
Sex Hormone Receptor Signaling in Bladder Cancer: A Potential Target for Enhancing the Efficacy of Conventional Non-Surgical Therapy



Abstract
1. Introduction
2. Sex Hormone Receptor Signaling and Bladder Cancer Progression
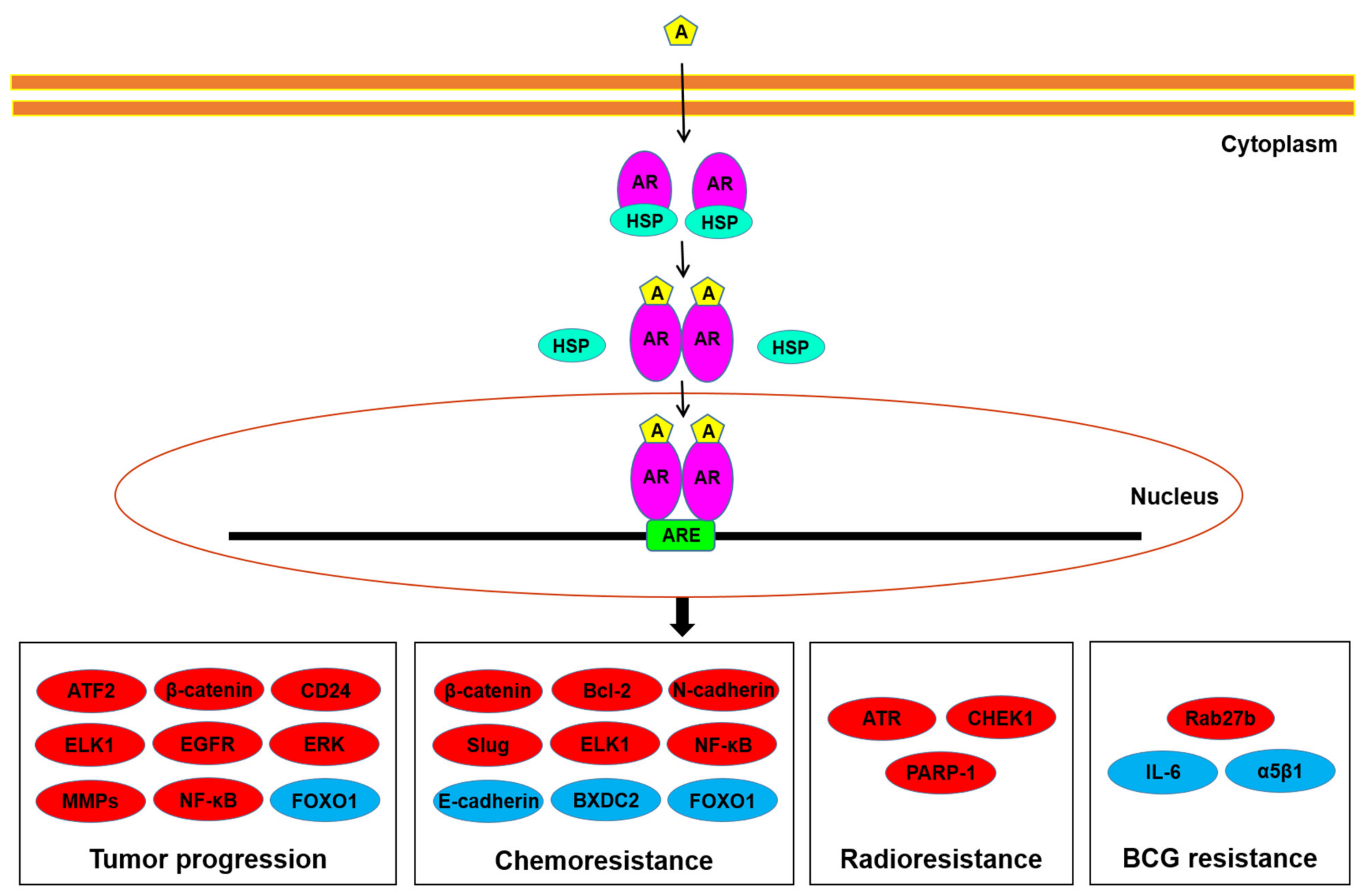
2.1. AR
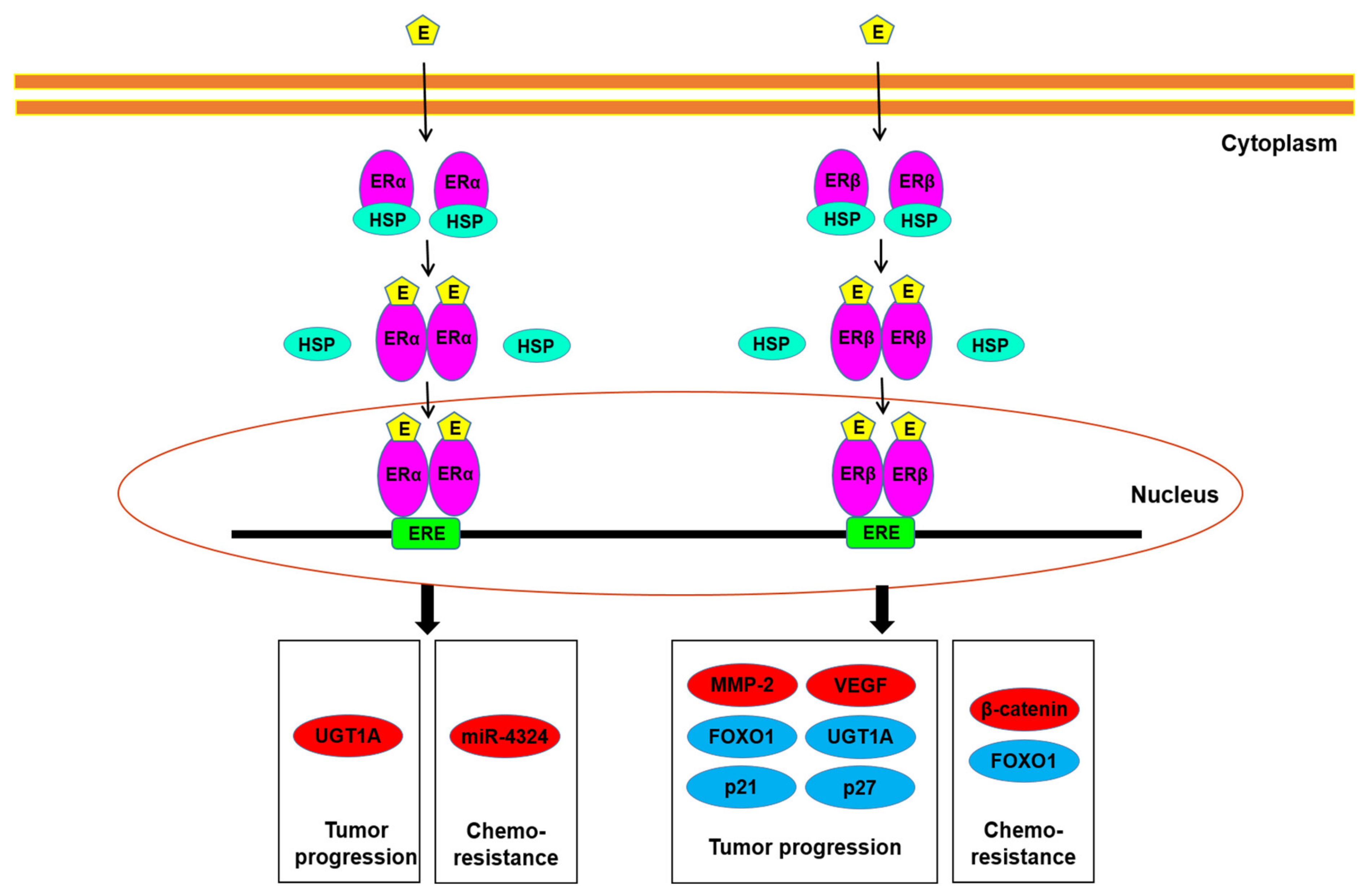
2.2. ERs
3. Sex Hormone Receptor Signaling and Sensitivity to Conventional Non-Surgical Treatment for Bladder Cancer
3.1. Chemotherapy
3.2. Radiotherapy
3.3. Immunotherapy
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef]
- Torre, L.A.; Bray, F.; Siegel, R.L.; Ferlay, J.; Lortet-Tieulent, J.; Jemal, A. Global cancer statistics, 2012. CA Cancer J. Clin. 2015, 65, 87–108. [Google Scholar] [CrossRef]
- Chou, R.; Selph, S.; Buckley, D.I.; Fu, R.; Griffin, J.C.; Grusing, S.; Gore, J.L. Intravesical therapy for the treatment of nonmuscle invasive bladder cancer: A systematic review and meta-analysis. J. Urol. 2017, 197, 1189–1199. [Google Scholar] [CrossRef]
- Ploussard, G.; Daneshmand, S.; Efstathiou, J.A.; Herr, H.W.; James, N.D.; Rodel, C.M.; Shariat, S.F.; Shipley, W.U.; Sternberg, C.N.; Thalmann, G.N.; et al. Critical analysis of bladder sparing with trimodal therapy in muscle-invasive bladder cancer: A systematic review. Eur. Urol. 2014, 66, 120–137. [Google Scholar] [CrossRef]
- Lobo, N.; Mount, C.; Omar, K.; Nair, R.; Thurairaja, R.; Khan, M.S. Landmarks in the treatment of muscle-invasive bladder cancer. Nat. Rev. Urol. 2017, 14, 565–574. [Google Scholar] [CrossRef] [PubMed]
- Lenis, A.T.; Lec, P.M.; Chamie, K.; Mshs, M.D. Bladder cancer: A review. JAMA 2020, 324, 1980–1991. [Google Scholar] [CrossRef] [PubMed]
- Patel, V.G.; Oh, W.K.; Galsky, M.D. Treatment of muscle-invasive and advanced bladder cancer in 2020. CA Cancer J. Clin. 2020, 70, 404–423. [Google Scholar] [CrossRef]
- Ide, H.; Miyamoto, H. The role of steroid hormone receptors in urothelial tumorigenesis. Cancers 2020, 12, 2155. [Google Scholar] [CrossRef] [PubMed]
- Miyamoto, H.; Yang, Z.; Chen, Y.T.; Ishiguro, H.; Uemura, H.; Kubota, Y.; Nagashima, Y.; Chang, Y.J.; Hu, Y.C.; Tsai, M.Y.; et al. Promotion of bladder cancer development and progression by androgen receptor signals. J. Natl. Cancer Inst. 2007, 99, 558–568. [Google Scholar] [CrossRef] [PubMed]
- Izumi, K.; Zheng, Y.; Hsu, J.W.; Chang, C.; Miyamoto, H. Androgen receptor signals regulate UDP-glucuronosyltransferases in the urinary bladder. Mol. Carcinog. 2013, 52, 94–102. [Google Scholar] [CrossRef]
- Nagata, Y.; Miyamoto, H. The prognostic role of steroid hormone receptor signaling pathways in urothelial carcinoma. Transl. Cancer Res. 2020, 9, 6596–6608. [Google Scholar] [CrossRef]
- Johnson, A.M.; O’Connell, M.J.; Messing, E.M.; Reeder, J.E. Decreased bladder cancer growth in parous mice. Urology 2008, 72, 470–473. [Google Scholar] [CrossRef] [PubMed]
- Wolpert, B.J.; Amr, S.; Ezzat, S.; Saleh, D.; Gouda, I.; Loay, I.; Hifnawy, T.; Mikhail, N.N.; Abdel-Hamid, M.; Zhan, M.; et al. Estrogen exposure and bladder cancer risk in Egyptian women. Maruritas 2010, 67, 353–357. [Google Scholar] [CrossRef]
- Boorjian, S.; Ugras, S.; Mongan, N.P.; Gudas, L.J.; You, X.; Tickoo, S.K.; Scherr, D.S. Androgen receptor expression is inversely correlated with pathologic tumor stage in bladder cancer. Urology 2004, 64, 383–388. [Google Scholar] [CrossRef] [PubMed]
- Boorjian, S.A.; Heemers, H.V.; Frank, I.; Farmer, S.A.; Schmidt, L.J.; Sebo, T.J.; Tindall, D.J. Expression and significance of androgen receptor coactivators in urothelial carcinoma of the bladder. Endocr. Relat. Cancer 2009, 16, 123–137. [Google Scholar] [CrossRef] [PubMed]
- Mir, C.; Shariat, S.F.; van der Kwast, T.H.; Ashfaq, R.; Lotan, Y.; Evans, A.; Skeldon, S.; Hanna, S.; Vajpeyi, R.; Kuk, C.; et al. Loss of androgen receptor expression is not associated with pathological stage, grade, gender or outcome in bladder cancer: A large multi-institutional study. BJU Int. 2011, 108, 24–30. [Google Scholar] [CrossRef] [PubMed]
- Tuygun, C.; Kankaya, D.; Imamoglu, A.; Sertcelik, A.; Zengin, K.; Oktay, M.; Sertcelik, N. Sex-specific hormone receptors in urothelial carcinomas of the human urinary bladder: A comparative analysis of clinicopathological features and survival outcomes according to receptor expression. Urol. Oncol. 2011, 29, 43–51. [Google Scholar] [CrossRef]
- Miyamoto, H.; Yao, J.L.; Chaux, A.; Zheng, Y.; Hsu, I.; Izumi, K.; Chang, C.; Messing, E.M.; Netto, G.J.; Yeh, S. Expression of androgen and oestrogen receptors and its prognostic significance in urothelial neoplasm of the urinary bladder. BJU Int. 2012, 109, 1716–1726. [Google Scholar] [CrossRef]
- Jing, Y.; Cui, D.; Guo, W.; Jiang, J.; Jiang, B.; Lu, Y.; Zhao, W.; Wang, X.; Jiang, Q.; Han, B.; et al. Activated androgen receptor promotes bladder cancer metastasis via Slug mediated epithelial-mesenchymal transition. Cancer Lett. 2014, 348, 135–145. [Google Scholar] [CrossRef]
- Nam, J.K.; Park, S.W.; Lee, S.D.; Chung, M.K. Prognostic value of sex-hormone receptor expression in non-muscle-invasive bladder cancer. Yonsei Med. J. 2014, 55, 1214–1221. [Google Scholar] [CrossRef]
- Elzamy, S.; Ms, A.A.; Kandeel, W. The prognostic significance of androgen receptor and β-catenin immunohistochemical expression in urothelial carcinoma with and without detrusor muscle invasion from an Egyptian institution. Pol. J. Pathol. 2018, 69, 234–242. [Google Scholar] [CrossRef] [PubMed]
- Tyagi, A.; Chandrasekaran, B.; Kolluru, V.; Rai, S.; Jordan, A.C.; Houda, A.; Messer, J.; Ankem, M.; Damodaran, C.; Haddad, A. Combination of androgen receptor inhibitor and cisplatin, an effective treatment strategy for urothelial carcinoma of the bladder. Urol. Oncol. 2019, 37, 492–502. [Google Scholar] [CrossRef]
- Yonekura, S.; Terauchi, F.; Hoshi, K.; Yamaguchi, T.; Kawai, S. Androgen receptor predicts first and multiple recurrences in non-muscle invasive urothelial carcinoma of the bladder. Pathol. Oncol. Res. 2019, 25, 987–994. [Google Scholar] [CrossRef] [PubMed]
- Toren, P.; Brisson, H.; Simonyan, D.; Hovington, H.; Lacombe, L.; Bergeron, A.; Fradet, Y. Androgen receptor and immune cell PD-L1 expression in bladder tumors predicts disease recurrence and survival. World J. Urol. 2020. [Google Scholar] [CrossRef]
- Ide, H.; Inoue, S.; Miyamoto, H. Histopathological and prognostic significance of the expression of sex hormone receptors in bladder cancer: A meta-analysis of immunohistochemical studies. PLoS ONE 2017, 12, 0174746. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.T.; Han, B.M.; Yu, S.Q.; Wang, H.P.; Xia, S.J. Androgen receptor is a potential therapeutic target for bladder cancer. Urology 2010, 75, 820–827. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.; Izumi, K.; Yao, J.L.; Miyamoto, H. Dihydrotestosterone upregulates the expression of epidermal growth factor receptor and ERBB2 in androgen receptor-positive bladder cancer cells. Endocr. Relat. Cancer 2011, 18, 451–464. [Google Scholar] [CrossRef]
- Izumi, K.; Zheng, Y.; Li, Y.; Zaengle, J.; Miyamoto, H. Epidermal growth factor induces bladder cancer cell proliferation through activation of the androgen receptor. Int. J. Oncol. 2012, 41, 1587–1592. [Google Scholar] [CrossRef]
- Overdevest, J.B.; Knubel, K.H.; Duex, J.E.; Thomas, S.; Nitz, M.D.; Harding, M.A.; Smith, S.C.; Frierson, H.F.; Conaway, M.; Theodorescu, D. CD24 expression is important in male urothelial tumorigenesis and metastasis in mice and is androgen regulated. Proc. Natl. Acad. Sci. USA 2012, 109, 3588–3596. [Google Scholar] [CrossRef]
- Shiota, M.; Takeuchi, A.; Yokomizo, A.; Kashiwagi, E.; Tatsugami, K.; Kuroiwa, K.; Naito, S. Androgen receptor signaling regulates cell growth and vulnerability to doxorubicin in bladder cancer. J. Urol. 2012, 188, 276–286. [Google Scholar] [CrossRef]
- Kawahara, T.; Ide, H.; Kashiwagi, E.; El-Shishtawy, K.A.; Li, Y.; Reis, L.O.; Zheng, Y.; Miyamoto, H. Enzalutamide inhibits androgen receptor-positive bladder cancer cell growth. Urol. Oncol. 2016, 34, 15–23. [Google Scholar] [CrossRef] [PubMed]
- Ide, H.; Mizushima, T.; Jiang, G.; Goto, T.; Nagata, Y.; Teramoto, Y.; Inoue, S.; Li, Y.; Kashiwagi, E.; Baras, A.S.; et al. FOXO1 as a tumor suppressor inactivated via AR/ERβ signals in urothelial cells. Endocr. Relat. Cancer 2020, 27, 231–244. [Google Scholar] [CrossRef]
- Ding, G.; Yu, S.; Cheng, S.; Li, G.; Yu, Y. Androgen receptor (AR) promotes male bladder cancer cell proliferation and migration via regulating CD24 and VEGF. Am. J. Transl. Res. 2016, 8, 578–587. [Google Scholar] [PubMed]
- Johnson, A.M.; O’Connell, M.J.; Miyamoto, H.; Huang, J.; Yao, J.L.; Messing, E.M.; Reeder, J.E. Androgenic dependence of exophytic tumor growth in a transgenic mouse model of bladder cancer: A role for thrombospondin-1. BMC Urol. 2008, 8, 7. [Google Scholar] [CrossRef]
- Inoue, S.; Mizushima, T.; Ide, H.; Jiang, G.; Goto, T.; Nagata, Y.; Netto, G.J.; Miyamoto, H. ATF2 promotes urothelial cancer outgrowth via cooperation with androgen receptor signaling. Endocr. Connect. 2018, 7, 1397–1408. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Zheng, Y.; Izumi, K.; Ishiguro, H.; Ye, B.; Li, F.; Miyamoto, H. Androgen activates β-catenin signaling in bladder cancer cells. Endocr. Relat. Cancer 2013, 20, 293–304. [Google Scholar] [CrossRef]
- Kawahara, T.; Shareef, H.K.; Aljarah, A.K.; Ide, H.; Li, Y.; Kashiwagi, E.; Netto, G.J.; Zheng, Y.; Miyamoto, H. ELK1 is up-regulated by androgen in bladder cancer cells and promotes tumor progression. Oncotarget 2015, 30, 29860–29876. [Google Scholar] [CrossRef] [PubMed]
- Chen, F.; Langenstroer, P.; Zhang, G.; Iwamoto, Y.; See, W. Androgen dependent regulation of bacillus Calmette-Guérin induced interleukin-6 expression in human transitional carcinoma cell lines. J. Urol. 2003, 170, 2009–2013. [Google Scholar] [CrossRef]
- Inoue, S.; Ide, H.; Mizushima, T.; Jiang, G.; Netto, G.J.; Gotoh, M.; Miyamoto, H. Nuclear factor-κB promotes urothelial tumorigenesis and cancer progression via cooperation with androgen receptor signaling. Mol. Cancer Ther. 2018, 17, 1303–1314. [Google Scholar] [CrossRef] [PubMed]
- Zhu, B.T.; Han, G.Z.; Shim, J.Y.; Wen, Y.; Jiang, X.R. Quantitative structure-activity relationship of various endogenous estrogen metabolites for human estrogen receptor α and β subtypes: Insights into the structural determinants favoring a differential subtype binding. Endocrinology 2006, 147, 4132–4150. [Google Scholar] [CrossRef] [PubMed]
- Imai, Y.; Noda, S.; Matsuyama, C.; Shimizu, A.; Kamai, T. Sex steroid hormone receptors in bladder cancer: Usefulness in differential diagnosis and implications in histogenesis of bladder cancer. Urol. Oncol. 2019, 37, 353. [Google Scholar] [CrossRef]
- Bernardo, C.; Santos, J.; Costa, C.; Tavares, A.; Amaro, T.; Marques, I.; Gouveia, M.J.; Felix, V.; Afreixo, V.; Brindley, P.J.; et al. Estrogen receptors in urogenital schistosomiasis and bladder cancer: Estrogen receptor alpha-mediated cell proliferation. In Urologic Oncology: Seminars and Original Investigations; Elesvier: Amsterdam, The Netherlands, 2020; Volume 38, pp. 738.e23–738.e35. [Google Scholar] [CrossRef] [PubMed]
- Croft, P.R.; Lathrop, S.L.; Feddersen, R.M.; Joste, N.E. Estrogen receptor expression in papillary urothelial carcinoma of the bladder and ovarian transitional cell carcinoma. Arch. Pathol. Lab. Med. 2005, 129, 194–199. [Google Scholar] [CrossRef]
- Shen, S.S.; Smith, C.L.; Hsieh, J.T.; Yu, J.; Kim, I.Y.; Jian, W.; Sonpavde, G.; Ayala, G.E.; Younes, M.; Lerner, S.P. Expression of estrogen receptors-α and -β in bladder cancer cell lines and human bladder tumor tissue. Cancer 2006, 106, 2610–2616. [Google Scholar] [CrossRef] [PubMed]
- Kontos, S.; Kominea, A.; Melachrinou, M.; Balampani, E.; Sotiropoulou-Bonikou, G. Inverse expression of estrogen receptor-β and nuclear factor-κB in urinary bladder carcinogenesis. Int. J. Urol. 2010, 17, 801–809. [Google Scholar] [CrossRef]
- Tan, W.; Boorjian, S.; Advani, P.; Farmer, S.; Lohse, C.; Cheville, J.; Kwon, E.; Leibovich, B. The Estrogen Pathway: Estrogen receptor-α, progesterone receptor, and estrogen receptor-β expression in radical cystectomy urothelial cell carcinoma specimens. Clin. Genitourin. Cancer 2015, 13, 476–484. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, D.P.; O’Malley, P.; Al Hussein Al Awamlh, B.; Furrer, M.A.; Mongan, N.P.; Robinson, B.D.; Wang, G.J.; Scherr, D.S. Association of aromatase with bladder cancer stage and long-term survival: New insights into the hormonal paradigm in bladder cancer. Clin. Genitourin. Cancer 2017, 15, 256–262. [Google Scholar] [CrossRef][Green Version]
- Andersson, S.; Sundberg, M.; Pristovsek, N.; Ibrahim, A.; Jonsson, P.; Katona, B.; Clausson, C.M.; Zieba, A.; Ramstrom, M.; Soderberg, O.; et al. Insufficient antibody validation challenges oestrogen receptor beta research. Nat. Commun. 2017, 8, 15840. [Google Scholar] [CrossRef] [PubMed]
- Nelson, A.W.; Groen, A.J.; Miller, J.L.; Warren, A.Y.; Holmes, K.A.; Tarulli, G.A.; Tilley, W.D.; Katzenellenbogen, B.S.; Hawse, J.R.; Gnanapragasam, V.J.; et al. Comprehensive assessment of estrogen receptor beta antibodies in cancer cell line models and tissue reveals critical limitations in reagent specificity. Mol. Cell. Endocrinol. 2017, 440, 138–150. [Google Scholar] [CrossRef]
- Teng, J.; Wang, Z.Y.; Jarrard, D.F.; Bjorling, D.E. Roles of estrogen receptor α and β in modulating urothelial cell proliferation. Endocr. Relat. Cancer 2008, 15, 351–364. [Google Scholar] [CrossRef]
- Hoffman, K.L.; Lerner, S.P.; Smith, C.L. Raloxifene inhibits growth of RT4 urothelial carcinoma cells via estrogen receptor-dependent induction of apoptosis and inhibition of proliferation. Horm. Cancer 2013, 4, 24–35. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.T.; Kim, B.C.; Kim, I.Y.; Mamura, M.; Seong, D.H.; Jang, J.J.; Kim, S.J. Raloxifene, a mixed estrogen agonist/antagonist, induces apoptosis through cleavage of BAD in TSU-PR1 human cancer cells. J. Biol. Chem. 2002, 277, 32510–32515. [Google Scholar] [CrossRef] [PubMed]
- Sonpavde, G.; Okuno, N.; Weiss, H.; Yu, J.; Shen, S.S.; Younes, M.; Jian, W.; Lerner, S.P.; Smith, C.L. Efficacy of selective estrogen receptor modulators in nude mice bearing human transitional cell carcinoma. Urology 2007, 69, 1221–1226. [Google Scholar] [CrossRef]
- Hsu, I.; Chuang, K.L.; Slavin, S.; Da, J.; Lim, W.X.; Pang, S.T.; O’Brien, J.H.; Yeh, S. Suppression of ERβ signaling via ERβ knockout or antagonist protects against bladder cancer development. Carcinogenesis 2014, 35, 651–661. [Google Scholar] [CrossRef]
- Huang, C.P.; Chen, J.; Chen, C.C.; Liu, G.; Zhang, Y.; Messing, E.; Yeh, S.; Chang, C. ASC-J9® increases the bladder cancer chemotherapy efficacy via altering the androgen receptor (AR) and NF-κB survival signals. J. Exp. Clin. Cancer Res. 2019, 38, 275. [Google Scholar] [CrossRef] [PubMed]
- Hsu, I.; Yeh, C.R.; Slavin, S.; Miyamoto, H.; Netto, G.J.; Tsai, Y.C.; Muyan, M.; Wu, X.R.; Messing, E.M.; Guancial, E.A.; et al. Estrogen receptor alpha prevents bladder cancer via INPP4B inhibited akt pathway in vitro and in vivo. Oncotarget 2014, 5, 7917–7935. [Google Scholar] [CrossRef]
- Izumi, K.; Li, Y.; Ishiguro, H.; Zheng, Y.; Yao, J.L.; Netto, G.J.; Miyamoto, H. Expression of UDP-glucuronosyltransferase 1A in bladder cancer: Association with prognosis and regulation by estrogen. Mol. Carcinog. 2014, 53, 314–324. [Google Scholar] [CrossRef] [PubMed]
- Han, B.; Cui, D.; Jing, Y.; Hong, Y.; Xia, S. Estrogen receptor β (ERβ) is a novel prognostic marker of recurrence survival in non-muscle-invasive bladder cancer potentially by inhibiting cadherin switch. World J. Urol. 2012, 30, 861–867. [Google Scholar] [CrossRef]
- George, S.K.; Tovar-Sepulveda, V.; Shen, S.S.; Jian, W.; Zhang, Y.; Hilsenbeck, S.G.; Lerner, S.P.; Smith, C.L. Chemoprevention of BBN-induced bladder carcinogenesis by the selective estrogen receptor modulator tamoxifen. Transl. Oncol. 2013, 6, 244–255. [Google Scholar] [CrossRef]
- Ding, M.; Liu, Y.; Li, J.; Yao, L.; Liao, X.; Xie, H.; Yang, K.; Zhou, Q.; Liu, Y.; Huang, W.; et al. Oestrogen promotes tumorigenesis of bladder cancer by inducing the enhancer RNA-eGREB1. J. Cell. Mol. Med. 2018, 22, 5919–5927. [Google Scholar] [CrossRef]
- Ding, M.; Zhan, H.; Liao, X.; Li, A.; Zhong, Y.; Gao, Q.; Liu, Y.; Huang, W.; Cai, Z. Enhancer RNA - P2RY2e induced by estrogen promotes malignant behaviors of bladder cancer. Int. J. Biol. Sci. 2018, 14, 1268–1276. [Google Scholar] [CrossRef]
- Ou, Z.; Wang, Y.; Chen, J.; Tao, L.; Zuo, L.; Sahasrabudhe, D.; Joseph, J.; Wang, L.; Yeh, S. Estrogen receptor β promotes bladder cancer growth and invasion via alteration of miR-92a/DAB2IP signals. Exp. Mol. Med. 2018, 50, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Ge, Q.; Lu, M.; Ju, L.; Qian, K.; Wang, G.; Wu, C.L.; Liu, X.; Xiao, Y.; Wang, X. miR-4324-RACGAP1-STAT3-ESR1 feedback loop inhibits proliferation and metastasis of bladder cancer. Int. J. Cancer 2019, 144, 3043–3055. [Google Scholar] [CrossRef]
- Wu, L.; Zhang, M.; Qi, L.; Zu, X.; Li, Y.; Liu, L.; Chen, M.; Li, Y.; He, W.; Hu, X.; et al. ERα-mediated alterations in circ_0023642 and miR-490-5p signaling suppress bladder cancer invasion. Cell Death Dis. 2019, 10, 635. [Google Scholar] [CrossRef] [PubMed]
- Goto, T.; Miyamoto, H. Why has the prognosis for muscle-invasive bladder cancer not significantly improved after decades of therapeutic advancements? Expert Rev. Anticancer Ther. 2020, 20, 229–231. [Google Scholar] [CrossRef]
- Pu, Y.S.; Hsieh, T.S.; Tsai, T.C.; Cheng, A.L.; Hsieh, C.Y.; Su, I.J.; Lai, M.K. Tamoxifen enhances the chemosensitivity of bladder carcinoma cells. J. Urol. 1995, 154, 601–605. [Google Scholar] [CrossRef]
- Pu, Y.S.; Hsieh, T.S.; Cheng, A.L.; Tseng, N.F.; Su, I.J.; Hsieh, C.Y.; Lai, M.K.; Tsai, T.C. Combined cytotoxic effects of tamoxifen and chemotherapeutic agents on bladder cancer cells: A potential use in intravesical chemotherapy. Br. J. Urol. 1996, 77, 76–85. [Google Scholar] [CrossRef]
- Kawahara, T.; Ide, H.; Kashiwagi, E.; Patterson, J.D.; Inoue, S.; Shareef, H.K.; Aljarah, A.K.; Zheng, Y.; Baras, A.S.; Miyamoto, H. Silodosin inhibits the growth of bladder cancer cells and enhances the cytotoxic activity of cisplatin via ELK1 inactivation. Am. J. Cancer Res. 2015, 5, 2959–2968. [Google Scholar] [PubMed]
- Shang, Z.; Li, Y.; Zhang, M.; Tian, J.; Han, R.; Shyr, C.R.; Messing, E.; Yeh, S.; Niu, Y.; Chang, C. Antiandrogen therapy with hydroxyflutamide or androgen receptor degradation enhancer ASC-J9 enhances BCG Efficacy to better suppress bladder cancer progression. Mol. Cancer Ther. 2015, 14, 2586–2594. [Google Scholar] [CrossRef]
- Takeuchi, H.; Mmeje, C.O.; Jinesh, G.G.; Taoka, R.; Kamat, A.M. Sequential gemcitabine and tamoxifen treatment enhances apoptosis and blocks transformation in bladder cancer cells. Oncol. Rep. 2015, 34, 2738–2744. [Google Scholar] [CrossRef] [PubMed]
- Kashiwagi, E.; Ide, H.; Inoue, S.; Kawahara, T.; Zheng, Y.; Reis, L.O.; Baras, A.S.; Miyamoto, H. Androgen receptor activity modulates responses to cisplatin treatment in bladder cancer. Oncotarget 2016, 7, 49169–49179. [Google Scholar] [CrossRef] [PubMed]
- Kameyama, K.; Horie, K.; Mizutani, K.; Kato, T.; Fujita, Y.; Kawakami, K.; Kojima, T.; Miyazaki, T.; Deguchi, T.; Ito, M. Enzalutamide inhibits proliferation of gemcitabine-resistant bladder cancer cells with increased androgen receptor expression. Int. J. Oncol. 2017, 50, 75–84. [Google Scholar] [CrossRef] [PubMed]
- Ide, H.; Inoue, S.; Mizushima, T.; Jiang, G.; Chuang, K.H.; Oya, M.; Miyamoto, H. Androgen receptor signaling reduces radiosensitivity in bladder cancer. Mol. Cancer Ther. 2018, 17, 1566–1574. [Google Scholar] [CrossRef] [PubMed]
- Long, X.; Xiong, W.; Zeng, X.; Qi, L.; Cai, Y.; Mo, M.; Jiang, H.; Zhu, B.; Chen, Z.; Li, Y. Cancer-associated fibroblasts promote cisplatin resistance in bladder cancer cells by increasing IGF-1/ERβ/Bcl-2 signalling. Cell Death Dis. 2019, 10, 375. [Google Scholar] [CrossRef]
- Sekino, Y.; Sakamoto, N.; Ishikawa, A.; Honma, R.; Shigematsu, Y.; Hayashi, T.; Sentani, K.; Oue, N.; Teishima, J.; Matsubara, A.; et al. Transcribed ultraconserved region Uc.63+ promotes resistance to cisplatin through regulation of androgen receptor signaling in bladder cancer. Oncol. Rep. 2019, 41, 3111–3118. [Google Scholar] [CrossRef]
- Goto, T.; Kashiwagi, E.; Jiang, G.; Nagata, Y.; Teramoto, Y.; Baras, A.S.; Yamashita, S.; Ito, A.; Arai, Y.; Miyamoto, H. strogen receptor-β signaling induces cisplatin resistance in bladder cancer. Am. J. Cancer Res. 2020, 10, 2523–2534. [Google Scholar]
- Ide, H.; Goto, T.; Teramoto, Y.; Mizushima, T.; Jiang, G.; Nagata, Y.; Inoue, S.; Baras, A.S.; Kashiwagi, E.; Miyamoto, H. FOXO1 inactivation induces cisplatin resistance in bladder cancer. Cancer Sci. 2020, 111, 3397–3400. [Google Scholar] [CrossRef]
- Mizushima, T.; Jiang, G.; Kawahara, T.; Li, P.; Han, B.; Inoue, S.; Ide, H.; Kato, I.; Jalalizadeh, M.; Miyagi, E.; et al. Androgen receptor signaling reduces the efficacy of bacillus Calmette-Guérin therapy for bladder cancer via modulating Rab27b-induced exocytosis. Mol. Cancer Ther. 2020, 19, 1930–1942. [Google Scholar] [CrossRef]
- Jiang, G.; Teramoto, Y.; Goto, T.; Mizushima, T.; Inoue, S.; Ide, H.; Nagata, Y.; Kashiwagi, E.; Baras, A.S.; Netto, G.J.; et al. Identification of BXDC2 as a key downstream effector of the androgen receptor in modulating cisplatin sensitivity in bladder cancer. Cancers 2021, 13, 975. [Google Scholar] [CrossRef]
- Lee, K.H.; Kim, B.C.; Jeong, S.H.; Jeong, C.W.; Ku, J.H.; Kim, H.H.; Kwak, C. Histone demethylase KDM7A regulates androgen receptor activity, and its chemical inhibitor TC-E 5002 overcomes cisplatin-resistance in bladder cancer cells. Int. J. Mol. Sci. 2020, 21, 5658. [Google Scholar] [CrossRef]
- Hsu, C.H.; Chen, J.; Wu, C.Y.; Cheng, A.L.; Pu, Y.S. Combination chemotherapy of cisplatin, methotrexate, vinblastine, and high-dose tamoxifen for transitional cell carcinoma. Anticancer Res. 2001, 21, 711–715. [Google Scholar] [PubMed]
- Wettstein, M.S.; Rooprai, J.K.; Pazhepurackel, C.; Wallis, C.J.D.; Klaassen, Z.; Uleryk, E.M.; Hermanns, T.; Fleshner, N.E.; Zlotta, A.R.; Kulkarni, G.S. Systematic review and meta-analysis on trimodal therapy versus radical cystectomy for muscle-invasive bladder cancer: Does the current quality of evidence justify definitive conclusions? PLoS ONE 2019, 14, 0216255. [Google Scholar] [CrossRef]
- Boorjian, S.A.; Zhu, F.; Herr, H.W. The effect of gender on response to bacillus Calmette-Guérin therapy for patients with non-muscle-invasive urothelial carcinoma of the bladder. BJU Int. 2010, 106, 357–361. [Google Scholar] [CrossRef]
- Uhlig, A.; Strauss, A.; Seif Amir Hosseini, A.; Lotz, J.; Trojan, L.; Schmid, M.; Uhlig, J. Gender-specific differences in recurrence of non-muscle-invasive bladder cancer: A systematic review and meta-analysis. Eur. Urol. Focus 2018, 4, 924–936. [Google Scholar] [CrossRef]
- Shang, Z.; Li, Y.; Hsu, I.; Zhang, M.; Tian, J.; Wen, S.; Han, R.; Messing, E.M.; Chang, C.; Niu, Y.; et al. Targeting estrogen/estrogen receptor alpha enhances bacillus Calmette-Guérin efficacy in bladder cancer. Oncotarget 2016, 7, 27325–27335. [Google Scholar] [CrossRef]
- Sun, L.; Zhang, L.; Yu, J.; Zhang, Y.; Pang, X.; Ma, C.; Shen, M.; Ruan, S.; Wasan, H.S.; Qiu, S. Clinical efficacy and safety of anti-PD-1/PD-L1 inhibitors for the treatment of advanced or metastatic cancer: A systematic review and meta-analysis. Sci. Rep. 2020, 10, 2083. [Google Scholar] [CrossRef]
- Necchi, A.; Lo Vullo, S.; Giannatempo, P.; Raggi, D.; Perrone, F.; Nicolai, N.; Catanzaro, M.; Biasoni, D.; Torelli, T.; Piva, L.; et al. Association of androgen receptor expression on tumor cells and PD-L1 expression in muscle-invasive and metastatic urothelial carcinoma: Insights for clinical research. Clin. Genitourin. Cancer 2018, 16, 403–410. [Google Scholar] [CrossRef] [PubMed]
- Zerdes, I.; Sifakis, E.G.; Matikas, A.; Chretien, S.; Tobin, N.P.; Hartman, J.; Rassidakis, G.Z.; Bergh, J.; Foukakis, T. Programmed death-ligand 1 gene expression is a prognostic marker in early breast cancer and provides additional prognostic value to 21-gene and 70-gene signatures in estrogen receptor-positive disease. Mol. Oncol. 2020, 14, 951–963. [Google Scholar] [CrossRef] [PubMed]
- Katleba, K.; Lombard, A.P.; Tsamouri, M.M.; Baek, H.B.; Nishida, K.S.; Libertini, S.J.; Platero, A.J.; Ma, A.H.; Pan, C.X.; Ghosh, P.M.; et al. Depletion of androgen receptor low molecular weight isoform reduces bladder tumor cell viability and induces apoptosis. Cancer Lett. 2021, 504, 49–57. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Author, Year [Ref] | Tumor Grade | Tumor Stage | Prognostic Significance | ||||
|---|---|---|---|---|---|---|---|
| Low-Grade | High-Grade | pa | NMI | MI | pa | ||
| Boorjian, 2004 [14] | 8/9 (89%) | 16/33 (48%) | 0.055 | 21/28 (75%) | 3/14 (21%) | 0.002 | NA |
| Boorjian, 2009 [15] | NA | NA | NA | 13/22 (59%) | 11/33 (33%) | 0.095 | NA |
| Mir, 2011 [16] | 11/90 (12%) | 50/382 (13%) | 0.864 | 11/126 (9%) | 46/305 (15%) | 0.086 | NS |
| Tuygun, 2011 [17] | 46/72 (64%) | 25/67 (37%) | 0.002 | 64/106 (60%) | 7/33 (21%) | <0.001 | p = 0.095 (RFS/NMI) |
| Miyamoto, 2012 [18] | 31/56 (55%) b | 48/132 (36%) | 0.023 | 49/97 (51%) | 30/91 (33%) | 0.018 | p = 0.0705 (PFS/MI) |
| Jing, 2014 [19] | 22/40 (55%) | 9/18 (50%) | 0.781 | 22/45 (49%) | 9/13 (69%) | 0.225 | NA |
| Nam, 2014 [20] | 47/120 (39%) b | 16/49 (33%) | 0.485 | NA | NA | NA | p = 0.001 (RFS) |
| Elzamy, 2018 [21] | 7/48 (15%) b | 30/58 (52%) | <0.001 | 5/27 (19%) | 32/79 (41%) | 0.060 | NS |
| Tyagi, 2019 [22] | NA | NA | NA | 17/38 (45%) | 22/34 (65%) | 0.103 | NA |
| Yonekura, 2019 [23] | 11/26 (42%) | 9/14 (64%) | 0.320 | NA | NA | NA | p < 0.05 (RFS&PFS/NMI) |
| Toren, 2020 [24] | 76/121 (63%) c | 79/194 (41%) c | <0.001 | 95/150 (63%) | 61/167 (37%) | <0.001 | p = 0.03 (RFS/RC) |
| Author, Year [Ref] | Tumor Grade | Tumor Stage | Prognostic Significance | ||||
|---|---|---|---|---|---|---|---|
| Low-Grade | High-Grade | pa | NMI | MI | pa | ||
| Miyamoto, 2012 [18] | 21/56 (38%) b | 30/132 (23%) | 0.048 | 34/97 (35%) | 17/91 (19%) | 0.014 | NS |
| Imai, 2019 [41] | 20/63 (32%) c | 28/62 (45%) c | 0.143 | 26/81 (32%) | 22/44 (50%) | 0.056 | NA |
| Bernardo, 2020 [42] | 2/12 (17%) | 12/68 (18%) | 1.000 | 7/40 (18%) | 7/40 (18%) | 1.000 | NS |
| Author, Year [Ref] | Tumor Grade | Tumor Stage | Prognostic Significance | ||||
|---|---|---|---|---|---|---|---|
| Low-Grade | High-Grade | pa | NMI | MI | pa | ||
| Croft, 2005 [43] | 6/50 (12%) b | 14/42 (33%) b | 0.021 | NA | NA | NA | NA |
| Shen, 2006 [44] | 66/114 (58%) b | 67/96 (70%) b | 0.085 | 78/145 (54%) | 47/59 (80%) | <0.001 | NA |
| Kontos, 2010 [45] | 54/57 (95%) b | 30/54 (56%) b | <0.001 | 25/30 (83%) | 22/41 (54%) | 0.011 | NA |
| Tuygun, 2011 [17] | 16/72 (22%) | 21/67 (31%) | 0.253 | 28/106 (26%) | 12/33 (36%) | 0.279 | p = 0.035 (PFS/NMI) |
| Miyamoto, 2012 [18] | 16/56 (29%) c | 77/132 (58%) | <0.001 | 39/97 (34%) | 60/91 (66%) | <0.001 | p < 0.01 (PFS/NMI); p < 0.01 (PFS&CSS/MI) |
| Nam, 2014 [20] | 32/120 (27%) c | 20/49 (41%) | 0.098 | NA | NA | NA | p < 0.05 (RFS&PFS) |
| Tan, 2015 [46] | 28/28 (100%) d | 262/262 (100%) d | 1.000 | 95/95 (100%) | 216/216 (100%) | 1.000 | p = 0.055–0.087 (CSS) |
| Nguyen, 2017 [47] | 2/6 (33%) | 16/24 (67%) | 0.184 | 3/11 (27%) | 15/19 (79%) | 0.009 | NS |
| Bernardo, 2020 [42] | 11/12 (92%) | 62/68 (91%) | 1.000 | 36/40 (90%) | 37/40 (93%) | 1.000 | NA |
| Author, Year [Ref] | Conventional Therapy | Receptor | Design/Model | Main Findings | Molecules/Pathways Involved |
|---|---|---|---|---|---|
| Pu, 1995 [66] | CT (CIS, DOX, MTX, VBL) | ER | T24/NTUB1/BFTCC905 cell viability | TAM ↑growth inhibition | NA |
| Pu, 1996 [67] | CT (DOX, MMC, TTP) | ER | TSGH8301/HTB9 cell viability | TAM ↑growth inhibition | NA |
| Shiota, 2012 [30] | CT (DOX) | AR | UMUC3 cell viability | DHT ↓sensitivity AR-siRNA ↑sensitivity | NA |
| Kawahara, 2015 [37] Kawahara, 2015 [68] | CT (CIS) | AR | UMUC3 cell viability | DHT ↑ELK1 ELK1-inactivation ↑sensitivity | ELK1 |
| Shang, 2015 [69] | BCG | AR | 253J/T24 cell viability BBN-induced tumor in mice | ASC-J9/HF ↑growth inhibition | integrin α5β1 |
| Takeuchi, 2015 [70] | CT (GEM) | ER | 5637/RT4/TCCSUP cell viability | TAM ↑growth inhibition | NA |
| Kashiwagi, 2016 [71] | CT (CIS) | AR | 5637/647V/UMUC3 cell viability | AR-overexpression ↓sensitivity AR-knockdown/HF ↑sensitivity | NF-κB |
| Kameyama, 2017 [72] | CT (GEM) | AR | T24 cell viability | ENZ ↑sensitivity | cyclin D1 |
| Ide, 2018 [73] | RT | AR | 5637/647V/UMUC3 cell viability | AR overexpression/DHT ↓sensitivity AR-knockdown/HF ↑sensitivity | ATR, CHEK1, PARP1 |
| Huang, 2019 [55] | CT (CIS, DOX, MMC) | AR | J82/TCCSUP cell viability J82 mouse xenograft | ASC-J9 ↑sensitivity | BAX, BCL2, p21 |
| Long, 2019 [74] | CT (CIS) | ERβ | 5637/T24 cell viability | Co-culture of CAF ↑ERβ expression ↓sensitivity | IGF1 |
| Sekino, 2019 [75] | CT (CIS) | AR | RT112/UMUC3 cell viability | AR-overexpression ↓sensitivity | Uc.63+ |
| Tyagi, 2019 [22] | CT (CIS) | AR | TCCSUP cell viability/migration/invasion | ENZ ↑sensitivity | EMT |
| Goto, 2020 [76] | CT (CIS) | ERβ | 5637/647V/UMUC3 cell viability | ERβ-knockdown/TAM ↑sensitivity | β-catenin |
| Ide, 2020 [32] Ide, 2020 [77] | CT (CIS) | AR/ERβ | 5637/647V/UMUC3 cell viability | AR/ERβ inactivate FOXO1 FOXO1-inactivation ↓sensitivity | FOXO1 |
| Mizushima, 2020 [78] | BCG | AR | 5637/MB49/UMUC3 cell viability | AR-overexpression/R1881 ↓sensitivity AR-knockdown ↑sensitivity | Rab27b |
| Jiang, 2021 [79] | CT (CIS) | AR | 5637/UMUC3 cell viability | AR-overexpression/DHT ↓BXDC2 BXDC2-knockdown ↓sensitivity | BXDC2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ide, H.; Miyamoto, H. Sex Hormone Receptor Signaling in Bladder Cancer: A Potential Target for Enhancing the Efficacy of Conventional Non-Surgical Therapy. Cells 2021, 10, 1169. https://doi.org/10.3390/cells10051169
Ide H, Miyamoto H. Sex Hormone Receptor Signaling in Bladder Cancer: A Potential Target for Enhancing the Efficacy of Conventional Non-Surgical Therapy. Cells. 2021; 10(5):1169. https://doi.org/10.3390/cells10051169
Chicago/Turabian StyleIde, Hiroki, and Hiroshi Miyamoto. 2021. "Sex Hormone Receptor Signaling in Bladder Cancer: A Potential Target for Enhancing the Efficacy of Conventional Non-Surgical Therapy" Cells 10, no. 5: 1169. https://doi.org/10.3390/cells10051169
APA StyleIde, H., & Miyamoto, H. (2021). Sex Hormone Receptor Signaling in Bladder Cancer: A Potential Target for Enhancing the Efficacy of Conventional Non-Surgical Therapy. Cells, 10(5), 1169. https://doi.org/10.3390/cells10051169