
Peripheral Blood Mononuclear Cell Populations Correlate with Outcome in Patients with Metastatic Breast Cancer

 ,
,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Cell Isolation
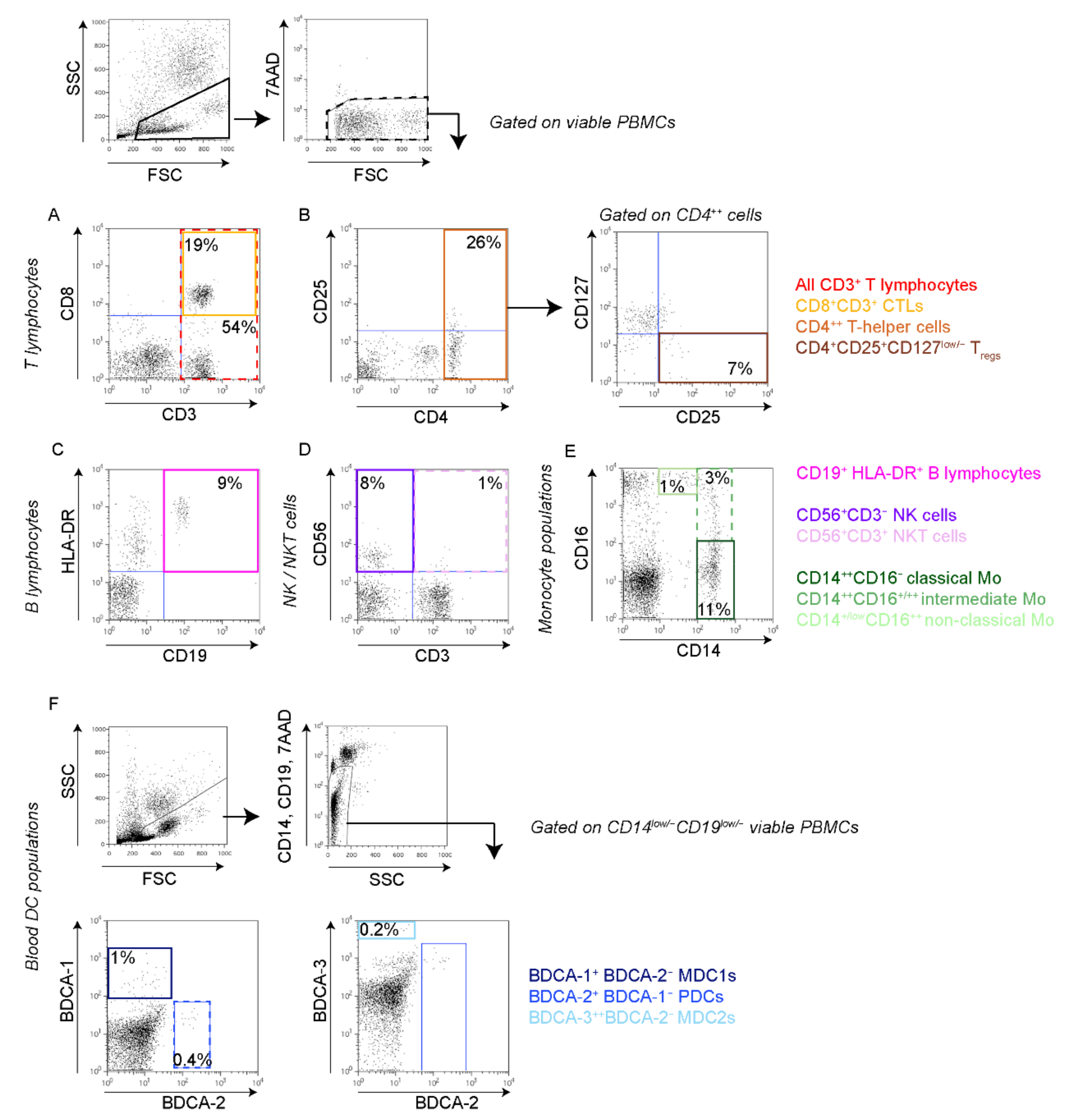
2.3. Flow Cytometry
2.4. Statistical Analyses
3. Results
3.1. Patient Characteristics
3.2. Associations between the Levels of Circulating T Lymphocyte Populations and Clinicopathological Variables
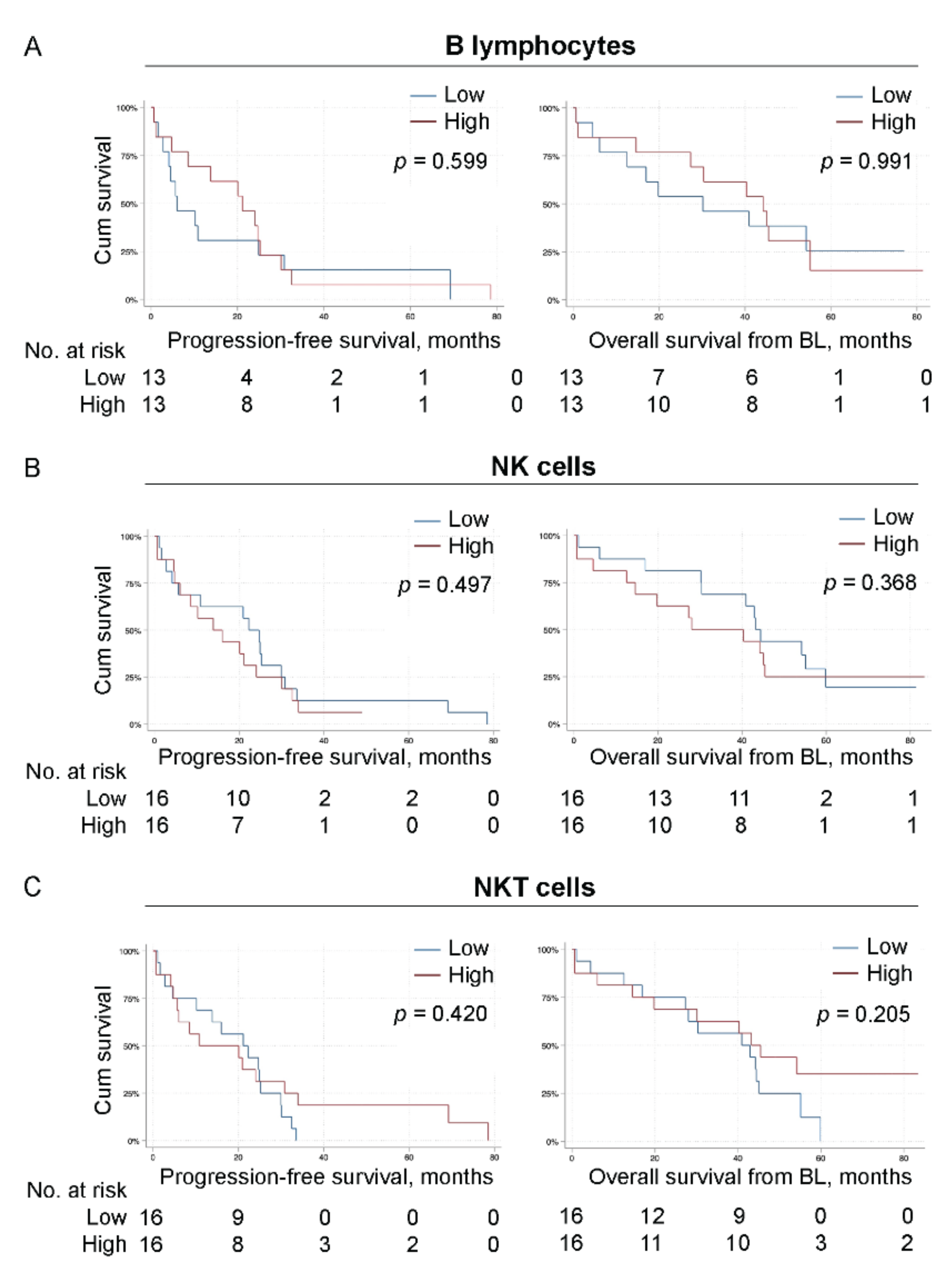
3.3. Associations between the Levels of B Lymphocytes, NK or NKT Cells and Clinicopathological Variables
3.4. Associations between the Levels of Monocyte Populations and Clinicopathological Variables
3.5. Associations between the Levels of Peripheral Blood Dendritic Cell Populations and Clinicopathological Variables
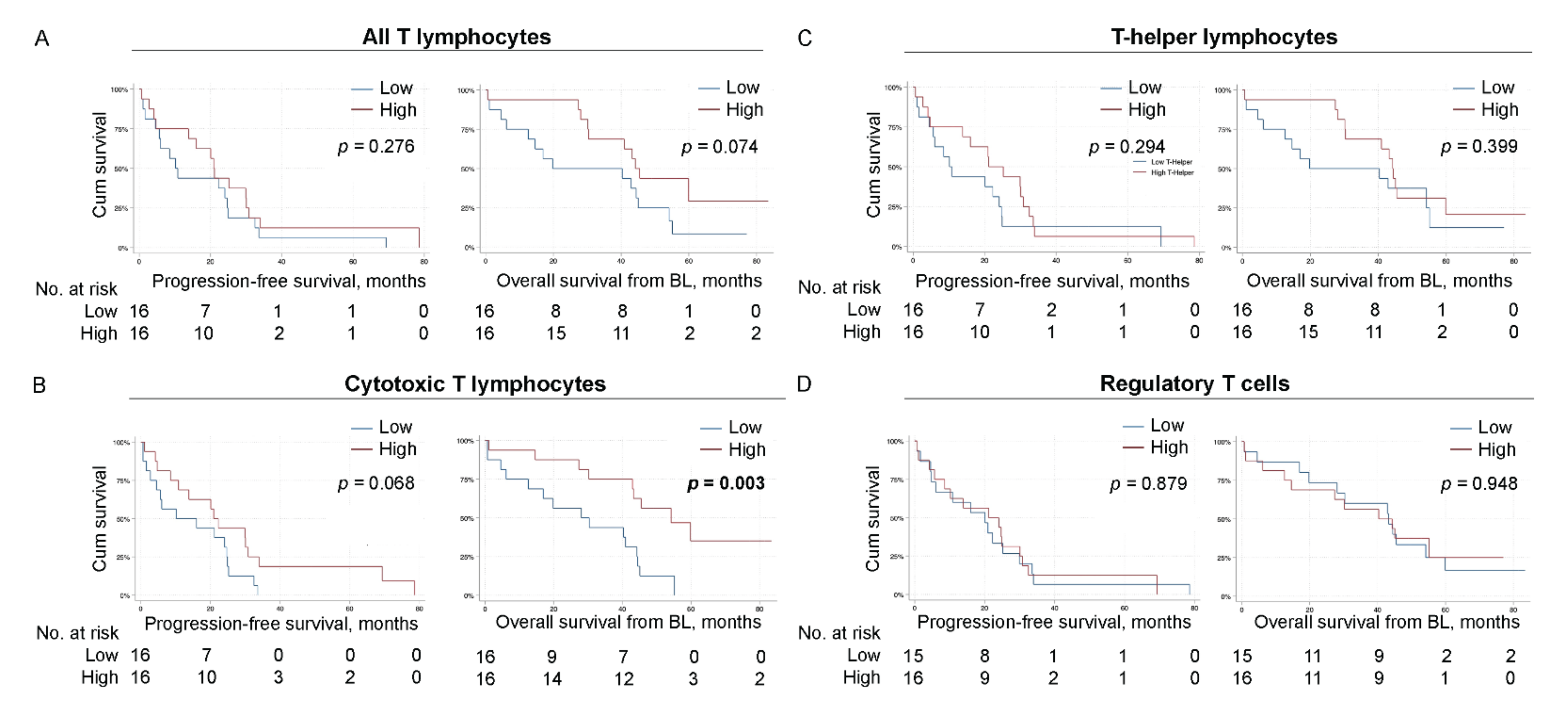
3.6. High Levels of Circulating CTLs Associate with Improved Overall Survival
3.7. Low levels of Intermediate Monocytes Associate with Improved Progression-Free Survival
3.8. High Levels of MDC2 Associate with Improved Progression-Free Survival
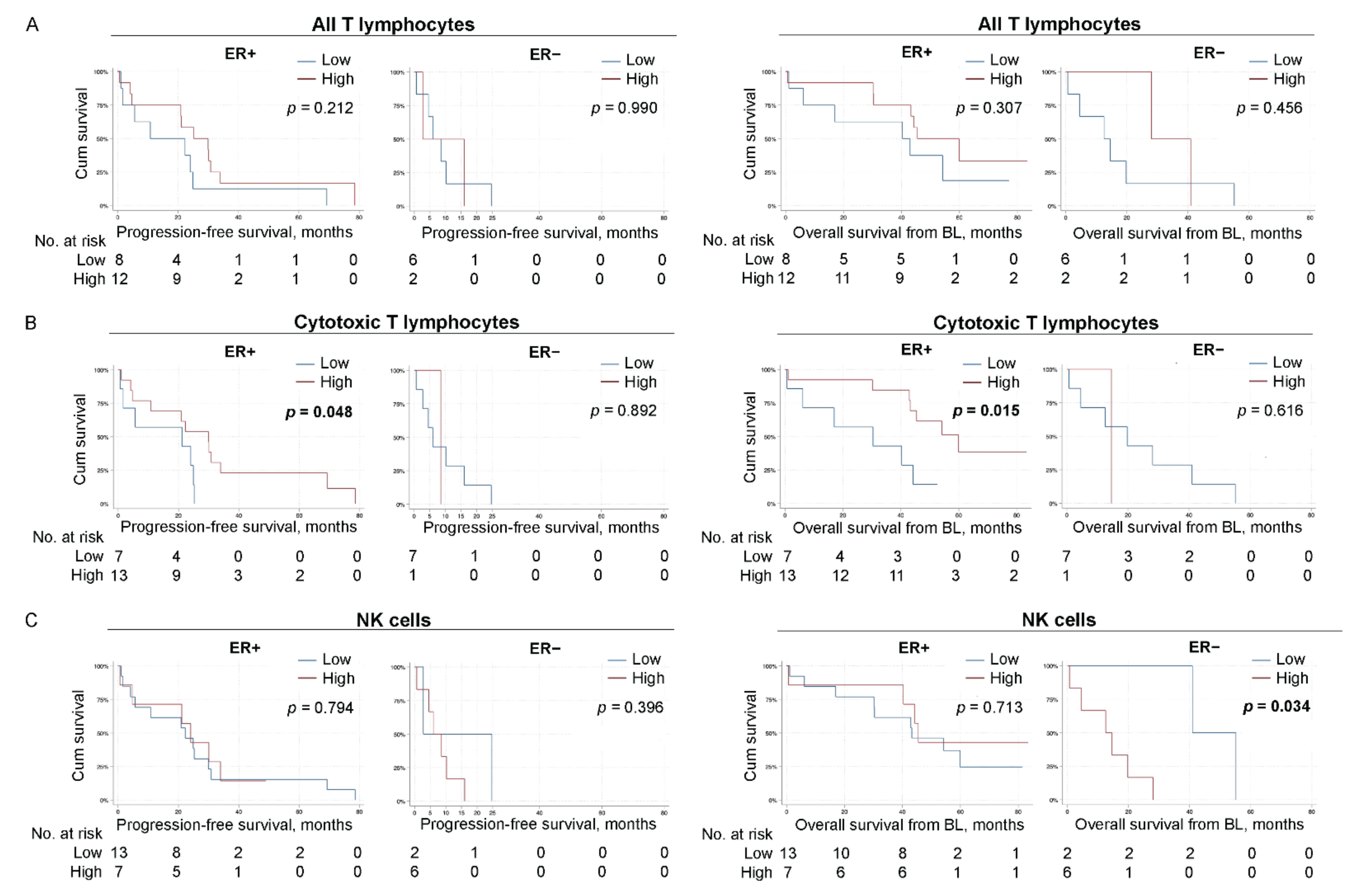
3.9. High Levels of CTLs Associate with Improved Survival in Patients with ER-Positive Primary Tumors
3.10. Low Levels of NK Cells Potentially Associate with Improved OS in Patients with ER-Negative Primary Tumors
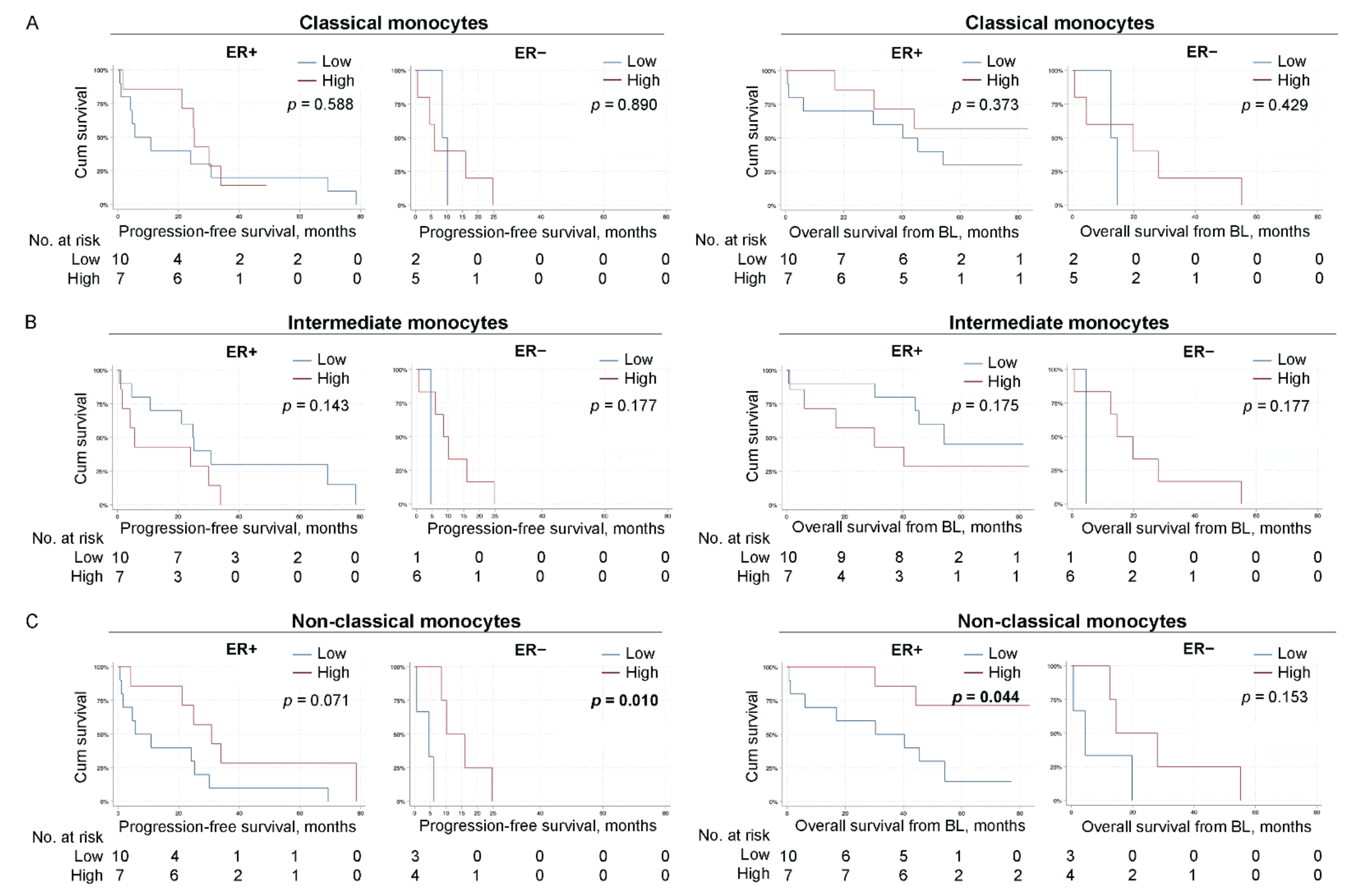
3.11. High Levels of Non-Classical Monocytes Associate with Improved Survival
3.12. Peripheral Blood Dendritic Cells Are Not Prognostic for Survival in Breast Cancer Patients
3.13. Uni- and Multivariable Cox Regression Analyses of Survival in Relation to CTLs
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Global Burden of Disease Cancer, C.; Fitzmaurice, C.; Allen, C.; Barber, R.M.; Barregard, L.; Bhutta, Z.A.; Brenner, H.; Dicker, D.J.; Chimed-Orchir, O.; Dandona, R.; et al. Global, Regional, and National Cancer Incidence, Mortality, Years of Life Lost, Years Lived with Disability, and Disability-Adjusted Life-years for 32 Cancer Groups, 1990 to 2015: A Systematic Analysis for the Global Burden of Disease Study. JAMA Oncol. 2017, 3, 524–548. [Google Scholar] [CrossRef] [PubMed]
- Harbeck, N.; Penault-Llorca, F.; Cortes, J.; Gnant, M.; Houssami, N.; Poortmans, P.; Ruddy, K.; Tsang, J.; Cardoso, F. Breast cancer. Nat. Rev. Dis. Primers 2019, 5, 66. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, F.; Paluch-Shimon, S.; Senkus, E.; Curigliano, G.; Aapro, M.S.; Andre, F.; Barrios, C.H.; Bergh, J.; Bhattacharyya, G.S.; Biganzoli, L.; et al. 5th ESO-ESMO international consensus guidelines for advanced breast cancer (ABC 5). Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. ESMO 2020, 31, 1623–1649. [Google Scholar] [CrossRef] [PubMed]
- Annaratone, L.; Cascardi, E.; Vissio, E.; Sarotto, I.; Chmielik, E.; Sapino, A.; Berrino, E.; Marchio, C. The Multifaceted Nature of Tumor Microenvironment in Breast Carcinomas. Pathobiology 2020, 87, 125–142. [Google Scholar] [CrossRef] [PubMed]
- Savas, P.; Salgado, R.; Denkert, C.; Sotiriou, C.; Darcy, P.K.; Smyth, M.J.; Loi, S. Clinical relevance of host immunity in breast cancer: From TILs to the clinic. Nat. Rev. Clin. Oncol. 2016, 13, 228–241. [Google Scholar] [CrossRef]
- Baxevanis, C.N.; Sofopoulos, M.; Fortis, S.P.; Perez, S.A. The role of immune infiltrates as prognostic biomarkers in patients with breast cancer. Cancer Immunol. Immunother 2019, 68, 1671–1680. [Google Scholar] [CrossRef]
- Solinas, C.; Carbognin, L.; De Silva, P.; Criscitiello, C.; Lambertini, M. Tumor-infiltrating lymphocytes in breast cancer according to tumor subtype: Current state of the art. Breast 2017, 35, 142–150. [Google Scholar] [CrossRef]
- Zhang, Z.; Zhu, Y.; Wang, Z.; Zhang, T.; Wu, P.; Huang, J. Yin-yang effect of tumor infiltrating B cells in breast cancer: From mechanism to immunotherapy. Cancer Lett. 2017, 393, 1–7. [Google Scholar] [CrossRef]
- Mao, Y.; Qu, Q.; Chen, X.; Huang, O.; Wu, J.; Shen, K. The Prognostic Value of Tumor-Infiltrating Lymphocytes in Breast Cancer: A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0152500. [Google Scholar] [CrossRef]
- Yeong, J.; Lim, J.C.T.; Lee, B.; Li, H.; Chia, N.; Ong, C.C.H.; Lye, W.K.; Putti, T.C.; Dent, R.; Lim, E.; et al. High Densities of Tumor-Associated Plasma Cells Predict Improved Prognosis in Triple Negative Breast Cancer. Front. Immunol. 2018, 9, 1209. [Google Scholar] [CrossRef]
- Muntasell, A.; Servitja, S.; Cabo, M.; Bermejo, B.; Perez-Buira, S.; Rojo, F.; Costa-Garcia, M.; Arpi, O.; Moraru, M.; Serrano, L.; et al. High Numbers of Circulating CD57(+) NK Cells Associate with Resistance to HER2-Specific Therapeutic Antibodies in HER2(+) Primary Breast Cancer. Cancer Immunol. Res. 2019, 7, 1280–1292. [Google Scholar] [CrossRef] [PubMed]
- Verma, C.; Kaewkangsadan, V.; Eremin, J.M.; Cowley, G.P.; Ilyas, M.; El-Sheemy, M.A.; Eremin, O. Natural killer (NK) cell profiles in blood and tumour in women with large and locally advanced breast cancer (LLABC) and their contribution to a pathological complete response (PCR) in the tumour following neoadjuvant chemotherapy (NAC): Differential restoration of blood profiles by NAC and surgery. J. Transl. Med. 2015, 13, 180. [Google Scholar] [CrossRef] [PubMed]
- Lundgren, C.; Bendahl, P.O.; Ekholm, M.; Ferno, M.; Forsare, C.; Kruger, U.; Nordenskjold, B.; Stal, O.; Ryden, L. Tumour-infiltrating lymphocytes as a prognostic and tamoxifen predictive marker in premenopausal breast cancer: Data from a randomised trial with long-term follow-up. Breast Cancer Res. BCR 2020, 22, 140. [Google Scholar] [CrossRef] [PubMed]
- Leek, R.D.; Lewis, C.E.; Whitehouse, R.; Greenall, M.; Clarke, J.; Harris, A.L. Association of macrophage infiltration with angiogenesis and prognosis in invasive breast carcinoma. Cancer Res. 1996, 56, 4625–4629. [Google Scholar] [PubMed]
- Finak, G.; Bertos, N.; Pepin, F.; Sadekova, S.; Souleimanova, M.; Zhao, H.; Chen, H.; Omeroglu, G.; Meterissian, S.; Omeroglu, A.; et al. Stromal gene expression predicts clinical outcome in breast cancer. Nat. Med. 2008, 14, 518–527. [Google Scholar] [CrossRef] [PubMed]
- Medrek, C.; Ponten, F.; Jirstrom, K.; Leandersson, K. The presence of tumor associated macrophages in tumor stroma as a prognostic marker for breast cancer patients. BMC Cancer 2012, 12, 306. [Google Scholar] [CrossRef]
- Gutkin, D.W.; Shurin, M.R. Clinical evaluation of systemic and local immune responses in cancer: Time for integration. Cancer Immunol Immunother 2014, 63, 45–57. [Google Scholar] [CrossRef][Green Version]
- Batalha, S.; Ferreira, S.; Brito, C. The Peripheral Immune Landscape of Breast Cancer: Clinical Findings and In Vitro Models for Biomarker Discovery. Cancers 2021, 13, 1305. [Google Scholar] [CrossRef]
- De Coana, Y.P.; Wolodarski, M.; Poschke, I.; Yoshimoto, Y.; Yang, Y.; Nystrom, M.; Edback, U.; Brage, S.E.; Lundqvist, A.; Masucci, G.V.; et al. Ipilimumab treatment decreases monocytic MDSCs and increases CD8 effector memory T cells in long-term survivors with advanced melanoma. Oncotarget 2017, 8, 21539–21553. [Google Scholar] [CrossRef]
- Sattui, S.; de la Flor, C.; Sanchez, C.; Lewis, D.; Lopez, G.; Rizo-Patron, E.; White, A.C., Jr.; Montes, M. Cryopreservation modulates the detection of regulatory T cell markers. Cytom. B Clin. Cytom. 2012, 82, 54–58. [Google Scholar] [CrossRef] [PubMed]
- Grutzner, E.; Stirner, R.; Arenz, L.; Athanasoulia, A.P.; Schrodl, K.; Berking, C.; Bogner, J.R.; Draenert, R. Kinetics of human myeloid-derived suppressor cells after blood draw. J. Transl. Med. 2016, 14, 2. [Google Scholar] [CrossRef] [PubMed]
- Bergenfelz, C.; Larsson, A.M.; von Stedingk, K.; Gruvberger-Saal, S.; Aaltonen, K.; Jansson, S.; Jernstrom, H.; Janols, H.; Wullt, M.; Bredberg, A.; et al. Systemic Monocytic-MDSCs Are Generated from Monocytes and Correlate with Disease Progression in Breast Cancer Patients. PLoS ONE 2015, 10, e0127028. [Google Scholar] [CrossRef] [PubMed]
- Bergenfelz, C.; Roxa, A.; Mehmeti, M.; Leandersson, K.; Larsson, A.M. Clinical relevance of systemic monocytic-MDSCs in patients with metastatic breast cancer. Cancer Immunol. Immunother 2020, 69, 435–448. [Google Scholar] [CrossRef]
- Yang, J.; Xu, J.; Sun, T. Predictive and prognostic value of circulating blood lymphocyte subsets in metastatic breast cancer. Cancer Med. 2019, 8, 492–500. [Google Scholar] [CrossRef] [PubMed]
- De Giorgi, U.; Mego, M.; Scarpi, E.; Giordano, A.; Giuliano, M.; Valero, V.; Alvarez, R.H.; Ueno, N.T.; Cristofanilli, M.; Reuben, J.M. Association between circulating tumor cells and peripheral blood monocytes in metastatic breast cancer. Adv. Med. Oncol. 2019, 11, 1758835919866065. [Google Scholar] [CrossRef] [PubMed]
- Mego, M.; Gao, H.; Cohen, E.N.; Anfossi, S.; Giordano, A.; Tin, S.; Fouad, T.M.; De Giorgi, U.; Giuliano, M.; Woodward, W.A.; et al. Circulating tumor cells (CTCs) are associated with abnormalities in peripheral blood dendritic cells in patients with inflammatory breast cancer. Oncotarget 2017, 8, 35656–35668. [Google Scholar] [CrossRef]
- Lafrenie, R.M.; Speigl, L.; Buckner, C.A.; Pawelec, G.; Conlon, M.S.; Shipp, C. Frequency of Immune Cell Subtypes in Peripheral Blood Correlates with Outcome for Patients with Metastatic Breast Cancer Treated with High-Dose Chemotherapy. Clin. Breast Cancer 2019, 19, 433–442. [Google Scholar] [CrossRef]
- Larsson, A.M.; Roxa, A.; Leandersson, K.; Bergenfelz, C. Impact of systemic therapy on circulating leukocyte populations in patients with metastatic breast cancer. Sci. Rep. 2019, 9, 13451. [Google Scholar] [CrossRef]
- Larsson, A.M.; Jansson, S.; Bendahl, P.O.; Levin Tykjaer Jorgensen, C.; Loman, N.; Graffman, C.; Lundgren, L.; Aaltonen, K.; Ryden, L. Longitudinal enumeration and cluster evaluation of circulating tumor cells improve prognostication for patients with newly diagnosed metastatic breast cancer in a prospective observational trial. Breast Cancer Res. BCR 2018, 20, 48. [Google Scholar] [CrossRef]
- Cardoso, F.; Costa, A.; Senkus, E.; Aapro, M.; Andre, F.; Barrios, C.H.; Bergh, J.; Bhattacharyya, G.; Biganzoli, L.; Cardoso, M.J.; et al. 3rd ESO-ESMO International Consensus Guidelines for Advanced Breast Cancer (ABC 3). Ann. Oncol. Off. J. Eur. Soc. Med. Oncol./ESMO 2017, 28, 16–33. [Google Scholar] [CrossRef]
- Wang, J.; Yang, J. Identification of CD4(+)CD25(+)CD127(-) regulatory T cells and CD14(+)HLA(-)DR(-)/low myeloid-derived suppressor cells and their roles in the prognosis of breast cancer. Biomed Rep. 2016, 5, 208–212. [Google Scholar] [CrossRef] [PubMed]
- Feng, A.L.; Zhu, J.K.; Sun, J.T.; Yang, M.X.; Neckenig, M.R.; Wang, X.W.; Shao, Q.Q.; Song, B.F.; Yang, Q.F.; Kong, B.H.; et al. CD16+ monocytes in breast cancer patients: Expanded by monocyte chemoattractant protein-1 and may be useful for early diagnosis. Clin. Exp. Immunol. 2011, 164, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Mego, M.; Gao, H.; Cohen, E.N.; Anfossi, S.; Giordano, A.; Sanda, T.; Fouad, T.M.; De Giorgi, U.; Giuliano, M.; Woodward, W.A.; et al. Circulating Tumor Cells (CTC) Are Associated with Defects in Adaptive Immunity in Patients with Inflammatory Breast Cancer. J. Cancer 2016, 7, 1095–1104. [Google Scholar] [CrossRef] [PubMed]
- DeNardo, D.G.; Brennan, D.J.; Rexhepaj, E.; Ruffell, B.; Shiao, S.L.; Madden, S.F.; Gallagher, W.M.; Wadhwani, N.; Keil, S.D.; Junaid, S.A.; et al. Leukocyte complexity predicts breast cancer survival and functionally regulates response to chemotherapy. Cancer Discov. 2011, 1, 54–67. [Google Scholar] [CrossRef]
- Liu, S.; Lachapelle, J.; Leung, S.; Gao, D.; Foulkes, W.D.; Nielsen, T.O. CD8+ lymphocyte infiltration is an independent favorable prognostic indicator in basal-like breast cancer. Breast Cancer Res. BCR 2012, 14, R48. [Google Scholar] [CrossRef]
- Mahmoud, S.M.; Paish, E.C.; Powe, D.G.; Macmillan, R.D.; Grainge, M.J.; Lee, A.H.; Ellis, I.O.; Green, A.R. Tumor-infiltrating CD8+ lymphocytes predict clinical outcome in breast cancer. J. Clin. Oncol. 2011, 29, 1949–1955. [Google Scholar] [CrossRef]
- Badr, N.M.; Berditchevski, F.; Shaaban, A.M. The Immune Microenvironment in Breast Carcinoma: Predictive and Prognostic Role in the Neoadjuvant Setting. Pathobiology 2020, 87, 61–74. [Google Scholar] [CrossRef]
- Stanton, S.E.; Disis, M.L. Clinical significance of tumor-infiltrating lymphocytes in breast cancer. J. Immunother Cancer 2016, 4, 59. [Google Scholar] [CrossRef]
- Shou, J.; Zhang, Z.; Lai, Y.; Chen, Z.; Huang, J. Worse outcome in breast cancer with higher tumor-infiltrating FOXP3+ Tregs: A systematic review and meta-analysis. BMC Cancer 2016, 16, 687. [Google Scholar] [CrossRef]
- Liu, S.; Foulkes, W.D.; Leung, S.; Gao, D.; Lau, S.; Kos, Z.; Nielsen, T.O. Prognostic significance of FOXP3+ tumor-infiltrating lymphocytes in breast cancer depends on estrogen receptor and human epidermal growth factor receptor-2 expression status and concurrent cytotoxic T-cell infiltration. Breast Cancer Res. BCR 2014, 16, 432. [Google Scholar] [CrossRef]
- Collin, M.; Bigley, V. Human dendritic cell subsets: An update. Immunology 2018, 154, 3–20. [Google Scholar] [CrossRef] [PubMed]
- Schmid, P.; Adams, S.; Rugo, H.S.; Schneeweiss, A.; Barrios, C.H.; Iwata, H.; Dieras, V.; Hegg, R.; Im, S.A.; Shaw Wright, G.; et al. Atezolizumab and Nab-Paclitaxel in Advanced Triple-Negative Breast Cancer. N. Engl. J. Med. 2018, 379, 2108–2121. [Google Scholar] [CrossRef] [PubMed]
- Cortes, J.; Cescon, D.W.; Rugo, H.S.; Nowecki, Z.; Im, S.A.; Yusof, M.M.; Gallardo, C.; Lipatov, O.; Barrios, C.H.; Holgado, E.; et al. Pembrolizumab plus chemotherapy versus placebo plus chemotherapy for previously untreated locally recurrent inoperable or metastatic triple-negative breast cancer (KEYNOTE-355): A randomised, placebo-controlled, double-blind, phase 3 clinical trial. Lancet 2020, 396, 1817–1828. [Google Scholar] [CrossRef]
- Egelston, C.; Guo, W.; Yost, S.; Lee, J.S.; Rose, D.; Avalos, C.; Ye, J.; Frankel, P.; Schmolze, D.; Waisman, J.; et al. Pre-existing effector T-cell levels and augmented myeloid cell composition denote response to CDK4/6 inhibitor palbociclib and pembrolizumab in hormone receptor-positive metastatic breast cancer. J Immunother Cancer 2021, 9, e002084. [Google Scholar] [CrossRef] [PubMed]
- Mehmeti-Ajradini, M.; Bergenfelz, C.; Larsson, A.M.; Carlsson, R.; Riesbeck, K.; Ahl, J.; Janols, H.; Wullt, M.; Bredberg, A.; Kallberg, E.; et al. Human G-MDSCs are neutrophils at distinct maturation stages promoting tumor growth in breast cancer. Life Sci. Alliance 2020, 3, e202000893. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient and Tumor Characteristics | CTLs | Tregs | CD8/ CD3 | CD4/ CD3 | B Cells | NK Cells | Classical Mo | Intermediate Mo | Non-Classical Mo | MDC1 |
|---|---|---|---|---|---|---|---|---|---|---|
| Age | 0.077 a | 0.200 a | 0.013a | 0.077 a | 0.695 a | 0.723 a | 0.842 a | 0.180 a | 0.568 a | 0.576 a |
| ECOG | 0.109 b | 0.493 b | 0.666 b | 0.666 b | 0.181 b | 0.859 b | 0.134 b | 1.000 b | 0.023b | 0.859 b |
| PT histological subtype | 0.754 b | 0.049b | 0.660 b | 1.000 b | 0.053 b | 0.050b | 0.446 b | 0.720 b | 0.092 b | 0.007b |
| PT NHG | 0.336 b | 0.021b | 1.000 b | 0.208 b | 0.322 b | 0.489 b | 1.000 b | 1.000 b | 0.087 b | 0.811 b |
| PT ER | 0.033b | 1.000 b | 0.410 b | 0.096 b | 0.405 b | 0.096 b | 0.371 b | 0.078 b | 0.659 b | 1.000 b |
| PT PR | 0.001a | 0.691 a | 0.004a | 0.00005a | 1.000 b | 0.038a | 0.006a | 0.292 a | 0.827 a | 0.462 a |
| PT HER2 | 1.000 b | 0.338 b | 0.045b | 0.311 b | 1.000 b | 0.149 b | 1.000 b | 1.000 b | 1.000 b | 0.149 b |
| MET ER | 0.429 b | 1.000 b | 1.000 b | 0.464 b | 0.478 b | 0.464 b | 0.478 b | 0.435 b | 1.000 b | 1.000 b |
| MET PR | 1.000 b | 0.248 b | 0.310 a | 0.047b | 0.391 b | 0.696 b | 0.099 b | 1.000 b | 0.387 b | 0.228 b |
| MET HER2 | 1.000 b | 0.593 b | 0.225 b | 1.000 b | 0.553 b | 0.238 b | 1.000 b | 0.229 b | 1.000 b | 0.565 b |
| No of metastatic sites (<3 vs. >/=3) | 0.072 a | 0.347 a | 0.719 a | 0.280 a | 0.047a | 0.280 a | 0.863 a | 0.168 a | 0.343 a | 0.213 a |
| Visceral metastases | 0.072 a | 0.886 a | 0.719 a | 0.280 a | 0.420 a | 0.719 a | 0.695 b | 1.000 b | 0.236 b | 0.038a |
| de novo MBC vs. distant recurrence | 1.000 b | 0.172 b | 0.043b | 0.333 b | 1.000 b | 0.333 b | 1.000 b | 1.000 b | 0.595 b | 0.654 b |
| CTC (</≥5) | 0.480 a | 0.210 a | 1.000 a | 1.000 a | 0.047a | 0.480 a | 0.816 a | 0.034a | 0.310 a | 0.366 a |
| Dead vs. alive | 0.037b | 0.685 b | 1.00 b | 0.685 b | 1.00 b | 1.00 b | 0.678 b | 0.420 b | 0.209 b | 0.220 b |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Larsson, A.-M.; Nordström, O.; Johansson, A.; Rydén, L.; Leandersson, K.; Bergenfelz, C. Peripheral Blood Mononuclear Cell Populations Correlate with Outcome in Patients with Metastatic Breast Cancer. Cells 2022, 11, 1639. https://doi.org/10.3390/cells11101639
Larsson A-M, Nordström O, Johansson A, Rydén L, Leandersson K, Bergenfelz C. Peripheral Blood Mononuclear Cell Populations Correlate with Outcome in Patients with Metastatic Breast Cancer. Cells. 2022; 11(10):1639. https://doi.org/10.3390/cells11101639
Chicago/Turabian StyleLarsson, Anna-Maria, Olle Nordström, Alexandra Johansson, Lisa Rydén, Karin Leandersson, and Caroline Bergenfelz. 2022. "Peripheral Blood Mononuclear Cell Populations Correlate with Outcome in Patients with Metastatic Breast Cancer" Cells 11, no. 10: 1639. https://doi.org/10.3390/cells11101639
APA StyleLarsson, A.-M., Nordström, O., Johansson, A., Rydén, L., Leandersson, K., & Bergenfelz, C. (2022). Peripheral Blood Mononuclear Cell Populations Correlate with Outcome in Patients with Metastatic Breast Cancer. Cells, 11(10), 1639. https://doi.org/10.3390/cells11101639