
Incremental Experience in In Vitro Primary Culture of Human Pulmonary Arterial Endothelial Cells Harvested from Swan-Ganz Pulmonary Arterial Catheters

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
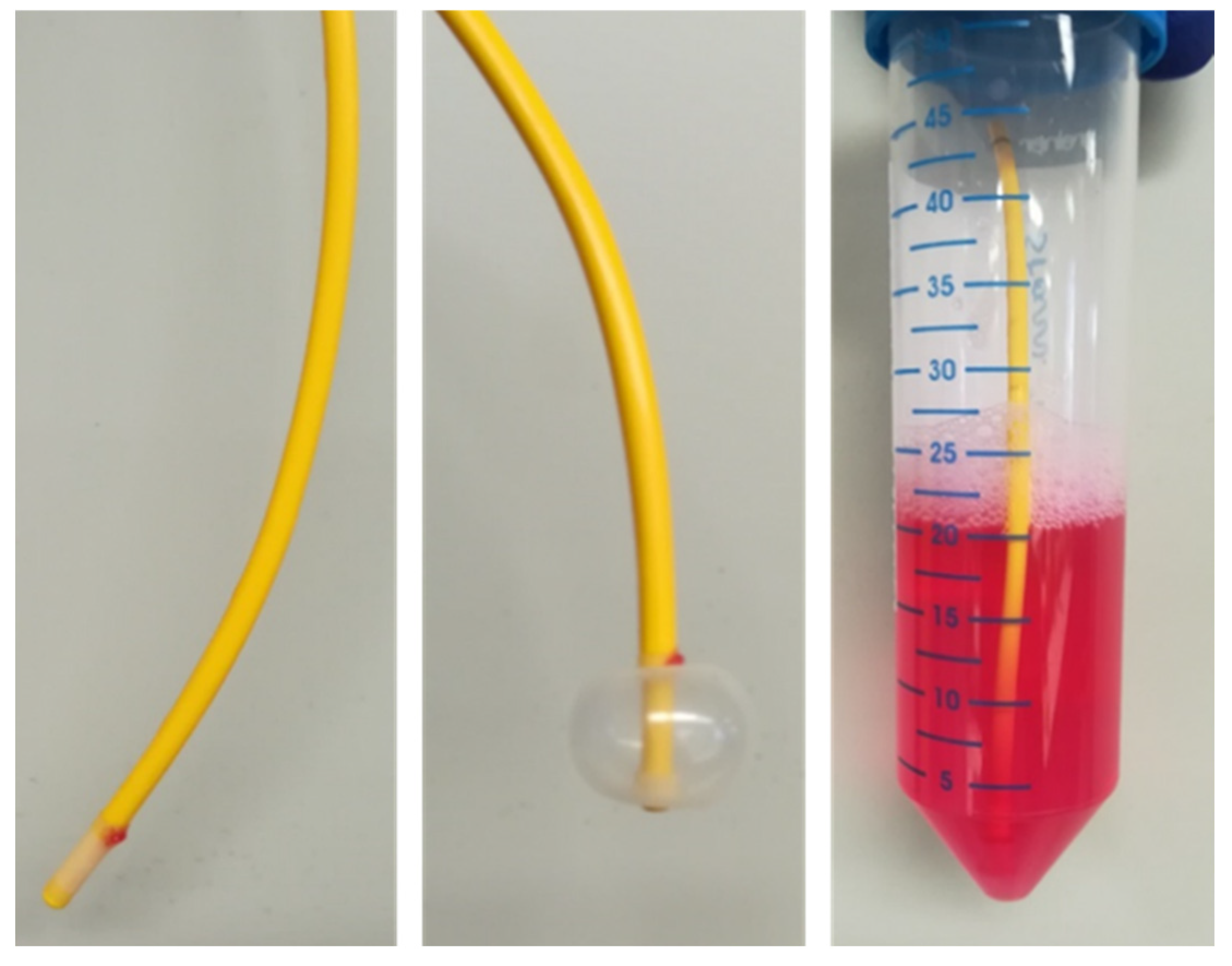
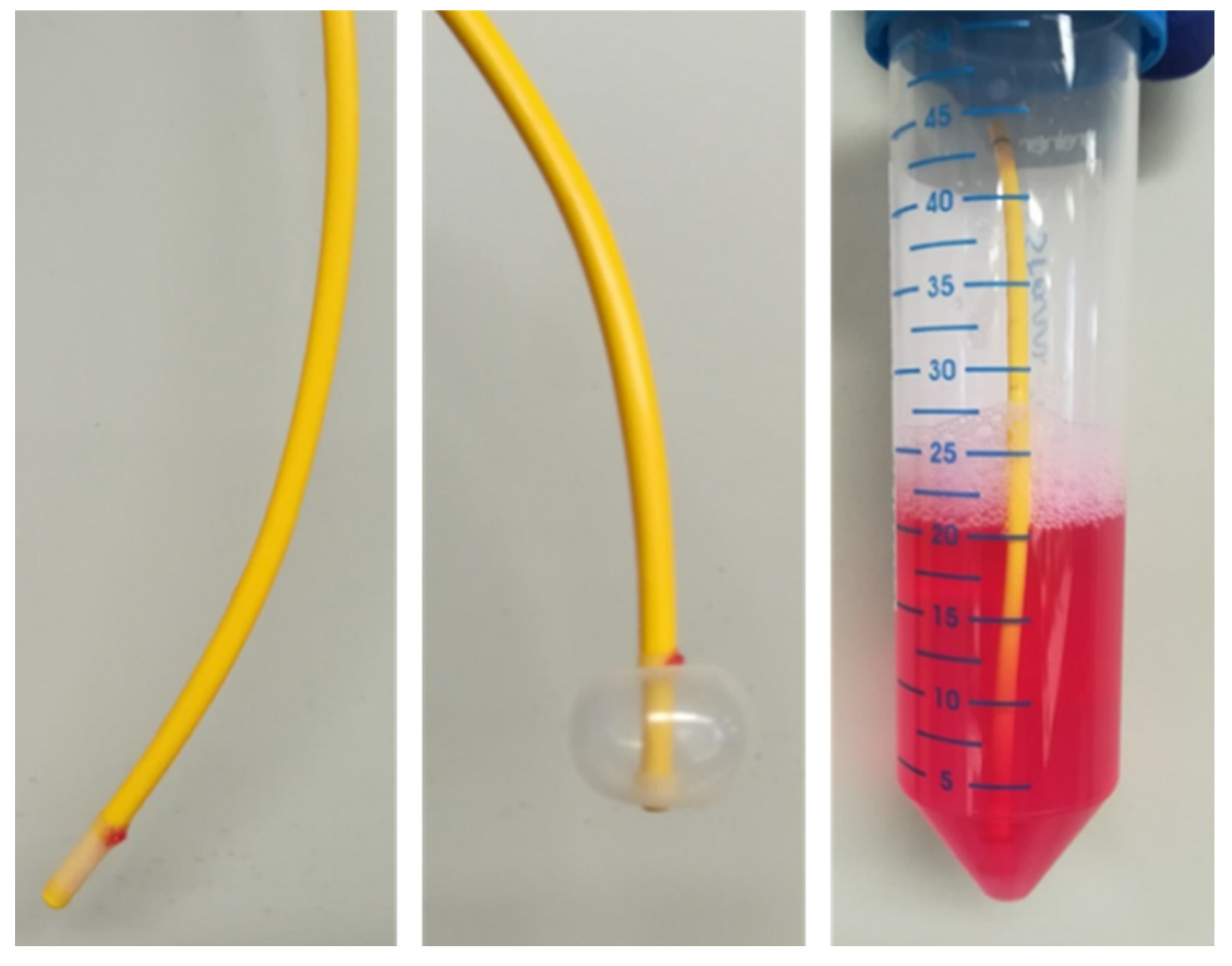
2.1. Isolation of PAECs from Swan-Ganz Pulmonary Arterial Catheters
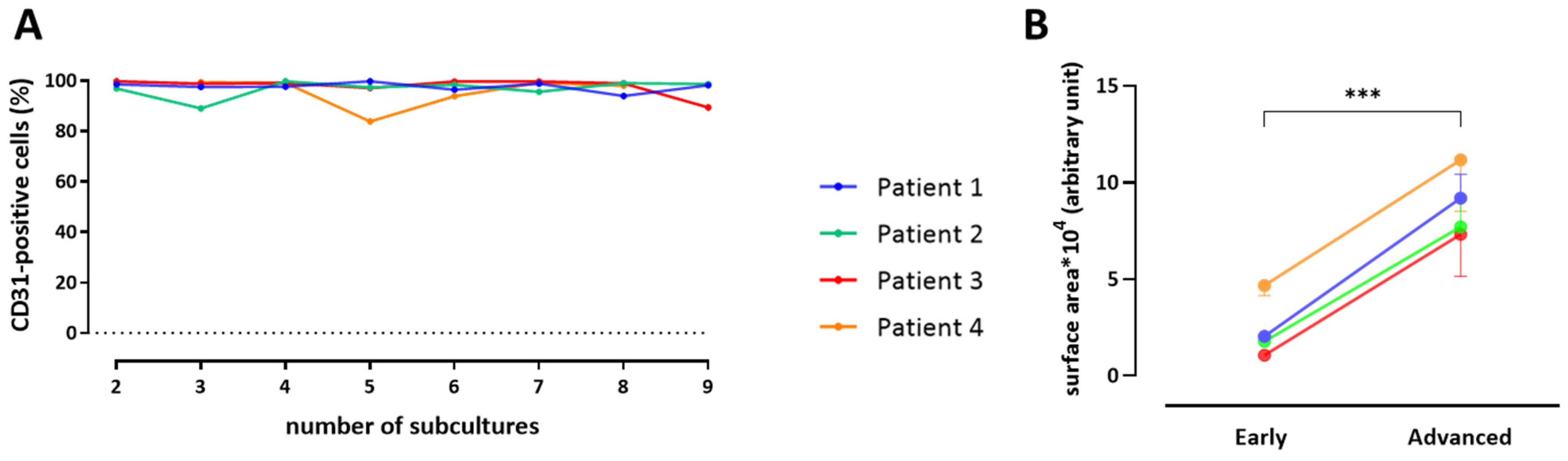
2.2. Quantitative Phenotyping by Flow Cytometry
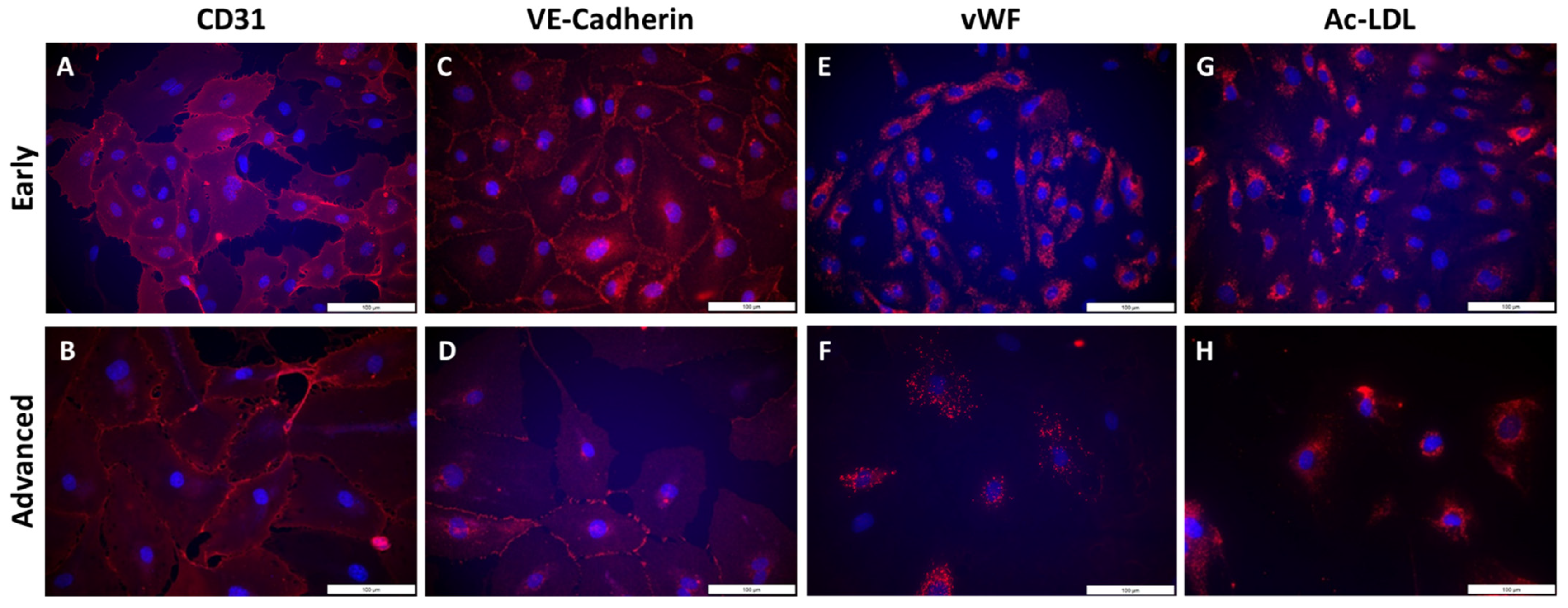
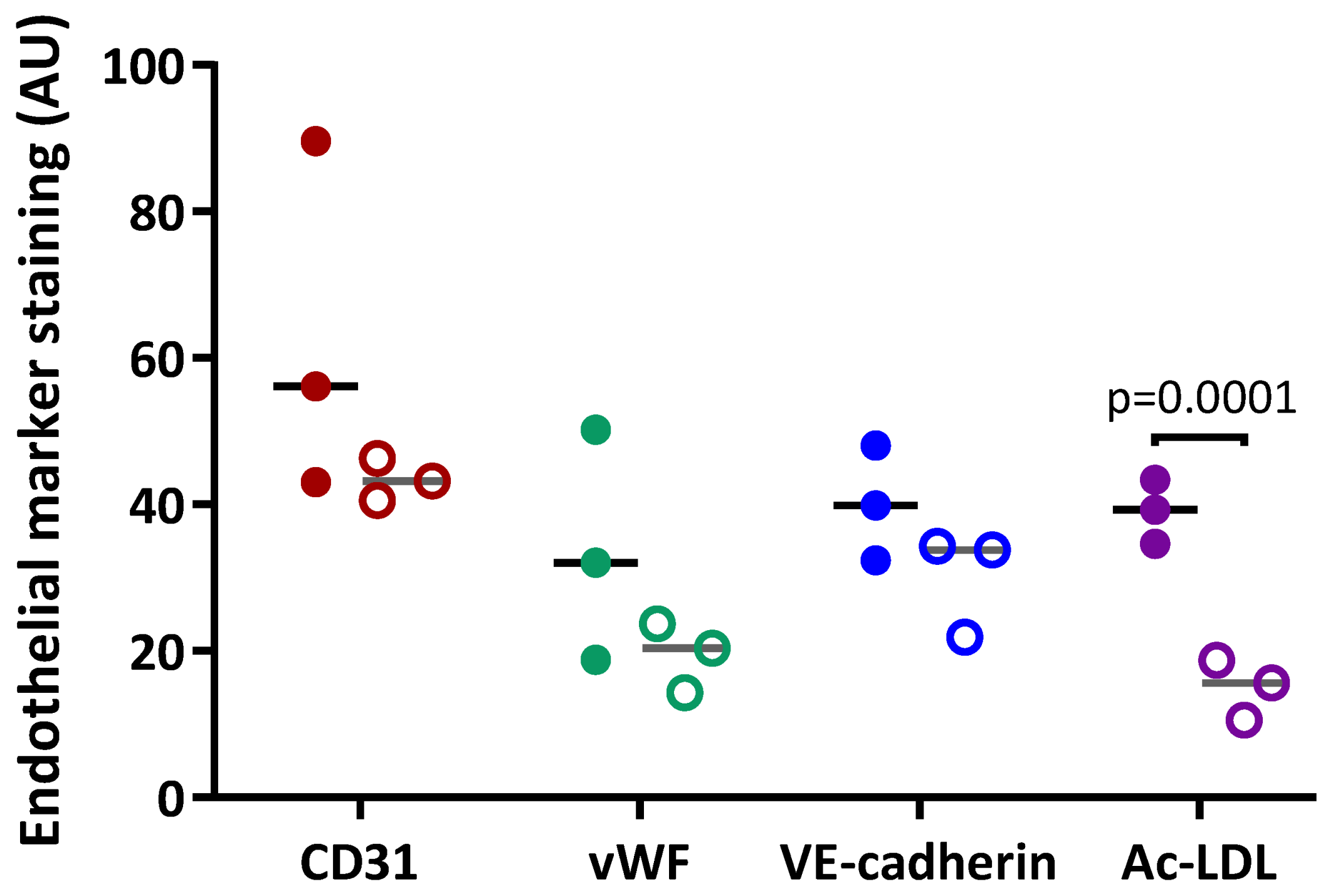
2.3. Qualitative Phenotyping of PAECs Using Immunofluorescence
2.4. Statistical Analysis
3. Results
3.1. Collection of Patient Cells and Patient Characteristics
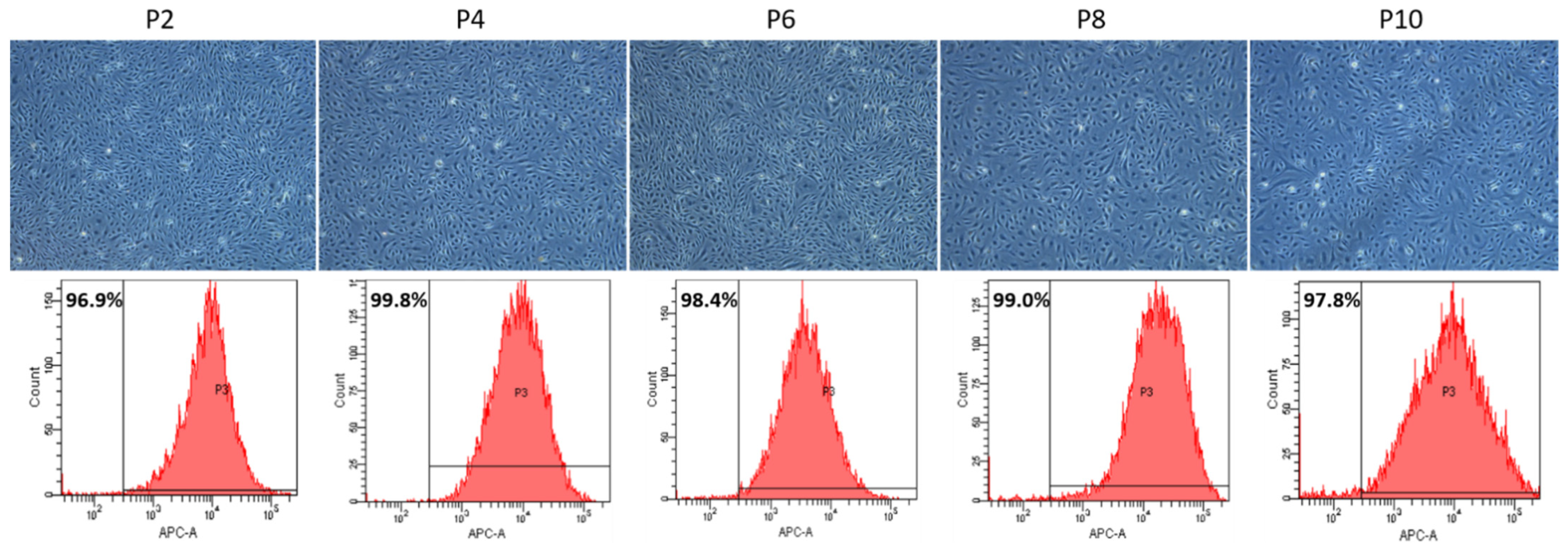
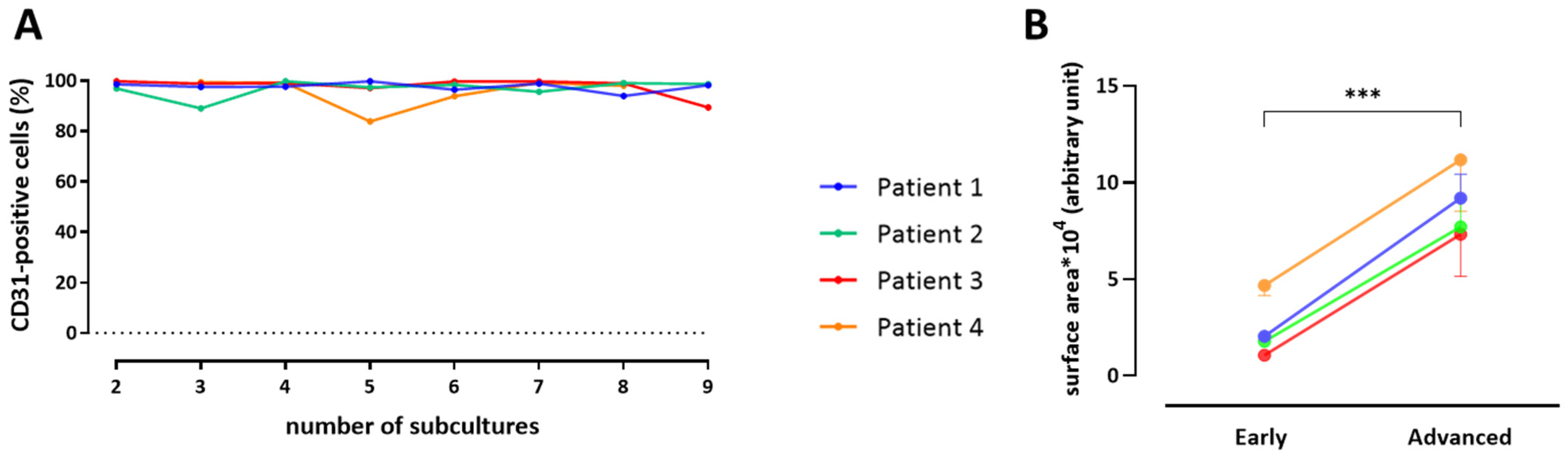
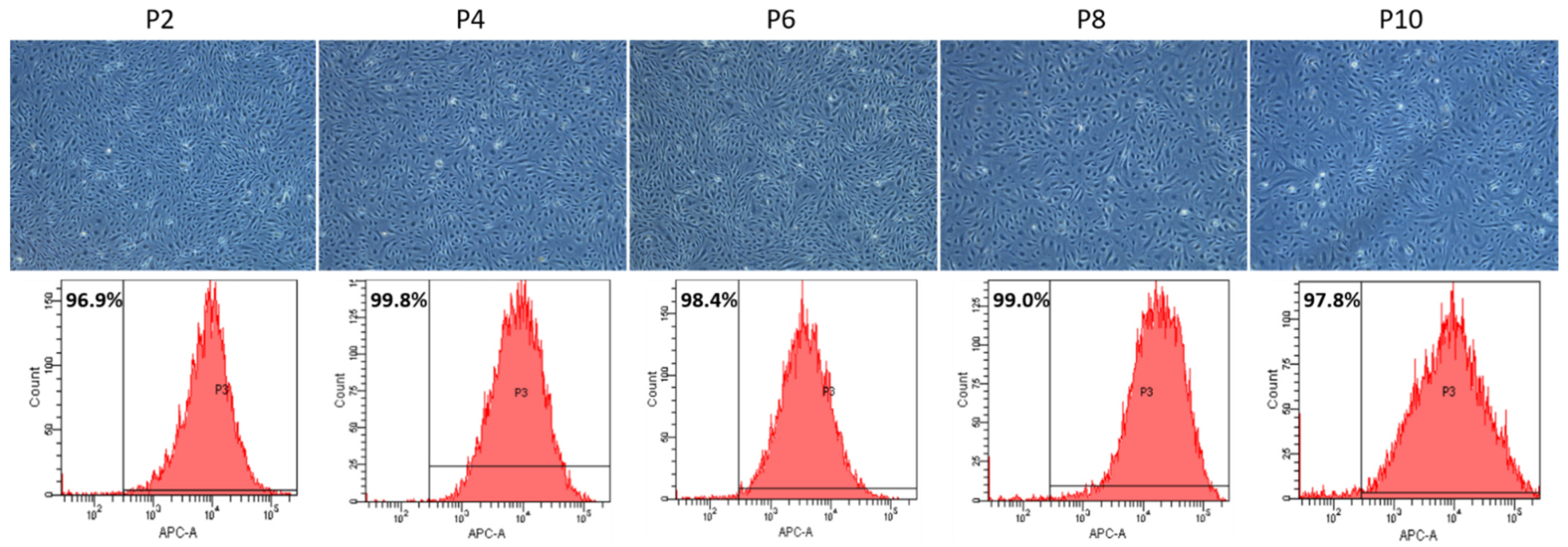
3.2. Quantitative Phenotyping of PAECs throughout Subcultures
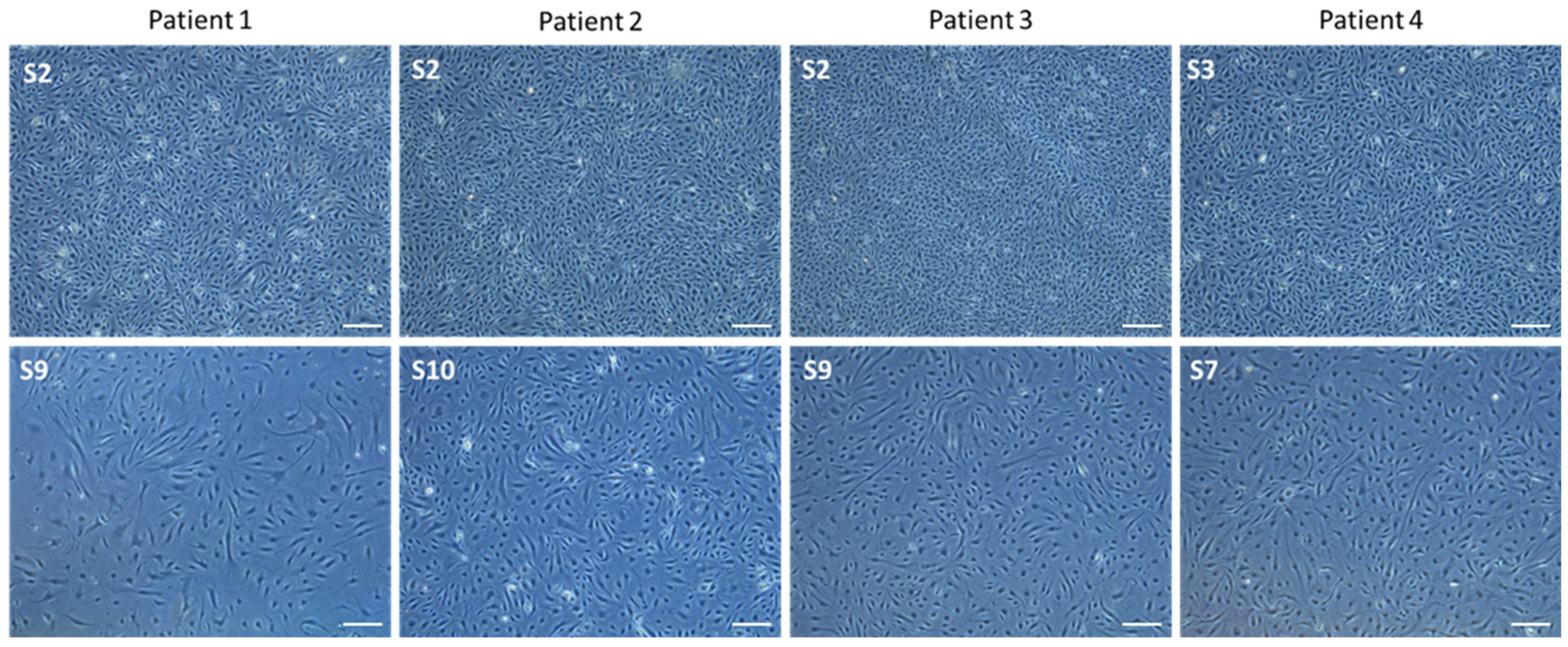
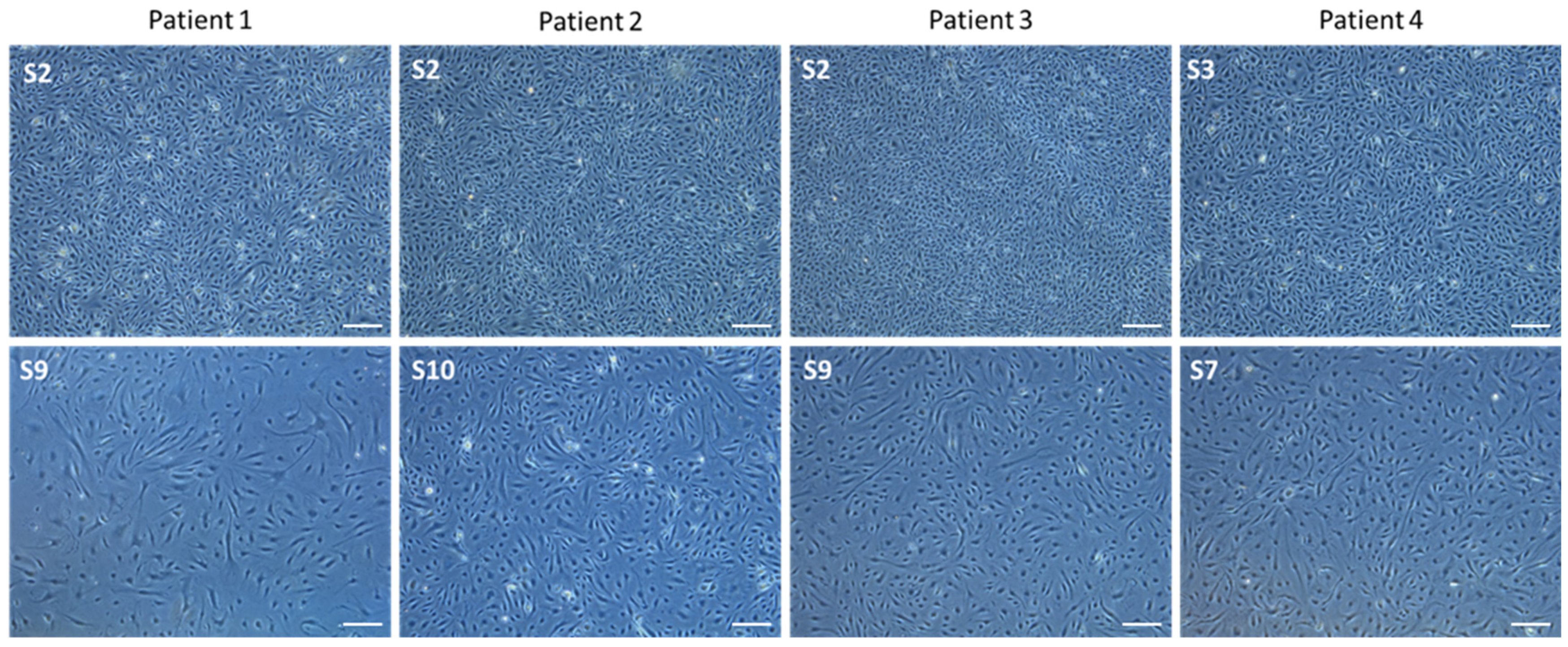
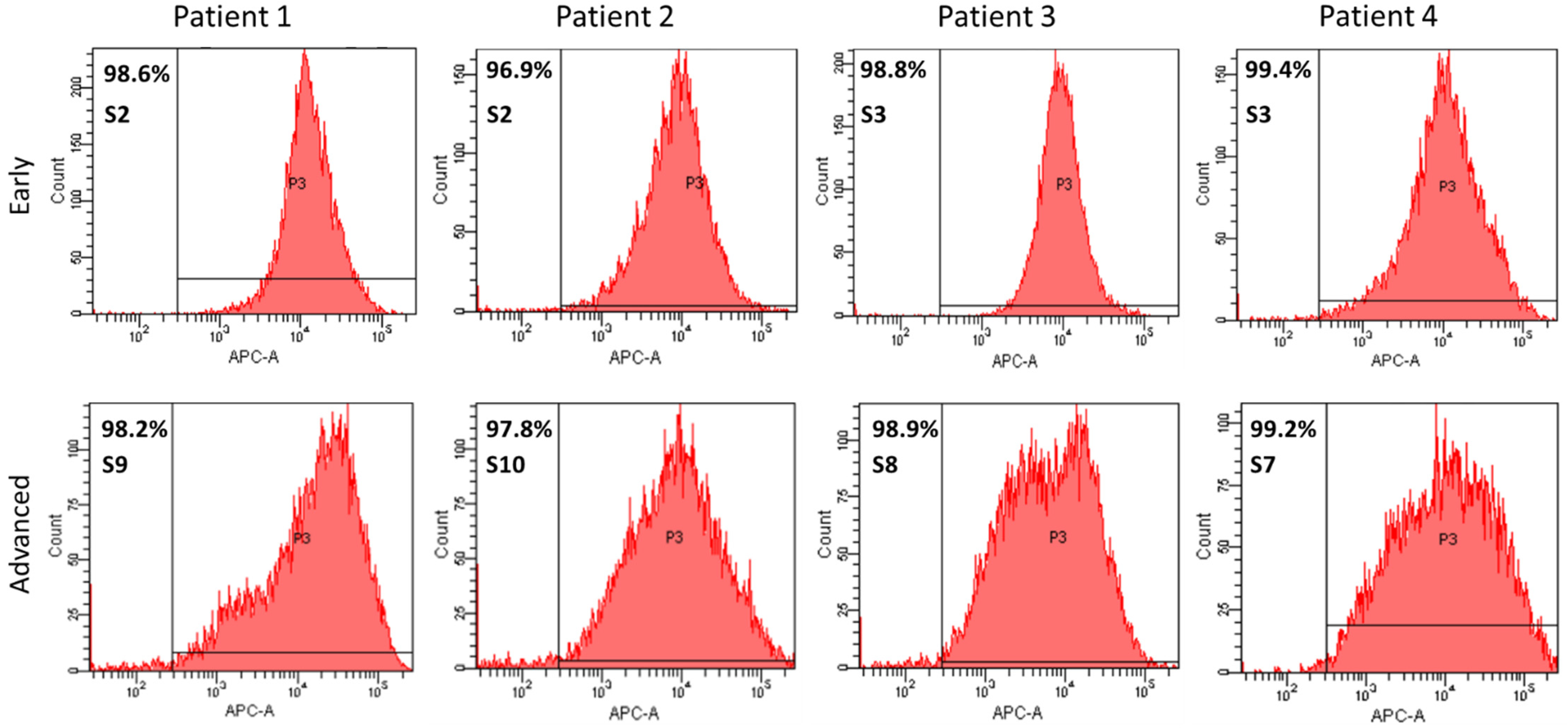
3.3. Qualitative Phenotyping of PAECs Using Endothelial-Specific Markers in Early and Late Subcultures
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Morrell, N.W. Pulmonary hypertension due to BMPR2 mutation: A new paradigm for tissue remodeling? Proc. Am. Thorac. Soc. 2006, 3, 680–686. [Google Scholar] [CrossRef] [PubMed]
- Budhiraja, R.; Tuder, R.M.; Hassoun, P.M. Endothelial dysfunction in pulmonary hypertension. Circulation 2004, 109, 159–165. [Google Scholar] [CrossRef] [PubMed]
- Benza, R.L.; Gomberg-Maitland, M.; Miller, D.P.; Frost, A.; Frantz, R.P.; Foreman, A.J.; Badesch, D.B.; McGoon, M.D. The REVEAL Registry Risk Score Calculator in Patients Newly Diagnosed With Pulmonary Arterial Hypertension. Chest 2012, 141, 354–362. [Google Scholar] [CrossRef] [PubMed]
- Galiè, N.; Channick, R.N.; Frantz, R.P.; Grünig, E.; Jing, Z.C.; Moiseeva, O.; Preston, I.R.; Pulido, T.; Safdar, Z.; Tamura, Y.; et al. Risk stratification and medical therapy of pulmonary arterial hypertension. Eur. Respir. J. 2019, 53, 1801889. [Google Scholar] [CrossRef] [PubMed]
- Carman, B.L.; Predescu, D.N.; Machado, R.; Predescu, S.A. Plexiform Arteriopathy in Rodent Models of Pulmonary Arterial Hypertension. Am. J. Pathol. 2019, 189, 1133–1144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tielemans, B.; Stoian, L.; Gijsbers, R.; Michiels, A.; Wagenaar, A.; Farre Marti, R.; Belge, C.; Delcroix, M.; Quarck, R. Cytokines trigger disruption of endothelium barrier function and p38 MAP kinase activation in BMPR2-silenced human lung microvascular endothelial cells. Pulm. Circ. 2019, 9, 2045894019883607. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geti, I.; Ormiston, M.L.; Rouhani, F.; Toshner, M.; Movassagh, M.; Nichols, J.; Mansfield, W.; Southwood, M.; Bradley, A.; Rana, A.A.; et al. A Practical and Efficient Cellular Substrate for the Generation of Induced Pluripotent Stem Cells from Adults: Blood-Derived Endothelial Progenitor Cells. STEM CELLS Transl. Med. 2012, 1, 855–865. [Google Scholar] [CrossRef] [PubMed]
- Gu, M.; Shao, N.Y.; Sa, S.; Li, D.; Termglinchan, V.; Ameen, M.; Karakikes, I.; Sosa, G.; Grubert, F.; Lee, J.; et al. Patient-specific iPSC-derived endothelial cells uncover pathways that protect against pulmonary hypertension in BMPR2 mutation carriers. Cell Stem Cell 2017, 20, 490–504. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pollett, J.B.; Benza, R.L.; Murali, S.; Shields, K.J.; Passineau, M.J. Harvest of pulmonary artery endothelial cells from patients undergoing right heart catheterization. J. Heart Lung Transpl. 2013, 32, 746–749. [Google Scholar] [CrossRef] [PubMed]
- Ventetuolo, C.E.; Aliotta, J.M.; Braza, J.; Chichger, H.; Dooner, M.; McGuirl, D.; Mullin, C.J.; Newton, J.; Pereira, M.; Princiotto, A.; et al. Culture of Pulmonary Arterial Endothelial Cells from Pulmonary Artery Catheter Balloon Tips: Considerations for Use in Pulmonary Vascular Disease. Eur. Respir. J. 2020, 55, 1901313. [Google Scholar] [CrossRef] [PubMed]
- Quarck, R.; Wynants, M.; Ronisz, A.; Sepulveda, M.R.; Wuytack, F.; Van, R.D.; Meyns, B.; Delcroix, M. Characterization of proximal pulmonary arterial cells from chronic thromboembolic pulmonary hypertension patients. Respir Res. 2012, 13, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vengethasamy, L.; Hautefort, A.; Tielemans, B.; Belge, C.; Perros, F.; Verleden, S.; Fadel, E.; Van, R.D.; Delcroix, M.; Quarck, R. BMPRII influences the response of pulmonary microvascular endothelial cells to inflammatory mediators. Pflügers Arch. 2016, 468, 1969–1983. [Google Scholar] [CrossRef] [Green Version]
- Humbert, M.; Guignabert, C.; Bonnet, S.; Dorfmüller, P.; Klinger, J.R.; Nicolls, M.R.; Olschewski, A.J.; Pullamsetti, S.S.; Schermuly, R.T.; Stenmark, K.R.; et al. Pathology and pathobiology of pulmonary hypertension: State of the art and research perspectives. Eur. Respir. J. 2019, 53, 1801887. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Passineau, M.J.; Gallo, P.H.; Williams, G.; Perez, R.; Benza, R.L. Harvest of Endothelial Cells from the Balloon Tips of Swan-Ganz Catheters after Right Heart Catheterization. J. Vis. Exp. 2019, 143, e58353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benza, R.L.; Williams, G.; Wu, C.; Shields, K.J.; Raina, A.; Murali, S.; Passineau, M.J. In situ expression of Bcl-2 in pulmonary artery endothelial cells associates with pulmonary arterial hypertension relative to heart failure with preserved ejection fraction. Pulm. Circ. 2016, 6, 551–556. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ormiston, M.L.; Toshner, M.R.; Kiskin, F.N.; Huang, C.J.Z.; Groves, E.; Morrell, N.W.; Rana, A.A. Generation and Culture of Blood Outgrowth Endothelial Cells from Human Peripheral Blood. J. Vis. Exp. JoVE 2015, 106, e53384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quarck, R.; Perros, F. Rescuing BMPR2-driven endothelial dysfunction in PAH: A novel treatment strategy for the future? Stem Cell Investig. 2017, 12, 4–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All (n = 132) | Successful (n = 56) | Unsuccessful (n = 76) | p-Value | |
|---|---|---|---|---|
| Age, years | 64 (23–89) | 64 (27–89) | 64 (23–83) | 0.72 |
| Gender, male (%) | 33 | 37 | 30 | |
| BMI kg/m2 | 25 (17–47) | 24 (18–47) | 26 (17–41) | 0.54 |
| Etiology (%) | ||||
| IPAH | 34 | 32 | 36 | |
| HPAH | 4 | 5 | 3 | |
| Drug/toxin | 6 | 7 | 5 | |
| APAH | 13 | 7 | 17 | |
| PVOD | 2 | 4 | 1 | |
| PH sec to HD | 5 | 2 | 8 | |
| PAH sec to LD | 2 | 4 | 1 | |
| CTEPH | 25 | 30 | 21 | |
| No PH | 8 | 9 | 8 | |
| PAH-specific therapy (%) | ||||
| treatment-naive | 49 | 45 | 53 | |
| monotherapy | 12 | 14 | 11 | |
| dual therapy | 21 | 20 | 22 | |
| triple therapy | 15 | 18 | 13 | |
| CCB | 2 | 4 | 1 | |
| NYHA FC | 0.43 | |||
| I | 12 | 5 | 7 | |
| II | 61 | 25 | 36 | |
| III | 54 | 23 | 31 | |
| IV | 5 | 3 | 2 | |
| RAP (mmHg) | 7 (1–25) | 7 (2–25) | 7 (1–22) | 0.46 |
| mPAP (mmHg) | 41 (11–106) | 39.5 (11–70) | 43 (13–106) | 0.75 |
| PAWP (mmHg) | 10 (2–57) | 10 (4–57) | 10 (2–22) | 0.70 |
| PVR (dyn·s·sec−5) | 530 (61–2187) | 539 (61–2187) | 527 (72–1706) | 0.97 |
| CI (L/min/m2) | 2.5 (1.1–4.7) | 2.5 (1.1–3.9) | 2.6 (1.3–4.7) | 0.33 |
| SvO2 (%) | 65.5 (37–95) | 65 (39–80) | 66 (37–95) | 0.38 |
| 6–MWD (m) | 360 (23–747) | 386 (60–580) | 349 (23–747) | 0.66 |
| NT–proBNP (ng/mL) | 807 (8–21834) | 753 (53–21834) | 807 (8–13395) | 0.55 |
| 2015 | 2016 | 2017 | 2018 | 2019 | Total | |
|---|---|---|---|---|---|---|
| Total SG catheters collected | 15 | 17 | 34 | 43 | 23 | 132 |
| Successful culture (%) | 6 (40%) | 4 (24%) | 15 (44%) | 20 (47%) | 11 (48%) | 56 (42%) |
| Stored PAECs (%) | 4 (25%) | 3 (18%) | 2 (6%) | 6 (14%) | 8 (35%) | 23 (27%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tielemans, B.; Stoian, L.; Wagenaar, A.; Leys, M.; Belge, C.; Delcroix, M.; Quarck, R. Incremental Experience in In Vitro Primary Culture of Human Pulmonary Arterial Endothelial Cells Harvested from Swan-Ganz Pulmonary Arterial Catheters. Cells 2021, 10, 3229. https://doi.org/10.3390/cells10113229
Tielemans B, Stoian L, Wagenaar A, Leys M, Belge C, Delcroix M, Quarck R. Incremental Experience in In Vitro Primary Culture of Human Pulmonary Arterial Endothelial Cells Harvested from Swan-Ganz Pulmonary Arterial Catheters. Cells. 2021; 10(11):3229. https://doi.org/10.3390/cells10113229
Chicago/Turabian StyleTielemans, Birger, Leanda Stoian, Allard Wagenaar, Mathias Leys, Catharina Belge, Marion Delcroix, and Rozenn Quarck. 2021. "Incremental Experience in In Vitro Primary Culture of Human Pulmonary Arterial Endothelial Cells Harvested from Swan-Ganz Pulmonary Arterial Catheters" Cells 10, no. 11: 3229. https://doi.org/10.3390/cells10113229
APA StyleTielemans, B., Stoian, L., Wagenaar, A., Leys, M., Belge, C., Delcroix, M., & Quarck, R. (2021). Incremental Experience in In Vitro Primary Culture of Human Pulmonary Arterial Endothelial Cells Harvested from Swan-Ganz Pulmonary Arterial Catheters. Cells, 10(11), 3229. https://doi.org/10.3390/cells10113229