


Monoclonal Antibodies against Calcitonin Gene-Related Peptide for Migraine Prophylaxis: A Systematic Review of Real-World Data



Abstract
1. Introduction
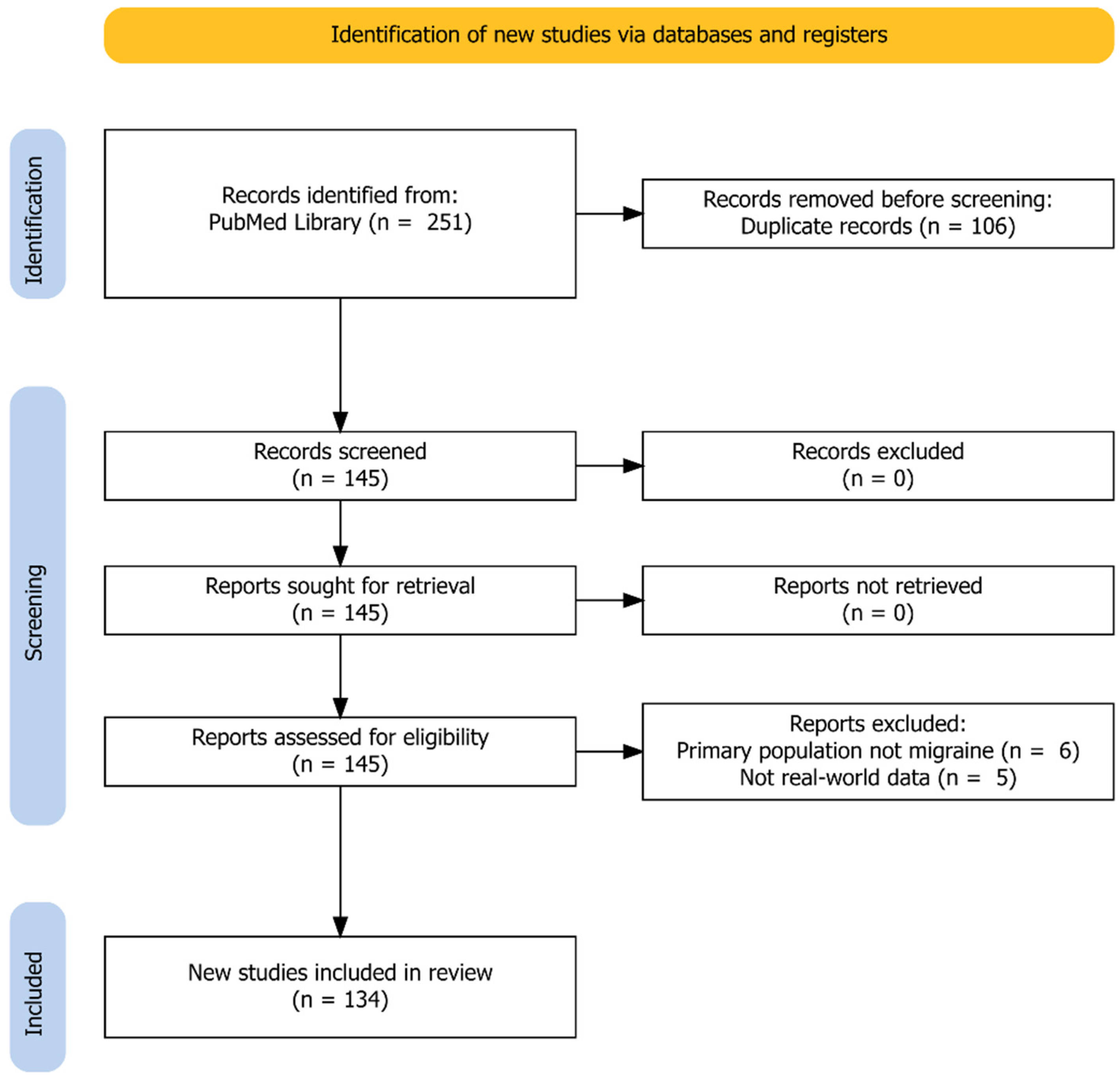
2. Methods
2.1. Search Methods
2.2. Selection Criteria
2.3. Review Preparation and Statistics
3. Study Characteristics
4. Pharmacoepidemiologic Studies
4.1. Acute Medication
4.2. Prophylactic Medication Apart from Anti-CGRP-mAbs
4.3. Adherence and Persistence
4.4. Health Care Resource Utilization
4.5. Sick-Leave and Impact of Migraine
4.6. Summary
5. Clinic-Based Studies
5.1. Study Design
5.2. Patients
5.3. Anti-CGRP-mAbs
5.4. Effectiveness
5.5. Concomitant Pharmacoprophylaxis
5.6. Treatment Break
5.7. Switching to Another Anti-CGRP-mAb
5.8. Discontinuation of Antibody Treatment
5.9. Adverse Events
5.10. Severe Adverse Events
5.11. Summary
6. Case Reports
- i.
- Improvement of a symptom or comorbid condition;
- ii.
- Effectiveness and no adverse events under special circumstances;
- iii.
- Adverse events in otherwise healthy individuals;
- iv.
- Adverse events because of possible drug interactions, or potentiation of side effects;
- v.
- Deterioration of preexisting disorder.
Summary
7. Other Articles
8. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Hepp, Z.; Bloudek, L.M.; Varon, S.F. Systematic Review of Migraine Prophylaxis Adherence and Persistence. J. Manag. Care Pharm. 2014, 20, 22–33. [Google Scholar] [CrossRef] [PubMed]
- Ohlsson, L.; Haanes, K.A.; Kronvall, E.; Xu, C.; Snellman, J.; Edvinsson, L. Erenumab (AMG 334), a monoclonal antagonist antibody against the canonical CGRP receptor, does not impair vasodilatory or contractile responses to other vasoactive agents in human isolated cranial arteries. Cephalalgia 2019, 39, 1745–1752. [Google Scholar] [CrossRef] [PubMed]
- Rubio-Beltrán, E.; Labastida-Ramírez, A.; Haanes, K.A.; Bogaerdt, A.V.D.; Bogers, A.J.; Dirven, C.; Danser, A.J.; Xu, C.; Snellman, J.; MaassenVanDenBrink, A. Characterisation of vasodilatory responses in the presence of the CGRP receptor antibody erenumab in human isolated arteries. Cephalalgia 2019, 39, 1735–1744. [Google Scholar] [CrossRef] [PubMed]
- Dodick, D.W.; Ashina, M.; Brandes, J.L.; Kudrow, D.; Lanteri-Minet, M.; Osipova, V.; Palmer, K.; Picard, H.; Mikol, D.D.; Lenz, R.A. ARISE: A Phase 3 randomized trial of erenumab for episodic migraine. Cephalalgia 2018, 38, 1026–1037. [Google Scholar] [CrossRef] [PubMed]
- Goadsby, P.J.; Reuter, U.; Hallström, Y.; Broessner, G.; Bonner, J.H.; Zhang, F.; Sapra, S.; Picard, H.; Mikol, D.D.; Lenz, R.A. A Controlled Trial of Erenumab for Episodic Migraine. N. Engl. J. Med. 2017, 377, 2123–2132. [Google Scholar] [CrossRef] [PubMed]
- Stauffer, V.L.; Dodick, D.W.; Zhang, Q.; Carter, J.N.; Ailani, J.; Conley, R.R. Evaluation of Galcanezumab for the Prevention of Episodic Migraine: The EVOLVE-1 Randomized Clinical Trial. JAMA Neurol. 2018, 75, 1080–1088. [Google Scholar] [CrossRef] [PubMed]
- Dodick, D.W.; Silberstein, S.D.; Bigal, M.E.; Yeung, P.P.; Goadsby, P.J.; Blankenbiller, T.; Grozinski-Wolff, M.; Yang, R.; Ma, Y.; Aycardi, E. Effect of Fremanezumab Compared With Placebo for Prevention of Episodic Migraine: A randomized clinical trial. JAMA 2018, 319, 1999–2008. [Google Scholar] [CrossRef]
- Ashina, M.; Saper, J.; Cady, R.; Schaeffler, B.A.; Biondi, D.M.; Hirman, J.; Pederson, S.; Allan, B.; Smith, J. Eptinezumab in episodic migraine: A randomized, double-blind, placebo-controlled study (PROMISE-1). Cephalalgia 2020, 40, 241–254. [Google Scholar] [CrossRef] [PubMed]
- Lipton, R.B.; Goadsby, P.J.; Smith, J.; Schaeffler, B.A.; Biondi, D.M.; Hirman, J.; Pederson, S.; Allan, B.; Cady, R. Efficacy and safety of eptinezumab in patients with chronic migraine: PROMISE-2. Neurology 2020, 94, e1365–e1377. [Google Scholar] [CrossRef]
- Silberstein, S.D.; Dodick, D.W.; Bigal, M.E.; Yeung, P.P.; Goadsby, P.J.; Blankenbiller, T.; Grozinski-Wolff, M.; Yang, R.; Ma, Y.; Aycardi, E. Fremanezumab for the Preventive Treatment of Chronic Migraine. N. Engl. J. Med. 2017, 377, 2113–2122. [Google Scholar] [CrossRef]
- Tepper, S.; Ashina, M.; Reuter, U.; Brandes, J.L.; Doležil, D.; Silberstein, S.; Winner, P.; Leonardi, D.; Mikol, D.; Lenz, R. Safety and efficacy of erenumab for preventive treatment of chronic migraine: A randomised, double-blind, placebo-controlled phase 2 trial. Lancet Neurol. 2017, 16, 425–434. [Google Scholar] [CrossRef] [PubMed]
- Detke, H.C.; Goadsby, P.J.; Wang, S.; Friedman, D.I.; Selzler, K.J.; Aurora, S.K. Galcanezumab in chronic migraine: The randomized, double-blind, placebo-controlled REGAIN study. Neurology 2018, 91, e2211–e2221. [Google Scholar] [CrossRef] [PubMed]
- Reuter, U.; Goadsby, P.J.; Lanteri-Minet, M.; Wen, S.; Hours-Zesiger, P.; Ferrari, M.D.; Klatt, J. Efficacy and tolerability of erenumab in patients with episodic migraine in whom two-to-four previous preventive treatments were unsuccessful: A randomised, double-blind, placebo-controlled, phase 3b study. Lancet 2018, 392, 2280–2287. [Google Scholar] [CrossRef] [PubMed]
- Goadsby, P.J.; Paemeleire, K.; Broessner, G.; Brandes, J.; Klatt, J.; Zhang, F.; Picard, H.; Lenz, R.; Mikol, D.D. Efficacy and safety of erenumab (AMG334) in episodic migraine patients with prior preventive treatment failure: A subgroup analysis of a randomized, double-blind, placebo-controlled study. Cephalalgia 2019, 39, 817–826. [Google Scholar] [CrossRef]
- Mulleners, W.M.; Kim, B.-K.; Láinez, M.J.A.; Lanteri-Minet, M.; Pozo-Rosich, P.; Wang, S.; Tockhorn-Heidenreich, A.; Aurora, S.K.; Nichols, R.M.; Yunes-Medina, L.; et al. Safety and efficacy of galcanezumab in patients for whom previous migraine preventive medication from two to four categories had failed (CONQUER): A multicentre, randomised, double-blind, placebo-controlled, phase 3b trial. Lancet Neurol. 2020, 19, 814–825. [Google Scholar] [CrossRef]
- Ferrari, M.D.; Diener, H.C.; Ning, X.; Galic, M.; Cohen, J.M.; Yang, R.; Mueller, M.; Ahn, A.H.; Schwartz, Y.C.; Grozinski-Wolff, M.; et al. Fremanezumab versus placebo for migraine prevention in patients with documented failure to up to four migraine preventive medication classes (FOCUS): A randomised, double-blind, placebo-controlled, phase 3b trial. Lancet 2019, 394, 1030–1040. [Google Scholar] [CrossRef]
- Smitherman, T.A.; Tietjen, G.E.; Schuh, K.; Skljarevski, V.; Lipsius, S.; D’Souza, D.N.; Pearlman, E.M. Efficacy of Galcanezumab for Migraine Prevention in Patients With a Medical History of Anxiety and/or Depression: A Post Hoc Analysis of the Phase 3, Randomized, Double-Blind, Placebo-Controlled REGAIN, and Pooled EVOLVE-1 and EVOLVE-2 Studies. Headache 2020, 60, 2202–2219. [Google Scholar] [CrossRef]
- Lipton, R.B.; Cohen, J.M.; Galic, M.; Seminerio, M.J.; Yeung, P.P.; Aycardi, E.; Bigal, M.E.; Bibeau, K.; Buse, D.C. Effects of fremanezumab in patients with chronic migraine and comorbid depression: Subgroup analysis of the randomized HALO CM study. Headache 2021, 61, 662–672. [Google Scholar] [CrossRef]
- Tepper, S.J.; Diener, H.-C.; Ashina, M.; Brandes, J.L.; Friedman, D.I.; Reuter, U.; Cheng, S.; Nilsen, J.; Leonardi, D.K.; Lenz, R.A.; et al. Erenumab in chronic migraine with medication overuse: Subgroup analysis of a randomized trial. Neurology 2019, 92, e2309–e2320. [Google Scholar] [CrossRef]
- Dodick, D.W.; Doty, E.G.; Aurora, S.K.; Ruff, D.D.; Stauffer, V.L.; Jedynak, J.; Dong, Y.; Pearlman, E.M. Medication overuse in a subgroup analysis of phase 3 placebo-controlled studies of galcanezumab in the prevention of episodic and chronic migraine. Cephalalgia 2021, 41, 340–352. [Google Scholar] [CrossRef]
- Silberstein, S.D.; Cohen, J.M.; Seminerio, M.J.; Yang, R.; Ashina, S.; Katsarava, Z. The impact of fremanezumab on medication overuse in patients with chronic migraine: Subgroup analysis of the HALO CM study. J. Headache Pain 2020, 21, 114. [Google Scholar] [CrossRef] [PubMed]
- Diener, H.; Marmura, M.J.; Tepper, S.J.; Cowan, R.; Starling, A.J.; Diamond, M.L.; Hirman, J.; Mehta, L.; Brevig, T.; Sperling, B.; et al. Efficacy, tolerability, and safety of eptinezumab in patients with a dual diagnosis of chronic migraine and medication-overuse headache: Subgroup analysis of PROMISE-2. Headache 2021, 61, 125–136. [Google Scholar] [CrossRef] [PubMed]
- Lipton, R.B.; Tepper, S.J.; Reuter, U.; Silberstein, S.; Stewart, W.F.; Nilsen, J.; Leonardi, D.K.; Desai, P.; Cheng, S.; Mikol, D.D.; et al. Erenumab in chronic migraine: Patient-reported outcomes in a randomized double-blind study. Neurology 2019, 92, e2250–e2260. [Google Scholar] [CrossRef] [PubMed]
- Lipton, R.B.; Cohen, J.M.; Gandhi, S.K.; Yang, R.; Yeung, P.P.; Buse, D.C. Effect of fremanezumab on quality of life and productivity in patients with chronic migraine. Neurology 2020, 95, e878–e888. [Google Scholar] [CrossRef]
- Ford, J.H.; Ayer, D.W.; Zhang, Q.; Carter, J.N.; Leroux, E.; Skljarevski, V.; Aurora, S.K.; Tockhorn-Heidenreich, A.; Lipton, R.B. Two randomized migraine studies of galcanezumab: Effects on patient functioning and disability. Neurology 2019, 93, e508–e517. [Google Scholar] [CrossRef]
- Lipton, R.B.; Charleston, L.; Tassorelli, C.; Brevig, T.; Hirman, J.; Cady, R. Patient-reported outcomes, health-related quality of life, and acute medication use in patients with a ≥75% response to eptinezumab: Subgroup pooled analysis of the PROMISE trials. J. Headache Pain 2022, 23, 23. [Google Scholar] [CrossRef]
- Ashina, M.; Goadsby, P.J.; Reuter, U.; Silberstein, S.; Dodick, D.W.; Xue, F.; Zhang, F.; Lima, G.P.d.S.; Cheng, S.; Mikol, D.D. Long-term efficacy and safety of erenumab in migraine prevention: Results from a 5-year, open-label treatment phase of a randomized clinical trial. Eur. J. Neurol. 2021, 28, 1716–1725. [Google Scholar] [CrossRef]
- Goadsby, P.J.; Silberstein, S.D.; Yeung, P.P.; Cohen, J.M.; Ning, X.; Yang, R.; Dodick, D.W. Long-term safety, tolerability, and efficacy of fremanezumab in migraine: A randomized study. Neurology 2020, 95, e2487–e2499. [Google Scholar] [CrossRef]
- Camporeale, A.; Kudrow, D.; Sides, R.; Wang, S.; Van Dycke, A.; Selzler, K.J.; Stauffer, V.L. A phase 3, long-term, open-label safety study of Galcanezumab in patients with migraine. BMC Neurol. 2018, 18, 188. [Google Scholar] [CrossRef]
- Kudrow, D.; Cady, R.K.; Allan, B.; Pederson, S.M.; Hirman, J.; Mehta, L.R.; Schaeffler, B.A. Long-term safety and tolerability of eptinezumab in patients with chronic migraine: A 2-year, open-label, phase 3 trial. BMC Neurol. 2021, 21, 126. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [PubMed]
- Autio, H.; Purmonen, T.; Kurki, S.; Mocevic, E.; Korolainen, M.A.; Tuominen, S.; Lassenius, M.I.; Nissilä, M. Erenumab Decreases Headache-Related Sick Leave Days and Health Care Visits: A Retrospective Real-World Study in Working Patients with Migraine. Neurol. Ther. 2022, 11, 223–235. [Google Scholar] [CrossRef] [PubMed]
- Chandler, D.; Szekely, C.; Aggarwal, S.; Cyprien, L.; Bensink, M. Migraine Characteristics, Comorbidities, Healthcare Resource Utilization, and Associated Costs of Early Users of Erenumab in the USA: A Retrospective Cohort Study Using Administrative Claims Data. Pain Ther. 2021, 10, 1551–1566. [Google Scholar] [CrossRef] [PubMed]
- Gladstone, J.; Chhibber, S.; Minhas, J.; Neish, C.S.; Power, G.S.; Lan, Z.; Rochdi, D.; Lanthier-Martel, J.; Bastien, N. Real-world persistence of erenumab for preventive treatment of chronic and episodic migraine: Retrospective real-world study. Headache 2022, 62, 78–88. [Google Scholar] [CrossRef]
- Hines, D.M.; Shah, S.; Multani, J.K.; Wade, R.L.; Buse, D.C.; Bensink, M. Erenumab patient characteristics, medication adherence, and treatment patterns in the United States. Headache 2021, 61, 590–602. [Google Scholar] [CrossRef]
- McAllister, P.; Lamerato, L.; Krasenbaum, L.J.; Cohen, J.M.; Tangirala, K.; Thompson, S.; Driessen, M.; Casciano, J.; Dotiwala, Z.; Mauskop, A. Real-world impact of fremanezumab on migraine symptoms and resource utilization in the United States. J. Headache Pain 2021, 22, 156. [Google Scholar] [CrossRef]
- Tepper, S.J.; Fang, J.; Zhou, L.; Shen, Y.; Vo, P.; Abdrabboh, A.; Glassberg, M.B.; Ferraris, M. Effectiveness of erenumab and onabotulinumtoxinA on acute medication usage and health care resource utilization as migraine prevention in the United States. J. Manag. Care Spéc. Pharm. 2021, 27, 1157–1170. [Google Scholar] [CrossRef]
- Tepper, S.J.; Fang, J.; Vo, P.; Shen, Y.; Zhou, L.; Abdrabboh, A.; Glassberg, M.; Ferraris, M. Impact of erenumab on acute medication usage and health care resource utilization among migraine patients: A US claims database study. J. Headache Pain 2021, 22, 27. [Google Scholar] [CrossRef]
- Varnado, O.J.; Manjelievskaia, J.; Ye, W.; Perry, A.; Schuh, K.; Wenzel, R. Treatment Patterns for Calcitonin Gene-Related Peptide Monoclonal Antibodies Including Galcanezumab versus Conventional Preventive Treatments for Migraine: A Retrospective US Claims Study. Patient Prefer. Adherence 2022, 16, 821–839. [Google Scholar] [CrossRef]
- Alex, A.; Vaughn, C.; Rayhill, M. Safety and Tolerability of 3 CGRP Monoclonal Antibodies in Practice: A Retrospective Cohort Study. Headache 2020, 60, 2454–2462. [Google Scholar] [CrossRef]
- Armanious, M.; Khalil, N.; Lu, Y.; Jimenez-Sanders, R. Erenumab and Onabotulinumtoxin A Combination Therapy for the Prevention of Intractable Chronic Migraine without Aura: A Retrospective Analysis. J. Pain Palliat. Care Pharmacother. 2021, 35, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Baraldi, C.; Castro, F.L.; Cainazzo, M.M.; Pani, L.; Guerzoni, S. Predictors of response to erenumab after 12 months of treatment. Brain Behav. 2021, 11, e2260. [Google Scholar] [CrossRef] [PubMed]
- Belvís, R.; Irimia, P.; Pozo-Rosich, P.; González-Oria, C.; Cano, A.; Viguera, J.; Sánchez, B.; Molina, F.; Beltrán, I.; Oterino, A.; et al. MAB-MIG: Registry of the spanish neurological society of erenumab for migraine prevention. J. Headache Pain 2021, 22, 74. [Google Scholar] [CrossRef] [PubMed]
- Blumenfeld, A.M.; Frishberg, B.M.; Schim, J.D.; Iannone, A.; Schneider, G.; Yedigarova, L.; Adams, A.M. Real-World Evidence for Control of Chronic Migraine Patients Receiving CGRP Monoclonal Antibody Therapy Added to Onabotulinumtoxin A: A Retrospective Chart Review. Pain Ther. 2021, 10, 809–826. [Google Scholar] [CrossRef] [PubMed]
- Cainazzo, M.M.; Baraldi, C.; Ferrari, A.; Castro, F.L.; Pani, L.; Guerzoni, S. Erenumab for the preventive treatment of chronic migraine complicated with medication overuse headache: An observational, retrospective, 12-month real-life study. Neurol. Sci. 2021, 42, 4193–4202. [Google Scholar] [CrossRef] [PubMed]
- Cohen, F.; Armand, C.; Lipton, R.B.; Vollbracht, S. Efficacy and Tolerability of Calcitonin Gene–Related Peptide–Targeted Monoclonal Antibody Medications as Add-on Therapy to Onabotulinumtoxin A in Patients with Chronic Migraine. Pain Med. 2021, 22, 1857–1863. [Google Scholar] [CrossRef]
- Dapkutė, A.; Vainauskienė, J.; Ryliškienė, K. Patient-reported outcomes of migraine treatment with erenumab: Results from a national patient survey. Neurol. Sci. 2022, 43, 3305–3312. [Google Scholar] [CrossRef]
- Dinh, B.B.K.; Aziz, W.H.; Terruzzi, A.; Krieger, D.W. Initial experience with novel CGRP-receptor inhibitor therapy in Migraine in the United Arab Emirates: A retrospective observational study. BMC Neurol. 2021, 21, 486. [Google Scholar] [CrossRef]
- Driessen, M.T.; Cohen, J.M.; Patterson-Lomba, O.; Thompson, S.F.; Seminerio, M.; Carr, K.; Totev, T.I.; Sun, R.; Yim, E.; Mu, F.; et al. Real-world effectiveness of fremanezumab in migraine patients initiating treatment in the United States: Results from a retrospective chart study. J. Headache Pain 2022, 23, 47. [Google Scholar] [CrossRef]
- Eghtesadi, M.; Leroux, E.; Pagé, G. Real-Life Response to Erenumab in a Therapy-Resistant Case Series of Migraine Patients From the Province of Québec, Eastern Canada. Clin. Drug Investig. 2021, 41, 733–739. [Google Scholar] [CrossRef]
- Faust, E.; Pivneva, I.; Yang, K.; Betts, K.A.; Ahmed, Z.; Joshi, S.; Hogan, R.; Blumenfeld, A.; Schim, J.; Feoktistov, A.; et al. Real-World Treatment Profiles, Clinical Outcomes, and Healthcare Resource Utilization of Patients with Migraine Prescribed Erenumab: A Multicenter Chart-Review Study of US Headache Centers. Neurol. Ther. 2021, 10, 293–306. [Google Scholar] [CrossRef] [PubMed]
- Gantenbein, A.R.; Agosti, R.; Gobbi, C.; Flügel, D.; Schankin, C.J.; Viceic, D.; Zecca, C.; Pohl, H. Impact on monthly migraine days of discontinuing anti-CGRP antibodies after one year of treatment—A real-life cohort study. Cephalalgia 2021, 41, 1181–1186. [Google Scholar] [CrossRef]
- Kanaan, S.; Hettie, G.; Loder, E.; Burch, R. Real-world effectiveness and tolerability of erenumab: A retrospective cohort study. Cephalalgia 2020, 40, 1511–1522. [Google Scholar] [CrossRef] [PubMed]
- López-Bravo, A.; Oliveros-Cid, A.; Sevillano-Orte, L. Treatment satisfaction with calcitonin gene-related peptide monoclonal antibodies as a new patient-reported outcome measure: A real-life experience in migraine. Acta Neurol. Scand. 2022, 145, 669–675. [Google Scholar] [CrossRef] [PubMed]
- Maraia, Z.; Ricci, D.; Rocchi, M.B.L.; Moretti, A.; Bufarini, C.; Cavaliere, A.; Peverini, M. Real-Life Analysis with Erenumab: First Target Therapy in the Episodic and Chronic Migraine’s Prophylaxis. J. Clin. Med. 2021, 10, 4425. [Google Scholar] [CrossRef] [PubMed]
- Mechtler, L.; Saikali, N.; McVige, J.; Hughes, O.; Traut, A.; Adams, A.M. Real-World Evidence for the Safety and Efficacy of CGRP Monoclonal Antibody Therapy Added to OnabotulinumtoxinA Treatment for Migraine Prevention in Adult Patients With Chronic Migraine. Front. Neurol. 2022, 12. [Google Scholar] [CrossRef]
- Nandyala, A.S.; Suri, H.; Dougherty, C.O.; Ailani, J. A retrospective evaluation of the combination of erenumab and onabotulinum toxin A for the prevention of chronic migraine. Clin. Neurol. Neurosurg. 2022, 215, 107200. [Google Scholar] [CrossRef]
- Ornello, R.; Baraldi, C.; Guerzoni, S.; Lambru, G.; Fuccaro, M.; Raffaelli, B.; Gendolla, A.; Barbanti, P.; Aurilia, C.; Cevoli, S.; et al. Gender Differences in 3-Month Outcomes of Erenumab Treatment—Study on Efficacy and Safety of Treatment With Erenumab in Men. Front. Neurol. 2021, 12, 774341. [Google Scholar] [CrossRef]
- Ornello, R.; Baraldi, C.; Guerzoni, S.; Lambru, G.; Andreou, A.P.; Raffaelli, B.; Gendolla, A.; Barbanti, P.; Aurilia, C.; Egeo, G.; et al. Comparing the relative and absolute effect of erenumab: Is a 50% response enough? Results from the ESTEEMen study. J. Headache Pain 2022, 23, 38. [Google Scholar] [CrossRef]
- Ornello, R.; Frattale, I.; Caponnetto, V.; De Matteis, E.; Pistoia, F.; Sacco, S. Menstrual Headache in Women with Chronic Migraine Treated with Erenumab: An Observational Case Series. Brain Sci. 2021, 11, 370. [Google Scholar] [CrossRef]
- Ornello, R.; Casalena, A.; Frattale, I.; Gabriele, A.; Affaitati, G.; Giamberardino, M.A.; Assetta, M.; Maddestra, M.; Marzoli, F.; Viola, S.; et al. Real-life data on the efficacy and safety of erenumab in the Abruzzo region, central Italy. J. Headache Pain 2020, 21, 32. [Google Scholar] [CrossRef] [PubMed]
- Overeem, L.H.; Peikert, A.; Hofacker, M.D.; Kamm, K.; Ruscheweyh, R.; Gendolla, A.; Raffaelli, B.; Reuter, U.; Neeb, L. Effect of antibody switch in non-responders to a CGRP receptor antibody treatment in migraine: A multi-center retrospective cohort study. Cephalalgia 2022, 42, 291–301. [Google Scholar] [CrossRef] [PubMed]
- Raffaelli, B.; Kalantzis, R.; Mecklenburg, J.; Overeem, L.H.; Neeb, L.; Gendolla, A.; Reuter, U. Erenumab in Chronic Migraine Patients Who Previously Failed Five First-Line Oral Prophylactics and Onabotulinumtoxin A: A Dual-Center Retrospective Observational Study. Front. Neurol. 2020, 11, 417. [Google Scholar] [CrossRef] [PubMed]
- Robblee, J.; Devick, K.L.; Mendez, N.; Potter, J.; Slonaker, J.; Starling, A.J. Real-World Patient Experience With Erenumab for the Preventive Treatment of Migraine. Headache 2020, 60, 2014–2025. [Google Scholar] [CrossRef]
- Ruiz, I.P.; Ferrández, J.S.-R.; Fonfría, A.C.; García, T.M. Early Experiences in Switching between Monoclonal Antibodies in Patients with Nonresponsive Migraine in Spain: A Case Series. Eur. Neurol. 2022, 85, 132–135. [Google Scholar] [CrossRef]
- Scheffler, A.; Schenk, H.; Wurthmann, S.; Nsaka, M.; Kleinschnitz, C.; Glas, M.; Holle, D. CGRP antibody therapy in patients with drug resistant migraine and chronic daily headache: A real-world experience. J. Headache Pain 2021, 22, 111. [Google Scholar] [CrossRef]
- Scheffler, A.; Messel, O.; Wurthmann, S.; Nsaka, M.; Kleinschnitz, C.; Glas, M.; Naegel, S.; Holle, D. Erenumab in highly therapy-refractory migraine patients: First German real-world evidence. J. Headache Pain 2020, 21, 84. [Google Scholar] [CrossRef]
- Sette, L.; Caponnetto, V.; Ornello, R.; Nežádal, T.; Čtrnáctá, D.; Šípková, J.; Matoušová, Z.; Sacco, S. Acute Medication Use in Patients With Migraine Treated With Monoclonal Antibodies Acting on the CGRP Pathway: Results From a Multicenter Study and Proposal of a New Index. Front. Neurol. 2022, 13, 846717. [Google Scholar] [CrossRef]
- Storch, P.; Burow, P.; Möller, B.; Kraya, T.; Heintz, S.; Politz, N.; Naegel, S. Pooled retrospective analysis of 70 mg erenumab in episodic and chronic migraine: A two tertiary headache centers experience during clinical practice. Acta Neurol. Belg. 2022, 122, 931–937. [Google Scholar] [CrossRef]
- Toni, T.; Tamanaha, R.; Newman, B.; Liang, Y.; Lee, J.; Carrazana, E.; Vajjala, V.; Viereck, J.; Liow, K.K. Effectiveness of dual migraine therapy with CGRP inhibitors and onabotulinumtoxin A injections: Case series. Neurol. Sci. 2021, 42, 5373–5376. [Google Scholar] [CrossRef]
- Viudez-Martínez, A.; Pascual-Carrasco, A.; Beltrán-Blasco, I.; Hernandez-Lorido, R.; de Apodaca, R.F.R. Effectiveness and safety of erenumab and galcanezumab in the prevention of chronic and episodic migraine: A retrospective cohort study. J. Clin. Pharm. Ther. 2022, 47, 814–823. [Google Scholar] [CrossRef] [PubMed]
- Barbanti, P.; Aurilia, C.; Egeo, G.; Fofi, L. Erenumab: From scientific evidence to clinical practice—The first Italian real-life data. Neurol. Sci. 2019, 40, 177–179. [Google Scholar] [CrossRef] [PubMed]
- Barbanti, P.; Aurilia, C.; Egeo, G.; Fofi, L.; Cevoli, S.; Colombo, B.; Filippi, M.; Frediani, F.; Bono, F.; Grazzi, L.; et al. Erenumab in the prevention of high-frequency episodic and chronic migraine: Erenumab in Real Life in Italy (EARLY), the first Italian multicenter, prospective real-life study. Headache 2021, 61, 363–372. [Google Scholar] [CrossRef] [PubMed]
- Barbanti, P.; Aurilia, C.; Cevoli, S.; Egeo, G.; Fofi, L.; Messina, R.; Salerno, A.; Torelli, P.; Albanese, M.; Carnevale, A.; et al. Long-term (48 weeks) effectiveness, safety, and tolerability of erenumab in the prevention of high-frequency episodic and chronic migraine in a real world: Results of the EARLY 2 study. Headache 2021, 61, 1351–1363. [Google Scholar] [CrossRef]
- Barbanti, P.; Egeo, G.; Aurilia, C.; D’Onofrio, F.; Albanese, M.; Cetta, I.; Di Fiore, P.; Zucco, M.; Filippi, M.; Bono, F.; et al. Fremanezumab in the prevention of high-frequency episodic and chronic migraine: A 12-week, multicenter, real-life, cohort study (the FRIEND study). J. Headache Pain 2022, 23, 46. [Google Scholar] [CrossRef]
- Becker, W.J.; Spacey, S.; Leroux, E.; Giammarco, R.; Gladstone, J.; Christie, S.; Akaberi, A.; Power, G.S.; Minhas, J.K.; Mancini, J.; et al. A real-world, observational study of erenumab for migraine prevention in Canadian patients. Headache 2022, 62, 522–529. [Google Scholar] [CrossRef]
- Caronna, E.; Gallardo, V.J.; Alpuente, A.; Torres-Ferrus, M.; Pozo-Rosich, P. Anti-CGRP monoclonal antibodies in chronic migraine with medication overuse: Real-life effectiveness and predictors of response at 6 months. J. Headache Pain 2021, 22, 120. [Google Scholar] [CrossRef]
- Cheng, S.; Jenkins, B.; Limberg, N.; Hutton, E. Erenumab in Chronic Migraine: An Australian Experience. Headache 2020, 60, 2555–2562. [Google Scholar] [CrossRef]
- De Luca, C.; Baldacci, F.; Mazzucchi, S.; Lombardo, I.; Curto, L.; Ulivi, M.; Chico, L.; Papa, M.; Siciliano, G.; Gori, S. CGRP Inhibitors and Oxidative Stress Biomarkers in Resistant Migraine: A Real-Life Study with Erenumab, Fremanezumab, and Galcanezumab. J. Clin. Med. 2021, 10, 4586. [Google Scholar] [CrossRef]
- De Matteis, E.; Affaitati, G.; Frattale, I.; Caponnetto, V.; Pistoia, F.; Giamberardino, M.A.; Sacco, S.; Ornello, R. Early outcomes of migraine after erenumab discontinuation: Data from a real-life setting. Neurol. Sci. 2021, 42, 3297–3303. [Google Scholar] [CrossRef]
- Lentsch, S.d.V.; Verhagen, I.E.; Hoek, T.C.V.D.; MaassenVanDenBrink, A.; Terwindt, G.M. Treatment with the monoclonal calcitonin gene-related peptide receptor antibody erenumab: A real-life study. Eur. J. Neurol. 2021, 28, 4194–4203. [Google Scholar] [CrossRef] [PubMed]
- Frattale, I.; Caponnetto, V.; Casalena, A.; Assetta, M.; Maddestra, M.; Marzoli, F.; Affaitati, G.; Giamberardino, M.A.; Viola, S.; Gabriele, A.; et al. Association between response to triptans and response to erenumab: Real-life data. J. Headache Pain 2021, 22, 1. [Google Scholar] [CrossRef] [PubMed]
- Guerzoni, S.; Baraldi, C.; Pensato, U.; Favoni, V.; Castro, F.L.; Cainazzo, M.M.; Cevoli, S.; Pani, L. Chronic migraine evolution after 3 months from erenumab suspension: Real-world-evidence-life data. Neurol. Sci. 2022, 43, 3823–3830. [Google Scholar] [CrossRef]
- Iannone, L.F.; Fattori, D.; Benemei, S.; Chiarugi, A.; Geppetti, P.; De Cesaris, F. Predictors of sustained response and effects of the discontinuation of anti-calcitonin gene related peptide antibodies and reinitiation in resistant chronic migraine. Eur. J. Neurol. 2022, 29, 1505–1513. [Google Scholar] [CrossRef] [PubMed]
- Kwon, S.; Gil, Y.-E.; Lee, M.J. Real-world efficacy of galcanezumab for the treatment of migraine in Korean patients. Cephalalgia 2022, 42, 705–714. [Google Scholar] [CrossRef] [PubMed]
- Lambru, G.; Hill, B.; Murphy, M.; Tylova, I.; Andreou, A.P. A prospective real-world analysis of erenumab in refractory chronic migraine. J. Headache Pain 2020, 21, 61. [Google Scholar] [CrossRef]
- Mahović, D.; Bračić, M.; Jakuš, L.; Cvetkovic, V.V.; Krpan, M. Effectiveness and safety of erenumab in chronic migraine: A Croatian real-world experience. Clin. Neurol. Neurosurg. 2022, 214, 107169. [Google Scholar] [CrossRef]
- Matteo, E.; Favoni, V.; Pascazio, A.; Pensato, U.; Benini, M.; Asioli, G.M.; Merli, E.; Calabrò, C.; Cortelli, P.; Pierangeli, G.; et al. Erenumab in 159 high frequency and chronic migraine patients: Real-life results from the Bologna Headache Center. Neurol. Sci. 2020, 41, 483–484. [Google Scholar] [CrossRef]
- Ornello, R.; Casalena, A.; Frattale, I.; Caponnetto, V.; Gabriele, A.; Affaitati, G.; Giamberardino, M.A.; Assetta, M.; Maddestra, M.; Marzoli, F.; et al. Conversion from chronic to episodic migraine in patients treated with erenumab: Real-life data from an Italian region. J. Headache Pain 2020, 21, 102. [Google Scholar] [CrossRef]
- Pensato, U.; Baraldi, C.; Favoni, V.; Cainazzo, M.M.; Torelli, P.; Querzani, P.; Pascazio, A.; Mascarella, D.; Matteo, E.; Quintana, S.; et al. Real-life assessment of erenumab in refractory chronic migraine with medication overuse headache. Neurol. Sci. 2022, 43, 1273–1280. [Google Scholar] [CrossRef]
- Pensato, U.; Favoni, V.; Pascazio, A.; Benini, M.; Asioli, G.M.; Merli, E.; Calabrò, C.; Cortelli, P.; Pierangeli, G.; Cevoli, S. Erenumab efficacy in highly resistant chronic migraine: A real-life study. Neurol. Sci. 2020, 41, 457–459. [Google Scholar] [CrossRef] [PubMed]
- Raffaelli, B.; Terhart, M.; Mecklenburg, J.; Neeb, L.; Overeem, L.H.; Siebert, A.; Steinicke, M.; Reuter, U. Resumption of migraine preventive treatment with CGRP(-receptor) antibodies after a 3-month drug holiday: A real-world experience. J. Headache Pain 2022, 23, 40. [Google Scholar] [CrossRef] [PubMed]
- Russo, A.; Silvestro, M.; di Clemente, F.S.; Trojsi, F.; Bisecco, A.; Bonavita, S.; Tessitore, A.; Tedeschi, G. Multidimensional assessment of the effects of erenumab in chronic migraine patients with previous unsuccessful preventive treatments: A comprehensive real-world experience. J. Headache Pain 2020, 21, 69. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Marín, B.; Ledesma, D.H.; Álvarez, A.L.; Ullrich, J.G. Immunotherapy for migraine: The use of erenumab in real life. Rev. Clin. Esp. 2021, 221, 557–559. [Google Scholar] [CrossRef]
- Schoenen, J.; Timmermans, G.; Nonis, R.; Manise, M.; Fumal, A.; Gérard, P. Erenumab for Migraine Prevention in a 1-Year Compassionate Use Program: Efficacy, Tolerability, and Differences Between Clinical Phenotypes. Front. Neurol. 2021, 12, 805334. [Google Scholar] [CrossRef]
- Talbot, J.; Stuckey, R.; Crawford, L.; Weatherby, S.; Mullin, S. Improvements in pain, medication use and quality of life in onabotulinumtoxinA-resistant chronic migraine patients following erenumab treatment—Real world outcomes. J. Headache Pain 2021, 22, 5. [Google Scholar] [CrossRef] [PubMed]
- Torres-Ferrús, M.; Gallardo, V.J.; Alpuente, A.; Caronna, E.; Gine-Cipres, E.; Pozo-Rosich, P. The impact of anti-CGRP monoclonal antibodies in resistant migraine patients: A real-world evidence observational study. J. Neurol. 2021, 268, 3789–3798. [Google Scholar] [CrossRef]
- Tziakouri, A.; Tsangari, H.; Michaelides, C. Assessment of the Effect of Erenumab on Efficacy and Quality-of-Life Parameters in a Cohort of Migraine Patients With Treatment Failure in Cyprus. Front. Neurol. 2021, 12, 687697. [Google Scholar] [CrossRef]
- Vernieri, F.; Altamura, C.; Brunelli, N.; Costa, C.M.; Aurilia, C.; Egeo, G.; Fofi, L.; Favoni, V.; Pierangeli, G.; Lovati, C.; et al. Galcanezumab for the prevention of high frequency episodic and chronic migraine in real life in Italy: A multicenter prospective cohort study (the GARLIT study). J. Headache Pain 2021, 22, 35. [Google Scholar] [CrossRef]
- Vernieri, F.; Altamura, C.; Brunelli, N.; Costa, C.M.; Aurilia, C.; Egeo, G.; Fofi, L.; Favoni, V.; Lovati, C.; Bertuzzo, D.; et al. Rapid response to galcanezumab and predictive factors in chronic migraine patients: A 3-month observational, longitudinal, cohort, multicenter, Italian real-life study. Eur. J. Neurol. 2022, 29, 1198–1208. [Google Scholar] [CrossRef]
- Vernieri, F.; Brunelli, N.; Messina, R.; Costa, C.M.; Colombo, B.; Torelli, P.; Quintana, S.; Cevoli, S.; Favoni, V.; D’Onofrio, F.; et al. Discontinuing monoclonal antibodies targeting CGRP pathway after one-year treatment: An observational longitudinal cohort study. J. Headache Pain 2021, 22, 154. [Google Scholar] [CrossRef] [PubMed]
- Zecca, C.; Cargnin, S.; Schankin, C.; Giannantoni, N.M.; Viana, M.; Maraffi, I.; Riccitelli, G.C.; Sihabdeen, S.; Terrazzino, S.; Gobbi, C. Clinic and genetic predictors in response to erenumab. Eur. J. Neurol. 2022, 29, 1209–1217. [Google Scholar] [CrossRef] [PubMed]
- Cetta, I.; Messina, R.; Zanandrea, L.; Colombo, B.; Filippi, M. Comparison of efficacy and safety of erenumab between over and under 65-year-old refractory migraine patients: A pivotal study. Neurol. Sci. 2022, 43, 5769–5771. [Google Scholar] [CrossRef] [PubMed]
- De Icco, R.; Vaghi, G.; Allena, M.; Ghiotto, N.; Guaschino, E.; Martinelli, D.; Ahmad, L.; Corrado, M.; Bighiani, F.; Tanganelli, F.; et al. Does MIDAS reduction at 3 months predict the outcome of erenumab treatment? A real-world, open-label trial. J. Headache Pain 2022, 23, 123. [Google Scholar] [CrossRef]
- Khalil, M.; Moreno-Ajona, D.; Villar-Martínez, M.D.; Greenwood, F.; Hoffmann, J.; Goadsby, P.J. Erenumab in chronic migraine: Experience from a UK tertiary centre and comparison with other real-world evidence. Eur. J. Neurol. 2022, 29, 2473–2480. [Google Scholar] [CrossRef] [PubMed]
- Alsaadi, T.; Noori, S.; Varakian, R.; Youssef, S.; Almadani, A. Real-world experience of erenumab in patients with chronic or episodic migraine in the UAE. BMC Neurol. 2022, 22, 221. [Google Scholar] [CrossRef] [PubMed]
- Cullum, C.K.; Do, T.P.; Ashina, M.; Bendtsen, L.; Hugger, S.S.; Iljazi, A.; Gusatovic, J.; Snellman, J.; Lopez-Lopez, C.; Ashina, H.; et al. Real-world long-term efficacy and safety of erenumab in adults with chronic migraine: A 52-week, single-center, prospective, observational study. J. Headache Pain 2022, 23, 61. [Google Scholar] [CrossRef]
- Gantenbein, A.R.; Agosti, R.; Kamm, C.P.; Landmann, G.; Meier, N.; Merki-Feld, G.S.; Petersen, J.A.; Pohl, H.; Ryvlin, P.; Schankin, C.J.; et al. Swiss QUality of life and healthcare impact Assessment in a Real-world Erenumab treated migraine population (SQUARE study): Interim results. J. Headache Pain 2022, 23, 142. [Google Scholar] [CrossRef]
- Schenk, H.; Holle, D.; Nsaka, M.; Kleinschnitz, C.; Glas, M.; Scheffler, A. Twelve-month safety, tolerability and susceptibility to adverse events of prophylactic migraine therapy with erenumab: A retrospective real-world study. J. Headache Pain 2022, 23, 55. [Google Scholar] [CrossRef]
- Andreou, A.P.; Fuccaro, M.; Hill, B.; Murphy, M.; Caponnetto, V.; Kilner, R.; Lambru, G. Two-year effectiveness of erenumab in resistant chronic migraine: A prospective real-world analysis. J. Headache Pain 2022, 23, 139. [Google Scholar] [CrossRef]
- Driessen, M.T.; Cohen, J.M.; Thompson, S.F.; Patterson-Lomba, O.; Seminerio, M.J.; Carr, K.; Totev, T.I.; Sun, R.; Yim, E.; Mu, F.; et al. Real-world effectiveness after initiating fremanezumab treatment in US patients with episodic and chronic migraine or difficult-to-treat migraine. J. Headache Pain 2022, 23, 56. [Google Scholar] [CrossRef] [PubMed]
- Altamura, C.; Brunelli, N.; Marcosano, M.; Aurilia, C.; Egeo, G.; Lovati, C.; Favoni, V.; Perrotta, A.; Maestrini, I.; Di Cola, F.S.; et al. Conversion from chronic to episodic migraine in patients treated with galcanezumab in real life in Italy: The 12-month observational, longitudinal, cohort multicenter GARLIT experience. J. Neurol. 2022, 269, 5848–5857. [Google Scholar] [CrossRef] [PubMed]
- Silvestro, M.; Tessitore, A.; Orologio, I.; De Micco, R.; Tartaglione, L.; Trojsi, F.; Tedeschi, G.; Russo, A. Galcanezumab effect on “whole pain burden” and multidimensional outcomes in migraine patients with previous unsuccessful treatments: A real-world experience. J. Headache Pain 2022, 23, 69. [Google Scholar] [CrossRef] [PubMed]
- Fofi, L.; Altamura, C.; Fiorentini, G.; Brunelli, N.; Marcosano, M.; Barbanti, P.; Vernieri, F. Improving distress perception and mutuality in migraine caregivers after 6 months of galcanezumab treatment. Headache 2022, 62, 1143–1147. [Google Scholar] [CrossRef]
- Vernieri, F.; Brunelli, N.; Marcosano, M.; Aurilia, C.; Egeo, G.; Lovati, C.; Favoni, V.; Perrotta, A.; Maestrini, I.; Rao, R.; et al. Maintenance of response and predictive factors of 1-year GalcanezumAb treatment in real-life migraine patients in Italy: The multicenter prospective cohort GARLIT study. Eur. J. Neurol. 2022, 30, 224–234. [Google Scholar] [CrossRef]
- Lentsch, S.d.V.; van der Arend, B.W.H.; Brink, A.M.V.D.; Terwindt, G.M. Blood Pressure in Patients With Migraine Treated With Monoclonal Anti-CGRP (Receptor) Antibodies: A Prospective Follow-up Study. Neurology 2022, 99, e1897–e1904. [Google Scholar] [CrossRef]
- Nowaczewska, M.; Straburzyński, M.; Waliszewska-Prosół, M.; Meder, G.; Janiak-Kiszka, J.; Kaźmierczak, W. Cerebral Blood Flow and Other Predictors of Responsiveness to Erenumab and Fremanezumab in Migraine—A Real-Life Study. Front. Neurol. 2022, 13, 895476. [Google Scholar] [CrossRef]
- Quintana, S.; Russo, M.; Manzoni, G.C.; Torelli, P. Comparison study between erenumab, fremanezumab, and galcanezumab in the preventive treatment of high frequency episodic migraine and chronic migraine. Neurol. Sci. 2022, 43, 5757–5758. [Google Scholar] [CrossRef]
- De Matteis, E.; Caponnetto, V.; Casalena, A.; Frattale, I.; Gabriele, A.; Affaitati, G.; Giamberardino, M.A.; Maddestra, M.; Viola, S.; Pistoia, F.; et al. Cranial autonomic symptoms and response to monoclonal antibodies targeting the Calcitonin gene-related peptide pathway: A real-world study. Front. Neurol. 2022, 13, 973226. [Google Scholar] [CrossRef]
- Cantarelli, L.; Grafiña, D.P.; Perez, A.G.; Gil, S.G.; Nicolás, F.G.; Santana, E.R.; Dávila, M.A.N.; Pérez, S.M.O.; Gómez, G.C.; Reyes, S.P.; et al. Efficacy and Safety of Erenumab, Galcanezumab, and Fremanezumab in the Treatment of Drug-Resistant Chronic Migraine: Experience in Real Clinical Practice. Ann. Pharmacother. 2022. [Google Scholar] [CrossRef]
- Barbanti, P.; Egeo, G.; Aurilia, C.; Altamura, C.; D’Onofrio, F.; Finocchi, C.; Albanese, M.; Aguggia, M.; Rao, R.; Zucco, M.; et al. Predictors of response to anti-CGRP monoclonal antibodies: A 24-week, multicenter, prospective study on 864 migraine patients. J. Headache Pain 2022, 23, 138. [Google Scholar] [CrossRef] [PubMed]
- Nsaka, M.; Scheffler, A.; Wurthmann, S.; Schenk, H.; Kleinschnitz, C.; Glas, M.; Holle, D. Real-world evidence following a mandatory treatment break after a 1-year prophylactic treatment with calcitonin gene-related peptide (pathway) monoclonal antibodies. Brain Behav. 2022, 12, e2662. [Google Scholar] [CrossRef] [PubMed]
- Al-Hassany, L.; de Vries, T.; A Carpay, J.; MaassenVanDenBrink, A. Could erectile dysfunction be a side effect of CGRP inhibition? A case report. Cephalalgia 2022, 42, 257–261. [Google Scholar] [CrossRef] [PubMed]
- Albanese, M.; Mercuri, N.B. Could the New Anti-CGRP Monoclonal Antibodies Be Effective in Migraine Aura? Case Reports and Literature Review. J. Clin. Med. 2022, 11, 1228. [Google Scholar] [CrossRef] [PubMed]
- Aradi, S.; Kaiser, E.; Cucchiara, B. Ischemic Stroke Associated With Calcitonin Gene-Related Peptide Inhibitor Therapy for Migraine: A Case Report. J. Stroke Cerebrovasc. Dis. 2019, 28, 104286. [Google Scholar] [CrossRef] [PubMed]
- Arca, K.N.; Starling, A.J. Treatment-Refractory Headache in the Setting of COVID-19 Pneumonia: Migraine or Meningoencephalitis? Case Report. SN Compr. Clin. Med. 2020, 2, 1200–1203. [Google Scholar] [CrossRef] [PubMed]
- Cullum, C.K.; Olsen, M.K.; Kocadag, H.B.; Ashina, M.; Amin, F.M. Extreme ecchymoses in a migraine patient using concomitant treatment with calcitonin gene-related peptide receptor antibodies and fish oil supplements: A case report. BMC Neurol. 2021, 21, 257. [Google Scholar] [CrossRef]
- Evans, R.W. Raynaud’s Phenomenon Associated With Calcitonin Gene-Related Peptide Monoclonal Antibody Antagonists. Headache 2019, 59, 1360–1364. [Google Scholar] [CrossRef]
- Fofi, L.; Egeo, G.; Aurilia, C.; Barbanti, P. Erenumab during pregnancy: A case report in a patient with chronic migraine. Neurol. Sci. 2021, 42, 2145–2146. [Google Scholar] [CrossRef]
- Frattale, I.; Ornello, R.; Pistoia, F.; Caponnetto, V.; Colangeli, E.; Sacco, S. Paralytic ileus after planned abdominal surgery in a patient on treatment with erenumab. Intern. Emerg. Med. 2021, 16, 227–228. [Google Scholar] [CrossRef]
- González-Quintanilla, V.; Pérez-Pereda, S.; González-Suárez, A.; Madera, J.; Toriello, M.; Pascual, J. Restless legs-like syndrome as an emergent adverse event of CGRP monoclonal antibodies: A report of two cases. Cephalalgia 2021, 41, 1272–1275. [Google Scholar] [CrossRef]
- Grassini, A.; Marcinnò, A.; Roveta, F.; Gallo, E.; Cermelli, A.; Boschi, S.; Rubino, E.; Rainero, I. Impact of COVID-19 on chronic migraine treated with erenumab: A case report. Neurol. Sci. 2021, 42, 3079–3081. [Google Scholar] [CrossRef] [PubMed]
- Henze, T. Erenumab During Breastfeeding. Breastfeed. Med. 2019, 14, 513–514. [Google Scholar] [CrossRef] [PubMed]
- Iannone, L.F.; Fattori, D.; Geppetti, P.; De Cesaris, F. Galcanezumab effectiveness on comorbid cluster headache and chronic migraine: A prospective case series. Neurol. Sci. 2022, 43, 697–703. [Google Scholar] [CrossRef] [PubMed]
- Iannone, L.F.; Geppetti, P.; Chiarugi, A.; De Cesaris, F. COVID-19 pneumonia during long-term migraine prophylaxis with fremanezumab: A case report. Intern. Emerg. Med. 2021, 16, 2309–2311. [Google Scholar] [CrossRef] [PubMed]
- Kearney, E.; Collins, T.; Sengupta, S. De Novo Visual Aura Onset in a Migraineur on Galcanezumab-Gnlm. Headache 2020, 60, 1435–1437. [Google Scholar] [CrossRef]
- Klager, S.; Khalil, M.; Shulman, K.; Sami, N. Galcanezumab-induced fixed drug eruption. JAAD Case Rep. 2021, 9, 90–92. [Google Scholar] [CrossRef] [PubMed]
- Lehman, L.L.; Bruccoleri, R.; Danehy, A.; Swanson, J.; Mrakotsky, C.; Smith, E.; Orbach, D.B.; Burstein, R. Adverse effects of erenumab on cerebral proliferative angiopathy: A case report. Cephalalgia 2021, 41, 122–126. [Google Scholar] [CrossRef]
- Makarevičius, G.; Ryliškienė, K. Successful treatment of primary headache associated with sexual activity using erenumab: Case report. Cephalalgia 2022, 42, 680–683. [Google Scholar] [CrossRef]
- Mathew, P.G.; Krivitski, D.; Sharon, R. Erenumab-Induced Severe Nausea Leading to Smoking Cessation: A Retrospective Case Series. Headache 2020, 60, 2563–2569. [Google Scholar] [CrossRef]
- Moya, B.; Barranco, R.; García-Moguel, I.; Puerta-Peña, M.; Alonso, L.; Fernández-Crespo, J. First confirmed case of nonimmediate hypersensitivity to fremanezumab during chronic migraine treatment. Contact Dermat. 2022, 86, 308–310. [Google Scholar] [CrossRef] [PubMed]
- Mullin, K.; Kudrow, D.; Croop, R.; Lovegren, M.; Conway, C.M.; Coric, V.; Lipton, R.B. Potential for treatment benefit of small molecule CGRP receptor antagonist plus monoclonal antibody in migraine therapy. Neurology 2020, 94, e2121–e2125. [Google Scholar] [CrossRef] [PubMed]
- Ornello, R.; Frattale, I.; Pistoia, F.; Sacco, S.; Notturno, F. Erenumab Plus Subcutaneous Immunoglobulin in a Patient With Comorbid Chronic Migraine and Myasthenia Gravis. Headache 2020, 60, 787–788. [Google Scholar] [CrossRef] [PubMed]
- Rota, E.; Aguggia, M.; Immovilli, P.; Morelli, N.; Renosio, D.; Barbanera, A. Change in the second exteroceptive suppression period of the temporalis muscle during erenumab treatment. Naunyn-Schmiedeberg’s Arch. Pharmacol. 2022, 395, 607–611. [Google Scholar] [CrossRef] [PubMed]
- Rozen, T.D.; A Bhatt, A. Reversible cerebral vasoconstriction syndrome developing after an erenumab injection for migraine prevention. Cephalalgia 2022, 42, 250–256. [Google Scholar] [CrossRef]
- Selvi-Sabater, P.; Carvajal-Sanchez, M.A.; Carrera-Hueso, F.J. Two possible cases of erenumab-induced xerostomia. J. Clin. Pharm. Ther. 2022, 47, 824–825. [Google Scholar] [CrossRef]
- Silvestro, M.; Tessitore, A.; di Clemente, F.S.; Battista, G.; Tedeschi, G.; Russo, A. Additive Interaction Between Onabotulinumtoxin-A and Erenumab in Patients With Refractory Migraine. Front. Neurol. 2021, 12, 656294. [Google Scholar] [CrossRef]
- Silvestro, M.; Tessitore, A.; Di Clemente, F.S.; Tedeschi, G.; Russo, A. Erenumab Efficacy on Comorbid Cluster Headache in Patients With Migraine: A Real-World Case Series. Headache 2020, 60, 1187–1195. [Google Scholar] [CrossRef]
- Spector, A.R.; Kerkow, J.F.; Collins, T.A.; Kerkow, M.J.F. Sleep terrors prodromal for migraine headaches responsive to galcanezumab: A case report. Headache 2021, 61, 216–217. [Google Scholar] [CrossRef]
- Wong, S.M.; Kim, J.Y.; A Maguire, G. Migraine and adult-onset stuttering: A proposed autoimmune phenomenon. Ann. Clin. Psychiatry 2021, 33, 56–57. [Google Scholar] [CrossRef]
- Wurthmann, S.; Nägel, S.; Hadaschik, E.; Schlott, S.; Scheffler, A.; Kleinschnitz, C.; Holle, D. Impaired wound healing in a migraine patient as a possible side effect of calcitonin gene-related peptide receptor antibody treatment: A case report. Cephalalgia 2020, 40, 1255–1260. [Google Scholar] [CrossRef] [PubMed]
- Ziegeler, C.; May, A. Non-Responders to Treatment With Antibodies to the CGRP-Receptor May Profit From a Switch of Antibody Class. Headache 2020, 60, 469–470. [Google Scholar] [CrossRef] [PubMed]
- Primiano, G.; Rollo, E.; Romozzi, M.; Calabresi, P.; Servidei, S.; Vollono, C. Preventive migraine treatment in mitochondrial diseases: A case report of erenumab efficacy and literature review. Neurol. Sci. 2022, 43, 6955–6959. [Google Scholar] [CrossRef] [PubMed]
- Göbel, C.H.; Heinze, A.; Karstedt, S.; Cirkel, A.; Münte, T.F.; Göbel, H. First Report of Symmetrical Drug-related Intertriginous and Flexural Exanthema (SDRIFE or Baboon Syndrome) After Erenumab Application for Migraine Prevention. Pain Ther. 2022, 11, 1483–1491. [Google Scholar] [CrossRef] [PubMed]
- Bonifácio, G.V.; de Carvalho, S.C.; Oliveira, R.; Gil-Gouveia, R. Gestational exposure to erenumab—The outcome of three pregnancies. Headache 2022, 62, 1218–1221. [Google Scholar] [CrossRef]
- Perino, J.; Corand, V.; Laurent, E.; Théophile, H.; Miremont-Salamé, G.; Pariente, A.; Colas, J.; Couffinhal, T.; Salvo, F. Myocardial infarction associated with erenumab: A case report. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2022, 42, 585–589. [Google Scholar] [CrossRef]
- Vig, S.J.; Garza, J.; Tao, Y. The use of erenumab for migraine prophylaxis during pregnancy: A case report and narrative review. Headache 2022, 62, 1256–1263. [Google Scholar] [CrossRef]
- Kawamura, S.; Katsuki, M.; Kashiwagi, K.; Koh, A. Fremanezumab Improved Migraine and Headache Attributed to Glioblastoma. Cureus 2022, 14, e30064. [Google Scholar] [CrossRef]
- Suzuki, S.; Suzuki, K.; Shiina, T.; Kobayashi, S.; Hirata, K. Can calcitonin gene-related peptide monoclonal antibody improve migraine and restless legs syndrome? J. Neurol. Sci. 2022, 443, 120462. [Google Scholar] [CrossRef]
- López-Bravo, A.; Oliveros-Cid, A.; Mínguez-Olaondo, A.; Cuadrado, M.L. Nummular headache responsive to anti-calcitonin gene-related peptide monoclonal antibodies in a patient with migraine. Headache 2022, 62, 1063–1066. [Google Scholar] [CrossRef]
- Ray, J.C.; Allen, P.; Bacsi, A.; Bosco, J.J.; Chen, L.; Eller, M.; Kua, H.; Lim, L.L.; Matharu, M.S.; Monif, M.; et al. Inflammatory complications of CGRP monoclonal antibodies: A case series. J. Headache Pain 2021, 22, 121. [Google Scholar] [CrossRef] [PubMed]
- Cetta, I.; Messina, R.; Colombo, B.; Filippi, M. Myocardial infarction in a patient with migraine and triptan overuse treated with anti-CGRP receptor monoclonal antibody: A case report. J. Neurol. 2022, 269, 5170–5172. [Google Scholar] [CrossRef]
- Dodick, D.W.; Tepper, S.J.; Ailani, J.; Pannacciulli, N.; Navetta, M.S.; Loop, B.; Zhang, F.; Khodavirdi, A.C.; Mann, A.; Abdrabboh, A.; et al. Risk of hypertension in erenumab-treated patients with migraine: Analyses of clinical trial and postmarketing data. Headache 2021, 61, 1411–1420. [Google Scholar] [CrossRef] [PubMed]
- Saely, S.; Croteau, D.; Jawidzik, L.; Brinker, A.; Kortepeter, C.; Saely, B.S. Hypertension: A new safety risk for patients treated with erenumab. Headache 2021, 61, 202–208. [Google Scholar] [CrossRef] [PubMed]
- Gérard, A.O.; Merino, D.; Van Obberghen, E.K.; Rocher, F.; Destere, A.; Lantéri-Minet, M.; Drici, M.-D. Calcitonin gene-related peptide-targeting drugs and Raynaud’s phenomenon: A real-world potential safety signal from the WHO pharmacovigilance database. J. Headache Pain 2022, 23, 53. [Google Scholar] [CrossRef] [PubMed]
- Silberstein, S.D.; Reshef, S.; Cohen, J.M.; Gandhi, S.; Seminerio, M.; Ramirez Campos, V.; Kessler, Y.; Thompson, S.F.; Blumenfeld, A. Adverse Events Reported with Therapies Targeting the CGRP Pathway During the First 6 Months Post-launch: A Retrospective Analysis Using the FDA Adverse Events Reporting System. Adv Ther. 2022. [Google Scholar] [CrossRef]
- Breen, I.D.; Brumfiel, C.M.; Patel, M.H.; Butterfield, R.J.; VanderPluym, J.H.; Griffing, L.; Pittelkow, M.R.; Mangold, A.R. Evaluation of the Safety of Calcitonin Gene-Related Peptide Antagonists for Migraine Treatment Among Adults With Raynaud Phenomenon. JAMA Netw. Open 2021, 4, e217934. [Google Scholar] [CrossRef]
- Headache Classification Committee of the International Headache Society (IHS). The International Classification of Headache Disorders, 3rd edition. Cephalalgia 2018, 38, 1–211. [Google Scholar] [CrossRef]
- Diener, H.-C.; Tassorelli, C.; Dodick, D.W.; Silberstein, S.D.; Lipton, R.B.; Ashina, M.; Becker, W.J.; Ferrari, M.D.; Goadsby, P.J.; Pozo-Rosich, P.; et al. Guidelines of the International Headache Society for controlled trials of preventive treatment of migraine attacks in episodic migraine in adults. Cephalalgia 2020, 40, 1026–1044. [Google Scholar] [CrossRef]
- Diener, H.-C.; Tassorelli, C.; Dodick, D.W.; Silberstein, S.D.; Lipton, R.B.; Ashina, M.; Becker, W.J.; Ferrari, M.D.; Goadsby, P.J.; Pozo-Rosich, P.; et al. Guidelines of the International Headache Society for controlled trials of acute treatment of migraine attacks in adults: Fourth edition. Cephalalgia 2019, 39, 687–710. [Google Scholar] [CrossRef]
- Tassorelli, C.; Diener, H.-C.; Dodick, D.W.; Silberstein, S.D.; Lipton, R.B.; Ashina, M.; Becker, W.J.; Ferrari, M.D.; Goadsby, P.J.; Pozo-Rosich, P.; et al. Guidelines of the International Headache Society for controlled trials of preventive treatment of chronic migraine in adults. Cephalalgia 2018, 38, 815–832. [Google Scholar] [CrossRef] [PubMed]
- Noseda, R.; Bedussi, F.; Gobbi, C.; Zecca, C.; Ceschi, A. Safety profile of erenumab, galcanezumab and fremanezumab in pregnancy and lactation: Analysis of the WHO pharmacovigilance database. Cephalalgia 2021, 41, 789–798. [Google Scholar] [CrossRef] [PubMed]
- Edvinsson, L.; Chan, K.Y.; Eftekhari, S.; Nilsson, E.; De Vries, R.; Säveland, H.; Dirven, C.M.; Danser, A.J.; MaassenVanDenBrink, A. Effect of the calcitonin gene-related peptide (CGRP) receptor antagonist telcagepant in human cranial arteries. Cephalalgia 2010, 30, 1233–1240. [Google Scholar] [CrossRef] [PubMed]
- Edvinsson, L.; Nilsson, E.; Jansen-Olesen, I. Inhibitory effect of BIBN4096BS, CGRP(8-37), a CGRP antibody and an RNA-Spiegelmer on CGRP induced vasodilatation in the perfused and non-perfused rat middle cerebral artery. Br. J. Pharmacol. 2007, 150, 633–640. [Google Scholar] [CrossRef]
- Benemei, S.; Cortese, F.; Labastida-Ramírez, A.; Marchese, F.; Pellesi, L.; Romoli, M.; Vollesen, A.L.; Lampl, C.; Ashina, M. School of Advanced Studies of the European Headache Federation (EHF-SAS). Triptans and CGRP blockade—Impact on the cranial vasculature. J. Headache Pain 2017, 18, 103. [Google Scholar] [CrossRef]


{kind=link}
| Reference | CGRP-mAb | Patients (n) | Women (%) | Mean Age (Years) | Migraine Diagnosis Available/Diagnosis According to | Inclusion of Patients with | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| Migraine with Aura | Chronic Migraine | Medication Overuse | Prior Treatment Failure | Other Prophylactic Medication | ||||||
| [32] | E | 82 | 85.4 | 45 | Yes/ICD-10 | NA | NA | NA | Yes | Yes |
| [33] | E | 4437 | 85.8 | 47 | Yes/ICD-10 | Yes | Yes | NA | NA | Yes |
| [34] | E | 14,282 | 83.0 | 46 | No | Yes | Yes | NA | Yes | NA |
| [35] | E | 29,451 | 79.2 | 47 | No | NA | NA | NA | Yes | Yes |
| [36] | F | 172 | 83.7 | 46 | No | NA | NA | NA | Yes | Yes |
| [37] | E, OBTA | 2676 | 91.6 | 50 | Yes/ICD | Yes | Yes | NA | Yes | Yes |
| [38] | E | 3171 | 84.8 | 51 | Yes/ICD | Yes | Yes | NA | Yes | Yes |
| [39] | E, F, G | 3082 | 85.7 | 44 | Yes/ICD-10 | Yes | Yes | NA | Yes | Yes |
| Adverse Event | Inquired (Number of Studies) | Observed (Number of Patients) |
|---|---|---|
| Constipation | 50 | 1251 |
| Reaction at injection site | 42 | 217 |
| Dizziness | 39 | 78 |
| Muscle cramps | 38 | 41 |
| Pruritus | 37 | 44 |
| Pain at injection site | 36 | 76 |
| Skin rash | 36 | 19 |
| Urticaria | 36 | 12 |
| Adverse Events in Otherwise Healthy Individuals | |||||
|---|---|---|---|---|---|
| Ref. | Age | Sex | Exposure | Adverse Event | Comment |
| [123] | 54 | M | G | Erectile dysfunction | More than 2 months after start, reversible after 2 half-lives, rare use of metoprolol for palpitations |
| [128] | 33 | M | E | Raynaud’s phenomenon | When in the cold cca. 1 h, had RP of all the fingers and toes bilateral with temperature change and numbness lasting about 1 h |
| [131] | 38 | F | E | Restless leg-like symptoms | De novo symptoms; erenumab continued despite symptoms |
| [131] | 47 | F | G | Restless leg-like symptoms | De novo symptoms; cessation of symptoms after erenumab discontinuation |
| [136] | 61 | F | G | Migraine aura | Unsuccessful with erenumab, 1 month after last injection switch to galcanezumab (240 mg loading dose, followed by a maintenance dose of 120 mg 28 days later), within 1 week after the first dose of 120 mg, experienced first visual aura |
| [137] | 48 | F | G | Skin lesions in fixed location | After several months, developed erythema and pruritus of left upper arm within 24 h of self-injection (lasting up to 3 days), evolved into a nonpruritic, non-painful, chronic, brown-to-blue patch. Each monthly injection of galcanezumab resulted in same clinical course (at identical site on the left arm), despite injecting different areas on body (incl. the abdomen and thighs), without reaction at injection site |
| [141] | 52 | F | F | Non-immediate rash | Causal relation confirmed with pinprick test |
| [144] | 26 | F | E | Stypsis | Exteroceptive suppression period of the temporalis muscle was assessed during a ten-day washout period, before starting erenumab and after 4 months of erenumab treatment |
| [146] | 60 | F | E | Xerostomia | After first injection, reported dry mouth in the next ten days; similar duration after 2nd injection |
| [151] | 51 | F | E | Impaired wound healing of trivial injury | Improvement after discontinuation of erenumab |
| [156] | 57 | F | E | Myocardial infarction | Former smoker, family history of cardiovascular disease |
| [162] | 55 | M | E | Myocardial infarction | BMI of 29, non-smoker, suffered from hypertension, dyslipidemia, and prior myocardial infarction in 2012 |
| [154] | 48 | F | E | Symmetrical drug-related intertriginous and flexural exanthema | Erenumab discontinued and switched to fremanezumab |
| Adverse events because of possible drug interactions, or potentiation of side effects | |||||
| Ref. | Age | Sex | Exposure | Adverse event | Comment |
| [127] | 41 | F | E + fish oil | Extreme ecchymoses | Improvement after discontinuation of fish oil |
| Deterioration of preexisting disorder | |||||
| Ref. | Age | Sex | Exposure | Adverse event | Comment |
| [128] | 45 | F | F | Raynaud’s phenomenon | At 6-month follow-up, reported frequent and more severe RP (the thumb was not involved) including mild digital ulcers (which had healed by the time of the visit) for about 1 month after receiving galcanezumab. |
| [128] | 65 | M | G | Raynaud’s phenomenon | Onset few weeks after fremanezumab injection, frequent episodes of RP involving all the fingers of both hands in cool temperatures |
| [130] | 39 | F | E | Paralytic ileus in a patient after undergone abdominal surgery | Paralytic ileus is a known complication of abdominal surgery |
| [146] | 35 | F | E | Xerostomia | Previous xerostomia, and patient was on amitriptyline |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pavelic, A.R.; Wöber, C.; Riederer, F.; Zebenholzer, K. Monoclonal Antibodies against Calcitonin Gene-Related Peptide for Migraine Prophylaxis: A Systematic Review of Real-World Data. Cells 2023, 12, 143. https://doi.org/10.3390/cells12010143
Pavelic AR, Wöber C, Riederer F, Zebenholzer K. Monoclonal Antibodies against Calcitonin Gene-Related Peptide for Migraine Prophylaxis: A Systematic Review of Real-World Data. Cells. 2023; 12(1):143. https://doi.org/10.3390/cells12010143
Chicago/Turabian StylePavelic, Antun R., Christian Wöber, Franz Riederer, and Karin Zebenholzer. 2023. "Monoclonal Antibodies against Calcitonin Gene-Related Peptide for Migraine Prophylaxis: A Systematic Review of Real-World Data" Cells 12, no. 1: 143. https://doi.org/10.3390/cells12010143
APA StylePavelic, A. R., Wöber, C., Riederer, F., & Zebenholzer, K. (2023). Monoclonal Antibodies against Calcitonin Gene-Related Peptide for Migraine Prophylaxis: A Systematic Review of Real-World Data. Cells, 12(1), 143. https://doi.org/10.3390/cells12010143