
Development of In-Situ Spray for Local Delivery of Antibacterial Drug for Hidradenitis Suppurativa: Investigation of Alternative Formulation

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Methodology
2.2.1. Formulation of In Situ Gelling System
2.2.2. Characterization of In Situ Gelling Formulation
2.2.3. Measurement of pH
2.2.4. Measurement of Viscosity
2.2.5. Spray Pattern
2.2.6. Ex Vivo Bioadhesion Test
2.2.7. Ex Vivo Retention Test
2.2.8. Preparation of Clindamycin In Situ Spray
2.2.9. Preparation of Standard Curve for Clindamycin
2.2.10. In Vitro Drug Release Test and Release Kinetics
2.2.11. Antimicrobial Test
2.2.12. Cytotoxicity Test
2.2.13. Statistical Analysis
3. Results
3.1. Formulation of In Situ Gelling System
3.2. Viscosity
3.3. Ex Vivo Bioadhesion Test
3.4. Ex Vivo Retention Test
3.5. pH of the In Situ Gelling Formulation
3.6. Spray Pattern
3.7. In Vitro Drug Release Test
3.8. Drug Release Kinetics
3.9. Antimicrobial Test
3.10. Cytotoxicity Test
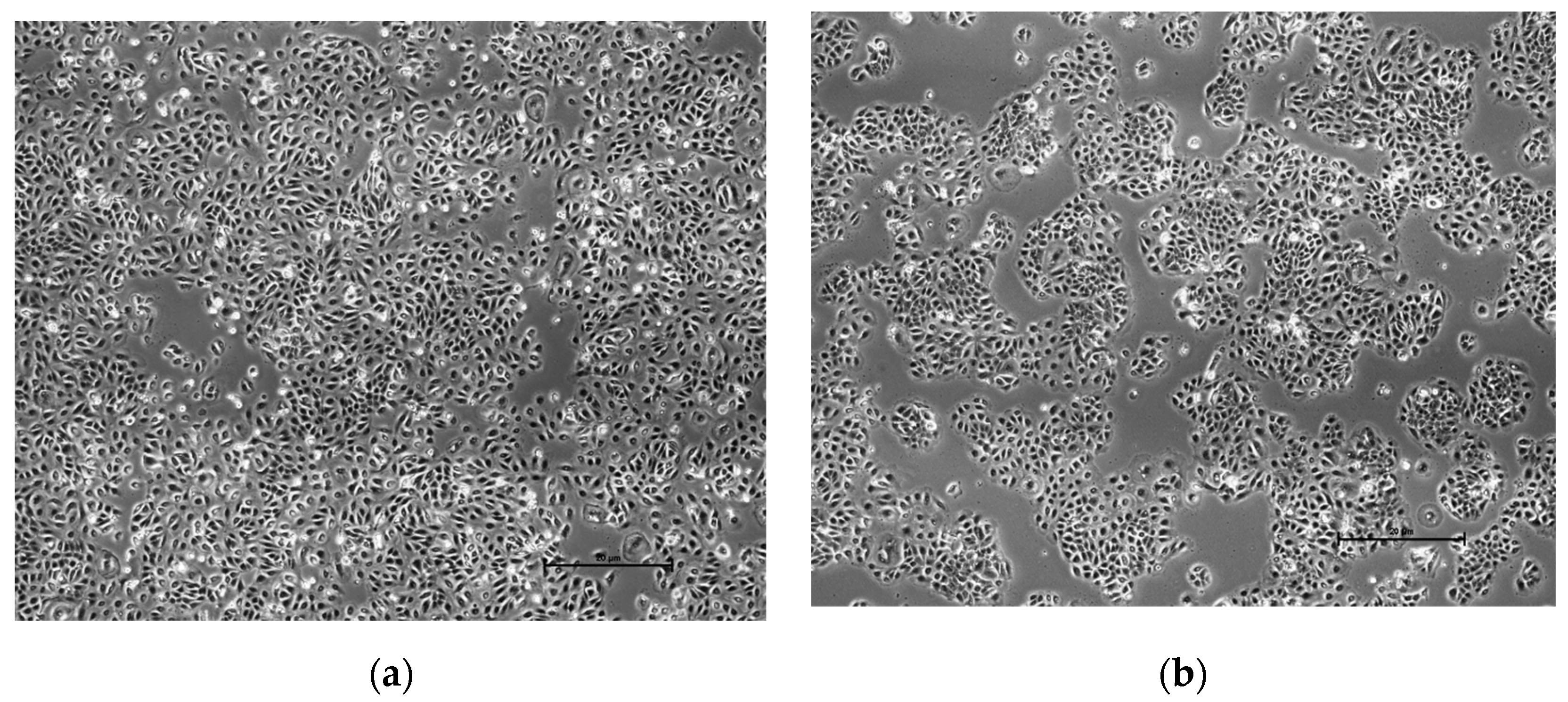
3.11. Cell Morphology
4. Discussion
5. Conclusions and Future Recommendation
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kassab, Y.; Muhamad, S.; Aldahoul, H.; Mohammed, I.; Paneerselvam, G.; Ayad, M. The impact of skin disorders on patients’ quality of life in Malaysia. J. Clin. Intensive Care Med. 2019, 4, 001–009. [Google Scholar]
- Szepietowski, J.C.; Matusiak, Ł. Hidradenitis Suppurativa: The Disease Which Stimulates Researchers and Clinicians. Dermatology 2020, 236, 5–7. [Google Scholar] [CrossRef]
- Ring, H.C.; Riis Mikkelsen, P.; Miller, I.M.; Jenssen, H.; Fuursted, K.; Saunte, D.M.; Jemec, G.B. The bacteriology of hidradenitis suppurativa: A systematic review. Exp. Dermatol. 2015, 24, 727–731. [Google Scholar] [CrossRef] [PubMed]
- Kokolakis, G.; Wolk, K.; Schneider-Burrus, S.; Kalus, S.; Barbus, S.; Gomis-Kleindienst, S.; Sabat, R. Delayed Diagnosis of Hidradenitis Suppurativa and Its Effect on Patients and Healthcare System. Dermatology 2020, 236, 421–430. [Google Scholar] [CrossRef] [PubMed]
- Ferris, A.; Harding, K. Hidradenitis suppurativa: A clinical summary. Wounds UK 2019, 15, 53–57. [Google Scholar]
- Scuderi, N.; Monfrecola, A.; Dessy, L.A.; Fabbrocini, G.; Megna, M.; Monfrecola, G. Medical and Surgical Treatment of Hidradenitis Suppurativa: A Review. Ski. Appendage Disord. 2017, 3, 95. [Google Scholar] [CrossRef] [Green Version]
- Napolitano, M.; Megna, M.; Timoshchuk, E.A.; Patruno, C.; Balato, N.; Fabbrocini, G.; Monfrecola, G. Hidradenitis suppurativa: From pathogenesis to diagnosis and treatment. Clin. Cosmet. Investig. Dermatol. 2017, 10, 105–115. [Google Scholar] [CrossRef] [Green Version]
- Nomura, T. Hidradenitis Suppurativa as a Potential Subtype of Autoinflammatory Keratinization Disease. Front. Immunol. 2020, 11, 847. [Google Scholar] [CrossRef]
- Dasankoppa, F.S.; Solankiy, P.; Sholapur, H.N.; Jamakandi, V.G.; Sajjanar, V.M.; Walveka, P.M. Design, formulation, and evaluation of in situ gelling ophthalmic drug delivery system comprising anionic and nonionic polymers. Indian J. Heal. Sci. Biomed. Res. 2017, 10, 323. [Google Scholar] [CrossRef]
- Kurniawansyah, I.S.; Sopyan, I.; Aditya, W.A.; Nuraini, H.; Dwi Alminda, F.; Nurlatifah, A. Preformed gel vs in situ gel: A review. Int. Res. J. Pharm. 2018, 9, 1. [Google Scholar]
- Lakshmi, P.; Harini, K. Design and Optimization of Thermo-reversible Nasal in situ Gel of Atomoxetine Hydrochloride Using Taguchi Orthogonal Array Design. Dhaka Univ. J. Pharm. Sci. 2019, 18, 183–193. [Google Scholar] [CrossRef] [Green Version]
- Hurler, J.; Škalko-Basnet, N. Potentials of Chitosan-Based Delivery Systems in Wound Therapy: Bioadhesion Study. J. Funct. Biomater. 2012, 3, 37–48. [Google Scholar] [CrossRef] [Green Version]
- Aslani, A.; Ghannadi, A.; Najafi, H. Design, formulation and evaluation of a mucoadhesive gel from Quercus brantii L. and coriandrum sativum L. as periodontal drug delivery. Adv. Biomed. Res. 2013, 2, 21. [Google Scholar] [CrossRef]
- Chin, L.Y.; Tan, J.Y.P.; Choudhury, H.; Pandey, M.; Sisinthy, S.P.; Gorain, B. Development and optimization of chitosan coated nanoemulgel of telmisartan for intranasal delivery: A comparative study. J. Drug Deliv. Sci. Technol. 2021, 62, 102341. [Google Scholar] [CrossRef]
- Gupta, A.; Garg, S.; Khar, R. Measurement of bioadhesive strength of mucoadhesive buccal tablets: Design of an in-vitro assembly. Indian Drugs 1993, 30, 152–155. [Google Scholar]
- Asmani, F.; Abdullah, I.; Khan, J.; Budiasih, S. Determination of Permeation Pathways of Clindamycin Phosphate into the Skin. Am. J. Pharm. Tech. Res. 2015, 5, 257. [Google Scholar]
- Fazli, N.; Khan, A.; Khan, A.; Nasir, F.; Iqbal, Z.; Khan, I.; Khan, J.A.; Khuda, F.; Zakir, S.; Yousaf, N.; et al. Development and evaluation of pluronic-and methylcellulose-based thermoreversible drug delivery system for insulin OrBito IMI Project View project Taste masking View project Development and evaluation of pluronic-and methylcellulose-based thermoreversible. Drug Dev. Ind. Pharm. 2013, 40, 1503–1508. [Google Scholar]
- Purushothama, P.S.; Nayak, M.; Bhargav, H.S.; Shastri, S.D.; Nayak, M.M. Measurement of the Zone of Inhibition of an Antibiotic. In Proceedings of the 2016 IEEE 6th International Conference on Advanced Computing, Andhra Pradesh, India, 27–28 February 2016; pp. 409–414. [Google Scholar]
- Petushkova, N.A.; Rusanov, A.L.; Pyatnitskiy, M.A.; Larina, O.V.; Zgoda, V.G.; Lisitsa, A.V.; Luzgina, N.G. Proteomic characterization of HaCaT keratinocytes provides new insights into changes associated with SDS exposure. Biomed. Dermatol. 2020, 4, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Riss, T.L.; Moravec, R.A.; Niles, A.L.; Duellman, S.; Benink, H.A.; Worzella, T.J.; Minor, L. Cell Viability Assays; NCBI Bookself; Eli Lilly & Company and the National Center for Advancing Translational Sciences: Bethesda, MD, USA, 2016. [Google Scholar]
- Hilton, A.; Armstrong, R. Stat note 6: Post hoc anova tests. Microbiologist 2006, 2006, 34–36. [Google Scholar]
- Frew, J.W.; Hawkes, J.E.; Krueger, J.G. Topical, systemic and biologic therapies in hidradenitis suppurativa: Pathogenic insights by examining therapeutic mechanisms. Ther. Adv. Chronic Dis. 2019, 10, 1–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mandhar, P.; Joshi, G. Development of Sustained Release Drug Delivery System: A Review. Asian Pac. J. Health Sci. 2015, 2, 179–185. [Google Scholar] [CrossRef]
- Rupal, J.; Mallikarjuna Setty, C.; Patel, D.; Kaushal, J.; Mallikarjuna, S.C.; Dipti, P. Preparation and Evaluation of Topical Gel of Valdecoxib. Artic. Int. J. Pharm. Sci. Drug Res. 2010, 2, 4. [Google Scholar]
- Sanjana, A.; Ahmed, M.G.; BH, J.G. Preparation and evaluation of in-situ gels containing hydrocortisone for the treatment of aphthous ulcer. J. Oral Biol. Craniofacial Res. 2021, 11, 269–276. [Google Scholar]
- Patel, P.; Patel, P. Formulation and evaluation of clindamycin HCL in situ gel for vaginal application. Int. J. Pharm. Investig. 2015, 5, 50–56. [Google Scholar] [CrossRef] [Green Version]
- Chatterjee, S.; Hui, P.C. Review of stimuli-responsive polymers in drug delivery and textile application. Molecules 2019, 24, 2547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bodratti, A.M.; Alexandridis, P. Formulation of Poloxamers for Drug Delivery. J. Funct. Biomater. 2018, 9, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagai, N.; Isaka, T.; Deguchi, S.; Minami, M.; Yamaguchi, M.; Otake, H.; Okamoto, N.; Nakazawa, Y. In Situ Gelling Systems Using Pluronic F127 Enhance Corneal Permeability of Indomethacin Nanocrystals. Int. J. Mol. Sci. 2020, 21, 7083. [Google Scholar] [CrossRef]
- Jain, D. Newer Trends in In Situ Gelling Systems for Controlled Ocular Drug Delivery. J. Anal. Pharm. Res. 2016, 2, 00022. [Google Scholar] [CrossRef]
- Yu, J.; Qiu, H.; Yin, S.; Wang, H.; Li, Y. Polymeric Drug Delivery System Based on Pluronics for Cancer Treatment. Molecules 2021, 26, 3610. [Google Scholar] [CrossRef] [PubMed]
- Cunha-Filho, M.S.S.; Alvarez-Lorenzo, C.; Martínez-Pacheco, R.; Landin, M. Temperature-sensitive gels for intratumoral delivery of β-lapachone: Effect of cyclodextrins and ethanol. Sci. World J. 2012, 2012, 8. [Google Scholar] [CrossRef] [Green Version]
- Geng, H.; Song, H.; Qi, J.; Cui, D. Sustained release of VEGF from PLGA nanoparticles embedded thermo-sensitive hydrogel in full-thickness porcine bladder acellular matrix. Nanoscale Res. Lett. 2011, 6, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Liu, L.; Yong, K.-T.; Roy, I.; Law, W.-C.; Ye, L.; Liu, J.; Liu, J.; Kumar, R.; Zhang, X.; Prasad, P.N. Bioconjugated Pluronic Triblock-Copolymer Micelle-Encapsulated Quantum Dots for Targeted Imaging of Cancer: In Vitro and In Vivo Studies. Theranostics 2012, 2, 705. [Google Scholar] [CrossRef] [Green Version]
- Swamy, G.N.; Abbas, Z. Mucoadhesive in situ gels as nasal drug delivery systems: An overview. Artic. Asian J. Pharm. Sci. 2012, 2012, 168–180. [Google Scholar]
- da Silva Júnior, W.F.; de Oliveira Pinheiro, J.G.; Moreira, C.D.L.F.A.; de Souza, F.J.J.; de Lima, Á.A.N. Alternative Technologies to Improve Solubility and Stability of Poorly Water-Soluble Drugs. In Multifunctional Systems for Combined Delivery, Biosensing and Diagnostics; Elsevier: Amsterdam, The Netherlands, 2017; pp. 281–305. [Google Scholar]
- Kaur, G.; Grewal, J.; Jyoti, K.; Jain, U.K.; Chandra, R.; Madan, J. Oral controlled and sustained drug delivery systems: Concepts, advances, preclinical, and clinical status. In Drug Targeting and Stimuli Sensitive Drug Delivery Systems; Elsevier: Amsterdam, The Netherlands, 2018; pp. 567–626. [Google Scholar]
- Shivakumara, L.R.; Demappa, T. Synthesis and Swelling Behavior of Sodium Alginate/Poly(vinyl alcohol) Hydrogels. Turkish J. Pharm. Sci. 2019, 16, 252. [Google Scholar] [CrossRef]
- Zhang, H.; Cheng, J.; Ao, Q. Preparation of Alginate-Based Biomaterials and Their Applications in Biomedicine. Mar. Drugs 2021, 19, 264. [Google Scholar] [CrossRef]
- Kumar, K.; Dhawan, N.; Sharma, H.; Vaidya, S.; Vaidya, B. Bioadhesive polymers: Novel tool for drug delivery. Artif. Cells Nanomed. Biotechnol. 2014, 42, 274–283. [Google Scholar] [CrossRef] [PubMed]
- Puscaselu, R.G.; Lobiuc, A.; Dimian, M.; Covasa, M. Alginate: From Food Industry to Biomedical Applications and Management of Metabolic Disorders. Polymers 2020, 12, 2417. [Google Scholar] [CrossRef] [PubMed]
- Hariyadi, D.M.; Islam, N. Current status of alginate in drug delivery. Adv. Pharmacol. Pharm. Sci. 2020, 2020, 8886095. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, D.D.; Lai, J.-Y. Advancing the stimuli response of polymer-based drug delivery systems for ocular disease treatment. Polym. Chem. 2020, 11, 6988–7008. [Google Scholar] [CrossRef]
- Chaudhari, S.D.; Misra, M.; Kumar Mandal, U. Formulation and evaluation of thermoreversible mucoadhesive microemulsion based in-situ gel (TMMIG) of an anti-osteoporotic agent. Artic. J. Glob. Pharma Technol. 2010, 2, 43–47. [Google Scholar]
- Ur-Rehman, T.; Tavelin, S.; Gröbner, G. Chitosan in situ gelation for improved drug loading and retention in poloxamer 407 gels. Int. J. Pharm. 2011, 409, 19–29. [Google Scholar] [CrossRef] [PubMed]
- Dasankoppa, F.S.; Kujur, S.; Sholapur, H.P.N.A.; Jamakandi, V.G. Design, formulation and evaluation of carboxy methyl tamarind based in situ gelling ophthalmic drug delivery system of dorzolamide hydrochloride. Indian J. Heal. Sci. Biomed. Res. 2016, 9, 56. [Google Scholar] [CrossRef]
- Thulluru, A.; Mohan Varma, M.; Setty, C.M.; Chintamaneni, P.K.; Samayamanthula, S. Effect of Sodium alginate in Combination With HPMC K 100 M in Extending the Release of Metoprolol Succinate from its Gastro-Retentive Floating Tablets. Indian J. Pharm. Educ. Res. 2015, 49, 293–303. [Google Scholar] [CrossRef] [Green Version]
- Zahir-Jouzdani, F.; Wolf, J.D.; Atyabi, F.; Bernkop-Schnürch, A. In situ gelling and mucoadhesive polymers: Why do they need each other? Expert Opin. Drug Deliv. 2018, 15, 1007–1019. [Google Scholar] [CrossRef]
- Padmaa Paarakh, M.; Ani Jose, P.; Setty, C.M.; Christoper, G.V.P. Release kinetics—Concepts and applications. Int. J. Pharm. Res. Technol. 2018, 8, 12–20. [Google Scholar]
- Guo, P.; Buttaro, B.A.; Xue, H.Y.; Tran, N.T.; Wong, H.L. Lipid-polymer hybrid nanoparticles carrying linezolid improve treatment of methicillin-resistant Staphylococcus aureus (MRSA) harbored inside bone cells and biofilms. Eur. J. Pharm. Biopharm. 2020, 151, 198. [Google Scholar] [CrossRef] [PubMed]
- Boateng, J.; Okeke, O. Evaluation of Clay-Functionalized Wafers and Films for Nicotine Replacement Therapy via Buccal Mucosa. Pharmaceutics 2019, 11, 104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, N.; Lalwani, D.; Gollmer, S.; Injeti, E.; Sari, Y.; Nesamony, J. Development and evaluation of a calcium alginate based oral ceftriaxone sodium formulation. Prog. Biomater. 2016, 5, 117–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohamed, M.A.; Nasr, M.; Elkhatib, W.F.; Eltayeb, W.N. In Vitro Evaluation of Antimicrobial Activity and Cytotoxicity of Different Nanobiotics Targeting Multidrug Resistant and Biofilm Forming Staphylococci. Biomed Res. Int. 2018, 2018, 7. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Concentration of Pluronic F-127 (%w/v) | Gelation Temperature (°C) (Mean ± SD) | Gelation Time (min) (Mean ± SD) | pH |
|---|---|---|---|
| 14 | No gelation | 6.634 | |
| 16 | 6.758 | ||
| 17 | 34.0 ± 1.08 | 3.21 ± 0.01 | 6.774 |
| 18 | 31.2 ± 0.58 | 2.22 ± 0.02 | 6.832 |
| 19 | 29.0 ± 1.00 | 1.43 ± 0.02 | 6.851 |
| 20 | 28.0 ± 0.50 | 1.25 ± 0.05 | 6.908 |
| 22 | 26.7 ± 0.76 | 1.12 ± 0.10 | 7.043 |
| Concentration of Pluronic F-127 (%w/v) | Conc. of HPMC (%w/v) | Conc. of SA (%w/v) | Gelation Temperature (°C) (mean ± SD) | Gelation Time (min) (mean ± SD) | pH |
|---|---|---|---|---|---|
| 17 | 0.2 | - | 32.3 ± 0.30 | 2.35 ± 0.30 | 6.218 |
| 18 | 0.2 | - | 29.2 ± 0.29 | 1.55 ± 0.70 | 6.322 |
| 19 | 0.2 | - | 28.0 ± 0.76 | 1.33 ± 0.10 | 6.439 |
| 20 | 0.2 | - | 27.5 ± 0.50 | 1.12 ± 0.30 | 6.508 |
| 22 | 0.2 | - | 25.7 ± 0.28 | 0.52 ± 0.40 | 6.628 |
| 17 | - | 0.2 | No gelation | 6.224 | |
| 18 | - | 0.2 | 28.8 ± 0.79 | 2.37 ± 0.50 | 6.346 |
| 19 | - | 0.2 | 27.2 ± 0.29 | 2.14 ± 0.60 | 6.445 |
| 20 | - | 0.2 | 26.0 ± 0.50 | 1.28 ± 0.20 | 6.513 |
| 22 | - | 0.2 | 24.5 ± 0.50 | 0.55 ± 0.70 | 6.631 |
| Concentration of Pluronic F-127 (%w/v) | Conc. of HPMC (%w/v) | Conc. of SA (%w/v) | Gelation Temperature (°C) (Mean ± SD) | Gelation Time (min) (Mean ± SD) | pH |
|---|---|---|---|---|---|
| 18 | 0.1 | - | 29.8 ± 0.58 | 2.13 ± 0.20 | 6.328 |
| 18 | 0.2 | - | 29.2 ± 0.29 | 1.55 ± 0.70 | 6.322 |
| 18 | 0.4 | - | 26.7 ± 0.28 | 1.23 ± 0.40 | 6.314 |
| 18 | - | 0.1 | 29.0 ± 0.50 | 2.44 ± 0.20 | 6.339 |
| 18 | - | 0.2 | 28.8 ± 0.79 | 2.37 ± 0.50 | 6.346 |
| 18 | - | 0.4 | 25.5 ± 0.87 | 2.25 ± 0.50 | 6.358 |
| 18 | 0.1 | 0.1 | 29.7 ± 0.29 | 2.23 ± 0.30 | 6.336 |
| 18 | 0.1 | 0.2 | 29.3 ± 0.29 | 1.48 ± 0.20 | 6.341 |
| 18 | 0.2 | 0.1 | 29.2 ± 0.28 | 2.11 ± 0.60 | 6.332 |
| 18 | 0.2 | 0.2 | 29.0 ± 0.50 | 1.35 ± 0.40 | 6.343 |
| Formulation Name | Concentration of Pluronic F-127 (%w/v) | Concentration of HPMC (%w/v) | Concentration of Sodium Alginate (%w/v) | Bioadhesion (Newton) (Mean ± SD) |
|---|---|---|---|---|
| F | 18 | - | - | 0.42 ± 0.012 |
| F1 | 18 | 0.2 | - | 0.53 ± 0.031 |
| F2 | 18 | - | 0.2 | 0.57 ± 0.019 |
| F3 | 18 | 0.2 | 0.2 | 0.80 ± 0.041 |
| F4 | 18 | 0.1 | 0.2 | 0.59 ± 0.020 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wong, Y.L.; Pandey, M.; Choudhury, H.; Lim, W.M.; Bhattamisra, S.K.; Gorain, B. Development of In-Situ Spray for Local Delivery of Antibacterial Drug for Hidradenitis Suppurativa: Investigation of Alternative Formulation. Polymers 2021, 13, 2770. https://doi.org/10.3390/polym13162770
Wong YL, Pandey M, Choudhury H, Lim WM, Bhattamisra SK, Gorain B. Development of In-Situ Spray for Local Delivery of Antibacterial Drug for Hidradenitis Suppurativa: Investigation of Alternative Formulation. Polymers. 2021; 13(16):2770. https://doi.org/10.3390/polym13162770
Chicago/Turabian StyleWong, Yoke Lan, Manisha Pandey, Hira Choudhury, Wei Meng Lim, Subrat Kumar Bhattamisra, and Bapi Gorain. 2021. "Development of In-Situ Spray for Local Delivery of Antibacterial Drug for Hidradenitis Suppurativa: Investigation of Alternative Formulation" Polymers 13, no. 16: 2770. https://doi.org/10.3390/polym13162770
APA StyleWong, Y. L., Pandey, M., Choudhury, H., Lim, W. M., Bhattamisra, S. K., & Gorain, B. (2021). Development of In-Situ Spray for Local Delivery of Antibacterial Drug for Hidradenitis Suppurativa: Investigation of Alternative Formulation. Polymers, 13(16), 2770. https://doi.org/10.3390/polym13162770