
Energy Drinks and Their Acute Effects on Heart Rhythm and Electrocardiographic Time Intervals in Healthy Children and Teenagers: A Randomized Trial

Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Statement
2.2. Study Population
2.3. Study Design
2.4. End Points
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
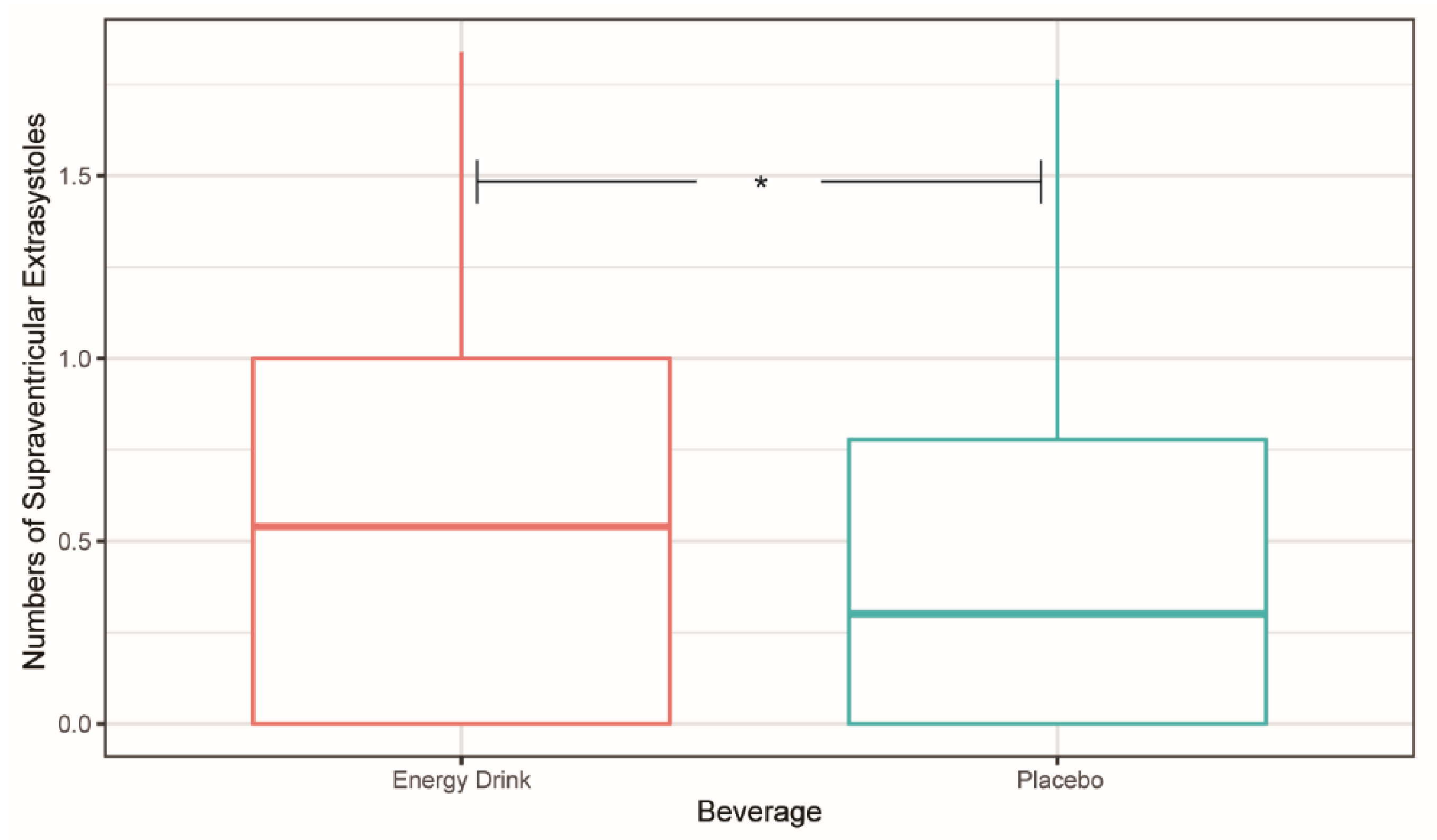
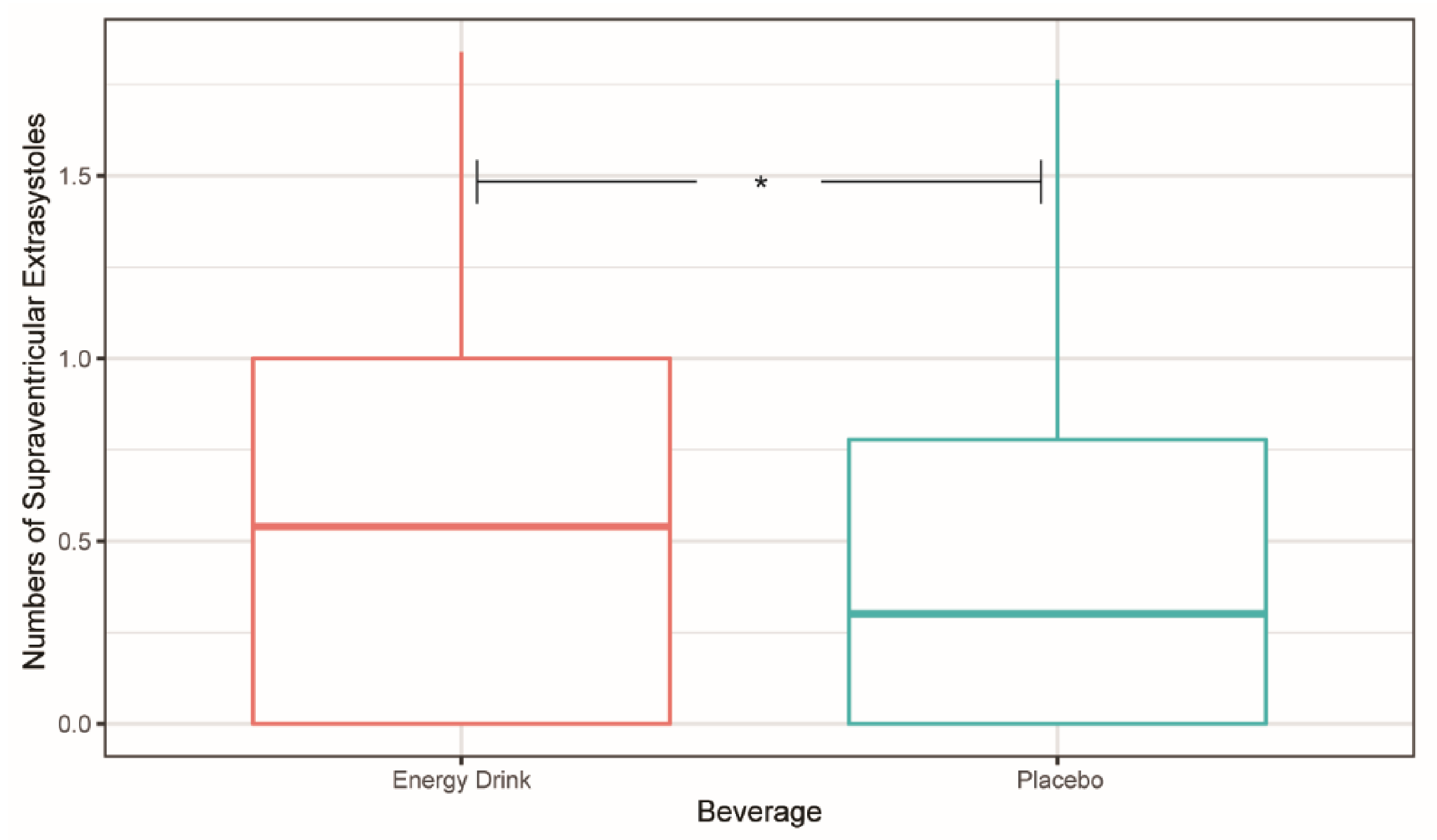
3.2. Heart Rhythm, Supraventricular, and Ventricular Extrasystoles
3.3. Electrocardiographic Time Intervals
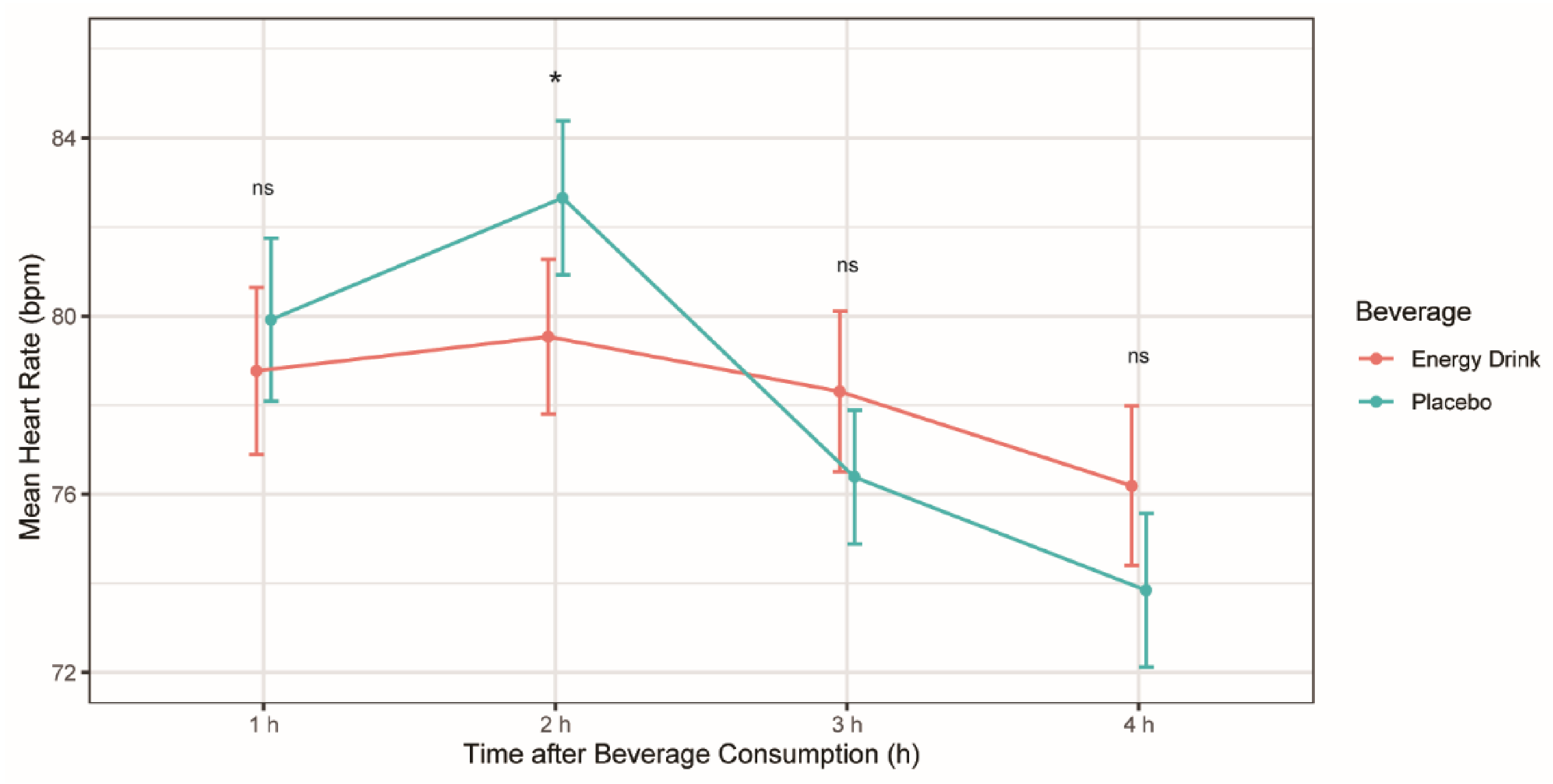
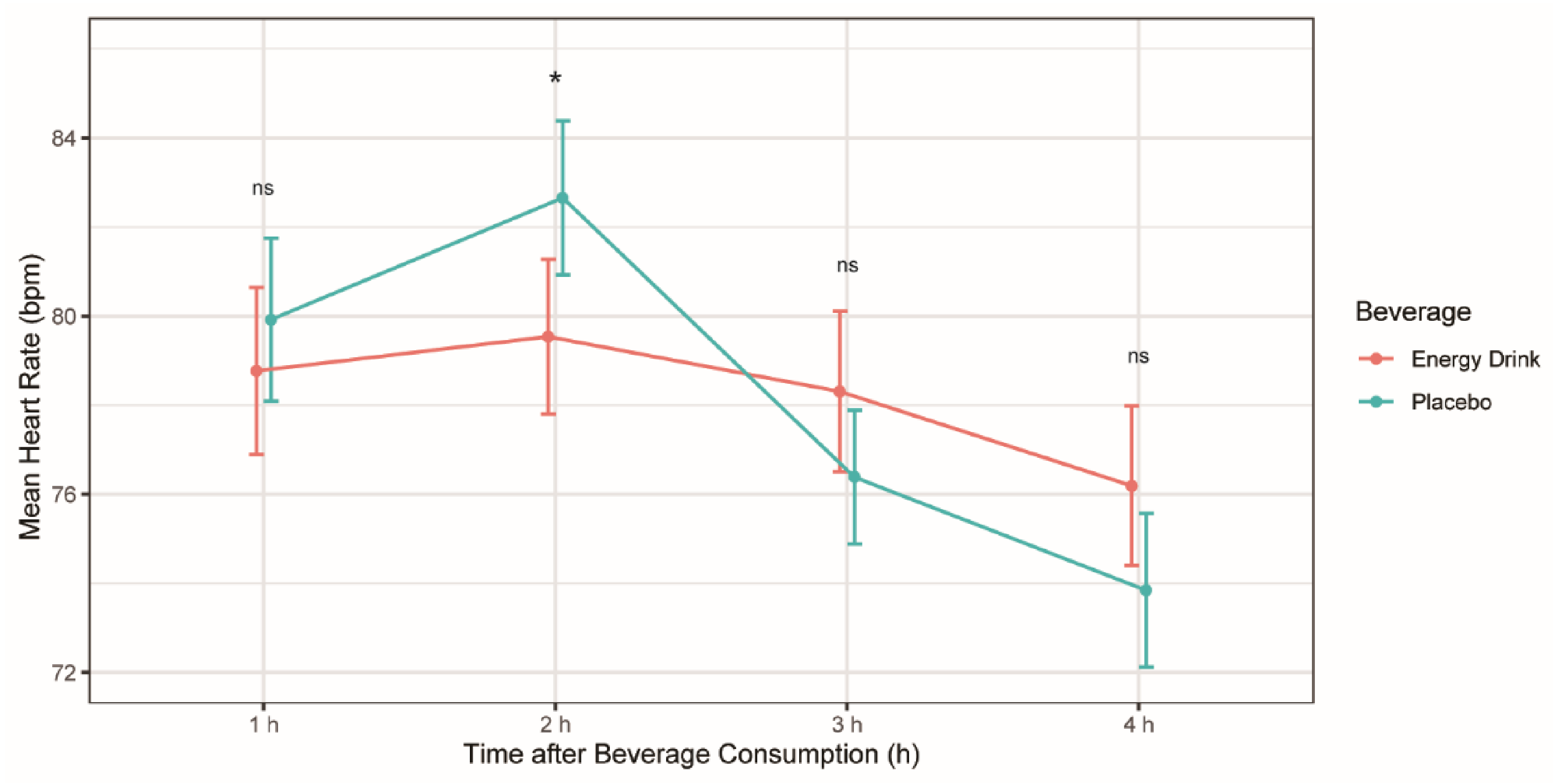
3.4. Mean Heart Rate

{kind=link}
{kind=link}
{kind=link}
| Parameters | Energy Drink (bpm) | Placebo (bpm) | p-Value |
|---|---|---|---|
| Time 1 h | 78.77 ± 9.58 | 79.92 ± 9.32 | 0.333 |
| Time 2 h | 79.54 ± 8.85 | 82.65 ± 8.81 | 0.012 * |
| Time 3 h | 78.31 ± 9.18 | 76.39 ± 7.64 | 0.125 |
| Time 4 h | 76.19 ± 9.14 | 73.85 ± 8.79 | 0.095 |
3.5. QTc
| Parameters | QTc Lead 1 | QTc Lead 2 | ||
|---|---|---|---|---|
| Energy Drink (ms) | Placebo (ms) | Energy Drink (ms) | Placebo (ms) | |
| Time 1 h | 429 ± 23.6 | 428 ± 27.0 | 427 ± 25.0 | 429 ± 28.3 |
| Time 2 h | 428 ± 22.6 | 429 ± 26.0 | 429 ± 20.9 | 432 ± 26.9 |
| Time 3 h | 427 ± 22.5 | 425 ± 22.5 | 426 ± 22.5 | 430 ± 24.1 |
| Time 4 h | 432 ± 23.6 | 429 ± 24.3 | 434 ± 24.3 | 434 ± 25.6 |
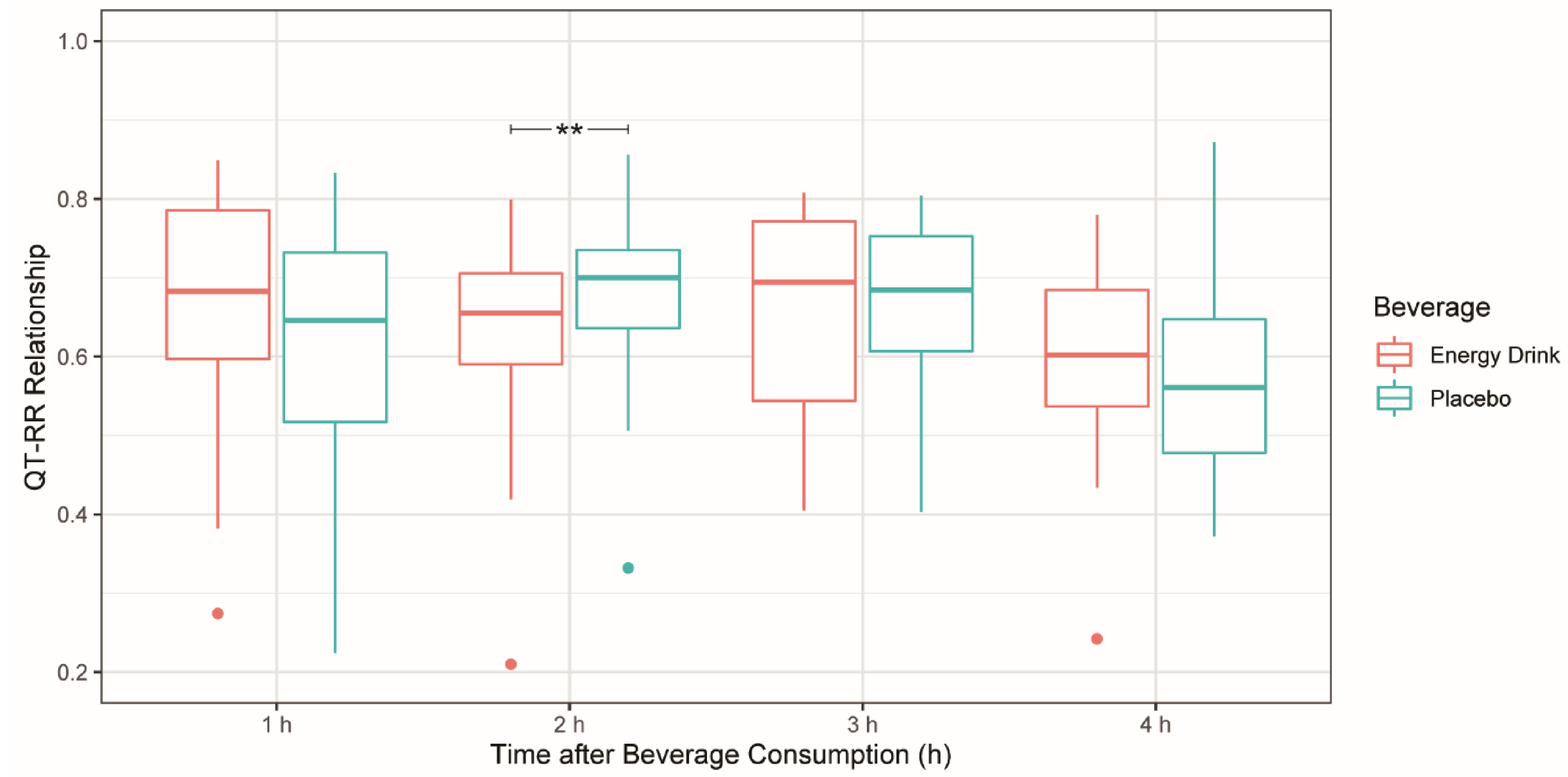
3.6. QT–RR Relationship
| Parameters | Energy Drink | Placebo | Difference | p-Value |
|---|---|---|---|---|
| Time 1 h | 0.683 | 0.646 | 0.047 | 0.069 |
| Time 2 h | 0.655 | 0.700 | −0.062 | 0.007 ** |
| Time 3 h | 0.695 | 0.685 | −0.017 | 0.316 |
| Time 4 h | 0.602 | 0.561 | 0.049 | 0.443 |

4. Discussion
4.1. Energy Drinks and Their Acute Effects on Heart Rhythm and Electrocardiographic Time Intervals
4.2. Energy Drinks: Potential Health Threat for Children and Teenagers?
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Insights, I.M. Energy Drink Sales Still on the Rise, Despite Slowdown in Innovation. Nutritional Outlook, 28 June 2018. [Google Scholar]
- Zucconi, S.; Volpato, C.; Adinolfi, F.; Gandini, E.; Gentile, E.; Loi, A.; Fioriti, L. Gathering Consumption Data on Specific Consumer Groups of Energy Drinks. EFSA Support. Publ. 2013, 10, 394E. [Google Scholar] [CrossRef] [Green Version]
- Bonar, E.E.; Cunningham, R.M.; Polshkova, S.; Chermack, S.T.; Blow, F.C.; Walton, M.A. Alcohol and Energy Drink Use among Adolescents Seeking Emergency Department Care. Addict. Behav. 2015, 43, 11–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cao, D.X.; Maiton, K.; Nasir, J.M.; Estes, N.A.M.; Shah, S.A. Energy Drink-Associated Electrophysiological and Ischemic Abnormalities: A Narrative Review. Front. Cardiovasc. Med. 2021, 8, 557. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.A.; Chu, B.W.; Lacey, C.S.; Riddock, I.C.; Lee, M.; Dargush, A.E. Impact of Acute Energy Drink Consumption on Blood Pressure Parameters: A Meta-Analysis. Ann. Pharmacother. 2016, 50, 808–815. [Google Scholar] [CrossRef]
- Fletcher, E.A.; Lacey, C.S.; Aaron, M.; Kolasa, M.; Occiano, A.; Shah, S.A. Randomized Controlled Trial of High-Volume Energy Drink Versus Caffeine Consumption on ECG and Hemodynamic Parameters. J. Am. Heart Assoc. 2017, 6, e004448. [Google Scholar] [CrossRef]
- Shah, S.A.; Szeto, A.H.; Farewell, R.; Shek, A.; Fan, D.; Quach, K.N.; Bhattacharyya, M.; Elmiari, J.; Chan, W.; O’Dell, K.; et al. Impact of High Volume Energy Drink Consumption on Electrocardiographic and Blood Pressure Parameters: A Randomized Trial. J. Am. Heart Assoc. 2019, 8, e011318. [Google Scholar] [CrossRef] [Green Version]
- Lemery, R.; Pecarskie, A.; Bernick, J.; Williams, K.; Wells, G.A. A Prospective Placebo Controlled Randomized Study of Caffeine in Patients with Supraventricular Tachycardia Undergoing Electrophysiologic Testing. J. Cardiovasc. Electrophysiol. 2015, 26, 1–6. [Google Scholar] [CrossRef]
- Li, P.; Mandilaras, G.; Dalla Pozza, R.; Jakob, A.; Haas, N.A.; Oberhoffer, F.S. Energy drinks and arterial stiffness in healthy children. Nieren-Hochdruckkrankheiten 2021, 50, 505–525. [Google Scholar] [CrossRef]
- Kromeyer-Hauschild, K.; Wabitsch, M.; Kunze, D.; Geller, F.; Geiß, H.C.; Hesse, V.; von Hippel, A.; Jaeger, U.; Johnsen, D.; Korte, W.; et al. Perzentile für den body-mass-index für das Kindes-und jugendalter unter heranziehung verschiedener deutscher stichproben. Mon. Kinderheilkd. 2001, 149, 807–818. [Google Scholar] [CrossRef] [Green Version]
- EFSA Panel on Dietetic Products, Nutrition and Allergies (NDA). Scientific Opinion on the Safety of Caffeine. EFSA J. 2015, 13, 4102. [Google Scholar] [CrossRef] [Green Version]
- Kligfield, P.; Gettes, L.S.; Bailey, J.J.; Childers, R.; Deal, B.J.; Hancock, E.W.; van Herpen, G.; Kors, J.A.; Macfarlane, P.; Mirvis, D.M.; et al. Recommendations for the Standardization and Interpretation of the Electrocardiogram. J. Am. Coll. Cardiol. 2007, 49, 1109–1127. [Google Scholar] [CrossRef] [Green Version]
- Bazett, H.C. An Analysis of the Time-Relations of Electrocardiograms. Ann. Noninvasive Electrocardiol. 1997, 2, 177–194. [Google Scholar] [CrossRef]
- Lindinger, A.; Paul, T. EKG Im Kindes-Und Jugendalter: EKG-Basisinformationen-Herzrhythmusstörungen-Angeborene Herzfehler Im Kindes-, Jugend-Und Erwachsenenalter; Georg Thieme Verlag: Stuttgart, Germany, 2016. [Google Scholar]
- Schneider, M.B.; Benjamin, H.J.; Fitness, Committee on Nutrition and the Council on Sports Medicine and Fitness. Sports Drinks and Energy Drinks for Children and Adolescents: Are They Appropriate? Pediatrics 2011, 127, 1182–1189. [Google Scholar] [CrossRef] [Green Version]
- Mitka, M. Hearing Raises Questions on Energy Drink Marketing. JAMA 2013, 310, 1015. [Google Scholar] [CrossRef]
- Lévy, S.; Santini, L.; Capucci, A.; Oto, A.; Santomauro, M.; Riganti, C.; Raviele, A.; Cappato, R. European Cardiac Arrhythmia Society Statement on the Cardiovascular Events Associated with the Use or Abuse of Energy Drinks. J. Interv. Card. Electrophysiol. 2019, 56, 99–115. [Google Scholar] [CrossRef]
- Frost, L.; Vestergaard, P. Caffeine and Risk of Atrial Fibrillation or Flutter: The Danish Diet, Cancer, and Health Study. Am. J. Clin. Nutr. 2005, 81, 578–582. [Google Scholar] [CrossRef] [Green Version]
- Zuchinali, P.; Ribeiro, P.A.B.; Pimentel, M.; da Rosa, P.R.; Zimerman, L.I.; Rohde, L.E. Effect of Caffeine on Ventricular Arrhythmia: A Systematic Review and Meta-Analysis of Experimental and Clinical Studies. EP Eur. 2016, 18, 257–266. [Google Scholar] [CrossRef]
- Goldfarb, M.; Tellier, C.; Thanassoulis, G. Review of Published Cases of Adverse Cardiovascular Events After Ingestion of Energy Drinks. Am. J. Cardiol. 2014, 113, 168–172. [Google Scholar] [CrossRef]
- Acharya, T.; Tringali, S.; Bhullar, M.; Nalbandyan, M.; Ilineni, V.K.; Carbajal, E.; Deedwania, P. Frequent Atrial Premature Complexes and Their Association With Risk of Atrial Fibrillation. Am. J. Cardiol. 2015, 116, 1852–1857. [Google Scholar] [CrossRef]
- Marx, M.; Albinni, S.; Luckner, D. Die Extrasystolie. Kinder-Jugendmed. 2013, 13, 21–27. [Google Scholar] [CrossRef]
- Schläpfer, J.; Staeger, P. Supraventrikuläre und ventrikuläre Extrasystolen. Swiss Med. Forum 2017, 17, 208–213. [Google Scholar] [CrossRef] [Green Version]
- Steinke, L.; Lanfear, D.E.; Dhanapal, V.; Kalus, J.S. Effect of “Energy Drink” Consumption on Hemodynamic and Electrocardiographic Parameters in Healthy Young Adults. Ann. Pharmacother. 2009, 43, 596–602. [Google Scholar] [CrossRef]
- Kozik, T.M.; Carey, M.G.; Bhattacharyya, M.; Chien, W.; Charos, G.S.; Connolly, T.F.; Hickman, M.C.; Schmidt, S.; Pelter, M.M. Cardiovascular Responses to ENERGY Drinks in a Healthy Population during EXercise: The C-Energy-X Study. J. Electrocardiol. 2018, 51, S1–S5. [Google Scholar] [CrossRef]
- Hnatkova, K.; Vicente, J.; Johannesen, L.; Garnett, C.; Stockbridge, N.; Malik, M. Errors of Fixed QT Heart Rate Corrections Used in the Assessment of Drug-Induced QTc Changes. Front. Physiol. 2019, 10, 635. [Google Scholar] [CrossRef]
- Malik, M.; Hnatkova, K.; Kowalski, D.; Keirns, J.J.; van Gelderen, E.M. QT/RR Curvatures in Healthy Subjects: Sex Differences and Covariates. Am. J. Physiol.-Heart Circ. Physiol. 2013, 305, H1798–H1806. [Google Scholar] [CrossRef] [Green Version]
- Fossa, A.A. The Impact of Varying Autonomic States on the Dynamic Beat-to-Beat QT–RR and QT–TQ Interval Relationships. Br. J. Pharmacol. 2008, 154, 1508–1515. [Google Scholar] [CrossRef] [Green Version]
| Characteristics | Total |
|---|---|
| Age (years) mean (SD) | 14.49 ± 2.44 |
| Sex, n (%) | |
| Male | 13 (50) |
| Female | 13 (50) |
| Weight Classification, n (%) | |
| Normal weight | 22 (84.62) |
| Overweight | 4 (15.38) |
| Obese | 0 (0) |
| Caffeine Consumption Behavior, n (%) a | |
| Rarely | 16 (61.54) |
| Occasionally | 3 (11.54) |
| Frequently | 5 (19.23) |
| Daily | 2 (7.69) |
| Energy Drink Consumption Behavior, n (%) b | |
| Never | 11 (42.31) |
| Rarely | 11 (42.31) |
| Occasionally | 1 (3.84) |
| Frequently | 3 (11.54) |
| Daily | 0 (0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mandilaras, G.; Li, P.; Dalla-Pozza, R.; Haas, N.A.; Oberhoffer, F.S. Energy Drinks and Their Acute Effects on Heart Rhythm and Electrocardiographic Time Intervals in Healthy Children and Teenagers: A Randomized Trial. Cells 2022, 11, 498. https://doi.org/10.3390/cells11030498
Mandilaras G, Li P, Dalla-Pozza R, Haas NA, Oberhoffer FS. Energy Drinks and Their Acute Effects on Heart Rhythm and Electrocardiographic Time Intervals in Healthy Children and Teenagers: A Randomized Trial. Cells. 2022; 11(3):498. https://doi.org/10.3390/cells11030498
Chicago/Turabian StyleMandilaras, Guido, Pengzhu Li, Robert Dalla-Pozza, Nikolaus Alexander Haas, and Felix Sebastian Oberhoffer. 2022. "Energy Drinks and Their Acute Effects on Heart Rhythm and Electrocardiographic Time Intervals in Healthy Children and Teenagers: A Randomized Trial" Cells 11, no. 3: 498. https://doi.org/10.3390/cells11030498
APA StyleMandilaras, G., Li, P., Dalla-Pozza, R., Haas, N. A., & Oberhoffer, F. S. (2022). Energy Drinks and Their Acute Effects on Heart Rhythm and Electrocardiographic Time Intervals in Healthy Children and Teenagers: A Randomized Trial. Cells, 11(3), 498. https://doi.org/10.3390/cells11030498