Mycoplasma genitalium Infection and Chronic Inflammation in Human Prostate Cancer: Detection Using Prostatectomy and Needle Biopsy Specimens

 ,
,  , , , ,
, , , , 
Abstract
1. Introduction
2. Methods
2.1. Patient Selection and Data Collection
2.2. Pathological Review of Prostate Cancer Specimens
2.3. DNA Isolation from Prostate Specimens
2.4. PCR Screening of Infectious Agents
2.5. Statistical Analysis
3. Results
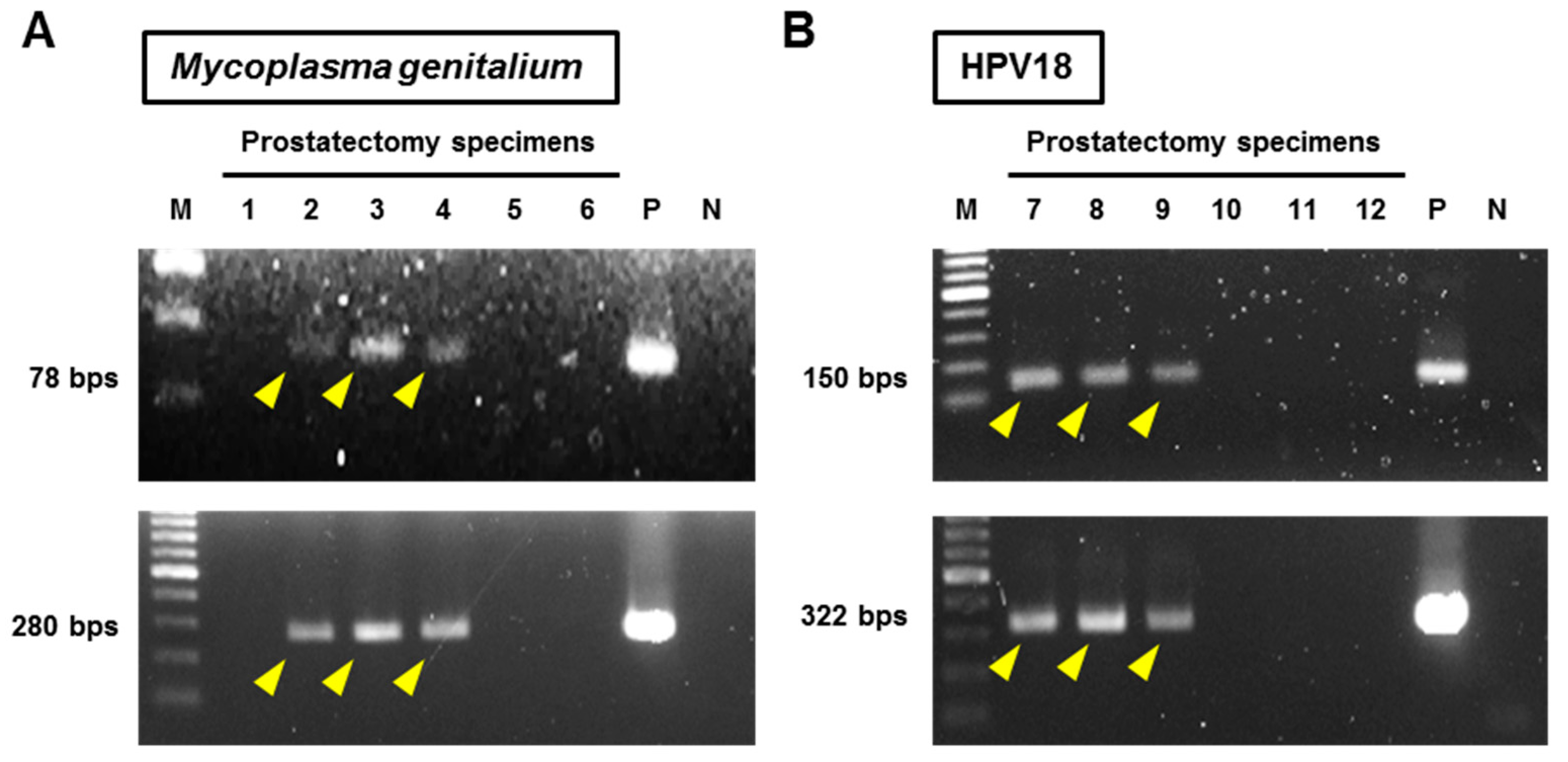
3.1. Infection Status of Prostate Surgical Specimens
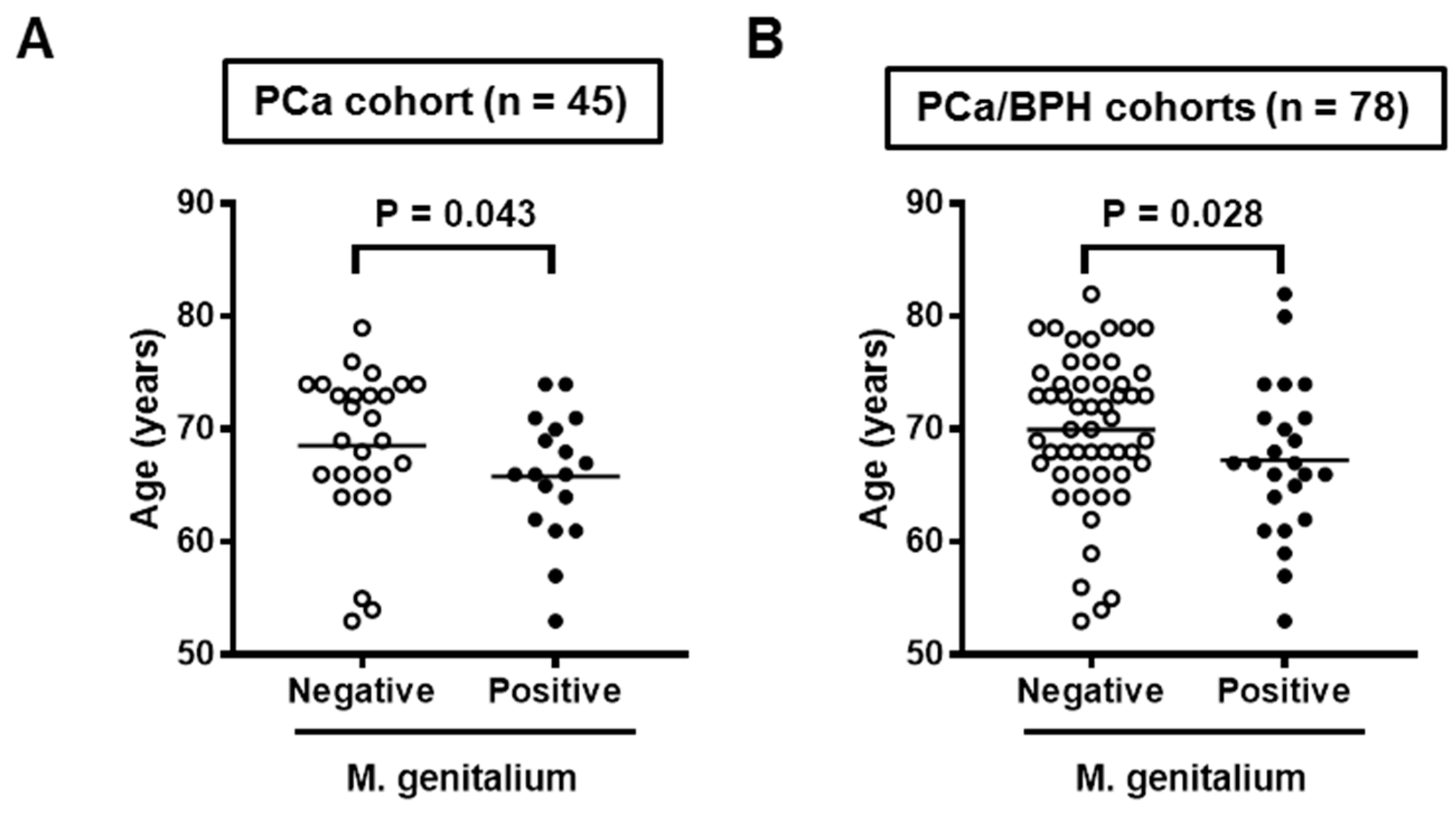
3.2. Mg Infection, Patient Background, and Prostate Inflammation in the PCa Cohort
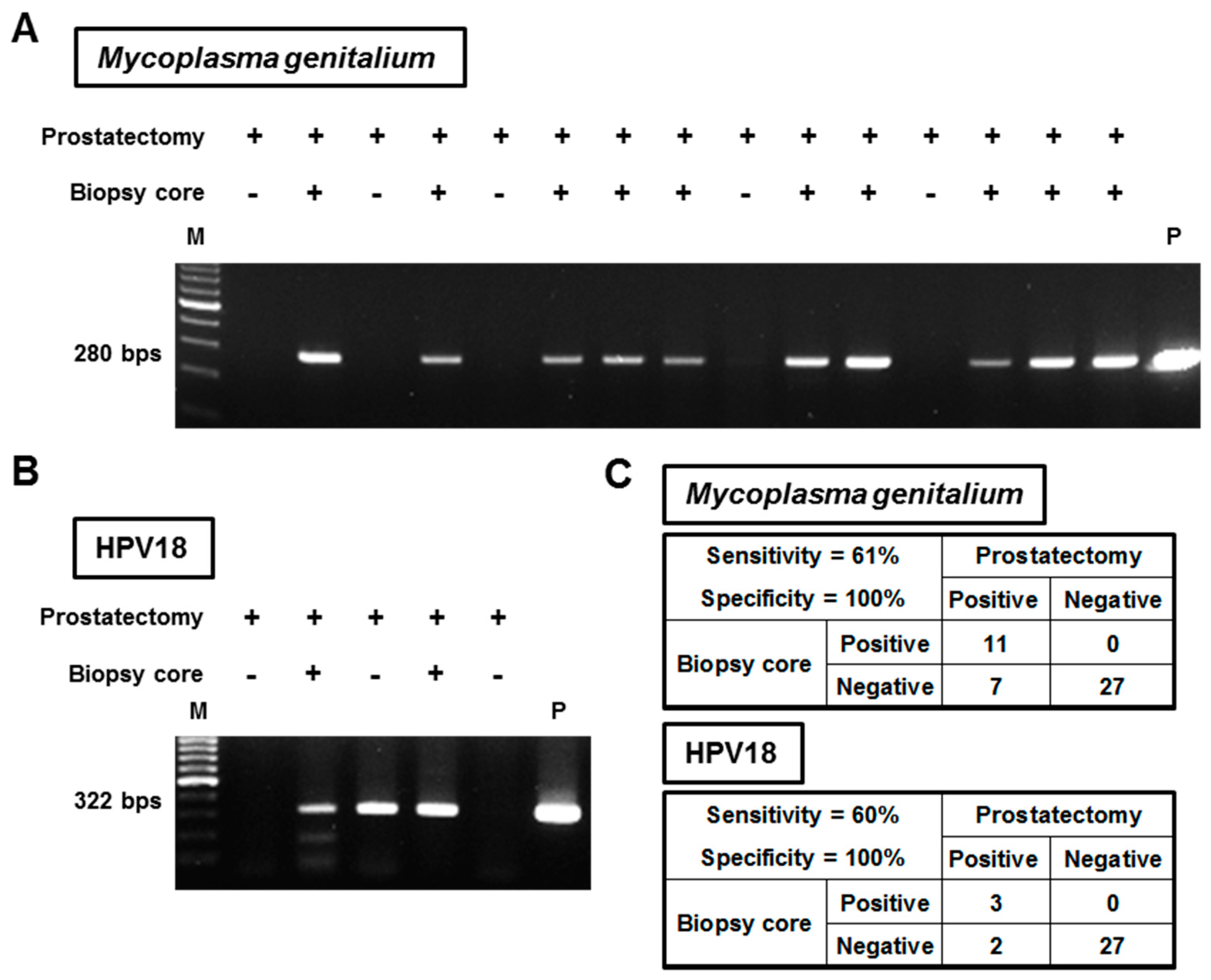
3.3. Detection Feasibility of Mg and HPVs from Prostate Needle Biopsy Specimens
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- de Martel, C.; Franceschi, S. Infections and cancer: Established associations and new hypotheses. Crit. Rev. Oncol. Hematol. 2009, 70, 183–194. [Google Scholar] [CrossRef] [PubMed]
- Ravich, A.; Ravich, R.A. Prophylaxis of cancer of the prostate, penis, and cervix by circumcision. N. Y. State J. Med. 1951, 51, 1519–1520. [Google Scholar] [PubMed]
- Taylor, M.L.; Mainous, A.G.; Wells, B.J. Prostate cancer and sexually transmitted diseases: A meta-analysis. Fam. Med. 2005, 37, 506–512. [Google Scholar] [PubMed]
- Dillner, J. The serological response to papillomaviruses. Semin. Cancer Biol. 1999, 9, 423–430. [Google Scholar] [CrossRef] [PubMed]
- Karan, D.; Dubey, S. From Inflammation to Prostate Cancer: The Role of Inflammasomes. Adv. Urol. 2016, 2016, 3140372. [Google Scholar] [CrossRef] [PubMed]
- Platz, E.A.; Kulac, I.; Barber, J.R.; Drake, C.G.; Joshu, C.E.; Nelson, W.G.; Lucia, M.S.; Klein, E.A.; Lippman, S.M.; Parnes, H.L.; et al. A Prospective Study of Chronic Inflammation in Benign Prostate Tissue and Risk of Prostate Cancer: Linked PCPT and SELECT Cohorts. Cancer Epidemiol. Biomark. Prev. 2017, 26, 1549–1557. [Google Scholar] [CrossRef] [PubMed]
- Sfanos, K.S.; Yegnasubramanian, S.; Nelson, W.G.; De Marzo, A.M. The inflammatory microenvironment and microbiome in prostate cancer development. Nat. Rev. Urol. 2018, 15, 11–24. [Google Scholar] [CrossRef] [PubMed]
- Yow, M.A.; Tabrizi, S.N.; Severi, G.; Bolton, D.M.; Pedersen, J.; Giles, G.G.; Southey, M.C. Characterisation of microbial communities within aggressive prostate cancer tissues. Infect. Agents Cancer 2017, 12, 4. [Google Scholar] [CrossRef] [PubMed]
- Cavarretta, I.; Ferrarese, R.; Cazzaniga, W.; Saita, D.; Lucianò, R.; Ceresola, E.R.; Locatelli, I.; Visconti, L.; Lavorgna, G.; Briganti, A.; et al. The Microbiome of the Prostate Tumor Microenvironment. Eur. Urol. 2017, 72, 625–631. [Google Scholar] [CrossRef] [PubMed]
- Nakai, Y.; Tanaka, N.; Anai, S.; Miyake, M.; Hori, S.; Tatsumi, Y.; Morizawa, Y.; Fujii, T.; Konishi, N.; Fujimoto, K. Transperineal template-guided saturation biopsy aimed at sampling one core for each milliliter of prostate volume: 103 cases requiring repeat prostate biopsy. BMC Urol. 2017, 17, 28. [Google Scholar] [CrossRef] [PubMed]
- Nickel, J.C.; True, L.D.; Krieger, J.N.; Berger, R.E.; Boag, A.H.; Young, I.D. Consensus development of a histopathological classification system for chronic prostatic inflammation. BJU Int. 2001, 87, 797–805. [Google Scholar] [CrossRef] [PubMed]
- Fujii, T.; Shimada, K.; Asai, O.; Tanaka, N.; Fujimoto, K.; Hirao, K.; Konishi, N. Immunohistochemical analysis of inflammatory cells in benign and precancerous lesions and carcinoma of the prostate. Pathobiology 2013, 80, 119–126. [Google Scholar] [CrossRef] [PubMed]
- Yow, M.A.; Tabrizi, S.N.; Severi, G.; Bolton, D.M.; Pedersen, J.; Longano, A.; Garland, S.M.; Southey, M.C.; Giles, G.G. Detection of infectious organisms in archival prostate cancer tissues. BMC Cancer 2014, 14, 579. [Google Scholar] [CrossRef] [PubMed]
- Namiki, K.; Goodison, S.; Porvasnik, S.; Allan, R.W.; Iczkowski, K.A.; Urbanek, C.; Reyes, L.; Sakamoto, N.; Rosser, C.J. Persistent exposure to Mycoplasma induces malignant transformation of human prostate cells. PLoS ONE 2009, 4, e6872. [Google Scholar] [CrossRef] [PubMed]
- Sotlar, K.; Diemer, D.; Dethleffs, A.; Hack, Y.; Stubner, A.; Vollmer, N.; Menton, S.; Menton, M.; Dietz, K.; Wallwiener, D.; et al. Detection and typing of human papillomavirus by e6 nested multiplex PCR. J. Clin. Microbiol. 2004, 42, 3176–3184. [Google Scholar] [CrossRef] [PubMed]
- Zarei, O.; Rezania, S.; Mousavi, A. Mycoplasma genitalium and cancer: A brief review. Asian Pac. J. Cancer Prev. 2013, 14, 3425–3428. [Google Scholar] [CrossRef] [PubMed]
- Biernat-Sudolska, M.; Szostek, S.; Rojek-Zakrzewska, D.; Klimek, M.; Kosz-Vnenchak, M. Concomitant infections with human papillomavirus and various mycoplasma and ureaplasma species in women with abnormal cervical cytology. Adv. Med. Sci. 2011, 56, 299–303. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.Y.; Zhou, L.P.; Zhang, Q. Isolation of Mycoplasma penetrans from blood and tissue specimens of patients with cervical cancer. Chin. J. Zoonose 2007, 23, 537. [Google Scholar]
- Barykova, Y.A.; Logunov, D.Y.; Shmarov, M.M.; Vinarov, A.Z.; Fiev, D.N.; Vinarova, N.A.; Rakovskaya, I.V.; Baker, P.S.; Shyshynova, I.; Stephenson, A.J.; et al. Association of Mycoplasma hominis infection with prostate cancer. Oncotarget 2011, 2, 289–297. [Google Scholar] [CrossRef] [PubMed]
- Baracaldo, R.; Foltzer, M.; Patel, R.; Bourbeau, P. Empyema caused by Mycoplasma salivarium. J. Clin. Microbiol. 2012, 50, 1805–1806. [Google Scholar] [CrossRef] [PubMed]
- Ketcham, C.M.; Anai, S.; Reutzel, R.; Sheng, S.; Schuster, S.M.; Brenes, R.B.; Agbandje-McKenna, M.; McKenna, R.; Rosser, C.J.; Boehlein, S.K. p37 Induces tumor invasiveness. Mol. Cancer Ther. 2005, 4, 1031–1038. [Google Scholar] [CrossRef] [PubMed]
- Goodison, S.; Nakamura, K.; Iczkowski, K.A.; Anai, S.; Boehlein, S.K.; Rosser, C.J. Exogenous mycoplasma p37 protein alters gene expression, growth and morphology of prostate cancer cells. Cytogenet. Genome Res. 2007, 118, 204–213. [Google Scholar] [CrossRef] [PubMed]
- Feng, S.H.; Tsai, S.; Rodriguez, J.; Lo, S.C. Mycoplasmal infections prevent apoptosis and induce malignant transformation of interleukin-3-dependent 32D hematopoietic cells. Mol. Cell. Biol. 1999, 19, 7995–8002. [Google Scholar] [CrossRef] [PubMed]
- Casey, G.; Neville, P.J.; Plummer, S.J.; Xiang, Y.; Krumroy, L.M.; Klein, E.A.; Catalona, W.J.; Nupponen, N.; Carpten, J.D.; Trent, J.M.; et al. RNASEL Arg462Gln variant is implicated in up to 13% of prostate cancer cases. Nat. Genet. 2002, 32, 581–583. [Google Scholar] [CrossRef] [PubMed]
- Panguluri, R.C.; Long, L.O.; Chen, W.; Wang, S.; Coulibaly, A.; Ukoli, F.; Jackson, A.; Weinrich, S.; Ahaghotu, C.; Isaacs, W.; et al. COX-2 gene promoter haplotypes and prostate cancer risk. Carcinogenesis 2004, 25, 961–966. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.C.; Giovannucci, E.; Lazarus, R.; Kraft, P.; Ketkar, S.; Hunter, D.J. Sequence variants of Toll-like receptor 4 and susceptibility to prostate cancer. Cancer Res. 2005, 65, 11771–11778. [Google Scholar] [CrossRef] [PubMed]
- Yu, H.; Meng, H.; Zhou, F.; Ni, X.; Shen, S.; Das, U.N. Urinary microbiota in patients with prostate cancer and benign prostatic hyperplasia. Arch. Med. Sci. 2015, 11, 385–394. [Google Scholar] [CrossRef] [PubMed]
- Fukase, K.; Kato, M.; Kikuchi, S.; Inoue, K.; Uemura, N.; Okamoto, S.; Terao, S.; Amagai, K.; Hayashi, S.; Asaka, M. Effect of eradication of Helicobacter pylori on incidence of metachronous gastric carcinoma after endoscopic resection of early gastric cancer: An open-label, randomised controlled trial. Lancet 2008, 372, 392–397. [Google Scholar] [CrossRef]
- Printz, C. FDA approves Gardasil 9 for more types of HPV. Cancer 2015, 121, 1156–1157. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Target Organism | Primer Sequence (5’ to 3’) | Annealing T (°C) | Product Size (bps) | |
|---|---|---|---|---|
| Neisseria gonorrhoeae | Forward | GCGACGTCATCGGTAAATACC | 60 | 68 |
| Reverse | CGCCATACGGACGATGGT | |||
| Chlamydia trachomatis | Forward | TGATGTATCCAGCCCAAATGC | 50 | 81 |
| Reverse | AATCCAGTTCTTCTCTGCCTCTCTAC | |||
| Mycoplasma genitalium (short amplicon) | Forward | GAGAAATACCTTGATGGTCAGCAA | 60 | 78 |
| Reverse | GTTAATATCATATAAAGCTCTACCGTTGTTATC | |||
| Mycoplasma genitalium (long amplicon) | Forward | AGTTGATGAAACCTTAACCCCTTGG | 60 | 280 |
| Reverse | CCGTTGAGGGGTTTTCCATTTTTGC | |||
| Mycoplasma hyorhinis | Forward | GATCACATTTCCACTTATTTGAAACA | 60 | 460 |
| Reverse | AAACGACGTCCATAAGCAACTTTA | |||
| Ureaplasma urealyticum | Forward | ACACCATGGGAGCTGGTAAT | 60 | 100 |
| Reverse | CTTCTCGACTTTCAGA | |||
| HPV MY09/MY11 | Forward | CGTCCMARRGGAWACTGATC | 60 | 450 |
| Reverse | GCMCAGGGWCATAAYAATGG | |||
| HPV GP5+/GP6+ | Forward | TTTGTTACTGTGGTAGATACTAC | 50 | 150 |
| Reverse | GAAAAATAAACTGTAAATCATAT | |||
| HPV16 | Forward | CACAGTTATGCACAGAGCTGC | 60 | 457 |
| Reverse | CATATATTCATGCAATGTAGGTGTA | |||
| HPV18 | Forward | CACTTCACTGCAAGACATAGA | 60 | 322 |
| Reverse | GTTGTGAAATCGTCGTTTTTCA | |||
| human b-actin | Forward | TGAGCGCGGCTACAGCTT | 60 | 60 |
| Reverse | TCCTTAATGTCACGCACGATTT | |||
| Target Organism | PCa (RALP) n = 45 | BPH (TURP) n = 33 | P Value |
|---|---|---|---|
| Age (years old) at Surgery | 67.5 ± 6.3 | 71.4 ± 6.9 | 0.01 |
| Neisseria gonorrhoeae | 0 | 0 | NA |
| Chlamydia trachomatis | 0 | 0 | NA |
| Mycoplasma genitalium | 18 (40%) | 6 (18%) | 0.03 |
| Mycoplasma hyorhinis | 0 | 0 | NA |
| Ureaplasma urealyticum | 0 | 0 | NA |
| HPV16 | 1 (2%) † | 0 | 0.39 |
| HPV18 | 5 (11%) † | 2 (6%) | 0.44 |
| Variables | Total (n = 45) | Mycoplasma genitalium | P Value | ||
|---|---|---|---|---|---|
| Negative (n = 27) | Positive (n = 18) | ||||
| Age (years) at RALP | mean ± SD | 67.5 ± 6.3 | 68.6 ± 6.7 | 65.8 ± 5.6 | 0.043 |
| median (range) | 68 (53–79) | 68 (53–79) | 66 (53–74) | ||
| initial PSA (ng/mL) | mean ± SD | 13.3 ± 13.1 | 13.2 ± 12.1 | 13.5 ± 14.8 | 0.85 |
| median (range) | 7.6 (3.8–61.3) | 7.6 (3.8–48.8) | 6.9 (4.2–61.3) | ||
| Preoperative urine WBC (/mL) | mean ± SD | 11.9 ± 34.2 | 13.2 ± 39.6 | 9.6 ± 22.4 | 0.93 |
| median (range) | 1.9 (0.3–199) | 1.9 (1.3–199) | 1.9 (0.3–88.6) | ||
| Preoperative IPSS | mean ± SD | 11.0 ± 7.6 | 10.5 ± 6.7 | 11.7 ± 8.7 | 0.93 |
| median (range) | 10 (1–31) | 9 (1–26) | 11 (2–31) | ||
| Hypertention | No | 24 (53%) | 17 (63%) | 7 (39%) | 0.11 |
| Yes | 21 (47%) | 10 (37%) | 11 (61%) | ||
| Diabetes mellitus | No | 39 (87%) | 24 (89%) | 15 (83%) | 0.59 |
| Yes | 6 (13%) | 3 (11%) | 3 (17%) | ||
| Prostatectomy Gleason score | 3 + 4 | 19 (42%) | 10 (37%) | 9 (50%) | 0.68 |
| 4 + 3 | 18 (40%) | 12 (44%) | 6 (33%) | ||
| 4 + 4/4 + 5 | 8 (18%) | 5 (19%) | 3 (17%) | ||
| Prostatectomy T category | pT2a | 15 (33%) | 12 (44%) | 3 (17%) | 0.027 † |
| pT2b | 4 (9%) | 3 (11%) | 1 (6%) | ||
| pT2c | 12 (27%) | 4 (15%) | 8 (44%) | ||
| pT3a | 10 (22%) | 5 (19%) | 5 (28%) | ||
| pT3b | 4 (9%) | 3 (11%) | 1 (6%) | ||
| Inflammation of peri-tumoral area | None | 17 (38%) | 10 (37%) | 7 (39%) | 0.58 |
| Mild | 23 (51%) | 15 (56%) | 8 (44%) | ||
| Moderate | 2 (4%) | 2 (7%) | 2 (11%) | ||
| Severe | 1 (2%) | 0 (0%) | 1 (6%) | ||
| Inflammation of non-tumoral area | None | 14 (31%) | 11 (41%) | 3 (17%) | 0.21 |
| Mild | 23 (51%) | 13 (48%) | 10 (56%) | ||
| Moderate | 7 (16%) | 3 (11%) | 4 (22%) | ||
| Severe | 1 (2%) | 0 (0%) | 1 (6%) | ||
| PIA | No | 44 (98%) | 26 (96%) | 18 (100%) | 0.82 |
| Present | 1 (2%) | 1 (4%) | 0 (0%) | ||
| HGPIN | No | 43 (96%) | 25 (93%) | 18 (100%) | 0.23 |
| Present | 2 (4%) | 2 (7%) | 0 (0%) | ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miyake, M.; Ohnishi, K.; Hori, S.; Nakano, A.; Nakano, R.; Yano, H.; Ohnishi, S.; Owari, T.; Morizawa, Y.; Itami, Y.; et al. Mycoplasma genitalium Infection and Chronic Inflammation in Human Prostate Cancer: Detection Using Prostatectomy and Needle Biopsy Specimens. Cells 2019, 8, 212. https://doi.org/10.3390/cells8030212
Miyake M, Ohnishi K, Hori S, Nakano A, Nakano R, Yano H, Ohnishi S, Owari T, Morizawa Y, Itami Y, et al. Mycoplasma genitalium Infection and Chronic Inflammation in Human Prostate Cancer: Detection Using Prostatectomy and Needle Biopsy Specimens. Cells. 2019; 8(3):212. https://doi.org/10.3390/cells8030212
Chicago/Turabian StyleMiyake, Makito, Kenta Ohnishi, Shunta Hori, Akiyo Nakano, Ryuichi Nakano, Hisakazu Yano, Sayuri Ohnishi, Takuya Owari, Yosuke Morizawa, Yoshitaka Itami, and et al. 2019. "Mycoplasma genitalium Infection and Chronic Inflammation in Human Prostate Cancer: Detection Using Prostatectomy and Needle Biopsy Specimens" Cells 8, no. 3: 212. https://doi.org/10.3390/cells8030212
APA StyleMiyake, M., Ohnishi, K., Hori, S., Nakano, A., Nakano, R., Yano, H., Ohnishi, S., Owari, T., Morizawa, Y., Itami, Y., Nakai, Y., Inoue, T., Anai, S., Torimoto, K., Tanaka, N., Fujii, T., Furuya, H., Rosser, C. J., & Fujimoto, K. (2019). Mycoplasma genitalium Infection and Chronic Inflammation in Human Prostate Cancer: Detection Using Prostatectomy and Needle Biopsy Specimens. Cells, 8(3), 212. https://doi.org/10.3390/cells8030212