KRAS and BRAF Mutations as Prognostic and Predictive Biomarkers for Standard Chemotherapy Response in Metastatic Colorectal Cancer: A Single Institutional Study


 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Mutational Analysis
2.3. Statistical Analysis
2.4. Ethics Statement
3. Results
3.1. Patients Characteristics
3.2. Patients That Received Biologic Treatment Showed a Better Outcome and Treatment Response
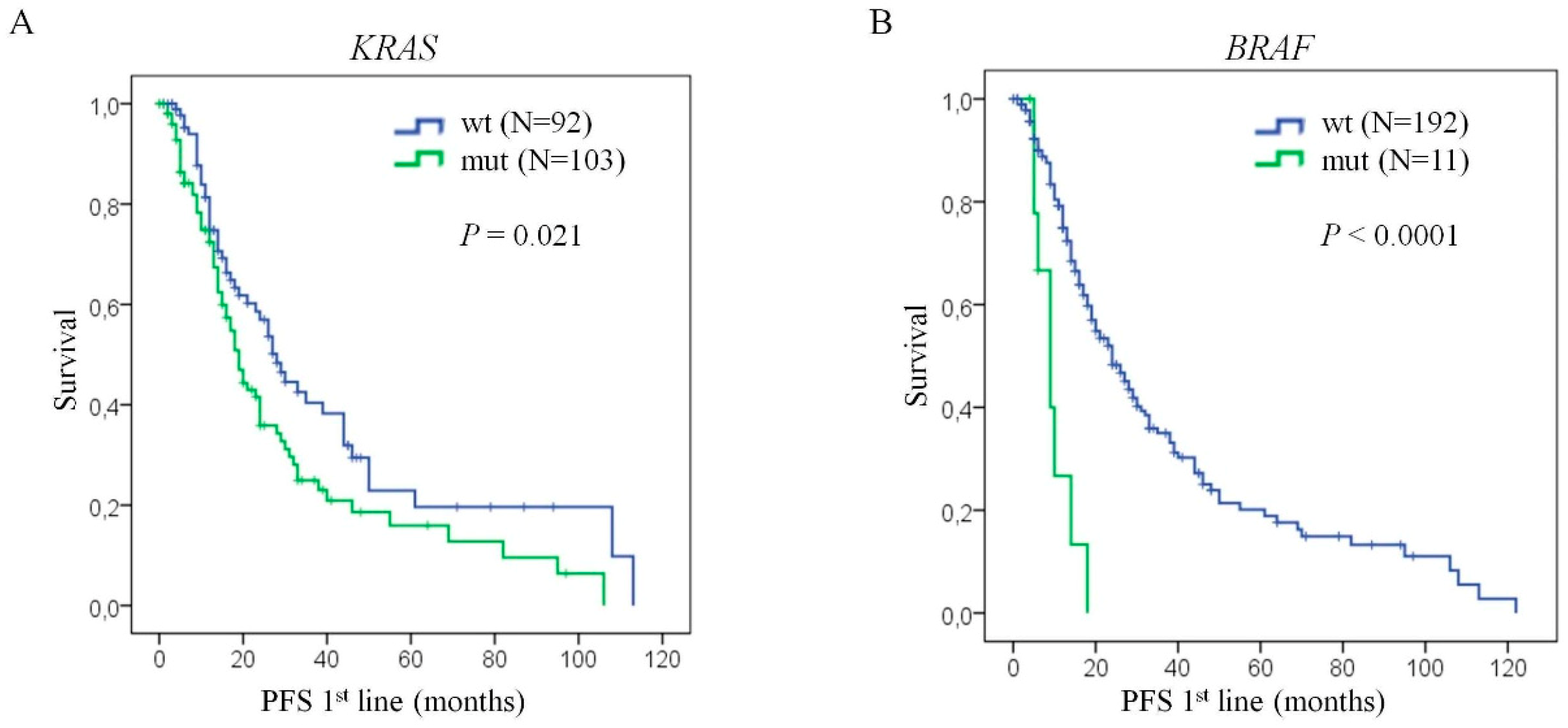
3.3. KRAS and BRAF Mutations Have An Impact on Progression-Free Survival of Patients
3.4. KRAS Mutation Status is Associated with a Lack of Benefit From Standard Chemotherapy
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2019. CA Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef] [PubMed]
- Van Abbema, D.; Vissers, P.; de Vos-Geelen, J.; Lemmens, V.; Janssen-Heijnen, M.; Tjan-Heijnen, V. Trends in Overall Survival and Treatment Patterns in Two Large Population-Based Cohorts of Patients with Breast and Colorectal Cancer. Cancers 2019, 11, 1239. [Google Scholar] [CrossRef] [PubMed]
- Zacharakis, M.; Xynos, I.D.; Lazaris, A.; Smaro, T.; Kosmas, C.; Dokou, A.; Felekouras, E.; Antoniou, E.; Polyzos, A.; Sarantonis, J.; et al. Predictors of Survival in Stage IV Metastatic Colorectal Cancer. Anticancer Res. 2010, 30, 653–660. [Google Scholar] [PubMed]
- Bhullar, D.S.; Barriuso, J.; Mullamitha, S.; Saunders, M.P.; O’Dwyer, S.T.; Aziz, O. Biomarker concordance between primary colorectal cancer and its metastases. EBioMedicine 2019, 40, 363–374. [Google Scholar] [CrossRef]
- Hamers, P.; Bos, A.C.R.K.; May, A.M.; Punt, C.J.A.; Koopman, M.; Vink, G.R. Recent changes in overall survival of real-life stage IV colorectal cancer patients. JCO 2019, 37, 3522. [Google Scholar] [CrossRef]
- Adam, R.; Kitano, Y. Multidisciplinary approach of liver metastases from colorectal cancer. Ann. Gastroenterol. Surg 2019, 3, 50–56. [Google Scholar] [CrossRef] [PubMed]
- Cremolini, C.; Schirripa, M.; Antoniotti, C.; Moretto, R.; Salvatore, L.; Masi, G.; Falcone, A.; Loupakis, F. First-line chemotherapy for mCRC—A review and evidence-based algorithm. Nat. Rev. Clin. Oncol. 2015, 12, 607–619. [Google Scholar] [CrossRef]
- Malka, D.; Rotolo, F.; Boige, V. First-line treatment in metastatic colorectal cancer: Important or crucial? Eur. J. Cancer 2017, 84, 363–366. [Google Scholar] [CrossRef]
- Porru, M.; Pompili, L.; Caruso, C.; Biroccio, A.; Leonetti, C. Targeting KRAS in metastatic colorectal cancer: Current strategies and emerging opportunities. J. Exp. Clin. Cancer Res. 2018, 37, 57. [Google Scholar] [CrossRef]
- Lièvre, A.; Bachet, J.-B.; Le Corre, D.; Boige, V.; Landi, B.; Emile, J.-F.; Côté, J.-F.; Tomasic, G.; Penna, C.; Ducreux, M.; et al. KRAS mutation status is predictive of response to cetuximab therapy in colorectal cancer. Cancer Res. 2006, 66, 3992–3995. [Google Scholar] [CrossRef]
- Atreya, C.E.; Yaeger, R.; Chu, E. Systemic Therapy for Metastatic Colorectal Cancer: From Current Standards to Future Molecular Targeted Approaches. Am. Soc. Clin. Oncol. Educ. Book 2017, 37, 246–256. [Google Scholar] [CrossRef] [PubMed]
- Bennouna, J.; Sastre, J.; Arnold, D.; Österlund, P.; Greil, R.; Van Cutsem, E.; von Moos, R.; Viéitez, J.M.; Bouché, O.; Borg, C.; et al. Continuation of bevacizumab after first progression in metastatic colorectal cancer (ML18147): A randomised phase 3 trial. Lancet Oncol. 2013, 14, 29–37. [Google Scholar] [CrossRef]
- Hurwitz, H.; Fehrenbacher, L.; Novotny, W.; Cartwright, T.; Hainsworth, J.; Heim, W.; Berlin, J.; Baron, A.; Griffing, S.; Holmgren, E.; et al. Bevacizumab plus irinotecan, fluorouracil, and leucovorin for metastatic colorectal cancer. N. Engl. J. Med. 2004, 350, 2335–2342. [Google Scholar] [CrossRef] [PubMed]
- Allegra, C.J.; Jessup, J.M.; Somerfield, M.R.; Hamilton, S.R.; Hammond, E.H.; Hayes, D.F.; McAllister, P.K.; Morton, R.F.; Schilsky, R.L. American Society of Clinical Oncology provisional clinical opinion: Testing for KRAS gene mutations in patients with metastatic colorectal carcinoma to predict response to anti-epidermal growth factor receptor monoclonal antibody therapy. J. Clin. Oncol. 2009, 27, 2091–2096. [Google Scholar] [CrossRef]
- Tol, J.; Nagtegaal, I.D.; Punt, C.J.A. BRAF mutation in metastatic colorectal cancer. N. Engl. J. Med. 2009, 361, 98–99. [Google Scholar] [CrossRef] [PubMed]
- Di Nicolantonio, F.; Martini, M.; Molinari, F.; Sartore-Bianchi, A.; Arena, S.; Saletti, P.; De Dosso, S.; Mazzucchelli, L.; Frattini, M.; Siena, S.; et al. Wild-type BRAF is required for response to panitumumab or cetuximab in metastatic colorectal cancer. J. Clin. Oncol. 2008, 26, 5705–5712. [Google Scholar] [CrossRef]
- Richman, S.D.; Seymour, M.T.; Chambers, P.; Elliott, F.; Daly, C.L.; Meade, A.M.; Taylor, G.; Barrett, J.H.; Quirke, P. KRAS and BRAF mutations in advanced colorectal cancer are associated with poor prognosis but do not preclude benefit from oxaliplatin or irinotecan: Results from the MRC FOCUS trial. J. Clin. Oncol. 2009, 27, 5931–5937. [Google Scholar] [CrossRef]
- Pietrantonio, F.; Vernieri, C.; Siravegna, G.; Mennitto, A.; Berenato, R.; Perrone, F.; Gloghini, A.; Tamborini, E.; Lonardi, S.; Morano, F.; et al. Heterogeneity of Acquired Resistance to Anti-EGFR Monoclonal Antibodies in Patients with Metastatic Colorectal Cancer. Clin. Cancer Res. 2017, 23, 2414–2422. [Google Scholar] [CrossRef]
- Foo, J.; Michor, F. Evolution of acquired resistance to anti-cancer therapy. J. Theor. Biol. 2014, 355, 10–20. [Google Scholar] [CrossRef]
- Chambers, A.E.; Frick, J.; Tanner, N.; Gerkin, R.; Kundranda, M.; Dragovich, T. Chemotherapy re-challenge response rate in metastatic colorectal cancer. J. Gastrointest. Oncol. 2018, 9, 679–686. [Google Scholar] [CrossRef]
- Poulogiannis, G.; Luo, F.; Arends, M.J. RAS signalling in the colorectum in health and disease. Cell Commun. Adhes. 2012, 19, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Cox, A.D.; Fesik, S.W.; Kimmelman, A.C.; Luo, J.; Der, C.J. Drugging the undruggable RAS: Mission possible? Nat. Rev. Drug Discov. 2014, 13, 828–851. [Google Scholar] [CrossRef] [PubMed]
- Guerrero, S.; Casanova, I.; Farré, L.; Mazo, A.; Capellà, G.; Mangues, R. K-ras codon 12 mutation induces higher level of resistance to apoptosis and predisposition to anchorage-independent growth than codon 13 mutation or proto-oncogene overexpression. Cancer Res. 2000, 60, 6750–6756. [Google Scholar] [PubMed]
- Davies, H.; Bignell, G.R.; Cox, C.; Stephens, P.; Edkins, S.; Clegg, S.; Teague, J.; Woffendin, H.; Garnett, M.J.; Bottomley, W.; et al. Mutations of the BRAF gene in human cancer. Nature 2002, 417, 949–954. [Google Scholar] [CrossRef] [PubMed]
- Korphaisarn, K.; Kopetz, S. BRAF-directed Therapy in Metastatic Colorectal Cancer. Cancer J. 2016, 22, 175–178. [Google Scholar] [CrossRef]
- Tiacci, E.; Trifonov, V.; Schiavoni, G.; Holmes, A.; Kern, W.; Martelli, M.P.; Pucciarini, A.; Bigerna, B.; Pacini, R.; Wells, V.A.; et al. BRAF Mutations in Hairy-Cell Leukemia. N. Engl. J. Med. 2011, 364, 2305–2315. [Google Scholar] [CrossRef]
- Greaves, W.O.; Verma, S.; Patel, K.P.; Davies, M.A.; Barkoh, B.A.; Galbincea, J.M.; Yao, H.; Lazar, A.J.; Aldape, K.D.; Medeiros, L.J.; et al. Frequency and spectrum of BRAF mutations in a retrospective, single-institution study of 1112 cases of melanoma. J. Mol. Diagn. 2013, 15, 220–226. [Google Scholar] [CrossRef]
- Kim, T.H.; Park, Y.J.; Lim, J.A.; Ahn, H.Y.; Lee, E.K.; Lee, Y.J.; Kim, K.W.; Hahn, S.K.; Youn, Y.K.; Kim, K.H.; et al. The association of the BRAF(V600E) mutation with prognostic factors and poor clinical outcome in papillary thyroid cancer: A meta-analysis. Cancer 2012, 118, 1764–1773. [Google Scholar] [CrossRef] [PubMed]
- Fukushima, T.; Suzuki, S.; Mashiko, M.; Ohtake, T.; Endo, Y.; Takebayashi, Y.; Sekikawa, K.; Hagiwara, K.; Takenoshita, S. BRAF mutations in papillary carcinomas of the thyroid. Oncogene 2003, 22, 6455–6457. [Google Scholar] [CrossRef]
- Brustugun, O.T.; Khattak, A.M.; Trømborg, A.K.; Beigi, M.; Beiske, K.; Lund-Iversen, M.; Helland, Å. BRAF-mutations in non-small cell lung cancer. Lung Cancer 2014, 84, 36–38. [Google Scholar] [CrossRef] [PubMed]
- Ding, X.; Zhang, Z.; Jiang, T.; Li, X.; Zhao, C.; Su, B.; Zhou, C. Clinicopathologic characteristics and outcomes of Chinese patients with non-small-cell lung cancer and BRAF mutation. Cancer Med. 2017, 6, 555–562. [Google Scholar] [CrossRef] [PubMed]
- Tie, J.; Gibbs, P.; Lipton, L.; Christie, M.; Jorissen, R.N.; Burgess, A.W.; Croxford, M.; Jones, I.; Langland, R.; Kosmider, S.; et al. Optimizing targeted therapeutic development: Analysis of a colorectal cancer patient population with the BRAFV600E mutation. Int. J. Cancer 2011, 128, 2075–2084. [Google Scholar] [CrossRef] [PubMed]
- Rajagopalan, H.; Bardelli, A.; Lengauer, C.; Kinzler, K.W.; Vogelstein, B.; Velculescu, V.E. Tumorigenesis: RAF/RAS oncogenes and mismatch-repair status. Nature 2002, 418, 934. [Google Scholar] [CrossRef] [PubMed]
- Morkel, M.; Riemer, P.; Bläker, H.; Sers, C. Similar but different: Distinct roles for KRAS and BRAF oncogenes in colorectal cancer development and therapy resistance. Oncotarget 2015, 6, 20785–20800. [Google Scholar] [CrossRef]
- Midthun, L.; Shaheen, S.; Deisch, J.; Senthil, M.; Tsai, J.; Hsueh, C.-T. Concomitant KRAS and BRAF mutations in colorectal cancer. J. Gastrointest. Oncol. 2019, 10, 577–581. [Google Scholar] [CrossRef]
- Tanaka, M.; Omura, K.; Watanabe, Y.; Oda, Y.; Nakanishi, I. Prognostic factors of colorectal cancer: K-ras mutation, overexpression of the p53 protein, and cell proliferative activity. J. Surg. Oncol. 1994, 57, 57–64. [Google Scholar] [CrossRef]
- Tran, B.; Kopetz, S.; Tie, J.; Gibbs, P.; Jiang, Z.-Q.; Lieu, C.H.; Agarwal, A.; Maru, D.M.; Sieber, O.; Desai, J. Impact of BRAF mutation and microsatellite instability on the pattern of metastatic spread and prognosis in metastatic colorectal cancer. Cancer 2011, 117, 4623–4632. [Google Scholar] [CrossRef]
- Ogino, S.; Nosho, K.; Kirkner, G.J.; Kawasaki, T.; Meyerhardt, J.A.; Loda, M.; Giovannucci, E.L.; Fuchs, C.S. CpG island methylator phenotype, microsatellite instability, BRAF mutation and clinical outcome in colon cancer. Gut 2009, 58, 90–96. [Google Scholar] [CrossRef]
- Ogino, S.; Meyerhardt, J.A.; Irahara, N.; Niedzwiecki, D.; Hollis, D.; Saltz, L.B.; Mayer, R.J.; Schaefer, P.; Whittom, R.; Hantel, A.; et al. KRAS mutation in stage III colon cancer and clinical outcome following intergroup trial CALGB 89803. Clin. Cancer Res. 2009, 15, 7322–7329. [Google Scholar] [CrossRef]
- Chouhan, H.; Sammour, T.; L Thomas, M.; W Moore, J. Prognostic significance of BRAF mutation alone and in combination with microsatellite instability in stage III colon cancer. Asia Pac. J. Clin. Oncol. 2019, 15, 69–74. [Google Scholar] [CrossRef]
- Lin, Y.-L.; Liang, Y.-H.; Tsai, J.-H.; Liau, J.-Y.; Liang, J.-T.; Lin, B.-R.; Hung, J.-S.; Lin, L.-I.; Tseng, L.-H.; Chang, Y.-L.; et al. Oxaliplatin-Based Chemotherapy Is More Beneficial in KRAS Mutant than in KRAS Wild-Type Metastatic Colorectal Cancer Patients. PLoS ONE 2014, 9, e86789. [Google Scholar] [CrossRef] [PubMed]
- Cui, D.; Cao, D.; Yang, Y.; Qiu, M.; Huang, Y.; Yi, C. Effect of BRAF V600E mutation on tumor response of anti-EGFR monoclonal antibodies for first-line metastatic colorectal cancer treatment: A meta-analysis of randomized studies. Mol. Biol. Rep. 2014, 41, 1291–1298. [Google Scholar] [CrossRef] [PubMed]
- Loriot, Y.; Mordant, P.; Deutsch, E.; Olaussen, K.A.; Soria, J.-C. Are RAS mutations predictive markers of resistance to standard chemotherapy? Nat. Rev. Clin. Oncol. 2009, 6, 528–534. [Google Scholar] [CrossRef] [PubMed]
- Grassadonia, A.; Di Marino, P.; Ficorella, C.; Cortellini, A.; Cannita, K.; Parisi, A.; Gamucci, T.; Zoratto, F.; Vici, P.; Barba, M.; et al. Impact of primary tumor location in patients with RAS wild-type metastatic colon cancer treated with first-line chemotherapy plus anti-EGFR or anti-VEGF monoclonal antibodies: A retrospective multicenter study. J. Cancer 2019, 10, 5926–5934. [Google Scholar] [CrossRef]
- Benavides, M.; Díaz-Rubio, E.; Carrato, A.; Abad, A.; Guillén, C.; Garcia-Alfonso, P.; Gil, S.; Cano, M.T.; Safont, M.J.; Gravalos, C.; et al. Tumour location and efficacy of first-line EGFR inhibitors in KRAS/RAS wild-type metastatic colorectal cancer: Retrospective analyses of two phase II randomised Spanish TTD trials. ESMO Open 2019, 4, e000599. [Google Scholar] [CrossRef]
- Jackson, S.E.; Chester, J.D. Personalised cancer medicine. Int. J. Cancer 2015, 137, 262–266. [Google Scholar] [CrossRef] [PubMed]
- Van Cutsem, E.; Cervantes, A.; Adam, R.; Sobrero, A.; Van Krieken, J.H.; Aderka, D.; Aranda Aguilar, E.; Bardelli, A.; Benson, A.; Bodoky, G.; et al. ESMO consensus guidelines for the management of patients with metastatic colorectal cancer. Ann. Oncol. 2016, 27, 1386–1422. [Google Scholar] [CrossRef]
- Sorich, M.J.; Wiese, M.D.; Rowland, A.; Kichenadasse, G.; McKinnon, R.A.; Karapetis, C.S. Extended RAS mutations and anti-EGFR monoclonal antibody survival benefit in metastatic colorectal cancer: A meta-analysis of randomized, controlled trials. Ann. Oncol. 2015, 26, 13–21. [Google Scholar] [CrossRef]
- Van Brummelen, E.M.J.; de Boer, A.; Beijnen, J.H.; Schellens, J.H.M. BRAF Mutations as Predictive Biomarker for Response to Anti-EGFR Monoclonal Antibodies. Oncologist 2017, 22, 864–872. [Google Scholar] [CrossRef]
- Pietrantonio, F.; Petrelli, F.; Coinu, A.; Di Bartolomeo, M.; Borgonovo, K.; Maggi, C.; Cabiddu, M.; Iacovelli, R.; Bossi, I.; Lonati, V.; et al. Predictive role of BRAF mutations in patients with advanced colorectal cancer receiving cetuximab and panitumumab: A meta-analysis. Eur. J. Cancer 2015, 51, 587–594. [Google Scholar] [CrossRef]
- Rossi, L.; Vakiarou, F.; Zoratto, F.; Bianchi, L.; Papa, A.; Basso, E.; Verrico, M.; Lo Russo, G.; Evangelista, S.; Rinaldi, G.; et al. Factors influencing choice of chemotherapy in metastatic colorectal cancer (mCRC). Cancer Manag. Res. 2013, 5, 377–385. [Google Scholar] [CrossRef][Green Version]
- Stein, A.; Bokemeyer, C. How to select the optimal treatment for first line metastatic colorectal cancer. World J. Gastroenterol. 2014, 20, 899–907. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.-L.; Liau, J.-Y.; Yu, S.-C.; Ou, D.-L.; Lin, L.-I.; Tseng, L.-H.; Chang, Y.-L.; Yeh, K.-H.; Cheng, A.-L. KRAS mutation is a predictor of oxaliplatin sensitivity in colon cancer cells. PLoS ONE 2012, 7, e50701. [Google Scholar] [CrossRef]
- Ergun, Y.; Acikgoz, Y.; Bal, O.; Ucar, G.; Dirikoc, M.; Caliskan Yildirim, E.; Akdeniz, N.; Uncu, D. KRAS codon 12 and 13 mutations may guide the selection of irinotecan or oxaliplatin in first-line treatment of metastatic colorectal cancer. Expert Rev. Mol. Diagn. 2019, 19, 1131–1140. [Google Scholar] [CrossRef]
- Cabart, M.; Frénel, J.-S.; Campion, L.; Ramée, J.-F.; Dupuis, O.; Senellart, H.; Hiret, S.; Douillard, J.-Y.; Bennouna, J. KRAS mutation does not influence oxaliplatin or irinotecan efficacy, in association with bevacizumab, in first line treatment of metastatic colorectal cancer]. Bull. Cancer 2016, 103, 541–551. [Google Scholar] [CrossRef] [PubMed]
- Nemunaitis, J.; Cox, J.; Meyer, W.; Courtney, A.; Mues, G. Irinotecan hydrochloride (CPT-11) resistance identified by K-ras mutation in patients with progressive colon cancer after treatment with 5-fluorouracil (5-FU). Am. J. Clin. Oncol. 1997, 20, 527–529. [Google Scholar] [CrossRef] [PubMed]
- Hutchins, G.; Southward, K.; Handley, K.; Magill, L.; Beaumont, C.; Stahlschmidt, J.; Richman, S.; Chambers, P.; Seymour, M.; Kerr, D.; et al. Value of Mismatch Repair, KRAS, and BRAF Mutations in Predicting Recurrence and Benefits From Chemotherapy in Colorectal Cancer. JCO 2011, 29, 1261–1270. [Google Scholar] [CrossRef] [PubMed]
- Jones, R.P.; Sutton, P.A.; Evans, J.P.; Clifford, R.; McAvoy, A.; Lewis, J.; Rousseau, A.; Mountford, R.; McWhirter, D.; Malik, H.Z. Specific mutations in KRAS codon 12 are associated with worse overall survival in patients with advanced and recurrent colorectal cancer. Br. J. Cancer 2017, 116, 923–929. [Google Scholar] [CrossRef]
- Lièvre, A.; Bachet, J.-B.; Boige, V.; Cayre, A.; Le Corre, D.; Buc, E.; Ychou, M.; Bouché, O.; Landi, B.; Louvet, C.; et al. KRAS Mutations as an Independent Prognostic Factor in Patients With Advanced Colorectal Cancer Treated With Cetuximab. JCO 2008, 26, 374–379. [Google Scholar] [CrossRef]
- Conlin, A.; Smith, G.; Carey, F.A.; Wolf, C.R.; Steele, R.J.C. The prognostic significance of K-ras, p53, and APC mutations in colorectal carcinoma. Gut 2005, 54, 1283–1286. [Google Scholar] [CrossRef]
- Kwak, M.S.; Cha, J.M.; Yoon, J.Y.; Jeon, J.W.; Shin, H.P.; Chang, H.J.; Kim, H.K.; Joo, K.R.; Lee, J.I. Prognostic value of KRAS codon 13 gene mutation for overall survival in colorectal cancer. Medicine 2017, 96, 7882. [Google Scholar] [CrossRef] [PubMed]
- Rose, J.S.; Serna, D.S.; Martin, L.K.; Li, X.; Weatherby, L.M.; Abdel-Misih, S.; Zhao, W.; Bekaii-Saab, T. Influence of KRAS Mutation Status in Metachronous and Synchronous Metastatic Colorectal Adenocarcinoma. Cancer 2012, 118, 6243–6252. [Google Scholar] [CrossRef] [PubMed]
- Won, D.D.; Lee, J.I.; Lee, I.K.; Oh, S.-T.; Jung, E.S.; Lee, S.H. The prognostic significance of KRAS and BRAF mutation status in Korean colorectal cancer patients. BMC Cancer 2017, 17, 403. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.-H.; Ahn, J.; Park, W.S.; Choe, E.K.; Kim, E.; Shin, R.; Heo, S.C.; Jung, S.; Kim, K.; Chai, Y.J.; et al. Colorectal Cancer Prognosis Is Not Associated with BRAF and KRAS Mutations-A STROBE Compliant Study. J. Clin. Med. 2019, 8, 111. [Google Scholar] [CrossRef]
- Price, T.J.; Hardingham, J.E.; Lee, C.K.; Weickhardt, A.; Townsend, A.R.; Wrin, J.W.; Chua, A.; Shivasami, A.; Cummins, M.M.; Murone, C.; et al. Impact of KRAS and BRAF Gene Mutation Status on Outcomes From the Phase III AGITG MAX Trial of Capecitabine Alone or in Combination With Bevacizumab and Mitomycin in Advanced Colorectal Cancer. J. Clin. Oncol. 2011, 29, 2675–2682. [Google Scholar] [CrossRef]
- Hayama, T.; Hashiguchi, Y.; Okamoto, K.; Okada, Y.; Ono, K.; Shimada, R.; Ozawa, T.; Toyoda, T.; Tsuchiya, T.; Iinuma, H.; et al. G12V and G12C mutations in the gene KRAS are associated with a poorer prognosis in primary colorectal cancer. Int. J. Colorectal Dis. 2019, 34, 1491–1496. [Google Scholar] [CrossRef]
- Li, W.; Liu, Y.; Cai, S.; Yang, C.; Lin, Z.; Zhou, L.; Liu, L.; Zeng, W. Not all mutations of KRAS predict poor prognosis in patients with colorectal cancer. Int. J. Clin. Exp. Pathol. 2019, 12, 957–967. [Google Scholar]
- Loupakis, F.; Ruzzo, A.; Cremolini, C.; Vincenzi, B.; Salvatore, L.; Santini, D.; Masi, G.; Stasi, I.; Canestrari, E.; Rulli, E.; et al. KRAS codon 61, 146 and BRAF mutations predict resistance to cetuximab plus irinotecan in KRAS codon 12 and 13 wild-type metastatic colorectal cancer. Br. J. Cancer 2009, 101, 715–721. [Google Scholar] [CrossRef]
- Takahashi, N.; Yamada, Y.; Taniguchi, H.; Akiyoshi, K.; Honma, Y.; Iwasa, S.; Kato, K.; Hamaguchi, T.; Shimada, Y. Mutations in NRAS codon 61, KRAS codon 146, and BRAF V600E as prognostic factors in patients who received anti-EGFR antibody for metastatic colorectal cancer. JCO 2012, 30, e14126. [Google Scholar] [CrossRef]
- Imamura, Y.; Lochhead, P.; Yamauchi, M.; Kuchiba, A.; Qian, Z.R.; Liao, X.; Nishihara, R.; Jung, S.; Wu, K.; Nosho, K.; et al. Analyses of clinicopathological, molecular, and prognostic associations of KRAS codon 61 and codon 146 mutations in colorectal cancer: Cohort study and literature review. Mol. Cancer 2014, 13, 135. [Google Scholar] [CrossRef]
- Slebos, R.J.; Kibbelaar, R.E.; Dalesio, O.; Kooistra, A.; Stam, J.; Meijer, C.J.; Wagenaar, S.S.; Vanderschueren, R.G.; van Zandwijk, N.; Mooi, W.J. K-ras oncogene activation as a prognostic marker in adenocarcinoma of the lung. N. Eng. J. Med. 1990, 323, 561–565. [Google Scholar] [CrossRef] [PubMed]
- Pao, W.; Wang, T.Y.; Riely, G.J.; Miller, V.A.; Pan, Q.; Ladanyi, M.; Zakowski, M.F.; Heelan, R.T.; Kris, M.G.; Varmus, H.E. KRAS Mutations and Primary Resistance of Lung Adenocarcinomas to Gefitinib or Erlotinib. PLoS Med. 2005, 2, e17. [Google Scholar] [CrossRef]
- Tveit, K.M.; Guren, T.; Glimelius, B.; Pfeiffer, P.; Sorbye, H.; Pyrhonen, S.; Sigurdsson, F.; Kure, E.; Ikdahl, T.; Skovlund, E.; et al. Phase III trial of cetuximab with continuous or intermittent fluorouracil, leucovorin, and oxaliplatin (Nordic FLOX) versus FLOX alone in first-line treatment of metastatic colorectal cancer: The NORDIC-VII study. J. Clin. Oncol. 2012, 30, 1755–1762. [Google Scholar] [CrossRef] [PubMed]
- Venderbosch, S.; Nagtegaal, I.D.; Maughan, T.S.; Smith, C.G.; Cheadle, J.P.; Fisher, D.; Kaplan, R.; Quirke, P.; Seymour, M.T.; Richman, S.D.; et al. Mismatch repair status and BRAF mutation status in metastatic colorectal cancer patients: A pooled analysis of the CAIRO, CAIRO2, COIN, and FOCUS studies. Clin. Cancer Res. 2014, 20, 5322–5330. [Google Scholar] [CrossRef] [PubMed]
- Van Cutsem, E.; Köhne, C.-H.; Láng, I.; Folprecht, G.; Nowacki, M.P.; Cascinu, S.; Shchepotin, I.; Maurel, J.; Cunningham, D.; Tejpar, S.; et al. Cetuximab plus irinotecan, fluorouracil, and leucovorin as first-line treatment for metastatic colorectal cancer: Updated analysis of overall survival according to tumor KRAS and BRAF mutation status. J. Clin. Oncol. 2011, 29, 2011–2019. [Google Scholar] [CrossRef] [PubMed]
- Hugdahl, E.; Kalvenes, M.B.; Puntervoll, H.E.; Ladstein, R.G.; Akslen, L.A. BRAF-V600E expression in primary nodular melanoma is associated with aggressive tumour features and reduced survival. Br. J. Cancer 2016, 114, 801–808. [Google Scholar] [CrossRef]
- Xing, M.; Alzahrani, A.S.; Carson, K.A.; Shong, Y.K.; Kim, T.Y.; Viola, D.; Elisei, R.; Bendlová, B.; Yip, L.; Mian, C.; et al. Association Between BRAF V600E Mutation and Recurrence of Papillary Thyroid Cancer. J. Clin. Oncol. 2015, 33, 42–50. [Google Scholar] [CrossRef]
- Carnerero Córdoba, L.; González Cebrián, I.; Rodríguez González, C.; González-Flores, E.; Conde, V.; Delgado Ureña, M.; Jurado García, J.; González-Astorga, B. Clinical significance of BRAF mutations in colorectal cancer: A retrospective study of one institution in a real-life population. Ann. Oncol. 2019, 30, 389. [Google Scholar] [CrossRef]
- Chiu, J.W.; Krzyzanowska, M.K.; Serra, S.; Knox, J.J.; Dhani, N.C.; Mackay, H.; Hedley, D.; Moore, M.; Liu, G.; Burkes, R.L.; et al. Molecular Profiling of Patients With Advanced Colorectal Cancer: Princess Margaret Cancer Centre Experience. Clin. Colorectal Cancer 2018, 17, 73–79. [Google Scholar] [CrossRef]
- Van Cutsem, E.; Huijberts, S.; Grothey, A.; Yaeger, R.; Cuyle, P.-J.; Elez, E.; Fakih, M.; Montagut, C.; Peeters, M.; Yoshino, T.; et al. Binimetinib, Encorafenib, and Cetuximab Triplet Therapy for Patients With BRAF V600E–Mutant Metastatic Colorectal Cancer: Safety Lead-In Results From the Phase III BEACON Colorectal Cancer Study. JCO 2019, 37, 1460–1469. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | N (%) | Characteristics | N (%) |
|---|---|---|---|
| Median age (range) | 68 years (24–93) | 1st line treatment response | |
| Gender | CR or PR | 94 (16.8%) | |
| Female | 224 (39.9%) | SD or PD | 186 (33.2%) |
| Male | 337 (60.1%) | N/A | 281 (50.0%) |
| Localization of primary tumor | Number of metastatic sites | ||
| Right colon | 158 (28.2%) | 1 | 394 (70.2%) |
| Left colon | 395 (70.4%) | >1 | 153 (27.3%) |
| N/A | 8 (1.4%) | N/A | 14 (2.5%) |
| Metastatic pattern | Liver metastasis | ||
| Metachronous | 237 (42.2%) | No | 185 (33.0%) |
| Synchronous | 323 (57.6%) | Yes | 375 (66.8%) |
| N/A | 1 (0.2%) | N/A | 1 (0.2%) |
| Differentiation grade | Lung metastasis | ||
| G1 | 86 (15.3%) | No | 372 (66.3%) |
| G2 | 381 (67.9%) | Yes | 187 (33.3%) |
| G3 | 53 (9.5%) | N/A | 2 (0.4%) |
| N/A | 41 (7.3%) | Lymph nodes metastasis | |
| ECOG | No | 423 (75.4%) | |
| 0 | 167 (29.8%) | Yes | 137 (24.4%) |
| 1 | 248 (44.2%) | N/A | 1 (0.2%) |
| 2 | 88 (15.7%) | Peritoneal metastasis | |
| 3 | 46 (8.2%) | No | 424 (75.6%) |
| N/A | 12 (2.1%) | Yes | 136 (24.2%) |
| Metastatic 1st backbone | N/A | 1 (0.2%) | |
| Oxaliplatin-based | 163 (29.1%) | KRAS mutational status | |
| Irinotecan-based | 74 (13.2%) | Wild-type | 254 (45.3%) |
| Fluoropyrimidines | 70 (12.5%) | Mutated in 12/13 | 259 (46.2%) |
| Other | 12 (2.1%) | Mutated in 61 | 19 (3.4%) |
| None | 242 (43.1%) | N/A | 29 (5.1%) |
| Metastatic 1st biologic | BRAF mutational status | ||
| None | 458 (81.6%) | Wild-type | 519 (92.5%) |
| Cetuximab | 39 (7.0%) | V600E Mutated | 34 (6.1%) |
| Bevacizumab | 64 (11.4%) | N/A | 8 (1.4%) |
| Clinico-Pathological Feature | KRAS Wt | KRAS Mut | p-Value | BRAF Wt | BRAF Mut | p-Value |
|---|---|---|---|---|---|---|
| Age (median, range) | 67.0 (27–93) | 69.0 (24–90) | 68.5 (24–93) | 63.5 (33–85) | ||
| Gender | 0.123 | 0.610 | ||||
| Male | 161 (63%) | 158 (57%) | 313 (60%) | 19 (56%) | ||
| Female | 93 (37%) | 120 (43%) | 206 (40%) | 15 (44%) | ||
| Tumor location | 0.179 | 0.000 | ||||
| Right colon | 65 (26%) | 84 (31%) | 130 (25%) | 27 (79%) | ||
| Left colon | 188 (74%) | 187 (69%) | 381 (75%) | 7 (21%) | ||
| Metastatic disease | 0.763 | 0.019 | ||||
| Metachronous | 104 (41%) | 117 (42%) | 228 (44%) | 8 (24%) | ||
| Synchronous | 150 (59%) | 160 (58%) | 290 (56%) | 26 (76%) | ||
| Grade | 0.113 | 0.098 | ||||
| G1 | 31 (13%) | 49 (19%) | 83 (17%) | 2 (7%) | ||
| G2 + G3 | 199 (87%) | 212 (81%) | 400 (83%) | 28 (93%) | ||
| ECOG | 0.005 | 0.771 | ||||
| 0/1 | 205 (82%) | 193 (71%) | 384 (76%) | 25 (74%) | ||
| 2/3 | 45 (18%) | 77 (29%) | 123 (24%) | 9 (26%) | ||
| Liver metastasis | 0.105 | 0.161 | ||||
| No | 91 (36%) | 81 (29%) | 168 (32%) | 15 (44%) | ||
| Yes | 163 (64%) | 196 (71%) | 350 (68%) | 19 (56%) | ||
| Lung metastasis | 0.400 | 0.200 | ||||
| No | 171 (68%) | 179 (64%) | 340 (66%) | 26 (76%) | ||
| Yes | 81 (32%) | 99 (36%) | 177 (34%) | 8 (24%) | ||
| Lymph nodes metastasis | 0.897 | 0.054 | ||||
| No | 194 (76%) | 210 (76%) | 396 (76%) | 21 (62%) | ||
| Yes | 60 (24%) | 67 (24%) | 122 (24%) | 13 (38%) | ||
| Peritoneal metastasis | 0.446 | 0.002 | ||||
| No | 190 (75%) | 215 (78%) | 399 (77%) | 18 (53%) | ||
| Yes | 64 (25%) | 62 (22%) | 119 (23%) | 16 (47%) | ||
| Number of metastatic sites | 0.564 | 0.483 | ||||
| 1 | 180 (73%) | 192 (71%) | 366 (72%) | 22 (67%) | ||
| >1 | 67 (27%) | 80 (29%) | 140 (28%) | 11 (33%) |
| Univariate PFS (95%CI) | ||||
|---|---|---|---|---|
| HR | Lower | Upper | p-Value | |
| Age (< vs. >68 years) | 1.137 | 0.802 | 1.612 | 0.470 |
| Gender (Female vs. Male) | 1.166 | 0.820 | 1.659 | 0.393 |
| Localization (Right colon vs. Left colon) | 1.245 | 0.840 | 1.844 | 0.275 |
| Grade | 0.757 | |||
| G1 | 1.000 | |||
| G2 | 0.859 | 0.311 | 2.370 | 0.769 |
| G3 | 1.056 | 0.428 | 2.603 | 0.906 |
| ECOG (0/1 vs. 2/3) | 1.331 | 0.775 | 2.284 | 0.300 |
| Metastatic 1st backbone | 0.301 | |||
| Oxaliplatin-based | 1.000 | |||
| Irinotecan-based | 0.914 | 0.615 | 1.360 | 0.659 |
| Fluoropyrimidines | 1.295 | 0.818 | 2.051 | 0.269 |
| Liver metastasis (No vs. Yes) | 1.691 | 1.177 | 2.432 | 0.005 |
| Lung metastasis (No vs. Yes) | 1.320 | 0.924 | 1.887 | 0.128 |
| Lymph nodes metastasis (No vs. Yes) | 1.178 | 0.809 | 1.716 | 0.393 |
| Peritoneal metastasis (No vs. Yes) | 1.333 | 0.892 | 1.991 | 0.161 |
| Number of metastasis sites (1 vs. >1) | 1.387 | 0.931 | 2.067 | 0.108 |
| KRASmutation (No vs. Yes) | 1.529 | 1.058 | 2.211 | 0.024 |
| BRAFmutation (No vs. Yes) | 4.288 | 2.033 | 9.046 | 0.000 |
| Multivariate PFS (95% CI) | ||||
| Liver metastasis (No vs. Yes) | 1.595 | 1.086 | 2.343 | 0.017 |
| KRASmutation (No vs. Yes) | 1.643 | 1.110 | 2.431 | 0.013 |
| BRAFmutation (No vs. Yes) | 5.861 | 2.531 | 13.570 | 0.000 |
| CR + PR | SD + PD | p-Value | |
|---|---|---|---|
| KRAS wild-type | 29 (38%) | 48 (62%) | |
| KRAS mutated | 18 (19%) | 75 (81%) | |
| 0.008 | |||
| BRAF wild-type | 46 (27%) | 122 (73%) | |
| BRAF mutated | 2 (22%) | 7 (78%) | |
| 0.540 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Garcia-Carbonero, N.; Martinez-Useros, J.; Li, W.; Orta, A.; Perez, N.; Carames, C.; Hernandez, T.; Moreno, I.; Serrano, G.; Garcia-Foncillas, J. KRAS and BRAF Mutations as Prognostic and Predictive Biomarkers for Standard Chemotherapy Response in Metastatic Colorectal Cancer: A Single Institutional Study. Cells 2020, 9, 219. https://doi.org/10.3390/cells9010219
Garcia-Carbonero N, Martinez-Useros J, Li W, Orta A, Perez N, Carames C, Hernandez T, Moreno I, Serrano G, Garcia-Foncillas J. KRAS and BRAF Mutations as Prognostic and Predictive Biomarkers for Standard Chemotherapy Response in Metastatic Colorectal Cancer: A Single Institutional Study. Cells. 2020; 9(1):219. https://doi.org/10.3390/cells9010219
Chicago/Turabian StyleGarcia-Carbonero, Nuria, Javier Martinez-Useros, Weiyao Li, Alberto Orta, Nuria Perez, Cristina Carames, Tatiana Hernandez, Irene Moreno, Gloria Serrano, and Jesus Garcia-Foncillas. 2020. "KRAS and BRAF Mutations as Prognostic and Predictive Biomarkers for Standard Chemotherapy Response in Metastatic Colorectal Cancer: A Single Institutional Study" Cells 9, no. 1: 219. https://doi.org/10.3390/cells9010219
APA StyleGarcia-Carbonero, N., Martinez-Useros, J., Li, W., Orta, A., Perez, N., Carames, C., Hernandez, T., Moreno, I., Serrano, G., & Garcia-Foncillas, J. (2020). KRAS and BRAF Mutations as Prognostic and Predictive Biomarkers for Standard Chemotherapy Response in Metastatic Colorectal Cancer: A Single Institutional Study. Cells, 9(1), 219. https://doi.org/10.3390/cells9010219