
The Clinical Outcomes and Safety of Sacituzumab Govitecan in Heavily Pretreated Metastatic Triple-Negative and HR+/HER2− Breast Cancer: A Multicenter Observational Study from Turkey

 , , , , , , and
, , , , , , and
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Intervention and Treatment Protocol
2.3. Outcome Measures
2.4. Statistical Analysis
2.5. Ethics Statement
3. Results
3.1. Baseline Characteristics
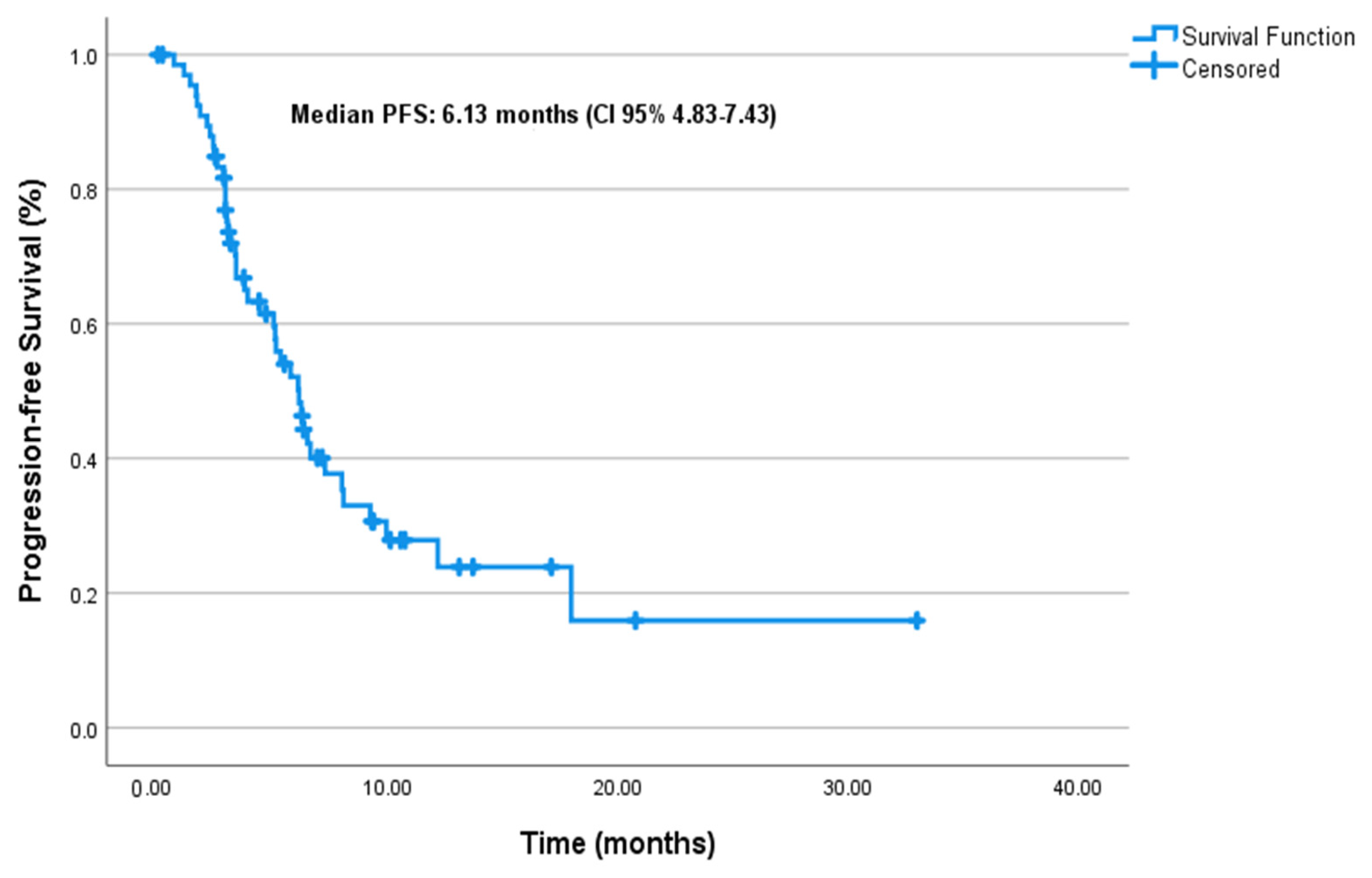
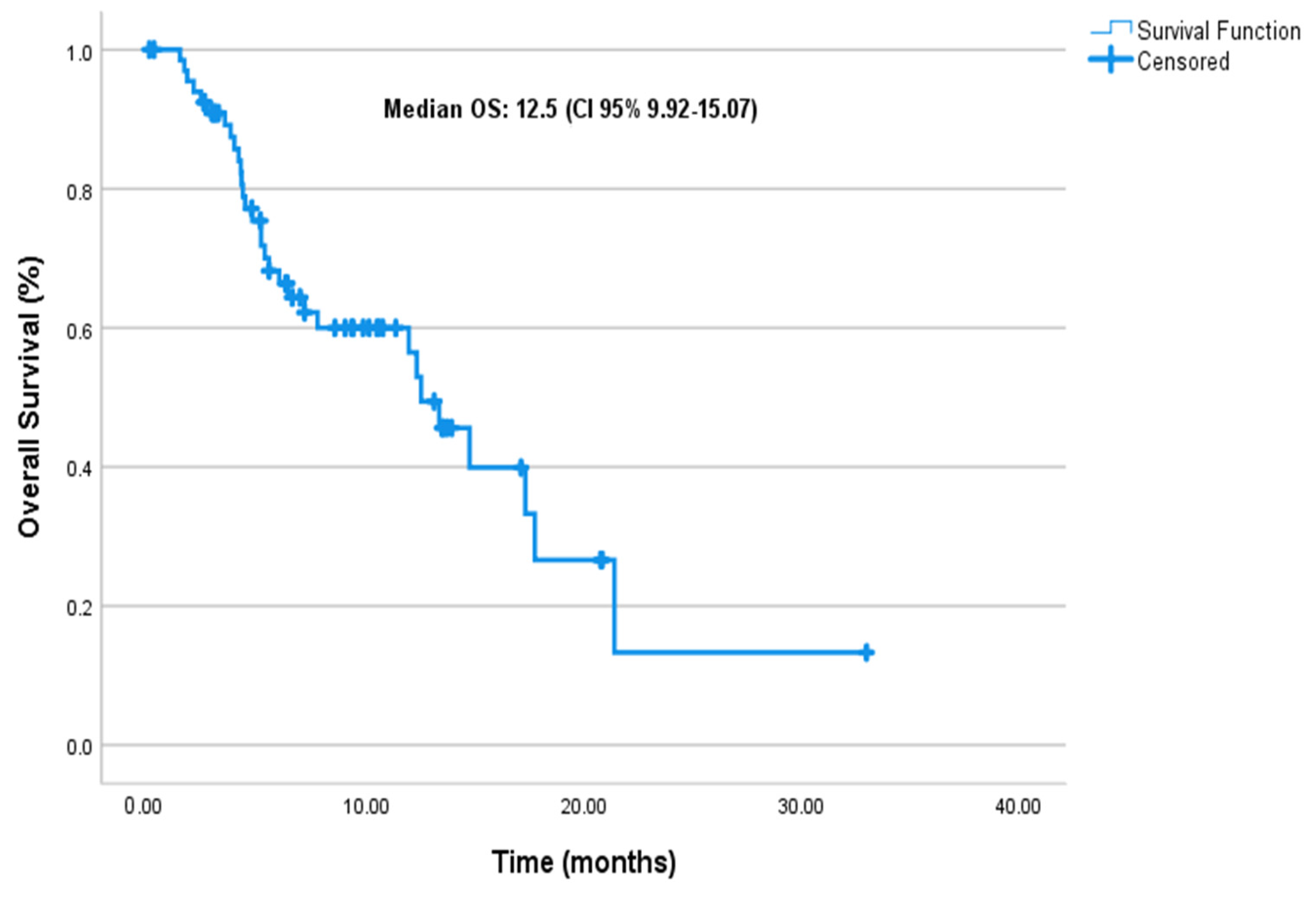
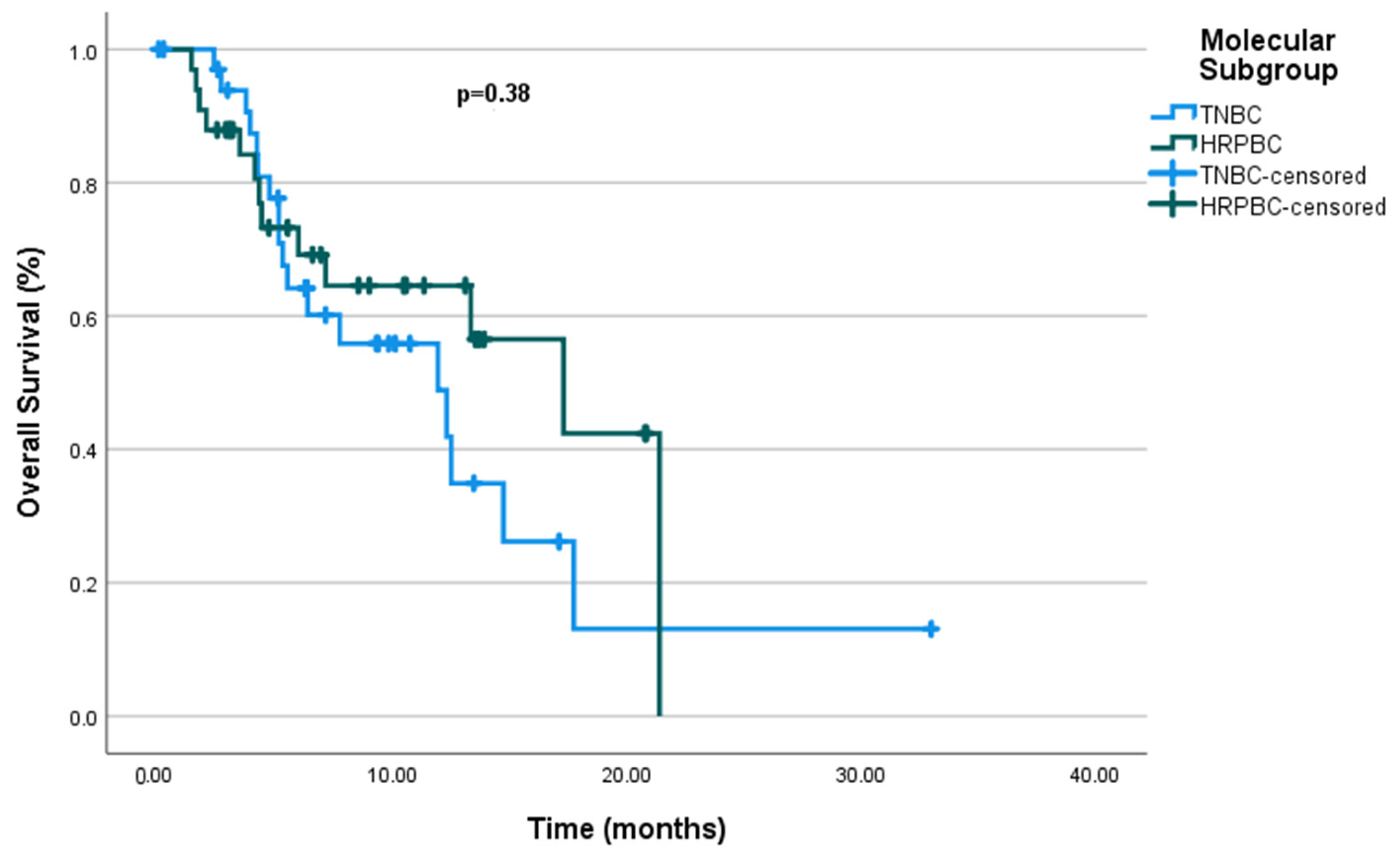
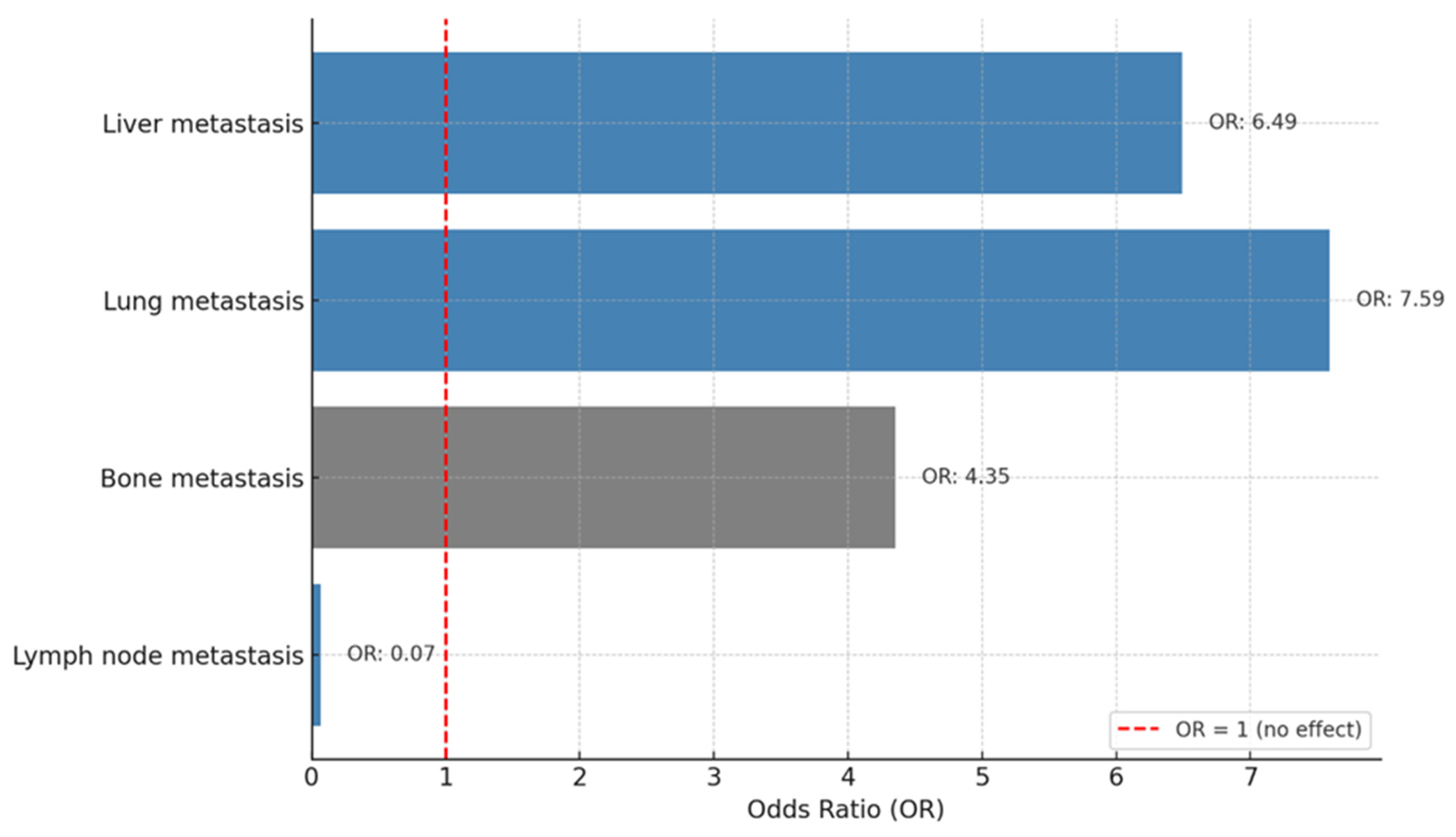
3.2. Clinical Outcomes
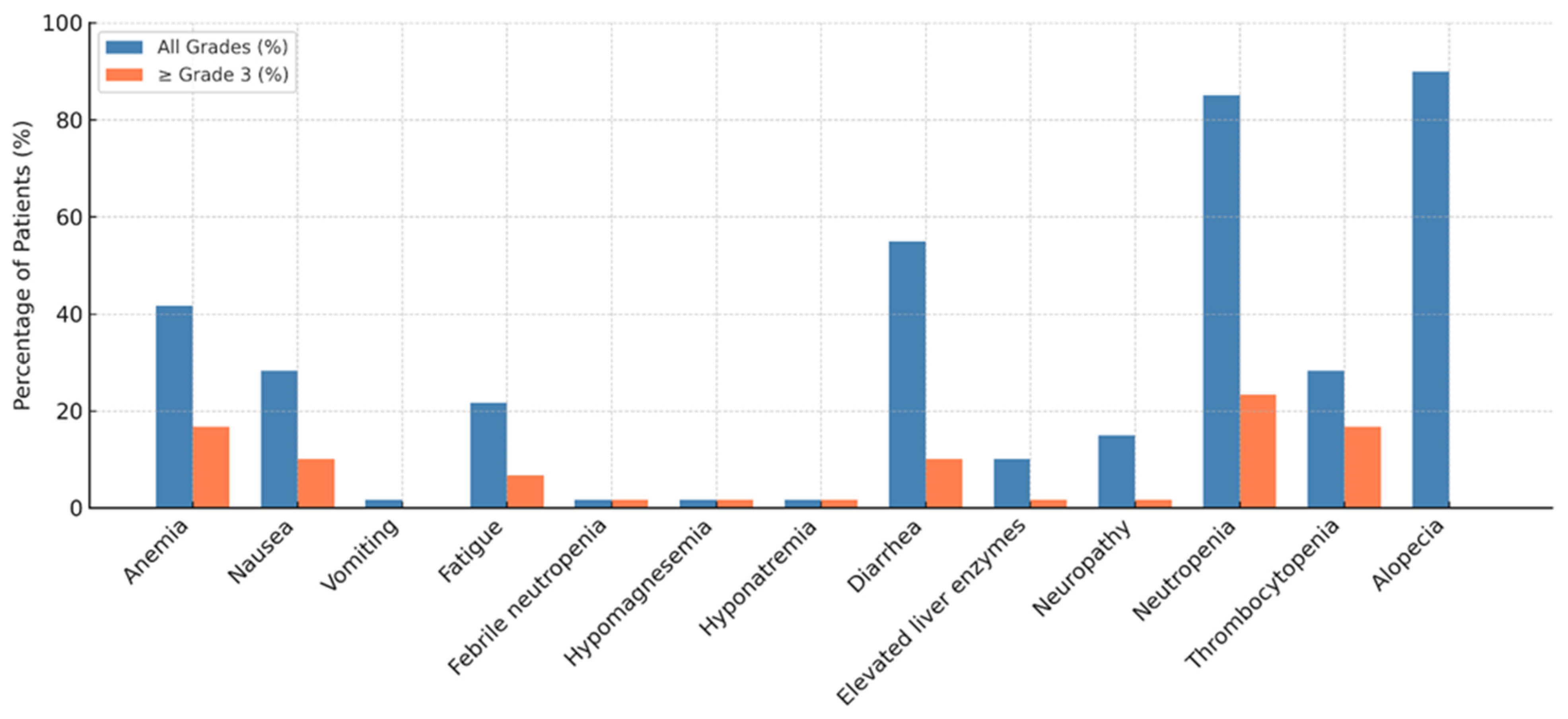
3.3. Safety and Adverse Events
4. Discussion
4.1. Real-World Outcomes Compared to Clinical Trials
4.2. Safety and Tolerability Profile
4.3. Limitations
4.4. Clinical Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jallah, J.K.; Dweh, T.J.; Anjankar, A.; Palma, O. A review of the advancements in targeted therapies for breast cancer. Cureus 2023, 15, e47847. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA A Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Cuyún Carter, G.; Mohanty, M.; Stenger, K.; Morato Guimaraes, C.; Singuru, S.; Basa, P.; Singh, S.; Tongbram, V.; Kuemmel, S.; Guarneri, V.; et al. Prognostic factors in hormone receptor-positive/human epidermal growth factor receptor 2-negative (HR+/HER2–) advanced breast cancer: A systematic literature review. Cancer Manag. Res. 2021, 13, 6537–6566. [Google Scholar] [CrossRef] [PubMed]
- Gradishar, W.J.; Moran, M.S.; Abraham, J.; Abramson, V.; Aft, R.; Agnese, D.; Allison, K.H.; Anderson, B.; Burstein, H.J.; Chew, H.; et al. NCCN Guidelines® insights: Breast cancer, version 4.2023: Featured updates to the NCCN guidelines. J. Natl. Compr. Cancer Netw. 2023, 21, 594–608. [Google Scholar] [CrossRef]
- Gennari, A.; André, F.; Barrios, C.; Cortes, J.; de Azambuja, E.; DeMichele, A.; Dent, R.; Fenlon, D.; Gligorov, J.; Hurvitz, S.A.; et al. ESMO Clinical Practice Guideline for the diagnosis, staging and treatment of patients with metastatic breast cancer☆. Ann. Oncol. 2021, 32, 1475–1495. [Google Scholar] [CrossRef]
- Li, C.H.; Karantza, V.; Aktan, G.; Lala, M. Current treatment landscape for patients with locally recurrent inoperable or metastatic triple-negative breast cancer: A systematic literature review. Breast Cancer Res. 2019, 21, 1–14. [Google Scholar] [CrossRef]
- Diana, A.; Franzese, E.; Centonze, S.; Carlino, F.; Della Corte, C.M.; Ventriglia, J.; Petrillo, A.; De Vita, F.; Alfano, R.; Ciardiello, F.; et al. Triple-negative breast cancers: Systematic review of the literature on molecular and clinical features with a focus on treatment with innovative drugs. Curr. Oncol. Rep. 2018, 20, 76. [Google Scholar] [CrossRef]
- Nardin, S.; Del Mastro, L. Sacituzumab Govitecan in HR-positive HER2-negative metastatic breast cancer. Ann. Transl. Med. 2023, 11, 228. [Google Scholar] [CrossRef]
- Goldenberg, D.M.; Cardillo, T.M.; Govindan, S.V.; Rossi, E.A.; Sharkey, R.M. Trop-2 is a novel target for solid cancer therapy with sacituzumab govitecan (IMMU-132), an antibody-drug conjugate (ADC). Oncotarget 2015, 6, 22496. [Google Scholar] [CrossRef]
- Goldenberg, D.M.; Sharkey, R.M. Sacituzumab govitecan, a novel, third-generation, antibody-drug conjugate (ADC) for cancer therapy. Expert Opin. Biol. Ther. 2020, 20, 871–885. [Google Scholar] [CrossRef]
- Nagayama, A.; Vidula, N.; Ellisen, L.; Bardia, A. Novel antibody–drug conjugates for triple negative breast cancer. Ther. Adv. Med. Oncol. 2020, 12, 1758835920915980. [Google Scholar] [CrossRef] [PubMed]
- Goldenberg, D.M.; Stein, R.; Sharkey, R.M. The emergence of trophoblast cell-surface antigen 2 (TROP-2) as a novel cancer target. Oncotarget 2018, 9, 28989. [Google Scholar] [CrossRef] [PubMed]
- Bardia, A.; Rugo, H.S.; Tolaney, S.M.; Loirat, D.; Punie, K.; Oliveira, M.; Brufsky, A.; Kalinsky, K.; Cortés, J.; Shaughnessy, J.O.; et al. Final results from the randomized phase III ASCENT clinical trial in metastatic triple-negative breast cancer and association of outcomes by human epidermal growth factor receptor 2 and trophoblast cell surface antigen 2 expression. J. Clin. Oncol. 2024, 42, 1738–1744. [Google Scholar] [CrossRef]
- Rugo, H.S.; Bardia, A.; Marmé, F.; Cortés, J.; Schmid, P.; Loirat, D.; Trédan, O.; Ciruelos, E.; Dalenc, F.; Pardo, P.G.; et al. Overall survival with sacituzumab govitecan in hormone receptor-positive and human epidermal growth factor receptor 2-negative metastatic breast cancer (TROPiCS-02): A randomised, open-label, multicentre, phase 3 trial. Lancet 2023, 402, 1423–1433. [Google Scholar] [CrossRef]
- Spring, L.M.; Nakajima, E.; Hutchinson, J.; Viscosi, E.; Blouin, G.; Weekes, C.; Rugo, H.; Moy, B.; Bardia, A. Sacituzumab govitecan for metastatic triple-negative breast cancer: Clinical overview and management of potential toxicities. Oncologist 2021, 26, 827–834. [Google Scholar] [CrossRef]
- Püsküllüoğlu, M.; Pieniążek, M.; Las-Jankowska, M.; Streb, J.; Ziobro, M.; Pacholczak-Madej, R.; Miegem, P.K.-V.; Rudzińska, A.; Grela-Wojewoda, A.; Łacko, A.; et al. Sacituzumab govitecan for second and subsequent line palliative treatment of patients with triple-negative breast cancer: A Polish real-world multicenter cohort study. Oncol. Ther. 2024, 12, 787–801. [Google Scholar] [CrossRef]
- Reinisch, M.; Bruzas, S.; Spoenlein, J.; Shenoy, S.; Traut, A.; Harrach, H.; Chiari, O.; Cremer, E.; Ataseven, B.; Gubelt, L.; et al. Safety and effectiveness of sacituzumab govitecan in patients with metastatic triple-negative breast cancer in real-world settings: First observations from an interdisciplinary breast cancer centre in Germany. Ther. Adv. Med. Oncol. 2023, 15, 17588359231200454. [Google Scholar] [CrossRef]
- Grinda, T.; Morganti, S.; Hsu, L.; Yoo, T.-K.; Kusmick, R.J.; Aizer, A.A.; Giordano, A.; Leone, J.P.; Hughes, M.; Tolaney, S.M.; et al. Real-World outcomes with sacituzumab govitecan among breast cancer patients with central nervous system metastases. NPJ Breast Cancer 2025, 11, 22. [Google Scholar] [CrossRef]
- Kalinsky, K.; Spring, L.; Yam, C.; Bhave, M.A.; Ntalla, I.; Lai, C.; Sjekloca, N.; Stwalley, B.; Stokes, M.; Taylor, A.; et al. Real-world use patterns, effectiveness, and tolerability of sacituzumab govitecan for second-line and later-line treatment of metastatic triple-negative breast cancer in the United States. Breast Cancer Res. Treat. 2024, 208, 203–214. [Google Scholar] [CrossRef]
- Kang, C. Sacituzumab Govitecan: A Review in Unresectable or Metastatic HR+/HER2− Breast Cancer. Target. Oncol. 2024, 19, 289–296. [Google Scholar] [CrossRef]
- WDeClue, R.; Fisher, M.D.; Gooden, K.; Walker, M.S.; Le, T.K. Real-world outcomes in metastatic HR+/HER2-, HER2+ and triple negative breast cancer after start of first-line therapy. Future Oncol. 2023, 19, 909–923. [Google Scholar] [CrossRef] [PubMed]
- Xu, B.; Wang, S.; Yan, M.; Sohn, J.; Li, W.; Tang, J.; Wang, X.; Wang, Y.; Im, S.-A.; Jiang, D.; et al. Sacituzumab govitecan in HR+ HER2− metastatic breast cancer: The randomized phase 3 EVER-132-002 trial. Nat. Med. 2024, 30, 3709–3716. [Google Scholar] [CrossRef] [PubMed]
- Caputo, R.; Buono, G.; Piezzo, M.; Martinelli, C.; Cianniello, D.; Rizzo, A.; Pantano, F.; Staropoli, N.; Cangiano, R.; Turano, S.; et al. Sacituzumab Govitecan for the treatment of advanced triple negative breast cancer patients: A multi-center real-world analysis. Front. Oncol. 2024, 14, 1362641. [Google Scholar] [CrossRef] [PubMed]
- Alaklabi, S.; Roy, A.M.; Zagami, P.; Chakraborty, A.; Held, N.; Elijah, J.; George, A.; Attwood, K.; Shaikh, S.S.; Chaudhary, L.N.; et al. Real-World Clinical Outcomes With Sacituzumab Govitecan in Metastatic Triple-Negative Breast Cancer. JCO Oncol. Pract. 2024. [Google Scholar] [CrossRef]
- Rizzo, A.; Rinaldi, L.; Massafra, R.; Cusmai, A.; Guven, D.C.; Forgia, D.L.; Latorre, A.; Giotta, F. Sacituzumab govitecan vs. chemotherapy for metastatic breast cancer: A meta-analysis on safety outcomes. Future Oncol. 2024, 20, 1427–1434. [Google Scholar] [CrossRef]
- Hanna, D.; Merrick, S.; Ghose, A.; Devlin, M.J.; Yang, D.D.; Phillips, E.; Okines, A.; Chopra, N.; Papadimatraki, E.; Ross, K.; et al. Real world study of sacituzumab govitecan in metastatic triple-negative breast cancer in the United Kingdom. Br. J. Cancer 2024, 130, 1916–1920. [Google Scholar] [CrossRef]
- Sathe, A.G.; Diderichsen, P.M.; Fauchet, F.; Phan, S.C.; Girish, S.; Othman, A.A. Exposure-Response Analyses of Sacituzumab Govitecan Efficacy and Safety in Patients With Metastatic Triple-Negative Breast Cancer. Clin Pharmacol Ther. 2025, 117, 570–578. [Google Scholar] [CrossRef]
- Yang, Y.; Li, H.; Yang, W.; Shi, Y. Improving efficacy of TNBC immunotherapy: Based on analysis and subtyping of immune microenvironment. Front. Immunol. 2024, 15, 1441667. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Value |
|---|---|
| Age (median, range) | 48 (29–78) |
| De novo metastasis | 18 (26.5%) |
| Molecular classification | |
| mTNBC | 35 (51.5%) |
| mHRPBC | 33 (48.5%) |
| Her2 status | |
| Her2 0 | 52 (76.4%) |
| Her2 + 1 | 10 (14.7%) |
| Her2 + 2 (FISH negative) | 6 (8.8%) |
| ECOG PS | |
| 0 | 48 (70.6%) |
| 1 | 20 (29.4%) |
| Metastatic sites | |
| Liver | 35 (51.5%) |
| Lung | 39 (57.4%) |
| Brain | 29 (42.6%) |
| Bone | 39 (57.4%) |
| Lymph node | 58 (85.3%) |
| Prior immunotherapy | 22 (32.4%) |
| Dose reduction due to toxicity | 20 (29.4%) |
| Treatment discontinuation due to toxicity | 2 (2.9%) |
| Prior chemotherapy agents | |
| Taxane | 64 (94.1%) |
| Anthracycline | 54 (79.4%) |
| Carboplatin | 48 (70.6%) |
| Capecitabine | 53 (77.9%) |
| Local treatment | 60 (88.2%) |
| Prior lines of therapy in metastatic set | |
| ≤3 lines | 29 (42.6%) |
| >3 lines | 38 (55.9%) |
| Number of SG cycles (median, range) | 7 (3–37) |
| G-CSF use with SG | 60 (88.2%) |
| Variable | mPFS (Months) | 95% CI | p-Value | HR (95% CI) | Multivariate p-Value |
|---|---|---|---|---|---|
| Molecular subgroup | 0.78 | 0.348 | |||
| mHRPBC | 5.76 | (4.28–7.24) | Ref. | ||
| mTNBC | 6.5 | (4.45–8.54) | 0.73 (0.384–1.401) | ||
| De novo metastases | 0.63 | ||||
| Absent | 6.13 | (4.71–7.88) | |||
| Present | 5.13 | (1.97–8.28) | |||
| ECOG PS | 0.004 | 0.050 | |||
| ECOG PS-0 | 7.26 | (5.32–9.21) | Ref. | ||
| ECOG PS-1 | 3.76 | (2.26–5.27) | 1.96 (0.999–3.875) | ||
| Liver metastases | 0.002 | 0.047 | |||
| Absent | NR | (4.83–7.43) | Ref. | ||
| Present | 4.43 | (2.74–6.12) | 2.04 (1.008–4.151) | ||
| Lung metastases | 0.088 | ||||
| Absent | 8.0 | (6.19–9.80) | |||
| Present | 3.9 | (2.30–7.76) | |||
| Brain metastases | 0.253 | ||||
| Absent | 6.50 | (5.44–7.55) | |||
| Present | 5.03 | (2.74–6.12) | |||
| Bone metastases | 0.004 | 0.095 | |||
| Absent | NR | NA | Ref. | ||
| Present | 5.03 | (3.18–6.88) | 1.87 (0.89–3.91) | ||
| Lymph node metastases | 0.086 | ||||
| Absent | 5.33 | (4.31–6.35) | |||
| Present | 6.50 | (4.07–8.92) | |||
| Prior ICIs | 0.886 | ||||
| Absent | 6.10 | (4.89–7.30) | |||
| Present | 6.30 | (2.31–10.28) | |||
| Prior chemotherapy | 0.352 | ||||
| Taxane | 6.13 | (4.86–7.40) | |||
| Antracycline | 6.13 | (4.79–7.47) | |||
| Carboplatin | 6.23 | (4.62–7.84) | |||
| Capecitabine | 6.13 | (4.94–7.32) | |||
| Local treatment | 0.929 | ||||
| Absent | 3.40 | (0.10–11.71) | |||
| Present | 6.13 | (4.90–7.36) | |||
| No. of chemotherapy lines | 0.796 | ||||
| ≤3 lines chemotherapy | 5.33 | (2.89–7.76) | |||
| >3 lines chemotherapy | 6.23 | (5.32–7.14) | |||
| Dose reduction due to toxicity | 0.270 | ||||
| Absent | 6.23 | (5.33–7.13) | |||
| Present | 3.13 | (0.13–6.13) | |||
| G-CSF use with SG | 0.097 | ||||
| Absent | NR | NA | |||
| Present | NR | NA | |||
| At diagnosis Ki-67 | 0.897 | ||||
| ≤20 | 6.13 | (4.55–7.71) | |||
| >20 | 5.76 | (4.27–7.25) | 0.897 | ||
| Metastatic setting Ki-67 | 1 | ||||
| ≤20 | 6.13 | (3.46–8.80) | |||
| >20 | 6.23 | (4.67–7.79) | 1 |
| Variable | mOS (Months) | 95% CI | p-Value | HR (95% CI) | Multivariate p-Value |
|---|---|---|---|---|---|
| Molecular subgroup | 0.380 | 0.046 | |||
| mHRPBC | 11.30 | (9.16–25.4) | Ref. | ||
| mTNBC | 11.93 | (5.22–18.64) | 0.46 (0.22–0.98) | ||
| De novo metastases | 0.716 | ||||
| Absent | 12.50 | (10.78–14.21) | |||
| Present | 14.73 | (4.23–25.23) | |||
| ECOG-PS | 0.178 | ||||
| ECOG-0 | 14.73 | (10.52–18.94) | |||
| ECOG-1 | 13.33 | (2.56–24.10) | |||
| Liver metastases | 0.001 | 0.022 | |||
| Absent | 17.73 | NA | Ref. | ||
| Present | 5.96 | (2.79–9.14) | 3.15 (1.184–8.383) | ||
| Lung metastases | 0.076 | ||||
| Absent | 17.30 | (11.29–23.31) | |||
| Present | 7.13 | (3.65–14.78) | |||
| Brain metastases | 0.025 | 0.429 | |||
| Absent | 17.30 | (11.12–23.47) | Ref. | ||
| Present | 7.13 | (1.07–13.18) | 1.39 (0.609–3.205) | ||
| Bone metastases | 0.008 | 0.073 | |||
| Absent | NR | NA | Ref. | ||
| Present | 11.93 | (4.98–18.88) | 2.28 (0.927–5.624) | ||
| Lymph node metastases | 0.884 | ||||
| Absent | 21.40 | NA | |||
| Present | 12.50 | (10.72–14.27) | |||
| Prior ICIs | 0.963 | ||||
| Absent | 14.73 | (4.89–24.57) | |||
| Present | 12.50 | (10.31–14.68) | |||
| Prior chemotherapy | 0.293 | ||||
| Taxane | - | - | |||
| Antracycline | 13.33 | (4.56–22.10) | |||
| Carboplatin | 12.30 | (4.71–19.88) | |||
| Capecitabine | 12.50 | (9.95–15.04) | |||
| Local treatment | 0.673 | ||||
| Absent | 6.36 | (0.10–16.03) | |||
| Present | 12.50 | (10.75–14.24) | |||
| No. of chemotherapy lines | 0.745 | ||||
| ≤3 lines chemotherapy | 14.73 | (4.99–24.47) | |||
| >3 lines chemotherapy | 12.30 | (5.81–18.79) | |||
| Dose reduction due to toxicity | 1.00 | ||||
| Absent | 12.50 | (10.70–14.29) | |||
| Present | NR | NA | |||
| G-CSF use with SG | 0.724 | ||||
| Absent | 12.30 | (0.10–24.75) | |||
| Present | 13.33 | (6.96–19.69) | |||
| At diagnosis Ki-67 | 0.460 | ||||
| ≤20% | 14.73 | (4.85–22.63) | |||
| >20% | 12.30 | (6.02–18.57) | |||
| Metastatic setting Ki-67 | 0.184 | ||||
| ≤20% | 14.73 | (2.81–30.21) | |||
| >20% | 12.50 | (10.82–14.17) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muğlu, H.; Helvacı, K.; Köylü, B.; Yücel, M.H.; Celayir, Ö.M.; Demirci, U.; Uluç, B.O.; Başaran, G.; Korkmaz, T.; Selçukbiricik, F.; et al. The Clinical Outcomes and Safety of Sacituzumab Govitecan in Heavily Pretreated Metastatic Triple-Negative and HR+/HER2− Breast Cancer: A Multicenter Observational Study from Turkey. Cancers 2025, 17, 1592. https://doi.org/10.3390/cancers17091592
Muğlu H, Helvacı K, Köylü B, Yücel MH, Celayir ÖM, Demirci U, Uluç BO, Başaran G, Korkmaz T, Selçukbiricik F, et al. The Clinical Outcomes and Safety of Sacituzumab Govitecan in Heavily Pretreated Metastatic Triple-Negative and HR+/HER2− Breast Cancer: A Multicenter Observational Study from Turkey. Cancers. 2025; 17(9):1592. https://doi.org/10.3390/cancers17091592
Chicago/Turabian StyleMuğlu, Harun, Kaan Helvacı, Bahadır Köylü, Mehmet Haluk Yücel, Özde Melisa Celayir, Umut Demirci, Başak Oyan Uluç, Gül Başaran, Taner Korkmaz, Fatih Selçukbiricik, and et al. 2025. "The Clinical Outcomes and Safety of Sacituzumab Govitecan in Heavily Pretreated Metastatic Triple-Negative and HR+/HER2− Breast Cancer: A Multicenter Observational Study from Turkey" Cancers 17, no. 9: 1592. https://doi.org/10.3390/cancers17091592
APA StyleMuğlu, H., Helvacı, K., Köylü, B., Yücel, M. H., Celayir, Ö. M., Demirci, U., Uluç, B. O., Başaran, G., Korkmaz, T., Selçukbiricik, F., Ölmez, Ö. F., & Bilici, A. (2025). The Clinical Outcomes and Safety of Sacituzumab Govitecan in Heavily Pretreated Metastatic Triple-Negative and HR+/HER2− Breast Cancer: A Multicenter Observational Study from Turkey. Cancers, 17(9), 1592. https://doi.org/10.3390/cancers17091592