
Impact of Preventive Measures on Subjective Symptoms and Antigen Sensitization against Japanese Cedar, Cypress Pollen and House Dust Mites in Patients with Allergic Rhinitis: A Retrospective Analysis in the COVID-19 Era

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Enrollment and Pollen Counts
2.2. Statistical Analyses
3. Results
3.1. Changes in the Proportions of SAR and PAR Patients
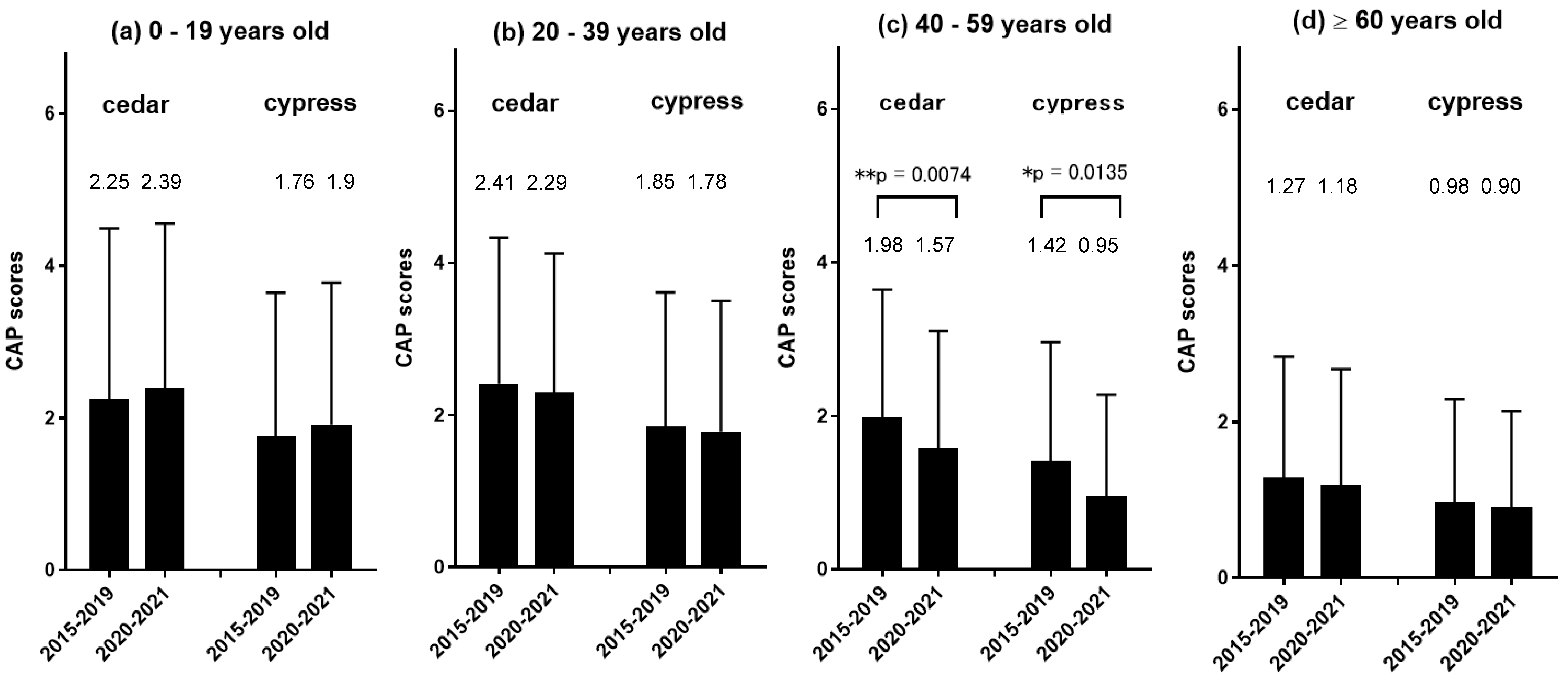
3.2. Changes in the CAP Scores for Pollens and House Dust
3.3. Changes in Subjective Nasal Symptoms after the Start of the COVID-19 Pandemic
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wu, F.; Zhao, S.; Yu, B.; Chen, Y.M.; Wang, W.; Song, Z.G.; Hu, Y.; Tao, Z.W.; Tian, J.H.; Pei, Y.Y.; et al. A new coronavirus associated with human respiratory disease in China. Nature 2020, 579, 265–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ministry of Health, Labour and Welfare (MHLW). Current situation in Japan of Coronavirus (COVID-19). Available online: https://www.mhlw.go.jp/stf/covid-19/kokunainohasseijoukyou_00006.html (accessed on 23 February 2022).
- Bun, S.; Kishimoto, K.; Shin, J.H.; Maekawa, T.; Takada, D.; Morishita, T.; Kunisawa, S.; Imanaka, Y. Impact of the COVID-19 pandemic on asthma exacerbations in children: A multi-center survey using an administrative database in Japan. Allergol. Int. 2021, 70, 489–491. [Google Scholar] [CrossRef] [PubMed]
- Okubo, K.; Kurono, Y.; Ichimura, K.; Enomoto, T.; Okamoto, Y.; Kawauchi, H.; Suzaki, H.; Fujieda, S.; Masuyama, K.; Japanese Society of Allergology. Japanese guidelines for allergic rhinitis 2020. Allergol. Int. 2020, 69, 331–345. [Google Scholar] [CrossRef] [PubMed]
- Matsubara, A.; Sakashita, M.; Gotoh, M.; Kawashima, K.; Matsuoka, T.; Kondo, S.; Yamada, T.; Takeno, S.; Takeuchi, K.; Urashima, M.; et al. Epidemiological survey of allergic rhinitis in Japan 2019. J. Otolaryngol. Jpn. 2020, 123, 485–490. (In Japanese) [Google Scholar] [CrossRef]
- Mengi, E.; Kara, C.O.; Alptürk, U.; Topuz, B. The effect of face mask usage on the allergic rhinitis symptoms in patients with pollen allergy during the covid-19 pandemic. Am. J. Otolaryngol. 2022, 43, 103206. [Google Scholar] [CrossRef] [PubMed]
- Dror, A.A.; Eisenbach, N.; Marshak, T.; Layous, E.; Zigron, A.; Shivatzki, S.; Morozov, N.G.; Taiber, S.; Alon, E.E.; Ronen, O.; et al. Reduction of allergic rhinitis symptoms with face mask usage during the COVID-19 pandemic. J. Allergy Clin. Immunol. Pract. 2020, 8, 3590–3593. [Google Scholar] [CrossRef] [PubMed]
- Air Pollutant Levels in Hiroshima Prefecture. Available online: https://www.pref.hiroshima.lg.jp/eco/e/kanshi/ (accessed on 30 May 2022).
- Sakashita, M.; Tsutsumiuchi, T.; Kubo, S.; Tokunaga, T.; Takabayashi, T.; Imoto, Y.; Kato, Y.; Yoshida, K.; Kimura, Y.; Kato, Y.; et al. Comparison of sensitization and prevalence of Japanese cedar pollen and mite-induced perennial allergic rhinitis between 2006 and 2016 in hospital workers in Japan. Allergol. Int. 2021, 70, 89–95. [Google Scholar] [CrossRef] [PubMed]
- Urashima, M.; Asaka, D.; Endo, T.; Omae, S.; Sugimoto, N.; Takaishi, S.; Mitsuyoshi, R.; Nakayama, T.; Nagakura, H.; Endo, T.; et al. Japanese cedar pollinosis in Tokyo residents born after massive national afforestation policy. Allergy 2018, 73, 2395–2397. [Google Scholar] [CrossRef] [PubMed]
- Yamada, T.; Saito, H.; Fujieda, S. Present state of Japanese cedar pollinosis: The national affliction. J. Allergy Clin. Immunol. 2014, 133, 632–639.e5. [Google Scholar] [CrossRef] [PubMed]
- Lambert, C.; Sarrat, A.; Bienvenu, F.; Brabant, S.; Nicaise-Roland, P.; Alyanakian, M.A.; Apoil, P.A.; Capron, C.; Couderc, R.; Evrard, B.; et al. The importance of EN ISO 15189 accreditation of allergen-specific IgE determination for reliable in vitro allergy diagnosis. Allergy 2015, 70, 180–186. [Google Scholar] [CrossRef] [PubMed]
- Okawa, T.; Konno, A.; Yamakoshi, T.; Numata, T.; Terada, N.; Shima, M. Analysis of natural history of Japanese cedar pollinosis. Int. Arch. Allergy Immunol. 2003, 131, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Itoh, S.; Horibe, Y.; Takeno, S.; Takahara, D.; Takemoto, K.; Sasaki, A.; Kono, T.; Taruya, T.; Ishino, T.; Hamamoto, T.; et al. Changes in the level of dispersion and the degree of antigen sensitization of Japanese cedar and cypress pollen in allergic rhinitis patients in Hiroshima prefecture. Pract. Oto-Rhino-Laryngol. 2020, 113, 481–486. (In Japanese) [Google Scholar] [CrossRef]
- Oberg, T.; Brosseau, L.M. Surgical mask filter and fit performance. Am. J. Infect. Control 2008, 36, 276–282. [Google Scholar] [CrossRef] [PubMed]
- Dubini, M.; Robotti, C.; Benazzo, M.; Rivolta, F. Impact of quarantine and face masks on ragweed-induced oculorhinitis during the COVID-19 pandemic in Northern Italy. Int. Forum. Allergy Rhinol. 2021, 12, 220–222. [Google Scholar] [CrossRef] [PubMed]
- Acevedo, N.; Zakzuk, J.; Caraballo, L. House dust mite allergy under changing environments. Allergy Asthma Immunol. Res. 2019, 11, 450–469. [Google Scholar] [CrossRef] [PubMed]
- d’Alessandro, M.; Bergantini, L.; Perrone, A.; Cameli, P.; Beltrami, V.; Alderighi, L.; Pini, L.; Bargagli, E.; Saletti, M. House Dust Mite Allergy and the Der p1 Conundrum: A Literature Review and Case Series. Allergies 2021, 1, 8. [Google Scholar] [CrossRef]
- Yonekura, S.; Okamoto, Y.; Horiguchi, S.; Sakurai, D.; Chazono, H.; Hanazawa, T.; Okawa, T.; Aoki, S.; Konno, A. Effects of aging on the natural history of seasonal allergic rhinitis in middle-aged subjects in South chiba, Japan. Int. Arch. Allergy Immunol. 2012, 157, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Nishijima, C.; Miyagawa, N.; Tsuboyama-Kasaoka, N.; Chiba, T.; Miyachi, M. Association between lifestyle changes and at-home hours during and after the state of emergency due to the COVID-19 pandemic in Japan. Nutrients 2021, 13, 2698. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pre-COVID-19 Era (2015–2019) | COVID-19 Era (2020–2021) | ||
|---|---|---|---|
| Patient, n (male/female) | Age, yrs. | ||
| 0–19 | 522 (316/206) | 200 (124/76) | |
| 20–39 | 268 (137/131) | 95 (48/47) | |
| 40–59 | 421 (223/198) | 164 (79/85) | |
| ≥60 | 668 (347/321) | 227 (130/97) | |
| Antigen-positive, n | Cedar/cypress | 999 (523/476) | 361 (181/180) |
| House dust | 667 (389/278) | 195 (108/87) |
| Pre-COVID-19 Era (2015–2019) | COVID-19 Era (2020–2021) | ||
| Mean season pollen counts, /cm2 (range) | Cedar | 4749.8 (1982–10,194) | 7542.8 (3403–11,682) |
| Cypress | 2812.8 (449–7051) | 1788.1 (1764–1812) | |
| Mean pollen dispersion period, days (range) | Cedar | 45.0 (36–56) | 48.5 (43–54) |
| Cypress | 28.6 (20–37) | 56.0 (48–64) | |
| Mean air pollutant level (range) | PM2.5, μg/m3 | 12.56 (11.1–13.7) | 11.6 (10–13.2) |
| SO2 and NOx, ppm | 0.0136 (0.012–0.015) | 0.0115 (0.011–0.012) |
| Pre-COVID-19 Era (2015–2019) | □ | ||||||||
| Patient, % | Cedar | Cypress | House Dust | ||||||
| CAP Score | 2–3 | ≥4 | Total (Male/Female) | 2–3 | ≥4 | Total (Male/Female) | 2–3 | ≥4 | Total (Male/Female) |
| Age, years | |||||||||
| 0–9 | 18.5 | 31.5 | 50.1 (51.9/44.5) | 23.9 | 19 | 42.9 (43.7/41.5) | 12.6 | 28.2 | 40.9 (50.8/24.3) |
| 10–19 | 23 | 39.5 | 62.6 (62.7/62.5) | 28.7 | 30.1 | 58.9 (59.2/58.5) | 14.7 | 51.9 | 66.6 (72.4/60) |
| 20–29 | 29.6 | 36.3 | 65.9 (71/60) | 39.2 | 20.6 | 59.8 (63.4/55.5) | 26.3 | 50.8 | 77.1 (80.3/73.6) |
| 30–39 | 35.6 | 30.3 | 65.9 (70/62.5) | 29.2 | 22.9 | 52.1 (57.1/48.1) | 29.2 | 35 | 64.2 (71.9/57.1) |
| 40–49 | 41.7 | 21.1 | 62.7 (62.76/62.7) | 38.7 | 9.3 | 54.6 (61.3/45.1) | 32.6 | 26 | 59.3 (65.5/51.2) |
| 50–59 | 45.4 | 18.2 | 63.6 (60.4/66.1) | 43.3 | 9.4 | 48.6 (44.4/57.5) | 24.7 | 14.6 | 39.4 (40.6/38.3) |
| 60–69 | 34.9 | 12.6 | 47.5 (47.5/47.5) | 33.9 | 4.3 | 38.2 (32.2/44.4) | 21.8 | 6.4 | 28.2 (30.7/25.3) |
| 70–79 | 28.6 | 10.7 | 39.3 (38.7/40) | 32.1 | 5 | 37.1 (38/36.2) | 14.8 | 3.6 | 18.4 (20.4/16.1) |
| 80– | 21.6 | 4.5 | 26.1 (31.7/21.3) | 24.4 | 0 | 24.4 (33.3/16.7) | 10.3 | 5.7 | 16.1 (17.1/15.2) |
| □ | COVID-19 Era (2020–2021) | ||||||||
| Patient, % | Cedar | Cypress | House Dust | ||||||
| CAP Score | 2–3 | ≥4 | Total (Male/Female) | 2–3 | ≥4 | Total (Male/Female) | 2–3 | ≥4 | Total (Male/Female) |
| Age, years | |||||||||
| 0–9 | 12.9 | 37 | 50 (49.2/52.1) | 25.9 | 16.8 | 42.8 (40.4/48.2) | 19.7 | 26.7 | 46.4 (48.7/43.3) |
| 10–19 | 24.4 | 45.3 | 69.7 (70.0/69.0) | 41 | 33.9 | 75 (57.5/71.8) | 21.5 | 39.2 | 60.7 (58.6/63.6) |
| 20–29 | 28.3 | 35.8 | 64.1 (64/64.2) | 27.7 | 27.7 | 55.5 (50/66.6) | 15.3 | 38.4 | 53.8 (50/56.5) ** |
| 30–39 | 41.8 | 18.6 | 60.4 (55/65.2) | 41.3 | 3.4 | 44.8 (38.4/50) | 23.3 | 16.6 | 40 (46.6/33.3) * |
| 40–49 | 42.8 | 11.9 | 54.7 (57.8/52.1) † | 28.3 | 5.6 | 33.9 (31/37.5) ** | 34.9 | 20.6 | 55.5 (43.5/52.9) |
| 50–59 | 37.6 | 10.5 | 48.2 (40.5/54.1) * | 28.5 | 0 | 28.6 (30.3/26.6) ** | 19.4 | 13.4 | 32.8 (44.8/23.6) |
| 60–69 | 41 | 3.6 | 44.6 (45.1/43.7) | 22.7 | 0 | 22.7 (24/22.2) * | 18.3 | 5 | 23.3 (29.7/13) |
| 70–79 | 33 | 13.2 | 46.2 (41.6/52.1) | 37.2 | 1.6 | 38.3 (31/45.1) | 24.4 | 1.1 | 25.5 (28/22.5) |
| 80– | 16.2 | 2.7 | 18.9 (10.5/27.8) | 21.4 | 0 | 25 (22.2/20) | 11.5 | 0 | 11.5 (7.1/16.6) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oda, T.; Maeda, F.; Takeno, S.; Tsuru, Y.; Ishikawa, C.; Ishino, T.; Takemoto, K.; Hamamoto, T.; Ueda, T.; Kawasumi, T.; et al. Impact of Preventive Measures on Subjective Symptoms and Antigen Sensitization against Japanese Cedar, Cypress Pollen and House Dust Mites in Patients with Allergic Rhinitis: A Retrospective Analysis in the COVID-19 Era. Atmosphere 2022, 13, 1000. https://doi.org/10.3390/atmos13071000
Oda T, Maeda F, Takeno S, Tsuru Y, Ishikawa C, Ishino T, Takemoto K, Hamamoto T, Ueda T, Kawasumi T, et al. Impact of Preventive Measures on Subjective Symptoms and Antigen Sensitization against Japanese Cedar, Cypress Pollen and House Dust Mites in Patients with Allergic Rhinitis: A Retrospective Analysis in the COVID-19 Era. Atmosphere. 2022; 13(7):1000. https://doi.org/10.3390/atmos13071000
Chicago/Turabian StyleOda, Takashi, Fumiaki Maeda, Sachio Takeno, Yuri Tsuru, Chie Ishikawa, Takashi Ishino, Kota Takemoto, Takao Hamamoto, Tsutomu Ueda, Tomohiro Kawasumi, and et al. 2022. "Impact of Preventive Measures on Subjective Symptoms and Antigen Sensitization against Japanese Cedar, Cypress Pollen and House Dust Mites in Patients with Allergic Rhinitis: A Retrospective Analysis in the COVID-19 Era" Atmosphere 13, no. 7: 1000. https://doi.org/10.3390/atmos13071000
APA StyleOda, T., Maeda, F., Takeno, S., Tsuru, Y., Ishikawa, C., Ishino, T., Takemoto, K., Hamamoto, T., Ueda, T., Kawasumi, T., Iwamoto, H., Kubota, K., Nakao, Y., & Kunimoto, M. (2022). Impact of Preventive Measures on Subjective Symptoms and Antigen Sensitization against Japanese Cedar, Cypress Pollen and House Dust Mites in Patients with Allergic Rhinitis: A Retrospective Analysis in the COVID-19 Era. Atmosphere, 13(7), 1000. https://doi.org/10.3390/atmos13071000