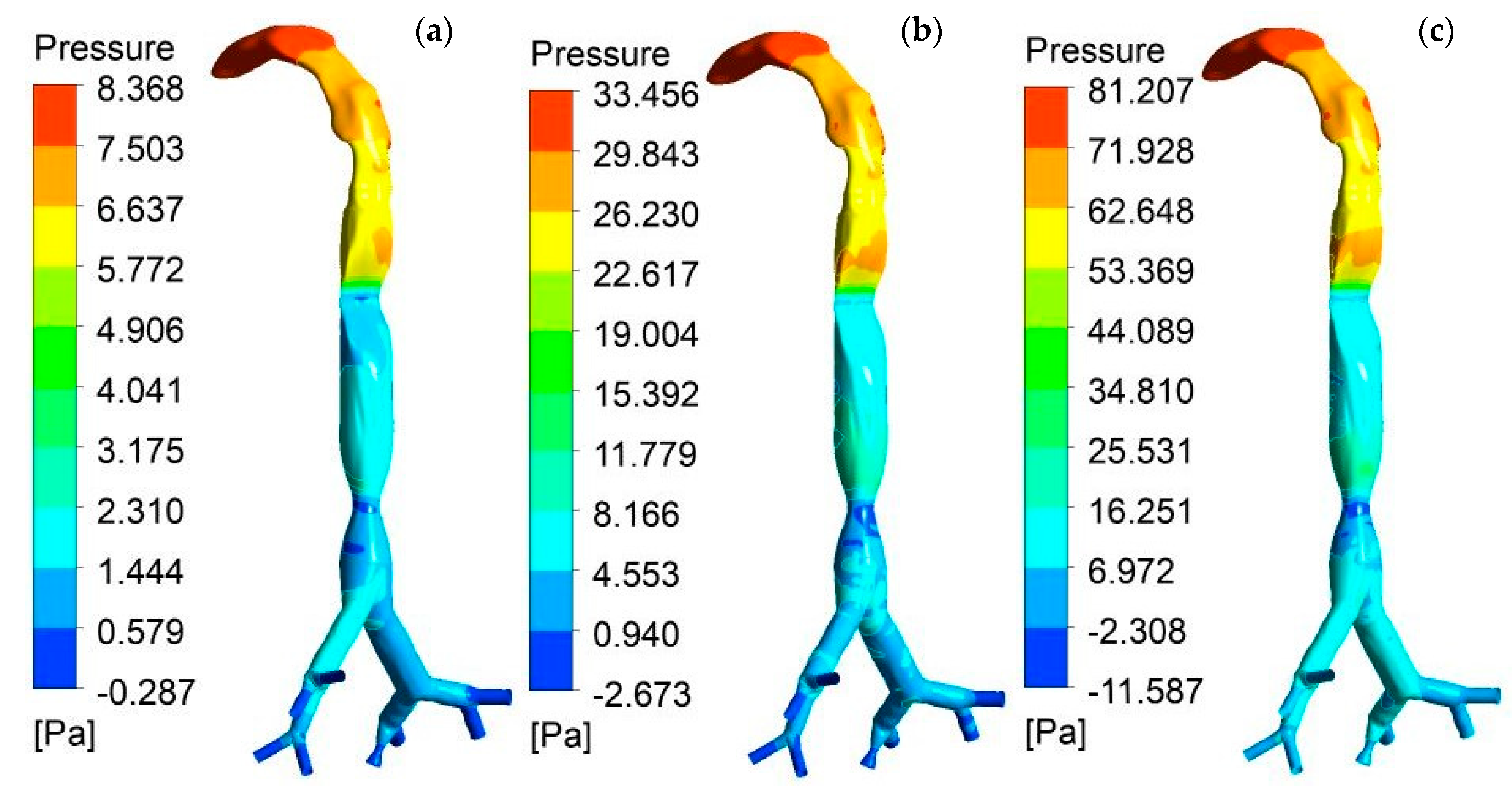
3.2.1. Pressure Contours
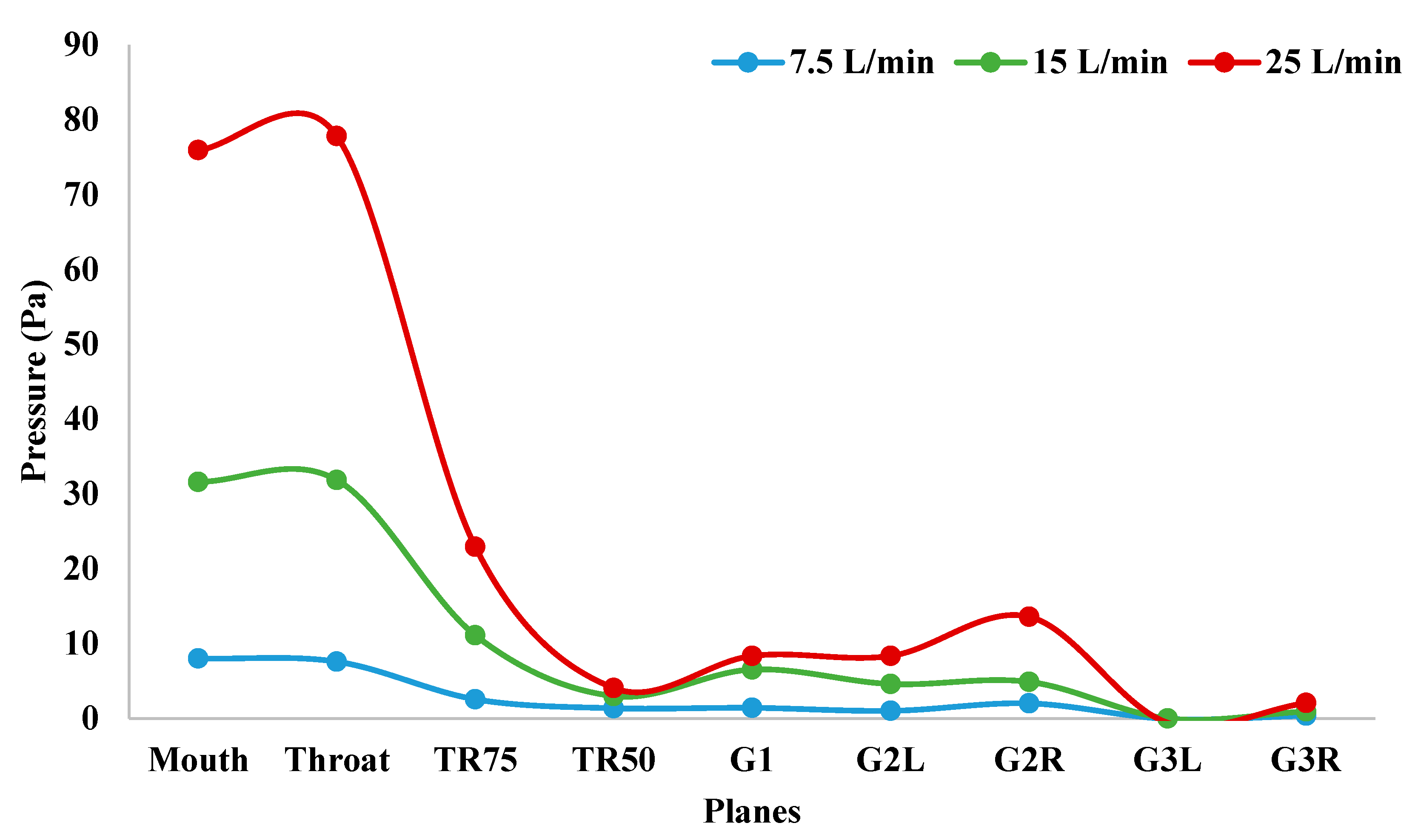
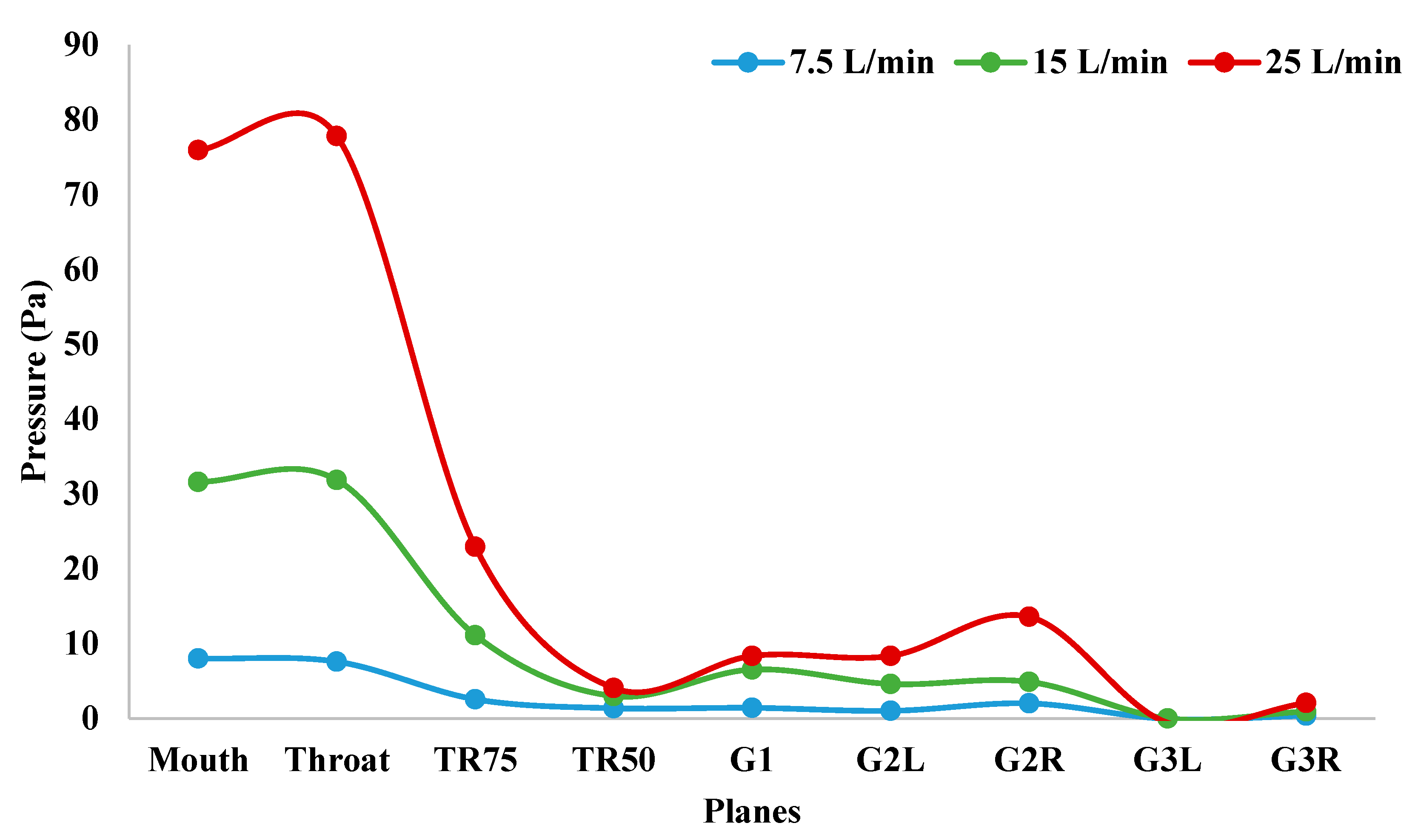
3.2.2. Pressure Variation
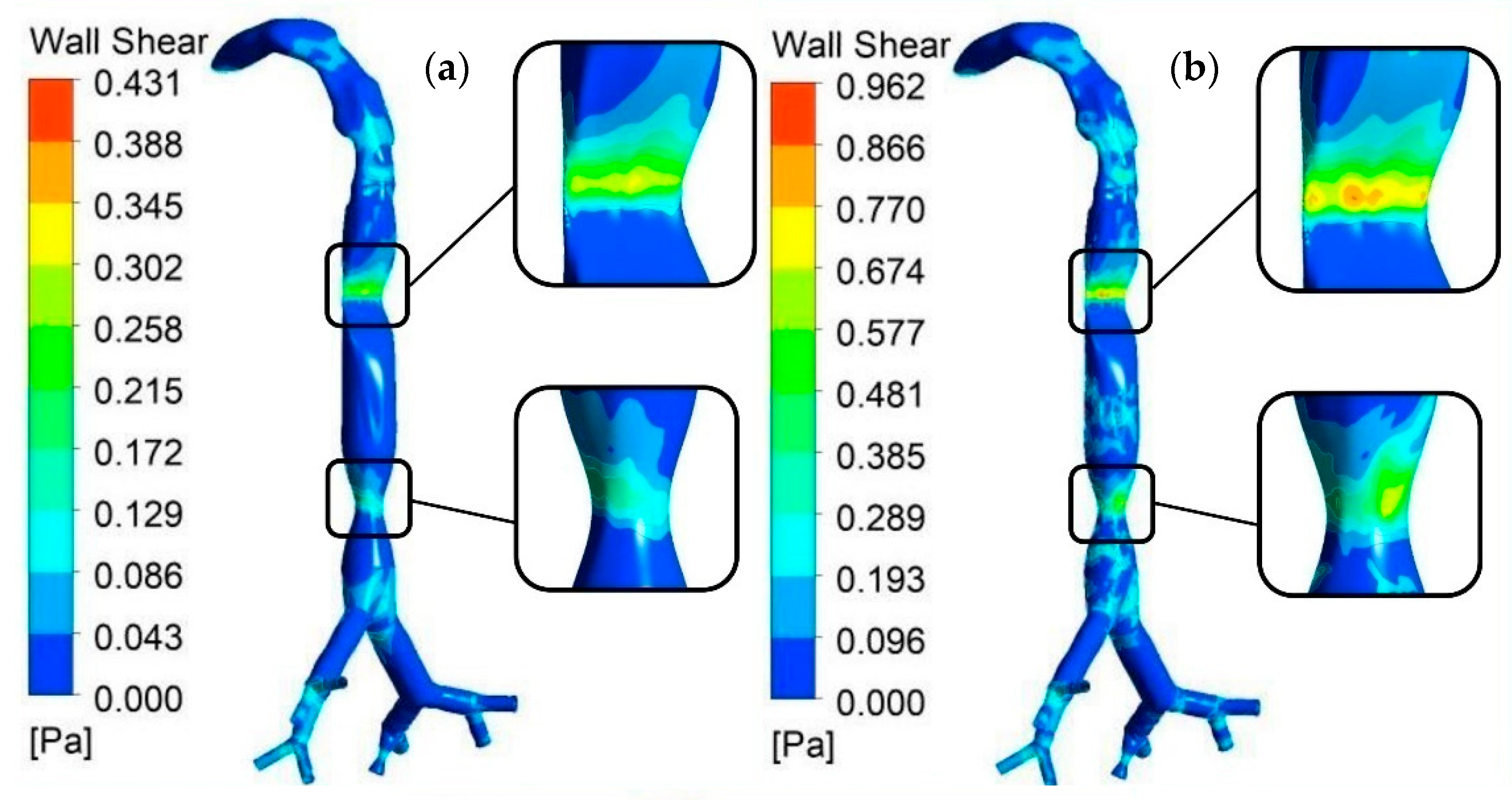
3.3. Wall Shear Analysis
3.4. Airflow Streamline Analysis
3.5. Particle Analysis
3.5.1. Particle Deposition
3.5.2. Particle Deposition Scenario
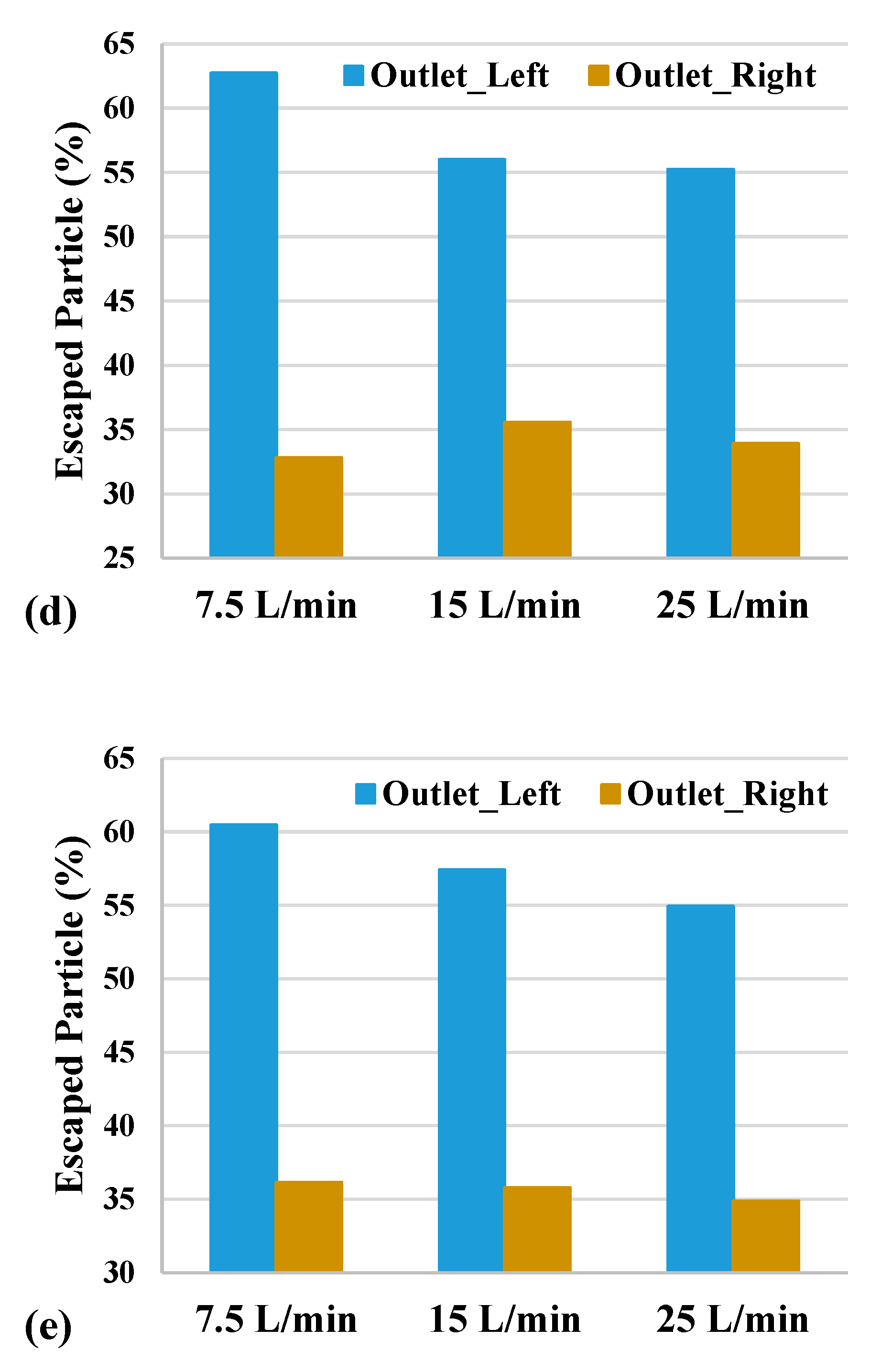
3.5.3. Escaped Particles
4. Conclusions and Future Perspectives
- ▪
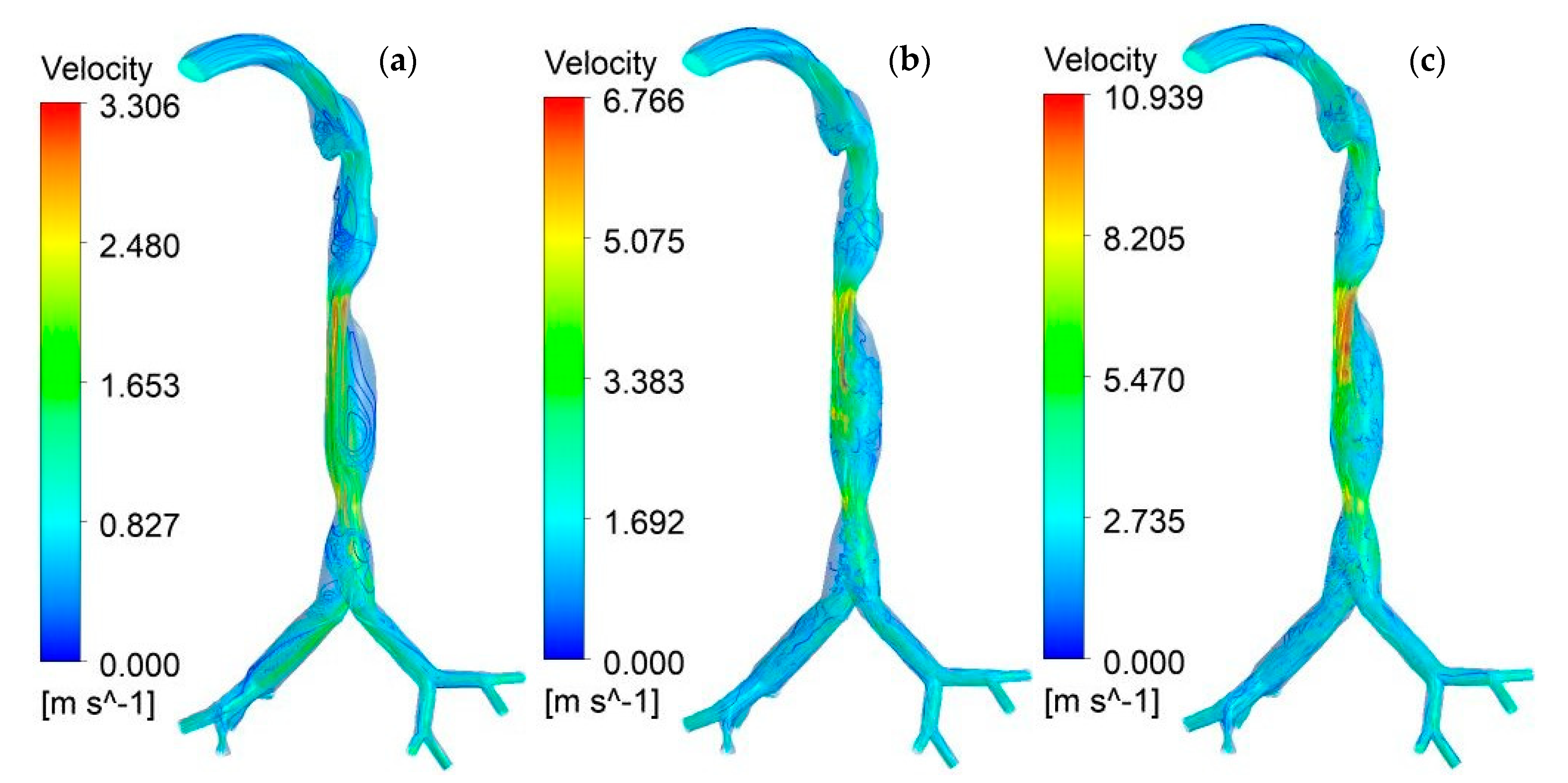
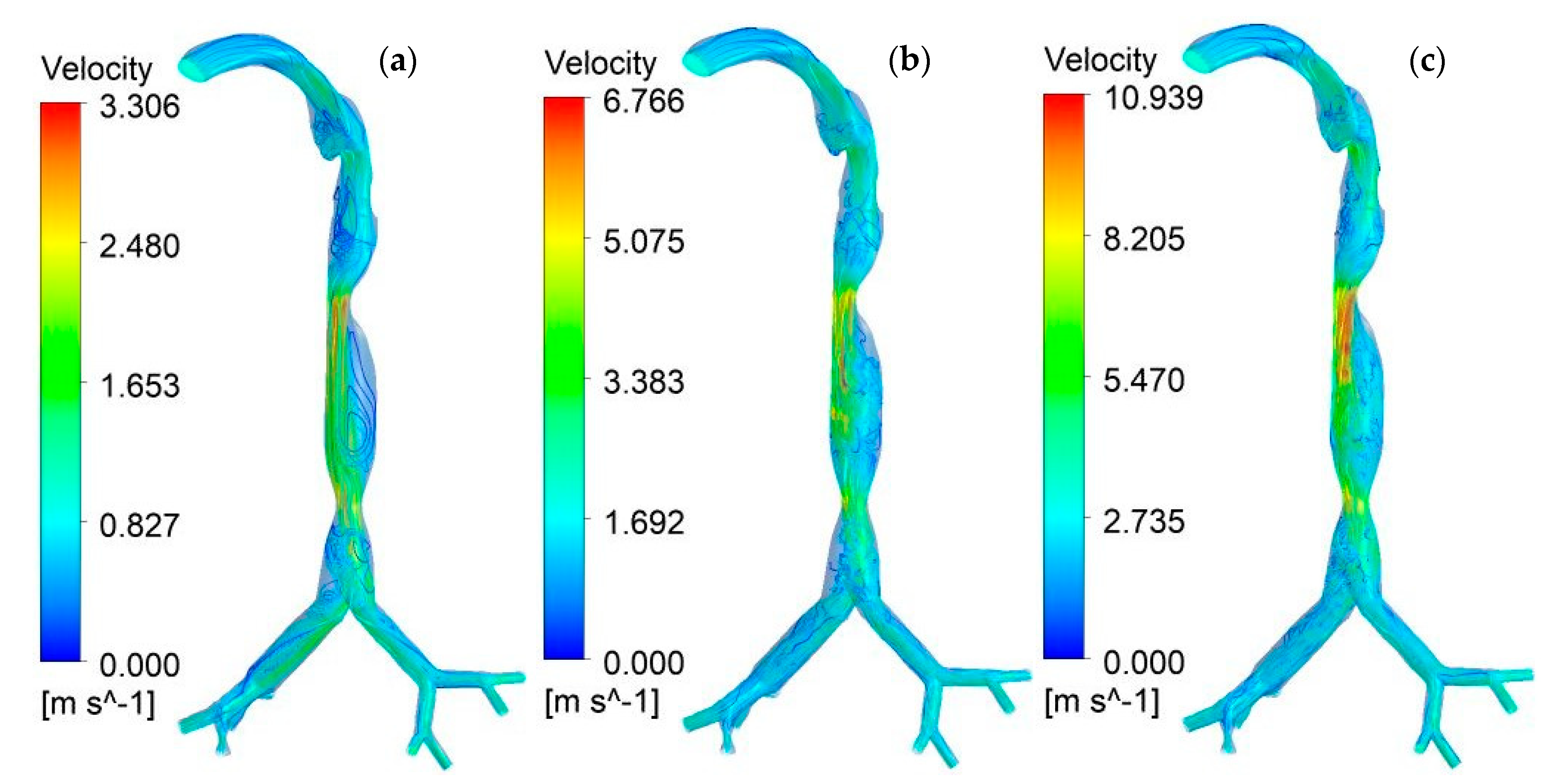
- The overall velocity field in the upper section of the mouth–throat model showed a fully developed profile. However, the velocity profile in the stenosis section was found to be highly complex. In the 75% stenosis section, the flow becomes highly chaotic with the increase in the flow rate and velocity magnitude. In the 50% stenosis section, the velocity flow field is less chaotic than that in the 75% stenosis section. A higher velocity magnitude was observed in the upper stenosis section than in the lower stenosis section.
- ▪
- The overall pressure drops in the mouth–throat section and upper airways showed a non-linear trend irrespective of the flow rates. The maximum pressure was observed in the upper part of the mouth. The maximum pressure decrease was observed in the 50% stenosis section. The overall drop in pressure increased with the flow rates.
- ▪
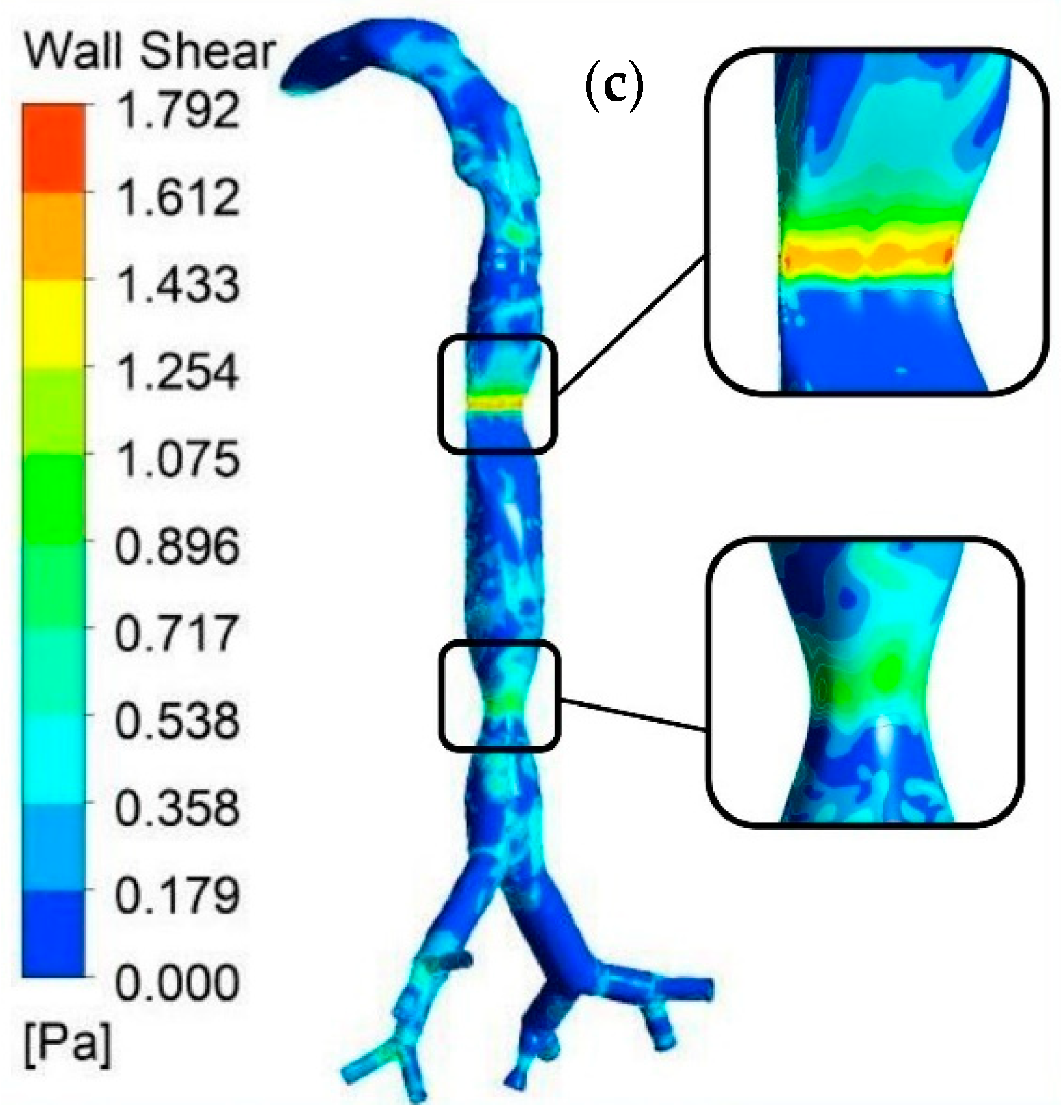
- At a high flow rate (25 L/min), the wall shear at the stenosis section was higher than that in the healthy part of the mouth–throat section and upper airways. The wall shear in the 75% stenosis section was higher than that in the 50% stenosis section of the airways.
- ▪
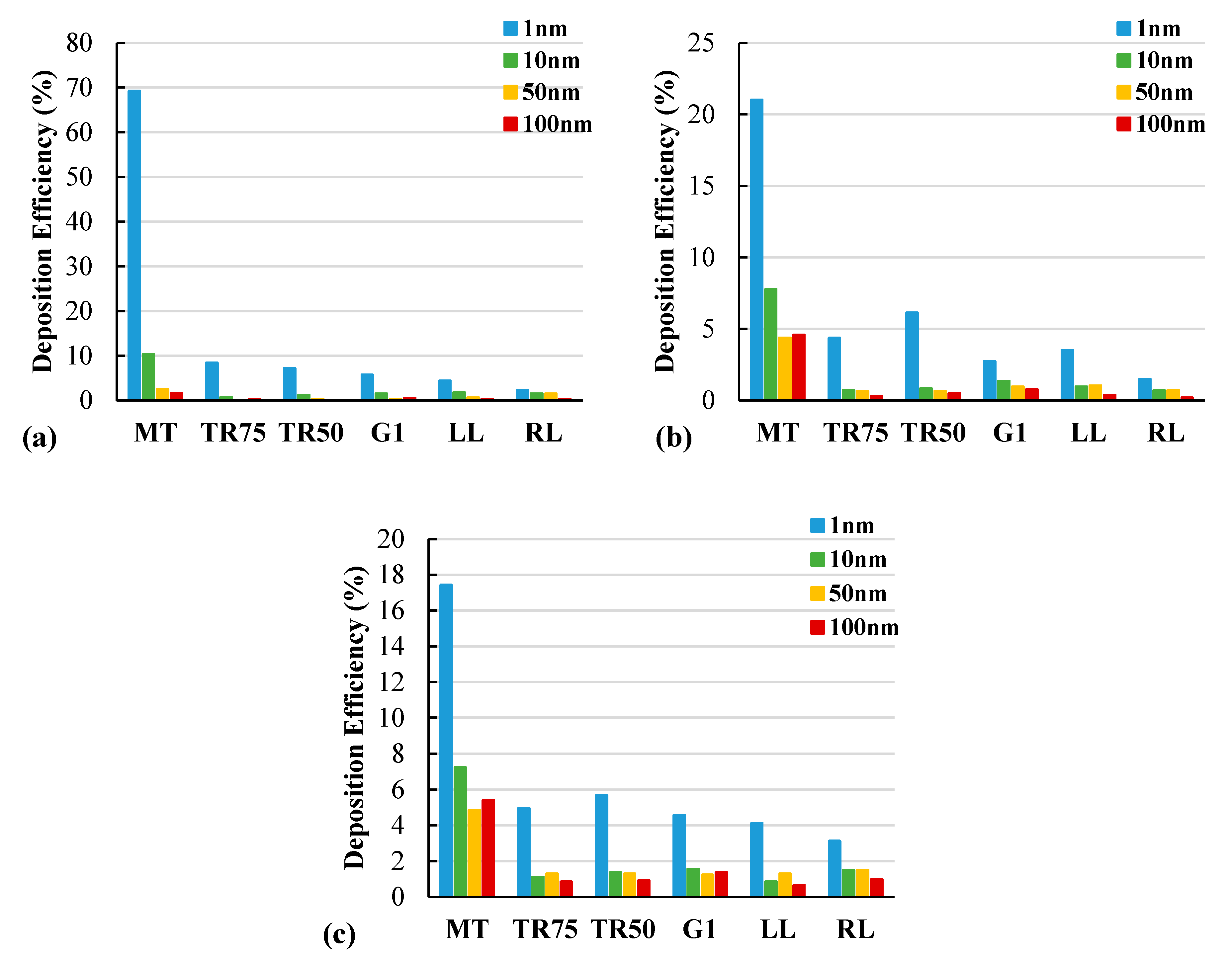
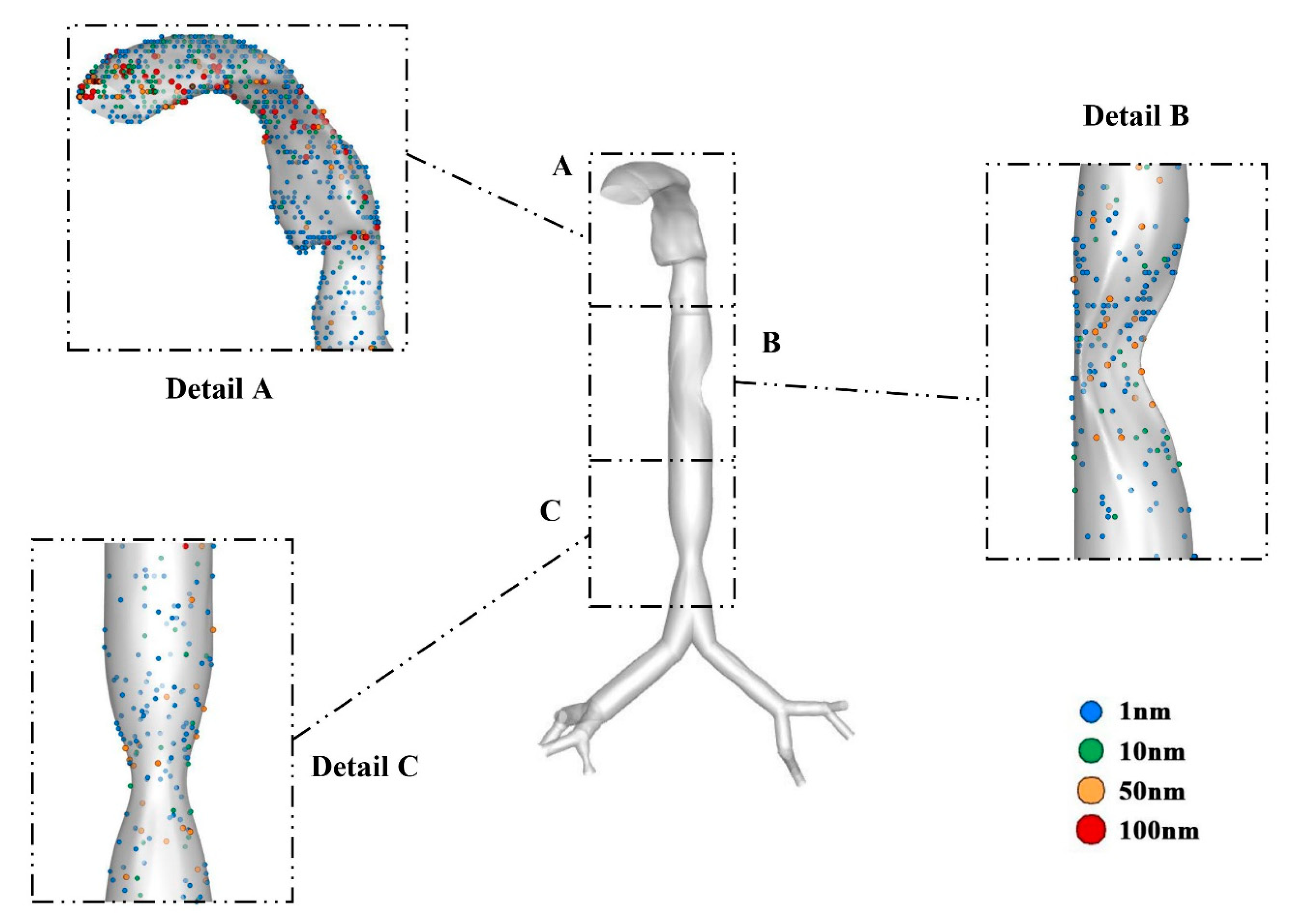
- The DE was non-linear for different flow rates of different particle diameters. The overall DE indicates that the Brownian motion and diffusion mechanism are dominant for the smaller diameter nanoparticles. The percentage of DE decreased proportionally with the increase in the flow rate. At 7.5 L/min, around 70% of nanoparticles having a size of 1 nm were trapped in the mouth–throat area. At other flow rates, around 20% of the particles having this size were trapped in this area. The DE in the stenosis sections was found to be less than 10% for both 75% and 50% reductions, and all flow rates.
- ▪
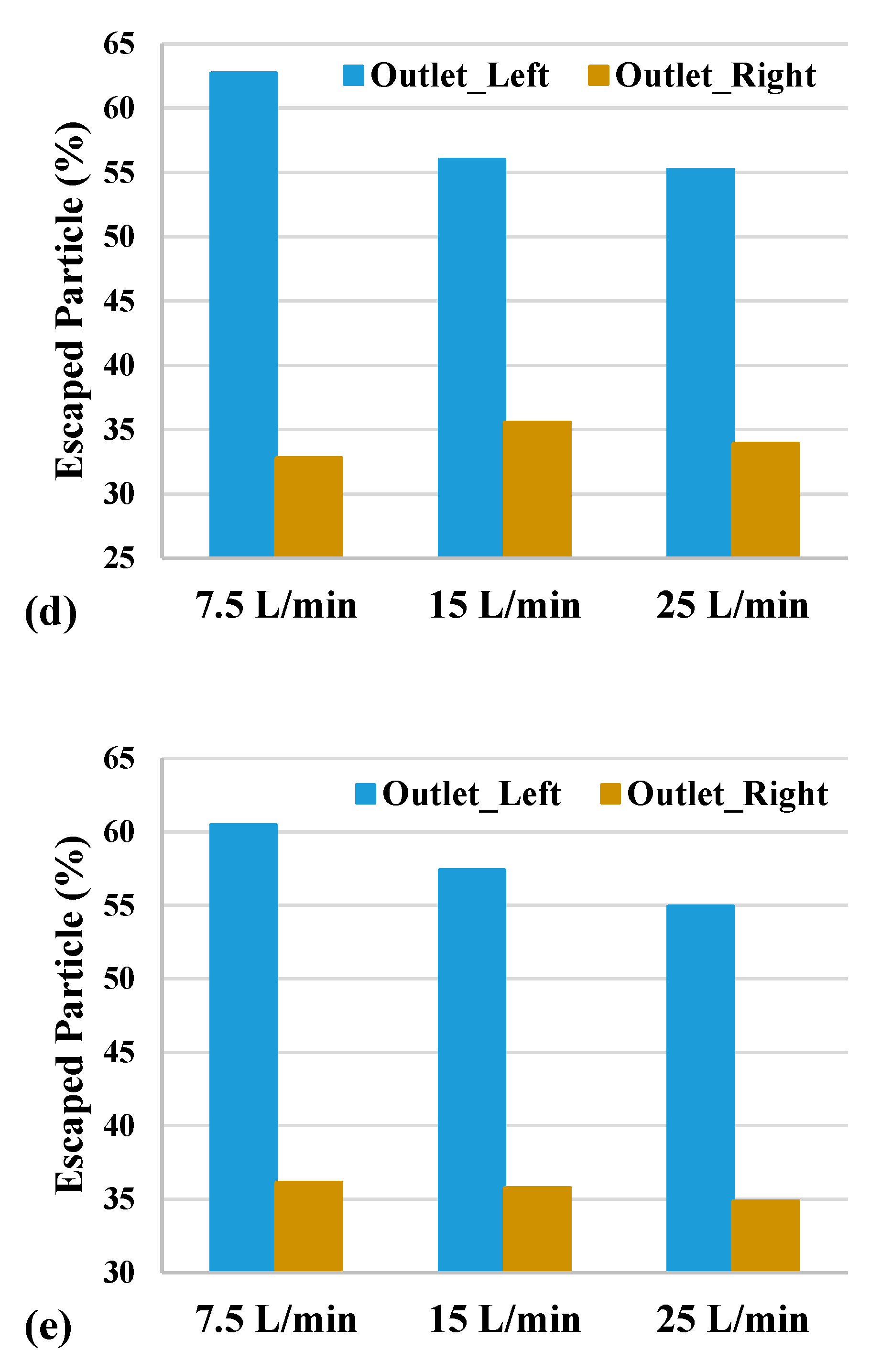
- More than 50% of the nanoparticles having a size of 10–100 nm escaped through the outlet at the left lung of the 3rd generation. For the outlet at the right lung of the same generation, less than 36% of escaped particles had a size of 10–100 nm. For the nanoparticles having a size of 1 nm, the proportion of escaped particles was less than 6% for both outlets.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Newsroom. Who. Int. Published 2021. Available online: https://www.who.int/news-room/air-pollution#:~:text=WHO%20estimates%20that%20around%207,deaths%20in%20the%20same%20period (accessed on 3 August 2021).
- Household Air Pollution and Health. Who. Int. Published 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/household-air-pollution-and-health (accessed on 3 August 2021).
- Larpruenrudee, P.; Surawski, N.C.; Islam, M.S. The Effect of Metro Construction on the Air Quality in the Railway Transport System of Sydney, Australia. Atmosphere 2022, 13, 759. [Google Scholar] [CrossRef]
- Duong, B.V.; Larpruenrudee, P.; Fang, T.; Hossain, S.I.; Saha, S.C.; Gu, Y.; Islam, M.S. Is the SARS-CoV-2 Omicron Variant Deadlier and More Transmissible than Delta Variant? Int. J. Environ. Res. Public Health 2022, 19, 4586. [Google Scholar] [CrossRef] [PubMed]
- Van Ertbruggen, C.; Hirsch, C.; Paiva, M. Anatomically based three-dimensional model of airways to simulate flow and particle transport using computational fluid dynamics. J. Appl. Physiol. 2005, 98, 970–980. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katz, I.M.; Martin, A.R.; Muller, P.-A.; Terzibachi, K.; Feng, C.-H.; Caillibotte, G.; Sandeau, J.; Texereau, J. The ventilation distribution of helium–oxygen mixtures and the role of inertial losses in the presence of heterogeneous airway obstructions. J. Biomech. 2011, 44, 1137–1143. [Google Scholar] [CrossRef]
- Borojeni, A.A.; Noga, M.L.; Martin, A.R.; Finlay, W.H. Validation of airway resistance models for predicting pressure loss through anatomically realistic conducting airway replicas of adults and children. J. Biomech. 2015, 48, 1988–1996. [Google Scholar] [CrossRef]
- Kumar, H.; Tawhai, M.; Hoffman, E.; Lin, C.-L. The effects of geometry on airflow in the acinar region of the human lung. J. Biomech. 2009, 42, 1635–1642. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soni, B.; Aliabadi, S. Large-scale CFD simulations of airflow and particle deposition in lung airway. Comput. Fluids 2013, 88, 804–812. [Google Scholar] [CrossRef]
- Heenan, A.F.; Matida, E.; Pollard, A.; Finlay, W.H. Experimental measurements and computational modeling of the flow field in an idealized human oropharynx. Exp. Fluids 2003, 35, 70–84. [Google Scholar] [CrossRef]
- Ghosh, A.; Islam, M.S.; Saha, S.C. Targeted Drug Delivery of Magnetic Nano-Particle in the Specific Lung Region. Computation 2020, 8, 10. [Google Scholar] [CrossRef] [Green Version]
- Islam, M.S.; Saha, S.C.; Sauret, E.; Ong, H.; Young, P.; Gu, Y. Euler–Lagrange approach to investigate respiratory anatomical shape effects on aerosol particle transport and deposition. Toxicol. Res. Appl. 2019, 3, 2397847319894675. [Google Scholar] [CrossRef] [Green Version]
- Rahimi-Gorji, M.; Pourmehran, O.; Gorji-Bandpy, M.; Gorji, T. CFD simulation of airflow behavior and particle transport and deposition in different breathing conditions through the realistic model of human airways. J. Mol. Liq. 2015, 209, 121–133. [Google Scholar] [CrossRef]
- Asgharian, B.; Price, O.; Hofmann, W. Prediction of particle deposition in the human lung using realistic models of lung ventilation. J. Aerosol Sci. 2006, 37, 1209–1221. [Google Scholar] [CrossRef]
- Islam, M.; Saha, S.; Sauret, E.; Gu, Y.; Ristovski, Z. Numerical Investigation of Aerosol Particle Transport and Deposition in Realistic Lung Airway. In 6th International Conference on Computational Methods, 2015; ScienTech Publisher: Auckland, New Zealand, 2015; pp. 1–9. [Google Scholar]
- Arsalanloo, A.; Abbasalizadeh, M.; Khalilian, M.; Saniee, Y.; Ramezanpour, A.; Islam, M.S. A computational approach to understand the breathing dynamics and pharmaceutical aerosol transport in a realistic airways. Adv. Powder Technol. 2022, 33, 103635. [Google Scholar] [CrossRef]
- Kim, J.; Heise, R.L.; Reynolds, A.M.; Pidaparti, R.M. Aging effects on airflow dynamics and lung function in human bronchioles. PLoS ONE 2017, 12, e0183654. [Google Scholar] [CrossRef]
- Islam, M.; Larpruenrudee, P.; Hossain, S.; Rahimi-Gorji, M.; Gu, Y.; Saha, S.; Paul, G. Polydisperse Aerosol Transport and Deposition in Upper Airways of Age-Specific Lung. Int. J. Environ. Res. Public Health 2021, 18, 6239. [Google Scholar] [CrossRef] [PubMed]
- Morin, C.; Proteau, S.; Rousseau, E.; Brayden, J. Organ-Cultured Airway Explants: A New Model of Airway Hyperresponsiveness. Exp. Lung Res. 2005, 31, 719–744. [Google Scholar] [CrossRef]
- Khaddaj-Mallat, R.; Rousseau, É. MAG-EPA and 17,18-EpETE target cytoplasmic signalling pathways to reduce short-term airway hyperresponsiveness. Pflüg. Arch.-Eur. J. Physiol. 2015, 467, 1591–1605. [Google Scholar] [CrossRef]
- Cheng, Y.-S.; Zhou, Y.; Chen, B.T. Particle Deposition in a Cast of Human Oral Airways. Aerosol Sci. Technol. 1999, 31, 286–300. [Google Scholar] [CrossRef]
- Cheng, K.-H.; Cheng, Y.-S.; Yeh, H.-C.; Swift, D.L. Deposition of Ultrafine Aerosols in the Head Airways During Natural Breathing and During Simulated Breath Holding Using Replicate Human Upper Airway Casts. Aerosol Sci. Technol. 1995, 23, 465–474. [Google Scholar] [CrossRef]
- Martin, A.R.; Finlay, W.H. A general, algebraic equation for predicting total respiratory tract deposition of micrometer-sized aerosol particles in humans. J. Aerosol Sci. 2007, 38, 246–253. [Google Scholar] [CrossRef]
- Stahlhofen, W.; Rudolf, G.; James, A. Intercomparison of Experimental Regional Aerosol Deposition Data. J. Aerosol Med. 1989, 2, 285–308. [Google Scholar] [CrossRef]
- Jayaraju, S.; Brouns, M.; Verbanck, S.; Lacor, C. Fluid flow and particle deposition analysis in a realistic extrathoracic airway model using unstructured grids. J. Aerosol Sci. 2007, 38, 494–508. [Google Scholar] [CrossRef]
- Luo, H.; Liu, Y. Modeling the bifurcating flow in a CT-scanned human lung airway. J. Biomech. 2008, 41, 2681–2688. [Google Scholar] [CrossRef] [PubMed]
- Xi, J.; Longest, P.W. Transport and Deposition of Micro-Aerosols in Realistic and Simplified Models of the Oral Airway. Ann. Biomed. Eng. 2007, 35, 560–581. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Kleinstreuer, C.; Kim, C.S. Comparison of analytical and CFD models with regard to micron particle deposition in a human 16-generation tracheobronchial airway model. J. Aerosol Sci. 2009, 40, 16–28. [Google Scholar] [CrossRef]
- Ilie, M.; Matida, E.A.; Finlay, W.H. Asymmetrical Aerosol Deposition in an Idealized Mouth with a DPI Mouthpiece Inlet. Aerosol Sci. Technol. 2008, 42, 10–17. [Google Scholar] [CrossRef] [Green Version]
- Sul, B.; Wallqvist, A.; Morris, M.J.; Reifman, J.; Rakesh, V. A computational study of the respiratory airflow characteristics in normal and obstructed human airways. Comput. Biol. Med. 2014, 52, 130–143. [Google Scholar] [CrossRef]
- Beni, H.M.; Mortazavi, H.; Tashvighi, E.; Islam, M.S. Investigation of the Upper Respiratory Tract of a Male Smoker with Laryngeal Cancer by Inhaling Air Associated with Various Physical Activity Levels. Atmosphere 2022, 13, 717. [Google Scholar] [CrossRef]
- Rahman, M.; Zhao, M.; Islam, M.S.; Dong, K.; Saha, S.C. Aging effects on airflow distribution and micron-particle transport and deposition in a human lung using CFD-DPM approach. Adv. Powder Technol. 2021, 32, 3506–3516. [Google Scholar] [CrossRef]
- Zhang, Z.; Kleinstreuer, C.; Donohue, J.; Kim, C. Comparison of micro- and nano-size particle depositions in a human upper airway model. J. Aerosol Sci. 2005, 36, 211–233. [Google Scholar] [CrossRef]
- Zhang, L.; Cheng, H.; Zhang, C.; Xu, Z.; Ye, J. Deposition Fraction of Aerosol Particles in a Human Oral Airway Model on Stable Condition. Aerosol Air Qual. Res. 2006, 6, 259–267. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Z.; Kleinstreuer, C. Airflow structures and nano-particle deposition in a human upper airway model. J. Comput. Phys. 2004, 198, 178–210. [Google Scholar] [CrossRef]
- Schroter, R.; Sudlow, M. Flow patterns in models of the human bronchial airways. Respir. Physiol. 1969, 7, 341–355. [Google Scholar] [CrossRef]
- Farkas, Á.; Balásházy, I. Simulation of the effect of local obstructions and blockage on airflow and aerosol deposition in central human airways. J. Aerosol Sci. 2007, 38, 865–884. [Google Scholar] [CrossRef]
- Li, Z.; Kleinstreuer, C.; Zhang, Z. Simulation of airflow fields and microparticle deposition in realistic human lung airway models. Part II: Particle transport and deposition. Eur. J. Mech.–B/Fluids 2007, 26, 650–668. [Google Scholar] [CrossRef]
- Kim, C.S.; Iglesias, A.J. Deposition of Inhaled Particles in Bifurcating Airway Models: I. Inspiratory Deposition. J. Aerosol Med. 1989, 2, 1–14. [Google Scholar] [CrossRef]
- Luo, H.; Liu, Y.; Yang, X. Particle deposition in obstructed airways. J. Biomech. 2007, 40, 3096–3104. [Google Scholar] [CrossRef]
- Jayaraju, S.; Brouns, M.; Lacor, C.; Belkassem, B.; Verbanck, S. Large eddy and detached eddy simulations of fluid flow and particle deposition in a human mouth–throat. J. Aerosol Sci. 2008, 39, 862–875. [Google Scholar] [CrossRef]
- Stapleton, K.; Guentsch, E.; Hoskinson, M.; Finlay, W. On the suitability of k–ε turbulence modeling for aerosol deposition in the mouth and throat: A comparison with experiment. J. Aerosol Sci. 2000, 31, 739–749. [Google Scholar] [CrossRef]
- Longest, P.; Kleinstreuer, C.; Buchanan, J.R. Efficient computation of micro-particle dynamics including wall effects. Comput. Fluids 2004, 33, 577–601. [Google Scholar] [CrossRef]
- Lilley, G. Turbulence Modelling for CFD DC Wilcox DCW Industries, 5354 Palm Drive, La Canada, CA 91011, USA. 1993. 460pp+ software diskette. Illustrated. $75. Aeronaut. J. 1994, 98, 405. [Google Scholar] [CrossRef]
- Hawkins, D.B. Glottic and subglottic stenosis from endotracheal intubation. Laryngoscope 1977, 87, 339–346. [Google Scholar] [CrossRef] [PubMed]
- Parkin, J.L.; Stevens, M.H.; Jung, A.L. Acquired and Congenital Subglottic Stenosis in the Infant. Ann. Otol. Rhinol. Laryngol. 1976, 85, 573–581. [Google Scholar] [CrossRef]
- Fearon, B.; Cotton, R. Surgical Correction of Subglottic Stenosis of the Larynx in Infants and Children; Progress Report. Ann. Otol. Rhinol. Laryngol. 1974, 83, 428–431. [Google Scholar] [CrossRef]
- Papsidero, M.J.; Pashley, N.R.T. Acquired Stenosis of the Upper Airway in Neonates an Increasing Problem. Ann. Otol. Rhinol. Laryngol. 1980, 89, 512–514. [Google Scholar] [CrossRef] [PubMed]
- Hartley, B.; Cotton, R. Paediatric airway stenosis: Laryngotracheal reconstruction or cricotracheal resection? Clin. Otolaryngol. 2000, 25, 342–349. [Google Scholar] [CrossRef]
- Linna, O.; Hyrynkangas, K.; Lanning, P.; Nieminen, P. Central airways stenosis in school-aged children: Differential diagnosis from asthma. Acta Paediatr. 2002, 91, 399–402. [Google Scholar] [CrossRef] [PubMed]
- Hoppe, H.; Dinkel, H.-P.; Walder, B.; von Allmen, G.; Gugger, M.; Vock, P. Grading Airway Stenosis Down to the Segmental Level Using Virtual Bronchoscopy. Chest 2004, 125, 704–711. [Google Scholar] [CrossRef]
- Iwamoto, Y.; Miyazawa, T.; Kurimoto, N.; Miyazu, Y.; Ishida, A.; Matsuo, K.; Watanabe, Y. Interventional Bronchoscopy in the Management of Airway Stenosis Due to Tracheobronchial Tuberculosis. Chest 2004, 126, 1344–1352. [Google Scholar] [CrossRef] [Green Version]
- Nakagishi, Y.; Morimoto, Y.; Fujita, M.; Ozeki, Y.; Maehara, T.; Kikuchi, M. Rabbit Model of Airway Stenosis Induced by Scraping of the Tracheal Mucosa. Laryngoscope 2005, 115, 1087–1092. [Google Scholar] [CrossRef] [PubMed]
- Freitag, L.; Ernst, A.; Unger, M.; Kovitz, K.; Marquette, C.H. A proposed classification system of central airway stenosis. Eur. Respir. J. 2007, 30, 7–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nouraei, S.A.R.; Singh, A.; Patel, A.; Ferguson, C.; Howard, D.J.; Sandhu, G.S. Early Endoscopic Treatment of Acute Inflammatory Airway Lesions Improves the Outcome of Postintubation Airway Stenosis. Laryngoscope 2006, 116, 1417–1421. [Google Scholar] [CrossRef] [PubMed]
- Hirshoren, N.; Eliashar, R. Wound-healing modulation in upper airway stenosis-Myths and facts. Head Neck 2009, 31, 111–126. [Google Scholar] [CrossRef] [PubMed]
- Kimura, M.; Miyajima, K.; Kojika, M.; Kono, T.; Kato, H. Photodynamic Therapy (PDT) with Chemotherapy for Advanced Lung Cancer with Airway Stenosis. Int. J. Mol. Sci. 2015, 16, 25466–25475. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guibert, N.; Didier, A.; Moreno, B.; Mhanna, L.; Brouchet, L.; Plat, G.; Hermant, C.; Mazieres, J. Treatment of Post-transplant Complex Airway Stenosis with a Three-Dimensional, Computer-assisted Customized Airway Stent. Am. J. Respir. Crit. Care Med. 2017, 195, e31–e33. [Google Scholar] [CrossRef] [PubMed]
- Islam, M.S.; Saha, S.C.; Young, P.M. Aerosol particle transport and deposition in a CT-based lung airway for helium-oxygen mixture. In Proceedings of the 21st Australasian Fluid Mechanics Conference, Adelaide, Australia, 10–13 December 2018. [Google Scholar]
- Larpruenrudee, P.; Islam, M.S.; Paul, G.; Paul, A.R.; Gu, Y.T.; Saha, S.C. Model for Pharmaceutical aerosol transport through stenosis airway. In Handbook of Lung Targeted Drug Delivery Systems: Recent Trends and Clinical Evidences; CRC Press: Boca Raton, FL, USA, 2021; pp. 91–128. [Google Scholar]
- Lintermann, A.; Schröder, W. Simulation of aerosol particle deposition in the upper human tracheobronchial tract. Eur. J. Mech.–B/Fluids 2017, 63, 73–89. [Google Scholar] [CrossRef]
- Tsuboi, N.; Matsumoto, S.; Nishimura, N.; Nakagawa, S.; Kobayashi, H. Fluid dynamics approach to airway obstruction. Med. Hypotheses 2019, 132, 109341. [Google Scholar] [CrossRef]
- Zhu, L.; Shen, J.; Gong, X.; Liu, L.; Liu, J.; Xu, Z. Effects of Different Modes of Mechanical Ventilation on Aerodynamics of the Patient-specific Airway: A Numerical Study. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; pp. 4961–4964. [Google Scholar] [CrossRef]
- Islam, M.S.; Saha, S.C.; Gemci, T.; Yang, I.A.; Sauret, E.; Gu, Y.T. Polydisperse Microparticle Transport and Deposition to the Terminal Bronchioles in a Heterogeneous Vasculature Tree. Sci. Rep. 2018, 8, 16387. [Google Scholar] [CrossRef]
- Singh, P.; Raghav, V.; Padhmashali, V.; Paul, G.; Islam, M.S.; Saha, S.C. Airflow and Particle Transport Prediction through Stenosis Airways. Int. J. Environ. Res. Public Health 2020, 17, 1119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weibel, E.R. Morphometry of the Human Lung; Academic Press: Cambridge, MA, USA, 1963; ISBN 978-1-4832-0076-7. [Google Scholar]
- Inthavong, K.; Tu, J.; Ahmadi, G. Computational Modelling of Gas-Particle Flows with Different Particle Morphology in the Human Nasal Cavity. J. Comput. Multiph. Flows 2009, 1, 57–82. [Google Scholar] [CrossRef] [Green Version]
- Longest, P.W.; Xi, J. Effectiveness of Direct Lagrangian Tracking Models for Simulating Nanoparticle Deposition in the Upper Airways. Aerosol Sci. Technol. 2007, 41, 380–397. [Google Scholar] [CrossRef]
- Xi, J.; Longest, P.W. Effects of Oral Airway Geometry Characteristics on the Diffusional Deposition of Inhaled Nanoparticles. J. Biomech. Eng. 2008, 130, 011008. [Google Scholar] [CrossRef] [PubMed]
- Cheng, K.-H.; Swift, D.L. Calculation of Total Deposition Fraction of Ultrafine Aerosols in Human Extrathoracic and Intrathoracic Regions. Aerosol Sci. Technol. 1995, 22, 194–201. [Google Scholar] [CrossRef]
- Islam, M.S.; Saha, S.C.; Gemci, T.; Yang, I.A.; Sauret, E.; Ristovski, Z.; Gu, Y.T. Euler-Lagrange Prediction of Diesel-Exhaust Polydisperse Particle Transport and Deposition in Lung: Anatomy and Turbulence Effects. Sci. Rep. 2019, 9, 12423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kleinstreuer, C.; Zhang, Z. Laminar-to-turbulent fluid-particle flows in a human airway model. Int. J. Multiph. Flow 2003, 29, 271–289. [Google Scholar] [CrossRef]
- Gemci, T.; Ponyavin, V.; Chen, Y.; Chen, H.; Collins, R. Computational model of airflow in upper 17 generations of human respiratory tract. J. Biomech. 2008, 41, 2047–2054. [Google Scholar] [CrossRef] [PubMed]
- Kuprat, A.; Jalali, M.; Jan, T.; Corley, R.; Asgharian, B.; Price, O.; Singh, R.; Colby, S.; Darquenne, C. Efficient bi-directional coupling of 3D computational fluid-particle dynamics and 1D Multiple Path Particle Dosimetry lung models for multiscale modeling of aerosol dosimetry. J. Aerosol Sci. 2020, 151, 105647. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Feng, Y.; Tian, G.; Taylor, C.; Arden, N.S. Influences of puff protocols and upper airway anatomy on cannabis pharmacokinetics: A CFPD-PK study. Comput. Biol. Med. 2021, 132, 104333. [Google Scholar] [CrossRef]
- Islam, M.S.; Larpruenrudee, P.; Paul, A.R.; Paul, G.; Gemci, T.; Gu, Y.; Saha, S.C. SARS-CoV-2 aerosol: How far it can travel to the lower airways? Phys. Fluids 2021, 33, 061903. [Google Scholar] [CrossRef]
- Islam, M.S.; Larpruenrudee, P.; Saha, S.; Pourmehran, O.; Paul, A.; Gemci, T.; Collins, R.; Paul, G.; Gu, Y. How severe acute respiratory syndrome coronavirus-2 aerosol propagates through the age-specific upper airways. Phys. Fluids 2021, 33, 081911. [Google Scholar] [CrossRef] [PubMed]
- Bass, K.; Thomas, M.L.; de Corput, M.P.C.K.-V.; Tiddens, H.A.W.M.; Longest, P.W. Development of characteristic airway bifurcations in cystic fibrosis. Aerosol Sci. Technol. 2021, 55, 1143–1164. [Google Scholar] [CrossRef]
- Chen, W.-H.; Chang, C.-M.; Mutuku, J.K.; Lam, S.S.; Lee, W.-J. Aerosol deposition and airflow dynamics in healthy and asthmatic human airways during inhalation. J. Hazard. Mater. 2021, 416, 125856. [Google Scholar] [CrossRef]
- Fan, Z.; Holmes, D.W.; Sauret, E.; Islam, M.S.; Saha, S.C.; Ristovski, Z.; Gu, Y.T. A multiscale modeling method incorporating spatial coupling and temporal coupling into transient simulations of the human airways. Int. J. Numer. Methods Fluids 2021, 93, 2905–2920. [Google Scholar] [CrossRef]
- Hayati, H.; Feng, Y.; Hinsdale, M. Inter-species variabilities of droplet transport, size change, and deposition in human and rat respiratory systems: An in silico study. J. Aerosol Sci. 2021, 154, 105761. [Google Scholar] [CrossRef]
- Haider, A.; Levenspiel, O. Drag coefficient and terminal velocity of spherical and nonspherical particles. Powder Technol. 1989, 58, 63–70. [Google Scholar] [CrossRef]
- Li, A.; Ahmadi, G. Dispersion and Deposition of Spherical Particles from Point Sources in a Turbulent Channel Flow. Aerosol Sci. Technol. 1992, 16, 209–226. [Google Scholar] [CrossRef]
- Saffman, P.G. The lift on a small sphere in a slow shear flow. J. Fluid Mech. 1965, 22, 385–400. [Google Scholar] [CrossRef] [Green Version]
- Kumar, B.; Srivastav, V.K.; Jain, A.; Paul, A.R. Study of Numerical Schemes for the CFD Simulation of Human Airways. Int. J. Integr. Eng. 2019, 11, 32–40. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Islam, M.R.; Larpruenrudee, P.; Rahman, M.M.; Ullah, S.; Godder, T.K.; Cui, X.; Mortazavy Beni, H.; Inthavong, K.; Dong, J.; Gu, Y.; et al. How Nanoparticle Aerosols Transport through Multi-Stenosis Sections of Upper Airways: A CFD-DPM Modelling. Atmosphere 2022, 13, 1192. https://doi.org/10.3390/atmos13081192
Islam MR, Larpruenrudee P, Rahman MM, Ullah S, Godder TK, Cui X, Mortazavy Beni H, Inthavong K, Dong J, Gu Y, et al. How Nanoparticle Aerosols Transport through Multi-Stenosis Sections of Upper Airways: A CFD-DPM Modelling. Atmosphere. 2022; 13(8):1192. https://doi.org/10.3390/atmos13081192
Chicago/Turabian StyleIslam, Md Rabiul, Puchanee Larpruenrudee, Md Mostafizur Rahman, Sana Ullah, Tapan Kumar Godder, Xinguang Cui, Hamidreza Mortazavy Beni, Kiao Inthavong, Jingliang Dong, Yuantong Gu, and et al. 2022. "How Nanoparticle Aerosols Transport through Multi-Stenosis Sections of Upper Airways: A CFD-DPM Modelling" Atmosphere 13, no. 8: 1192. https://doi.org/10.3390/atmos13081192
APA StyleIslam, M. R., Larpruenrudee, P., Rahman, M. M., Ullah, S., Godder, T. K., Cui, X., Mortazavy Beni, H., Inthavong, K., Dong, J., Gu, Y., & Islam, M. S. (2022). How Nanoparticle Aerosols Transport through Multi-Stenosis Sections of Upper Airways: A CFD-DPM Modelling. Atmosphere, 13(8), 1192. https://doi.org/10.3390/atmos13081192