
The Eye of the Storm: Investigating the Long-Term Cardiovascular Effects of COVID-19 and Variants



Abstract
:
{kind=link}
{kind=link}
{kind=link}
{kind=link}
1. Introduction
2. Early Discoveries and Variants
2.1. Alpha, Delta, Omicron and Their Immediate Risks
2.2. Long-Term Effects of Alpha, Delta, and Omicron
2.3. Acute Cardiac Complications
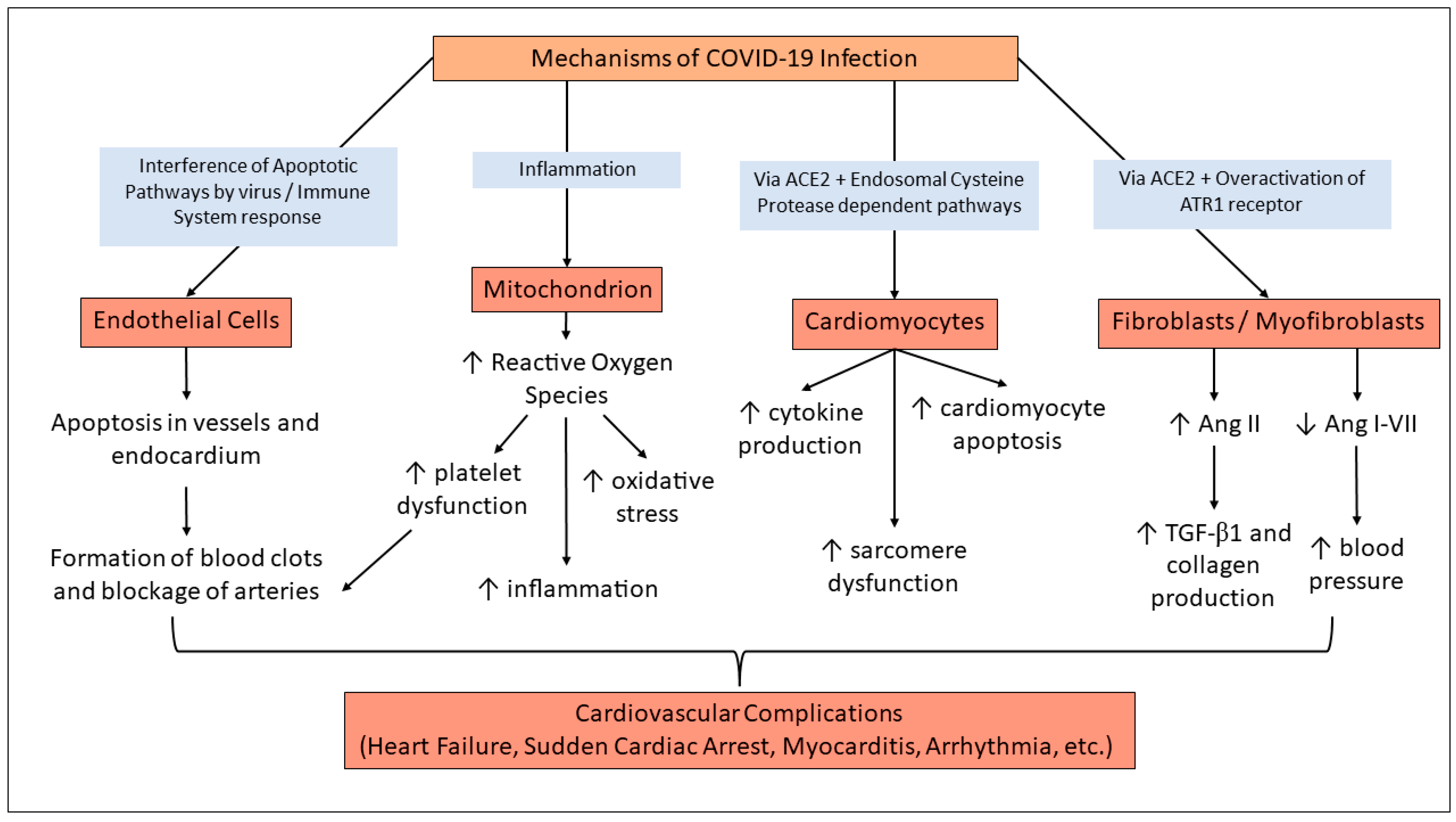
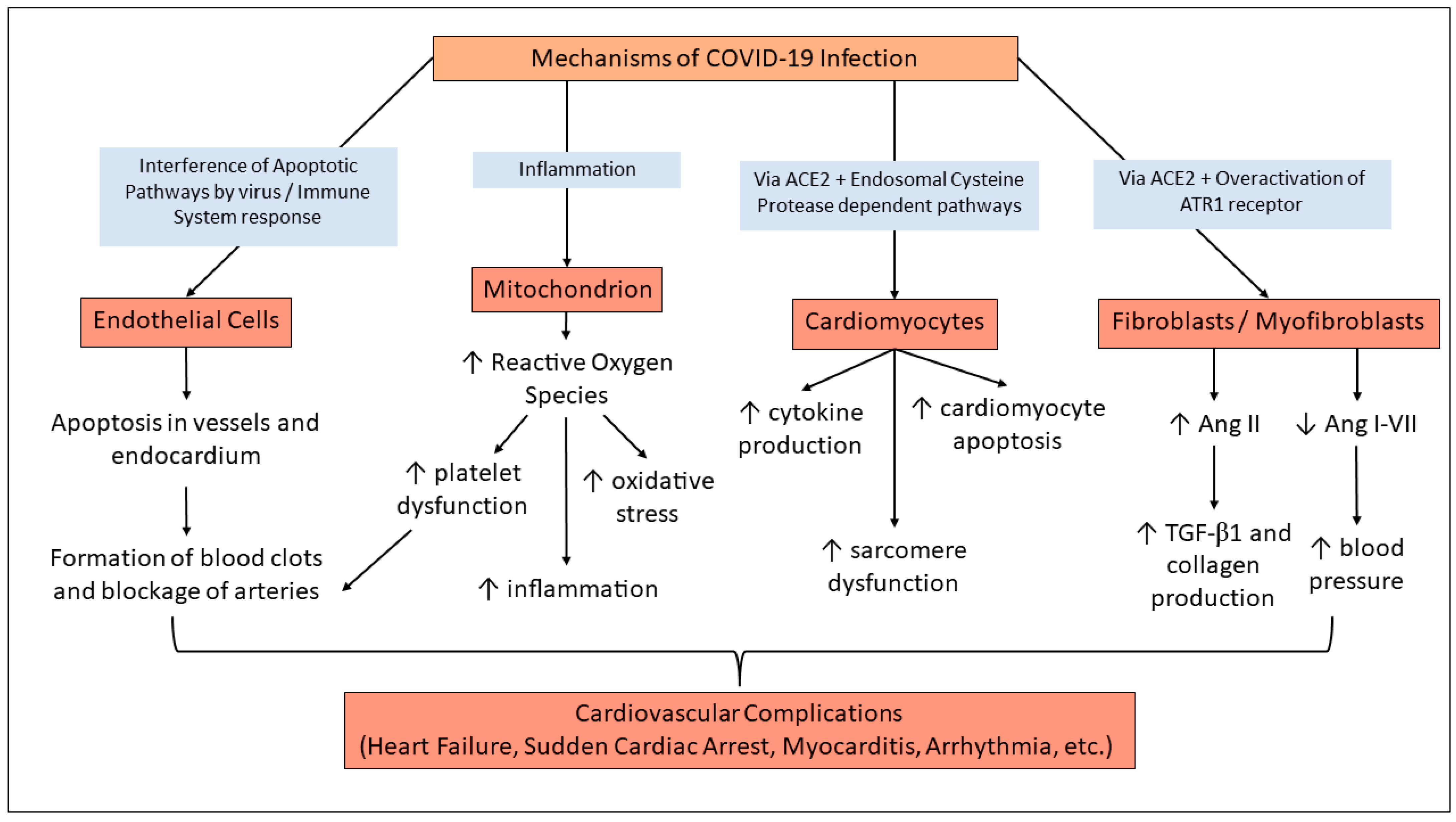
2.4. Mechanisms of COVID-Induced Cardiac Complications
3. Emerging Variants and Clinical Observations
3.1. Immediate Risks for Rising Variants
3.2. Long-Term Effects of the New Variants
4. Long Term Implications
4.1. Long COVID
4.2. Long-Term Cardiovascular Complications
4.3. Effects of COVID-19 Vaccinations
5. Gaps and Future Directions
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tsao, C.W.; Aday, A.W.; Almarzooq, Z.I.; Anderson, C.A.; Arora, P.; Avery, C.L.; Baker-Smith, C.M.; Beaton, A.Z.; Boehme, A.K.; Buxton, A.E.; et al. Heart Disease and Stroke Statistics—2023 Update: A Report From the American Heart Association. Circulation 2023, 147, e93–e621. [Google Scholar] [CrossRef] [PubMed]
- Xie, Y.; Xu, E.; Bowe, B.; Al-Aly, Z. Long-term cardiovascular outcomes of COVID-19. Nat. Med. 2022, 28, 583–590. [Google Scholar] [CrossRef] [PubMed]
- Hiscott, J.; Alexandridi, M.; Muscolini, M.; Tassone, E.; Palermo, E.; Soultsioti, M.; Zevini, A. The global impact of the coronavirus pandemic. Cytokine Growth Factor Rev. 2020, 53, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Greenberg, G.C.; Vishwakarma, N.; Tirupattur, M.P.; Sprague, H.M.; Katwa, L.C. Implications of COVID-19 Pandemic on Pregnancy: Current Status and Controversies. COVID 2023, 3, 859–873. [Google Scholar] [CrossRef]
- El-Shabasy, R.M.; Nayel, M.A.; Taher, M.M.; Abdelmonem, R.; Shoueir, K.R.; Kenawy, E.R. Three waves changes, new variant strains, and vaccination effect against COVID-19 pandemic. Int. J. Biol. Macromol. 2022, 204, 161–168. [Google Scholar] [CrossRef] [PubMed]
- Katwa, L.C.; Mendoza, C.; Clements, M. CVD and COVID-19: Emerging Roles of Cardiac Fibroblasts and Myofibroblasts. Cells 2022, 11, 1316. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.-H.; Zhao, L.; Yang, X.-C.; Wang, P. Cardiovascular complications of SARS-CoV-2 infection (COVID-19): A systematic review and meta-analysis. Rev. Cardiovasc. Med. 2021, 22, 159. [Google Scholar] [CrossRef]
- Tsai, E.J.; Čiháková, D.; Tucker, N.R. Cell-Specific Mechanisms in the Heart of COVID-19 Patients. Circ. Res. 2023, 132, 1290–1301. [Google Scholar] [CrossRef]
- Bailey, A.L.; Dmytrenko, O.; Greenberg, L.; Bredemeyer, A.L.; Ma, P.; Liu, J.; Penna, V.; Winkler, E.S.; Sviben, S.; Brooks, E.; et al. SARS-CoV-2 Infects Human Engineered Heart Tissues and Models COVID-19 Myocarditis. JACC Basic Transl. Sci. 2021, 6, 331–345. [Google Scholar] [CrossRef]
- Katwa, L.C.; Shashikant, C. Cardiac Remodeling and Fibrosis: Role of Myofibroblasts. In The Cardiac Fibroblast; Research Signpost: Kerala, India, 2011; pp. 29–52. [Google Scholar]
- CDC. SARS-CoV-2 Variant Classifications and Definitions. Center for Disease Control and Prevention. 11 February 2020. Available online: https://www.cdc.gov/coronavirus/2019-ncov/variants/variant-classifications.html#anchor_1679059484954 (accessed on 24 July 2023).
- CoVariants. CoVariants.org. 2023. Available online: https://covariants.org/ (accessed on 16 July 2023).
- Molteni, E.; Graham, M.; Canas, L.S.; Antonelli, M.; Chen, L.; Deng, J.; Murray, B.; Kerfoot, E.; Wolf, J.; May, A.; et al. COVID-19 due to the B.1.617.2 (Delta) variant compared to B.1.1.7 (Alpha) variant of SARS-CoV-2: A prospective observational cohort study. Sci. Rep. 2022, 12, 10904. [Google Scholar] [CrossRef]
- Hernández-Aceituno, A.; García-Hernández, A.; Larumbe-Zabala, E. COVID-19 long-term sequelae: Omicron versus Alpha and Delta variants. Infect. Dis. Now 2023, 53, 104688. [Google Scholar] [CrossRef]
- Earnest, R.; Uddin, R.; Matluk, N.; Renzette, N.; Turbett, S.E.; Siddle, K.J.; Loreth, C.; Adams, G.; Tomkins-Tinch, C.H.; Petrone, M.E.; et al. Comparative transmissibility of SARS-CoV-2 variants Delta and Alpha in New England, USA. Cell Rep. Med. 2022, 3, 100583. [Google Scholar] [CrossRef]
- CDC. Understanding Risk. Center for Disease Control and Prevention. 11 February 2020. Available online: https://www.cdc.gov/coronavirus/2019-ncov/your-health/understanding-risk.html (accessed on 16 July 2023).
- Augusto, D.G.; Murdolo, L.D.; Chatzileontiadou, D.S.M.; Sabatino, J.J.; Yusufali, T.; Peyser, N.D.; Butcher, X.; Kizer, K.; Guthrie, K.; Murray, V.W.; et al. A common allele of HLA is associated with asymptomatic SARS-CoV-2 infection. Nature 2023, 620, 128–136. [Google Scholar] [CrossRef]
- CDC. CDC Archives—COVID Data. Center for Disease Control and Prevention. 2023. Available online: https://archive.cdc.gov/#/details?q=covid%2019%20hospitalization%20death%20rate%20&start=0&rows=10&url=https://www.cdc.gov/coronavirus/2019-ncov/covid-data/investigations-discovery/hospitalization-death-by-age.html (accessed on 16 July 2023).
- CDC. Symptoms of COVID-19. Center for Disease Control and Prevention. 11 February 2020. Available online: https://www.cdc.gov/coronavirus/2019-ncov/symptoms-testing/symptoms.html (accessed on 16 July 2023).
- Tobler, D.L.; Pruzansky, A.J.; Naderi, S.; Ambrosy, A.P.; Slade, J.J. Long-Term Cardiovascular Effects of COVID-19: Emerging Data Relevant to the Cardiovascular Clinician. Curr. Atheroscler. Rep. 2022, 24, 563–570. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Wong, J.Y.; Cheung, J.K.; Lin, Y.; Bond, H.S.; Lau, E.H.Y.; Ip, D.K.M.; Cowling, B.J.; Wu, P. Intrinsic and Effective Severity of Coronavirus Disease 2019 Cases Infected With the Ancestral Strain and Omicron BA.2 Variant in Hong Kong. J. Infect. Dis. 2023. ahead-of-print. [Google Scholar] [CrossRef]
- Buchan, S.A.; Chung, H.; Brown, K.A.; Austin, P.C.; Fell, D.B.; Gubbay, J.B.; Nasreen, S.; Schwartz, K.L.; Sundaram, M.E.; Tadrous, M.; et al. Estimated Effectiveness of COVID-19 Vaccines Against Omicron or Delta Symptomatic Infection and Severe Outcomes. JAMA Netw. Open 2022, 5, e2232760. [Google Scholar] [CrossRef]
- Arabi, M.; Al-Najjar, Y.; Mhaimeed, N.; Salameh, M.A.; Paul, P.; AlAnni, J.; Abdelati, A.A.; Laswi, I.; Khanjar, B.; Al-Ali, D.; et al. Severity of the Omicron SARS-CoV-2 variant compared with the previous lineages: A systematic review. J. Cell. Mol. Med. 2023, 27, 1443–1464. [Google Scholar] [CrossRef]
- Lewnard, J.A.; Hong, V.X.; Patel, M.M.; Kahn, R.; Lipsitch, M.; Tartof, S.Y. Clinical outcomes associated with SARS-CoV-2 Omicron (B.1.1.529) variant and BA.1/BA.1.1 or BA.2 subvariant infection in Southern California. Nat. Med. 2022, 28, 1933–1943. [Google Scholar] [CrossRef]
- Wang, L.; Berger, N.A.; Kaelber, D.C.; Davis, P.B.; Volkow, N.D.; Xu, R. COVID infection rates, clinical outcomes, and racial/ethnic and gender disparities before and after Omicron emerged in the US. medRxiv 2022. [Google Scholar] [CrossRef]
- Antonelli, M.; Pujol, J.C.; Spector, T.D.; Ourselin, S.; Steves, C.J. Risk of long COVID associated with delta versus omicron variants of SARS-CoV-2. Lancet 2022, 399, 2263–2264. [Google Scholar] [CrossRef] [PubMed]
- Spinicci, M.; Graziani, L.; Tilli, M.; Nkurunziza, J.; Vellere, I.; Borchi, B.; Mencarini, J.; Campolmi, I.; Gori, L.; Giovannoni, L.; et al. Infection with SARS-CoV-2 Variants Is Associated with Different Long COVID Phenotypes. Viruses 2022, 14, 2367. [Google Scholar] [CrossRef] [PubMed]
- Del Prete, A.; Conway, F.; Della Rocca, D.G.; Biondi-Zoccai, G.; De Felice, F.; Musto, C.; Picichè, M.; Martuscelli, E.; Natale, A.; Versaci, F. COVID-19, Acute Myocardial Injury, and Infarction. Card. Electrophysiol. Clin. 2022, 14, 29–39. [Google Scholar] [CrossRef] [PubMed]
- Benhuri, B.; Aikawa, T.; Takagi, H.; Benhuri, D.; Kuno, T. Elevated Natriuretic Peptides in Patients With Severe or Critical COVID-19: A Meta-Analysis. Tex. Heart Inst. J. 2022, 49, e207404. [Google Scholar] [CrossRef] [PubMed]
- DePace, N.L.; Colombo, J. Long-COVID Syndrome and the Cardiovascular System: A Review of Neurocardiologic Effects on Multiple Systems. Curr. Cardiol. Rep. 2022, 24, 1711–1726. [Google Scholar] [CrossRef]
- Fishman, B.; Goitein, O.; Berkovitch, A.; Rahav, G.; Matetzky, S. First report of myocarditis in two patients with COVID-19 Omicron variant: Case report. Eur. Heart J.—Case Rep. 2022, 6, ytac407. [Google Scholar] [CrossRef]
- Saleh, J.; Peyssonnaux, C.; Singh, K.K.; Edeas, M. Mitochondria and microbiota dysfunction in COVID-19 pathogenesis. Mitochondrion 2020, 54, 1–7. [Google Scholar] [CrossRef]
- Xavier, L.L.; Neves, P.F.R.; Paz, L.V.; Neves, L.T.; Bagatini, P.B.; Timmers, L.F.S.M.; Rasia-Filho, A.A.; Mestriner, R.G.; Wieck, A. Does Angiotensin II Peak in Response to SARS-CoV-2? Front. Immunol. 2021, 11, 577875. [Google Scholar] [CrossRef]
- Camargo, R.L.; Bombassaro, B.; Monfort-Pires, M.; Mansour, E.; Palma, A.C.; Ribeiro, L.C.; Ulaf, R.G.; Bernardes, A.F.; Nunes, T.A.; Agrela, M.V.; et al. Plasma Angiotensin II Is Increased in Critical Coronavirus Disease 2019. Front. Cardiovasc. Med. 2022, 9, 847809. [Google Scholar] [CrossRef]
- Xu, S.-W.; Ilyas, I.; Weng, J.-P. Endothelial dysfunction in COVID-19: An overview of evidence, biomarkers, mechanisms and potential therapies. Acta Pharmacol. Sin. 2023, 44, 695–709. [Google Scholar] [CrossRef]
- Lemarié, C.A.; Schiffrin, E.L. The angiotensin II type 2 receptor in cardiovascular disease. J. Renin-Angiotensin-Aldosterone Syst. 2010, 11, 19–31. [Google Scholar] [CrossRef] [PubMed]
- WHO. XBB.1.5 Rapid Risk Assessment, 11 January 2023; World Health Organization: Geneva, Switzerland, 2023; Available online: https://www.who.int/docs/default-source/coronaviruse/11jan2023_xbb15_rapid_risk_assessment.pdf (accessed on 16 July 2023).
- WHO. XBB.1.5 Updated Rapid Risk Assessment, 25 January 2023; World Health Organization: Geneva, Switzerland, 2023; Available online: https://www.who.int/docs/default-source/coronaviruse/25012023xbb.1.pdf?sfvrsn=c3956081_1 (accessed on 16 July 2023).
- WHO. XBB.1.5 Updated Risk Assessment, 24 February 2023; World Health Organization: Geneva, Switzerland, 2023; Available online: https://www.who.int/docs/default-source/coronaviruse/22022024xbb.1.5ra.pdf (accessed on 16 July 2023).
- Africa, N.I.D.S. Tracking SARS-CoV-2 Variants. National Institute for Communicable Diseases. 2023. Available online: https://www.nicd.ac.za/wp-content/uploads/2023/02/Update-of-SA-sequencing-data-from-GISAID-17-Feb-2023_Final.pdf (accessed on 16 July 2023).
- Iwu-Jaja, C.; Taukobong, S.; Rachida, S.; Ndlovu, N.; Macheke, M.; Howard, W.; Moonsamy, S.; Pocock, G.; Coetzee, L.; Mans, J.; et al. Detection, Quantitation and Genomic Sequencing at Sentinel Sites in South Africa, Co-Funded by the Water Research Commission, the Bill and Melinda Gates Foundation and the NICD City of Cape Town Health Department Wastewater-Based Epidemiology for SARS-CoV-2 Surveillance in South Africa. 2021. Available online: https://www.nicd.ac.za/diseases-a-z-index/disease- (accessed on 16 July 2023).
- Yue, C.; Song, W.; Wang, L.; Jian, F.; Chen, X.; Gao, F.; Shen, Z.; Wang, Y.; Wang, X.; Cao, Y. ACE2 binding and antibody evasion in enhanced transmissibility of XBB.1.5. Lancet Infect. Dis. 2023, 23, 278–280. [Google Scholar] [CrossRef] [PubMed]
- WHO. XBB.1.16 Updated Risk Assessment, 5 June 2023; World Health Organization: Geneva, Switzerland, 2023. [Google Scholar]
- Karyakarte, R.P.; Das, R.; Rajmane, M.V.; Dudhate, S.; Agarasen, J.; Pillai, P.; Chandankhede, P.M.; Labhshetwar, R.S.; Gadiyal, Y.; Kulkarni, P.P.; et al. Chasing SARS-CoV-2 XBB.1.16 Recombinant Lineage in India and the Clinical Profile of XBB.1.16 Cases in Maharashtra, India. Cureus 2023, 15, e39816. [Google Scholar] [CrossRef] [PubMed]
- DeGrasse, D.C.; Black, S.D. The Rise of SARS-CoV-2 (COVID-19) Omicron Subvariant Pathogenicity. Cureus 2023, 15, e40148. [Google Scholar] [CrossRef]
- WHO. Coronavirus Disease (COVID-19) Pandemic; World Health Organization: Geneva, Switzerland, 2023. [Google Scholar]
- Patel, K.; Hipskind, J.E. Cardiac Arrest. In StatPearls [Internet]; National Center for Biotechnology Information: Bethesda, MD, USA, 2023. Available online: https://www.ncbi.nlm.nih.gov/books/NBK534866/ (accessed on 16 July 2023).
- Chugh, H.S.; Sargsyan, A.; Nakamura, K.; Uy-Evanado, A.; Dizon, B.; Norby, F.L.; Young, C.; Hadduck, K.; Jui, J.; Shepherd, D.; et al. Sudden cardiac arrest during the COVID-19 pandemic: A two-year prospective evaluation in a North American community. HeartRhythm 2023, 20, 947–955. [Google Scholar] [CrossRef]
- Davis, H.E.; McCorkell, L.; Vogel, J.M.; Topol, E.J. Long COVID: Major findings, mechanisms and recommendations. Nat. Rev. Microbiol. 2023, 21, 133–146. [Google Scholar] [CrossRef]
- Maitz, T.; Parfianowicz, D.; Vojtek, A.; Rajeswaran, Y.; Vyas, A.V.; Gupta, R. COVID-19 Cardiovascular Connection: A Review of Cardiac Manifestations in COVID-19 Infection and Treatment Modalities. Curr. Probl. Cardiol. 2023, 48, 101186. [Google Scholar] [CrossRef]
- Otifi, H.M.; Adiga, B.K. Endothelial Dysfunction in COVID-19 Infection. Am. J. Med. Sci. 2022, 363, 281–287. [Google Scholar] [CrossRef]
- Nappi, F.; Giacinto, O.; Ellouze, O.; Nenna, A.; Singh, S.S.A.; Chello, M.; Bouzguenda, A.; Copie, X. Association between COVID-19 Diagnosis and Coronary Artery Thrombosis: A Narrative Review. Biomedicines 2022, 10, 702. [Google Scholar] [CrossRef]
- Rinaldi, R.; Basile, M.; Salzillo, C.; Grieco, D.L.; Caffè, A.; Masciocchi, C.; Lilli, L.; Damiani, A.; La Vecchia, G.; Iannaccone, G.; et al. Myocardial Injury Portends a Higher Risk of Mortality and Long-Term Cardiovascular Sequelae after Hospital Discharge in COVID-19 Survivors. J. Clin. Med. 2022, 11, 5964. [Google Scholar] [CrossRef]
- CDC. COVID-19: Medical Conditions. Center for Disease Control and Prevention May 2023. Available online: https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/people-with-medical-conditions.html (accessed on 16 July 2023).
- Jayaraman, R.; Reinier, K.; Nair, S.; Aro, A.L.; Uy-Evanado, A.; Rusinaru, C.; Stecker, E.C.; Gunson, K.; Jui, J.; Chugh, S.S.; et al. Risk Factors of Sudden Cardiac Death in the Young. Circulation 2018, 137, 1561–1570. [Google Scholar] [CrossRef] [PubMed]
- Baldi, E.; Sechi, G.M.; Mare, C.; Canevari, F.; Brancaglione, A.; Primi, R.; Klersy, C.; Palo, A.; Contri, E.; Ronchi, V.; et al. Out-of-Hospital Cardiac Arrest during the COVID-19 Outbreak in Italy. N. Engl. J. Med. 2020, 383, 496–498. [Google Scholar] [CrossRef] [PubMed]
- Hayek, S.S.; Brenner, S.K.; Azam, T.U.; Shadid, H.R.; Anderson, E.; Berlin, H.; Pan, M.; Meloche, C.; Feroz, R.; O’hayer, P.; et al. In-hospital cardiac arrest in critically ill patients with COVID-19: Multicenter cohort study. BMJ 2020, 371, m3513. [Google Scholar] [CrossRef] [PubMed]
- COVID.org. In Long COVID Terms and Definitions Development Explained; Department of Health and Human Services: Washington, DC, USA, 2023.
- Lam, I.C.H.; Wong, C.K.H.; Zhang, R.; Chui, C.S.L.; Lai, F.T.T.; Li, X.; Chan, E.W.Y.; Luo, H.; Zhang, Q.; Man, K.K.C.; et al. Long-term post-acute sequelae of COVID-19 infection: A retrospective, multi-database cohort study in Hong Kong and the UK. EClinicalMedicine 2023, 60, 102000. [Google Scholar] [CrossRef]
- Lopez-Leon, S.; Wegman-Ostrosky, T.; Perelman, C.; Sepulveda, R.; Rebolledo, P.A.; Cuapio, A.; Villapol, S. More than 50 long-term effects of COVID-19: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 16144. [Google Scholar] [CrossRef]
- Davido, B.; Seang, S.; Tubiana, R.; de Truchis, P. Post–COVID-19 chronic symptoms: A postinfectious entity? Clin. Microbiol. Infect. 2020, 26, 1448–1449. [Google Scholar] [CrossRef]
- Toori, K.U.; Qureshi, M.A.; Chaudhry, A. Lymphopenia: A useful predictor of COVID-19 disease severity and mortality. Pak. J. Med. Sci. 2021, 37, 1984–1988. [Google Scholar] [CrossRef]
- Alqahtani, M.S.; Abbas, M.; Alsabaani, A.; Alqarni, A.; Almohiy, H.M.; Alsawqaee, E.; Alshahrani, R.; Alshahrani, S. The Potential Impact of COVID-19 Virus on the Heart and the Circulatory System. Infect. Drug Resist. 2022, 2022, 1175–1189. [Google Scholar] [CrossRef]
- Raman, B.; Bluemke, D.A.; Lüscher, T.F.; Neubauer, S. Long COVID: Post-acute sequelae of COVID-19 with a cardiovascular focus. Eur. Heart J. 2022, 43, 1157–1172. [Google Scholar] [CrossRef]
- Puntmann, V.O.; Carerj, M.L.; Wieters, I.; Fahim, M.; Arendt, C.; Hoffmann, J.; Shchendrygina, A.; Escher, F.; Vasa-Nicotera, M.; Zeiher, A.M.; et al. Outcomes of Cardiovascular Magnetic Resonance Imaging in Patients Recently Recovered From Coronavirus Disease 2019 (COVID-19). JAMA Cardiol. 2020, 5, 1265. [Google Scholar] [CrossRef]
- Xie, Y.; Choi, T.; Al-Aly, Z. Association of Treatment With Nirmatrelvir and the Risk of Post–COVID-19 Condition. JAMA Intern. Med. 2023, 183, 554–564. [Google Scholar] [CrossRef] [PubMed]
- Novotná, E.; Filipová, P.; Vonke, I.; Kuta, B.; Chrdle, A. Rapid Progression of COVID-19-Associated Fatal Capillary Leak Syndrome. Infect. Dis. Rep. 2022, 14, 884–888. [Google Scholar] [CrossRef] [PubMed]
- Choi, G.-J.; Baek, S.H.; Kim, J.; Kim, J.H.; Kwon, G.-Y.; Kim, D.K.; Jung, Y.H.; Kim, S. Fatal Systemic Capillary Leak Syndrome after SARS-CoV-2Vaccination in Patient with Multiple Myeloma. Emerg. Infect. Dis. 2021, 27, 2973–2975. [Google Scholar] [CrossRef] [PubMed]
- Bowe, B.; Xie, Y.; Al-Aly, Z. Acute and postacute sequelae associated with SARS-CoV-2 reinfection. Nat. Med. 2022, 28, 2398–2405. [Google Scholar] [CrossRef]
- CDC. Trends in Laboratory-Confirmed SARS-CoV-2 Reinfections and Associated Hospitalizations and Deaths Among Adults Aged ≥18 Years—18 U.S. Jurisdictions, September 2021–December 2022; Center for Disease Control and Prevention: Atlanta, GA, USA, 2023.

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vishwakarma, N.; Goud, R.B.; Tirupattur, M.P.; Katwa, L.C. The Eye of the Storm: Investigating the Long-Term Cardiovascular Effects of COVID-19 and Variants. Cells 2023, 12, 2154. https://doi.org/10.3390/cells12172154
Vishwakarma N, Goud RB, Tirupattur MP, Katwa LC. The Eye of the Storm: Investigating the Long-Term Cardiovascular Effects of COVID-19 and Variants. Cells. 2023; 12(17):2154. https://doi.org/10.3390/cells12172154
Chicago/Turabian StyleVishwakarma, Nandini, Reshma B. Goud, Myna Prakash Tirupattur, and Laxmansa C. Katwa. 2023. "The Eye of the Storm: Investigating the Long-Term Cardiovascular Effects of COVID-19 and Variants" Cells 12, no. 17: 2154. https://doi.org/10.3390/cells12172154
APA StyleVishwakarma, N., Goud, R. B., Tirupattur, M. P., & Katwa, L. C. (2023). The Eye of the Storm: Investigating the Long-Term Cardiovascular Effects of COVID-19 and Variants. Cells, 12(17), 2154. https://doi.org/10.3390/cells12172154