
Profiling Complement System Components in Primary CNS Vasculitis

Abstract
1. Introduction
2. Materials and Methods
2.1. Study Subjects
2.2. Complement Profiling
2.3. Statistics
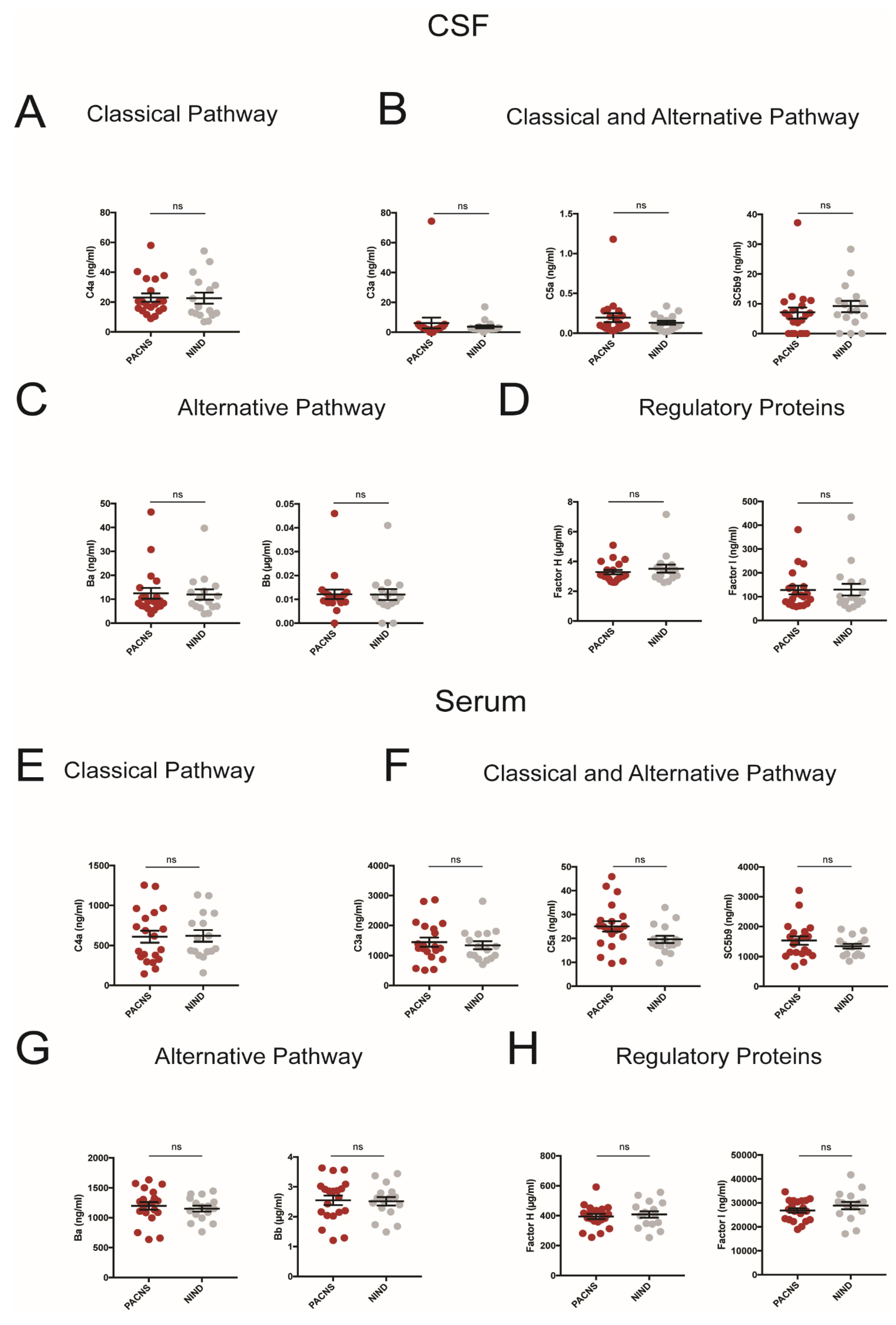
3. Results
4. Discussion and Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mandel-Brehm, C.; Retallack, H.; Knudsen, G.M.; Yamana, A.; Hajj-Ali, R.A.; Calabrese, L.H.; Tihan, T.; Sample, H.A.; Zorn, K.C.; Gorman, M.P.; et al. Exploratory proteomic analysis implicates the alternative complement cascade in primary CNS vasculitis. Neurology 2019, 93, e433–e444. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.; McGookey, M.; Wang, Y.; Cataland, S.R.; Wu, H.M. Effect of Blood Sampling, Processing, and Storage on the Measurement of Complement Activation Biomarkers. Am. J. Clin. Pathol. 2015, 143, 558–565. [Google Scholar] [CrossRef] [PubMed]
- Tange, C.E.; Johnson-Brett, B.; Cook, A.; Stordeur, P.; Brohet, F.; Jolles, S.; Steven, R.; Ponsford, M.; Roberts, A.; El-Shanawany, T.; et al. Quantification of human complement C2 protein using an automated turbidimetric immunoassay. Clin. Chem. Lab. Med. 2018, 56, 1498–1506. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, V.; Póvoa, P.; Costa, A.; Ducla-Soares, J. Cerebrospinal fluid and therapy of isolated angiitis of the central nervous system. Stroke 1994, 25, 1693–1695. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.; Jayne, D.R.W.; Zhao, M.C.M.-H. Complement in ANCA-associated vasculitis: Mechanisms and implications for management. Nat. Rev. Nephrol. 2017, 13, 359–367. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Clinical, Demographical and Laboratory Characteristics | PACNS | NINDS |
|---|---|---|
| Age–median (IQR) | 44.5 (33.75–44.5) | 59.5 (33.25–66.5) |
| Male—n (%) | 10/20 (50) | 9 (56.3) |
| Immunosuppression at time of CSF/Blood sampling—n (%) | 9/20 (45) | - |
| Brain Imaging | - | |
| Angiographic abnormality—n (%) | 16/20 (80) | - |
| Contrast-enhancement leptomeningeal/parenchymatous—n (%) | 4/20 (20) | - |
| CSF parameters | - | |
| WBC count, cells/µL—median (IQR) | 5 (1.25–56.0) | 3 (2–4.75) |
| Protein level, mg/L—median (IQR) | 493.5 (362–607.5) | 415.5 (353.75–542.5) |
| Oligoclonal bands, pos—n (%) | 5/20 (25) | 0 |
| Intrathecal Ig-synthesis, yes—n (%) | 7/20 (35) | 0 |
| Brain biopsy—n (%) | 11/20 (55) | - |
| High-suspected—n (%) | 15/20 (75) | - |
| Biopsy-proven—n (%) | 6/20 (30) | - |
| Lymphocytic—n (%) | 4/6 (66.6) | - |
| Granulomatous—n (%) | 2/6 (33.3) | - |
| Necrotizing—n (%) | 0 (0) | - |
| Active disease—n (%) | 18 (90) | - |
| In Remission—n (%) | 2 (10) | - |
| With Immunosuppression | 1/2 (50) | - |
| Without Immunosuppression | 1/2 (50) | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Deb-Chatterji, M.; Keller, C.W.; Koch, S.; Wiendl, H.; Gerloff, C.; Magnus, T.; Lünemann, J.D. Profiling Complement System Components in Primary CNS Vasculitis. Cells 2021, 10, 1139. https://doi.org/10.3390/cells10051139
Deb-Chatterji M, Keller CW, Koch S, Wiendl H, Gerloff C, Magnus T, Lünemann JD. Profiling Complement System Components in Primary CNS Vasculitis. Cells. 2021; 10(5):1139. https://doi.org/10.3390/cells10051139
Chicago/Turabian StyleDeb-Chatterji, Milani, Christian W. Keller, Simon Koch, Heinz Wiendl, Christian Gerloff, Tim Magnus, and Jan D. Lünemann. 2021. "Profiling Complement System Components in Primary CNS Vasculitis" Cells 10, no. 5: 1139. https://doi.org/10.3390/cells10051139
APA StyleDeb-Chatterji, M., Keller, C. W., Koch, S., Wiendl, H., Gerloff, C., Magnus, T., & Lünemann, J. D. (2021). Profiling Complement System Components in Primary CNS Vasculitis. Cells, 10(5), 1139. https://doi.org/10.3390/cells10051139