
Neoadjuvant Intratumoral Immunotherapy with Cowpea Mosaic Virus Induces Local and Systemic Antitumor Efficacy in Canine Mammary Cancer Patients

 , , , , , , ,
, , , , , , ,  , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Canine Patient Recruitment and Selection Criteria
2.2. eCPMV Immunotherapy Treatment Protocol
2.3. Quality of Life (QOL) and Tumor Response Evaluation
2.4. Hematological, Biochemical, Flow Cytometry, and Cytokine Analyses
2.5. Detection of Anti-eCPMV Antibodies in Canine Plasma
2.6. Histopathology and Immunohistochemistry (IHC) Assays
2.7. RNA Analyses
2.8. Statistical Analyses
3. Results
3.1. Epidemiological and Clinico-Pathological Characteristics of CMC Patients
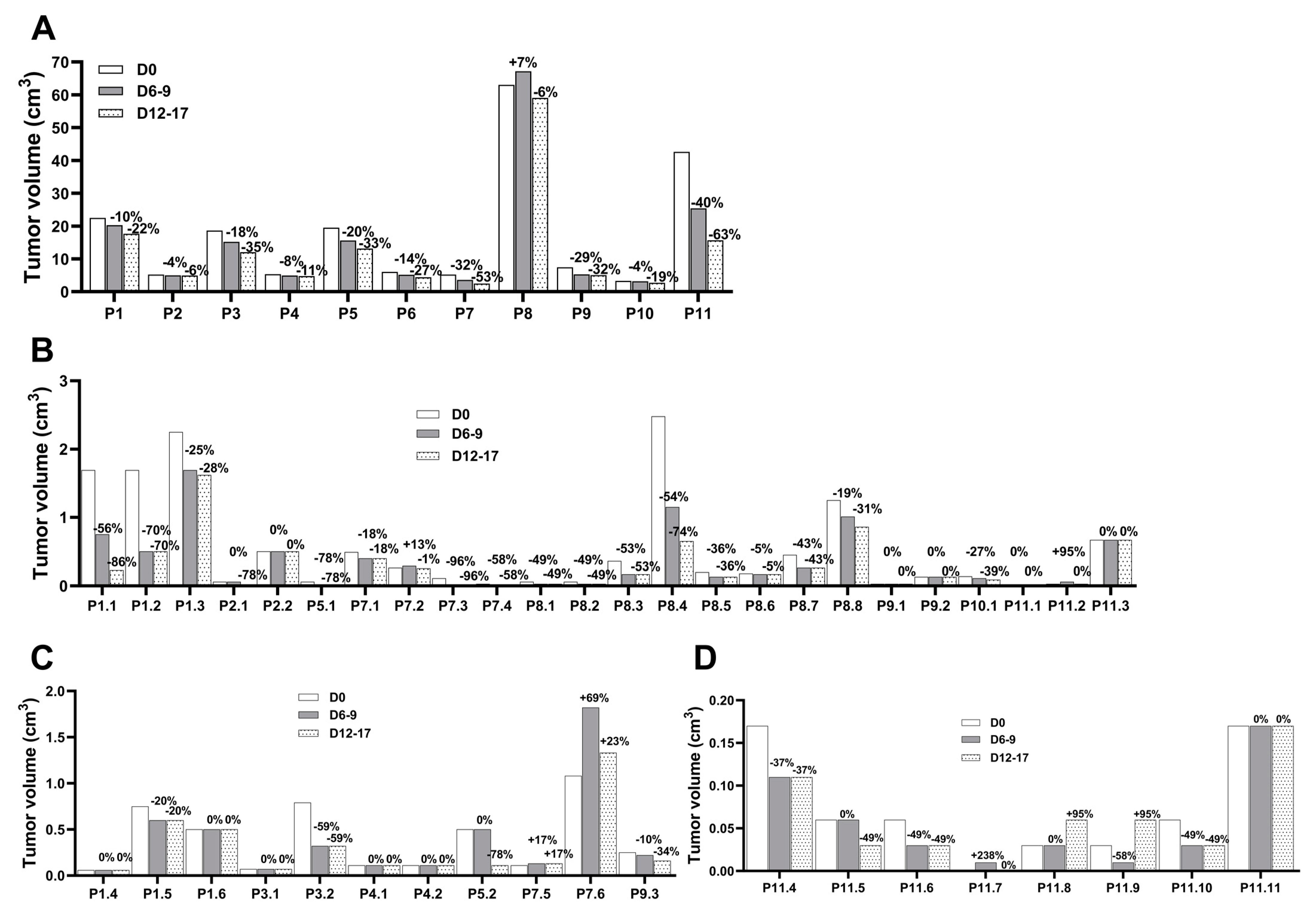
3.2. eCPMV Immunotherapy Induces Tumor Reduction in Injected and Noninjected CMC Tumors
3.3. eCPMV Immunotherapy Is not Toxic
3.4. eCPMV Immunotherapy Induces Modest Changes in Immune Blood Cell Populations
3.5. eCPMV Immunotherapy Induces Changes in Cytokine Plasma Levels
3.6. Anti-CPMV Antibodies Do Not Block Treatment Efficacy
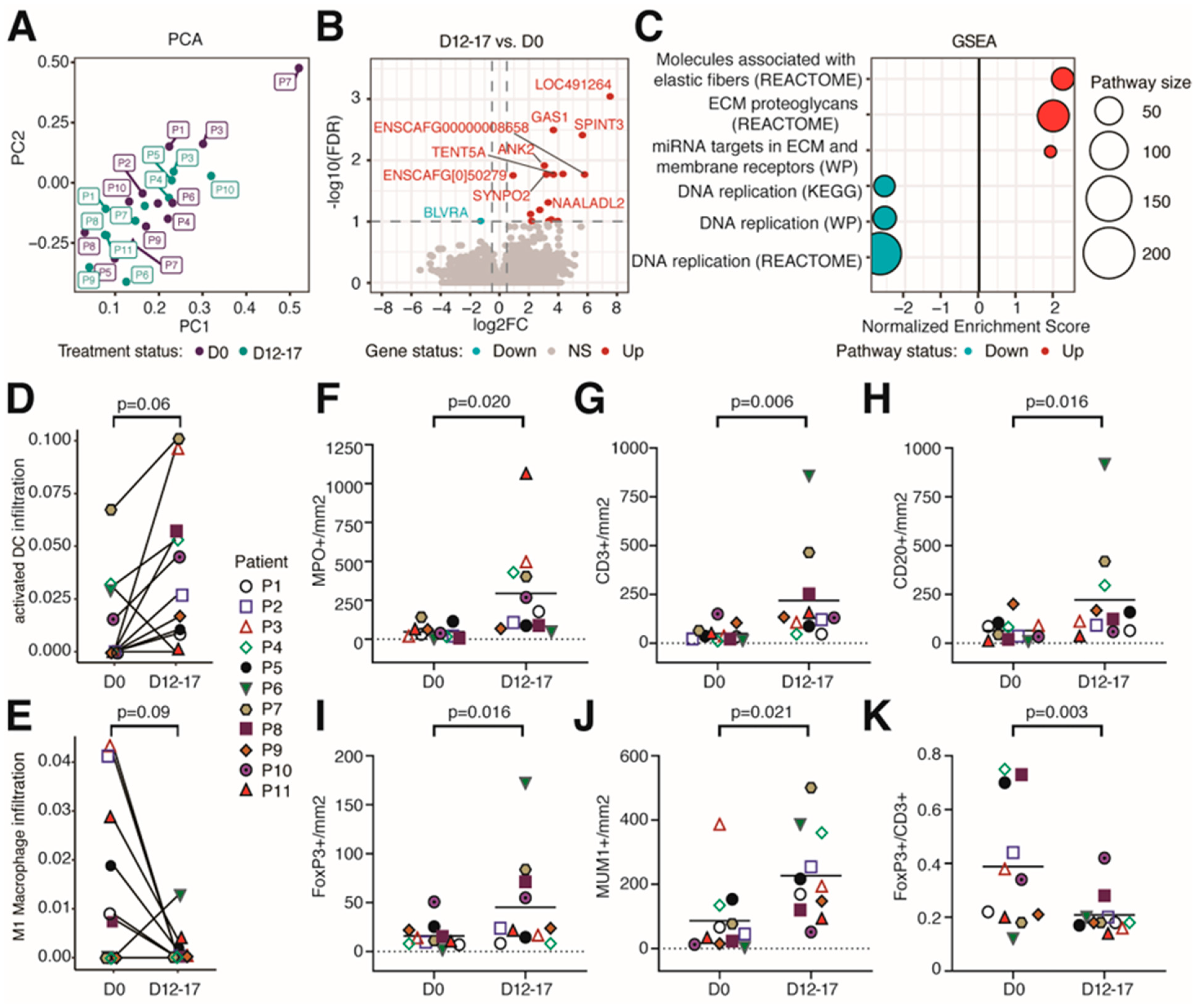
3.7. eCPMV Immunotherapy Induces Significant Changes in the TME
3.8. eCPMV Immunotherapy Does Not Affect QOL and Is Associated with Improved Survival in CMC Patients
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Emens, L.A. Breast Cancer Immunotherapy: Facts and Hopes. Clin. Cancer Res. 2018, 24, 511–520. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Wagle, N.S.; Jemal, A. Cancer statistics, 2023. CA A Cancer J. Clin. 2023, 73, 17–48. [Google Scholar] [CrossRef] [PubMed]
- Tevaarwerk, A.J.; Gray, R.J.; Schneider, B.P.; Smith, M.L.; Wagner, L.I.; Fetting, J.H.; Davidson, N.; Goldstein, L.J.; Miller, K.D.; Sparano, J.A. Survival in patients with metastatic recurrent breast cancer after adjuvant chemotherapy. Cancer 2013, 119, 1140–1148. [Google Scholar] [CrossRef]
- Mariotto, A.B.; Etzioni, R.; Hurlbert, M.; Penberthy, L.; Mayer, M. Estimation of the Number of Women Living with Metastatic Breast Cancer in the United States. Cancer Epidemiol. Biomark. Prev. 2017, 26, 809–815. [Google Scholar] [CrossRef] [PubMed]
- Caudle, A.S.; Gonzalez-Angulo, A.M.; Hunt, K.K.; Liu, P.; Pusztai, L.; Symmans, W.F.; Kuerer, H.M.; Mittendorf, E.A.; Hortobagyi, G.N.; Meric-Bernstam, F. Predictors of Tumor Progression During Neoadjuvant Chemotherapy in Breast Cancer. J. Clin. Oncol. 2010, 28, 1821–1828. [Google Scholar] [CrossRef] [PubMed]
- Connolly, R.M.; Stearns, V. Current approaches for neoadjuvant chemotherapy in breast cancer. Eur. J. Pharmacol. 2013, 717, 58–66. [Google Scholar] [CrossRef]
- Waks, A.G.; Winer, E.P. Breast Cancer Treatment: A Review. JAMA 2019, 321, 288–300. [Google Scholar] [CrossRef]
- National Cancer Institute Surveillance, Epidemiology, and End Results Program. Cancer Stat Facts: Female Breast Cancer 2020. Available online: https://seer.cancer.gov/statfacts/html/breast.html (accessed on 5 May 2023).
- Schmid, P.; Cortés, J.; Dent, R.; Pusztai, L.; McArthur, H.; Kuemmel, S.; Bergh, J.; Denkert, C.; Park, Y.; Hui, R.; et al. KEYNOTE-522: Phase 3 study of pembrolizumab (pembro) + chemotherapy (chemo) vs placebo (pbo) + chemo as neoadjuvant treatment, followed by pembro vs pbo as adjuvant treatment for early triple-negative breast cancer (TNBC). Ann. Oncol. 2019, 30, v851–v934. [Google Scholar] [CrossRef]
- Cortes, J.; Cescon, D.W.; Rugo, H.S.; Nowecki, Z.; Im, S.A.; Yusof, M.M.; Gallardo, C.; Lipatov, O.; Barrios, C.H.; Holgado, E.; et al. Pembrolizumab plus chemotherapy versus placebo plus chemotherapy for previously untreated locally recurrent inoperable or metastatic triple-negative breast cancer (KEYNOTE-355): A randomised, placebo-controlled, double-blind, phase 3 clinical trial. Lancet 2020, 396, 1817–1828. [Google Scholar] [CrossRef]
- Schmid, P.; Cortes, J.; Pusztai, L.; McArthur, H.; Kümmel, S.; Bergh, J.; Denkert, C.; Park, Y.H.; Hui, R.; Harbeck, N.; et al. Pembrolizumab for Early Triple-Negative Breast Cancer. N. Engl. J. Med. 2020, 382, 810–821. [Google Scholar] [CrossRef]
- Cheon, D.J.; Orsulic, S. Mouse models of cancer. Annu. Rev. Pathol. 2011, 6, 95–119. [Google Scholar] [CrossRef]
- Schiffman, J.D.; Breen, M. Comparative oncology: What dogs and other species can teach us about humans with cancer. Philos. Trans. R. Soc. B 2015, 370, 20140231. [Google Scholar] [CrossRef] [PubMed]
- Valdivia, G.; Alonso-Diez, Á.; Pérez-Alenza, D.; Peña, L. From Conventional to Precision Therapy in Canine Mammary Cancer: A Comprehensive Review. Front. Vet. Sci. 2021, 8, 623800. [Google Scholar] [CrossRef]
- Dow, S. A Role for Dogs in Advancing Cancer Immunotherapy Research. Front. Immunol. 2020, 10, 2935. [Google Scholar] [CrossRef]
- Raposo, T.P.; Arias-Pulido, H.; Chaher, N.; Fiering, S.N.; Argyle, D.J.; Prada, J.; Pires, I.; Queiroga, F.L. Comparative aspects of canine and human inflammatory breast cancer. Semin. Oncol. 2017, 44, 288–300. [Google Scholar] [CrossRef] [PubMed]
- Pinello, K.; Pires, I.; Castro, A.F.; Carvalho, P.T.; Santos, A.; de Matos, A.; Queiroga, F.; Canadas-Sousa, A.; Dias-Pereira, P.; Catarino, J.; et al. Cross Species Analysis and Comparison of Tumors in Dogs and Cats, by Age, Sex, Topography and Main Morphologies. Data from Vet-OncoNet. Vet. Sci. 2022, 9, 167. [Google Scholar] [CrossRef]
- Moe, L. Population-based incidence of mammary tumours in some dog breeds. J. Reprod. Fertil. Suppl. 2001, 57, 439–443. [Google Scholar] [PubMed]
- Perez Alenza, M.D.; Pena, L.; de Castillo, N.; Nieto, A. Factors influencing the incidence and prognosis of canine mammary tumours. J. Small Anim. Pract. 2000, 41, 287–291. [Google Scholar] [CrossRef]
- Pastor, N.; Caballé, N.C.; Santella, M.; Ezquerra, L.J.; Tarazona, R.; Durane, E. Epidemiological study of canine mammary tumors: Age, breed, size and malignancy. Austral J. Vet. Sci. 2018, 50, 143–147. [Google Scholar] [CrossRef]
- Lizotte, P.H.; Wen, A.M.; Sheen, M.R.; Fields, J.; Rojanasopondist, P.; Steinmetz, N.F.; Fiering, S. In situ vaccination with cowpea mosaic virus nanoparticles suppresses metastatic cancer. Nat. Nanotechnol. 2016, 11, 295–303. [Google Scholar] [CrossRef]
- Kerstetter-Fogle, A.; Shukla, S.; Wang, C.; Beiss, V.; Harris, P.L.R.; Sloan, A.E.; Steinmetz, N.F. Plant Virus-Like Particle In Situ Vaccine for Intracranial Glioma Immunotherapy. Cancers 2019, 11, 515. [Google Scholar] [CrossRef]
- Cai, H.; Wang, C.; Shukla, S.; Steinmetz, N.F. Cowpea Mosaic Virus Immunotherapy Combined with Cyclophosphamide Reduces Breast Cancer Tumor Burden and Inhibits Lung Metastasis. Adv. Sci. 2019, 6, 1802281. [Google Scholar] [CrossRef]
- Hoopes, P.J.; Wagner, R.J.; Duval, K.; Kang, K.; Gladstone, D.J.; Moodie, K.L.; Crary-Burney, M.; Ariaspulido, H.; Veliz, F.A.; Steinmetz, N.F.; et al. Treatment of Canine Oral Melanoma with Nanotechnology-Based Immunotherapy and Radiation. Mol. Pharm. 2018, 15, 3717–3722. [Google Scholar] [CrossRef]
- Alonso-Miguel, D.; Valdivia, G.; Guerrera, D.; Perez-Alenza, M.D.; Pantelyushin, S.; Alonso-Diez, A.; Beiss, V.; Fiering, S.; Steinmetz, N.F.; Suarez-Redondo, M.; et al. Neoadjuvant in situ vaccination with cowpea mosaic virus as a novel therapy against canine inflammatory mammary cancer. J. ImmunoTherapy Cancer 2022, 10, e004044. [Google Scholar] [CrossRef] [PubMed]
- Mao, C.; Beiss, V.; Fields, J.; Steinmetz, N.F.; Fiering, S. Cowpea mosaic virus stimulates antitumor immunity through recognition by multiple MYD88-dependent toll-like receptors. Biomaterials 2021, 275, 120914. [Google Scholar] [CrossRef]
- Wang, C.; Beiss, V.; Steinmetz, N.F. Cowpea Mosaic Virus Nanoparticles and Empty Virus-Like Particles Show Distinct but Overlapping Immunostimulatory Properties. J. Virol. 2019, 93, e00129-19. [Google Scholar] [CrossRef] [PubMed]
- Zappulli, V.; Pena, L.; Rassoto, R.; Goldschmidt, M.; Gama, A.; Seruggs, J.; Kiupel, M. Classification of Canine Mammary Tumors. In Surgical Pathology of Tumors of Domestic Animals. Volume 2: Mammary Tumors; Kiupel, M., Ed.; Davis-Thompson DVM Foundation: Gurnee, IL, USA, 2019; Volume 2, pp. 60–196. [Google Scholar]
- Peña, L.; De Andrés, P.J.; Clemente, M.; Cuesta, P.; Pérez-Alenza, M.D. Prognostic value of histological grading in noninflammatory canine mammary carcinomas in a prospective study with two-year follow-up: Relationship with clinical and histological characteristics. Vet. Pathol. 2013, 50, 94–105. [Google Scholar] [CrossRef]
- Rutteman, G.R.; Withrow, S.J.; MacEwen, E.G. Tumors of the mammary gland. In Small Animal Clinical Oncology, 3rd ed.; Withrow, S.J., MacEwen, E.G., Eds.; W.B. Saunders: Philadelphia, PA, USA, 2001; pp. 455–477. [Google Scholar]
- Saunders, K.; Sainsbury, F.; Lomonossoff, G.P. Efficient generation of cowpea mosaicvirus empty virus-like particles by the proteolytic processing of precursors in insect cells and plants. Virology 2009, 393, 329–337. [Google Scholar] [CrossRef] [PubMed]
- Lynch, S.; Savary-Bataille, K.; Leeuw, B.; Argyle, D.J. Development of a questionnaire assessing health-related quality-of-life in dogs and cats with cancer. Vet. Comp. Oncol. 2011, 9, 172–182. [Google Scholar] [CrossRef]
- Goldmacher, G.V.; Khilnani, A.D.; Andtbacka, R.H.I.; Luke, J.J.; Hodi, F.S.; Marabelle, A.; Harrington, K.; Perrone, A.; Tse, A.; Madoff, D.C.; et al. Response Criteria for Intratumoral Immunotherapy in Solid Tumors: itRECIST. J. Clin. Oncol. 2020, 38, 2667–2676. [Google Scholar] [CrossRef]
- LeBlanc, A.K.; Atherton, M.; Bentley, R.T.; Boudreau, C.E.; Burton, J.H.; Curran, K.M.; Dow, S.; Giuffrida, M.A.; Kellihan, H.B.; Mason, N.J.; et al. Veterinary Cooperative Oncology Group-Common Terminology Criteria for Adverse Events (VCOG-CTCAE v2) following investigational therapy in dogs and cats. Vet. Comp. Oncol. 2021, 19, 311–352. [Google Scholar] [CrossRef]
- Shukla, S.; Wang, C.; Beiss, V.; Steinmetz, N.F. Antibody Response against Cowpea Mosaic Viral Nanoparticles Improves In Situ Vaccine Efficacy in Ovarian Cancer. ACS Nano 2020, 14, 2994–3003. [Google Scholar] [CrossRef]
- Albakri, M.M.; Veliz, F.A.; Fiering, S.N.; Steinmetz, N.F.; Sieg, S.F. Endosomal toll-like receptors play a key role in activation of primary human monocytes by cowpea mosaic virus. Immunology 2020, 159, 183–192. [Google Scholar] [CrossRef] [PubMed]
- Rzepecka, A.; Żmigrodzka, M.; Witkowska-Piłaszewicz, O.; Cywińska, A.; Winnicka, A. CD4 and MHCII phenotypic variability of peripheral blood monocytes in dogs. PLoS ONE 2019, 14, e0219214. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.J.; Rutledge, B.J.; Rollins, B.J. Structure/activity analysis of human monocyte chemoattractant protein-1 (MCP-1) by mutagenesis. Identification of a mutated protein that inhibits MCP-1-mediated monocyte chemotaxis. J. Biol. Chem. 1994, 269, 15918–15924. [Google Scholar] [CrossRef]
- de Waal Malefyt, R.; Abrams, J.; Bennett, B.; Figdor, C.G.; de Vries, J.E. Interleukin 10(IL-10) inhibits cytokine synthesis by human monocytes: An autoregulatory role of IL-10 produced by monocytes. J. Exp. Med. 1991, 174, 1209–1220. [Google Scholar] [CrossRef]
- Futosi, K.; Fodor, S.; Mócsai, A. Neutrophil cell surface receptors and their intracellular signal transduction pathways. Int. Immunopharmacol. 2013, 17, 638–650. [Google Scholar] [CrossRef] [PubMed]
- Tecchio, C.; Micheletti, A.; Cassatella, M.A. Neutrophil-derived cytokines: Facts beyond expression. Front. Immunol. 2014, 5, 508. [Google Scholar] [CrossRef]
- Puga, I.; Cols, M.; Barra, C.M.; He, B.; Cassis, L.; Gentile, M.; Comerma, L.; Chorny, A.; Shan, M.; Xu, W.; et al. B cell-helper neutrophils stimulate the diversification and production of immunoglobulin in the marginal zone of the spleen. Nat. Immunol. 2011, 13, 170–180. [Google Scholar] [CrossRef]
- Pelletier, M.; Maggi, L.; Micheletti, A.; Lazzeri, E.; Tamassia, N.; Costantini, C.; Cosmi, L.; Lunardi, C.; Annunziato, F.; Romagnani, S.; et al. Evidence for a cross-talk between human neutrophils and Th17 cells. Blood 2010, 115, 335–343. [Google Scholar] [CrossRef]
- Polak, D.; Bohle, B. Neutrophils-typical atypical antigen presenting cells? Immunol. Lett. 2022, 247, 52–58. [Google Scholar] [CrossRef]
- Mole, R.H. Whole body irradiation; radiobiology or medicine? Br. J. Radiol. 1953, 26, 234–241. [Google Scholar] [CrossRef] [PubMed]
- Song, F.; Li, X.; Song, F.; Zhao, Y.; Li, H.; Zheng, H.; Gao, Z.; Wang, J.; Zhang, W.; Chen, K. Comparative genomic analysis reveals bilateral breast cancers are genetically independent. Oncotarget 2015, 6, 31820–31829. [Google Scholar] [CrossRef]
- Hamy, A.S.; Abécassis, J.; Driouch, K.; Darrigues, L.; Vandenbogaert, M.; Laurent, C.; Zaccarini, F.; Sadacca, B.; Delomenie, M.; Laas, E.; et al. Evolution of synchronous female bilateral breast cancers and response to treatment. Nat. Med. 2023, 29, 646–655. [Google Scholar] [CrossRef]
- Graim, K.; Gorenshteyn, D.; Robinson, D.G.; Carriero, N.J.; Cahill, J.A.; Chakrabarti, R.; Goldschmidt, M.H.; Durham, A.C.; Funk, J.; Storey, J.D.; et al. Modeling molecular development of breast cancer in canine mammary tumors. Genome Res. 2020, 31, 337–347. [Google Scholar] [CrossRef]
- Affonso de Oliveira, J.F.; Chan, S.K.; Omole, A.O.; Agrawal, V.; Steinmetz, N.F. In Vivo Fate of Cowpea Mosaic Virus In Situ Vaccine: Biodistribution and Clearance. ACS Nano 2022, 16, 18315–18328. [Google Scholar] [CrossRef] [PubMed]
- Davda, J.; Declerck, P.; Hu-Lieskovan, S.; Hickling, T.P.; Jacobs, I.A.; Chou, J.; Salek-Ardakani, S.; Kraynov, E. Immunogenicity of immunomodulatory, antibody-based, oncology therapeutics. J. ImmunoTherapy Cancer 2019, 7, 105. [Google Scholar] [CrossRef]
- Peña, L.; Perez-Alenza, M.D.; Rodriguez-Bertos, A.; Nieto, A. Canine inflammatory mammary carcinoma: Histopathology, immunohistochemistry and clinical implications of 21 cases. Breast Cancer Res. Treat. 2003, 78, 141–148. [Google Scholar] [CrossRef] [PubMed]
- Perez Alenza, M.D.; Tabanera, E.; Pena, L. Inflammatory mammary carcinoma in dogs: 33 cases (1995–1999). J. Am. Vet. Med. Assoc. 2001, 219, 1110–1114. [Google Scholar] [CrossRef]
- Mao, C.; Beiss, V.; Ho, G.W.; Fields, J.; Steinmetz, N.F.; Fiering, S. In situ vaccination with cowpea mosaic virus elicits systemic antitumor immunity and potentiates immune checkpoint blockade. J. Immunother. Cancer 2022, 10, e005834. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Steinmetz, N.F. A Combination of Cowpea Mosaic Virus and Immune Checkpoint Therapy Synergistically Improves Therapeutic Efficacy in Three Tumor Models. Adv. Funct. Mater. 2020, 30, 2002299. [Google Scholar] [CrossRef] [PubMed]
- Burrai, G.P.; Gabrieli, A.; Moccia, V.; Zappulli, V.; Porcellato, I.; Brachelente, C.; Pirino, S.; Polinas, M.; Antuofermo, E. A Statistical Analysis of Risk Factors and Biological Behavior in Canine Mammary Tumors: A Multicenter Study. Animals 2020, 10, 1687. [Google Scholar] [CrossRef]
- Sorenmo, K.U.; Kristiansen, V.M.; Cofone, M.A.; Shofer, F.S.; Breen, A.-M.; Langeland, M.; Mongil, C.M.; Grondahl, A.M.; Teige, J.; Goldschmidt, M.H. Canine Mammary Gland Tumours; a Histological Continuum from Benign to Malignant; Clinical and Histopathological Evidence. Vet. Comp. Oncol. 2009, 7, 162–172. [Google Scholar] [CrossRef]
- Percie du Sert, N.; Hurst, V.; Ahluwalia, A.; Alam, S.; Avey, M.T.; Baker, M.; Browne, W.J.; Clark, A.; Cuthill, I.C.; Dirnagl, U.; et al. The ARRIVE Guidelines 2.0: Updated Guidelines for Reporting Animal Research. PLoS Biol. 2020, 18, e3000410. [Google Scholar] [CrossRef]
- Marabelle, A.; Andtbacka, R.; Harrington, K.; Melero, I.; Leidner, R.; de Baere, T.; Robert, C.; Ascierto, P.A.; Baurain, J.-F.; Imperiale, M.; et al. Starting the Fight in the Tumor: Expert Recommendations for the Development of Human Intratumoral Immunotherapy (HIT-IT). Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2018, 29, 2163–2174. [Google Scholar] [CrossRef] [PubMed]
- Pantelyushin, S.; Ranninger, E.; Bettschart-Wolfensberger, R.; Vom Berg, J. OMIP-065: Dog Immunophenotyping and T-Cell Activity Evaluation with a 14-Color Panel. Cytometry. Part J J. Int. Soc. Anal. Cytol. 2020, 97, 1024–1027. [Google Scholar] [CrossRef]
- Carvalho, M.I.; Pires, I.; Prada, J.; Lobo, L.; Queiroga, F.L. Ki-67 and PCNA Expression in Canine Mammary Tumors and Adjacent Nonneoplastic Mammary Glands: Prognostic Impact by a Multivariate Survival Analysis. Vet. Pathol. 2016, 53, 1138–1146. [Google Scholar] [CrossRef] [PubMed]
- Peña, L.; Gama, A.; Goldschmidt, M.H.; Abadie, J.; Benazzi, C.; Castagnaro, M.; Díez, L.; Gärtner, F.; Hellmén, E.; Kiupel, M.; et al. Canine Mammary Tumors: A Review and Consensus of Standard Guidelines on Epithelial and Myoepithelial Phenotype Markers, HER2, and Hormone Receptor Assessment Using Immunohistochemistry. Vet. Pathol. 2014, 51, 127–145. [Google Scholar] [CrossRef]
- Sauerbrei, W.; Taube, S.E.; McShane, L.M.; Cavenagh, M.M.; Altman, D.G. Reporting Recommendations for Tumor Marker Prognostic Studies (REMARK): An Abridged Explanation and Elaboration. J. Natl. Cancer Inst. 2018, 110, 803–811. [Google Scholar] [CrossRef]
- Babraham Bioinformatics-FastQC A Quality Control Tool for High Throughput Sequence Data. Available online: https://www.bioinformatics.babraham.ac.uk/projects/fastqc/ (accessed on 5 March 2023).
- Martin, M. Cutadapt Removes Adapter Sequences from High-Throughput Sequencing Reads. EMBnet J. 2011, 17, 10–12. [Google Scholar] [CrossRef]
- Dobin, A.; Davis, C.A.; Schlesinger, F.; Drenkow, J.; Zaleski, C.; Jha, S.; Batut, P.; Chaisson, M.; Gingeras, T.R. STAR: Ultrafast Universal RNA-Seq Aligner. Bioinformatics 2013, 29, 15–21. [Google Scholar] [CrossRef]
- Liao, Y.; Smyth, G.K.; Shi, W. FeatureCounts: An Efficient General Purpose Program for Assigning Sequence Reads to Genomic Features. Bioinformatics 2014, 30, 923–930. [Google Scholar] [CrossRef]
- Leek, J.T.; Johnson, W.E.; Parker, H.S.; Jaffe, A.E.; Storey, J.D. The Sva Package for Removing Batch Effects and Other Unwanted Variation in High-Throughput Experiments. Bioinformatics 2012, 28, 882–883. [Google Scholar] [CrossRef]
- Anders, S.; Huber, W. Differential Expression Analysis for Sequence Count Data. Genome Biol. 2010, 11, R106. [Google Scholar] [CrossRef] [PubMed]
- Korotkevich, G.; Sukhov, V.; Budin, N.; Shpak, B.; Artyomov, M.; Sergushichev, A. Fast Gene Set Enrichment Analysis|BioRxiv. Available online: https://www.biorxiv.org/content/10.1101/060012v3 (accessed on 7 March 2023).
- Subramanian, A.; Tamayo, P.; Mootha, V.K.; Mukherjee, S.; Ebert, B.L.; Gillette, M.A.; Paulovich, A.; Pomeroy, S.L.; Golub, T.R.; Lander, E.S.; et al. Gene Set Enrichment Analysis: A Knowledge-Based Approach for Interpreting Genome-Wide Expression Profiles. Proc. Natl. Acad. Sci. USA 2005, 102, 15545–15550. [Google Scholar] [CrossRef] [PubMed]
- Newman, A.M.; Steen, C.B.; Liu, C.L.; Gentles, A.J.; Chaudhuri, A.A.; Scherer, F.; Khodadoust, M.S.; Esfahani, M.S.; Luca, B.A.; Steiner, D.; et al. Determining Cell Type Abundance and Expression from Bulk Tissues with Digital Cytometry. Nat. Biotechnol. 2019, 37, 773–782. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Patient | Age, y. | Weight, kg | Clin. Stage | Histotype; Carcinoma Grade | LNI | * TS, cm | ** TS, cm3 | Molecular Subtype | Adj. Ther. | Rec. Met. | OS, Days | Status |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| P1 | 10.4 | 39.2 | II | I | No | 5.0 | 22.5 | Luminal A | No | No | 1345 | Alive |
| P2 | 5.8 | 37.8 | I | I | No | 2.6 | 5.2 | Luminal A | No | No | 1226 | Alive |
| P3 | 9.1 | 20.5 | IV | I | Yes | 6.2 | 18.6 | Luminal A | No | No | 1250 | Alive |
| P4 | 8.4 | 6.5 | II | I | No | 3.3 | 5.3 | Luminal A | No | No | 1202 | Alive |
| P5 | 8.0 | 32.7 | II | I | No | 4.2 | 19.5 | Luminal A | No | No | 1135 | Alive |
| P6 | 9.6 | 33.2 | IV | III | Yes | 6.6 | 6.0 | TN | No | No | 217 | NCRD |
| P7 | 13.0 | 9.2 | I | I | No | 2.9 | 5.2 | Luminal A | No | No | 411 | Alive |
| P8 | 12.1 | 30.3 | III | I | No | 7.5 | 63.0 | Luminal A | No | No | 425 | Alive |
| P9 | 10.8 | 9.3 | I | I | No | 2.7 | 7.5 | Luminal A | No | No | 449 | Alive |
| P10 | 12.5 | 23.3 | I | III | No | 2.3 | 3.3 | TN | mCTX + F | No | 414 | Alive |
| P11 | 14.8 | 6.1 | III | II | No | 5.9 | 42.6 | Luminal B | mCTX | No | 267 | Alive |
| Patient | Day | Tv, cm3 | %TGI | p Value |
|---|---|---|---|---|
| P1 | D0 | 22.5 | ||
| (L2) | D8 | 20.3 | −10.0 | |
| D16 | 17.6 | −21.6 | 0.037 | |
| P2 | D0 | 5.2 | ||
| (R5) | D7 | 5.0 | −3.8 | |
| D14 | 4.9 | −5.8 | 0.121 | |
| P3 | D0 | 18.6 | ||
| (R3) | D7 | 15.2 | −18.4 | |
| D13 | 12.0 | −35.4 | 0.011 | |
| P4 | D0 | 5.3 | ||
| (R4) | D6 | 4.9 | −8.1 | |
| D13 | 4.8 | −10.8 | 0.212 | |
| P5 | D0 | 19.5 | ||
| (R4) | D9 | 15.6 | −20.1 | |
| D17 | 13.2 | −32.5 | 0.087 | |
| P6 | D0 | 6.0 | ||
| (L5) | D6 | 5.2 | −14.3 | |
| D13 | 4.4 | −27.0 | <0.001 | |
| P7 | D0 | 5.2 | ||
| (L5) | D8 | 3.6 | −31.5 | |
| D15 | 2.5 | −53.2 | 0.068 | |
| P8 | D0 | 63.0 | ||
| (L4) | D7 | 67.2 | 6.6 | |
| D12 | 59.0 | −6.3 | 0.642 | |
| P9 | D0 | 7.5 | ||
| (L5) | D7 | 5.3 | −29.0 | |
| D13 | 5.1 | −32.0 | 0.238 | |
| P10 | D0 | 3.3 | ||
| (L3) | D6 | 3.2 | −4.3 | |
| D13 | 2.7 | −19.1 | 0.213 | |
| P11 | D0 | 42.6 | ||
| (R3) | D8 | 25.4 | −40.3 | |
| D15 | 15.7 | −63.2 | 0.073 |
| Ipsilateral Chain | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ID | P1—Gr. I | P2—Gr. I | P5—Gr. I | P7—Gr. I | P8—Gr. I | P9—Gr. I | P10—Gr. III | P11—Gr. II | ||||||||||
| V, cm3 | %TGI | V, cm3 | %TGI | V, cm3 | %TGI | V, cm3 | %TGI | V, cm3 | %TGI | V, cm3 | %TGI | V, cm3 | %TGI | V, cm3 | %TGI | V, cm3 | %TGI | |
| P1.1—Gr. I | P2.1—Benign | P5.1 Gr. I | P7.1—Gr. II | P8.1—Gr. I | P8.5—Benign | P9.1—HD | P10.1—Gr. I | P11.1—Gr. I | ||||||||||
| D0 | 1.69 | 0.06 | 0.06 | 0.49 | 0.06 | 0.20 | 0.03 | 0.14 | 0.01 | |||||||||
| DTx2 | 0.75 | −55.56 | 0.06 | 0.00 | 0.01 | −78.40 | 0.40 | −18.24 | 0.03 | −48.80 | 0.13 | −36.36 | 0.03 | 0.00 | 0.11 | −26.48 | 0.01 | 0.00 |
| DSx | 0.23 | −86.11 | 0.01 | −78.40 | 0.01 | −78.40 | 0.40 | −18.24 | 0.03 | −48.80 | 0.13 | −36.36 | 0.03 | 0.00 | 0.09 | −39.24 | 0.01 | 0.00 |
| P1.2—HD | P2.2—Benign | P7.2—Gr. I | P8.2—Gr. I | P8.6—Gr. I | P9.2—Benign | P11.2—Gr. II | ||||||||||||
| D0 | 1.69 | 0.50 | 0.26 | 0.06 | 0.18 | 0.13 | 0.03 | |||||||||||
| DTx2 | 0.50 | −70.37 | 0.50 | 0.00 | 0.29 | 12.50 | 0.03 | −48.80 | 0.17 | −4.72 | 0.13 | 0.00 | 0.06 | 95.31 | ||||
| DSx | 0.50 | −70.37 | 0.50 | 0.00 | 0.25 | −1.12 | 0.03 | −48.80 | 0.17 | −4.72 | 0.13 | 0.00 | 0.03 | 0.00 | ||||
| P1.3—HD | P7.3—HD | P8.3—Gr. I | P8.7—Gr. I | P11.3—Gr. II | ||||||||||||||
| D0 | 2.25 | 0.11 | 0.36 | 0.45 | 0.67 | |||||||||||||
| DTx2 | 1.69 | −25.00 | 0.004 | −96.30 | 0.17 | −52.95 | 0.26 | −42.54 | 0.67 | 0.00 | ||||||||
| DSx | 1.62 | −27.96 | 0.004 | −96.30 | 0.17 | −52.95 | 0.26 | −42.54 | 0.67 | 0.00 | ||||||||
| P7.4—Benign | P8.4—Benign. | P8.8—Gr. I | ||||||||||||||||
| D0 | 0.03 | 2.48 | 1.25 | |||||||||||||||
| DTx2 | 0.01 | −57.81 | 1.15 | −53.56 | 1.01 | −19.36 | ||||||||||||
| DSx | 0.01 | −57.81 | 0.65 | −73.74 | 0.86 | −31.23 | ||||||||||||
| Contralateral chain | ||||||||||||||||||
| ID | P1—Gr. I | P3—Gr. I | P4—Gr. I | P5—Gr. I | P7—Gr. I | P9—Gr. I | P11—Gr. II | |||||||||||
| V, cm3 | %TGI | V, cm3 | %TGI | V, cm3 | %TGI | V, cm3 | %TGI | V, cm3 | %TGI | V, cm3 | %TGI | V, cm3 | %TGI | V, cm3 | %TGI | |||
| P1.4—Benign | P3.1—Benign | P4.1—Benign | P5.2—Unknown | P7.5—Gr. I | P9.3—Benign | P11.4—Unknown | P11.8—Unknown | |||||||||||
| D0 | 0.06 | 0.07 | 0.11 | 0.50 | 0.11 | 0.25 | 0.17 | 0.03 | ||||||||||
| DTx2 | 0.06 | 0.00 | 0.07 | 0.00 | 0.11 | 0.00 | 0.50 | 0.00 | 0.13 | 16.67 | 0.22 | −10.00 | 0.11 | −37.03 | 0.03 | 0.00 | ||
| DSx | 0.06 | 0.00 | 0.07 | 0.00 | 0.11 | 0.00 | 0.11 | −78.40 | 0.13 | 16.67 | 0.16 | −33.88 | 0.11 | −37.03 | 0.06 | 95.31 | ||
| P1.5—HD | P3.2—Benign | P4.2—Benign | P7.6—Gr. I | P11.5—Unknown | P11.9—Unknown | |||||||||||||
| D0 | 0.75 | 0.79 | 0.11 | 1.08 | 0.06 | 0.03 | ||||||||||||
| DTx2 | 0.60 | −20.00 | 0.32 | −59.17 | 0.11 | 0.00 | 1.82 | 68.75 | 0.06 | 0.00 | 0.01 | −57.81 | ||||||
| DSx | 0.60 | −20.00 | 0.32 | −59.17 | 0.11 | 0.00 | 1.33 | 22.97 | 0.03 | −48.80 | 0.06 | 95.31 | ||||||
| P1.6—Gr. I | P11.6—Unknown | P11.10—Unknown | ||||||||||||||||
| D0 | 0.50 | 0.06 | 0.06 | |||||||||||||||
| DTx2 | 0.50 | 0.00 | 0.03 | −48.80 | 0.03 | −48.80 | ||||||||||||
| DSx | 0.50 | 0.00 | 0.03 | −48.80 | 0.03 | −48.80 | ||||||||||||
| P11.7—Unknown | P11.11—Unknown | |||||||||||||||||
| D0 | 0.004 | 0.17 | ||||||||||||||||
| DTx2 | 0.014 | 237.50 | 0.17 | 0.00 | ||||||||||||||
| DSx | 0.004 | 0.00 | 0.17 | 0.00 | ||||||||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Valdivia, G.; Alonso-Miguel, D.; Perez-Alenza, M.D.; Zimmermann, A.B.E.; Schaafsma, E.; Kolling, F.W., IV; Barreno, L.; Alonso-Diez, A.; Beiss, V.; Affonso de Oliveira, J.F.; et al. Neoadjuvant Intratumoral Immunotherapy with Cowpea Mosaic Virus Induces Local and Systemic Antitumor Efficacy in Canine Mammary Cancer Patients. Cells 2023, 12, 2241. https://doi.org/10.3390/cells12182241
Valdivia G, Alonso-Miguel D, Perez-Alenza MD, Zimmermann ABE, Schaafsma E, Kolling FW IV, Barreno L, Alonso-Diez A, Beiss V, Affonso de Oliveira JF, et al. Neoadjuvant Intratumoral Immunotherapy with Cowpea Mosaic Virus Induces Local and Systemic Antitumor Efficacy in Canine Mammary Cancer Patients. Cells. 2023; 12(18):2241. https://doi.org/10.3390/cells12182241
Chicago/Turabian StyleValdivia, Guillermo, Daniel Alonso-Miguel, Maria Dolores Perez-Alenza, Anna Barbara Emilia Zimmermann, Evelien Schaafsma, Fred W. Kolling, IV, Lucia Barreno, Angela Alonso-Diez, Veronique Beiss, Jessica Fernanda Affonso de Oliveira, and et al. 2023. "Neoadjuvant Intratumoral Immunotherapy with Cowpea Mosaic Virus Induces Local and Systemic Antitumor Efficacy in Canine Mammary Cancer Patients" Cells 12, no. 18: 2241. https://doi.org/10.3390/cells12182241
APA StyleValdivia, G., Alonso-Miguel, D., Perez-Alenza, M. D., Zimmermann, A. B. E., Schaafsma, E., Kolling, F. W., IV, Barreno, L., Alonso-Diez, A., Beiss, V., Affonso de Oliveira, J. F., Suárez-Redondo, M., Fiering, S., Steinmetz, N. F., vom Berg, J., Peña, L., & Arias-Pulido, H. (2023). Neoadjuvant Intratumoral Immunotherapy with Cowpea Mosaic Virus Induces Local and Systemic Antitumor Efficacy in Canine Mammary Cancer Patients. Cells, 12(18), 2241. https://doi.org/10.3390/cells12182241