
Changing Emissions Results in Changed PM2.5 Composition and Health Impacts


Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Policies and Economic Drivers Affecting PM2.5 Concentrations
3.1.1. Electricity Generating Units
3.1.2. Vehicles and Liquid Fuel Quality
3.2. Trends in Concentrations
3.3. Source Apportionments
3.4. Trends in Source Contributions
3.5. Trends in Health Outcomes
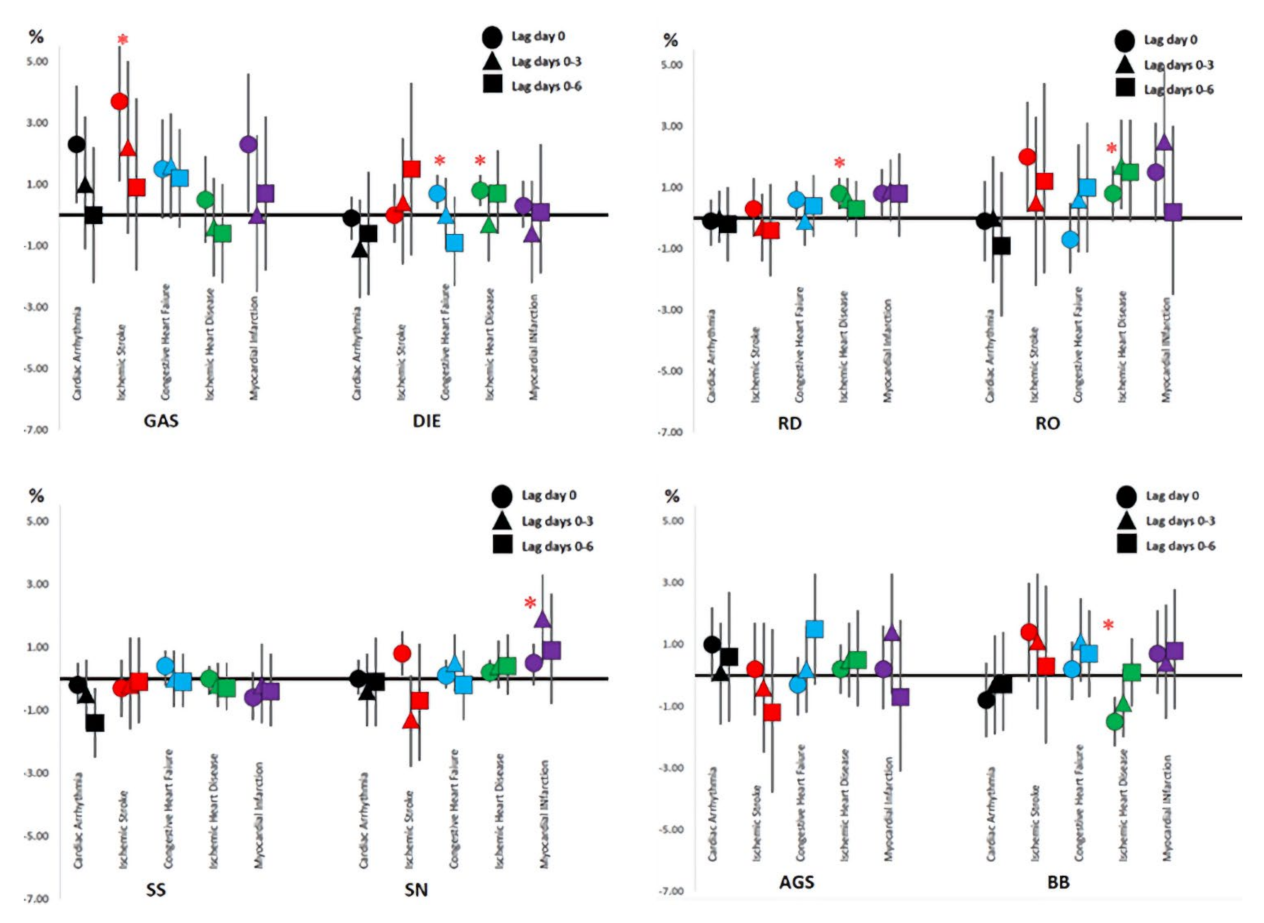
3.5.1. Cardiovascular Diseases
3.5.2. Respiratory Infections
3.5.3. Respiratory Diseases
4. Discussion
4.1. Changes in PM2.5 Composition
4.2. Changes in Health Outcomes
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- U.S. Environmental Protection Agency (US EPA). Inhalable Particulate Network Annual Report: Operation and Data Summary (Mass Concentrations Only); April 1979–June 1980, Report No. EPA-600/4-81-037; US Environmental Protection Agency: Washington, DC, USA, 1981; p. 265.
- Particulate Matter (PM2.5) Trends. Available online: https://www.epa.gov/air-trends/particulate-matter-pm25-trends (accessed on 21 December 2021).
- Squizzato, S.; Masiol, M.; Rich, D.Q.; Hopke, P.K. PM2.5 and gaseous pollutants in New York State during 2005–2016: Spatial variability, temporal trends, and economic influences. Atmos. Environ. 2018, 183, 209–224. [Google Scholar] [CrossRef]
- Blanchard, C.L.; Shaw, S.L.; Edgerton, E.S.; Schwab, J.J. Emission influences on air pollutant concentrations in New York State: I. ozone. Atmos. Environ. X 2019, 3, 100033. [Google Scholar] [CrossRef]
- Blanchard, C.L.; Shaw, S.L.; Edgerton, E.S.; Schwab, J.J. Emission influences on air pollutant concentrations in New York state: II. PM2.5 organic and elemental carbon constituents. Atmos. Environ. X 2019, 3, 100039. [Google Scholar] [CrossRef]
- Pitiranggon, M.; Johnson, S.; Haney, J.; Eisl, H.; Ito, K. Long-term trends in local and transported PM2.5 pollution in New York City. Atmos. Environ. 2021, 248, 118238. [Google Scholar] [CrossRef]
- Squizzato, S.; Masiol, M.; Rich, D.Q.; Hopke, P.K. A long-term source apportionment of PM2.5 in New York State during 2005–2016. Atmos. Environ. 2018, 192, 35–47. [Google Scholar] [CrossRef]
- Masiol, M.; Squizzato, S.; Rich, D.Q.; Hopke, P.K. Long-term trends (2005–2016) of source apportioned PM2.5 across New York State. Atmos. Environ. 2019, 201, 110–120. [Google Scholar] [CrossRef]
- Zhang, W.; Lin, S.; Hopke, P.K.; Thurston, S.W.; Van Wijngaarden, E.; Croft, D.; Squizzato, S.; Masiol, M.; Rich, D.Q. Triggering of cardiovascular hospital admissions by fine particle concentrations in New York state: Before, during, and after implementation of multiple environmental policies and a recession. Environ. Pollut. 2018, 242, 1404–1416. [Google Scholar] [CrossRef]
- Rich, D.Q.; Zhang, W.; Shao, L.; Squizzato, S.; Thurston, S.W.; van Wijngaarden, E.; Croft, D.; Masiol, M.; Hopke, P.K. Triggering of cardiovascular hospital admissions by source specific fine particle concentrations in urban centers of New York State. Environ. Int. 2019, 126, 387–394. [Google Scholar] [CrossRef]
- Solomon, P.A.; Crumpler, D.; Flanagan, J.B.; Jayanty, R.K.M.; Rickman, E.E.; McDade, C.E.U.S. National PM2.5Chemical Speciation Monitoring Networks—CSN and IMPROVE: Description of networks. J. Air Waste Manag. Assoc. 2014, 64, 1410–1438. [Google Scholar] [CrossRef] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2017; Available online: https://www.R-project.org/ (accessed on 21 December 2021).
- Carslaw, D.C.; Ropkins, K. Openair—An R package for air quality data analysis. Environ. Model. Softw. 2012, 27–28, 52–61. [Google Scholar] [CrossRef]
- Maclure, M. 1991. The case-crossover design: A method for studying transient effects on the risk of acute events. Am. J. Epidemiol. 1991, 133, 144e153. [Google Scholar] [CrossRef] [PubMed]
- Levy, D.; Lumley, T.; Sheppard, L.; Kaufman, J.; Checkoway, H. Referent Selection in Case-Crossover Analyses of Acute Health Effects of Air Pollution. Epidemiology 2001, 12, 186–192. [Google Scholar] [CrossRef] [PubMed]
- Croft, D.P.; Zhang, W.; Lin, S.; Thurston, S.W.; Hopke, P.K.; Masiol, M.; Squizzato, S.; Van Wijngaarden, E.; Utell, M.J.; Rich, D.Q. The Association between Respiratory Infection and Air Pollution in the Setting of Air Quality Policy and Economic Change. Ann. Am. Thorac. Soc. 2019, 16, 321–330. [Google Scholar] [CrossRef] [PubMed]
- Hopke, P.K.; Croft, D.; Zhang, W.; Shao, L.; Masiol, M.; Squizzato, S.; Thurston, S.W.; van Wijngaarden, E.; Utell, M.J.; Rich, D.Q. Changes in the acute response of respiratory disease to PM2.5 in New York state from 2005 to 2016. Sci. Total Environ. 2019, 677, 328–339. [Google Scholar] [CrossRef] [PubMed]
- Croft, D.P.; Zhang, W.; Lin, S.; Thurston, S.W.; Hopke, P.K.; Van Wijngaarden, E.; Squizzato, S.; Masiol, M.; Utell, M.J.; Rich, D.Q. The associations between source specific particulate matter and of respiratory infections in New York state adults. Environ. Sci. Technol. 2020, 54, 975–984. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hopke, P.K.; Croft, D.; Zhang, W.; Shao, L.; Masiol, M.; Squizzato, S.; Thurston, S.W.; van Wijngaarden, E.; Utell, M.J.; Rich, D.Q. Changes in the hospitalization and ED visit rates for respiratory diseases associated with source-specific PM2.5 in New York State from 2005 to 2016. Environ. Res. 2020, 181, 108912. [Google Scholar] [CrossRef]
- U.S. EPA. Finding of Significant Contribution and Rulemaking for Certain States in the Ozone Transport Assessment Group Region for Purposes of Reducing Regional Transport of Ozone. Fed. Regist. 1998, 63, 57356–57538. [Google Scholar]
- Napolitano, S.; Stevens, G.; Schreifels, J.; Culligan, K. The NOx Budget Trading Program: A Collaborative, Innovative Approach to Solving a Regional Air Pollution Problem. Electr. J. 2007, 20, 65–76. [Google Scholar] [CrossRef]
- U.S. EPA. Cross-state Air Pollution Rule Update for the 2008 Ozone NAAQS. Fed. Regist. 2015, 80, 75706–75778. [Google Scholar]
- U.S. EPA. Cross-state Air Pollution Rule Update for the 2008 Ozone NAAQS. Fed. Regist. 2016, 81, 74504–74650. [Google Scholar]
- U.S. EPA. Revised Cross-State Air Pollution Rule Update for the 2008 Ozone NAAQS. Fed. Regist. 2021, 86, 23054–23235. [Google Scholar]
- U.S. Department of Justice. 2007. Available online: https://www.justice.gov/enrd/us-v-american-elect-power-co (accessed on 21 December 2021).
- U.S. EPA. Control of Air Pollution from New Motor Vehicles: Tier 2 Motor Vehicle Emissions Standards and Gasoline Sulfur Control Requirements. Fed. Regist. 2000, 65, 6698–6870. [Google Scholar]
- U.S. EPA. Control of Emissions of Air Pollution From 2004 and Later Model Year Heavy-Duty Highway Engines and Vehicles; Revision of Light-Duty Truck Definition. Fed. Regist. 1999, 64, 58472–58566. [Google Scholar]
- U.S. EPA. Highway and Nonroad, Locomotive, and Marine (NRLM) Diesel Fuel Sulfur Standards. Office of Transportation and Air Quality EPA-420-B-16–1005. 2016. Available online: https://nepis.epa.gov/Exe/ZyPDF.cgi?Dockey=P100O9ZI.pdf (accessed on 21 December 2021).
- U.S. EPA. Control of Emissions of Air Pollution from Nonroad Diesel Engines and Fuel; Final Rule. Fed. Regist. 2004, 69, 38958–39273. [Google Scholar]
- Kheirbek, I.; Haney, J.; Douglas, S.; Ito, K.; Caputo, S., Jr.; Matte, T. The public health benefits of reducing fine particulate matter through conversion to cleaner heating fuels in New York City. Environ. Sci. Technol. 2014, 48, 13573–13582. [Google Scholar] [CrossRef] [PubMed]
- Theil, H. A Rank-Invariant Method of Linear and Polynomial Regression Analysis. In Henri Theil’s Contributions to Economics and Econometrics; Springer: Dordrecht, The Netherlands, 1992; pp. 345–381. [Google Scholar]
- Sen, P.K. Estimates of the regression coefficient based on Kendall’s tau. J. Am. Stat. Assoc. 1968, 63, 1379–1389. [Google Scholar] [CrossRef]
- Chow, J.C.; Watson, J.G.; Chen, L.-W.A.; Chang, M.C.O.; Robinson, N.F.; Trimble, D.; Kohl, S. The IMPROVE_A Temperature Protocol for Thermal/Optical Carbon Analysis: Maintaining Consistency with a Long-Term Database. J. Air Waste Manag. Assoc. 2007, 57, 1014–1023. [Google Scholar] [CrossRef] [Green Version]
- Kim, E.; Hopke, P.K.; Edgerton, E.S. Improving Source Identification of Atlanta Aerosol Using Temperature-Resolved Carbon Fractions in Positive Matrix Factorization. Atmos. Environ. 2004, 38, 3349–3362. [Google Scholar] [CrossRef]
- Kim, E.; Hopke, P.K. Source apportionment of fine particles at Washington, DC utilizing temperature resolved carbon fractions. J. Air Waste Manage. Assoc. 2004, 54, 773–785. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Hopke, P.K.; Rattigan, O.V.; Chalupa, D.C.; Utell, M.J. Multiple-year black carbon measurements and source apportionment using delta-C in Rochester, New York. J. Air Waste Manag. Assoc. 2012, 62, 880–887. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.; Hopke, P.K.; Xia, X.; Rattigan, O.V.; Chalupa, D.C.; Utell, M.J. Source apportionment of airborne particulate matter using inorganic and organic species as tracers. Atmos. Environ. 2012, 55, 525–532. [Google Scholar] [CrossRef]
- Kim, E.; Hopke, P.K. Improving source identification of fine particles in a rural northeastern U.S. area utilizing temperature resolved carbon fractions. J. Geophys. Res. 2004, 109, D09204. [Google Scholar] [CrossRef]
- Kruskal, W.H.; Wallis, W.A. Use of Ranks in One-Criterion Variance Analysis. J. Am. Stat. Assoc. 1952, 47, 583–621. [Google Scholar] [CrossRef]
- Zhao, Y.; Lambe, A.T.; Saleh, R.; Saliba, G. Secondary Organic Aerosol Production from Gasoline Vehicle Exhaust: Effects of Engine Technology, Cold Start, and Emission Certification Standard. Environ. Sci. Technol. 2018, 52, 1253–1261. [Google Scholar] [CrossRef]
- Zhao, Y.L.; Hennigan, C.J.; May, A.A.; Tkacik, D.S.; de Gouw, J.A.; Gilman, J.B.; Kuster, W.C.; Borbon, A.; Robinson, A.L. Intermediate-Volatility Organic Compounds: A Large Source of Secondary Organic Aerosol. Environ. Sci. Technol. 2014, 48, 13743–13750. [Google Scholar] [CrossRef]
- Lim, H.-J.; Turpin, B.J. Origins of Primary and Secondary Organic Aerosol in Atlanta: Results of Time-Resolved Measurements during the Atlanta Supersite Experiment. Environ. Sci. Technol. 2002, 36, 4489–4496. [Google Scholar] [CrossRef]
- Robinson, A.L.; Donahue, N.M.; Shrivastava, M.; Weitkamp, E.A.; Sage, A.M.; Grieshop, A.P.; Lane, T.E.; Pierce, J.R.; Pandis, S.N. Rethinking Organic Aerosol: Semivolatile Emissions and Photochemical Aging. Science 2007, 315, 1259–1262. [Google Scholar] [CrossRef]
- Li, X.; Han, J.; Hopke, P.K.; Hu, J.; Shu, Q.; Chang, Q.; Ying, Q. Quantifying primary and secondary humic-like substances in urban aerosol based on emission source characterization and a source-oriented air quality model. Atmos. Chem. Phys. 2019, 19, 2327–2341. [Google Scholar] [CrossRef] [Green Version]
- Hopke, P.K. Chapter 1: Reactive ambient particles. In Air Pollution and Health Effects, Molecular and Integrative Toxicology; Nadadur, S.S., Hollingsworth, J.W., Eds.; Springer: London, UK, 2015; pp. 1–24. [Google Scholar]
- Anastasopolos, A.T.; Sofowote, U.M.; Hopke, P.K.; Rouleau, M.; Shin, T.; Dheri, A.; Peng, H.; Kulka, R.; Gibson, M.D.; Farah, P.-M.; et al. Air quality in Canadian port cities after regulation of low-sulphur marine fuel in the North American Emissions Control Area. Sci. Total. Environ. 2021, 791, 147949. [Google Scholar] [CrossRef]
- Docherty, K.S.; Wu, W.; Lim, Y.B.; Ziemann, P.J. Contributions of organic peroxides to secondary organic aerosol formed from reactions of monoterpenes with O3. Environ. Sci. Technol. 2005, 39, 4049–4059. [Google Scholar] [CrossRef]
- Chen, X.; Hopke, P.K.; Carter, W.P.L. Secondary organic aerosol from ozonolysis of biogenic volatile organic compounds: Chamber studies of particle and reactive oxygen species formation. Environ. Sci. Technol. 2010, 45, 276–282. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.; Cheng, Y.; Qiu, X.; Cao, G.; Fang, Y.; Wang, J.; Zhu, T.; Yu, J.; Hu, D. Sources and oxidative potential of water-soluble humic-like substances (HULISWS) in fine particulate matter (PM2.5) in Beijing. Atmos. Chem. Phys. 2018, 18, 5607–5617. [Google Scholar] [CrossRef] [Green Version]
- Sarkar, K.; Sil, P.C. Infectious Lung Diseases and Endogenous Oxidative Stress. Oxidative Stress Lung Dis. 2019, 2, 125–148. [Google Scholar]
- Kozlov, E.M.; Ivanova, E.; Grechko, A.V.; Wu, W.-K.; Starodubova, A.V.; Orekhov, A.N. Involvement of Oxidative Stress and the Innate Immune System in SARS-CoV-2 Infection. Diseases 2021, 9, 17. [Google Scholar] [CrossRef] [PubMed]
- Bi, J.; D’Souza, R.R.; Rich, D.Q.; Hopke, P.K.; Russell, A.G.; Liu, Y.; Chang, H.H.; Ebelt, S. Temporal changes in short-term associations between cardiorespiratory emergency department visits and PM2.5 in Los Angeles, 2005 to 2016. Environ. Res. 2020, 190, 109967. [Google Scholar] [CrossRef] [PubMed]
- Hopke, P.K.; Hill, E.L. Health and charge benefits from decreasing PM2.5 concentrations in New York State: Effects of changing compositions. Atmos. Pollut. Res. 2021, 12, 47–53. [Google Scholar] [CrossRef]
- Abrams, J.Y.; Klein, M.; Henneman, L.R.F.; Sarnat, S.E.; Chang, H.H.; Strickland, M.J.; Mulholland, J.A.; Russell, A.G.; Tolbert, P.E. Impact of air pollution control policies on cardiorespiratory emergency department visits, Atlanta, GA, 1999–2013. Environ. Int. 2019, 126, 627–634. [Google Scholar] [CrossRef] [PubMed]
- Henneman, L.R.F.; Liu, C.; Chang, H.; Mulholland, J.; Tolbert, P.; Russell, A. Air quality accountability: Developing long-term daily time series of pollutant changes and uncertainties in Atlanta, Georgia resulting from the 1990 Clean Air Act Amendments. Environ. Int. 2019, 123, 522–534. [Google Scholar] [CrossRef]
- Russell, A.G.; Tolbert, P.E.; Henneman, L.R.F.; Abrams, J.; Liu, C.; Klein, M.; Mulholland, J.A.; Sarnat, S.; Hu, Y.; Chang, H.H.; et al. Impacts of regulations on air quality and emergency department visits in the Atlanta metropolitan area, 1999–2013. In Research Report 195; Health Effects Institute: Boston, MA, USA, 2018. [Google Scholar]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Site | All | Winter | Summer | Transition |
|---|---|---|---|---|
| Slope (l.ci, u.ci; p-Value) % y−1[Start Date–End Date] | Slope (l.ci, u.ci; p-Value) % y−1[Start Date–End Date] | Slope (l.ci, u.ci; p-Value) % y−1[Start Date–End Date] | Slope (l.ci, u.ci; p-Value) % y−1[Start Date–End Date] | |
| Albany | −3.8 (−4.4, −3.1; 0) [1 January 2005–12 January 2016] | −4.2 (−5.6, −2.5; 0) [1 January 2005–12 January 2016] | −4.6 (−5.5, −3.4; 0) [6 January 2005–8 January 2016] | −3.3 (−4.3, −2.5; 0) [3 January 2005–11 January 2016] |
| Buffalo | −3.7 (−4.1, −3.1; 0) [1 January 2005–12 January 2016] | −4.2 (−5.2, −2.7; 0) [1 January 2005–12 January 2016] | −4.3 (−5.6, −3.2; 0) [6 January 2005–8 January 2016] | −3.7 (−4.6, −2.6; 0) [3 January 2005–11 January 2016] |
| Rochester | −3.4 (−3.9, −2.7; 0) [1 January 2005–12 January 2016] | −3.3 (−4.7, −1.8; 0) [1 January 2005–12 January 2016] | −4 (−5.4, −1.8; 0) [6 January 2005–8 January 2016] | −3.6 (−4.6, −2.3; 0) [3 January 2005–11 January 2016] |
| Manhattan | −3.7 (−4.5, −2.8; 0) [3 January 2007–12 January 2016] | −2.5 (−4.4, 0.4; 0.07) [12 January 2007–12 January 2016] | −5.9 (−6.5, −3.3; 0) [6 January 2007–8 January 2016] | −3.4 (−4.3, −2.4; 0) [3 January 2007–11 January 2016] |
| Bronx | −3.3 (−3.7, −2.5; 0) [1 January 2005–12 January 2016] | −3.1 (−3.7, −2.3; 0) [1 January 2005–12 January 2016] | −5 (−5.6, −4; 0) [6 January 2005–8 January 2016] | −3.5 (−4.3, −2.7; 0) [3 January 2005–11 January 2016] |
| Queens | −3.9 (−4.3, −3.3; 0) [1 January 2005–12 January 2016] | −3 (−4.3, −1.6; 0) [1 January 2005–12 January 2016] | −4.8 (−5.4, −4.2; 0) [6 January 2005–8 January 2016] | −3.6 (−4.4, −2.8; 0) [3 January 2005–11 January 2016] |
| Source | Secondary Sulfate | Secondary Nitrate | Spark-Ignition | Diesel | Road Dust | Biomass Burning | OP-Rich | Aged Sea Salt | Road Salt | Fresh Sea Salt | Residual Oil | Industrial |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Albany | ||||||||||||
| pre-OC/EC change | 4.0 ± 5.5 | 1.6 ± 1.8 | 1.5 ± 1.5 | 1.9 ± 1.7 | 0.4 ± 0.5 | 0.5 ± 0.5 | 0.1 ± 0.3 | |||||
| post-OC/EC change | 2.1 ± 2.0 | 0.9 ± 1.3 | 2.2 ± 2.0 | 0.5 ± 0.3 | 0.2 ± 0.2 | 0.4 ± 0.5 | 1.2 ± 1.3 | 0.1 ± 0.5 | ||||
| Bronx | ||||||||||||
| pre-OC/EC change | 4.3 ± 4.9 | 3.1 ± 3.9 | 1.5 ± 1.6 | 1.4 ± 1.0 | 0.3 ± 0.3 | 0.3 ± 0.5 | 0.8 ± 0.9 | 0.4 ± 1.1 | 1.0 ± 1.0 | |||
| post-OC/EC change | 2.7 ± 3.5 | 0.7 ± 1.0 | 2.0 ± 1.9 | 0.8 ± 0.5 | 0.4 ± 0.4 | 0.1 ± 0.2 | 1.4 ± 1.8 | 0.4 ± 0.6 | 0.1 ± 0.3 | 1.0 ± 1.1 | ||
| Buffalo | ||||||||||||
| pre-OC/EC change | 4.4 ± 5.3 | 1.7 ± 2.2 | 1.2 ± 1.4 | 1.9 ± 1.6 | 0.2 ± 0.2 | 1.1 ± 1.1 | 0.5 ± 1.5 | 0.3 ± 0.3 | ||||
| post-OC/EC change | 2.6 ± 3.3 | 1.6 ± 2.4 | 1.5 ± 1.7 | 0.6 ± 0.4 | 0.2 ± 0.2 | 0.6 ± 0.7 | 0.9 ± 1.0 | 0.0 ± 0.1 | 0.2 ± 0.1 | |||
| Manhattan | ||||||||||||
| pre-OC/EC change | 4.5 ± 5.7 | 3.9 ± 4.4 | 1.0 ± 0.9 | 1.6 ± 1.2 | 1.0 ± 0.8 | 0.5 ± 0.7 | 0.7 ± 0.8 | 0.4 ± 1.0 | 0.6 ± 0.7 | |||
| post-OC/EC change | 2.4 ± 2.7 | 1.1 ± 1.5 | 1.9 ± 2.0 | 1.3 ± 0.7 | 0.5 ± 0.5 | 0.3 ± 0.3 | 1.7 ± 2.3 | 0.6 ± 0.7 | 0.1 ± 0.2 | 0.6 ± 0.8 | ||
| Queens | ||||||||||||
| pre-OC/EC change | 4.7 ± 5.1 | 2.2 ± 2.7 | 1.5 ± 1.5 | 1.4 ± 1.1 | 0.5 ± 0.5 | 0.6 ± 0.7 | 0.3 ± 0.4 | 0.3 ± 0.7 | 0.4 ± 0.5 | |||
| post-OC/EC change | 2.2 ± 2.3 | 1.1 ± 1.7 | 1.7 ± 1.6 | 0.7 ± 0.5 | 0.3 ± 0.3 | 0.3 ± 0.3 | 0.9 ± 1.0 | 0.6 ± 0.7 | 0.1 ± 0.2 | 0.4 ± 0.5 | ||
| Rochester | ||||||||||||
| pre-OC/EC change | 3.6 ± 4.6 | 2.6 ± 3.3 | 1.5 ± 1.4 | 0.4 ± 0.3 | 0.2 ± 0.2 | 0.8 ± 1.1 | 0.2 ± 0.3 | |||||
| post-OC/EC change | 2.1 ± 2.5 | 1.5 ± 2.3 | 1.4 ± 1.6 | 0.8 ± 0.6 | 0.1 ± 0.1 | 0.6 ± 0.5 | 0.6 ± 0.6 | 0.1 ± 0.2 |
| GDI Market Share | ||
|---|---|---|
| Model Year | Cars | Light Trucks |
| 2007 | 0.3% | 0.00% |
| 2008 | 3.1% | 1.10% |
| 2009 | 4.2% | 4.20% |
| 2010 | 9.2% | 6.8% |
| 2011 | 18.4% | 11.3% |
| 2012 | 27.4% | 13.5% |
| 2013 | 37.3% | 18.4% |
| 2014 | 42.7% | 29.7% |
| 2015 | 44.0% | 39.0% |
| 2016 | 50.7% | 43.2% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hopke, P.K.; Hidy, G. Changing Emissions Results in Changed PM2.5 Composition and Health Impacts. Atmosphere 2022, 13, 193. https://doi.org/10.3390/atmos13020193
Hopke PK, Hidy G. Changing Emissions Results in Changed PM2.5 Composition and Health Impacts. Atmosphere. 2022; 13(2):193. https://doi.org/10.3390/atmos13020193
Chicago/Turabian StyleHopke, Philip K., and George Hidy. 2022. "Changing Emissions Results in Changed PM2.5 Composition and Health Impacts" Atmosphere 13, no. 2: 193. https://doi.org/10.3390/atmos13020193
APA StyleHopke, P. K., & Hidy, G. (2022). Changing Emissions Results in Changed PM2.5 Composition and Health Impacts. Atmosphere, 13(2), 193. https://doi.org/10.3390/atmos13020193