
Supercritical Carbon Dioxide Decellularized Xenograft-3D CAD/CAM Carved Bone Matrix Personalized for Human Bone Defect Repair

 ,
,
Abstract
:
1. Introduction
2. Materials and Methods
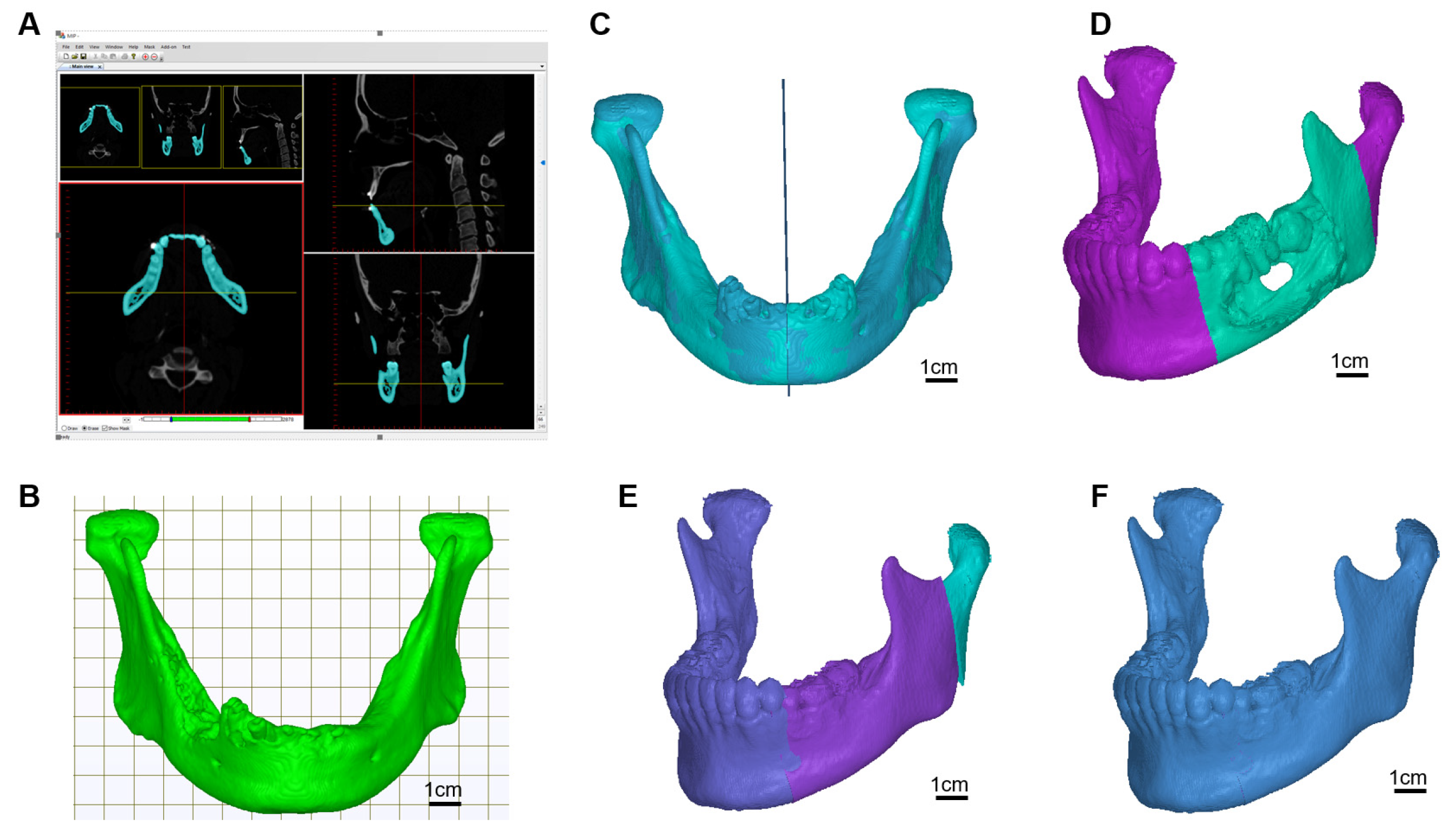
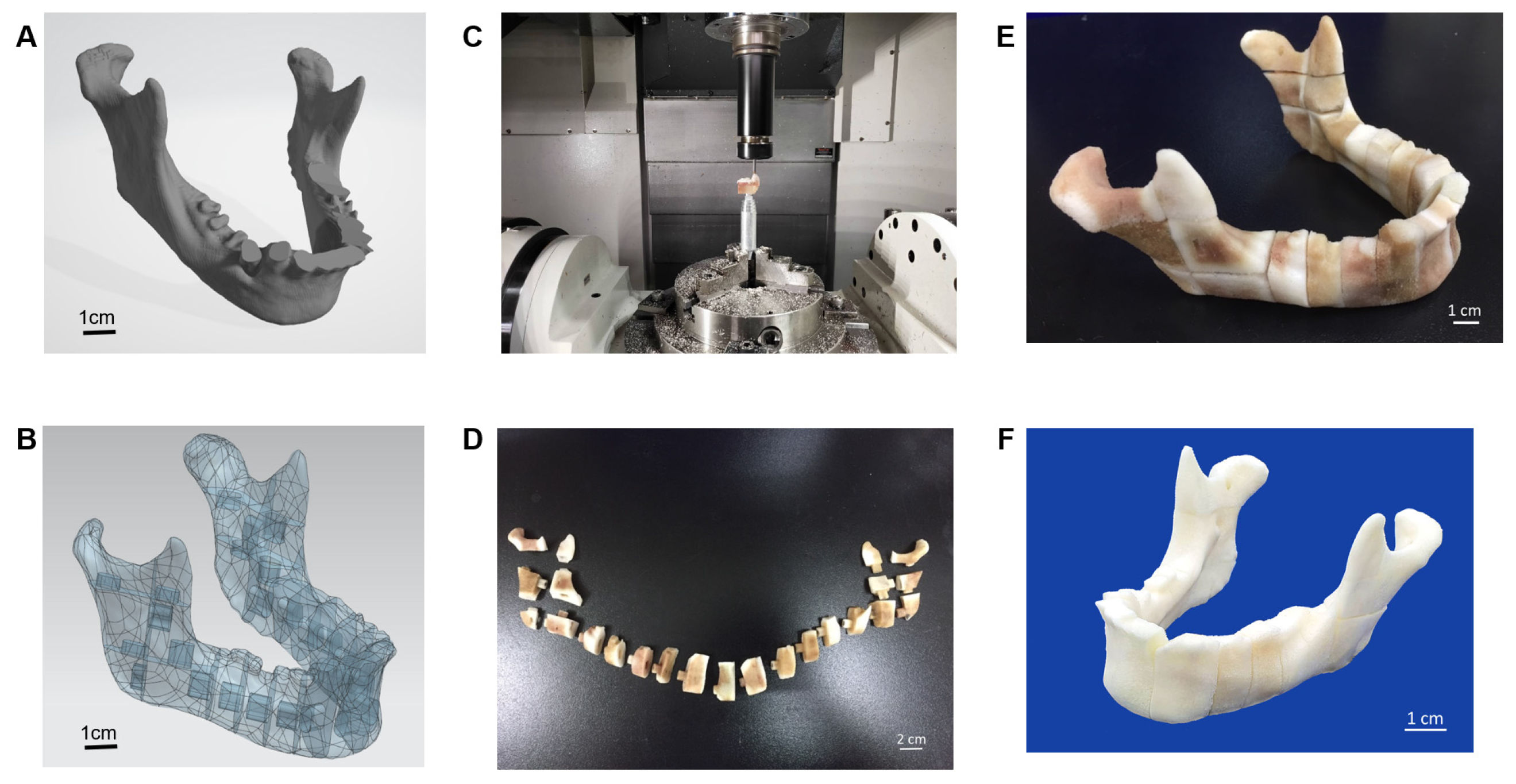
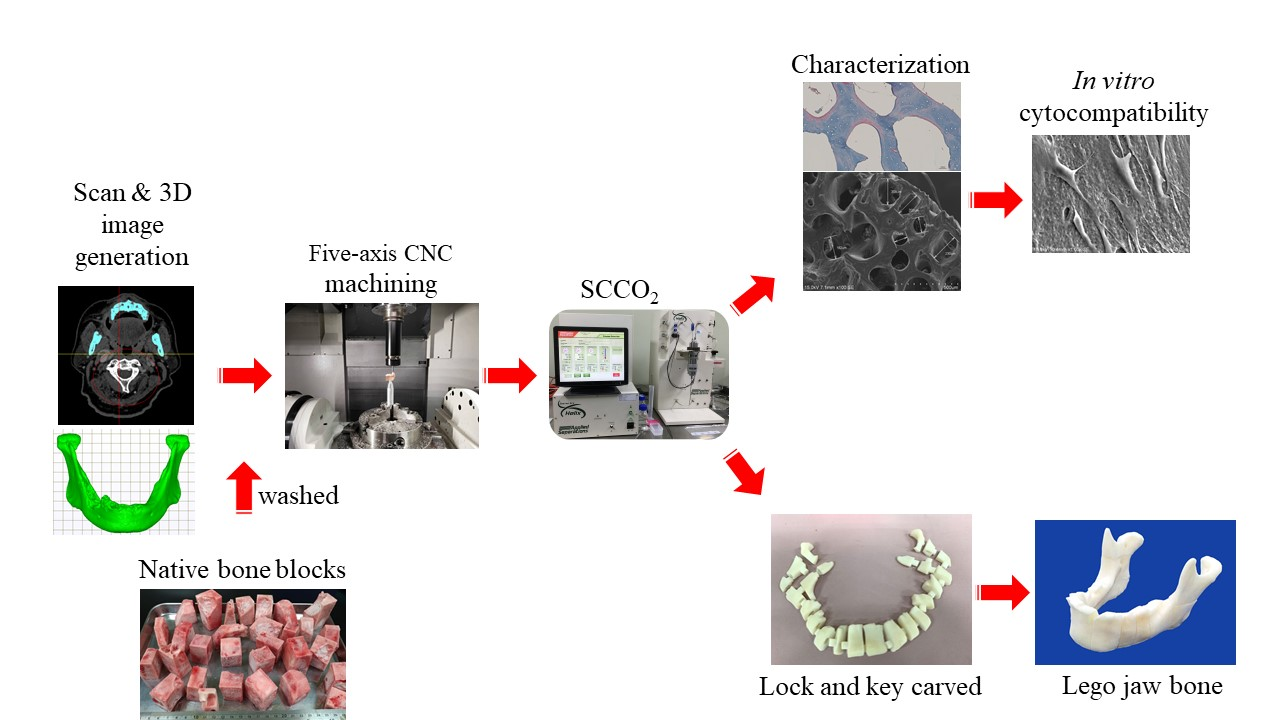
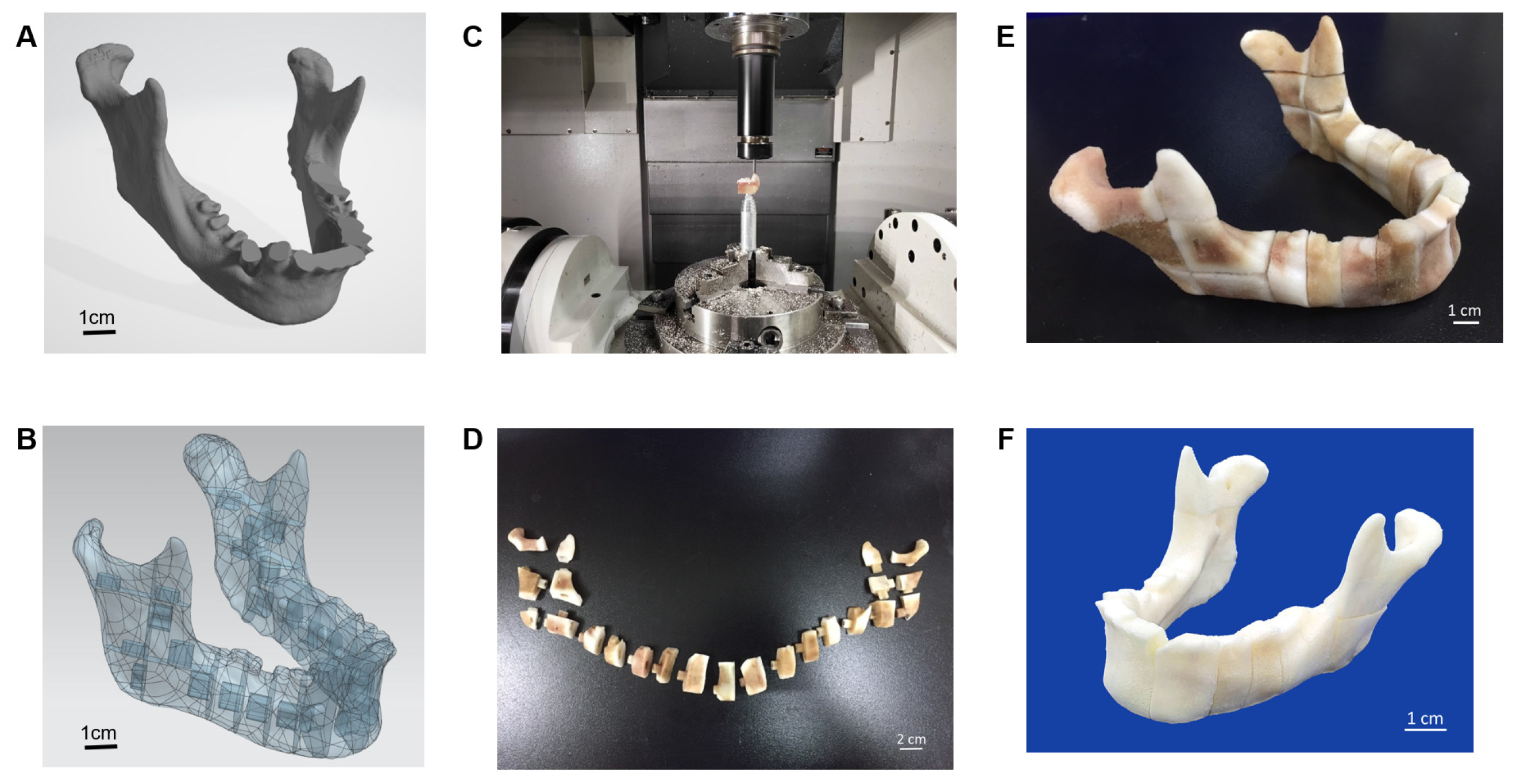
2.1. 3D Mandibular Model Construction
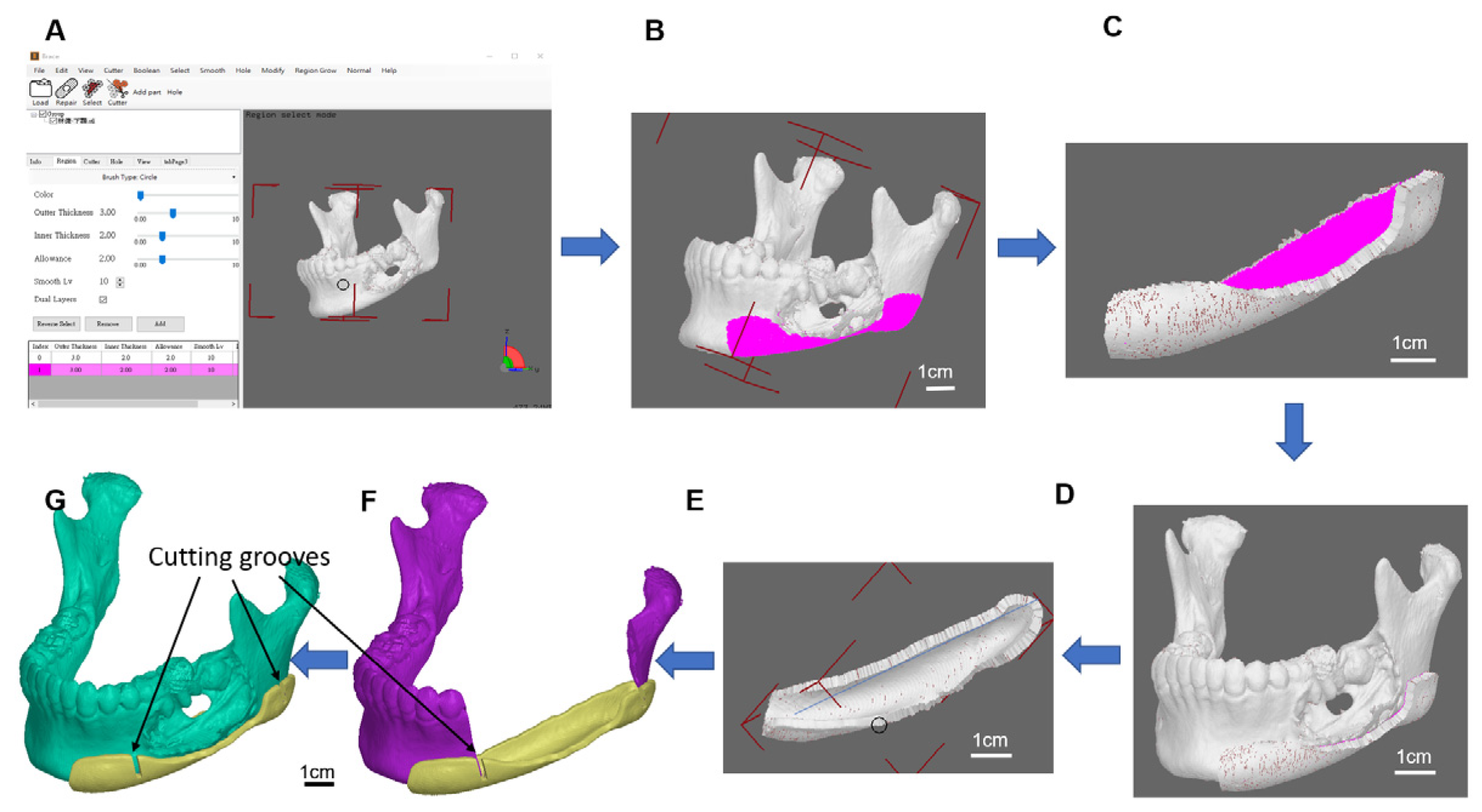
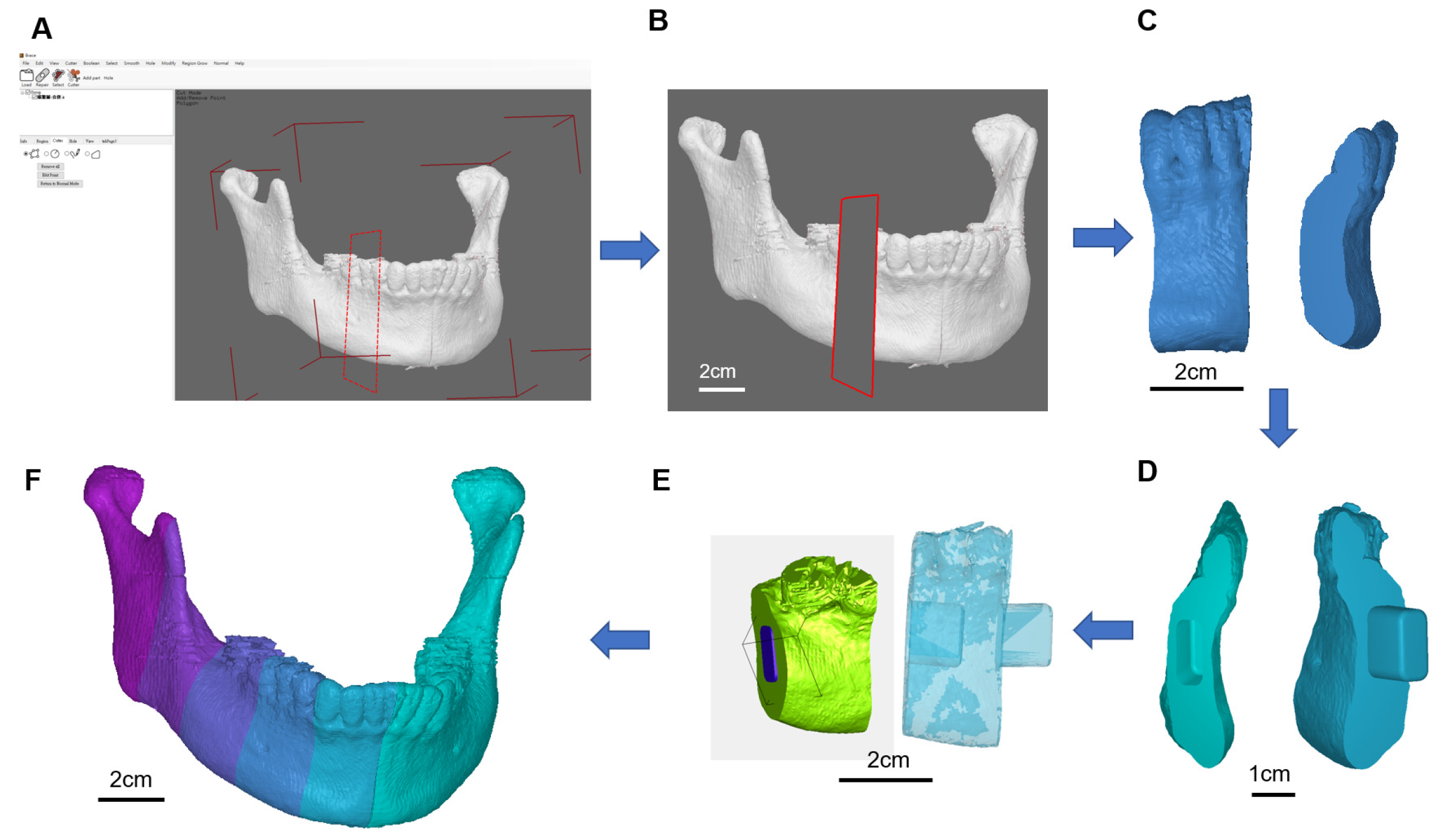
2.2. Osteotomy Guide Fabrication and Multi-Piece Puzzle Setup
2.3. Cutting and Milling a Set of Multi-Piece Lego Assembly for Defect Replacement
2.4. Porcine Bone Preparation
2.5. The SCCO2 Decellularization of Bone Blocks
2.6. Fat Analysis of SCCO2 Decellularized Porcine Bone Blocks
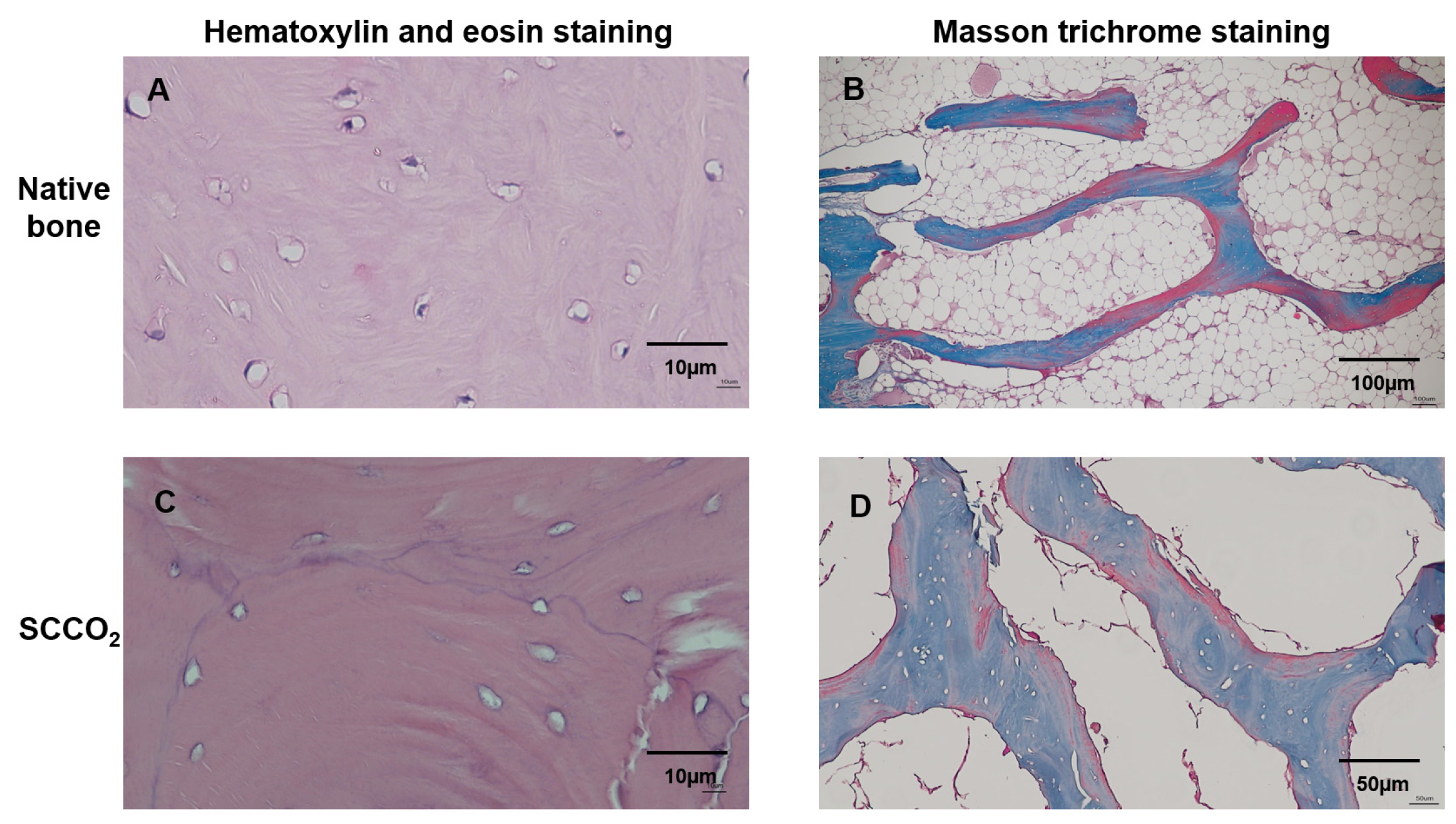
2.7. Hematoxylin and Eosin Staining of SCCO2 Decellularized Porcine Bone Blocks
2.8. Collagen Staining by Masson’s Trichrome Stain of SCCO2 Decellularized Porcine Bone Blocks
2.9. Collagen Quantification by Estimating Hydroxyproline of SCCO2 Decellularized Porcine Bone Blocks
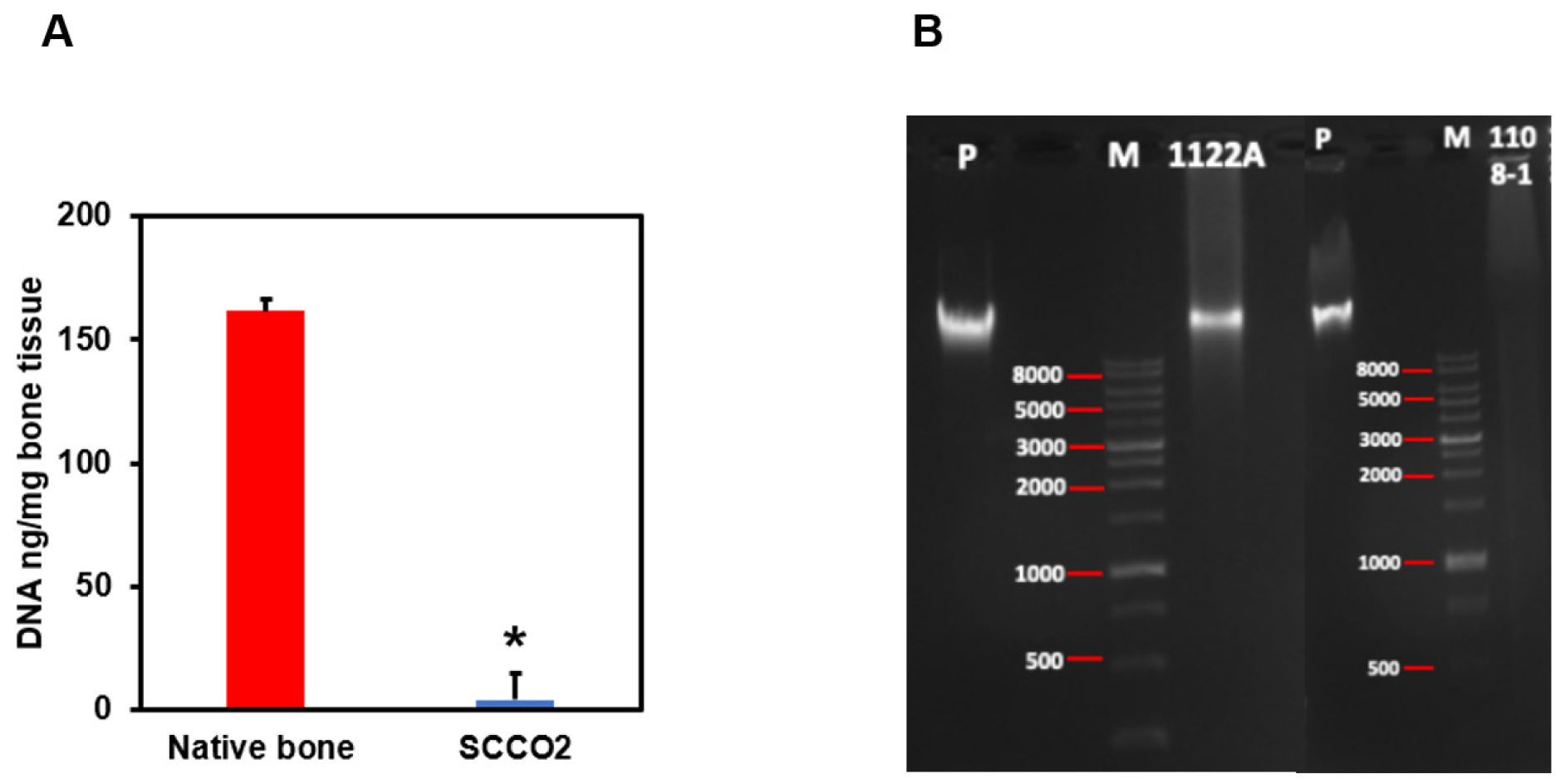
2.10. DNA Quantification and Agarose Gel Electrophoresis of SCCO2 Decellularized Porcine Bone Blocks
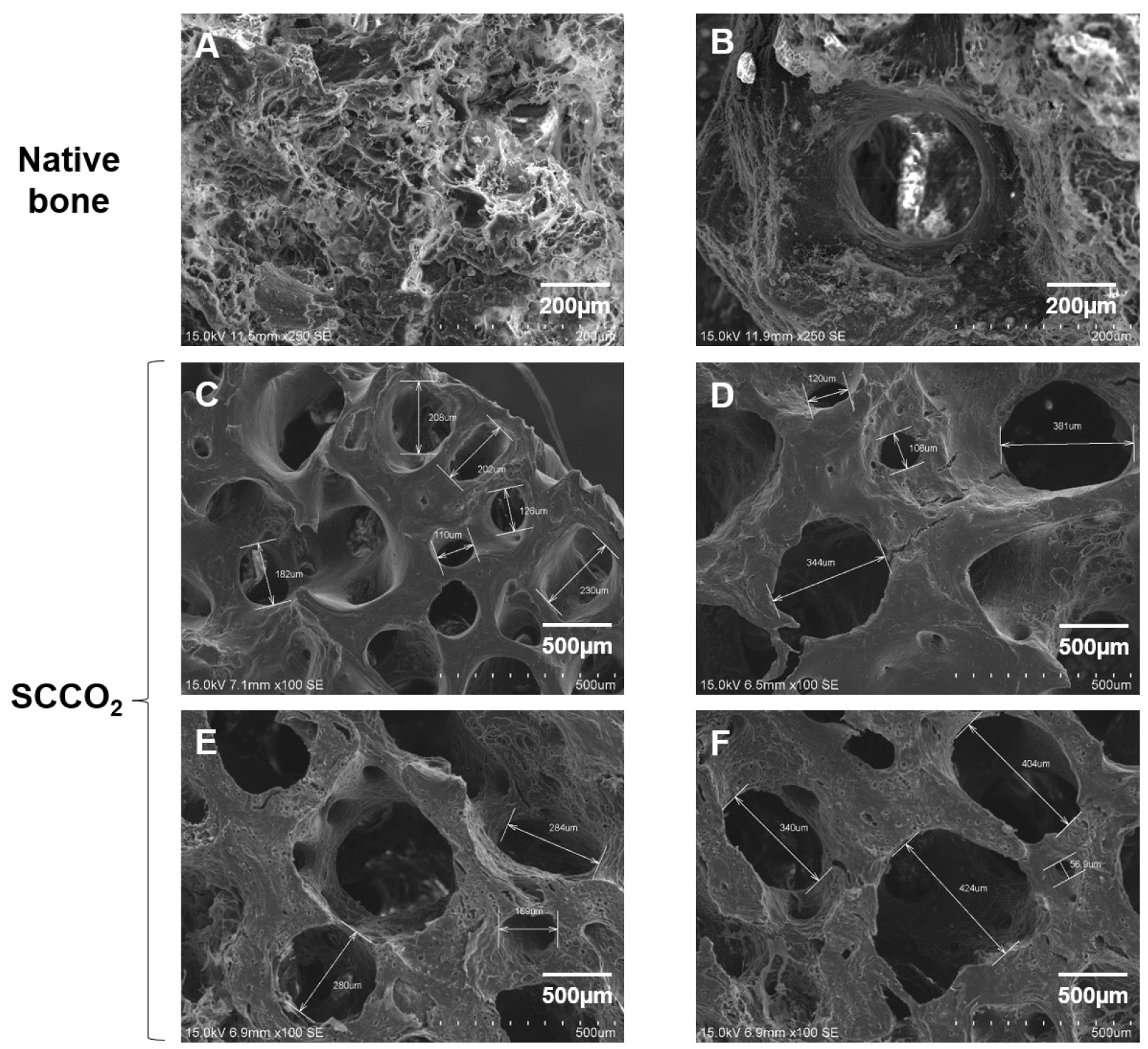
2.11. Electron Microscopy of SCCO2 Decellularized Porcine Bone Blocks
2.12. Stress Analysis of the Decellularized Bone Blocks
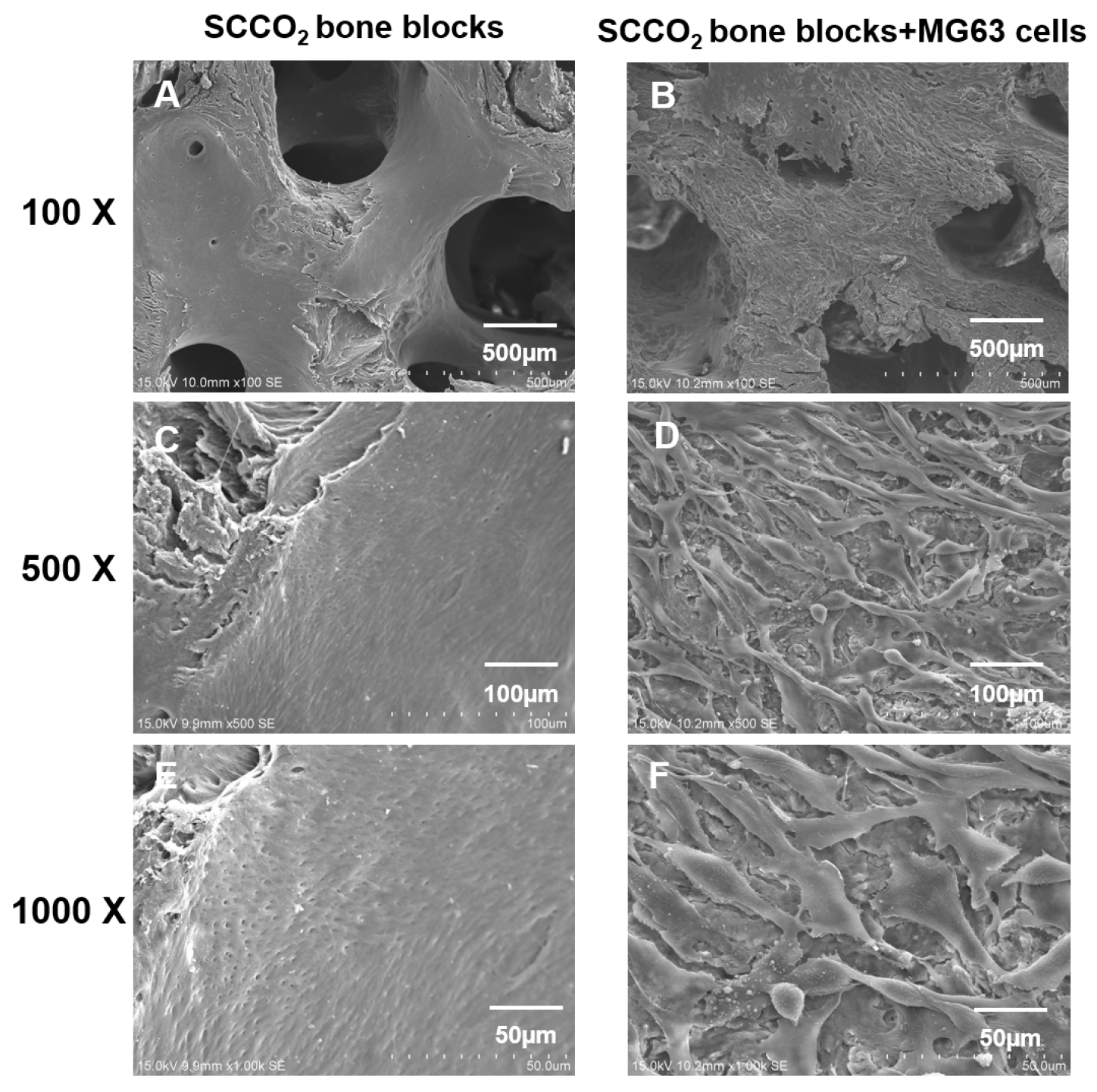
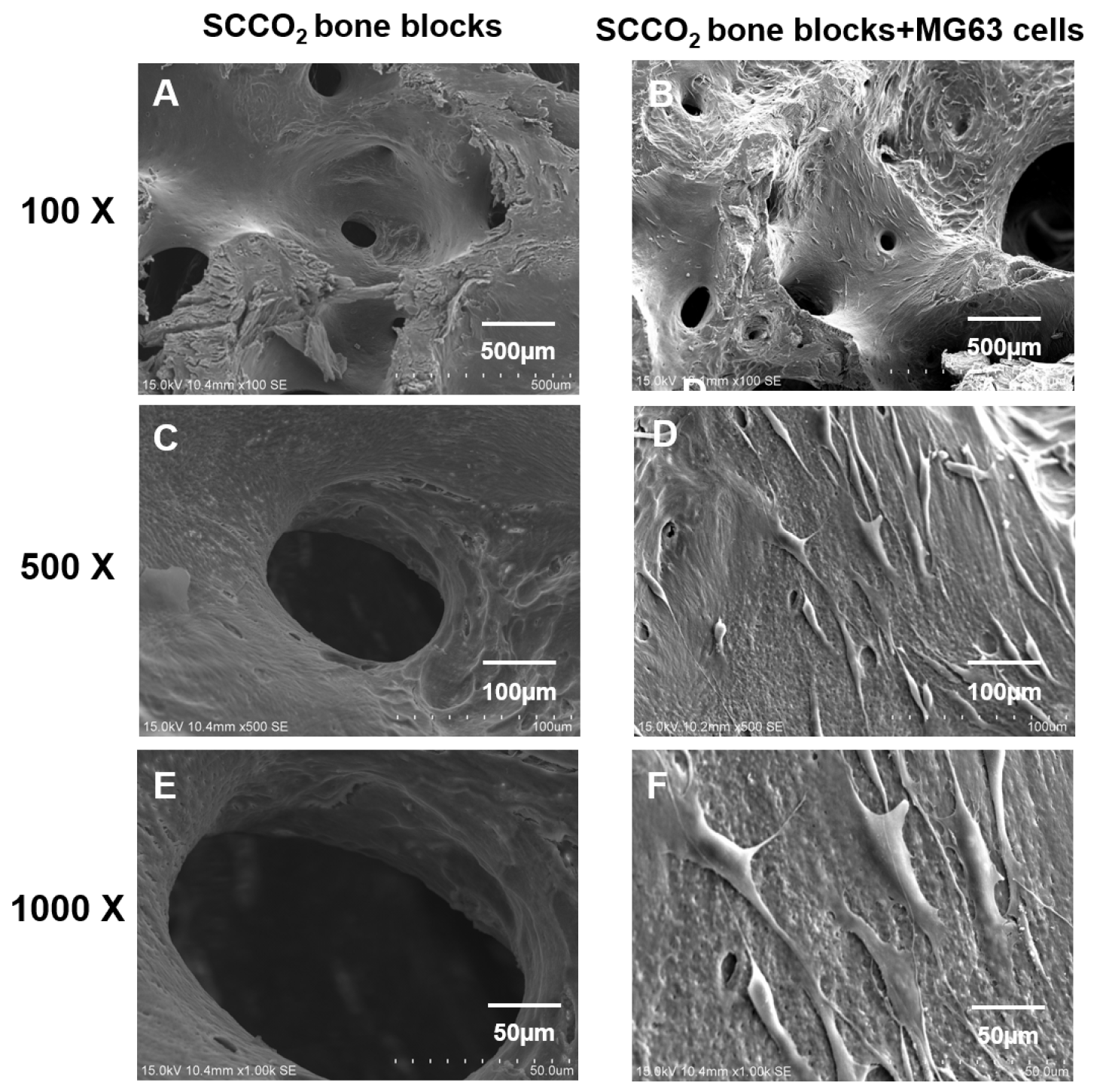
2.13. Cell Adhesion and Growth Analysis on the Decellularized Bone Blocks by SEM
3. Results
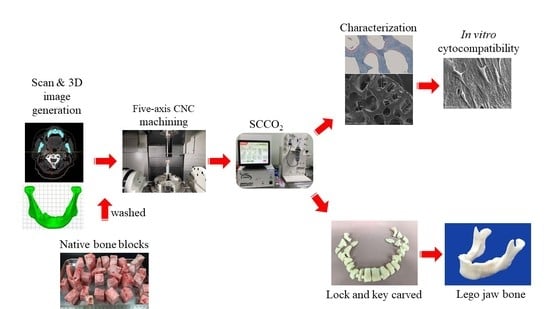
3.1. 3D Tissue Model Reconstruction and Lego Jaw Bone Carving Using 5 Axis CNC Machine
3.2. Characterization of SCCO2 Derived Bone Blocks
3.2.1. Fat Content
3.2.2. H&E Staining
3.2.3. Masson Trichrome Staining
3.2.4. Residual DNA Content
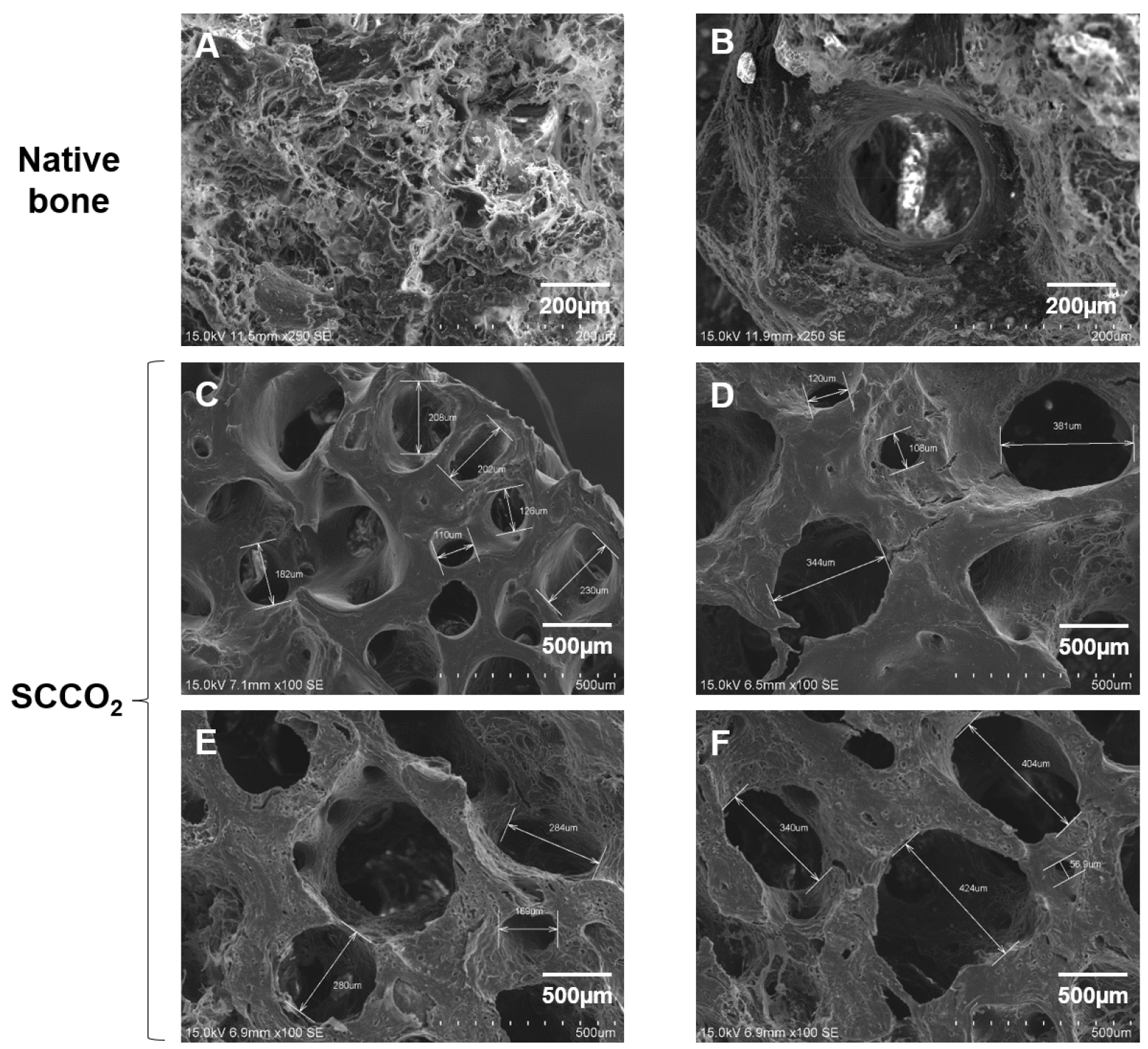
3.2.5. Characterization of SCCO2-Processed Bone Blocks by SEM
3.2.6. Mechanical Strength of SCCO2-Processed Bone Blocks
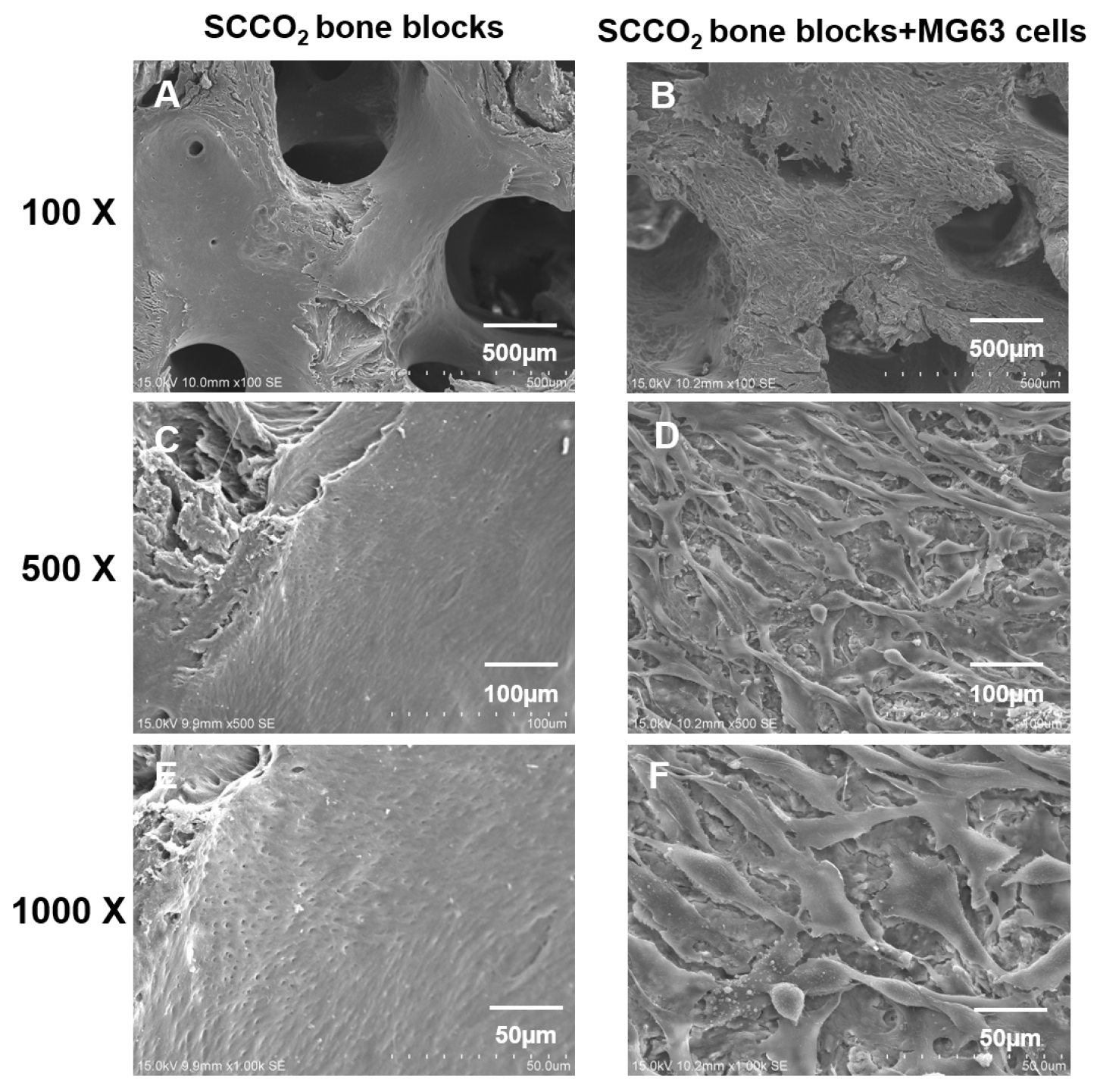
3.2.7. Cell Adhesion and Growth on SCCO2-Processed Bone Blocks by SEM
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Betz, R.R. Limitations of autograft and allograft: New synthetic solutions. Orthopaedics 2002, 25 (Suppl. 5), 561–570. [Google Scholar] [CrossRef] [PubMed]
- Kumar, P.; Vinitha, B.; Fathima, G. Bone grafts in dentistry. J. Pharm. Bioallied Sci. 2013, 5 (Suppl. 1), S125–S127. [Google Scholar] [CrossRef] [PubMed]
- Conrad, E.U.; Gretch, D.R.; Obermeyer, K.R.; Moogk, M.S.; Sayers, M.; Wilson, J.J.; Strong, D.M. Transimission of the hepatitis-C virus by tissue transplantation. J. Bone Jt Surg. Am. 1995, 77, 214–224. [Google Scholar] [CrossRef]
- Phelps, A.M. Transplantation of tissue from lower animals to man, and a report of the case of bone-transplantation at Charity Hospital, Black well’s Island, N.Y. 1891. Clin. Orthop. Relat. Res. 2000, 371, 3–9. [Google Scholar] [CrossRef]
- Fages, J.; Marty, A.; Delga, C.; Condoret, J.S.; Combes, D.; Frayssinet, P. Use of supercritical CO2 for bone delipidation. Biomaterials 1994, 15, 650–656. [Google Scholar] [CrossRef]
- Chen, Y.W.; Hsieh, D.J.; Periasamy, S.; Yen, K.C.; Wang, H.C.; Chien, H.H. Development of a decellularized porcine bone graft by supercritical carbon dioxide extraction technology for bone regeneration. J. Tissue Eng. Regen. Med. 2021, 15, 401–414. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.W.; Chen, M.Y.; Hsieh, D.J.; Periasamy, S.; Yen, K.C.; Chuang, C.T.; Wang, H.C.; Tseng, F.W.; Kuo, J.C.; Chien, H.H. Evaluating the bone-regenerative role of the decellularized porcine bone xenograft in a canine extraction socket model. Clin. Exp. Dent. Res. 2021, 7, 409–418. [Google Scholar] [CrossRef] [PubMed]
- Oryan, A.; Alidadi, S.; Moshiri, A.; Maffulli, N. Bone regenerative medicine: Classic options, novel strategies, and future directions. J. Orthop. Surg. Res. 2014, 9, 18. [Google Scholar] [CrossRef] [Green Version]
- Fernández, M.P.R.; Gehrke, S.A.; Martinez, C.P.A.; Guirado, J.L.C.; de Aza, P.N. SEM-EDX study of the degradation process of two xenograft materials used in sinus lift procedures. Materials 2017, 10, 542. [Google Scholar] [CrossRef] [Green Version]
- Ginebra, M.; Espanol, M.; Maazouz, Y.; Bergez, V.; Pastorino, D. Bioceramics and bone healing. EFORT Open Rev. 2018, 3, 173–183. [Google Scholar] [CrossRef] [PubMed]
- Markopoulos, A.K. Current aspects on oral squamous cell carcinoma. Open Dent. J. 2012, 6, 126–130. [Google Scholar] [CrossRef] [PubMed]
- Rogers, S.N.; Devine, J.; Lowe, D.; Shokar, P.; Brown, J.S.; Vaugman, E.D. Longitudinal health-related quality of life after mandibular resection for oral cancer: A comparison between rim and segment. Head Neck 2004, 26, 54–62. [Google Scholar] [CrossRef]
- Davey, M.; McInerney, N.M.; Barry, T.; Hussey, A.; Potter, S. Virtual Surgical Planning Computer-aided Design-guided Osteocutaneous Fibular Free Flap for Craniofacial Reconstruction: A Novel Surgical Approach. Cureus 2019, 11, e6256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antony, A.K.; Chen, W.F.; Kolokythas, A.; Weimer, K.A.; Cohen, M. Use of virtual surgery and stereolithography-guided osteotomy for mandibular reconstruction with the free fibula. Plast. Reconstr. Surg. 2011, 128, 1080–1084. [Google Scholar] [CrossRef] [PubMed]
- Jindal, S.K.; Sherriff, M.; Waters, M.G.; Smay, J.E. Development of a 3D printable maxillofacial silicone: Part II. Optimization of moderator and thixotropic agent. J. Prosthet. Dent. 2018, 119, 299–304. [Google Scholar] [CrossRef]
- Elbashti, M.; Hattori, M.; Sumita, Y.; Aswehlee, A.; Yoshi, S.; Taniguchi, H. Creating a digitized database of maxillofacial prostheses (obturators): A pilot study. J. Adv. Prosthodont. 2016, 8, 219–223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cristache, C.M.; Tudor, I.; Moraru, L.; Cristache, G.; Lanza, A.; Burlibasa, M. Digital Workflow in Maxillofacial Prosthodontics—An Update on Defect Data Acquisition, Editing and Design Using Open-Source and Commercial Available Software. Appl. Sci. 2021, 11, 973. [Google Scholar] [CrossRef]
- Sharaf, B.; Levine, J.P.; Hirsch, D.L.; Bastidas, J.A.; Schiff, B.A.; Garfein, E.S. Importance of computer-aided design and manufacturing technology in the multidisciplinary approach to head and neck reconstruction. J. Craniofac. Surg. 2010, 21, 1277–1280. [Google Scholar] [CrossRef] [PubMed]
- Bhumiratana, S.; Bernhard, J.C.; Alfi, D.M.; Yeager, K.; Eton, R.E.; Bova, J.; Shah, F.; Gimble, J.M.; Lopez, M.J.; Eisig, S.B.; et al. Tissue-engineered autologous grafts for facial bone reconstruction. Sci. Transl. Med. 2016, 8, 34–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mangano, F.; Zecca, P.; Pozzi-Taubert, S.; Macchi, A.; Ricci, M.; Luongo, G.; Mangano, C. Maxillary sinus augmentation using computer-aided design/computer-aided manufacturing (CAD/CAM) technology. Int. J. Med. Robot. 2013, 9, 331–338. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.F.; Xu, L.W.; Zhu, H.Y.; Liu, S.S. Technical procedures for template-guided surgery for mandibular reconstruction based on digital design and manufacturing. Biomed. Eng. Online 2014, 13, 63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Figliuzzi, M.; Mangano, F.G.; Fortunato, L.; De Fazio, R.; Macchi, A.; Iezzi, G.; Piattelli, A.; Mangano, C. Vertical ridge augmentation of the atrophic posterior mandible with custommade, computer-aided design/computer-aided manufacturing porous hydroxyapatite scaffolds. J. Craniofac. Surg. 2013, 24, 856–859. [Google Scholar] [CrossRef] [PubMed]
- Helal, M.H.; Hendawy, H.D.; Gaber, R.A.; Helal, N.R.; Aboushelib, M.N. Osteogenesis ability of CAD-CAM biodegradable polylactic acid scaffolds for reconstruction of jaw defects. J. Prosthet. Dent. 2019, 121, 118–123. [Google Scholar] [CrossRef] [PubMed]
- Wong, T.-Y.; Liu, J.-K.; Fang, J.-J.; Wu, T.-C.; Tu, Y.-S. Use of the Matching-Optimal-Symmetry-Plane Method in Planning Surgical Correction of Facial Asymmetry—A preliminary report on 20 patients. J. Oral Maxillofac. Surg. 2014, 72, 1180.e1–1180.e13. [Google Scholar] [CrossRef]
- Scarano, A.; Piattelli, A.; Perrotti, V.; Manzon, L.; Iezzi, G. Maxillary Sinus Augmentation in Humans Using Cortical Porcine Bone: A Histological and Histomorphometrical Evaluation after 4 and 6 Months. Clin. Implant. Dent. Relat. Res. 2011, 13, 13–18. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.H.; Tseng, F.W.; Chang, W.H.; Peng, I.C.; Hsieh, D.J.; Wu, S.W.; Yeh, M.L. Preparation of acellular scaffold for corneal tissue engineering by supercritical carbon dioxide extraction technology. Acta Biomater. 2017, 58, 238–243. [Google Scholar] [CrossRef] [PubMed]
- Liang, C.M.; Hsieh, D.J.; Tseng, F.W.; Srinivasan, P.; Yeh, M.L.; Tai, M.C. Acellular Porcine Cornea Produced by Supercritical Carbon Dioxide Extraction: A Potential Substitute for Human Corneal Regeneration. Cornea 2022, 41, 328–338. [Google Scholar] [CrossRef]
- Chou, P.R.; Lin, Y.N.; Wu, S.H.; Lin, S.D.; Srinivasan, P.; Hsieh, D.J.; Huang, S.H. Supercritical Carbon Dioxide-decellularized Porcine Acellular Dermal Matrix combined with Autologous Adipose-derived Stem Cells: Its Role in Accelerated Diabetic Wound Healing. Int. J. Med. Sci. 2020, 17, 354–367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, K.F.; Chen, R.F.; Li, Y.T.; Lin, Y.N.; Hsieh, D.J.; Periasamy, S.; Lin, S.D.; Kuo, Y.R. Supercritical Carbon Dioxide Decellularized Bone Matrix Seeded with Adipose-Derived Mesenchymal Stem Cells Accelerated Bone Regeneration. Biomedicines 2021, 9, 1825. [Google Scholar] [CrossRef]
- Huang, C.H.; Hsieh, D.J.; Wu, Y.C.; Yen, K.C.; Srinivasan, P.; Lee, H.C.; Chen, Y.C.; Lee, S.S. Reconstruction of the orbital floor using supercritical CO(2) decellularized porcine bone graft. Int. J. Med. Sci. 2021, 18, 3684–3691. [Google Scholar] [CrossRef] [PubMed]
- Toth, B.A.; Ellis, D.S.; Stewart, W.B. Computer-designed prostheses for orbitocranial reconstruction. Plast. Reconstr. Surg. 1988, 81, 315–324. [Google Scholar] [CrossRef] [PubMed]
- Panicker, P.P.; Mohan, S.P.; Nallusamy, J.; Lakshmi, S.J.; Johny, J.; Bhaskaran, M.K. Reconstruction of Craniofacial Bone Defects with Autologous Human Bone Marrow Stem Cells and Autogenous Bone Grafts: A Case Report with Review of Literature. J. Pharm. Bioallied. Sci. 2020, 12 (Suppl. 1), S394–S398. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.J.; Lee, H.P.; Tse, K.M.; Cheong, E.C.; Lim, S.P. Computer-aided design and rapid prototyping-assisted contouring of costal cartilage graft for facial reconstructive surgery. Craniomaxillofac. Trauma Reconstr. 2012, 5, 75–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seyler, T.M.; Bracey, D.N.; Plate, J.F.; Lively, M.O.; Mannava, S.; Smith, T.L.; Whitlock, P.W. The development of a xenograft-derived scaffold for tendon and ligament reconstruction using a decellurisation and oxidation protocol. Arthroscopy 2017, 33, 374–386. [Google Scholar] [CrossRef] [PubMed]
- Elder, S.; Chenault, H.; Gloth, P.; Webb, K.; Recinos, R.; Wright, E.; Cooley, A. Effects of antigen removal on a porcine osteochondral xenograft for articular cartilage repair. J. Biomed. Mater. Res. A 2018, 106, 2251–2260. [Google Scholar] [CrossRef] [PubMed]
- Bertoldi, S.; Fare, S.; Tanzi, M.C. Assessment of scaffold porosity: The new route of micro-CT. J. Appl. Biomech. 2011, 9, 165–175. [Google Scholar] [CrossRef] [PubMed]
- Bracey, D.N.; Seyler, T.M.; Jinnah, A.H.; Lively, M.O.; Willey, J.S.; Smith, T.L.; Whitlock, P.W. A decellularized porcine xenograftderived bone scaffold for clinical use as a bone graft substitute: A critical evaluation of processing and structure. J. Funct. Biomater. 2018, 9, 45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vilela, M.J.C.; Colaço, B.J.A.; Ventura, J.; Monteiro, F.J.M.; Salgado, C.L. Translational Research for Orthopedic Bone Graft Development. Materials 2021, 14, 4130. [Google Scholar] [CrossRef] [PubMed]
- Ling, Y.; Xu, W.; Yang, L.; Liang, C.; Xu, B. Improved the biocompatibility of cancellous bone with compound physicochemical decellurisation process. Regen. Biomater. 2020, 7, 443–451. [Google Scholar] [CrossRef] [PubMed]
- Maté Sánchez de Val, J.E.; Calvo-Guirado, J.L.; Gómez-Moreno, G.; Pérez- Albacete Martínez, C.; Mazón, P.; De Aza, P.N. Influence of hydroxyapatite granule size, porosity, and crystallinity on tissue reaction in vivo. Part A: Synthesis, characterization of the materials, and SEM analysis. Clin. Implant Dent. Relat. Res. 2016, 27, 1331–1338. [Google Scholar] [CrossRef] [PubMed]
- de Almeida, C.S.; Sartoretto, S.C.; Durte, I.M.; Alves, A.T.N.N.; Barreto, H.V.; Resende, R.F.B.; Calasans-Maia, M.D.; de Albuquerque, J.C. In Vivo Evaluation of Bovine Xenograft Associated with Oxygen Therapy in Alveolar Bone Repair. J. Oral Implantol. 2021, 47, 465–471. [Google Scholar] [CrossRef] [PubMed]
- International Organisation for Standardisation [ISO]. ISO 10993-11: Biological Evaluation of Medical Devices—Part 11 Tests for Systemic Toxicity. 2017. Available online: http://nhiso.com/wp-content/uploads/2018/05/ISO-10993-11-2017.pdf (accessed on 10 February 2022).
- Gilpin, A.; Yang, Y. Decellurisation strategies for regenerative medicine: From processing techniques to applications. Biomed. Res. Int. 2017, 2017, 9831534. [Google Scholar] [CrossRef] [Green Version]
- Goetze, E.; Gielisch, M.; Moergel, M.; Al-Nawas, B. Accelerated workflow for primary jaw reconstruction with microvascular fibula graft. 3D Print Med. 2017, 3, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gerressen, M.; Pastaschek, C.I.; Riediger, D.; Hilgers, R.D.; Hölzle, F.; Noroozi, N.; Ghassemi, A. Microsurgical Free Flap Reconstructions of Head and Neck Region in 406 Cases: A 13-Year Experience. J. Oral Maxillofac. Surg. 2013, 71, 628–635. [Google Scholar] [CrossRef]
- Rodby, K.A.; Turin, S.; Jacobs, R.J.; Cruz, J.F.; Hassid, V.J.; Kolokythas, A.; Antony, A.K. Advances in oncologic head and neck reconstruction: Systematic review and future considerations of virtual surgical planning and computer aided design/computer aided modeling. J. Plast. Reconstr. Aesthet. Surg. 2014, 67, 1171–1185. [Google Scholar] [CrossRef]
- Sieira Gil, R.; Roig, A.M.; Obispo, C.A.; Morla, A.; Pages, C.M.; Perez, J.L. Surgical planning and microvascular reconstruction of the mandible with a fibular flap using computer-aided design, rapid prototype modelling, and precontoured titanium reconstruction plates: A prospective study. Br. J. Oral Maxillofac. Surg. 2015, 53, 49–53. [Google Scholar] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| SCCO2 Derived Bone Blocks | Mechanical Stiffness (MPa) Mean ± SD |
|---|---|
| 2 × 3 × 2 cm3 | 13.75 ± 3.99 |
| 2 × 2 × 2 cm3 | 11.34 ± 1.74 |
| 2 × 1 × 2 cm3 | 3.46 ± 3.04 |
| 1 × 1 × 2 cm3 | 12.18 ± 1.40 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, M.-Y.; Fang, J.-J.; Lee, J.-N.; Periasamy, S.; Yen, K.-C.; Wang, H.-C.; Hsieh, D.-J. Supercritical Carbon Dioxide Decellularized Xenograft-3D CAD/CAM Carved Bone Matrix Personalized for Human Bone Defect Repair. Genes 2022, 13, 755. https://doi.org/10.3390/genes13050755
Chen M-Y, Fang J-J, Lee J-N, Periasamy S, Yen K-C, Wang H-C, Hsieh D-J. Supercritical Carbon Dioxide Decellularized Xenograft-3D CAD/CAM Carved Bone Matrix Personalized for Human Bone Defect Repair. Genes. 2022; 13(5):755. https://doi.org/10.3390/genes13050755
Chicago/Turabian StyleChen, Meng-Yen, Jing-Jing Fang, Jeng-Nan Lee, Srinivasan Periasamy, Ko-Chung Yen, Hung-Chou Wang, and Dar-Jen Hsieh. 2022. "Supercritical Carbon Dioxide Decellularized Xenograft-3D CAD/CAM Carved Bone Matrix Personalized for Human Bone Defect Repair" Genes 13, no. 5: 755. https://doi.org/10.3390/genes13050755
APA StyleChen, M.-Y., Fang, J.-J., Lee, J.-N., Periasamy, S., Yen, K.-C., Wang, H.-C., & Hsieh, D.-J. (2022). Supercritical Carbon Dioxide Decellularized Xenograft-3D CAD/CAM Carved Bone Matrix Personalized for Human Bone Defect Repair. Genes, 13(5), 755. https://doi.org/10.3390/genes13050755