
Autologous Stem Cells Transplants in the Treatment of Temporomandibular Joints Disorders: A Systematic Review and Meta-Analysis of Clinical Trials

 ,
,  , , ,
, , ,  ,
,  and
and
Abstract
:
1. Introduction
1.1. Rationale
1.2. Objectives
2. Methods
2.1. Eligibility Criteria
2.2. Information Sources and Search Strategy
2.3. Selection Process and Data Collection Process
2.4. Data Items, Study Risk of Bias Assessment, and Synthesis Methods
3. Results
3.1. Study Selection
3.2. Study Characteristics
3.3. Risk of Bias in Studies
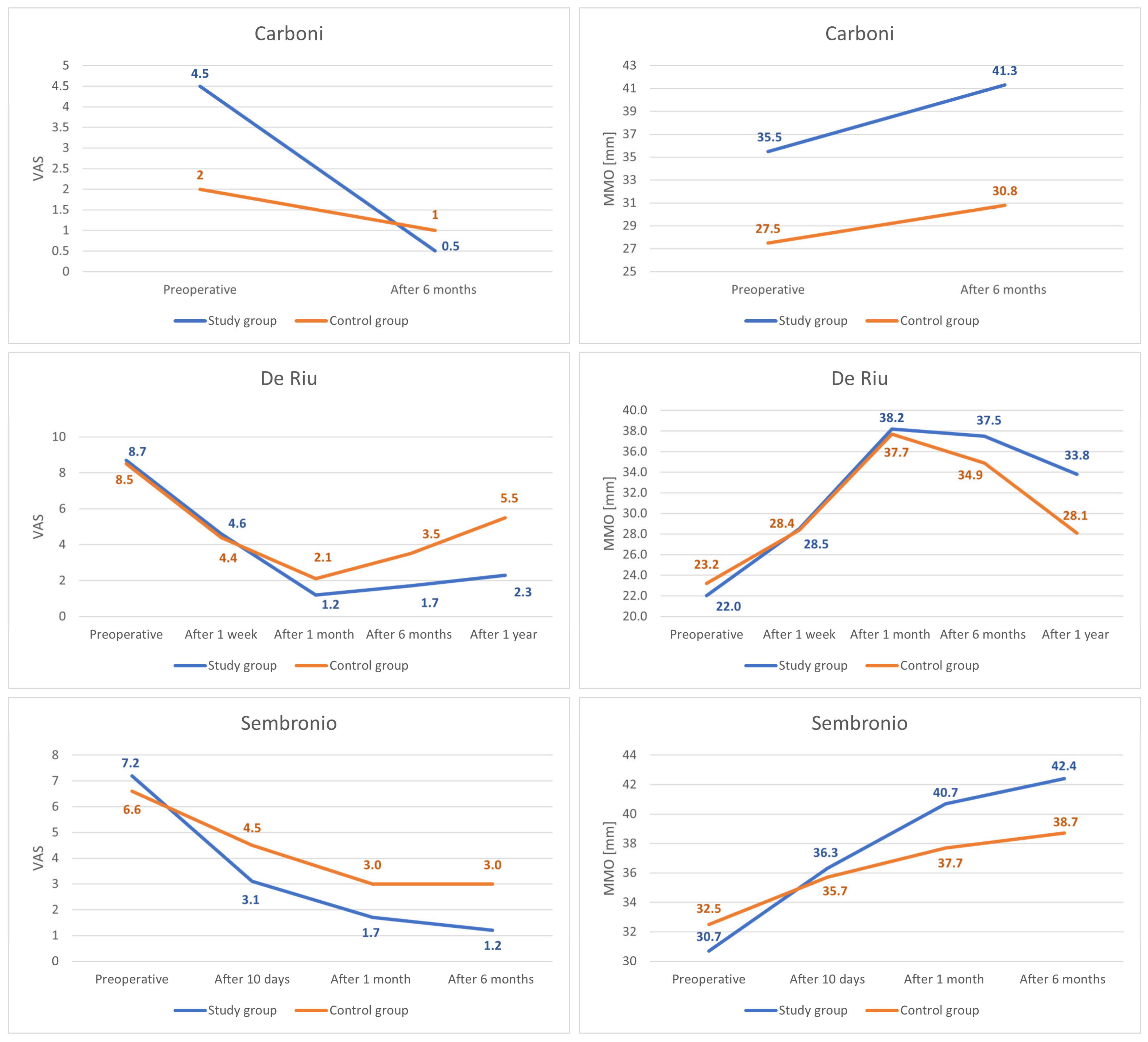
3.4. Results of Individual Studies
3.5. Results of Syntheses
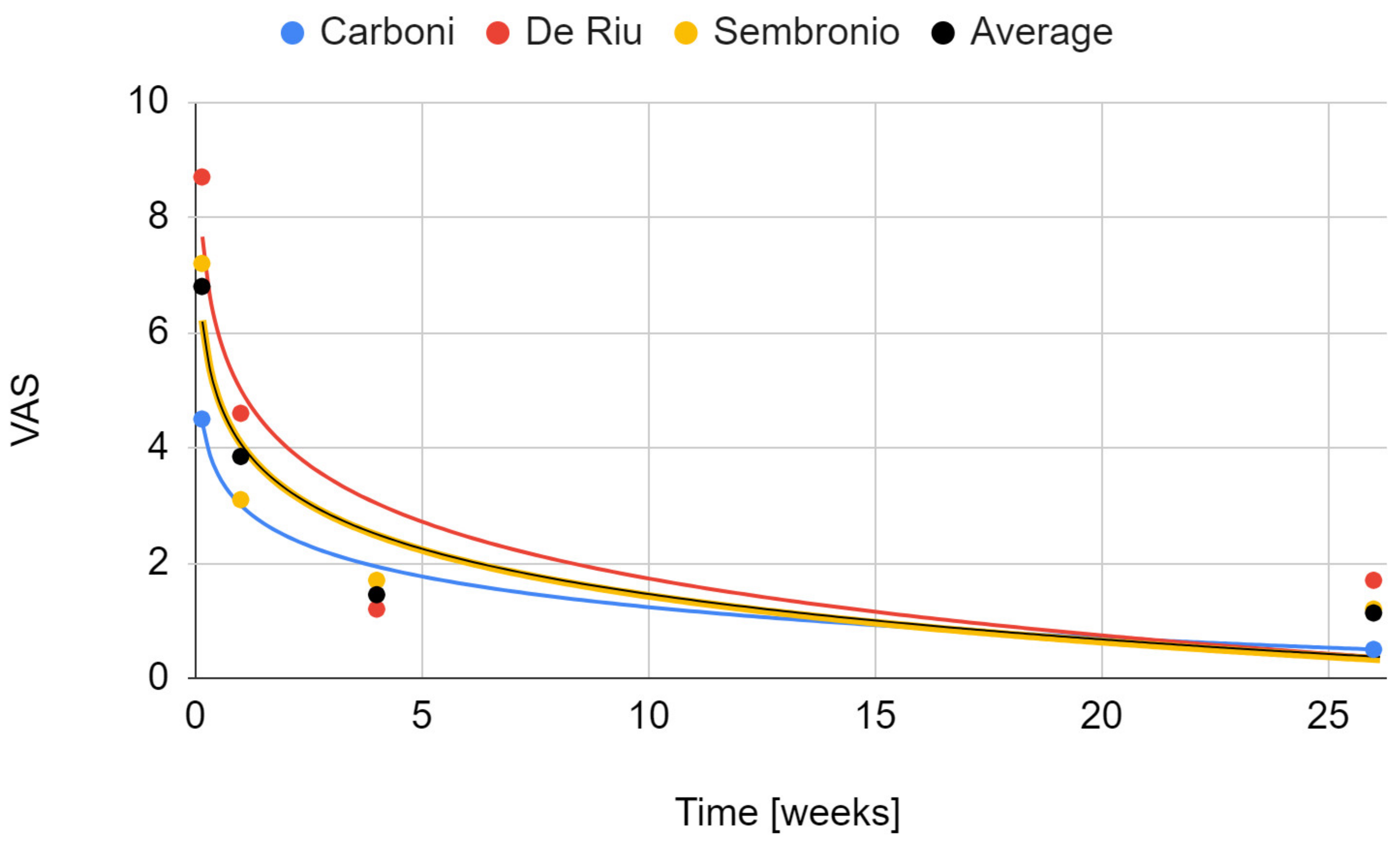
3.5.1. Pain
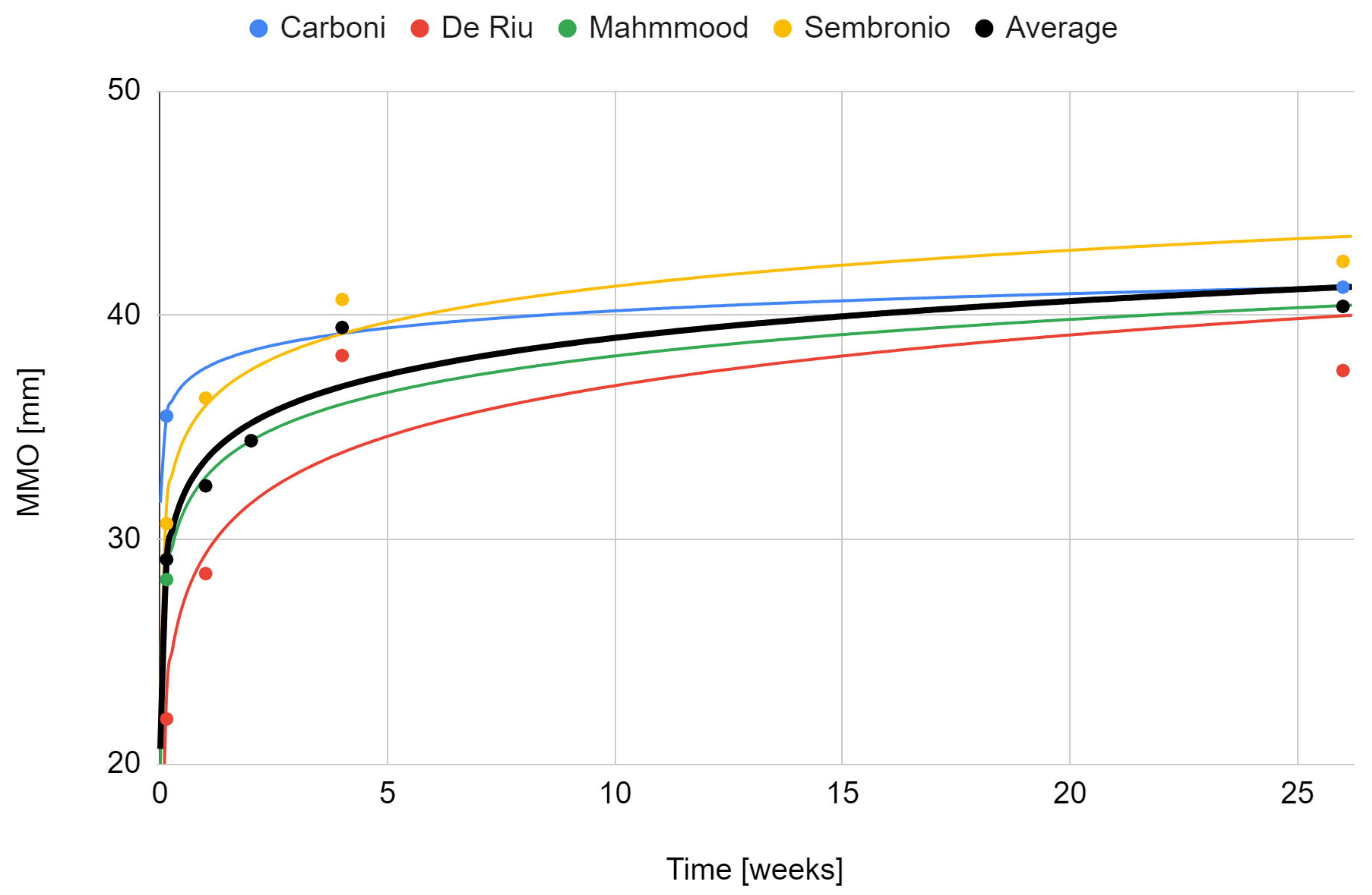
3.5.2. Maximum Mouth Opening
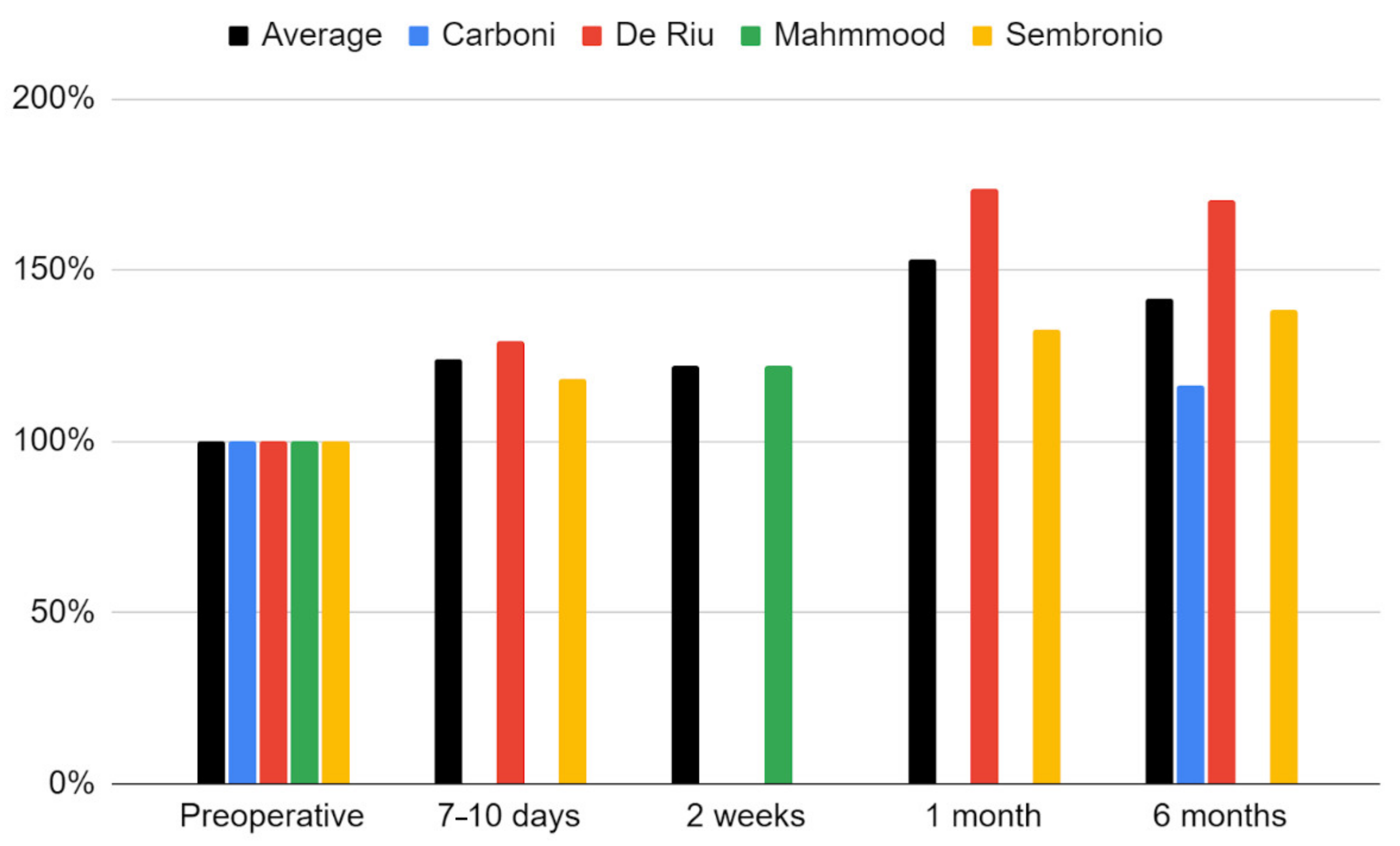
3.5.3. Comparison with Control Groups
4. Discussion
4.1. Interpretation of the Results
4.2. Treatment Technique
4.3. Effectiveness
4.4. Complications
4.5. Differential Diagnosis
4.6. Further Research
4.7. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Search Engine | Search Query |
|---|---|
| ACM Digital | [All: temporomandibular] AND [[All: intra-articular] OR [All: injection] OR [All: injectable]] AND [[All: transplants] OR [All: stem]] Searched the ACM Guide to Computing Literature |
| BASE | temporomandibular AND (intra-articular injection injectable) AND (transplants stem) |
| EBSCOhost | temporomandibular AND (intra-articular OR injection OR injectable) AND (transplants OR stem) |
| Google Scholar | allintitle: temporomandibular AND (intra-articular OR injection OR injectable) AND (transplants OR stem) |
| PubMed | temporomandibular AND (intra-articular OR injection OR injectable) AND (transplants OR stem) |
| Scopus | TITLE-ABS-KEY (temporomandibular AND (intra-articular OR injection OR injectable) AND (transplants OR stem)) |
| Web of Science | temporomandibular AND (intra-articular OR injection OR injectable) AND (transplants OR stem) (All Fields) |
| First Author | Report | Reason for Exclusion |
|---|---|---|
| Embree [50] | Exploiting endogenous fibrocartilage stem cells to regenerate cartilage and repair joint injury | No human in vivo studies |
| Guarda-Nardini [116] | Human Amniotic Membrane Positioning in the Surgical Treatment of Temporomandibular Joint Degenerative Disorder | Wrong intervention |
| Serakinci [4] | Modeling Mesenchymal Stem Cells in TMJ Rheumatoid Arthritis and Osteoarthritis Therapy | Review article |
| Ward [117] | Umbilical Cord Stem Cell Lysate: A New Biologic Injection for Treatment of Temporomandibular Joint Inflammation | Animal study |
| Yang [24] | Bone marrow mesenchymal stem cell transplantation for the treatment of temporomandibular joint osteoarthrosis | Animal study |
| Zhu [118] | NEL-like molecule-1-modified bone marrow mesenchymal stem cells/poly lactic-co-glycolic acid composite improves repair of large osteochondral defects in mandibular condyle | Wrong problem |
| First Author | Control Group Size (F/M) | Patients’ Age (Average) | Patients Treated Unilaterally/Bilaterally | Number of Joints Treated | Interventions |
|---|---|---|---|---|---|
| Carboni [55] | 4 (2/2) | 28–62 (44.0) | 0/4 | 8 | Saline injection |
| De Riu [57] | 15 (14/1) | 33–61 (44.5) | 15/0 | 15 | Arthrocentesis + HA |
| Sembronio [75] | 20 (N/S) | 17–74 (50.7) | 15/5 | 25 | Arthrocentesis + HA |
References
- Rodríguez-Fuentes, D.E.; Fernández-Garza, L.E.; Samia-Meza, J.A.; Barrera-Barrera, S.A.; Caplan, A.I.; Barrera-Saldaña, H.A. Mesenchymal Stem Cells Current Clinical Applications: A Systematic Review. Arch. Med. Res. 2021, 52, 93–101. [Google Scholar] [CrossRef] [PubMed]
- He, F.; Zhou, A.; Feng, S.; Li, Y.; Liu, T. Mesenchymal Stem Cell Therapy for Paraquat Poisoning: A Systematic Review and Meta-Analysis of Preclinical Studies. PLoS ONE 2018, 13, e0194748. [Google Scholar] [CrossRef] [PubMed]
- Kapetanos, K.; Asimakopoulos, D.; Christodoulou, N.; Vogt, A.; Khan, W. Chronological Age Affects MSC Senescence In Vitro—A Systematic Review. Int. J. Mol. Sci. 2021, 22, 7945. [Google Scholar] [CrossRef]
- Serakinci, N.; Savtekin, G. Modeling Mesenchymal Stem Cells in TMJ Rheumatoid Arthritis and Osteoarthritis Therapy. Crit. Rev. Eukaryot. Gene Expr. 2017, 27, 205–210. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.; Zhang, J.; Xu, H.; Lin, Z.; Chang, H.; Liu, W.; Kong, L. Mesenchymal Stem Cells in Knee Osteoarthritis Treatment: A Systematic Review and Meta-Analysis. J. Orthop. Transl. 2020, 24, 121–130. [Google Scholar] [CrossRef]
- Bojanic, C.; To, K.; Hatoum, A.; Shea, J.; Seah, K.T.M.; Khan, W.; Malata, C.M. Mesenchymal Stem Cell Therapy in Hypertrophic and Keloid Scars. Cell Tissue Res. 2021, 383, 915–930. [Google Scholar] [CrossRef]
- Chihaby, N.; Orliaguet, M.; Le Pottier, L.; Pers, J.-O.; Boisramé, S. Treatment of Sjögren’s Syndrome with Mesenchymal Stem Cells: A Systematic Review. Int. J. Mol. Sci. 2021, 22, 10474. [Google Scholar] [CrossRef]
- Wang, J.-H.; Liu, X.-L.; Sun, J.-M.; Yang, J.-H.; Xu, D.-H.; Yan, S.-S. Role of Mesenchymal Stem Cell Derived Extracellular Vesicles in Autoimmunity: A Systematic Review. World J. Stem Cells 2020, 12, 879–896. [Google Scholar] [CrossRef]
- Alonso-Goulart, V.; Carvalho, L.N.; Marinho, A.L.G.; de Oliveira Souza, B.L.; de Aquino Pinto Palis, G.; Lage, H.G.D.; de Lima, I.L.; Guimarães, L.D.; Peres, L.C.; Silveira, M.M.; et al. Biomaterials and Adipose-Derived Mesenchymal Stem Cells for Regenerative Medicine: A Systematic Review. Materials 2021, 14, 4641. [Google Scholar] [CrossRef]
- Li, T.; Luo, C.; Zhang, J.; Wei, L.; Sun, W.; Xie, Q.; Liu, Y.; Zhao, Y.; Xu, S.; Wang, L. Efficacy and Safety of Mesenchymal Stem Cells Co-Infusion in Allogeneic Hematopoietic Stem Cell Transplantation: A Systematic Review and Meta-Analysis. Stem Cell Res. Ther. 2021, 12, 246. [Google Scholar] [CrossRef]
- Zeng, L.; Yu, G.; Yang, K.; Xiang, W.; Li, J.; Chen, H. Efficacy and Safety of Mesenchymal Stem Cell Transplantation in the Treatment of Autoimmune Diseases (Rheumatoid Arthritis, Systemic Lupus Erythematosus, Inflammatory Bowel Disease, Multiple Sclerosis, and Ankylosing Spondylitis): A Systematic Review and Meta-Analysis of Randomized Controlled Trial. Stem Cells Int. 2022, 2022, 9463314. [Google Scholar] [CrossRef]
- To, K.; Romain, K.; Mak, C.; Kamaraj, A.; Henson, F.; Khan, W. The Treatment of Cartilage Damage Using Human Mesenchymal Stem Cell-Derived Extracellular Vesicles: A Systematic Review of in Vivo Studies. Front. Bioeng. Biotechnol. 2020, 8, 580. [Google Scholar] [CrossRef] [PubMed]
- Jeong, H.; Yim, H.W.; Park, H.-J.; Cho, Y.; Hong, H.; Kim, N.J.; Oh, I.-H. Mesenchymal Stem Cell Therapy for Ischemic Heart Disease: Systematic Review and Meta-Analysis. Int. J. Stem Cells 2018, 11, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Liu, W.; Bai, Y.; Zhou, Y.; Zhang, Y.; Wang, C.; Lin, S.; He, H. Transplantation of Mesenchymal Stem Cells for Spinal Cord Injury: A Systematic Review and Network Meta-Analysis. J. Transl. Med. 2021, 19, 178. [Google Scholar] [CrossRef]
- Tan, S.H.S.; Wong, J.R.Y.; Sim, S.J.Y.; Tjio, C.K.E.; Wong, K.L.; Chew, J.R.J.; Hui, J.H.P.; Toh, W.S. Mesenchymal Stem Cell Exosomes in Bone Regenerative Strategies—A Systematic Review of Preclinical Studies. Mater. Today Bio. 2020, 7, 100067. [Google Scholar] [CrossRef] [PubMed]
- Yazhen, Z.; Wenyi, C.; Bing, F.; Hongcui, C. The Clinical Efficacy and Safety of Stem Cell Therapy for Diabetes Mellitus: A Systematic Review and Meta-Analysis. Aging Dis. 2020, 11, 141. [Google Scholar] [CrossRef]
- Kvistad, C.E.; Kråkenes, T.; Gjerde, C.; Mustafa, K.; Rekand, T.; Bø, L. Safety and Clinical Efficacy of Mesenchymal Stem Cell Treatment in Traumatic Spinal Cord Injury, Multiple Sclerosis and Ischemic Stroke—A Systematic Review and Meta-Analysis. Front. Neurol. 2022, 13, 891514. [Google Scholar] [CrossRef] [PubMed]
- Migliorini, F.; Eschweiler, J.; Goetze, C.; Pastor, T.; Giorgino, R.; Hildebrand, F.; Maffulli, N. Cell Therapies for Chondral Defects of the Talus: A Systematic Review. J. Orthop. Surg. 2022, 17, 308. [Google Scholar] [CrossRef]
- Malik, D.; Luck, J.; Smith, O.J.; Mosahebi, A. A Systematic Review of Autologous Fat Grafting in the Treatment of Acute and Chronic Cutaneous Wounds. Plast. Reconstr. Surg. Glob. Open 2020. Publish Ahead of Print. [Google Scholar] [CrossRef]
- Krastev, T.K.; Schop, S.J.; Hommes, J.; Piatkowski, A.; van der Hulst, R.R.W.J. Autologous Fat Transfer to Treat Fibrosis and Scar-Related Conditions: A Systematic Review and Meta-Analysis. J. Plast. Reconstr. Aesthet. Surg. 2020, 73, 2033–2048. [Google Scholar] [CrossRef]
- Pak, J.; Lee, J.; Pak, N.; Pak, Y.; Park, K.; Jeon, J.; Jeong, B.; Lee, S. Cartilage Regeneration in Humans with Adipose Tissue-Derived Stem Cells and Adipose Stromal Vascular Fraction Cells: Updated Status. Int. J. Mol. Sci. 2018, 19, 2146. [Google Scholar] [CrossRef] [PubMed]
- Jankauskaite, L.; Malinauskas, M.; Aukstikalne, L.; Dabasinskaite, L.; Rimkunas, A.; Mickevicius, T.; Pockevičius, A.; Krugly, E.; Martuzevicius, D.; Ciuzas, D.; et al. Functionalized Electrospun Scaffold–Human-Muscle-Derived Stem Cell Construct Promotes In Vivo Neocartilage Formation. Polymers 2022, 14, 2498. [Google Scholar] [CrossRef] [PubMed]
- Sheng, R.; Chen, J.; Wang, H.; Luo, Y.; Liu, J.; Chen, Z.; Mo, Q.; Chi, J.; Ling, C.; Tan, X.; et al. Nanosilicate-Reinforced Silk Fibroin Hydrogel for Endogenous Regeneration of Both Cartilage and Subchondral Bone. Adv. Healthc. Mater. 2022, 2200602. [Google Scholar] [CrossRef]
- Yang, X.-H.; Peng, L.; Liu, Y.-S.; Xing, Z.-C.; Li, H.-F.; Li, Y.-Q.; Liu, M. Bone marrow mesenchymal stem cell transplantation for the treatment of temporomandibular joint osteoarthrosis. Chin. J. Tissue Eng. Res. 2013, 17, 3488–3494. [Google Scholar] [CrossRef]
- Zhang, J.; Hu, Y.; Wang, Z.; Wu, X.; Yang, C.; Yang, H. Hypoxia-Inducible Factor Expression Is Related to Apoptosis and Cartilage Degradation in Temporomandibular Joint Osteoarthritis. BMC Musculoskelet. Disord. 2022, 23, 583. [Google Scholar] [CrossRef]
- Sikora, M.; Czerwińska-Niezabitowska, B.; Chęciński, M.A.; Sielski, M.; Chlubek, D. Short-Term Effects of Intra-Articular Hyaluronic Acid Administration in Patients with Temporomandibular Joint Disorders. J. Clin. Med. 2020, 9, 1749. [Google Scholar] [CrossRef] [PubMed]
- Sikora, M.; Sielski, M.; Chęciński, M.; Nowak, Z.; Czerwińska-Niezabitowska, B.; Chlubek, D. Repeated Intra-Articular Administration of Platelet-Rich Plasma (PRP) in Temporomandibular Disorders: A Clinical Case Series. J. Clin. Med. 2022, 11, 4281. [Google Scholar] [CrossRef]
- Bitiniene, D.; Zamaliauskiene, R.; Kubilius, R.; Leketas, M.; Gailius, T.; Smirnovaite, K. Quality of Life in Patients with Temporomandibular Disorders. A Systematic Review. Stomatologija 2018, 20, 3–9. [Google Scholar]
- Işık, G.; Kenç, S.; Özveri Koyuncu, B.; Günbay, S.; Günbay, T. Injectable Platelet-Rich Fibrin as Treatment for Temporomandibular Joint Osteoarthritis: A Randomized Controlled Clinical Trial. J. Cranio-Maxillo-Fac. Surg. Off. Publ. Eur. Assoc. Cranio-Maxillo-Fac. Surg. 2022, 50, 576–582. [Google Scholar] [CrossRef]
- Sikora, M.; Chęciński, M.; Chlubek, D. Retro-Auricular Approach to the Fractures of the Mandibular Condyle: A Systematic Review. J. Clin. Med. 2021, 10, 230. [Google Scholar] [CrossRef]
- Sikora, M.; Chęciński, M.; Nowak, Z.; Chlubek, D. Variants and Modifications of the Retroauricular Approach Using in Temporomandibular Joint Surgery: A Systematic Review. J. Clin. Med. 2021, 10, 2049. [Google Scholar] [CrossRef] [PubMed]
- Derwich, M.; Mitus-Kenig, M.; Pawlowska, E. Mechanisms of Action and Efficacy of Hyaluronic Acid, Corticosteroids and Platelet-Rich Plasma in the Treatment of Temporomandibular Joint Osteoarthritis—A Systematic Review. Int. J. Mol. Sci. 2021, 22, 7405. [Google Scholar] [CrossRef] [PubMed]
- Chęciński, M.; Sikora, M.; Chęcińska, K.; Nowak, Z.; Chlubek, D. The Administration of Hyaluronic Acid into the Temporomandibular Joints’ Cavities Increases the Mandible’s Mobility: A Systematic Review and Meta-Analysis. J. Clin. Med. 2022, 11, 1901. [Google Scholar] [CrossRef] [PubMed]
- Ibi, M. Inflammation and Temporomandibular Joint Derangement. Biol. Pharm. Bull. 2019, 42, 538–542. [Google Scholar] [CrossRef]
- Chęciński, M.; Chęcińska, K.; Nowak, Z.; Sikora, M.; Chlubek, D. Treatment of Mandibular Hypomobility by Injections into the Temporomandibular Joints: A Systematic Review of the Substances Used. J. Clin. Med. 2022, 11, 2305. [Google Scholar] [CrossRef]
- Pihut, M.; Szuta, M.; Ferendiuk, E.; Zeńczak-Więckiewicz, D. Evaluation of Pain Regression in Patients with Temporomandibular Dysfunction Treated by Intra-Articular Platelet-Rich Plasma Injections: A Preliminary Report. BioMed Res. Int. 2014, 2014, 132369. [Google Scholar] [CrossRef]
- Kałużyński, K.; Trybek, G.; Smektała, T.; Masiuk, M.; Myśliwiec, L.; Sporniak-Tutak, K. Effect of Methylprednisolone, Hyaluronic Acid and Pioglitazone on Histological Remodeling of Temporomandibular Joint Cartilage in Rabbits Affected by Drug-Induced Osteoarthritis. Postepy Hig. Med. Dosw. Online 2016, 70, 74–79. [Google Scholar] [CrossRef]
- Javadi Hedayatabad, J.; Kachooei, A.R.; Taher Chaharjouy, N.; Vaziri, N.; Mehrad-Majd, H.; Emadzadeh, M.; Abolghasemian, M.; Ebrahimzadeh, M.H. The Effect of Ozone (O3) versus Hyaluronic Acid on Pain and Function in Patients with Knee Osteoarthritis: A Systematic Review and Meta-Analysis. Arch. Bone Jt. Surg. 2020, 8, 343–354. [Google Scholar] [CrossRef]
- Laver, L.; Marom, N.; Dnyanesh, L.; Mei-Dan, O.; Espregueira-Mendes, J.; Gobbi, A. PRP for Degenerative Cartilage Disease: A Systematic Review of Clinical Studies. Cartilage 2017, 8, 341–364. [Google Scholar] [CrossRef]
- Pavone, V.; Vescio, A.; Turchetta, M.; Giardina, S.M.C.; Culmone, A.; Testa, G. Injection-Based Management of Osteoarthritis of the Knee: A Systematic Review of Guidelines. Front. Pharmacol. 2021, 12, 661805. [Google Scholar] [CrossRef]
- Phillips, M.; Bhandari, M.; Grant, J.; Bedi, A.; Trojian, T.; Johnson, A.; Schemitsch, E. A Systematic Review of Current Clinical Practice Guidelines on Intra-Articular Hyaluronic Acid, Corticosteroid, and Platelet-Rich Plasma Injection for Knee Osteoarthritis: An International Perspective. Orthop. J. Sports Med. 2021, 9, 232596712110302. [Google Scholar] [CrossRef] [PubMed]
- Bjørnland, T.; Gjærum, A.A.; Møystad, A. Osteoarthritis of the Temporomandibular Joint: An Evaluation of the Effects and Complications of Corticosteroid Injection Compared with Injection with Sodium Hyaluronate. J. Oral Rehabil. 2007, 34, 583–589. [Google Scholar] [CrossRef] [PubMed]
- Parra, D.A.; Chan, M.; Krishnamurthy, G.; Spiegel, L.; Amaral, J.G.; Temple, M.J.; John, P.R.; Connolly, B.L. Use and Accuracy of US Guidance for Image-Guided Injections of the Temporomandibular Joints in Children with Arthritis. Pediatr. Radiol. 2010, 40, 1498–1504. [Google Scholar] [CrossRef] [PubMed]
- Stoll, M.L.; Good, J.; Sharpe, T.; Beukelman, T.; Young, D.; Waite, P.D.; Cron, R.Q. Intra-Articular Corticosteroid Injections to the Temporomandibular Joints Are Safe and Appear to Be Effective Therapy in Children with Juvenile Idiopathic Arthritis. J. Oral Maxillofac. Surg. 2012, 70, 1802–1807. [Google Scholar] [CrossRef] [PubMed]
- Skármeta, N.P.; Hormazábal, F.A.; Alvarado, J.; Rodriguez, A.M. Subcutaneous Lipoatrophy and Skin Depigmentation Secondary to TMJ Intra-Articular Corticosteroid Injection. J. Oral Maxillofac. Surg. 2017, 75, 2540.e1–2540.e5. [Google Scholar] [CrossRef]
- Isacsson, G.; Schumann, M.; Nohlert, E.; Mejersjö, C.; Tegelberg, Å. Pain Relief Following a Single-dose Intra-articular Injection of Methylprednisolone in the Temporomandibular Joint Arthralgia—A Multicentre Randomised Controlled Trial. J. Oral Rehabil. 2019, 46, 5–13. [Google Scholar] [CrossRef]
- Zhang, S.; Yap, A.U.J.; Toh, W.S. Stem Cells for Temporomandibular Joint Repair and Regeneration. Stem Cell Rev. Rep. 2015, 11, 728–742. [Google Scholar] [CrossRef]
- Satué, M.; Schüler, C.; Ginner, N.; Erben, R.G. Intra-Articularly Injected Mesenchymal Stem Cells Promote Cartilage Regeneration, but Do Not Permanently Engraft in Distant Organs. Sci. Rep. 2019, 9, 10153. [Google Scholar] [CrossRef]
- Zhang, S.; Hu, B.; Liu, W.; Wang, P.; Lv, X.; Chen, S.; Liu, H.; Shao, Z. Articular Cartilage Regeneration: The Role of Endogenous Mesenchymal Stem/Progenitor Cell Recruitment and Migration. Semin. Arthritis Rheum. 2020, 50, 198–208. [Google Scholar] [CrossRef]
- Embree, M.C.; Chen, M.; Pylawka, S.; Kong, D.; Iwaoka, G.M.; Kalajzic, I.; Yao, H.; Shi, C.; Sun, D.; Sheu, T.-J.; et al. Exploiting Endogenous Fibrocartilage Stem Cells to Regenerate Cartilage and Repair Joint Injury. Nat. Commun. 2016, 7, 13073. [Google Scholar] [CrossRef]
- Liao, W.-T.; Sun, J.-D.; Wang, Y.; He, Y.-Q.; Su, K.; Lu, Y.-Y.; Liao, G.; Sun, Y.-P. Histone Deacetylase Inhibitors Attenuated Interleukin-1β-Induced Chondrogenesis Inhibition in Synovium-Derived Mesenchymal Stem Cells of the Temporomandibular Joint. Bone Jt. Res. 2022, 11, 40–48. [Google Scholar] [CrossRef]
- Fan, Y.; Cui, C.; Li, P.; Bi, R.; Lyu, P.; Li, Y.; Zhu, S. Fibrocartilage Stem Cells in the Temporomandibular Joint: Insights from Animal and Human Studies. Front. Cell Dev. Biol. 2021, 9, 665995. [Google Scholar] [CrossRef] [PubMed]
- Bi, R.; Yin, Q.; Mei, J.; Chen, K.; Luo, X.; Fan, Y.; Zhu, S. Identification of Human Temporomandibular Joint Fibrocartilage Stem Cells with Distinct Chondrogenic Capacity. Osteoarthr. Cartil. 2020, 28, 842–852. [Google Scholar] [CrossRef]
- Liu, W.; Luo, H.; Wang, R.; Kang, Y.; Liao, W.; Sun, Y.; Chen, G.; Shao, L. Rapamycin-Induced Autophagy Promotes the Chondrogenic Differentiation of Synovium-Derived Mesenchymal Stem Cells in the Temporomandibular Joint in Response to IL-1β. BioMed Res. Int. 2020, 2020, 4035306. [Google Scholar] [CrossRef] [PubMed]
- Carboni, A.; Amodeo, G.; Perugini, M.; Arangio, P.; Orsini, R.; Scopelliti, D. Temporomandibular Disorders Clinical and Anatomical Outcomes After Fat-Derived Stem Cells Injection. J. Craniofac. Surg. 2019, 30, 793–797. [Google Scholar] [CrossRef] [PubMed]
- Mahmmood, V.H.; Shihab, S.M. Assessment of Therapeutic Effect of Intra-Articular Nanofat Injection for Temporomandibular Disorders. J. Craniofac. Surg. 2019, 30, 659–662. [Google Scholar] [CrossRef]
- De Riu, G.; Vaira, L.A.; Carta, E.; Meloni, S.M.; Sembronio, S.; Robiony, M. Bone Marrow Nucleated Cell Concentrate Autograft in Temporomandibular Joint Degenerative Disorders: 1-Year Results of a Randomized Clinical Trial. J. Cranio-Maxillofac. Surg. 2019, 47, 1728–1738. [Google Scholar] [CrossRef]
- Karic, V.; Chandran, R.; Abrahamse, H. Laser-Induced Differentiation of Human Adipose-Derived Stem Cells to Temporomandibular Joint Disc Cells. Lasers Surg. Med. 2021, 53, 567–577. [Google Scholar] [CrossRef]
- Karic, V.; Chandran, R.; Abrahamse, H. Photobiomodulation and Stem Cell Therapy for Temporomandibular Joint Disc Disorders. Photobiomodulation Photomed. Laser Surg. 2020, 38, 398–408. [Google Scholar] [CrossRef]
- Liau, L.L.; Looi, Q.H.; Chia, W.C.; Subramaniam, T.; Ng, M.H.; Law, J.X. Treatment of Spinal Cord Injury with Mesenchymal Stem Cells. Cell Biosci. 2020, 10, 112. [Google Scholar] [CrossRef]
- Molnar, V.; Pavelić, E.; Vrdoljak, K.; Čemerin, M.; Klarić, E.; Matišić, V.; Bjelica, R.; Brlek, P.; Kovačić, I.; Tremolada, C.; et al. Mesenchymal Stem Cell Mechanisms of Action and Clinical Effects in Osteoarthritis: A Narrative Review. Genes 2022, 13, 949. [Google Scholar] [CrossRef] [PubMed]
- Pagotto, L.E.C.; de Santana Santos, T.; Pastore, G.P. The Efficacy of Mesenchymal Stem Cells in Regenerating Structures Associated with the Temporomandibular Joint: A Systematic Review. Arch. Oral Biol. 2021, 125, 105104. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Samson, D.; Schoelles, K.M. Chapter 2: Medical Tests Guidance (2) Developing the Topic and Structuring Systematic Reviews of Medical Tests: Utility of PICOTS, Analytic Frameworks, Decision Trees, and Other Frameworks. J. Gen. Intern. Med. 2012, 27, 11–19. [Google Scholar] [CrossRef]
- About ACM. Available online: https://www.acm.org/about-acm (accessed on 25 June 2022).
- BASE—Bielefeld Academic Search Engine|What Is BASE? Available online: https://www.base-search.net/about/en/ (accessed on 25 June 2022).
- EBSCOhost Research Platform|EBSCO. Available online: https://www.ebsco.com/products/ebscohost-research-platform (accessed on 30 June 2022).
- About Google Scholar. Available online: https://scholar.google.com/intl/en/scholar/about.html (accessed on 25 June 2022).
- About. PubMed Overview. Available online: https://pubmed.ncbi.nlm.nih.gov/about/ (accessed on 25 June 2022).
- About|Elsevier Scopus Blog. Available online: https://blog.scopus.com/about (accessed on 30 June 2022).
- Matthews, T. LibGuides: Resources for Librarians: Web of Science Coverage Details. Available online: https://clarivate.libguides.com/librarianresources/coverage (accessed on 30 June 2022).
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A Web and Mobile App for Systematic Reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A Revised Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A Tool for Assessing Risk of Bias in Non-Randomised Studies of Interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef]
- Sembronio, S.; Tel, A.; Tremolada, C.; Lazzarotto, A.; Isola, M.; Robiony, M. Temporomandibular Joint Arthrocentesis and Microfragmented Adipose Tissue Injection for the Treatment of Internal Derangement and Osteoarthritis: A Randomized Clinical Trial. J. Oral Maxillofac. Surg. 2021, 79, 1447–1456. [Google Scholar] [CrossRef]
- De Souza Tesch, R.; Takamori, E.R.; Menezes, K.; Carias, R.B.V.; Dutra, C.L.M.; de Freitas Aguiar, M.; de Sousa Torraca, T.S.; Senegaglia, A.C.; Rebelatto, C.L.K.; Daga, D.R.; et al. Temporomandibular Joint Regeneration: Proposal of a Novel Treatment for Condylar Resorption after Orthognathic Surgery Using Transplantation of Autologous Nasal Septum Chondrocytes, and the First Human Case Report. Stem Cell Res. Ther. 2018, 9, 94. [Google Scholar] [CrossRef]
- Sit, R.W.-S.; Reeves, K.D.; Zhong, C.C.; Wong, C.H.L.; Wang, B.; Chung, V.C.; Wong, S.Y.; Rabago, D. Efficacy of Hypertonic Dextrose Injection (Prolotherapy) in Temporomandibular Joint Dysfunction: A Systematic Review and Meta-Analysis. Sci. Rep. 2021, 11, 14638. [Google Scholar] [CrossRef]
- Altman, R.; Hackel, J.; Niazi, F.; Shaw, P.; Nicholls, M. Efficacy and Safety of Repeated Courses of Hyaluronic Acid Injections for Knee Osteoarthritis: A Systematic Review. Semin. Arthritis Rheum. 2018, 48, 168–175. [Google Scholar] [CrossRef] [PubMed]
- Katagiri, W.; Endo, S.; Takeuchi, R.; Suda, D.; Saito, N.; Kobayashi, T. Conditioned Medium from Mesenchymal Stem Cells Improves Condylar Resorption Induced by Mandibular Distraction Osteogenesis in a Rat Model. Heliyon 2021, 7, e06530. [Google Scholar] [CrossRef]
- Oyonarte, R.; Becerra, D.; Díaz-Zúñiga, J.; Rojas, V.; Carrion, F. Morphological Effects of Mesenchymal Stem Cells and Pulsed Ultrasound on Condylar Growth in Rats: A Pilot Study. Aust. Orthod. J. 2013, 29, 3–12. [Google Scholar] [PubMed]
- Vega, A.; Martín-Ferrero, M.A.; Del Canto, F.; Alberca, M.; García, V.; Munar, A.; Orozco, L.; Soler, R.; Fuertes, J.J.; Huguet, M.; et al. Treatment of Knee Osteoarthritis with Allogeneic Bone Marrow Mesenchymal Stem Cells: A Randomized Controlled Trial. Transplantation 2015, 99, 1681–1690. [Google Scholar] [CrossRef] [PubMed]
- Park, Y.; Ha, C.; Lee, C.; Yoon, Y.C.; Park, Y. Cartilage Regeneration in Osteoarthritic Patients by a Composite of Allogeneic Umbilical Cord Blood-Derived Mesenchymal Stem Cells and Hyaluronate Hydrogel: Results from a Clinical Trial for Safety and Proof-of-Concept with 7 Years of Extended Follow-Up. Stem Cells Transl. Med. 2017, 6, 613–621. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Xie, L. An Update on Mesenchymal Stem Cell-Centered Therapies in Temporomandibular Joint Osteoarthritis. Stem Cells Int. 2021, 2021, 6619527. [Google Scholar] [CrossRef]
- Liu, W.; Sun, Y.; He, Y.; Zhang, H.; Zheng, Y.; Yao, Y.; Zhang, Z. IL-1β Impedes the Chondrogenic Differentiation of Synovial Fluid Mesenchymal Stem Cells in the Human Temporomandibular Joint. Int. J. Mol. Med. 2017, 39, 317–326. [Google Scholar] [CrossRef]
- Inoue, S.; Popp, F.C.; Koehl, G.E.; Piso, P.; Schlitt, H.J.; Geissler, E.K.; Dahlke, M.H. Immunomodulatory Effects of Mesenchymal Stem Cells in a Rat Organ Transplant Model. Transplantation 2006, 81, 1589–1595. [Google Scholar] [CrossRef]
- Waterman, R.S.; Tomchuck, S.L.; Henkle, S.L.; Betancourt, A.M. A New Mesenchymal Stem Cell (MSC) Paradigm: Polarization into a pro-Inflammatory MSC1 or an Immunosuppressive MSC2 Phenotype. PLoS ONE 2010, 5, e10088. [Google Scholar] [CrossRef]
- Holm, J.S.; Toyserkani, N.M.; Sorensen, J.A. Adipose-Derived Stem Cells for Treatment of Chronic Ulcers: Current Status. Stem Cell Res. Ther. 2018, 9, 142. [Google Scholar] [CrossRef]
- Szantyr, A.; Orski, M.; Marchewka, I.; Szuta, M.; Orska, M.; Zapała, J. Ocular Complications Following Autologous Fat Injections into Facial Area: Case Report of a Recovery from Visual Loss After Ophthalmic Artery Occlusion and a Review of the Literature. Aesthetic Plast. Surg. 2017, 41, 580–584. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nitecka-Buchta, A.; Walczynska-Dragon, K.; Kempa, W.M.; Baron, S. Platelet-Rich Plasma Intramuscular Injections—Antinociceptive Therapy in Myofascial Pain Within Masseter Muscles in Temporomandibular Disorders Patients: A Pilot Study. Front. Neurol. 2019, 10, 250. [Google Scholar] [CrossRef] [PubMed]
- Nitecka-Buchta, A.; Walczynska-Dragon, K.; Batko-Kapustecka, J.; Wieckiewicz, M. Comparison between Collagen and Lidocaine Intramuscular Injections in Terms of Their Efficiency in Decreasing Myofascial Pain within Masseter Muscles: A Randomized, Single-Blind Controlled Trial. Pain Res. Manag. 2018, 2018, 8261090. [Google Scholar] [CrossRef] [PubMed]
- Nowak, Z.; Chęciński, M.; Nitecka-Buchta, A.; Bulanda, S.; Ilczuk-Rypuła, D.; Postek-Stefańska, L.; Baron, S. Intramuscular Injections and Dry Needling within Masticatory Muscles in Management of Myofascial Pain. Systematic Review of Clinical Trials. Int. J. Environ. Res. Public. Health 2021, 18, 9552. [Google Scholar] [CrossRef] [PubMed]
- Nitecka-Buchta, A.; Nowak-Wachol, A.; Wachol, K.; Walczyńska-Dragon, K.; Olczyk, P.; Batoryna, O.; Kempa, W.; Baron, S. Myorelaxant Effect of Transdermal Cannabidiol Application in Patients with TMD: A Randomized, Double-Blind Trial. J. Clin. Med. 2019, 8, 1886. [Google Scholar] [CrossRef]
- Walczyńska-Dragon, K.; Baron, S.; Nitecka-Buchta, A.; Tkacz, E. Correlation between TMD and Cervical Spine Pain and Mobility: Is the Whole Body Balance TMJ Related? BioMed Res. Int. 2014, 2014, 582414. [Google Scholar] [CrossRef]
- Sikora, M.; Chęciński, M.; Sielski, M.; Chlubek, D. The Use of 3D Titanium Miniplates in Surgical Treatment of Patients with Condylar Fractures. J. Clin. Med. 2020, 9, 2923. [Google Scholar] [CrossRef]
- Chęcińska, K.; Chęciński, M.; Sikora, M.; Nowak, Z.; Karwan, S.; Chlubek, D. The Effect of Zirconium Dioxide (ZrO2) Nanoparticles Addition on the Mechanical Parameters of Polymethyl Methacrylate (PMMA): A Systematic Review and Meta-Analysis of Experimental Studies. Polymers 2022, 14, 1047. [Google Scholar] [CrossRef]
- Delcanho, R.; Val, M.; Nardini, L.G.; Manfredini, D. Botulinum Toxin for Treating Temporomandibular Disorders: What Is the Evidence? J. Oral Facial Pain Headache 2022, 36, 6–20. [Google Scholar] [CrossRef]
- Sikora, M.; Chęciński, M.; Nowak, Z.; Chęcińska, K.; Olszowski, T.; Chlubek, D. The Use of Titanium 3D Mini-Plates in the Surgical Treatment of Fractures of the Mandibular Condyle: A Systematic Review and Meta-Analysis of Clinical Trials. J. Clin. Med. 2021, 10, 3604. [Google Scholar] [CrossRef]
- Nitecka-Buchta, A.; Marek, B.; Baron, S. CGRP Plasma Level Changes in Patients with Temporomandibular Disorders Treated with Occlusal Splints—A Randomised Clinical Trial. Endokrynol. Pol. 2014, 65, 217–223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Sousa, D.F.M.; Malavazzi, T.C.D.S.; Deana, A.M.; Horliana, A.C.R.T.; Fernandes, K.P.S.; Bussadori, S.K.; Mesquita-Ferrari, R.A. Simultaneous Red and Infrared Light-Emitting Diodes Reduced Pain in Individuals with Temporomandibular Disorder: A Randomized, Controlled, Double-Blind, Clinical Trial. Lasers Med. Sci. 2022. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, F.Y.; Castelo, P.M.; Politti, F.; Rocha, M.M.; Beltramin, R.Z.; Salgueiro, M.D.C.C.; Gonçalves, M.L.L.; Nammour, S.; Brugnera Júnior, A.; Sfalcin, R.A.; et al. Immediate Evaluation of the Effect of Infrared LED Photobiomodulation on Childhood Sleep Bruxism: A Randomized Clinical Trial. Life 2022, 12, 964. [Google Scholar] [CrossRef] [PubMed]
- Pereira, E.D.B.M.; Basting, R.T.; Abdalla, H.B.; Garcez, A.S.; Napimoga, M.H.; Clemente-Napimoga, J.T. Photobiomodulation Inhibits Inflammation in the Temporomandibular Joint of Rats. J. Photochem. Photobiol. B 2021, 222, 112281. [Google Scholar] [CrossRef]
- Herpich, C.M.; Leal-Junior, E.C.P.; Politti, F.; de Paula Gomes, C.A.F.; Dos Santos Glória, I.P.; de Souza Amaral, M.d.F.R.; Herpich, G.; de Azevedo, L.M.A.; de Oliveira Gonzalez, T.; Biasotto-Gonzalez, D.A. Intraoral Photobiomodulation Diminishes Pain and Improves Functioning in Women with Temporomandibular Disorder: A Randomized, Sham-Controlled, Double-Blind Clinical Trial: Intraoral Photobiomodulation Diminishes Pain in Women with Temporomandibular Disorder. Lasers Med. Sci. 2020, 35, 439–445. [Google Scholar] [CrossRef]
- Costa, D.R.; Pessoa, D.R.; Seefeldt, V.B.; Costa, D.R.; Maia, D.T.L.; Dos Santos Maciel, T.; Mota, B.B.M.; Delpasso, C.A.; Ribeiro, C.A.D.; Nicolau, R.A. Orofacial Evaluation of Individuals with Temporomandibular Disorder after LED Therapy Associated or Not of Occlusal Splint: A Randomized Double-Blind Controlled Clinical Study. Lasers Med. Sci. 2021, 36, 1681–1689. [Google Scholar] [CrossRef]
- Nitecka-Buchta, A.; Buchta, P.; Tabeńska-Bosakowska, E.; Walczyńska-Dragoń, K.; Baron, S. Myorelaxant Effect of Bee Venom Topical Skin Application in Patients with RDC/TMD Ia and RDC/TMD Ib: A Randomized, Double Blinded Study. BioMed Res. Int. 2014, 2014, 296053. [Google Scholar] [CrossRef]
- Montes-Carmona, J.-F.; Gonzalez-Perez, L.-M.; Infante-Cossio, P. Treatment of Localized and Referred Masticatory Myofascial Pain with Botulinum Toxin Injection. Toxins 2020, 13, 6. [Google Scholar] [CrossRef]
- Gong, S.; Emperumal, C.P.; Al-Eryani, K.; Enciso, R. Regeneration of Temporomandibular Joint Using in Vitro Human Stem Cells: A Review. J. Tissue Eng. Regen. Med. 2022, 16, 591–604. [Google Scholar] [CrossRef]
- Chen, K.; Man, C.; Zhang, B.; Hu, J.; Zhu, S.-S. Effect of in Vitro Chondrogenic Differentiation of Autologous Mesenchymal Stem Cells on Cartilage and Subchondral Cancellous Bone Repair in Osteoarthritis of Temporomandibular Joint. Int. J. Oral Maxillofac. Surg. 2013, 42, 240–248. [Google Scholar] [CrossRef]
- Zaki, A.A.; Zaghloul, M.; Helal, M.E.; Mansour, N.A.; Grawish, M.E. Impact of Autologous Bone Marrow-Derived Stem Cells on Degenerative Changes of Articulating Surfaces Associated with the Arthritic Temporomandibular Joint: An Experimental Study in Rabbits. J. Oral Maxillofac. Surg. 2017, 75, 2529–2539. [Google Scholar] [CrossRef] [PubMed]
- El Qashty, R.M.N.; Mohamed, N.N.; Radwan, L.R.S.; Ibrahim, F.M.M. Effect of Bone Marrow Mesenchymal Stem Cells on Healing of Temporomandibular Joints in Rats with Induced Rheumatoid Arthritis. Eur. J. Oral Sci. 2018, 126, 272–281. [Google Scholar] [CrossRef] [PubMed]
- Köhnke, R.; Ahlers, M.O.; Birkelbach, M.A.; Ewald, F.; Krueger, M.; Fiedler, I.; Busse, B.; Heiland, M.; Vollkommer, T.; Gosau, M.; et al. Temporomandibular Joint Osteoarthritis: Regenerative Treatment by a Stem Cell Containing Advanced Therapy Medicinal Product (ATMP)—An In Vivo Animal Trial. Int. J. Mol. Sci. 2021, 22, 443. [Google Scholar] [CrossRef] [PubMed]
- Matheus, H.R.; Özdemir, Ş.D.; Guastaldi, F.P.S. Stem Cell-Based Therapies for Temporomandibular Joint Osteoarthritis and Regeneration of Cartilage/Osteochondral Defects: A Systematic Review of Preclinical Experiments. Osteoarthr. Cartil. 2022, 30, 1174–1185. [Google Scholar] [CrossRef]
- Ha, C.-W.; Park, Y.-B.; Kim, S.H.; Lee, H.-J. Intra-Articular Mesenchymal Stem Cells in Osteoarthritis of the Knee: A Systematic Review of Clinical Outcomes and Evidence of Cartilage Repair. Arthrosc. J. Arthrosc. Relat. Surg. Off. Publ. Arthrosc. Assoc. N. Am. Int. Arthrosc. Assoc. 2019, 35, 277–288.e2. [Google Scholar] [CrossRef]
- Punshon, G.; Vara, D.S.; Sales, K.M.; Seifalian, A.M. A Novel Method for the Extraction and Culture of Progenitor Stem Cells from Human Peripheral Blood for Use in Regenerative Medicine. Biotechnol. Appl. Biochem. 2011, 58, 328–334. [Google Scholar] [CrossRef]
- Hu, R.; Yang, Z.-Y.; Li, Y.-H.; Zhou, Z. Promotes Endothelial Differentiation and Angiogenesis of Periodontal Ligament Stem Cells by Activating Piezo1. Int. J. Stem Cells 2022. Online ahead of print. [Google Scholar] [CrossRef]
- Ogasawara, N.; Kano, F.; Hashimoto, N.; Mori, H.; Liu, Y.; Xia, L.; Sakamaki, T.; Hibi, H.; Iwamoto, T.; Tanaka, E.; et al. Factors Secreted from Dental Pulp Stem Cells Show Multifaceted Benefits for Treating Experimental Temporomandibular Joint Osteoarthritis. Osteoarthr. Cartil. 2020, 28, 831–841. [Google Scholar] [CrossRef]
- Guarda-Nardini, L.; Trojan, D.; Montagner, G.; Cogliati, E.; Bendini, M.; Manfredini, D. Human Amniotic Membrane Positioning in the Surgical Treatment of Temporomandibular Joint Degenerative Disorder. Case Rep. Surg. 2019, 2019, 6037191. [Google Scholar] [CrossRef]
- Ward, C.K.; Gill, R.G.; Davies, J.E. Umbilical Cord Stem Cell Lysate: A New Biologic Injection for Treatment of Temporomandibular Joint Inflammation. J. Oral Maxillofac. Surg. 2021, 79, e32–e33. [Google Scholar] [CrossRef]
- Zhu, S.; Zhang, B.; Man, C.; Ma, Y.; Hu, J. NEL-like Molecule-1-Modified Bone Marrow Mesenchymal Stem Cells/Poly Lactic-Co-Glycolic Acid Composite Improves Repair of Large Osteochondral Defects in Mandibular Condyle. Osteoarthr. Cartil. 2011, 19, 743–750. [Google Scholar] [CrossRef] [PubMed] [Green Version]


| Inclusion Criteria | Exclusion Criteria | |
|---|---|---|
| Problem | Human patients with temporomandibular joint disorders | Orthognathic surgery, mandibular condyle fracture, and ankylosis cases |
| Intervention | Intra-articular injections with stem cells | Non-autologous transplants, injections of other substances |
| Comparison | Any or none | - |
| Outcomes | Joint pain and mandibular mobility assessments | No initial values of the variables provided |
| Timeframe | No limits | |
| Settings | Primary studies | Non-English reports |
| First Author | Study Group Size (F/M) | Patients’ Age (Average) | Patients Treated Unilaterally/Bilaterally | Number of Joints Treated | Co-Intervention |
|---|---|---|---|---|---|
| Carboni [55] | 4 (1/3) | N/S (N/S) | 1/3 | 7 | Arthrocentesis |
| De Riu [57] | 15 (15/0) | 35–67 (48.2) | 15/0 | 15 | Arthrocentesis |
| Mahmmood [56] | 11 (8/3) | 18–34 (24.1) | 3/8 | 19 | None |
| Sembronio [75] | 20 (N/S) | 17–74 (43.3) | 14/6 | 26 | Arthrocentesis |
| de Souza Tesch [76] | 1 (0/1) | 27 (27) | 0/1 | 2 | Arthrocentesis |
| First Author | Study Type | (1) | (2) | (3) | (4) | (5) | (6) | (7) | (8) | Overall Risk of Bias |
|---|---|---|---|---|---|---|---|---|---|---|
| Carboni [55] | RT | Low | High | Low | S/C | Low | N/A | N/A | N/A | High |
| De Riu [57] | RT | Low | High | Low | Low | Low | N/A | N/A | N/A | High |
| Mahmmood [56] | NRSoI | N/A | Low | High | Low | Low | Low | Low | Low | High |
| Sembronio [75] | RT | Low | High | Low | S/C | Low | N/A | N/A | N/A | High |
| First Author | Group | Preoperative | After 7–10-Days | After 1-Month | After 6-Months | After 1-Year |
|---|---|---|---|---|---|---|
| Carboni [55] | Study group | 4.5 (100%) | 0.5 (11%) | |||
| Control group | 2 (100%) | 1 (50%) | ||||
| De Riu [57] | Study group | 8.7 (100%) | 4.6 (53%) | 1.2 (14%) | 1.7 (20%) | 2.3 (26%) |
| Control group | 8.5 (100%) | 4.4 (52%) | 2.1 (25%) | 3.5 (41%) | 5.5 (65%) | |
| Sembronio [75] | Study group | 7.2 (100%) | 3.1 (43%) | 1.7 (24%) | 1.2 (17%) | |
| Control group | 6.6 (100%) | 4.5 (68%) | 3.0 (45%) | 3.0 (45%) | ||
| Average | Study group | 6.8 (100%) | 3.9 (48%) | 1.5 (19%) | 1.1 (16%) | 2.3 (26%) |
| Control group | 5.7 (100%) | 4.5 (60%) | 2.6 (35%) | 2.5 (45%) | 5.5 (65%) | |
| Standard deviation | Study group | 2.1 | 1.1 | 0.4 | 0.6 | |
| Control group | 3.3 | 0.1 | 0.6 | 1.3 |
| First Author | Group | Preoperative | After 7–10-Days | After 14-Days | After 1-Month | After 6-Months | After 1-Year |
|---|---|---|---|---|---|---|---|
| Carboni [55] | Study group | 35.5 (100%) | 41.3 (116%) | ||||
| Control group | 27.5 (100%) | 30.8 (112%) | |||||
| De Riu [57] | Study group | 22.0 (100%) | 28.5 (129%) | 38.2 (174%) | 37.5 (171%) | 33.8 (154%) | |
| Control group | 23.2 (100%) | 28.4 (122%) | 37.7 (163%) | 34.9 (150%) | 28.1 (121%) | ||
| Mahmmood [56] | Study group | 28.2 (100%) | 34.4 (122%) | ||||
| Sembronio [75] | Study group | 30.7 (100%) | 36.3 (118%) | 40.7 (133%) | 42.4 (138%) | ||
| Control group | 32.5 (100%) | 35.7 (110%) | 37.7 (116%) | 38.7 (119%) | |||
| Average of the above | Study group | 29.1 (100%) | 32.4 (124%) | 34.4 (122%) | 39.5 (153%) | 40.4 (142%) | 33.8 (154%) |
| Control group | 27.7 (100%) | 32.1 (116%) | 37.7 (140%) | 34.8 (127%) | 28.1 (121%) | ||
| Standard deviation of the above | Study group | 5.6 | 5.5 | 1.8 | 2.5 | ||
| Control group | 4.7 | 5.2 | 0 | 4.0 | |||
| de Souza Tesch [76] | Study group | 23.0 (100%) | 30.0 (130%) | 27.0 (117%) | 32.0 (139%) | 36 (157%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chęciński, M.; Chęcińska, K.; Turosz, N.; Kamińska, M.; Nowak, Z.; Sikora, M.; Chlubek, D. Autologous Stem Cells Transplants in the Treatment of Temporomandibular Joints Disorders: A Systematic Review and Meta-Analysis of Clinical Trials. Cells 2022, 11, 2709. https://doi.org/10.3390/cells11172709
Chęciński M, Chęcińska K, Turosz N, Kamińska M, Nowak Z, Sikora M, Chlubek D. Autologous Stem Cells Transplants in the Treatment of Temporomandibular Joints Disorders: A Systematic Review and Meta-Analysis of Clinical Trials. Cells. 2022; 11(17):2709. https://doi.org/10.3390/cells11172709
Chicago/Turabian StyleChęciński, Maciej, Kamila Chęcińska, Natalia Turosz, Monika Kamińska, Zuzanna Nowak, Maciej Sikora, and Dariusz Chlubek. 2022. "Autologous Stem Cells Transplants in the Treatment of Temporomandibular Joints Disorders: A Systematic Review and Meta-Analysis of Clinical Trials" Cells 11, no. 17: 2709. https://doi.org/10.3390/cells11172709
APA StyleChęciński, M., Chęcińska, K., Turosz, N., Kamińska, M., Nowak, Z., Sikora, M., & Chlubek, D. (2022). Autologous Stem Cells Transplants in the Treatment of Temporomandibular Joints Disorders: A Systematic Review and Meta-Analysis of Clinical Trials. Cells, 11(17), 2709. https://doi.org/10.3390/cells11172709