
Ambient Technology to Assist Elderly People in Indoor Risks



Abstract
:1. Introduction
2. Methodology
2.1. Search Items
2.2. Inclusion/Exclusion Criteria
2.3. Data Extraction and Analysis
3. Major Indoor Risks Affecting Elderly People and the Assistive Technology
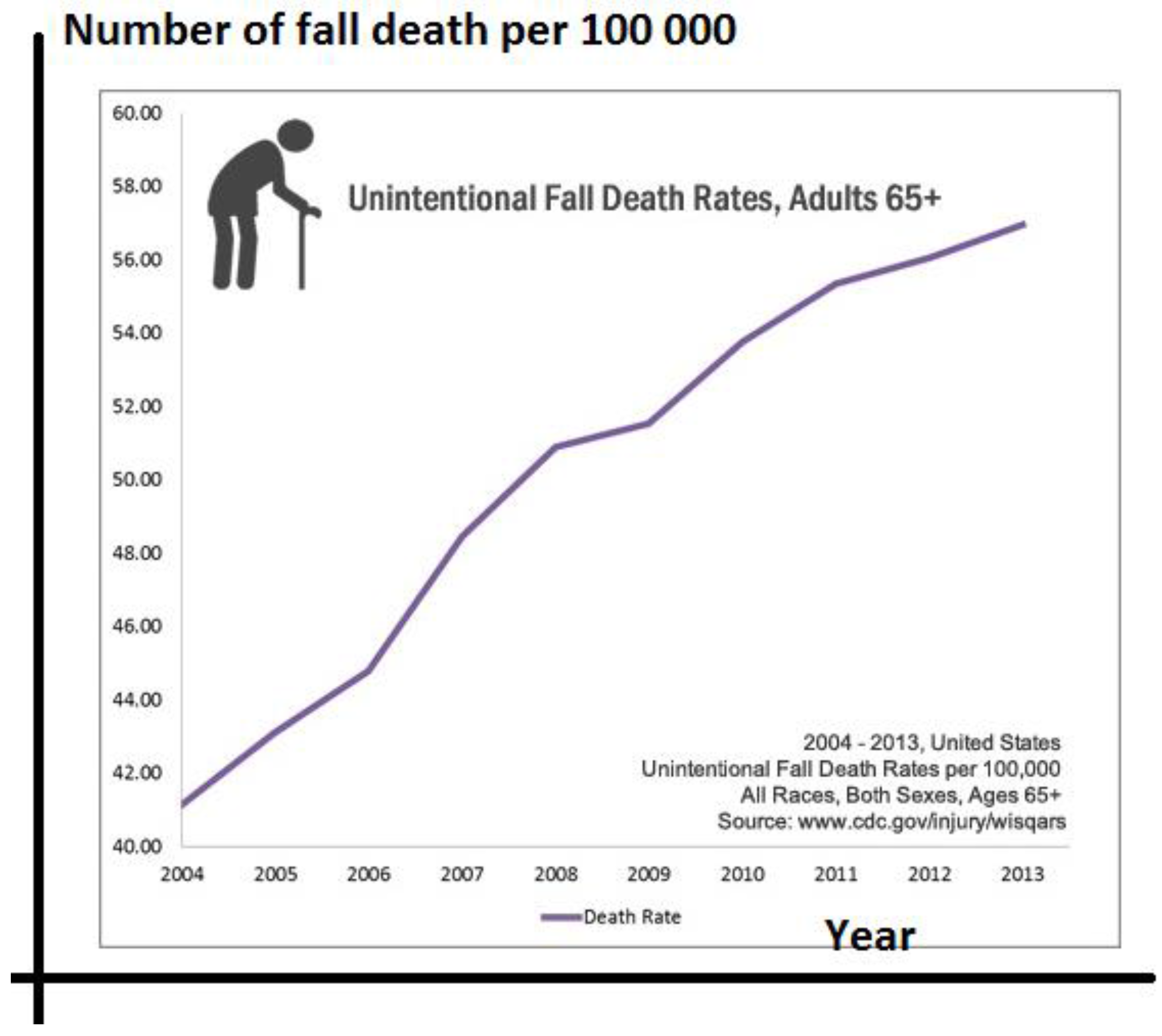
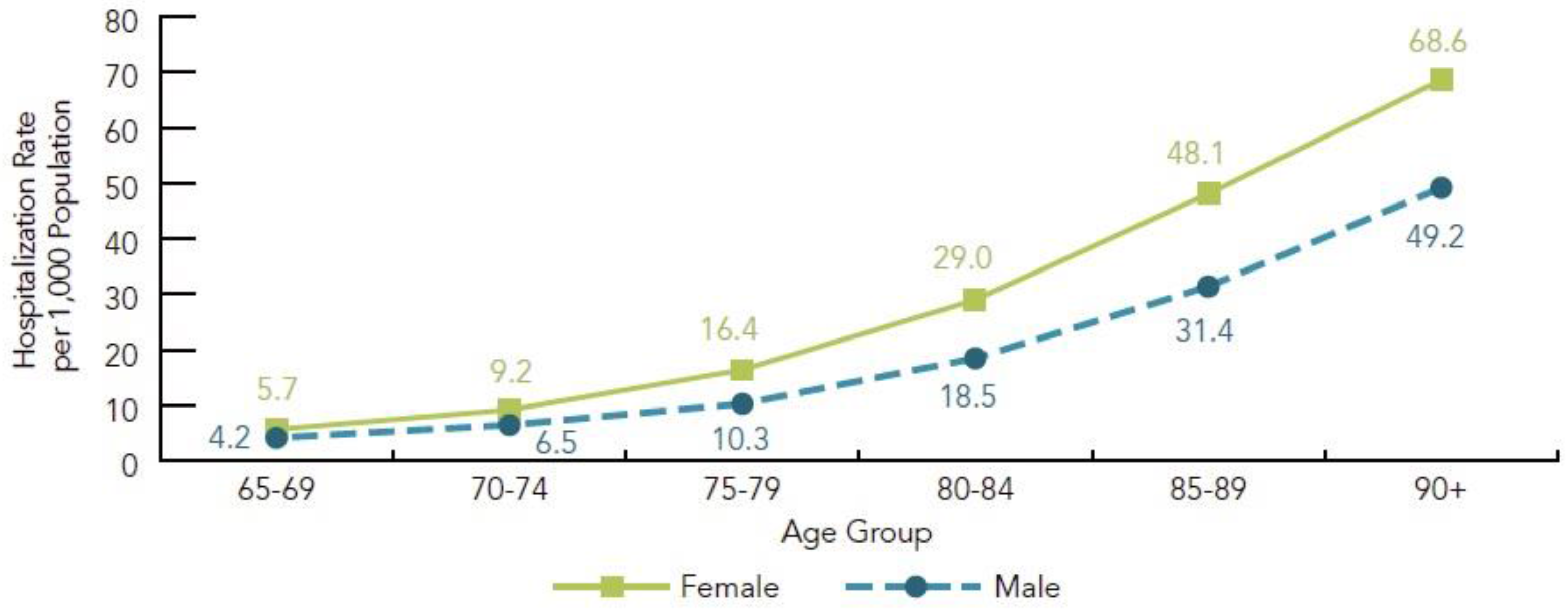
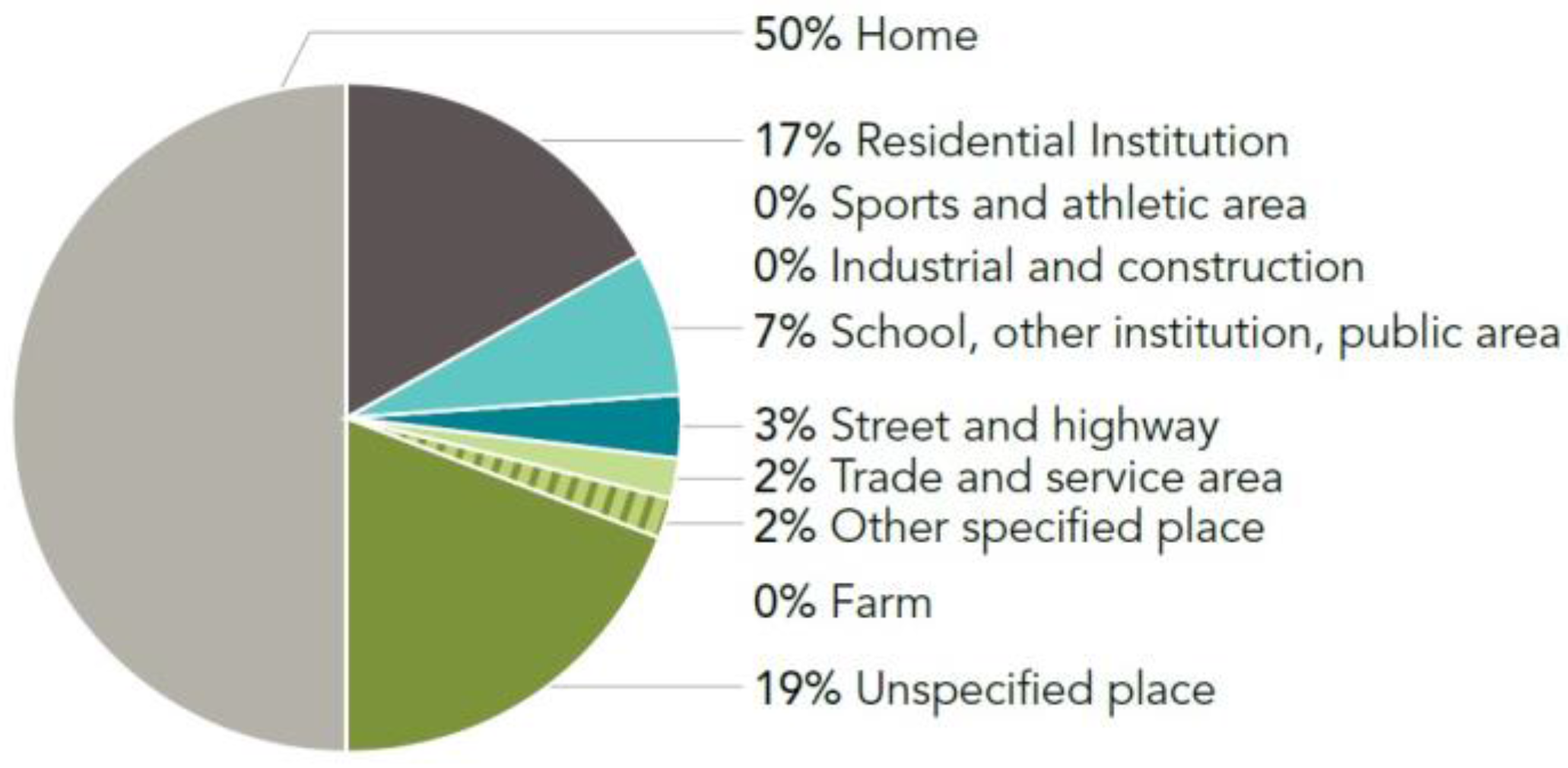
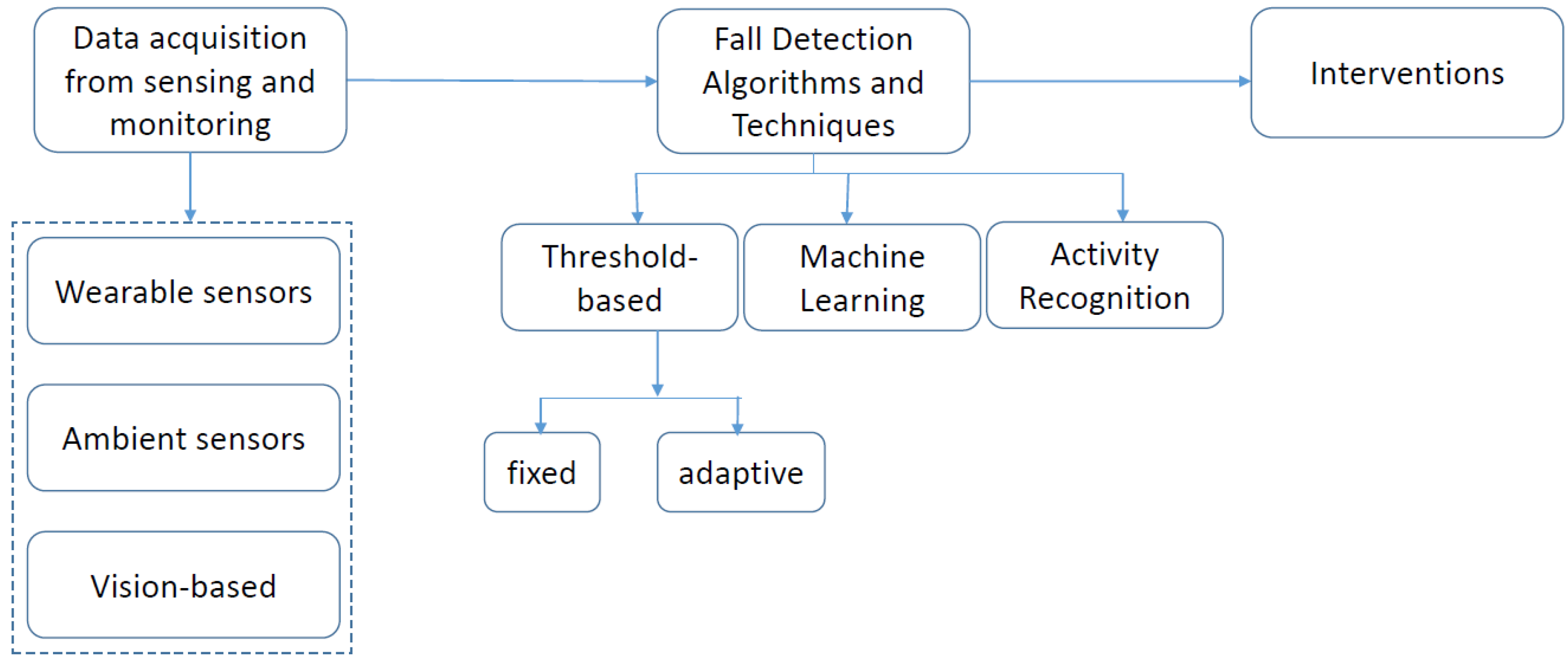
3.1. Fall Risk
3.1.1. Ambient Assistive Technology for Indoor Fall Risk
3.1.2. Discussion
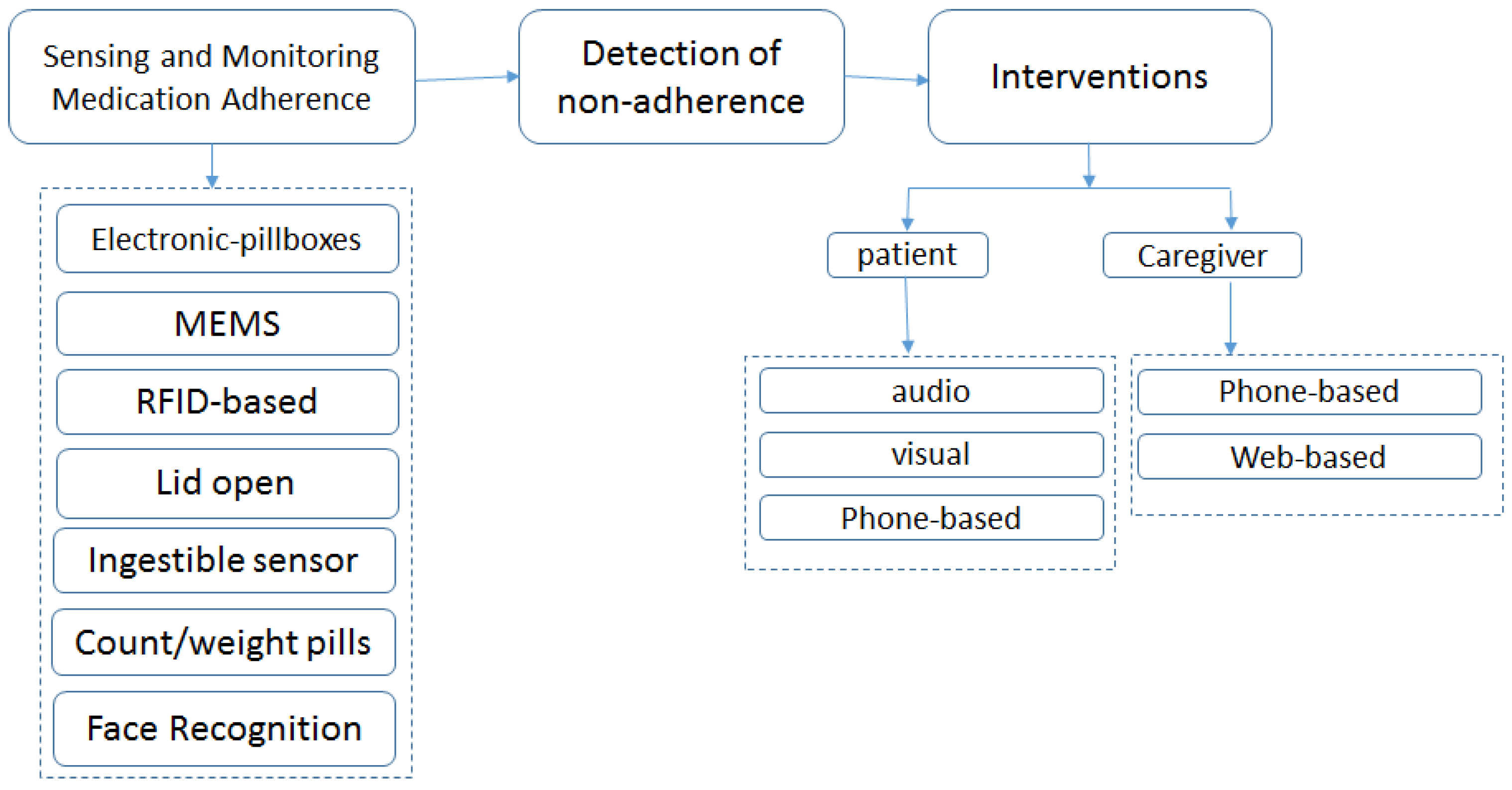
3.2. Risk of Wrong Self-Medication Management (Non-Adherence, Abuse and Misuse)
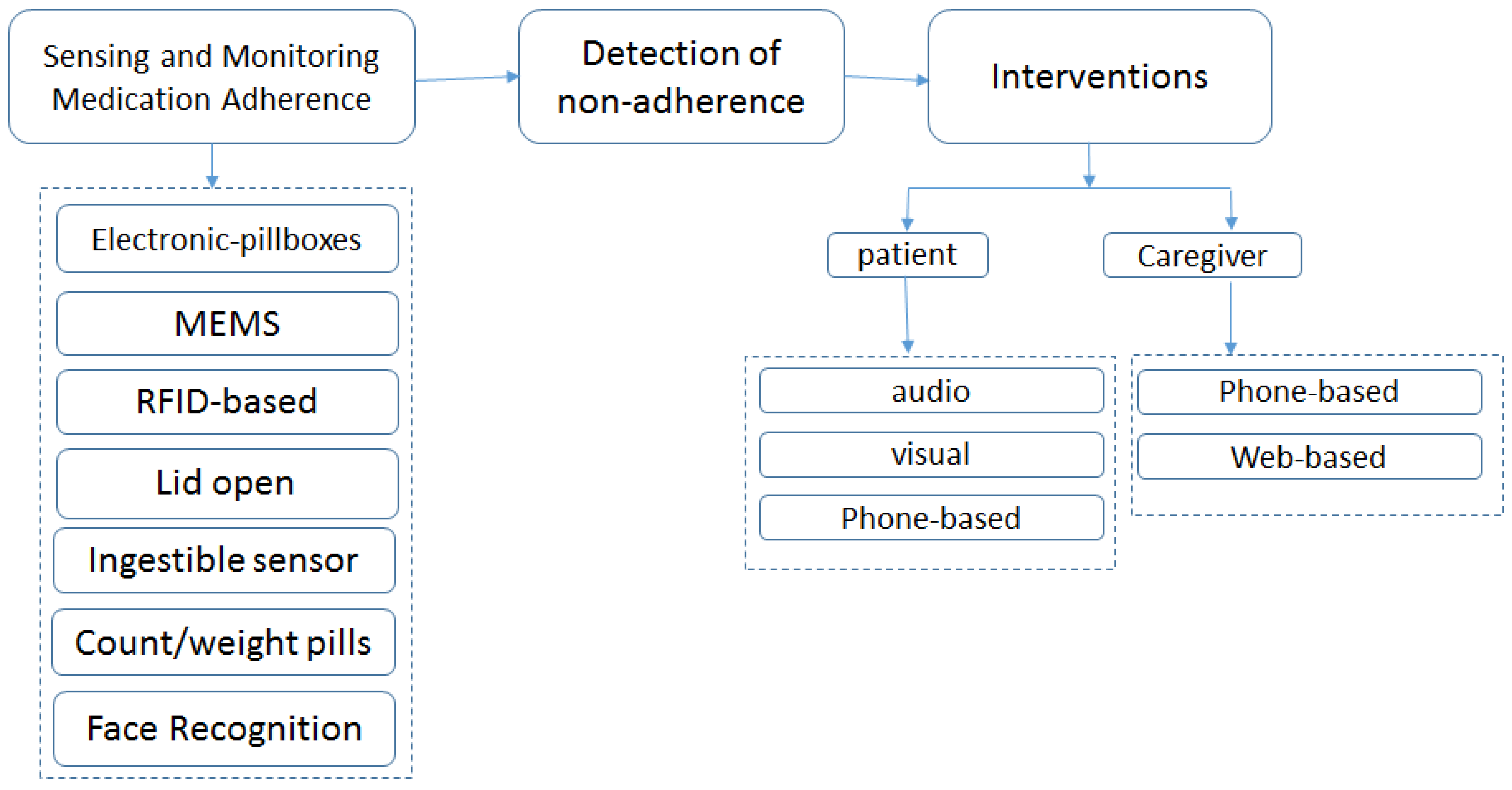
3.2.1. Ambient Assistive Technology for Wrong Self-Medication Management Risk
3.2.2. Discussion
3.3. Risks of Fire, Burns and Intoxication by Gas/Smoke
3.3.1. Risk of Fire
3.3.2. Risk of Burns
3.3.3. Risk of Intoxication by Gas/Smoke
3.3.4. Ambient Assistive Technology for Fire Risk
3.3.5. Ambient Assistive Technology for Burn Risk
3.3.6. Ambient Assistive Technology for Intoxication by Gas/Smoke Risk
3.3.7. Discussion
3.4. Risk of Inactivity and the Assistive Technology
Discussion
4. Conclusions and Future Directions
Conflicts of Interest
References
- Zoncu, R.; Efeyan, A.; Sabatini, M. mTOR: From growth signal integration to cancer, diabetes and ageing. Nat. Rev. Mol. Cell Biol. 2011, 12, 21–35. [Google Scholar] [CrossRef] [PubMed]
- Mynatt, D.; Rogers, A. Understanding User Needs and Attitudes. Gesture 2004, 3, 36–41. [Google Scholar]
- Billette, J.; Janz, T. Living Arrangements of Seniors; Canadian Census: Ottawa, ON, Canada, 2011. Available online: http://www12.statcan.gc.ca/census-recensement/2011/as-sa/98-312-x/98-312-x2011003_4-eng.pdf (accessed on 8 October 2016).
- Martel, L.; Menard, F. Statistics Canada; Canadian Census, Demography Division: Ottawa, ON, Canada, 2011. Available online: http://www12.statcan.gc.ca/census-recensement/2011/as-sa/98-311-x/98-311-x2011001-eng.pdf (accessed on 8 October 2016).
- Toshio, O.; Iwasaki, N. Innovative applications and strategy on ICT applications for aging society: Case study of Japan for silver ICT innovations. In Proceedings of the 7th ACM International Conference on Theory and Practice of Electronic Governance, Seoul, Korea, 22–25 October 2013.
- Loraine, A.; Cole, S.; Goodkind, D.; He, W. 65+ in the United States; U.S. Census Bureau, Government Printing Office: Washington, DC, USA, 2014.
- Jacobsen, A.; Kent, M.; Lee, M.; Mather, M. America’s Aging Population. Popul. Bull. 2011, 66, 1–20. [Google Scholar]
- Robinovitch, S.; Brumer, R.; Maurer, J. Effect of the squat protective response on impact velocity during backward falls. J. Biomech. 2004, 37, 1329–1337. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.; Hoey, J. Review of Fall Detection Techniques: A Data Availability Perspective. 2016; arXiv:1605.09351. [Google Scholar]
- World Health Organization. WHO Global Report on Falls Prevention in Older Age. Available online: http://www.who.int/violence_injury_prevention/publications/other_injury/falls_prevention (accessed on 22 July 2016).
- Rubenstein, L.; Josephson, K.; Robbins, A. Falls in the nursing home. Ann. Intern. Med. 1994, 121, 442–451. [Google Scholar] [CrossRef] [PubMed]
- Important Facts about Falls. Available online: http://www.cdc.gov/HomeandRecreationalSafety/Falls/adultfalls.html (accessed on 23 July 2016).
- Seniors’ Falls in Canada: Second Report. Public Health Agency of Canada, 2014. Available online: http://www.phac-aspc.gc.ca/seniors-aines/publications/public/injury-blessure/seniors_falls-chutes_aines/index-eng.php (accessed on 8 October 2016).
- Injury Prevention & Control: Data & Statistics (WISQARSTM). Available online: http://www.cdc.gov/injury/wisqars/fatal_injury_reports.html (accessed on 27 July 2016).
- Alexander, H.; Rivara, P.; Wolf, E. The cost and frequency of hospitalization for fall-related injuries in older adults. Am. J. Public Health 1992, 82, 1020–1023. [Google Scholar] [CrossRef] [PubMed]
- Sterling, A.; O’Connor, A.; Bonadies, J. Geriatric falls: Injury severity is high and disproportionate to mechanism. J. Trauma Acute Care Surg. 2001, 50, 116–119. [Google Scholar] [CrossRef]
- Parkkari, J.; Kannus, P.; Palvanen, M.; Natri, A.; Vainio, J.; Aho, H.; Vuori, I.; Järvinen, M. Majority of hip fractures occur as a result of a fall and impact on the greater trochanter of the femur: A prospective controlled hip fracture study with 206 consecutive patients. Calcif. Tissue Int. 1999, 65, 183–187. [Google Scholar] [CrossRef] [PubMed]
- Hayes, C.; Myers, R.; Morris, N.; Gerhart, N.; Yett, S.; Lipsitz, A. Impact near the hip dominates fracture risk in elderly nursing home residents who fall. Calcif. Tissue Int. 1993, 52, 192–198. [Google Scholar] [CrossRef] [PubMed]
- Jager, E.; Weiss, B.; Coben, H.; Pepe, E. Traumatic brain injuries evaluated in U.S. emergency departments, 1992–1994. Acad. Emerg. Med. 2000, 7, 134–140. [Google Scholar] [CrossRef] [PubMed]
- Stevens, A.; Corso, S.; Finkelstein, A.; Miller, R. The costs of fatal and nonfatal falls among older adults. Injury Prev. 2006, 12, 290–295. [Google Scholar] [CrossRef] [PubMed]
- Vellas, J.; Wayne, J.; Romero, J.; Baumgartner, N.; Garry, J. Fear of falling and restriction of mobility in elderly fallers. Age Ageing 1997, 26, 189–193. [Google Scholar] [CrossRef] [PubMed]
- Gillespie, D.; Robertson, C.; Gillespie, J.; Sherrington, C.; Gates, S.; Clemson, M.; Lamb, E. Interventions for preventing falls in older people living in the community. Cochrane Database Syst. Rev. 2009, 2. [Google Scholar] [CrossRef]
- Chaudhuri, S.; Thompson, H.; Demiris, G. Fall detection devices and their use with older adults: A systematic review. J. Geriatr. Phys. Ther. 2014, 37, 178–196. [Google Scholar] [CrossRef] [PubMed]
- Porter, E.J. Wearing and using personal emergency response system buttons. J. Gerontol. Nurs. 2005, 31, 26–33. [Google Scholar] [CrossRef] [PubMed]
- Fleming, J.; Brayne, C. Inability to get up after falling, subsequent time on floor, and summoning help: Prospective cohort study in people over 90. BMJ 2008, 337. [Google Scholar] [CrossRef] [PubMed]
- Bourke, K.; O’Brien, V.; Lyons, M. Evaluation of a threshold-based tri-axial accelerometer fall detection algorithm. Gait Posture 2007, 26, 194–199. [Google Scholar] [CrossRef] [PubMed]
- Bourke, K.; van de Ven, W.; Chaya, E.; OLaighin, M.; Nelson, J. Testing of a long-term fall detection system incorporated into a custom vest for the elderly. In Proceedings of the IEEE Engineering in Medicine and Biology Society, Vancouver, BC, Canada, 20–25 August 2008; pp. 2844–2847.
- Kangas, M.; Vikman, I.; Wiklander, J.; Lindgren, P.; Nyberg, L.; Jämsä, T. Sensitivity and specificity of fall detection in people aged 40 years and over. Gait Posture 2009, 29, 571–574. [Google Scholar] [CrossRef] [PubMed]
- Bourke, K.; van de Ven, P.; Gamble, M.; O’Connor, R.; Murphy, K.; Bogan, E.; McQuade, E.; Finucane, P.; Olaighin, G.; Nelson, J. Assessment of waist-worn tri-axial accelerometer based fall-detection algorithms using continuous unsupervised activities. In Proceedings of the IEEE Engineering in Medicine and Biology Society, Buenos Aires, Argentina, 1–4 September 2010.
- Bloch, F.; Gautier, V.; Noury, N.; Lundy, E.; Poujaud, J.; Claessens, E.; Rigaud, S. Evaluation under real-life conditions of a stand-alone fall detector for the elderly subjects. Ann. Phys. Rehabil. Med. 2011, 54, 391–398. [Google Scholar] [CrossRef] [PubMed]
- Igual, R.; Medrano, C.; Plaza, I. Challenges, issues and trends in fall detection systems. BiolMed. Eng. Online 2013, 12. [Google Scholar] [CrossRef] [PubMed]
- Belshaw, M.; Taati, B.; Giesbercht, D.; Mihailidis, A. Intelligent Vision-Based Fall Detection System: Preliminary Results from a Real World Deployment. In Proceedings of the RESNA/ICTA 2011: Advancing Rehabilitation Technologies for an Aging Society, Toronto, ON, Canada, 5–8 June 2011.
- Belshaw, M.; Taati, B.; Snoek, J.; Mihailidis, A. Towards a single sensor passive solution for automated fall detection. In Proceedings of the IEEE Engineering in Medicine and Biology Society, Boston, MA, USA, 30 August–3 September 2011; pp. 1773–1776.
- Sixsmith, A.; Johnson, N. A smart sensor to detect the falls of the elderly. IEEE Pervasive Comput. 2004, 3, 42–47. [Google Scholar] [CrossRef]
- Li, Y.; Zeng, Z.; Popescu, M.; Ho, K.C. Acoustic fall detection using a circular microphone array. In Proceedings of the IEEE Engineering in Medicine and Biology Society, Buenos Aires, Argentina, 31 August–4 September 2010.
- Popescu, M.; Li, Y.; Skubic, M.; Rantz, M. An acoustic fall detector system that uses sound height information to reduce the false alarm rate. In Proceedings of the IEEE Engineering in Medicine and Biology Society, Vancouver, BC, Canada, 20–25 August 2008.
- Alwan, M.; Rajendran, P.J.; Kell, S.; Mack, D.; Dalal, S.; Wolfe, M.; Felder, R. A Smart and Passive Floor-Vibration Based Fall Detector for Elderly. In Proceedings of the 2nd International Conference on Information & Communication Technologies: From Theory to Applications (ICTTA), Omayyad Palace Damascus, Syria, 24–28 April 2006.
- Yu, X. Approaches and principles of fall detection for elderly and patient. In Proceedings of the IEEE 10th International Conference on e-Health Networking Applications and Services (HealthCom’08), Singapore, 7–9 July 2008; pp. 42–47.
- Habib, M.A.; Mohktar, M.S.; Kamaruzzaman, S.B.; Lim, K.S.; Pin, T.M.; Ibrahim, F. Smartphone-based solutions for fall detection and prevention: Challenges and open issues. Sensors 2014, 14, 7181–7208. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.; Robinovitch, S.; Park, E. Inertial sensing-based pre-impact detection of falls involving near-fall scenarios. IEEE Trans. Neural Syst. Rehabil. Eng. 2015, 23, 258–266. [Google Scholar] [CrossRef] [PubMed]
- Bourke, A.; Lyons, G. A threshold-based fall-detection algorithm using a bi-axial gyroscope sensor. Med. Eng. Phys. 2008, 30, 84–90. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Kwong, K.; Chang, D.; Luk, J.; Bajcsy, R. Wearable sensors for reliable fall detection. In Proceedings of the 27th Annual International Conference in EMBS, Shanghai, China, 1–4 September 2005.
- Li, Q.; Stankovic, J.; Hanson, M.; Barth, A.; Lach, J.; Zhou, G. Accurate fast fall detection using gyroscopes and accelerometer-derived posture information. In Proceedings of the 2009 Sixth International Workshop on Wearable and Implantable Body Sensor Networks, Berkeley, CA, USA, 3–5 June 2009; pp. 138–143.
- Sposaro, F.; Tyson, G. iFall: An Android application for fall monitoring and response. In Proceedings of the Annual International Conference of the IEEE on Engineering in Medicine and Biology Society (EMBC), Minneapolis, MN, USA, 3–6 September 2009.
- Lopes, I.C.; Vaidya, B.; Rodrigues, J. SensorFall—An accelerometer based mobile application. In Proceedings of the 2nd International Conference on Computational Science and Its Applications, Jeju, Korea, 10–12 December 2009.
- Perry, J.; Kellog, S.; Vaidya, S.; Youn, J.-H.; Ali, H.; Sharif, H. Survey and evaluation of real-time fall detection approaches. In Proceedings of the 6th International Symposium on High-Capacity Optical Networks and Enabling Technologies (HONET), Alexandria, Egypt, 28–30 December 2009.
- Bourke, K.; O’Donovan, J.; OLaighin, M. Distinguishing falls from normal ADL using vertical velocity profiles. In Proceedings of the IEEE Engineering in Medicine and Biology Society, Lyon, France, 23–26 August 2007.
- Bourke, K.; O’Donovan, J.; Olaighin, M. The identification of vertical velocity profiles using an inertial sensor to investigate pre-impact detection of falls. Med. Eng. Phys. 2008, 30, 937–946. [Google Scholar] [CrossRef] [PubMed]
- Zhang, T.; Wang, J.; Xu, L.; Liu, P. Fall detection by wearable sensor and one-class SVM algorithm. In Proceedings of the Intelligent Computing in Signal Processing and Pattern Recognition, Kunming, China, 16–19 August 2006; Springer: Berlin/Heidelberg, Germany, 2006; Volume 345, pp. 858–863. [Google Scholar]
- Lester, J.; Choudhury, T.; Kern, N.; Borriello, G.; Hannaford, B. A Hybrid Discriminative/Generative Approach for Modeling Human Activities; IJCAI, Professional Book Center: Edinburgh, Scotland, 2005; pp. 766–772. [Google Scholar]
- Tong, L.; Song, Q.; Ge, Y.; Liu, M. HMM-based human fall detection and prediction method using tri-axial accelerometer. IEEE Sens. J. 2013, 13, 1849–1856. [Google Scholar] [CrossRef]
- Florentino-Liano, B.; O’Mahony, N.; Artes-Rodrıguez, A. Hierarchical dynamic model for human daily activity recognition. In Proceedings of the Bio-Inspired Systems and Signal Processing (BIOSIGNALS), Vilamoura, Portugal, 1–4 February 2012; pp. 61–68.
- Florentino-Liano, B.; O’Mahony, N.; Artes-Rodrıguez, A. Human activity recognition using inertial sensors with invariance to sensor orientation. In Proceedings of the 3rd IEEE Workshop on Cognitive Information Processing (CIP), Baiona, Spain, 28–30 May 2012.
- Yin, J.; Yang, Q.; Pan, J. Sensor-based abnormal human-activity detection. IEEE Trans. Knowledge Data Eng. 2008, 20, 1082–1090. [Google Scholar] [CrossRef]
- Yu, M.; Naqvi, S.; Rhuma, A.; Chambers, J. One class boundary method classifiers for application in a video-based fall detection system. Comput. Vis. 2012, 6, 90–100. [Google Scholar] [CrossRef]
- Han, C.; Wu, K.; Wang, Y.; Ni, L. Wifall: Device-free fall detection by wireless networks. In Proceedings of the IEEE Transactions on Mobile Computing (INFOCOM), Toronto, ON, Canada, 27 April–2 May 2014; pp. 271–279.
- Zhang, D.; Wang, H.; Wang, Y.; Ma, J. Anti-fall: A non-intrusive and real-time fall detector leveraging CSI from commodity WiFi devices. In Proceedings of the International Conference on Smart Homes and Health Telematics, Geneva, Switzerland, 10–12 June 2015; pp. 181–193.
- Khan, M.; Yu, M.; Feng, P.; Wang, L.; Chambers, J. An unsupervised acoustic fall detection system using source separation for sound interference suppression. Signal Process. 2015, 110, 199–210. [Google Scholar] [CrossRef]
- Parisi, G.I.; Wermter, S. Hierarchical SOM-based detection of novel behavior for 3D human tracking. In Proceedings of the International Joint Conference on Neural Networks (IJCNN), Dallas, TX, USA, 4–9 August 2013; pp. 1–8.
- Noury, N.; Fleury, A.; Rumeau, P.; Bourke, A.K.; Laighin, G.O.; Rialle, V.; Lundy, J.E. Fall detection—Principles and methods. In Proceedings of the IEEE Engineering in Medicine and Biology Society, Lyon, France, 23–26 August 2007.
- Auvinet, E.; Reveret, L.; St-Arnaud, A.; Rousseau, J.; Meunier, J. Fall detection using multiple cameras. In Proceedings of the Engineering in Medicine and Biology Society, Vancouver, BC, Canada, 20–25 August 2008.
- Zigel, Y.; Litvak, D.; Gannot, I. A method for automatic fall detection of elderly people using floor vibrations and sound—Proof of concept on human mimicking doll falls. IEEE Trans. Biomed. Eng. 2009, 56, 2858–2867. [Google Scholar] [CrossRef] [PubMed]
- Horton, K. Falls in older people: The place of telemonitoring in rehabilitation. Rehabil. Res. Dev. 2008, 45, 1183–1194. [Google Scholar] [CrossRef]
- Brownsell, S.; Hawley, M. Fall detectors: Do they work or reduce the fear of falling? Hous. Care Support 2004, 7, 18–24. [Google Scholar] [CrossRef]
- Kulkarni, A.U. Intelligent Pill Box. U.S. Patent 7,877,268, 25 January 2011. [Google Scholar]
- De Oliveira, R.; Cherubini, M.; Nuria, O. MoviPill: Improving medication compliance for elders using a mobile persuasive social game. In Proceedings of the 12th ACM International Conference on Ubiquitous Computing, Copenhagen, Denmark, 26–29 September 2010.
- MacLaughlin, E.J.; Raehl, C.L.; Treadway, A.K.; Sterling, T.L.; Zoller, D.P.; Bond, C.A. Assessing medication adherence in the elderly. Drugs Aging 2005, 22, 231–255. [Google Scholar] [CrossRef] [PubMed]
- Moisan, J.; Gaudet, M.; Grégoire, J.-P.; Bouchard, R. Non-compliance with drug treatment and reading difficulties with regard to prescription labeling among seniors. Gerontology 2002, 48, 44–51. [Google Scholar] [CrossRef] [PubMed]
- (SAMHSA) Substance Abuse and Mental Health Services Administration and Administration on Aging (AoA); Behavioral Health Technical Assistance Center: Rockville, MD, USA, 2012.
- Yamamoto, Y.; Huang, R.; Ma, J. Medicine management and medicine taking assistance system for supporting elderly care at home. In Proceedings of the 2nd IEEE International Symposium on Aware Computing, Tainan, Taiwan, 1–4 November 2010.
- Simoni-Wastila, L.; Yang, K. Psychoactive drug abuse in older adults. Am. J. Geriatr. Pharmacother. 2006, 4, 380–394. [Google Scholar] [CrossRef] [PubMed]
- Center for Substance Abuse Treatment. Substance Abuse among Older Adults. Treatment Improvement Protocol; Substance Abuse and Mental Health Services Administration: Rockville, MD, USA, 1998.
- National Institute on Alcohol Abuse and Alcoholism. Diagnostic Criteria for Alcohol Abuse; Alcohol Alert: Washington, DC, USA, 1995.
- Cutler, M.; Everett, W. Thinking outside the pillbox—Medication adherence as a priority for health care reform. N. Engl. J. Med. 2010, 362, 1553–1555. [Google Scholar] [CrossRef] [PubMed]
- Maddigan, L.; Farris, B.; Keating, N.; Wiens, A.; Johnson, A. Predictors of older adults’ capacity for medication management in a self-medication program: A retrospective chart review. J. Aging Health 2003, 15, 332–352. [Google Scholar] [CrossRef] [PubMed]
- Nikolaus, T.; Kruse, W.; Bach, M.; Specht-Leible, N.; Oster, P.; Schlierf, G. Elderly patients’ problems with medication. An in-hospital and follow-up study. Eur. J. Clin. Pharmacol. 1996, 49, 255–259. [Google Scholar] [CrossRef] [PubMed]
- Mowerson, A. Helping patients with vision impairment adhere to a medication regime. J. Gerontol. Nurs. 2002, 28, 15–18. [Google Scholar] [CrossRef] [PubMed]
- DiMatteo, R. Social support and patient adherence to medical treatment: A meta-analysis. Health Psychol. 2004, 23, 207–218. [Google Scholar] [CrossRef] [PubMed]
- Agoulmine, N.; Deen, M.J.; Lee, J.S.; Meyyappan, M. U-health smart home. IEEE Nanotechnol. Mag. 2011, 5, 6–11. [Google Scholar] [CrossRef]
- Yared, R.; Mallat, H.K.; Abdulrazak, B. Ambient Technology to Support Elderly People in Outdoor Risk Situations. In Information and Communication Technologies for Ageing Well and e-Health, Proceedings of the 1st International Conference on Information and Communication Technologies for Ageing Well and e-Health (ICT4AgeingWell), Lisbon, Portugal, 20–22 May 2015; Helfert, M., Holzinger, A., Ziefle, M., Fred, A., O’Donoghue, J., Röcker, C., Eds.; Communications in Computer and Information Science. Springer: Berlin/Heidelberg, Germany, 2015; Volume 578, pp. 35–36. [Google Scholar]
- Mallat, H.K.; Yared, R.; Abdulrazak, B. Assistive Technology for Risks Affecting Elderly People in Outdoor Environment. In Proceedings of the 1st International Conference on Information and Communication Technologies for Ageing Well and e-Health (ICT4AgeingWell), Lisbon, Portugal, 20–22 May 2015; pp. 5–16.
- Hayes, T.L.; Hunt, J.M.; Adami, A.; Kaye, J.A. An electronic pillbox for continuous monitoring of medication adherence. In Proceedings of the 28th Annual IEEE Conference on Engineering in Medicine and Biology Society, New York, NY, USA, 31 August–3 September 2006.
- Sterns, A.; Hughes, J.; Masstandrea, N.; Smith, J. Medication Event Monitoring System. U.S. Patent 14,357,052, 12 November 2012. [Google Scholar]
- Cramer, J.A.; Mattson, R.H.; Prevey, M.L.; Scheyer, R.D.; Ouellette, V.L. How often is medication taken as prescribed? A novel assessment technique. JAMA 1989, 261, 3273–3277. [Google Scholar] [CrossRef] [PubMed]
- Keram, S.; Williams, M.E. Quantifying the ease or difficulty older persons experience in opening medication containers. J. Am. Geriatr. Soc. 1988, 36, 198–201. [Google Scholar] [CrossRef] [PubMed]
- Atkin, P.A.; Finnegan, T.P.; Ogle, S.J.; Shenfield, G.M. Functional ability of patients to manage medication packaging: A survey of geriatric inpatients. Age Ageing 1994, 23, 113–116. [Google Scholar] [CrossRef] [PubMed]
- Branin, J.J. The role of memory strategies in medication adherence among the elderly. Home Health Care Serv. Q. 2001, 20, 1–16. [Google Scholar] [CrossRef] [PubMed]
- DiCarlo, L.A. Role for direct electronic verification of pharmaceutical ingestion in pharmaceutical development. Contemp. Clin. Trials 2012, 33, 593–600. [Google Scholar] [CrossRef] [PubMed]
- Mobile Medication Therapy Management System Wins $1M NIH Grant. Available online: http://mobihealthnews.com/18496/mobile-medication-therapy-management-system-wins-1m-nih-grant/ (accessed on 8 October 2016).
- Wan, D. Magic Medicine Cabinet: A situated portal for consumer healthcare. In Proceedings of the International Symposium on Handheld and Ubiquitous Computing HUC’99, Karlsruhe, Germany, 27–29 September 1999.
- Fishkin, K.; Wang, M.; Borriello, G. A ubiquitous system for medication monitoring. In Proceedings of the Second International Conference on Pervasive Computing, Vienna, Austria, 21–23 April 2004.
- Vinjumur, J.K.; Becker, E.; Ferdous, S.; Galatas, G.; Makedon, F. Web based medicine intake tracking application. In Proceedings of the 3rd ACM International Conference on Pervasive Technologies Related to Assistive Environments, Samos, Greece, 23–25 June 2010.
- Marek, K.D.; Stetzer, F.; Ryan, P.A.; Bub, L.D.; Adams, S.J.; Schlidt, A.; Lancaster, R.; O’Brien, A.M. Nurse care coordination and technology effects on health status of frail elderly via enhanced self-management of medication: Randomized clinical trial to test efficacy. Nurs. Res. 2013, 62, 269–278. [Google Scholar] [CrossRef] [PubMed]
- Sherrard, H.; Struthers, C.; Kearns, S.A.; Wells, G.; Chen, L.; Mesana, T. Using technology to create a medication safety net for cardiac surgery patients: A nurse-led randomized control trial. Can. J. Cardiovasc. Nurs. 2009, 19, 9–15. [Google Scholar] [PubMed]
- Naditz, A. Medication compliance—Helping patients through technology: Modern “smart” pillboxes keep memory-short patients on their medical regimen. Telemed. J. e-Health 2008, 14, 875–880. [Google Scholar] [CrossRef] [PubMed]
- Buckwalter, K.C.; Wakefield, B.J.; Hanna, B.; Lehmann, J. New technology for medication adherence: Electronically managed medication dispensing system. J. Gerontol. Nurs. 2004, 30, 5–8. [Google Scholar] [CrossRef] [PubMed]
- Reminders, e-pill Medication e-pill Automatic Pill Dispensers 2011. Available online: http://www.epill.com/dispenser.html (accessed on 8 October 2016).
- Russell, C.L.; Conn, V.S.; Jantarakupt, P. Older adult medication compliance: Integrated review of randomized controlled trials. Am. J. Health Behav. 2006, 30, 635–650. [Google Scholar] [CrossRef]
- Campbell, N.L.; Boustani, M.A.; Skopelja, E.N.; Gao, S.; Unverzagt, F.W.; Murray, M.D. Medication adherence in older adults with cognitive impairment: A systematic evidence-based review. Am. J. Geriatr. Pharmacother. 2012, 10, 165–177. [Google Scholar] [CrossRef] [PubMed]
- Mehaffey, J.R.; Bert, J.L. Fire Protection Report; U.S. Department of Health and Human Services, National Institute for Occupational Safety and Health (NIOSH), Centers for Disease Control and Prevention: Washington, DC, USA, 1997.
- Karter, M. National Fire Protection Association (NFPA)’s Latest Fire Loss Figures. NFPA J. 1996, 52–59. [Google Scholar]
- Runyan, C.W.; Johnson, R.M.; Yang, J.; Waller, A.E.; Perkis, D.; Marshall, S.W.; McGee, K.S. Risk and protective factors for fires, burns, and carbon monoxide poisoning in US households. Am. J. Prev. Med. 2005, 28, 102–108. [Google Scholar] [CrossRef] [PubMed]
- Ahrens, M. Home Smoke Alarms: The Data as Context for Decision. Fire Technol. 2008, 44, 313–327. [Google Scholar] [CrossRef]
- Office of the Fire Marshal. Reducing Stovetop Fire; Fire Marshal’s Public: Brockville, ON, Canada, 2009. [Google Scholar]
- Lushaka, B.; Zalok, E. Development of a sensing device to reduce the risk from kitchen fires. Fire Technol. J. 2014, 50, 791–803. [Google Scholar] [CrossRef]
- Hall, J.R. Home Cooking Fire Patterns and Trends; National Fire Incident Reporting System (NFIRS): Quincy, MA, USA, 2006.
- Abdulrazak, B.; Yared, R.; Tessier, T.; Mabilleau, P. Toward pervasive computing system to enhance safety of ageing people in smart kitchen. In Proceedings of the 1st International Conference of Information and Communication Technologies for Ageing Well and e-Health (ICT4AgeingWell2015), Lisbon, Portugal, 20–22 May 2015.
- Yared, R.; Abdulrazak, B. Toward Context-Aware Smart Oven to Prevent Cooking Risks in Kitchen of Elderly People; Springer: Berlin/Heidelberg, Germany, 2015; pp. 57–77. [Google Scholar]
- U.S. Fire Administration. Let’s Retire Fire: A Factsheet for Older Americans; Department of Homeland Security: Emmitsburg, MD, USA, 2006.
- Warda, L.; Tenenbein, M.; Moffatt, M.E. House fire injury prevention update. Part I. A review of risk factors for fatal and non-fatal house fire injury. Injury Prev. 1999, 5, 145–150. [Google Scholar] [CrossRef]
- Grant, E.J. Preventing burns in the elderly: A guide for home healthcare professionals. Home Healthc. Nurse 2013, 31, 561–573. [Google Scholar] [CrossRef] [PubMed]
- Stockhausen, A.L.; Katcher, M.L. Burn injury from products in the home: Prevention and counseling. Wis. Med. J. 2001, 100, 39–44. [Google Scholar]
- American Academy of Pediatrics. Fires and burns. In Injury Prevention and Control for Children and Youth, 3rd ed.; Widome, M.D., Ed.; American Academy of Pediatrics, Committee on Injury and Poison Prevention: Elk Grove Village, IL, USA, 1997. [Google Scholar]
- Burn Prevention Fact Sheet/Older Adult Educator’s Guide; American Burn Association: Chicago, IL, USA, 2012.
- Runyan, C.W.; Casteel, C.; Perkis, D. Unintentional injuries in the home in the United States. Part I: Mortality. Am. J. Prev. Med. 2005, 28, 73–79. [Google Scholar] [CrossRef] [PubMed]
- Harwood, B. Common products that cause uncommonly severe burn injuries. NFPA J. 1995, 90, 79–83. [Google Scholar]
- Macarthur, C. Evaluation of Safe Kids Week 2001: Prevention of scald and burn injuries in young children. Injury Prev. 2003, 9, 112–116. [Google Scholar] [CrossRef]
- Rivara, F.P. Burns: The importance of prevention. Injury Prev. 2000, 6, 243–244. [Google Scholar] [CrossRef]
- Stone, M.; Evans, A.J. The continuing risk of domestic hot water scalds to the elderly. Burns 2000, 26, 347–350. [Google Scholar] [CrossRef]
- Weaver, A.M.; Himel, H.N.; Edlich, R.F. Immersion scald burns: Strategies for prevention. J. Emerg. Med. 1993, 11, 397–402. [Google Scholar] [CrossRef]
- Shields, W.C.; Perry, E.C.; Szanton, S.L.; Andrews, M.R.; Stepnitz, R.L.; McDonald, E.M.; Gielen, A.C. Knowledge and injury prevention practices in homes of older adults. Geriatr. Nurs. 2013, 34, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Bishai, D.; Lee, S. Heightened risk of fire deaths among older African Americans and Native Americans. Public Health Rep. 2010, 125, 406–413. [Google Scholar] [PubMed]
- Ault, K.L. Estimates of Non-Fire Carbon Monoxide Poisoning Deaths and Injuries; U.S. Consumer Product Safety Commission: Washington, DC, USA, 1997.
- Centers for Disease Control and Prevention. Use of unvented residential heating appliances—United States, 1988–1994. MMWR Morb. Mortal. Wkly. Rep. 1997, 46, 1221–1224. [Google Scholar]
- Centers for Disease Control and Prevention. Unintentional carbon monoxide poisoning in residential settings—Connecticut, November 1993–March 1994. MMWR Morb. Mortal. Wkly. Rep. 1995, 44, 765–767. [Google Scholar]
- Daley, W.R.; Smith, A.; Paz-Argandona, E.; Malilay, J.; McGeehin, M. An outbreak of carbon monoxide poisoning after a major ice storm in Maine. J. Emerg. Med. 2000, 18, 87–93. [Google Scholar] [CrossRef]
- Girman, J.R.; Chang, Y.L.; Hayward, S.B.; Liu, K.S. Causes of unintentional deaths from carbon monoxide poisonings in California. West. J. Med. 1998, 168, 158–165. [Google Scholar] [PubMed]
- Bizovi, K.E.; Leikin, J.B.; Hryhorczuk, D.O.; Frateschi, L.J. Night of the sirens: Analysis of carbon monoxide-detector experience in suburban Chicago. Ann. Emerg. Med. 1998, 31, 737–740. [Google Scholar] [CrossRef]
- Meredith, T.; Vale, A. Carbon monoxide poisoning. Br. Med. J. 1988, 296, 77–79. [Google Scholar] [CrossRef]
- Kelly, J.S.; Sophocleus, G.J. Retinal hemorrhages in subacute carbon monoxide poisoning. JAMA 1978, 239, 1515–1517. [Google Scholar] [CrossRef]
- Stewart, R.D.; Hake, C.L. Paint-remover hazard. JAMA 1976, 235, 398–401. [Google Scholar] [CrossRef] [PubMed]
- Stewart, R.D.; Baretta, E.D.; Platte, L.R.; Stewart, E.B.; Kalbfleisch, J.H.; Van Yserloo, B.; Rimm, A.A. Carboxyhemoglobin levels in American blood donors. JAMA 1974, 229, 1187–1195. [Google Scholar] [CrossRef] [PubMed]
- Harvey, P.A.; Sacks, J.J.; Ryan, G.W.; Bender, P.F. Residential smoke alarms and fire escape plans. Public Health Rep. 1998, 113, 459–464. [Google Scholar] [PubMed]
- Mayer, M.; LeClere, F.B. Injury prevention measures in households with children in the United States. Adv. Data 1994, 250, 1–16. [Google Scholar] [PubMed]
- Centers for Disease Control and Prevention. Deaths resulting from residential fires and the prevalence of smoke alarms—United States, 1991–1995. MMWR Morb. Mortal. Wkly. Rep. 1998, 47, 803–806. [Google Scholar]
- Doman, K.; Kuai, Y.; Takahashi, T.; Ide, I.; Murase, H. Video Cooking: Towards the Synthesis of Multimedia Cooking Recipes. In Advances in Multimedia Modeling, Proceedings of the 17th International Multimedia Modeling Conference, MMM 2011, Taipei, Taiwan, 5–7 January 2011; Lee, K.-T., Tsai, W.-H., Liao, H.-Y.M., Chen, T., Hsieh, J.-W., Tseng, C.-C., Eds.; Lecture Notes in Computer Science. Springer: Berlin/Heidelberg, Germany, 2011; Volume 6524, pp. 135–145. [Google Scholar]
- Li, Y.; Asghar, Z.; Pulii, P. Visually-aided smart kitchen environment for senior citizens suffering from dementia. In Proceedings of the IEEE International Joint Conference on Awareness Science and Technology and Ubi-Media Computing (iCAST-UMEDIA), Aizuwakamatsu, Japan, 2–4 November 2013.
- Sanchez, A.; Burnell, L. Intelligent and Adaptive Educational-Learning Systems. In Smart Innovation, Systems and Technologies; Springer: Berlin/Heidelberg, Germany, 2013; Volume 17, pp. 293–314. [Google Scholar]
- Alwan, M.; Dalal, S.; Mack, D.; Kell, B.; Turner, J. Leachtenauer and Felder. Impact of monitoring technology in assisted living: Outcome pilot. IEEE Trans. Inf. Technol. Biomed. 2006, 10, 192–198. [Google Scholar] [CrossRef] [PubMed]
- Wai, A.; Shanthini, D.; Biswas, J.; Panda, S. Pervasive intelligence system to enable safety and assistance in kitchen for home-alone elderly. In Toward Useful Services for Elderly and People with Disabilities; Springer: Berlin/Heidelberg, Germany, 2011; pp. 276–280. [Google Scholar]
- Yuan, M.Y.; Green, J.R.; Goubran, R. Thermal imaging for assisted living at home: Improving kitchen safety. J. Med. Biol. Eng. 2012, 33, 380–387. [Google Scholar] [CrossRef]
- Nagashima, T.; Mammoto, A.; Yamauchi, Y.; Watanabe, K.; Mizobuchi, M. Optimization of sensitivity characteristics of photoelectric smoke detector to various smokes. Fire Saf. Sci. 1988, 3, 319–334. [Google Scholar]
- Chen, S.; Bao, H.; Zeng, X.; Yang, Y. A fire detecting method based on multi-sensor data fusion. In Proceedings of the IEEE International Conference on Systems, Man and Cybernetics, Washington, DC, USA, 5–8 October 2003; Volume 4, pp. 3775–3780.
- Hagen, C.; Milke, A. The use of gaseous fire signatures as a mean to detect fires. Fire Saf. J. 2000, 34, 55–67. [Google Scholar] [CrossRef]
- Johnson, E. Study of Technology for Detecting Pre-Ignition Conditions of Cooking-Related Fires Associated with Electric and Gas Ranges and Cooktops; Technical Report; US Department of Commerce, Technology Administration, National Institute of Standards and Technology: Gaithersburg, MD, USA, 1998.
- Milke, A.; McAvoy, J. Analysis of signature patterns for discriminating fire detection with multiple sensors. Fire Technol. 1995, 31, 120–136. [Google Scholar] [CrossRef]
- Milke, A.; Hulcher, E.; Worrell, L.; Gottuk, T.; Williams, W. Investigation of Multi-Sensor algorithms for fire detection. Fire Technol. 2003, 39, 363–382. [Google Scholar] [CrossRef]
- Bashyal, S.; Venayagamoorthy, G.; Paudel, B. Embedded neural network for fire classification using an array of gas sensors. In Proceedings of the IEEE Symposium on Sensors Applications, Daegu, Korea, 12–14 February 2008.
- Charumporn, B.; Yoshioka, M.; Fujinaka, T.; Omatu, S. Early stage fire detection using reliable metal oxide gas sensors and artificial neural networks. In Proceedings of the International Joint Conference on Neural Networks, Portland, OR, USA, 20–24 July 2003; pp. 3185–3188.
- Yared, R.; Abdulrazak, B.; Tessier, T.; Mabilleau, P. Cooking risk analysis to enhance safety of elderly people in smart kitchen. In Proceedings of the 8th ACM International Conference on Pervasive Technologies Related to Assistive Environments (PETRA’2015), Corfu, Greece, 1–3 July 2015.
- Abdulrazak, B.; Yared, R. Prevent Cooking Risks in Kitchen of Elderly People: Adaptable Reasoning Engine Based on Fuzzy Logic for Smart Oven. In Proceedings of the IEEE International Conference on Computer and Information Technology; Ubiquitous Computing and Communications; Dependable, Autonomic and Secure Computing; Pervasive Intelligence and Computing (CIT/IUCC/DASC/PICOM), Liverpool, UK, 26–28 October 2015; pp. 2165–2172.
- Virtual Flame. Available online: http://www.samsung.com/uk/consumer/home-appliances/cooking-appliances/induction/NZ63J9770EK/EU (accessed on 8 October 2016).
- Carbon Monoxide Detectors Can Save Lives; U.S. Consumer Product Safety Commission: Washington, DC, USA, 2003.
- Yoon, S.S.; Macdonald, S.C.; Parrish, R.G. Deaths from unintentional carbon monoxide poisoning and potential for prevention with carbon monoxide detectors. JAMA 1998, 279, 685–687. [Google Scholar] [CrossRef] [PubMed]
- Clifton, J.C.; Leikin, J.B.; Hryhorczuk, D.O.; Krenzelok, E.P. Surveillance for carbon monoxide poisoning using a national media clipping service. Am. J. Emerg. Med. 2001, 19, 106–108. [Google Scholar] [CrossRef] [PubMed]
- Krenzelok, E.P.; Roth, R.; Full, R. Carbon monoxide ... the silent killer with an audible solution. Am. J. Emerg. Med. 1996, 14, 484–486. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Use of carbon monoxide alarms of prevent poisonings during a power outage—North Carolina, December 2002. MMWR Morb. Mortal. Wkly. Rep. 2004, 53, 189–192. [Google Scholar]
- Jain, P.C.; Kushwaha, R. Wireless gas sensor network for detection and monitoring of harmful gases in utility areas and industries. In Proceedings of the IEEE Sixth International Conference on Sensing Technology (ICST), West Bangal, India, 18–21 December 2012.
- Harper, A.; Croft-Baker, J. Carbon monoxide poisoning: Undetected by both patients and their doctors. Age Ageing 2004, 33, 105–109. [Google Scholar] [CrossRef] [PubMed]
- Helal, A.; Mokhtari, M.; Abdulrazak, B. The Engineering Handbook of Smart Technology for Aging, Disability, and Independence; Wiley: Hoboken, NJ, USA, 2008. [Google Scholar]
- Alspach, J.G. Loneliness and social isolation: Risk factors long overdue for surveillance. Crit. Care Nurse 2013, 33, 8–13. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.X.; Karp, A.; Winblad, B.; Fratiglioni, L. Late-life engagement in social and leisure activities is associated with a decreased risk of dementia: A longitudinal study from the Kungsholmen project. Am. J. Epidemiol. 2002, 155, 1081–1087. [Google Scholar] [CrossRef] [PubMed]
- Morrow-Howell, N.; Putnam, M.; Lee, Y.S.; Greenfield, J.C.; Inoue, M.; Chen, H. An investigation of activity profiles of older adults. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2014. [Google Scholar] [CrossRef] [PubMed]
- Phillips, E.M.; Schneider, J.C.; Mercer, G.R. Motivating elders to initiate and maintain exercise. Arch. Phys. Med. Rehabil. 2004, 85 (Suppl. 3), 52–57. [Google Scholar] [CrossRef]
- Krueger, K.R.; Wilson, R.S.; Kamenetsky, J.M.; Barnes, L.L.; Bienias, J.L.; Bennett, D.A. Social engagement and cognitive function in old age. Exp. Aging Res. 2009, 35, 45–60. [Google Scholar] [CrossRef] [PubMed]
- Unger, J.B.; McAvay, G.; Bruce, M.L.; Berkman, L.; Seeman, T. Variation in the Impact of Social Network Characteristics on Physical Functioning in Elderly Persons: MacArthur Studies of Successful Aging. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 1999, 54, S245–S251. [Google Scholar] [CrossRef]
- Araullo, J.; Potter, L.E. Promoting physical activity in seniors: Future opportunities with emerging technologies. In Proceedings of the 2016 ACM SIGMIS Conference on Computers and People Research, Washington, DC, USA, 2–4 June 2016; pp. 57–64.
- Lee, I.M.; Shiroma, E.J.; Lobelo, F.; Puska, P.; Blair, S.N.; Katzmarzyk, P.T.; Lancet Physical Activity Series Working Group. Effect of physical inactivity on major non-communicable diseases worldwide: An analysis of burden of disease and life expectancy. Lancet 2012, 380, 219–229. [Google Scholar] [CrossRef]
- Buttussi, F.; Chittaro, L. Smarter phones for healthier lifestyles: An adaptive fitness game. IEEE Pervasive Comput. 2010, 9, 51–57. [Google Scholar] [CrossRef]
- Madeira, R.N.; Costa, L.; Postolache, O. PhysioMate-Pervasive physical rehabilitation based on NUI and gamification. In Proceedings of the IEEE International Conference on Electrical and Power Engineering (EPE), Iasi, Romania, 16–18 October 2014; pp. 612–616.
- Barua, D.; Kay, J.; Paris, C. Viewing and controlling personal sensor data: What do users want? In Proceedings of the International Conference on Persuasive Technology, Sydney, Australia, 3–5 April 2013; Springer: Berlin/Heidelberg, Germany, 2013; pp. 15–26. [Google Scholar]
- Mitchell, L.; Ziviani, J.; Oftedal, S.; Boyd, R. The effect of virtual reality interventions on physical activity in children and adolescents with early brain injuries including cerebral palsy. Dev. Med. Child Neurol. 2012, 54, 667–671. [Google Scholar] [CrossRef] [PubMed]
- Bice, M.R.; Ball, J.W.; McClaran, S. Technology and physical activity motivation. Int. J. Sport Exerc. Psychol. 2015, 1–10. [Google Scholar] [CrossRef]
- Consolvo, S.; Everitt, K.; Smith, I.; Landay, J.A. Design requirements for technologies that encourage physical activity. In Proceedings of the SIGCHI Conference on Human Factors in Computing Systems, Montreal, QC, Canada, 24–27 April 2006; Volume 1, pp. 457–466.
- Stanley, K.G.; Livingston, I.; Bandurka, A.; Kapiszka, R.; Mandryk, R.L. “PiNiZoRo”: A GPS-based exercise game for families. In Proceedings of the International Academic Conference on the Future of Game Design and Technology (FuturePlay’10), Vancouver, BC, Canada, 6–7 May 2010; pp. 243–246.
- Brox, E.; Hernandez, J.E.G. Exergames for elderly: Social exergames to persuade seniors to increase physical activity. In Proceedings of the 5th IEEE International Conference on Pervasive Computing Technology for Healthcare, Dublin, Ireland, 23–26 May 2011; pp. 546–549.
- Albaina, I.M.; Visser, T.; van der Mast, C.A.P.G.; Vastenburg, M.H. Flowie: A persuasive virtual coach to motivate elderly individuals to walk. In Proceedings of the International ICST Conference on Pervasive Computing Technologies for Healthcare, London, UK, 1–3 April 2009; pp. 1–7.
- Ponce, V.; Deschamps, J.P.; Giroux, L.P.; Salehi, F.; Abdulrazak, B. QueFaire: Context-aware in-person social activity recommendation system for active aging. In Proceedings of the International Conference on Smart Homes and Health Telematics, Geneva, Switzerland, 10–12 June 2015; pp. 64–75.
- Romero, N.; Sturm, J.; Bekker, T.; de Valk, L.; Kruitwagen, S. Playful persuasion to support older adults’ social and physical activities. Interact. Comput. 2010, 22, 485–495. [Google Scholar] [CrossRef]
- Pasikowska, A.; Zaraki, A.; Lazzeri, N. A dialogue with a virtual imaginary interlocutor as a form of a psychological support for well-being. In Proceedings of the ACM International Conference on Multimedia, Interaction, Design and Innovation, Warsaw, Poland, 24–25 June 2013.
- Bentley, F.R.; Basapur, S.; Chowdhury, S.K. Promoting intergenerational communication through location-based asynchronous video communication. In Proceedings of the 13th ACM International Conference on Ubiquitous Computing, Beijing, China, 17–21 September 2011; pp. 31–40.
- MELCO project. Available online: www.melco.cs.ucy.ac.cy (accessed on 8 October 2016).
- Co-Living project. Available online: http://project-coliving.eu (accessed on 8 October 2016).
- Kaplan, A.M.; Haenlein, M. Users of the world, unite! The challenges and opportunities of social media. Bus. Horiz. 2010, 53, 59–68. [Google Scholar] [CrossRef]
- Buettner, D. The Blue Zones: Lessons for Living Longer from the People Who’ve Lived the Longest; National Geographic Society: Washington, DC, USA, 2009. [Google Scholar]
- Cohen-Mansfield, J.; Biddison, J. The scope and future trends of gerontechnology: Consumers’ opinions and literature survey. J. Technol. Hum. Serv. 2007, 25, 1–19. [Google Scholar] [CrossRef]
- Bolton, M. Older People, Technology and Community: The Potential of Technology to Help Older People Renew or Develop Social Contacts and to Actively Engage in Their Communities; Independent Age: London, UK, 2010. [Google Scholar]
- Vichitvanichphong, S.; Talaei-Khoei, A.; Kerr, D.; Ghapanchi, A.H. Assistive technologies for aged care: Supportive or empowering? Australas. J. Inf. Syst. 2014, 18. [Google Scholar] [CrossRef]
- Olphert, W.; Damodaran, L.; Balatsoukas, P.; Parkinson, C. Process requirements for building sustainable digital assistive technology for older people. J. Assis. Technol. 2009, 3, 4–13. [Google Scholar] [CrossRef]
- Nikou, S. Mobile technology and forgotten consumers: The young-elderly. Int. J. Consum. Stud. 2015, 39, 294–304. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Indoor Risk | # Reviewed Papers | # Selected Relevant Papers |
|---|---|---|
| Falls | 2630 | 200 |
| Wrong self-medication management (non-adherence, abuse and misuse) | 123 | 73 |
| Fire, burns and intoxication by gas/smoke | 84 | 32 |
| Inactivity | 812 | 35 |
| Wearable Devices | Non-Wearable Devices | |||
|---|---|---|---|---|
| Sufficient training data | Fixed threshold | [45] | Vision-based sensors/one class classification to distinguish fall from other activities. | [55] |
| Adaptive threshold | [44] | |||
| one-class SVM | [49] | |||
| Sequential classification (HMM) | [50,51] | Channel State Information (CSI) of WiFi signals | [56,57] | |
| Insufficient training data | Fall as abnormal activity | [54] | Acoustic sensors/one class SVM | [58] |
| Self-Organizing Maps | [59] | |||
| System | Monitoring and Detection of Medication Adherence | Interventions |
|---|---|---|
| SmartPillBox [65] | Pill count/weight. | Reminds patients to take the prescribed medications, and contacts caregivers through telephone to store the information of the patient’s compliance. |
| Electronic pillboxes, MedTracker [82] | Opening lid of a sub-compartment of the pillbox. | Not found in the paper. |
| Medication Event Monitoring Systems (MEMS) [83] | Associated sensing and recording devices. Displays information about the date and time of opening the vial. | It can be programmed to alert patients to take medication. A medication event monitoring system operates through the Internet, interconnecting and accommodating the transfer of information and data between a patient, a caregiver, and a pharmacist. |
| Ingestible sensor [88] | Ingestible sensor microchips embedded in medication transmit a signal when the medication is ingested or even metabolized. | The sensor communicates with the monitor that is worn on the user’s torso. The information stored in the monitor is sent wirelessly using Bluetooth to a mobile phone. |
| Magic Medicine Cabinet [90] | RFID to identify which medications were taken out of a cabinet, face recognition to identify who approached the device. | Reminds patients to take medication. |
| Medication management [70] | RFID- and wireless sensors–based medication taking monitoring; situation awareness and decision-making. The inference of reminding time is based on fuzzy logic. | Reminds an elderly person to take medications in a predicted time based on learning person’s habits and regular meal-taking schedule. |
| Web-based medicine intake tracking application [92] | RFID readers and tags, motion sensors, and a wireless sensor mote. | A Web-based caregiver module. |
| Automated medication dispensers [93,94,95,96], HealthWatch, Beep N Tel [67] | Dispense medication at preprogrammed intervals. | Voice-mail reminders, video-telephone reminders, automated telephone calls. Reminders are both audible (spoken words and tones) and visual (a flashing red strobe light). Caregiver/family member notification. |
| MoviPill [66] | Persuasive technology. | A mobile phone–based game that persuades elderly patients to be more adherent to their medication prescription by means of social competition. |
| System | Detection | Intervention |
|---|---|---|
| Fire/Smoke Alarms | Fire Signature | Sound Alert |
| Existing commercial cooking devices: e.g., StoveGuard, SafeCook and HomeSensor | Programmable cooking modes. Temperature of the oven surface. | Integrate LEDs to indicate that an oven surface is hot. Switch off an oven if there is no attendance after certain programmed time. |
| Lushaka et al. [106] | Existing smoke alarms to detect a potential fire risk. | Switching off oven power supply. |
| Doman et al. [136] | Reminds user to follow the correct steps when performing a cooking task through audio and video. No reaction if a risk occurs. | |
| Yahui et al. [137] | Visual surveillance system with multiple cameras enables to observe cooking conditions, and track user activities. | Not completely automatic, since it requires observer intervention (caregiver). |
| Sanchez et al. [138] | Detects rapid variations in temperature and smoke in the kitchen. | Sends a notification (with camera shots) to the fire department and caregivers. In addition, the system activates exhaust fans and a fire extinguishing suppression system. |
| Alwan et al. [139] Wai et al. [140] | Measure oven usage. Detect unsafe usage of the oven, the levels of abnormality in the kitchen. Both systems use embedded temperature sensors to measure the burner status, ultrasonic sensors to detect the presence of a pot and electric current sensors to detect the oven usage. | Switches off power. |
| Yuan et al. [141] | Thermal camera to detect dangerous situation. | Alerts user or caregiver when a dangerous situation occurs. |
| Yared et al. [107,108,151] | Preventive approach. Fire detection based on measurements of the concentration of the volatile organic compounds (VOC) and alcohol in the cooking smoke using appropriate selected VOC and alcohol sensors. Fire risk is determined by fuzzy logic reasoning. | Alerts user ubiquitously through audio and visual notification that a risk situation occurs. The interventions depend on the severity level of the detected risk. |
| Chen et al., Hagen et al., Johnson, Milke et al., [143,144,145,146,147] | Intelligent techniques and methods are used to fuse the data obtained by diverse sensors that lead to determine the fire probability. Multi-sensor data fusion detection technology based on fuzzy logic [143]. Fire detection by monitoring: carbon monoxide (CO), carbon dioxide (CO2), or volatile organic compounds (VOC). | No interventions. |
| Bashyal et al. [148] Charumporn et al. [149] | Classify fire situations according to their triggering reasons by monitoring: VOC, humidity, and ambient temperature. Fire detection algorithm based on neural networks. | No interventions. |
| Physical/Social Activities Promoting Representative Examples | |
|---|---|
| Video games | PiNiZoRo [175] |
| Exergaming | Social exergames to persuade seniors to increase physical activity [176] |
| Motivation | QueFaire [178], Flowie [177], Playful [179] |
| Communication between people (virtual or real) | Virtual imaginary interlocutor [180] Promoting Intergenerational communication through location-based asynchronous video communication [181] |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yared, R.; Abdulrazak, B. Ambient Technology to Assist Elderly People in Indoor Risks. Computers 2016, 5, 22. https://doi.org/10.3390/computers5040022
Yared R, Abdulrazak B. Ambient Technology to Assist Elderly People in Indoor Risks. Computers. 2016; 5(4):22. https://doi.org/10.3390/computers5040022
Chicago/Turabian StyleYared, Rami, and Bessam Abdulrazak. 2016. "Ambient Technology to Assist Elderly People in Indoor Risks" Computers 5, no. 4: 22. https://doi.org/10.3390/computers5040022
APA StyleYared, R., & Abdulrazak, B. (2016). Ambient Technology to Assist Elderly People in Indoor Risks. Computers, 5(4), 22. https://doi.org/10.3390/computers5040022