
Association between Long-Term Exposure to PM2.5 and Lung Imaging Phenotype in CODA Cohort



Abstract
1. Introduction
2. Methods and Materials
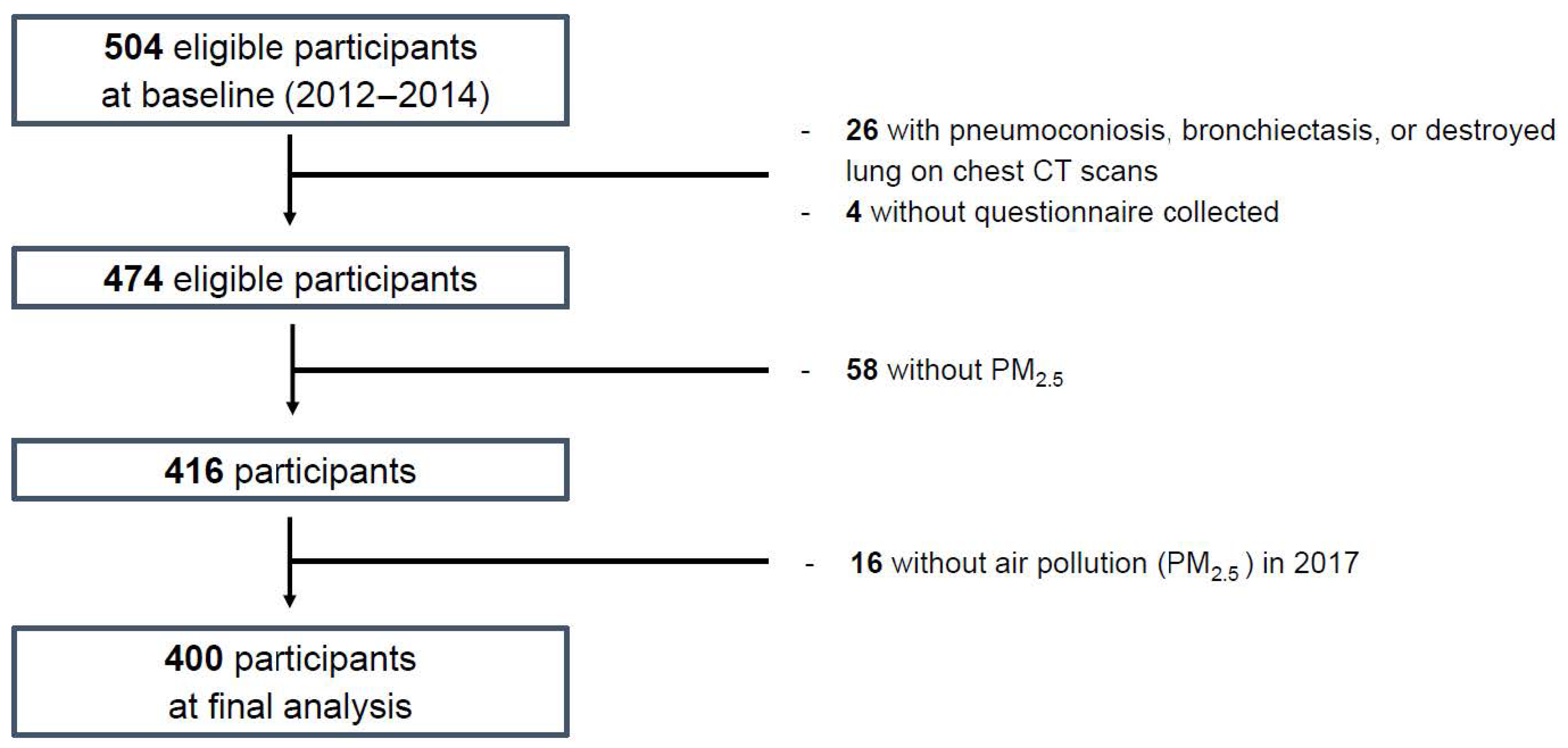
2.1. Study Design and Participants
2.2. Lung Function and Image Measurements
2.3. PM2.5 Concentration Using Satellite Data
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics of Study Groups
3.2. Association of Image Measurements with PM2.5 Concentration
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jia, Y.-Y.; Wang, Q.; Liu, T. Toxicity Research of PM2.5 Compositions In Vitro. Int. J. Environ. Res. Public Health 2017, 14, 232. [Google Scholar] [CrossRef]
- Donaldson, K.; Stone, V.; Borm, P.J.; Jimenez, L.A.; Gilmour, P.S.; Schins, R.P.; Knaapen, A.M.; Rahman, I.; Faux, S.P.; Brown, D.M.; et al. Oxidative stress and calcium signaling in the adverse effects of environmental particles (PM10). Free. Radic. Biol. Med. 2003, 34, 1369–1382. [Google Scholar] [CrossRef]
- Feng, S.; Gao, D.; Liao, F.; Zhou, F.; Wang, X. The health effects of ambient PM2.5 and potential mechanisms. Ecotoxicol. Environ. Saf. 2016, 128, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Lei, Y.C.; Chan, C.C.; Wang, P.Y.; Lee, C.T.; Cheng, T.J. Effects of Asian dust event particles on inflammation markers in peripheral blood and bronchoalveolar lavage in pulmonary hypertensive rats. Environ. Res. 2004, 95, 71–76. [Google Scholar] [CrossRef]
- GBD 2016 Risk Factors Collaborators. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and meta-bolic risks or clusters of risks, 1990-2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1345–1422. [Google Scholar] [CrossRef]
- Chen, L.; Yang, W.; Jennison, B.L.; Omaye, S.T. Air particulate pollution and hospital admissions for chronic obstructive pulmonary disease in Reno, Nevada. Inhal. Toxicol. 2000, 12, 281–298. [Google Scholar]
- Choi, J.; Oh, J.Y.; Lee, Y.S.; Min, K.H.; Hur, G.Y.; Lee, S.Y.; Kang, K.H.; Shim, J.J. Harmful impact of air pollution on severe acute exacerbation of chronic obstructive pulmonary disease: Particulate matter is hazardous. Int. J. Chron. Obstruct. Pulmon. Dis. 2018, 13, 1053–1059. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Zhou, Y.; Liu, S.; Chen, X.; Zou, W.; Zhao, D.; Li, X.; Pu, J.; Huang, L.; Chen, J.; et al. Association between exposure to ambient particulate matter and chronic obstructive pulmonary disease: Results from a cross-sectional study in China. Thorax 2017, 72, 788–795. [Google Scholar] [CrossRef] [PubMed]
- Schikowski, T.; Adam, M.; Marcon, A.; Cai, Y.; Vierkötter, A.; Carsin, A.E.; Jacquemin, B.; Al Kanani, Z.; Beelen, R.; Birk, M.; et al. Association of ambient air pollution with the prevalence and incidence of COPD. Eur. Respir. J. 2014, 44, 614–626. [Google Scholar] [CrossRef]
- Han, Y.; Heo, Y.; Hong, Y.; Kwon, S.O.; Kim, W.J. Correlation between Physical Activity and Lung Function in Dusty Areas: Results from the Chronic Obstructive Pulmo-nary Disease in Dusty Areas (CODA) Cohort. Tuberc. Respir. Dis. 2019, 82, 311–318. [Google Scholar] [CrossRef]
- Kwon, S.O.; Hong, S.H.; Han, Y.-J.; Bak, S.H.; Kim, J.; Lee, M.K.; London, S.J.; Kim, W.J.; Kim, S.-Y. Long-term exposure to PM10 and NO2 in relation to lung function and imaging phenotypes in a COPD cohort. Respir. Res. 2020, 21, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Jin, Y.H.W.; Hong, Y.; Kwon, J.-W.; Lee, S.-A.; Han, Y.J.; Moon, J.Y.; Kim, H.Y.; Han, S.-S.; Lee, S.-J.; Kim, W.J. Methodology of an Observational Cohort Study for Subjects with Chronic Obstructive Pulmonary Disease in Dusty Areas Near Cement Plants. J. Pulm. Respir. Med. 2014, 4, 1–5. [Google Scholar] [CrossRef]
- Bak, S.H.; Kwon, S.O.; Han, S.-S.; Kim, W.J. Computed tomography-derived area and density of pectoralis muscle associated disease severity and longitudinal changes in chronic obstructive pulmonary disease: A case control study. Respir. Res. 2019, 20, 1–12. [Google Scholar] [CrossRef]
- Ogundele, L.T.; Owoade, O.K.; Hopke, P.K.; Olise, F.S. Heavy metals in industrially emitted particulate matter in Ile-Ife, Nigeria. Environ. Res. 2017, 156, 320–325. [Google Scholar] [CrossRef] [PubMed]
- Son, J.-Y.; Lee, J.-T.; Kim, K.-H.; Jung, K.; Bell, M.L. Characterization of Fine Particulate Matter and Associations between Particulate Chemical Constituents and Mortality in Seoul, Korea. Environ. Health Perspect. 2012, 120, 872–878. [Google Scholar] [CrossRef]
- Kim, W.J.L.C. Environmental exposures and chronic obstructive pulmonary disease. Mol. Cell Toxicol. 2017, 13, 251–255. [Google Scholar] [CrossRef]
- Liu, C.; Chen, R.; Sera, F.; Vicedo-Cabrera, A.M.; Guo, Y.; Tong, S.; Coelho, M.S.Z.S.; Saldiva, P.H.N.; Lavigne, E.; Matus, P.; et al. Ambient Particulate Air Pollution and Daily Mortality in 652 Cities. N. Engl. J. Med. 2019, 381, 705–715. [Google Scholar] [CrossRef] [PubMed]
- Bloemsma, L.D.; Hoek, G.; Smit, L.A. Panel studies of air pollution in patients with COPD: Systematic review and meta-analysis. Environ. Res. 2016, 151, 458–468. [Google Scholar] [CrossRef] [PubMed]
- Gauderman, W.J.; Avol, E.; Gilliland, F.; Vora, H.; Thomas, D.; Berhane, K.; McConnell, R.; Kuenzli, N.; Lurmann, F.; Rappaport, E.; et al. The Effect of Air Pollution on Lung Development from 10 to 18 Years of Age. New Engl. J. Med. 2004, 351, 1057–1067. [Google Scholar] [CrossRef] [PubMed]
- Downs, S.H.; Schindler, C.; Liu, L.-J.S.; Keidel, D.; Bayer-Oglesby, L.; Brutsche, M.H.; Gerbase, M.W.; Keller, R.; Künzli, N.; Leuenberger, P.; et al. Reduced Exposure to PM10and Attenuated Age-Related Decline in Lung Function. New Engl. J. Med. 2007, 357, 2338–2347. [Google Scholar] [CrossRef] [PubMed]
- Guo, C.; Zhang, Z.; Lau, A.K.H.; Lin, C.Q.; Chuang, Y.C.; Chan, J.; Jiang, W.K.; Tam, T.; Yeoh, E.-K.; Chan, T.-C.; et al. Effect of long-term exposure to fine particulate matter on lung function decline and risk of chronic obstructive pulmonary disease in Taiwan: A longitudinal, cohort study. Lancet Planet Health 2018, 2, e114–e125. [Google Scholar] [CrossRef]
- Adar, S.D.; Kaufman, J.D.; Diez-Roux, A.V.; Hoffman, E.A.; D’Souza, J.; Stukovsky, K.H.; Rich, S.S.; Rotter, J.I.; Guo, X.; Raffel, L.J.; et al. Air Pollution and Percent Emphysema Identified by Computed Tomography in the Multi-Ethnic Study of Atherosclerosis. Environ. Health Perspect. 2015, 123, 144–151. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | Total (N = 400) |
|---|---|
| Sex, male (%) | 301 (75.3) |
| Age (years) | 71.7 ± 7.4 |
| Patients in each age group (%) | |
| 44–59 years old | 27 (6.7) |
| 60–69 years old | 96 (24.0) |
| 70–79 years old | 232 (58.0) |
| 80–96 years old | 45 (11.3) |
| Height (cm) | 159.7 ± 9.2 |
| Weight (kg) | 60.0 ± 10.5 |
| BMI (kg/m2) | 23.5 ± 3.3 |
| <23.0 | 184 (46.0) |
| 23.0–24.9 | 92 (23.0) |
| ≥25.0 | 124 (31.0) |
| Smoking status | |
| Never smoker | 136 (34.0) |
| Ex-smoker | 174 (43.5) |
| Current smoker | 90 (22.5) |
| Smoking amount (pack-years) | 18.4 ± 23.9 |
| Education | |
| <Elementary school | 125 (31.5) |
| Elementary school | 149 (37.5) |
| Middle school | 59 (14.9) |
| ≥High school | 64 (16.1) |
| Income per month (×104 won) | |
| ≤49 | 250 (64.4) |
| 50–99 | 61 (15.7) |
| ≥100 | 77 (19.9) |
| Pulmonary function test, post-bronchodilator response | |
| FVC, L | 3.03 ± 0.82 |
| FVC, % predicted | 97.1 ± 19.0 |
| FEV1, L | 1.96 ± 0.61 |
| FEV1, %predicted | 86.2 ± 22.3 |
| FEV1/FVC | 0.65 ± 0.11 |
| Asthma history (yes, %) | 70 (17.6) |
| Emphysema index | 6.63 ± 0.70 |
| Mean wall area | 68.8 ± 5.2 |
| CAT | 16.0 ± 9.6 |
| mMRC dyspnea scale score | 1.37 ± 1.13 |
| 0 | 93 (23.3) |
| 1 | 164 (41.0) |
| 2 | 61 (15.3) |
| 3 | 66 (16.5) |
| 4 | 16 (4.0) |
| Physical activity (yes, %) | 299 (74.7) |
| Previous exacerbation history (≥1, %) | 12 (3.0) |
| Charlson comorbidity index | |
| 0 | 225 (56.7) |
| 1 | 91 (22.9) |
| ≥2 | 81 (20.4) |
| Total (N = 400) | Emphysema Index | Mean Wall Area (%) | ||
|---|---|---|---|---|
| β (95% CI) | p Value | β (95% CI) | p Value | |
| 1-year +, 1 km | −0.393 (−2.817, 2.032) | 0.750 | 0.042 (−2.035, 2.118) | 0.969 |
| 1-year +, 3 km | 0.748 (−2.244, 3.739) | 0.623 | 0.468 (−2.094, 3.030) | 0.720 |
| 1-year +, 5 km | −1.366 (−4.140, 1.407) | 0.333 | 0.489 (−1.888, 2.867) | 0.686 |
| 3-year ++, 1 km | −0.978 (−3.225, 1.269) | 0.393 | −0.816 (−2.754, 1.122) | 0.408 |
| 3-year ++, 3 km | −0.197 (−2.955, 2.562) | 0.889 | −0.550 (−2.928, 1.828) | 0.650 |
| 3-year ++, 5 km | −1.980 (−4.499, 0.539) | 0.123 | −0.635 (−2.814, 1.544) | 0.567 |
| 5-year #, 1 km | −0.921 (−2.983, 1.141) | 0.381 | −0.802 (−2.588, 0.983) | 0.377 |
| 5-year #, 3 km | −0.337 (−2.844, 2.169) | 0.791 | −0.644 (−2.814, 1.525) | 0.560 |
| 5-year #, 5 km | −1.801 (−4.080, 0.478) | 0.121 | −0.690 (−2.669, 1.288) | 0.493 |
| Total (N = 400) | EIr ¥ | Mean Wall Area (%) | ||
|---|---|---|---|---|
| β (95% CI) | p Value | β (95% CI) | p Value | |
| Normal (N = 132) | ||||
| 1-year +, 1 km | 0.585 (0.024, 1.146) | 0.041 | −4.646 (−9.339, 0.048) | 0.052 |
| 1-year +, 3 km | 1.181 (0.404, 1.958) | 0.003 | −3.943 (−10.733, 2.847) | 0.251 |
| 1-year +, 5 km | 0.758 (0.118, 1.398) | 0.021 | −0.589 (−6.114, 4.935) | 0.832 |
| 3-year ++, 1 km | 0.498 (−0.020, 1.015) | 0.059 | −6.572 (−10.980, −2.164) | 0.004 |
| 3-year ++, 3 km | 1.051 (0.305, 1.797) | 0.006 | −7.088 (−13.763, −0.413) | 0.038 |
| 3-year ++, 5 km | 0.629 (0.035, 1.222) | 0.038 | −3.677 (−8.963, 1.609) | 0.170 |
| 5-year #, 1 km | 0.433 (−0.031, 0.897) | 0.067 | −5.689 (−9.754, −1.624) | 0.007 |
| 5-year #, 3 km | 0.880 (0.218, 1.541) | 0.010 | −6.622 (−12.643, −0.600) | 0.032 |
| 5-year #, 5 km | 0.544 (0.012, 1.077) | 0.045 | −3.769 (−8.597, 1.059) | 0.124 |
| COPD (N = 268) | ||||
| 1-year +, 1 km | −0.074 (−0.286, 0.139) | 0.494 | 0.987 (−1.352, 3.327) | 0.407 |
| 1-year +, 3 km | −0.097 (−0.348, 0.154) | 0.448 | 1.112 (−1.656, 3.881) | 0.429 |
| 1-year +, 5 km | −0.245 (−0.482, −0.009) | 0.042 | 0.977 (−1.649, 3.603) | 0.464 |
| 3-year ++, 1 km | −0.147 (−0.344, 0.050) | 0.142 | 0.359 (−1.806, 2.525) | 0.744 |
| 3-year ++, 3 km | −0.183 (−0.413, 0.047) | 0.118 | 0.421 (−2.108, 2.950) | 0.743 |
| 3-year ++, 5 km | −0.304 (−0.518, −0.090) | 0.006 | 0.273 (−2.109, 2.654) | 0.822 |
| 5-year #, 1 km | −0.136 (−0.318, 0.046) | 0.143 | 0.259 (−1.738, 2.255) | 0.799 |
| 5-year #, 3 km | −0.167 (−0.378, 0.044) | 0.120 | 0.296 (−2.019, 2.612) | 0.801 |
| 5-year #, 5 km | −0.263 (−0.458, −0.067) | 0.009 | 0.180 (−1.984, 2.344) | 0.870 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, Y.; Bak, S.H.; Kwon, S.O.; Kim, H.; Kim, W.J.; Lee, C.Y. Association between Long-Term Exposure to PM2.5 and Lung Imaging Phenotype in CODA Cohort. Atmosphere 2021, 12, 282. https://doi.org/10.3390/atmos12020282
Kim Y, Bak SH, Kwon SO, Kim H, Kim WJ, Lee CY. Association between Long-Term Exposure to PM2.5 and Lung Imaging Phenotype in CODA Cohort. Atmosphere. 2021; 12(2):282. https://doi.org/10.3390/atmos12020282
Chicago/Turabian StyleKim, Youlim, So Hyeon Bak, Sung Ok Kwon, Ho Kim, Woo Jin Kim, and Chang Youl Lee. 2021. "Association between Long-Term Exposure to PM2.5 and Lung Imaging Phenotype in CODA Cohort" Atmosphere 12, no. 2: 282. https://doi.org/10.3390/atmos12020282
APA StyleKim, Y., Bak, S. H., Kwon, S. O., Kim, H., Kim, W. J., & Lee, C. Y. (2021). Association between Long-Term Exposure to PM2.5 and Lung Imaging Phenotype in CODA Cohort. Atmosphere, 12(2), 282. https://doi.org/10.3390/atmos12020282