
Short-Term Evaluation of Cellular Fate in an Ovine Bone Formation Model

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Animal Experiments
2.2. Selection of STRO-4-Positive MSCs
2.3. CM-Dil Labelling
2.4. MNP Labelling of STRO-4-Positive oMSCs
2.5. Encapsulation of oMSCs within an ECM Gel Construct for In Vivo Delivery
2.6. Assessment of Cellular Viability by LDH Staining
2.7. Histology
2.8. Immunocytochemistry
2.9. Quantification of C-Reactive Protein Levels by ELISA
2.10. Statistical Analysis
3. Results
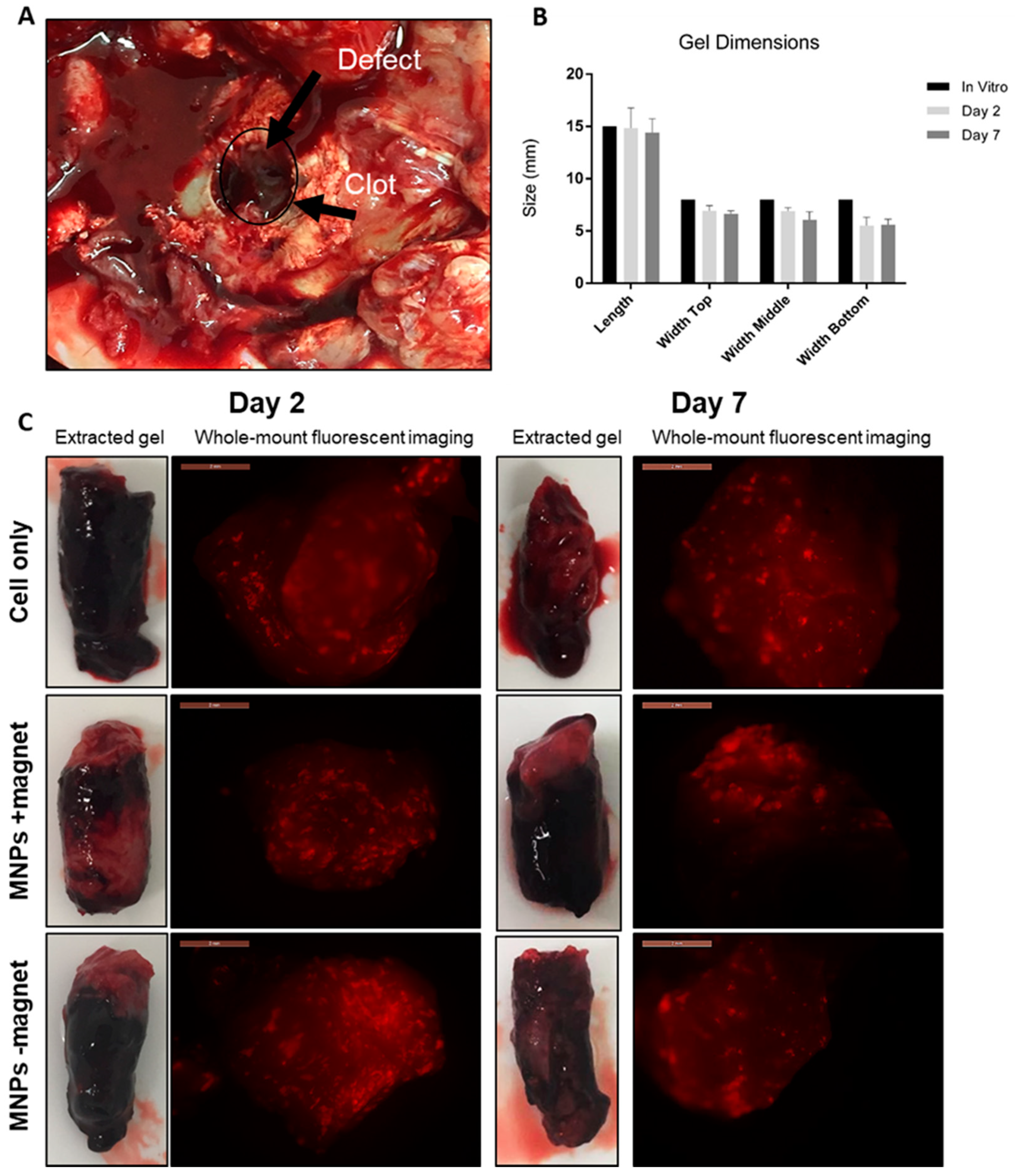
3.1. Implants Remained Intact with No Degradation Observed at Either 2 or 7 Days Post-Implantation
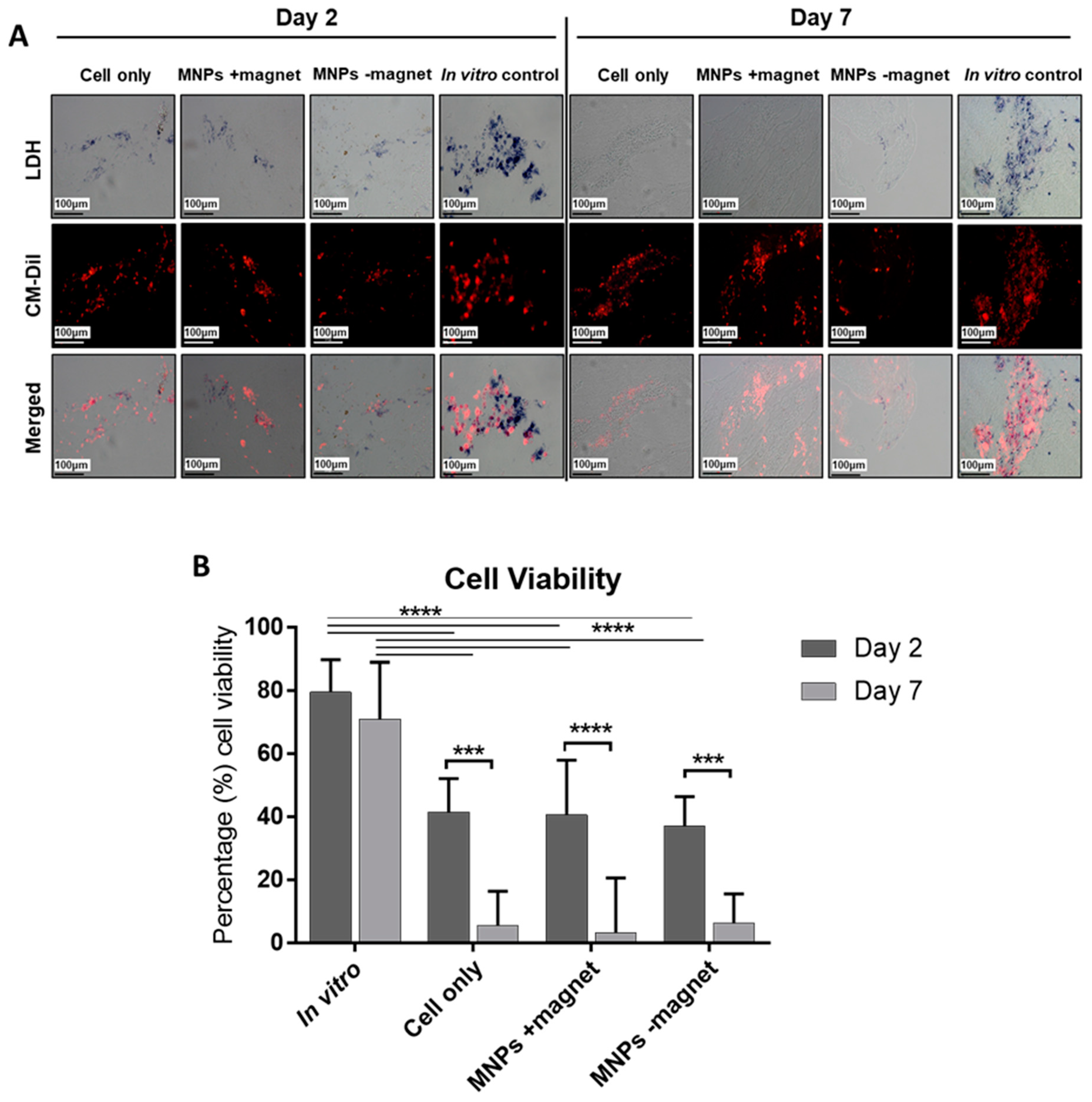
3.2. Significant Loss in Cell Viability Determined at 7 Days Post-Implantation
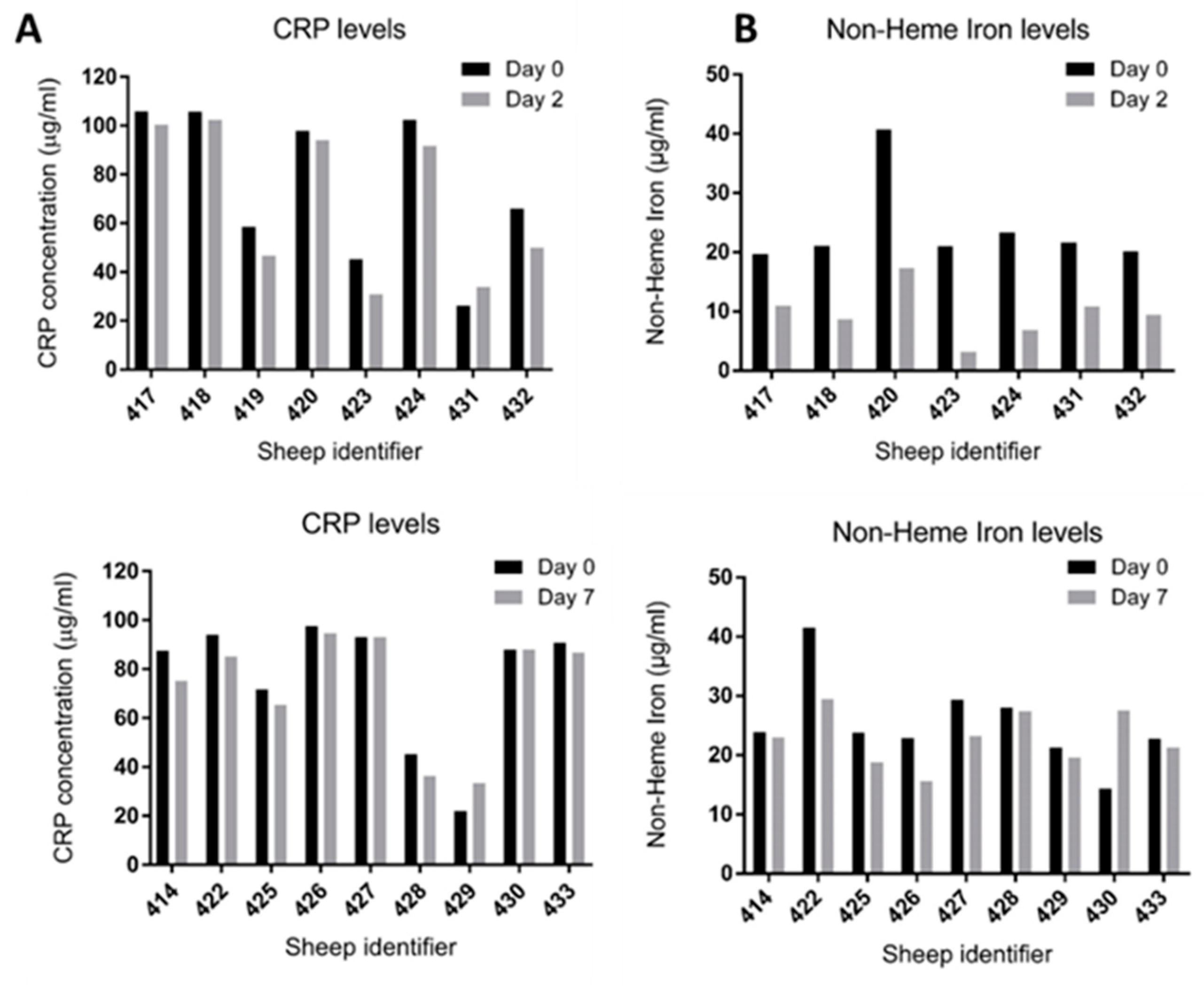
3.3. No Adverse Inflammatory Response and No Elevation in Non-Haem Iron Level Detected at Days 2 and 7
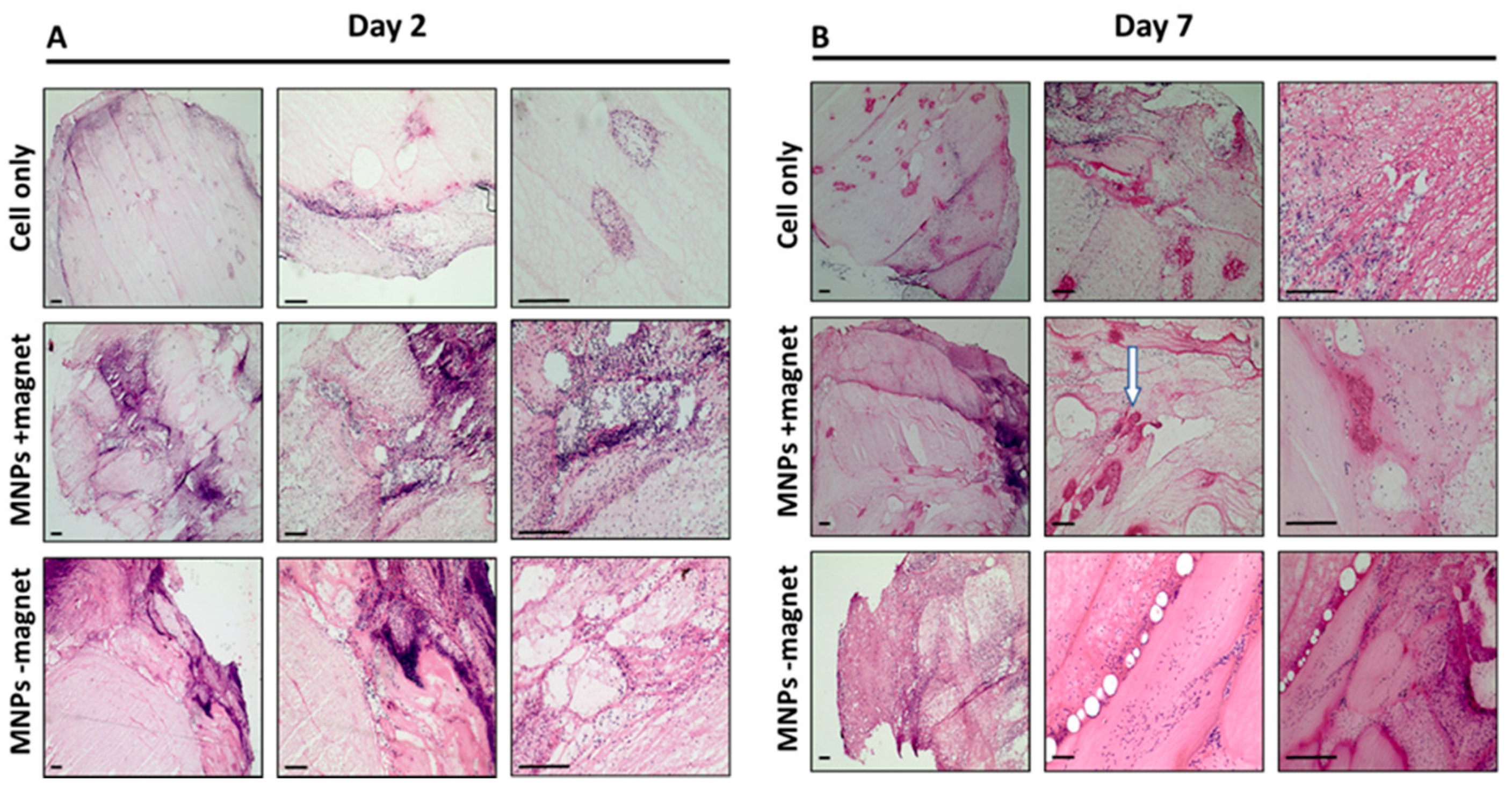
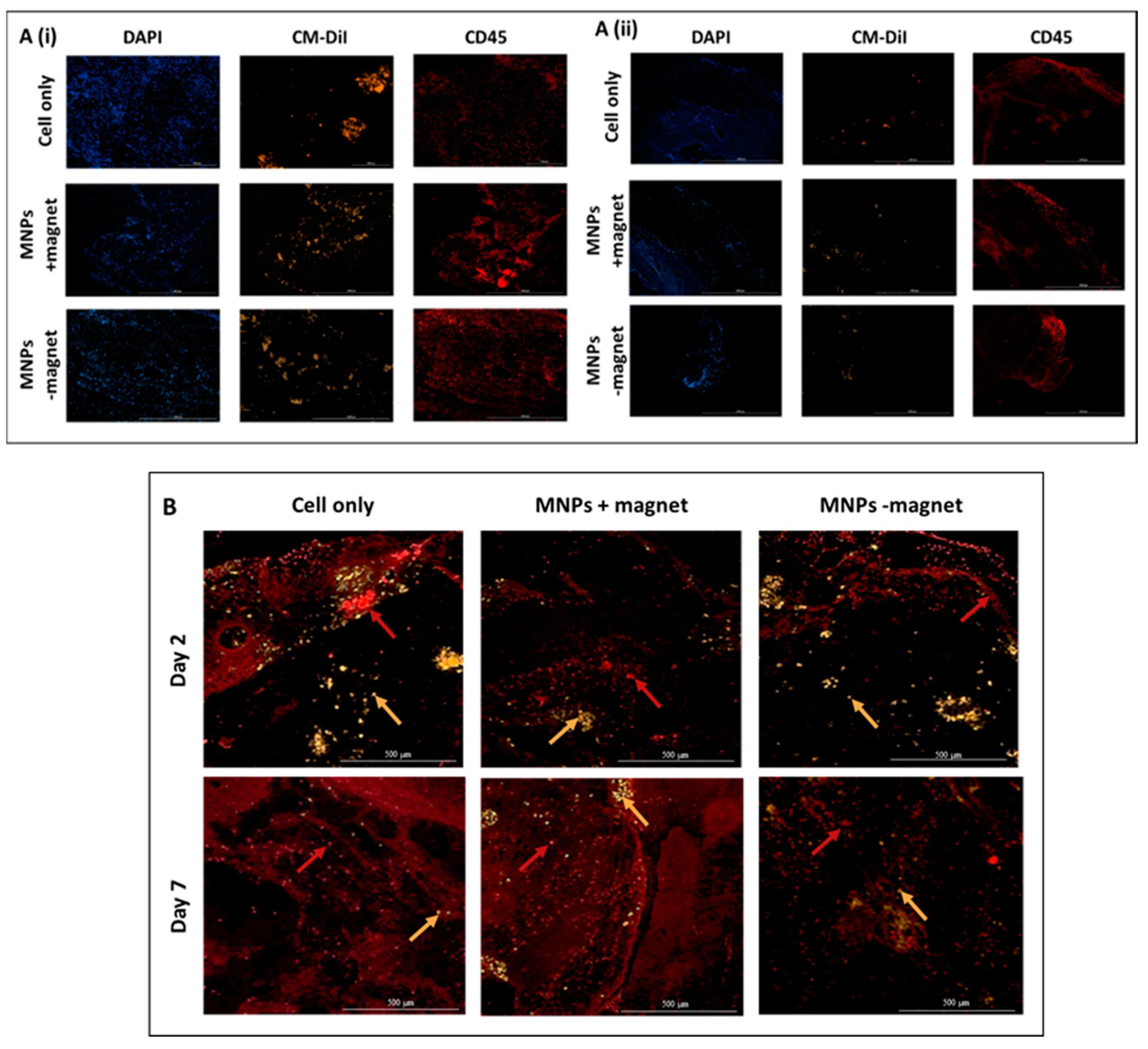
3.4. Cellular Infiltration within the ECM Construct Is Observed for All Groups
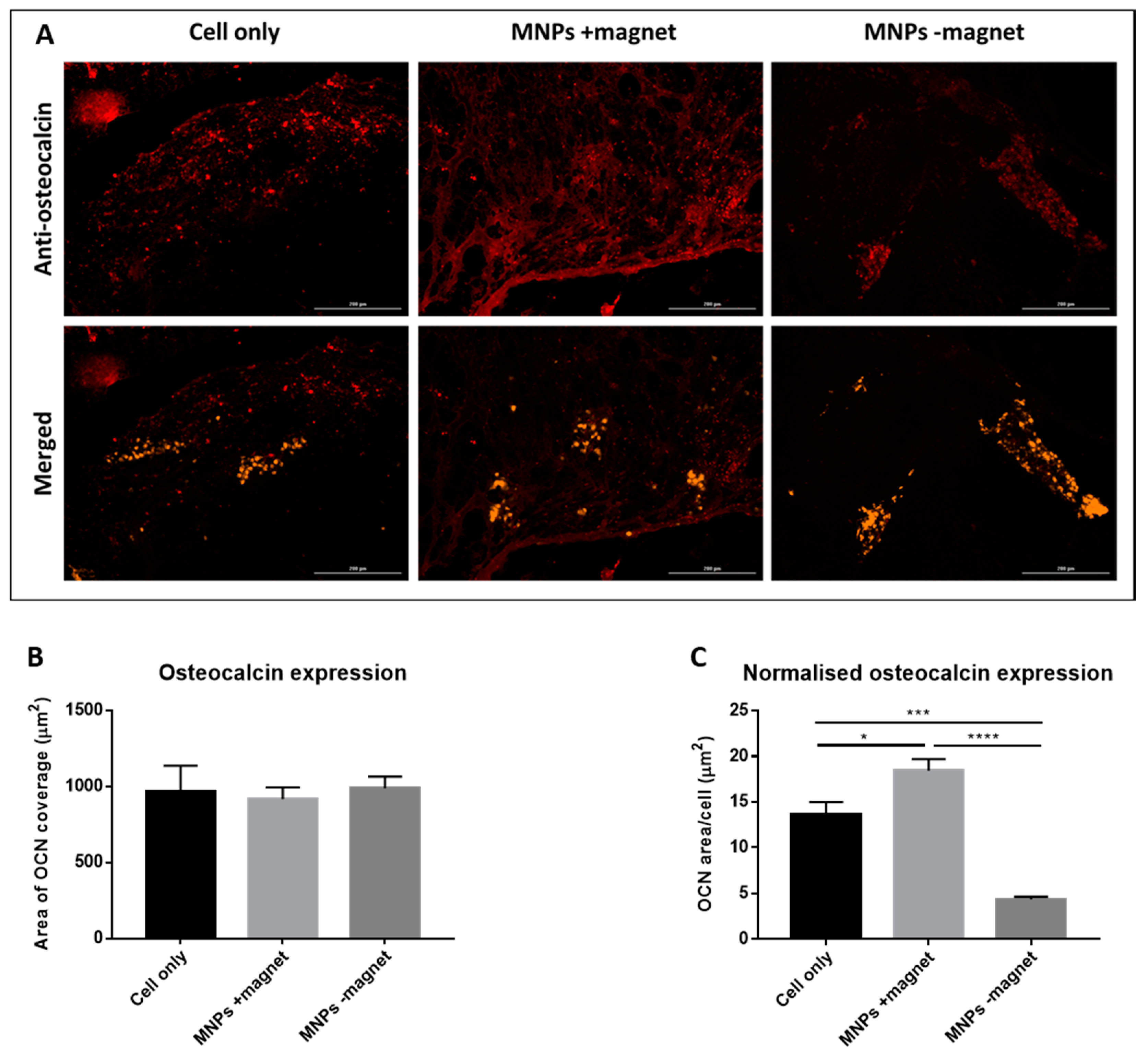
3.5. Osteocalcin Expression by Implanted Cells Is Observed in Day 7 ECM Constructs from All Three Groups
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Markides, H.; Rotherham, M.; El Haj, A.J. Biocompatibility and Toxicity of Magnetic Nanoparticles in Regenerative Medicine. J. Nanomater. 2012, 2012. [Google Scholar] [CrossRef] [Green Version]
- Pearce, A.I.; Richards, R.; Milz, S.; Schneider, E.; Pearce, S.G. Animal models for implant biomaterial research in bone: A review. Eur. Cells Mater. 2007, 13, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Gothard, D.; Smith, E.L.; Kanczler, J.; Rashidi, H.; Qutachi, O.; Henstock, J.; Rotherham, M.; El Haj, A.; Shakesheff, K.; Oreffo, R. Tissue engineered bone using select growth factors: A comprehensive review of animal studies and clinical translation studies in man. Eur. Cells Mater. 2014, 28, 166–208. [Google Scholar] [CrossRef] [PubMed]
- Amini, A.R.; Laurencin, C.T.; Nukavarapu, S.P. Bone Tissue Engineering: Recent Advances and Challenges. Crit. Rev. Biomed. Eng. 2012, 40, 363–408. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Markides, H.; Newell, K.J.; Rudorf, H.; Ferreras, L.B.; Dixon, J.E.; Morris, R.H.; Graves, M.; Kaggie, J.; Henson, F.; El Haj, A.J. Ex Vivo MRI cell tracking of autologous mesenchymal stromal cells in an ovine osteochondral defect model. Stem Cell Res. Ther. 2019, 10, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Markides, H.; Kehoe, O.; Morris, R.H.; El Haj, A.J. Whole body tracking of superparamagnetic iron oxide nanoparticle-labelled cells—a rheumatoid arthritis mouse model. Stem Cell Res. Ther. 2013, 4, 126. [Google Scholar] [CrossRef] [Green Version]
- Harrison, R.; Markides, H.; Morris, R.H.; Richards, P.; El Haj, A.J.; Sottile, V. Autonomous magnetic labelling of functional mesenchymal stem cells for improved traceability and spatial control in cell therapy applications. J. Tissue Eng. Regen. Med. 2016, 11, 2333–2348. [Google Scholar] [CrossRef]
- Kwan, T.D.; Markides, H.; Wang, W.; Yu, T.; Chen, G.-Q.; Liu, W.; El Haj, A.J. The Application of Nanomagnetic Approaches for Targeting Adipose Derived Stem Cells for Use in Tendon Repair. J. Nanosci. Nanotechnol. 2016, 16, 8989–8999. [Google Scholar] [CrossRef]
- Gonçalves, A.; Rotherham, M.; Markides, H.; Rodrigues, M.; Reis, R.; Gomes, M.; El Haj, A. Triggering the activation of Activin A type II receptor in human adipose stem cells towards tenogenic commitment using mechanomagnetic stimulation. Nanomed. Nanotechnol. Biol. Med. 2018, 14, 1149–1159. [Google Scholar] [CrossRef] [PubMed]
- Pankhurst, Q.A.; Connolly, J.; Jones, S.K.; Dobson, J. Applications of magnetic nanoparticles in biomedicine. J. Phys. D Appl. Phys. 2003, 36, R167–R181. [Google Scholar] [CrossRef] [Green Version]
- Banerjee, R.; Katsenovich, Y.; Lagos, L.; McIintosh, M.; Zhang, X.; Li, C.-Z. Nanomedicine: Magnetic Nanoparticles and their Biomedical Applications. Curr. Med. Chem. 2010, 17, 3120–3141. [Google Scholar] [CrossRef]
- Markides, H.; McLaren, J.S.; El Haj, A.J. Overcoming translational challenges—The delivery of mechanical stimuli in vivo. Int. J. Biochem. Cell Biol. 2015, 69, 162–172. [Google Scholar] [CrossRef] [PubMed]
- Hughes, S.; McBain, S.; Dobson, J.; El Haj, A.J. Selective activation of mechanosensitive ion channels using magnetic parti-cles. J. R. Soc. Interface 2008, 5, 855. [Google Scholar] [CrossRef] [PubMed]
- Hughes, S.; El Haj, A.J.; Dobson, J. Magnetic micro- and nanoparticle mediated activation of mechanosensitive ion channels. Med Eng. Phys. 2005, 27, 754–762. [Google Scholar] [CrossRef]
- Rotherham, M.; Henstock, J.R.; Qutachi, O.; El Haj, A.J. Remote regulation of magnetic particle targeted Wnt signaling for bone tissue engineering. Nanomed. Nanotechnol. Biol. Med. 2018, 14, 173–184. [Google Scholar] [CrossRef] [PubMed]
- McLaren, J.S.; White, L.J.; Cox, H.C.; Ashraf, W.; Rahman, C.V.; Blunn, G.W.; Goodship, A.E.; Quirk, R.A.; Shakesheff, K.; Bayston, R.; et al. A biodegradable antibiotic-impregnated scaffold to prevent osteomyelitis in a contaminated in vivo bone defect model. Eur. Cells Mater. 2014, 27, 332–349. [Google Scholar] [CrossRef] [PubMed]
- Hollinger, J.O.; Kleinschmidt, J.C. The Critical Size Defect as an Experimental Model to Test Bone Repair Materials. J. Craniofacial Surg. 1990, 1, 60–68. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.; Wu, G.; Gu, Z.; Wismeijer, D.; Liu, Y. A critical-sized bone defect. Bone 2014, 68, 163–164. [Google Scholar] [CrossRef] [PubMed]
- Mountziaris, P.M.; Mikos, A.G. Modulation of the Inflammatory Response for Enhanced Bone Tissue Regeneration. Tissue Eng. Part B Rev. 2008, 14, 179–186. [Google Scholar] [CrossRef]
- Schell, H.; Epari, D.; Kassi, J.P.; Bragulla, H.; Bail, H.J.; Duda, G.N. The course of bone healing is influenced by the initial shear fixation stability. J. Orthop. Res. 2005, 23, 1022–1028. [Google Scholar] [CrossRef]
- Ma, J.; Both, S.K.; Yang, F.; Cui, F.-Z.; Pan, J.; Meijer, G.J.; Jansen, J.A.; Beucken, J.J.V.D. Concise Review: Cell-Based Strategies in Bone Tissue Engineering and Regenerative Medicine. Stem Cells Transl. Med. 2014, 3, 98–107. [Google Scholar] [CrossRef]
- Lucarelli, E.; Fini, M.; Beccheroni, A.; Giavaresi, G.; Di Bella, C.; Aldini, N.N.; Guzzardella, G.; Martini, L.; Cenacchi, A.; Di Maggio, N.; et al. Stromal Stem Cells and Platelet-Rich Plasma Improve Bone Allograft Integration. Clin. Orthop. Relat. Res. 2005, 435, 62–68. [Google Scholar] [CrossRef] [PubMed]
- Field, J.R.; McGee, M.; Stanley, R.; Ruthenbeck, G.; Papadimitrakis, T.; Zannettino, A.; Gronthos, S.; Itescu, S. The efficacy of allogeneic mesenchymal precursor cells for the repair of an ovine tibial segmental defect. Vet. Comp. Orthop. Traumatol. 2011, 24, 113–121. [Google Scholar] [CrossRef] [PubMed]
- Niemeyer, P.; Fechner, K.; Milz, S.; Richter, W.; Suedkamp, N.P.; Mehlhorn, A.T.; Pearce, S.; Kasten, P. Comparison of mes-enchymal stem cells from bone marrow and adipose tissue for bone regeneration in a critical size defect of the sheep tibia and the influence of platelet-rich plasma. Biomaterials 2010, 31, 3572–3579. [Google Scholar] [CrossRef]
- Markides, H.; McLaren, J.S.; Telling, N.D.; Alom, N.; Al-Mutheffer, E.A.; Oreffo, R.O.C.; Zannettino, A.; Scammell, B.E.; White, L.J.; El Haj, A.J. Translation of remote control regenerative technologies for bone repair. NPJ Regen. Med. 2018, 3, 9. [Google Scholar] [CrossRef] [Green Version]
- Gronthos, S.; Mccarty, R.; Mrozik, K.; Fitter, S.; Paton, S.; Menicanin, D.; Itescu, S.; Bartold, P.; Xian, C.; Zannettino, A.C. Heat Shock Protein-90 beta Is Expressed at the Surface of Multipotential Mesenchymal Precursor Cells: Generation of a Novel Monoclonal Antibody, STRO-4, With Specificity for Mesenchymal Precursor Cells from Human and Ovine Tissues. Stem Cells Dev. 2009, 18, 1253–1262. [Google Scholar] [CrossRef]
- Sawkins, M.; Bowen, W.; Dhadda, P.; Markides, H.; Sidney, L.; Taylor, A.; Rose, F.; Badylak, S.; Shakesheff, K.; White, L. Hydrogels derived from demineralized and decellularized bone extracellular matrix. Acta Biomater. 2013, 9, 7865–7873. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schell, H.; Duda, G.N.; Peters, A.; Tsitsilonis, S.; Johnson, K.A.; Schmidt-Bleek, K. The haematoma and its role in bone healing. J. Exp. Orthop. 2017, 4, 5. [Google Scholar] [CrossRef] [Green Version]
- Baht, G.S.; Vi, L.; Alman, B.A. The Role of the Immune Cells in Fracture Healing. Curr. Osteoporos. Rep. 2018, 16, 138–145. [Google Scholar] [CrossRef] [Green Version]
- Einhorn, T.A.; Gerstenfeld, L.C. Fracture healing: Mechanisms and interventions. Nat. Rev. Rheumatol. 2015, 11, 45–54. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.; Choi, E.; Cha, M.-J.; Hwang, K.-C. Cell Adhesion and Long-Term Survival of Transplanted Mesenchymal Stem Cells: A Prerequisite for Cell Therapy. Oxidative Med. Cell. Longev. 2015, 2015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, L.; Chen, X.; Wang, W.E.; Zeng, C. How to Improve the Survival of Transplanted Mesenchymal Stem Cell in Ischemic Heart? Stem Cells Int. 2016, 2016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lukomska, B.; Stanaszek, L.; Zuba-Surma, E.; Legosz, P.; Sarzynska, S.; Drela, K. Challenges and Controversies in Human Mesenchymal Stem Cell Therapy. Stem Cells Int. 2019, 2019. [Google Scholar] [CrossRef] [Green Version]
- Amer, M.; Rose, F.R.A.J.; Shakesheff, K.M.; Modo, M.; White, L.J. Translational considerations in injectable cell-based therapeutics for neurological applications: Concepts, progress and challenges. NPJ Regen. Med. 2017, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdelwahid, E.; Kalvelyte, A.; Stulpinas, A.; de Carvalho, K.A.T.; Guarita-Souza, L.C.; Foldes, G. Stem cell death and survival in heart regeneration and repair. Apoptosis 2016, 21, 252–268. [Google Scholar] [CrossRef] [Green Version]
- Paluch, E.K.; Nelson, C.M.; Biais, N.; Fabry, B.; Moeller, J.; Pruitt, B.L.; Wollnik, C.; Kudryasheva, G.; Rehfeldt, F.; Federle, W. Mechanotransduction: Use the force(s). BMC Biol. 2015, 13, 1–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Selden, C.; Fuller, B. Role of Bioreactor Technology in Tissue Engineering for Clinical Use and Therapeutic Target Design. Bioengineering 2018, 5, 32. [Google Scholar] [CrossRef] [Green Version]
- Cartmell, S.H.; Dobson, J.; Verschueren, S.; Hughes, S.; El Haj, A.J. Mechanical conditioning of bone cells in vitro using magnetic micro particle technology. Eur. Cells Mater. 2002, 4, 130–131. [Google Scholar]
- Hu, B.; El Haj, A.J.; Dobson, J. Receptor-Targeted, Magneto-Mechanical Stimulation of Osteogenic Differentiation of Human Bone Marrow-Derived Mesenchymal Stem Cells. Int. J. Mol. Sci. 2013, 14, 19276–19293. [Google Scholar] [CrossRef]
- Henstock, J.R.; Rotherham, M.; Rashidi, H.; Shakesheff, K.; El Haj, A.J. Remotely Activated Mechanotransduction via Magnetic Nanoparticles Promotes Mineralization Synergistically With Bone Morphogenetic Protein 2: Applications for Injectable Cell Therapy. STEM CELLS Transl. Med. 2014, 3, 1363–1374. [Google Scholar] [CrossRef]
- Kanczler, J.M.; Sura, H.S.; Magnay, J.; Green, D.; Oreffo, R.O.; Dobson, J.P.; El Haj, A.J. Controlled Differentiation of Human Bone Marrow Stromal Cells Using Magnetic Nanoparticle Technology. Tissue Eng. Part A 2010, 16, 3241–3250. [Google Scholar] [CrossRef] [PubMed]
- Rotherham, M.; El Haj, A.J. Remote Activation of the Wnt/β-Catenin Signalling Pathway Using Functionalised Magnetic Particles. PLoS ONE 2015, 10, e0121761. [Google Scholar] [CrossRef] [Green Version]
- Henstock, J.; Rotherham, M.; Rose, J.; El Haj, A. Cyclic hydrostatic pressure stimulates enhanced bone development in the foetal chick femur in vitro. Bone 2013, 53, 468–477. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Cells | MNPs | Magnet | CM-Dil Stain | Number of Defects | Time Point |
|---|---|---|---|---|---|---|
| 1 (MNPs + magnet) | + | + | + | Yes | 6 | 2 days |
| 2 (Cell only) | + | − | − | Yes | 6 | 2 days |
| 3 (MNPs − magnet) | + | + | − | Yes | 6 | 2 days |
| 4 (MNPs + magnet) | + | + | + | Yes | 6 | 7 days |
| 5 (Cell only) | + | − | − | Yes | 6 | 7 days |
| 6 (MNPs − magnet) | + | + | − | Yes | 6 | 7 days |
| Primary Antibody | Product Code | Secondary Antibody |
|---|---|---|
| Anti-Stro-4 (20 µg/mL) | Gift from Professor Andrew Zannettino | Invitrogen, A21236 (10 µg/mL) |
| Anti-CD45 (10 µg/mL) | WS0544B-100 (Kingfisher Biotech) | Invitrogen, A21236 (10 µg/mL) |
| Anti-dextran (1 µg/mL) | 60026 (Stemcell Technologies) | Invitrogen, A21236 (10 µg/mL) |
| Anti-osteocalcin | ab13420 (Abcam) | Invitrogen, A21236 (10 µg/mL) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Markides, H.; Foster, N.C.; McLaren, J.S.; Hopkins, T.; Black, C.; Oreffo, R.O.C.; Scammell, B.E.; Echevarria, I.; White, L.J.; El Haj, A.J. Short-Term Evaluation of Cellular Fate in an Ovine Bone Formation Model. Cells 2021, 10, 1776. https://doi.org/10.3390/cells10071776
Markides H, Foster NC, McLaren JS, Hopkins T, Black C, Oreffo ROC, Scammell BE, Echevarria I, White LJ, El Haj AJ. Short-Term Evaluation of Cellular Fate in an Ovine Bone Formation Model. Cells. 2021; 10(7):1776. https://doi.org/10.3390/cells10071776
Chicago/Turabian StyleMarkides, Hareklea, Nicola C. Foster, Jane S. McLaren, Timothy Hopkins, Cameron Black, Richard O. C. Oreffo, Brigitte E. Scammell, Iria Echevarria, Lisa J. White, and Alicia J. El Haj. 2021. "Short-Term Evaluation of Cellular Fate in an Ovine Bone Formation Model" Cells 10, no. 7: 1776. https://doi.org/10.3390/cells10071776
APA StyleMarkides, H., Foster, N. C., McLaren, J. S., Hopkins, T., Black, C., Oreffo, R. O. C., Scammell, B. E., Echevarria, I., White, L. J., & El Haj, A. J. (2021). Short-Term Evaluation of Cellular Fate in an Ovine Bone Formation Model. Cells, 10(7), 1776. https://doi.org/10.3390/cells10071776