
Temperature Changes during Implant Osteotomy Preparations in Human Cadaver Tibiae Comparing MIS® Straight Drills with Densah® Burs

 ,
,  , ,
, ,
Abstract
1. Introduction
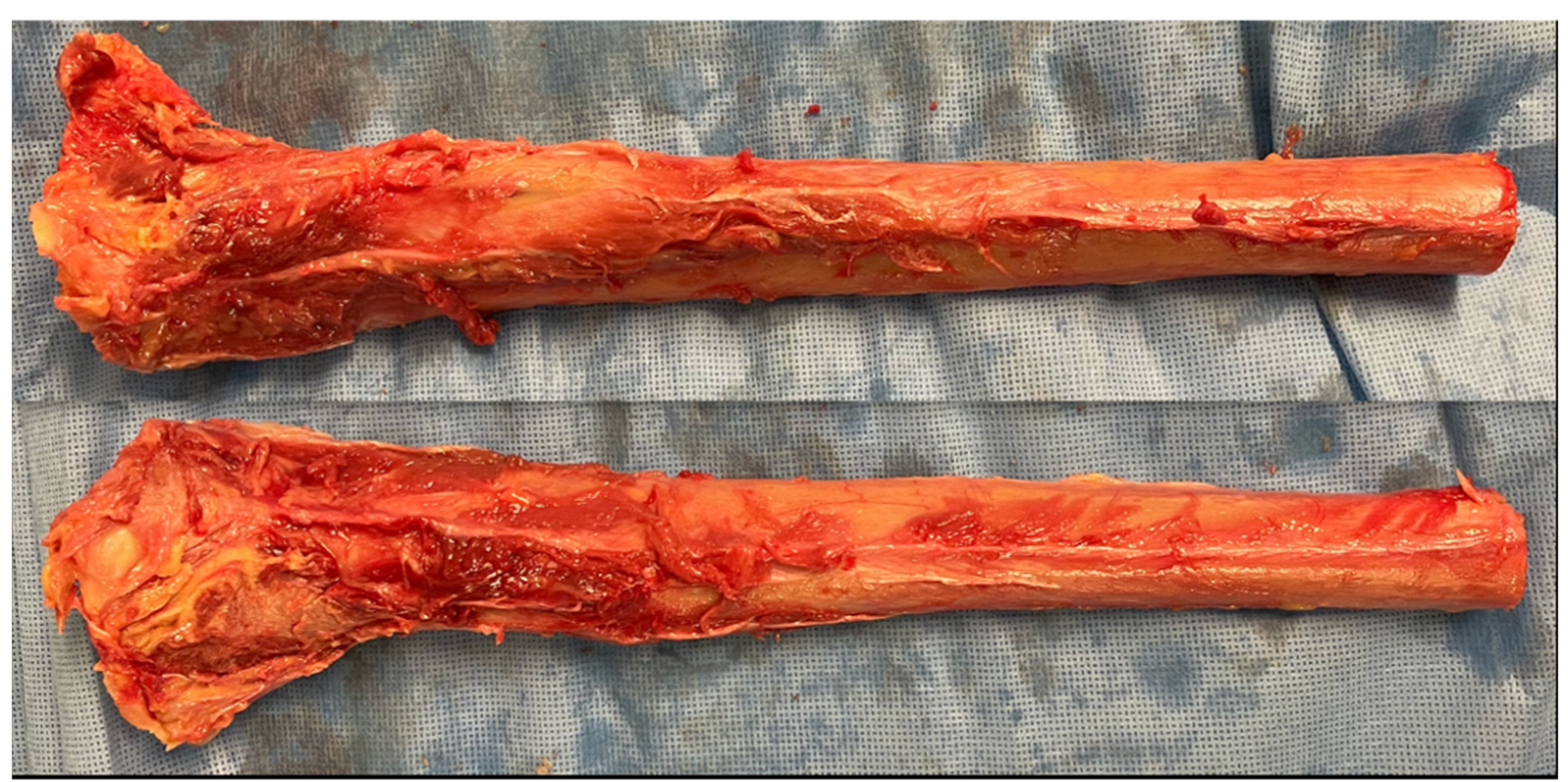
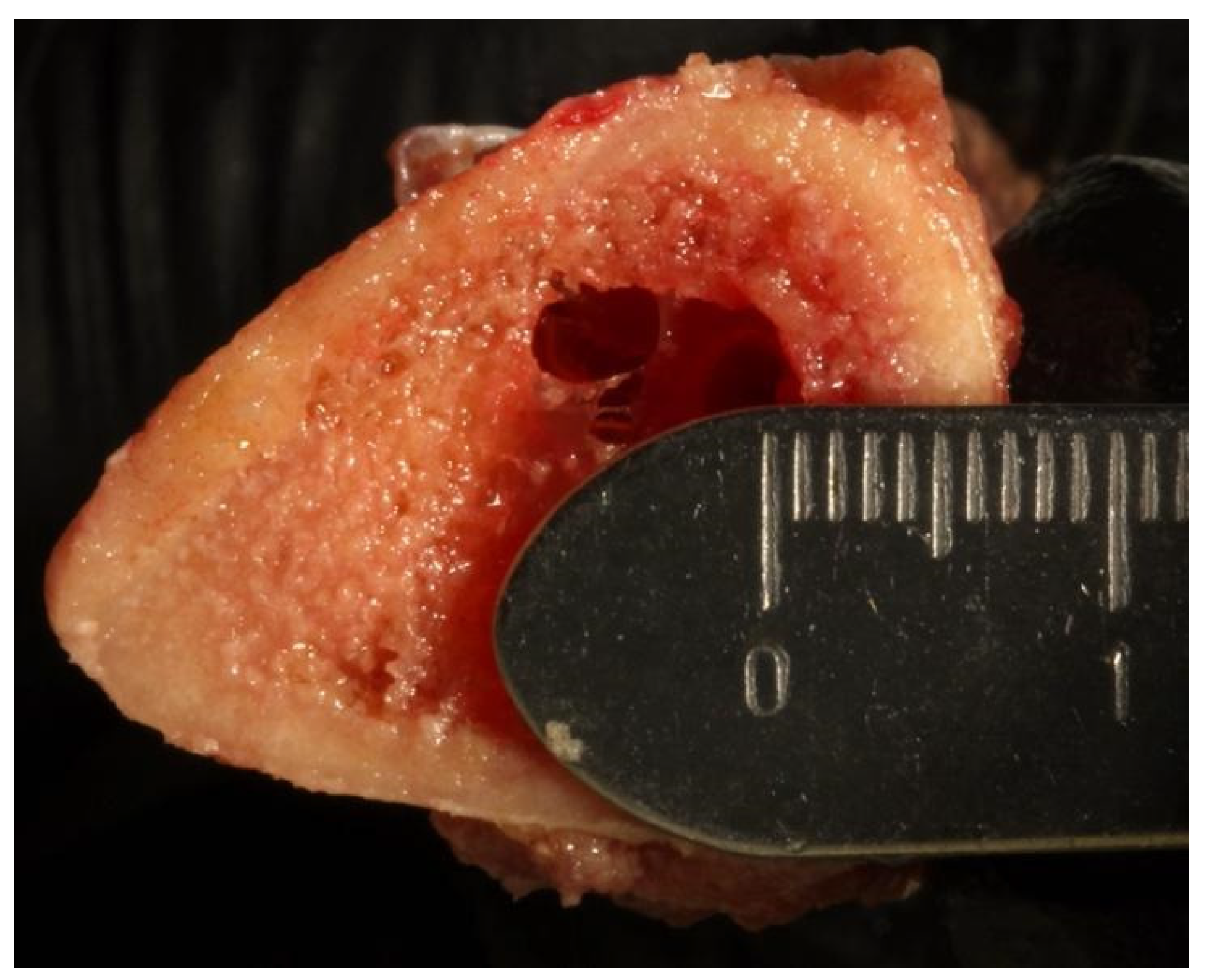
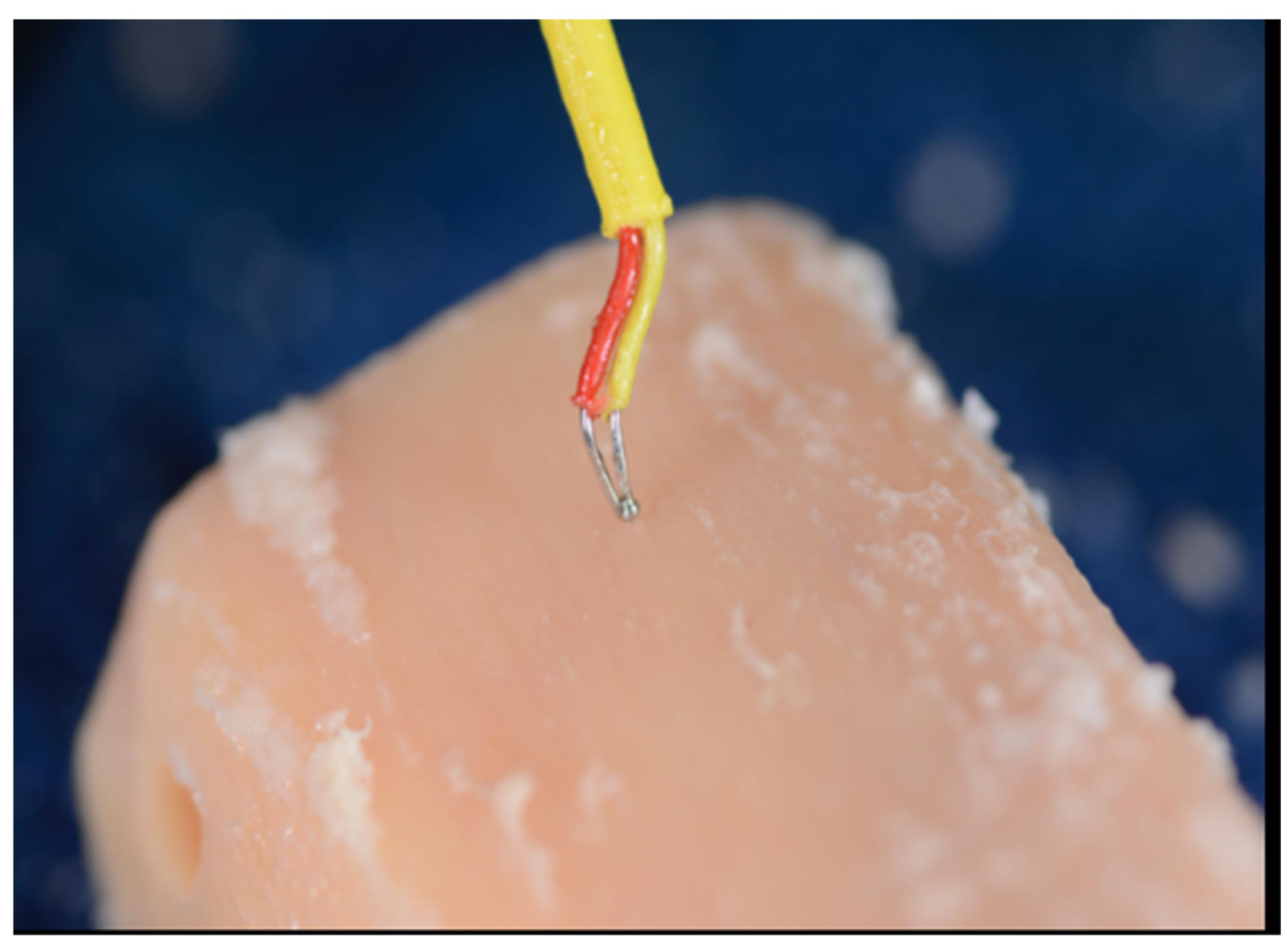
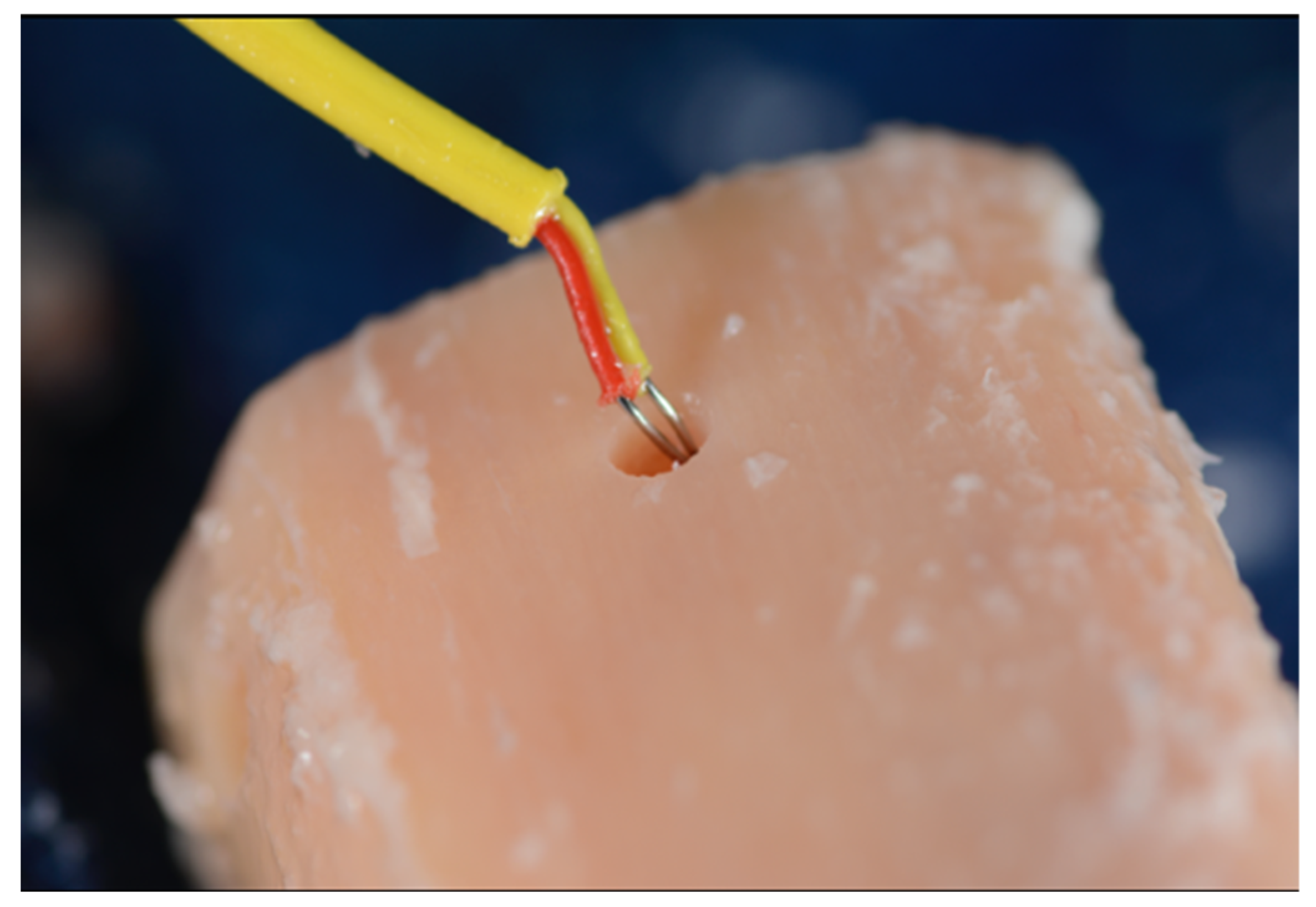
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lioubavina-Hack, N.; Lang, N.P.; Karring, T. Significance of primary stability for osseointegration of dental implants. Clin. Oral Implant. Res. 2006, 17, 244–250. [Google Scholar] [CrossRef] [PubMed]
- Cardemil, C.; Ristevski, Z.; Alsén, B.; Dahlin, C. Influence of Different Operatory Setups on Implant Survival Rate: A Retrospective Clinical Study. Clin. Implant Dent. Relat. Res. 2009, 11, 288–291. [Google Scholar] [CrossRef] [PubMed]
- Pandey, R.K.; Panda, S. Drilling of bone: A comprehensive review. J. Clin. Orthop. Trauma 2013, 4, 15–30. [Google Scholar] [CrossRef]
- Eriksson, A.R.; Albrektsson, T.; Grane, B.; McQueen, D. Thermal injury to bone: A vital microscopic description of heat effects. Int. J. Oral Surg. 1982, 11, 115–121. [Google Scholar] [CrossRef]
- Eriksson, R.A.; Albrektsson, T. The effect of heat on bone regeneration: An experimental study in the rabbit using the bone growth chamber. J. Oral Maxillofac. Surg. 1984, 42, 705–711. [Google Scholar] [CrossRef]
- Eriksson, A.R.; Albrektsson, T. Assessment of bone viability after heat trauma. Scand. J. Plast. Reconstr. Surg. 1984, 18, 261–268. [Google Scholar]
- Watanabe, F.; Tawada, Y.; Komatsu, S.; Hata, Y. Heat distribution in bone during preparation of implant sites: Heat analysis by real-time thermography. Int. J. Oral Maxillofac. Implant. 1992, 7, 212–219. [Google Scholar]
- Trisi, P.; Berardini, M.; Falco, A.; Vulpiani, M.P.; Masciotra, L. Effect of 50 to 60 °C Heating on Osseointegration of Dental Implants in Dense Bone. An in vivo histological study. Implant Dent. 2014, 23, 516–521. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Chacon, G.E.; Bower, D.L.; Larsen, P.E.; McGlumphy, E.A.; Beck, F.M. Heat Production by 3 Implant Drill Systems after Repeated Drilling and Sterilization. J. Oral Maxillofac. Surg. 2006, 64, 265–269. [Google Scholar] [CrossRef]
- Gehrke, S.A.; Neto, H.L.; Mardegan, F.E. Investigation of the effect of movement and irrigation systems on temperature in the conventional drilling of cortical bone. Br. J. Oral Maxillofac. Surg. 2013, 51, 953–957. [Google Scholar] [CrossRef]
- Gehrke, S.A.; Pazetto, M.K.; de Oliveira, S.; Corbella, S.; Taschieri, S.; Mardegan, F.E.C. Study of temperature variation in cortical bone during osteotomies with trephine drills. Clin. Oral Investig. 2014, 18, 1749–1755. [Google Scholar] [CrossRef] [PubMed]
- Ercoli, C.; Funkenbusch, P.D.; Lee, H.J.; Moss, M.E.; Graser, G.N. The influence of drill wear on cutting efficiency and heat production during osteotomy preparation for dental implants: A study of drill durability. Int. J. Oral Maxillofac. Implant. 2004, 19, 335–349. [Google Scholar]
- Tuijthof, G.; Frühwirt, C.; Kment, C. Influence of tool geometry on drilling performance of cortical and trabecular bone. Med. Eng. Phys. 2013, 35, 1165–1172. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, A.R.; Albrektsson, T.; Albrektsson, B. Heat caused by drilling cortical bone. Temperature measured in vivo in patients and animals. Acta Orthop. Scand. 1984, 55, 629–631. [Google Scholar] [CrossRef]
- Yacker, M.J.; Klein, M. The effect of irrigation on osteotomy depth and bur diameter. Int. J. Oral Maxillofac. Implant. 1996, 11, 634–638. [Google Scholar]
- Stelzle, F.; Frenkel, C.; Riemann, M.; Knipfer, C.; Stockmann, P.; Nkenke, E. The effect of load on heat production, thermal effects, and expenditure of time during implant site preparation—An experimental ex vivo comparison between piezosurgery and conventional drilling. Clin. Oral Implant. Res. 2014, 25, 140–148. [Google Scholar] [CrossRef]
- Albrektsson, T.; Albrektsson, B. Microcirculation in grafted bone. A chamber technique for vital microscopy of rabbit bone transplants. Acta Orthop. Scand. 1978, 49, 1–7. [Google Scholar] [CrossRef]
- Jochum, R.M.; Reichart, P.A. Influence of multiple use of Timedur-titanium cannon drills: Thermal response and scanning electron microscopic findings. Clin. Oral Implant. Res. 2000, 11, 139–144. [Google Scholar] [CrossRef]
- Strbac, G.D.; Unger, E.; Donner, R.; Bijak, M.; Watzek, G.; Zechner, W. Thermal effects of a combined irrigation method during implant site drilling. A standardized in vitro study using a bovine rib model. Clin. Oral Implant. Res. 2012, 25, 665–674. [Google Scholar] [CrossRef]
- Calvo-Guirado, J.L.; Delgado-Peña, J.; Maté-Sánchez, J.E.; Mareque Bueno, J.; Delgado-Ruiz, R.A.; Romanos, G.E. Novel hybrid drilling protocol. Evaluation for the implant healing. Thermal changes, crestal bone loss, and bone-to-implant contact. Clin. Oral Implant. Res. 2015, 26, 753–760. [Google Scholar] [CrossRef]
- Eriksson, A.R.; Adell, R. Temperatures during drilling for the placement of implants using the osseointegration technique. J. Oral Maxillofac. Surg. 1986, 44, 4–7. [Google Scholar] [CrossRef]
- Matthews, L.S.; Hirsch, C. Temperatures Measured in Human Cortical Bone When Drilling. J. Bone Jt. Surg. 1972, 54, 297–308. [Google Scholar] [CrossRef]
- Moss, R.W. Histopathologic reaction of bone to surgical cutting. Oral Surg. Oral Med. Oral Pathol. 1964, 17, 405–414. [Google Scholar] [CrossRef]
- Soldatos, N.; Nelson-Rabe, L.; Palanker, N.; Angelov, N.; Romanos, G.; Weltman, R. Temperature Changes during Implant Osteotomy Preparations in Fresh Human Cadaver Tibiae, Comparing Straight with Tapered Drills. Materials 2022, 15, 2369. [Google Scholar] [CrossRef]
- Huwais, S.; Meyer, E.G. A Novel Osseous Densification Approach in Implant Osteotomy Preparation to Increase Biomechanical Primary Stability, Bone Mineral Density, and Bone-to-Implant Contact. Int. J. Oral Maxillofac. Implant. 2017, 32, 27–36. [Google Scholar] [CrossRef]
- Misch, C.; Qu, Z.; Bidez, W. Mechanical properties of trabecular bone in the human mandible: Implications for dental implant treatment planning and surgical placement. J. Oral Maxillofac. Surg. 1999, 57, 700–706. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2021; Available online: https://www.R-project.org/ (accessed on 29 June 2021).
- dos Santos, P.L.; Queiroz, T.P.; Margonar, R.; de Souza Carvalho, A.C.G.; Betoni, W., Jr. Evaluation of bone heating, drill deformation, and drill roughness after implant osteotomy: Guided surgery and classic drilling procedure. Int. J. Oral Maxillofac. Implant. 2014, 29, 51–58. [Google Scholar] [CrossRef]
- Borges, M.A.D.C.; Margonar, R.; Spinelli, M.A.; Cavalcanti, I.M.G.; De Oliveira, G.J.P.L.; Queiroz, T.P. Semiautomatic device for in vitro/experimental bone perforation in dental implant research. J. Cranio-Maxillofac. Surg. 2019, 47, 991–995. [Google Scholar] [CrossRef]
- Trisi, P.; Berardini, M.; Falco, A.; Vulpiani, M.P. Effect of temperature on the dental implant osseointegration development in low-density bone: An in vivo histological evaluation. Implant Dent. 2015, 24, 96–100. [Google Scholar] [CrossRef]
- Mendes, G.C.B.; Padovan, L.E.M.; Ribeiro-Júnior, P.D.; Sartori, E.M.; Valgas, L.; Claudino, M. Influence of implant drill materials on wear, deformation, and roughness after repeated drilling and sterilization. Implant Dent. 2014, 23, 188–194. [Google Scholar] [CrossRef]
- Barrak, I.; Joób-Fancsaly, Á.; Braunitzer, G.; Varga, E., Jr.; Boa, K.; Piffkó, J. Intraosseous heat generation during osteotomy performed freehand and through template with an integrated metal guide sleeve: An in vitro study. Implant Dent. 2018, 27, 342–350. [Google Scholar] [CrossRef] [PubMed]
- Kirstein, K.; Dobrzyński, M.; Kosior, P.; Chrószcz, A.; Dudek, K.; Fita, K.; Parulska, O.; Rybak, Z.; Skalec, A.; Szklarz, M.; et al. Infrared Thermographic Assessment of Cooling Effectiveness in Selected Dental Implant Systems. BioMed Res. Int. 2016, 2016, 1879468. [Google Scholar] [CrossRef]
- Koo, K.-T.; Kim, M.-H.; Kim, H.-Y.; Wikesjö, U.M.E.; Yang, J.-H.; Yeo, I.-S. Effects of Implant Drill Wear, Irrigation, and Drill Materials on Heat Generation in Osteotomy Sites. J. Oral Implant. 2015, 41, e19–e23. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.-F.; Wu, J.-L.; Zhang, J.-X.; Peng, W.; Liao, W.-Q. Numerical and Experimental Analyses on the Temperature Distribution in the Dental Implant Preparation Area When Using a Surgical Guide. J. Prosthodont. 2016, 27, 42–51. [Google Scholar] [CrossRef]
- Strbac, G.D.; Giannis, K.; Unger, E.; Mittlbock, M.; Watzek, G.; Zechner, W. A novel standardized bone model forthermal evaluation of bone osteotomies with various irrigation methods. Clin. Oral Implant. Res. 2014, 25, 622–631. [Google Scholar] [CrossRef]
- Soldatos, N.; Gozalo, D.; Font, K.; Moreno, D.; Powell, C. Temperature changes during implant osteotomies utilizing three different implant systems: A pilot study. J. Implant Adv. Clin. Dent. 2016, 8, 34–43. [Google Scholar]
- Cordioli, G.; Majzoub, Z. Heat generation during implant site preparation: An in vitro study. Int. J. Oral Maxillofac. Implant. 1997, 12, 186–193. [Google Scholar]
- Oliveira, N.; Alaejos-Algarra, F.; Mareque-Bueno, J.; Ferrés-Padró, E.; Hernández-Alfaro, F. Thermal changes, and drill wear in bovine bone during implant site preparation. A comparative in vitro study: Twisted stainless steel and ceramic drills. Clin. Oral Implant. Res. 2013, 23, 963–969. [Google Scholar] [CrossRef]
- Lundskog, J. Heat and bone tissue. An experimental investigation of the thermal properties of bone and threshold levels for thermal injury. Scand. J. Plast. Reconstr. Surg. 1972, 9, 1–80. [Google Scholar] [PubMed]
- Iyer, S.; Weiss, C.; Mehta, A. Effect of drill speed on heat production and the rate and quality of bone formation in dental osteotomies. Part II: Relationship between drill speed and healing. Int. J. Prosthodont. 1997, 10, 536. [Google Scholar] [PubMed]
- Flanagan, D. Osteotomy irrigation: Is it necessary? Implant Dent. 2010, 19, 241–249. [Google Scholar] [CrossRef] [PubMed]
- Oh, J.-H.; Fang, Y.; Jeong, S.-M.; Choi, B.-H. The effect of low-speed drilling without irrigation on heat generation: An experimental study. J. Korean Assoc. Oral Maxillofac. Surg. 2016, 42, 9–12. [Google Scholar] [CrossRef] [PubMed]
- Scarano, A.; Piattelli, A.; Assenza, B.; Carinci, F.; Di Donato, L.; Romani, G.L.; Merla, A. Infrared Thermographic Evaluation of Temperature Modifications Induced during Implant Site Preparation with Cylindrical versus Conical Drills. Clin. Implant Dent. Relat. Res. 2009, 13, 319–323. [Google Scholar] [CrossRef]
- Misic, T.; Markovic, A.; Todorovic, A.; Colic, S.; Miodrag, S.; Milicic, B. An in vitro study of temperature changes in type 4 bone during implant placement: Bone condensing versus bone drilling. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2011, 112, 28–33. [Google Scholar] [CrossRef] [PubMed]
- Rashad, A.; Kaiser, A.; Prochnow, N.; Schmitz, I.; Hoffmann, E.; Maurer, P. Heat production during different ultrasonic and conventional osteotomy preparations for dental implants. Clin. Oral Implant. Res. 2011, 22, 1361–1365. [Google Scholar] [CrossRef] [PubMed]
- Bulloch, S.E.; Olsen, R.G.; Bulloch, B. Comparison of heat generation between internally guided (cannulated) single drill and traditional sequential drilling with and without a drill guide for dental implants. Int. J. Oral Maxillofac. Implant. 2012, 27, 1456–1460. [Google Scholar]
- Eichler, J.; Berg, R. Influence of temperature on the compact bone substance during drilling, thread cutting and insertion of bone screws. Z. Orthop. Ihre Grenzgeb. 1972, 110, 909–913. [Google Scholar]
- Trisi, P.; Berardi, D.; Paolantonio, M.; Spoto, G.; D’Addona, A.; Perfetti, G. Primary stability, insertion torque, and bone density of conical implants with internal hexagon, is there a relationship? J. Craniofac. Surg. 2013, 24, 841–844. [Google Scholar] [CrossRef]
- Renders, G.A.P.; Mulder, L.; Van Ruijven, L.J.; Van Eijden, T.M.G.J. Porosity of human mandibular condylar bone. J. Anat. 2007, 210, 239–248. [Google Scholar] [CrossRef]
- Allsobrook, O.F.L.; Leichter, J.; Holborow, D.; Swain, M. Descriptive Study of the Longevity of Dental Implant Surgery Drills. Clin. Implant Dent. Relat. Res. 2011, 13, 244–254. [Google Scholar] [CrossRef]
- Sumer, M.; Misir, A.F.; Telcioglu, N.T.; Guler, A.U.; Yenisey, M. Comparison of Heat Generation During Implant Drilling Using Stainless Steel and Ceramic Drills. J. Oral Maxillofac. Surg. 2011, 69, 1350–1354. [Google Scholar] [CrossRef] [PubMed]
- Sharawy, M.; Misch, C.E.; Weller, N.; Tehemar, S. Heat generation during implant drilling: The significance of motor speed. J. Oral Maxillofac. Surg. 2002, 60, 1160–1169. [Google Scholar] [CrossRef] [PubMed]
- Salomó-Coll, O.; Auriol-Muerza, B.; Lozano-Carrascal, N.; Hernández-Alfaro, F.; Wang, H.-L.; Gargallo-Albiol, J. Influence of bone density, drill diameter, drilling speed, and irrigation on temperature changes during implant osteotomies: An in vitro study. Clin. Oral Investig. 2021, 25, 1047–1053. [Google Scholar] [CrossRef] [PubMed]
- Pellicer-Chover, H.; Peñarrocha-Oltra, D.; Aloy-Prosper, A.; Sanchis-Gonzalez, J.C.; Peñarrocha-Diago, M.; Peñarrocha-Diago, M. Comparison of peri-implant bone loss between conventional drilling with irrigation versus low-speed drilling without irrigaqtion. Med. Oral Patol. Oral Cir. Bucal 2017, 22, e730–e736. [Google Scholar]
- Mihali, S.G.; Canjau, S.; Cernescu, A.V.; Bortun, C.M.; Wang, H.-L.; Bratu, E. Effects of a Short Drilling Implant Protocol on Osteotomy Site Temperature and Drill Torque. Implant Dent. 2018, 27, 63–68. [Google Scholar] [CrossRef]
- Bratu, E.; Mihali, S.; Shapira, L.; Bratu, D.C.; Wang, H.-L. Crestal Bone Remodeling around Implants Placed Using a Short Drilling Protocol. Int. J. Oral Maxillofac. Implant. 2015, 30, 435–440. [Google Scholar] [CrossRef]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Source | SS | df | F | p Value |
|---|---|---|---|---|
| Design | 681.5 | 1 | 160.67 | <2.2 × 10−16 * |
| RPM | 496.6 | 2 | 58.54 | <2.2 × 10−16 * |
| Width | 1312.8 | 1 | 309.51 | <2.2 × 10−16 * |
| Design/RPM | 228.4 | 2 | 26.93 | <3.9 × 10−12 * |
| Design/width | 79.2 | 1 | 18.68 | <1.7 × 10−5 * |
| RPM/width | 35.6 | 2 | 4.19 | <0.015 * |
| Design/RPM/width | 88.7 | 2 | 10.46 | <3.17 × 10−5 * |
| Source | F | df | DF.res | p Value |
|---|---|---|---|---|
| Drillfreq | 1.82 | 1 | 227.78 | <0.18 |
| Design/drillfreq | 0.11 | 1 | 230.63 | <0.73 |
| RPM/drillfreq | 2.03 | 2 | 227.78 | <0.13 |
| Width/drillfreq | 0.58 | 1 | 828.22 | <0.45 |
| Design/RPM/drillfreq | 1.25 | 2 | 230.63 | <0.29 |
| Design/width/drillfreq | 0.02 | 1 | 828.22 | <0.88 |
| RPM/width/drillfreq | 2.29 | 2 | 828.22 | <0.10 |
| Design/RPM/width/drillfreq | 0.10 | 2 | 828.22 | <0.90 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Soldatos, N.; Pham, H.; Fakhouri, W.D.; Ngo, B.; Lampropoulos, P.; Tran, T.; Weltman, R. Temperature Changes during Implant Osteotomy Preparations in Human Cadaver Tibiae Comparing MIS® Straight Drills with Densah® Burs. Genes 2022, 13, 1716. https://doi.org/10.3390/genes13101716
Soldatos N, Pham H, Fakhouri WD, Ngo B, Lampropoulos P, Tran T, Weltman R. Temperature Changes during Implant Osteotomy Preparations in Human Cadaver Tibiae Comparing MIS® Straight Drills with Densah® Burs. Genes. 2022; 13(10):1716. https://doi.org/10.3390/genes13101716
Chicago/Turabian StyleSoldatos, Nikolaos, Huy Pham, Walid D. Fakhouri, Binh Ngo, Panagiotis Lampropoulos, Tiffany Tran, and Robin Weltman. 2022. "Temperature Changes during Implant Osteotomy Preparations in Human Cadaver Tibiae Comparing MIS® Straight Drills with Densah® Burs" Genes 13, no. 10: 1716. https://doi.org/10.3390/genes13101716
APA StyleSoldatos, N., Pham, H., Fakhouri, W. D., Ngo, B., Lampropoulos, P., Tran, T., & Weltman, R. (2022). Temperature Changes during Implant Osteotomy Preparations in Human Cadaver Tibiae Comparing MIS® Straight Drills with Densah® Burs. Genes, 13(10), 1716. https://doi.org/10.3390/genes13101716