
Pre-Treatment SEPTIN9 Gene Methylation Ratio Predicts Tumor Response to Total Neoadjuvant Therapy in Patients with Locally Advanced Rectal Cancer

 , , , ,
, , , ,  , and
, and 
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients’ Selection
2.2. LARC Diagnosis
2.3. Treatment of LARC
2.4. Evaluation of Tumor Response to TNT
2.5. SEPT9m Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CRC | Colorectal cancer |
| RC | Rectal cancer |
| LARC | Locally advanced rectal cancer |
| cCR | Complete clinical response |
| TNT | Total neoadjuvant therapy |
| WW | Watch and wait |
| SEPT9m | SEPTIN9 gene methylation |
| SEPT9mr | SEPTIN9 gene methylation ratio |
| DRE | Digital rectal examination |
| MRI | Magnetic resonance imaging |
| mTRG | MRI Tumor Regression Grade |
| cfDNA | Cell-free DNA |
| ddPCR | Droplet digital polymerase chain reaction |
| cTR | Complete tumor response |
| cPR | Complete pathological response |
| CEA | Carcinoembryonic antigen |
References
- Colorectal Cancer: Statistics|Cancer.Net [Internet]. Available online: https://www.cancer.net/cancer-types/colorectal-cancer/statistics (accessed on 4 March 2025).
- Kasi, A.; Abbasi, S.; Handa, S.; Al-Rajabi, R.; Saeed, A.; Baranda, J.; Sun, W. Total Neoadjuvant Therapy vs Standard Therapy in Locally Advanced Rectal Cancer: A Systematic Review and Meta-analysis. JAMA Netw. Open 2020, 3, e2030097. [Google Scholar] [CrossRef]
- Kang, S.B.; Cho, J.R.; Jeong, S.Y.; Oh, J.H.; Ahn, S.; Choi, S.; Kim, D.W.; Lee, B.H.; Youk, E.G.; Park, S.C.; et al. Quality of life after sphincter preservation surgery or abdominoperineal resection for low rectal cancer (ASPIRE): A long-term prospective, multicentre, cohort study. Lancet Reg. Health West. Pac. 2020, 6, 100087. [Google Scholar] [CrossRef] [PubMed]
- Kokaine, L.; Gardovskis, A.; Gardovskis, J. Evaluation and Predictive Factors of Complete Response in Rectal Cancer after Neoadjuvant Chemoradiation Therapy. Medicina 2021, 57, 1044. [Google Scholar] [CrossRef] [PubMed]
- Hariharan, R.; Jenkins, M. Utility of the methylated SEPT9 test for the early detection of colorectal cancer: A systematic review and meta-analysis of diagnostic test accuracy. BMJ Open Gastroenterol. 2020, 7, e000355. [Google Scholar] [CrossRef] [PubMed]
- Leon Arellano, M.; García-Arranz, M.; Ruiz, R.; Olivera, R.; Magallares, S.; Olmedillas-Lopez, S.; Valdes-Sanchez, T.; Guadalajara, H.; García-Olmo, D. A First Step to a Biomarker of Curative Surgery in Colorectal Cancer by Liquid Biopsy of Methylated Septin 9 Gene. Dis. Markers. 2020, 2020, 9761406. [Google Scholar] [CrossRef]
- Leon Arellano, M.; García-Arranz, M.; Guadalajara, H.; Olivera-Salazar, R.; Valdes-Sanchez, T.; García-Olmo, D. Analysis of Septin 9 Gene Hypermethylation as Follow-Up Biomarker of Colorectal Cancer Patients after Curative Surgery. Diagnostics 2022, 12, 993. [Google Scholar] [CrossRef]
- Patel, U.B.; Taylor, F.; Blomqvist, L.; George, C.; Evans, H.; Tekkis, P.; Quirke, P.; Sebag-Montefiore, D.; Moran, B.; Heald, R.; et al. Magnetic resonance imaging-detected tumor response for locally advanced rectal cancer predicts survival outcomes: MERCURY experience. J. Clin. Oncol. 2011, 29, 3753–3760. [Google Scholar] [CrossRef]
- Fukushige, S.; Horii, A. DNA methylation in cancer: A gene silencing mechanism and the clinical potential of its biomarkers. Tohoku J. Exp. Med. 2013, 229, 173–185. [Google Scholar] [CrossRef] [PubMed]
- Mostowy, S.; Cossart, P. Septins: The fourth component of the cytoskeleton. Nat. Rev. Mol. Cell Biol. 2012, 13, 183–194. [Google Scholar] [CrossRef]
- Peterson, E.A.; Petty, E.M. Conquering the complex world of human septins: Implications for health and disease. Clin. Genet. 2010, 77, 511–524. [Google Scholar] [CrossRef]
- Abd El Kader, L.; Soliman, A.H.; Salem, S.E.; Akel, S.Y.; Ibrahim, N.H. The Clinical Significance of Septin 9 and Colon Cancer Specific Antigen-2 (CCSA-2) in Colorectal Cancer. Asian Pac. J. Cancer Prev. 2023, 24, 1027–1036. [Google Scholar] [CrossRef] [PubMed]
- Ma, Z.Y.; Chan, C.S.Y.; Lau, K.S.; Ng, L.; Cheng, Y.Y.; Leung, W.K. Application of droplet digital polymerase chain reaction of plasma methylated septin 9 on detection and early monitoring of colorectal cancer. Sci. Rep. 2021, 11, 23446. [Google Scholar] [CrossRef]
- Ponomaryova, A.A.; Rykova, E.Y.; Solovyova, A.I.; Tarasova, A.S.; Kostromitsky, D.N.; Dobrodeev, A.Y.; Afanasiev, S.A.; Cherdyntseva, N.V. Dynamic Changes in Circulating Methylated Markers in Response to Antitumor Therapy of Rectal Cancer. J. Gastrointest. Cancer. 2024, 55, 1190–1198. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Hu, P.; Liu, J.; Chen, L. mSEPT9 Can Monitor the Response and Predict the Prognosis of Stage IV Colorectal Cancer Patients with Liver Metastasis Undergoing Potentially Curative Surgery. J. Surg. Res. 2021, 267, 485–494. [Google Scholar] [CrossRef]
- Empuku, S.; Nakajima, K.; Akagi, T.; Kaneko, K.; Hijiya, N.; Etoh, T.; Shiraishi, N.; Moriyama, M.; Inomata, M. An 80-gene set to predict response to preoperative chemoradiotherapy for rectal cancer by principle component analysis. Mol. Clin. Oncol. 2016, 4, 733–739. [Google Scholar] [CrossRef]
- Yao, Y.; Xu, X.; Yang, L.; Zhu, J.; Wan, J.; Shen, L.; Xia, F.; Fu, G.; Deng, Y.; Pan, M.; et al. Patient-Derived Organoids Predict Chemoradiation Responses of Locally Advanced Rectal Cancer. Cell Stem Cell. 2020, 26, 17–26.e6. [Google Scholar] [CrossRef]
- Timmerman, C.; Taveras, L.R.; Huerta, S. Clinical and molecular diagnosis of pathologic complete response in rectal cancer: An update. Expert. Rev. Mol. Diagn. 2018, 18, 887–896. [Google Scholar] [CrossRef]
- Dayde, D.; Tanaka, I.; Jain, R.; Tai, M.C.; Taguchi, A. Predictive and Prognostic Molecular Biomarkers for Response to Neoadjuvant Chemoradiation in Rectal Cancer. Int. J. Mol. Sci. 2017, 18, 573. [Google Scholar] [CrossRef]
- De Palma, F.D.E.; Luglio, G.; Tropeano, F.P.; Pagano, G.; D’Armiento, M.; Kroemer, G.; Maiuri, M.C.; De Palma, G.D. The Role of Micro-RNAs and Circulating Tumor Markers as Predictors of Response to Neoadjuvant Therapy in Locally Advanced Rectal Cancer. Int. J. Mol. Sci. 2020, 21, 7040. [Google Scholar] [CrossRef]
- Yi, Y.; Shen, L.; Shi, W.; Xia, F.; Zhang, H.; Wang, Y.; Zhang, J.; Wang, Y.; Sun, X.; Zhang, Z.; et al. Gut Microbiome Components Predict Response to Neoadjuvant Chemoradiotherapy in Patients with Locally Advanced Rectal Cancer: A Prospective, Longitudinal Study. Clin. Cancer Res. 2021, 27, 1329–1340. [Google Scholar] [CrossRef]
- Patel, P.M.; Harris, K.; Huerta, S. Clinical and molecular diagnosis of pathologic complete response in rectal cancer. Expert. Rev. Mol. Diagn. 2015, 15, 1505–1516. [Google Scholar] [CrossRef] [PubMed]
- Bedrikovetski, S.; Traeger, L.; Vather, R.; Moore, J.W.; Sammour, T. Clinical and biochemical predictors of tumor response after neoadjuvant therapy in rectal cancer. Asia Pac. J. Clin. Oncol. 2023, 19, 365–373. [Google Scholar] [CrossRef] [PubMed]
- Yildirim, E.; Bektas, S.; Pelen, Z.; Yanik, I.; Er, A.M.; Cengel, F.; Gumuskaya, P.Ö. Histopathological, Radiological, and Demographic Factors Predicting the Response to Neoadjuvant Therapy for Rectal Cancer. J. Gastrointest. Cancer. 2022, 53, 22–30. [Google Scholar] [CrossRef] [PubMed]
- Kim, N.K.; Hur, H. New Perspectives on Predictive Biomarkers of Tumor Response and Their Clinical Application in Preoperative Chemoradiation Therapy for Rectal Cancer. Yonsei Med. J. 2015, 56, 1461–1477. [Google Scholar] [CrossRef]
- Fowler, H.; Clifford, R.E.; Bowden, D.; Sutton, P.A.; Govindarajah, N.; Fok, M.; Glenn, M.; Wall, M.; Rubbi, C.; Buczacki, S.J.A.; et al. Myoferlin: A Potential Marker of Response to Radiation Therapy and Survival in Locally Advanced Rectal Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2024, 120, 1111–1123. [Google Scholar] [CrossRef]
- Wen, X.; Zee, S.Y.; Shroyer, K.R.; Bandovic, J. Intratumoral Budding and Tumor Microenvironment in Pretreatment Rectal Cancer Biopsies Predict the Response to Neoadjuvant Chemoradiotherapy. Appl. Immunohistochem. Mol. Morphol. 2022, 30, 1–7. [Google Scholar] [CrossRef]
- Alden, S.L.; Lee, V.; Narang, A.K.; Meyer, J.; Gearhart, S.L.; Christenson, E.S. Circulating Tumor DNA to Predict Radiographic and Pathologic Response to Total Neoadjuvant Therapy in Locally Advanced Rectal Cancer. Oncologist 2024, 29, e414–e418. [Google Scholar] [CrossRef]
- Zhou, H.; Chen, Y.; Xiao, Y.; Wu, Q.; Li, H.; Li, Y.; Su, G.; Ke, L.; Wu, J.; Li, J. Evaluation of the ability of fatty acid metabolism signature to predict response to neoadjuvant chemoradiotherapy and prognosis of patients with locally advanced rectal cancer. Front. Immunol. 2022, 13, 1050721. [Google Scholar] [CrossRef]
- Jeon, S.H.; Song, C.; Chie, E.K.; Kim, B.; Kim, Y.H.; Chang, W.; Lee, Y.J.; Chung, J.H.; Chung, J.B.; Lee, K.W.; et al. Combining Radiomics and Blood Test Biomarkers to Predict the Response of Locally Advanced Rectal Cancer to Chemoradiation. In Vivo 2020, 34, 2955–2965. [Google Scholar] [CrossRef]
- Huang, Y.; Lee, D.; Young, C. Predictors for complete pathological response for stage II and III rectal cancer following neoadjuvant therapy—A systematic review and meta-analysis. Am. J. Surg. 2020, 220, 300–308. [Google Scholar] [CrossRef]
- Strous, M.T.A.; Faes, T.K.E.; Heemskerk, J.; Lohman, B.G.P.M.; Simons, P.C.G.; Janssen Heijnen, M.L.G.; Vogelaar, F.J.; de Bruïne, A.P. Tumour-stroma ratio to predict pathological response to neo-adjuvant treatment in rectal cancer. Surg. Oncol. 2022, 45, 101862. [Google Scholar] [CrossRef] [PubMed]
- Fischer, J.; Eglinton, T.W.; Frizelle, F.A. Clinical predictors of response to chemoradiotherapy for rectal cancer as an aid to organ preservation. ANZ J. Surg. 2021, 91, 1190–1195. [Google Scholar] [CrossRef] [PubMed]
- Chapman, B.C.; Lai, S.H.; Friedrich, T.; Lieu, C.H.; Moskalenko, M.; Olsen, J.R.; Herter, W.; Birnbaum, E.H.; McCarter, M.D.; Vogel, J.D. Rectal Cancer: Clinical and Molecular Predictors of a Complete Response to Total Neoadjuvant Therapy. Dis. Colon. Rectum. 2023, 66, 521–530. [Google Scholar] [CrossRef]
- Xu, Y.J.; Tao, D.; Qin, S.B.; Xu, X.Y.; Yang, K.W.; Xing, Z.X.; Zhou, J.Y.; Jiao, Y.; Wang, L.L. Prediction of pathological complete response and prognosis in locally advanced rectal cancer. World J. Gastrointest. Oncol. 2024, 16, 2520–2530. [Google Scholar] [CrossRef]
- Yilmaz, S.; Liska, D.; Conces, M.L.; Tursun, N.; Elamin, D.; Ozgur, I.; Maspero, M.; Rosen, D.R.; Khorana, A.A.; Balagamwala, E.H.; et al. What Predicts Complete Response to Total Neoadjuvant Therapy in Locally Advanced Rectal Cancer? Dis. Colon. Rectum. 2025, 68, 60–68. [Google Scholar] [CrossRef]
- Lech, G.; Słotwiński, R.; Słodkowski, M.; Krasnodębski, I.W. Colorectal cancer tumour markers and biomarkers: Recent therapeutic advances. World J. Gastroenterol. 2016, 22, 1745–1755. [Google Scholar] [CrossRef]
- Shen, D.; Wang, X.; Wang, H.; Xu, G.; Xie, Y.; Zhuang, Z.; Huang, Z.; Li, J.; Lin, J.; Wang, P.; et al. Current Surveillance After Treatment is Not Sufficient for Patients With Rectal Cancer With Negative Baseline CEA. J. Natl. Compr. Canc Netw. 2022, 20, 653–662.e3. [Google Scholar] [CrossRef]
- Mishra, S.; Raval, M.; Kachhawaha, A.S.; Tiwari, B.S.; Tiwari, A.K. Aging: Epigenetic modifications. Prog. Mol. Biol. Transl. Sci. 2023, 197, 171–209. [Google Scholar] [CrossRef]
- Johnson, A.A.; Akman, K.; Calimport, S.R.; Wuttke, D.; Stolzing, A.; de Magalhães, J.P. The role of DNA methylation in aging, rejuvenation, and age-related disease. Rejuvenation Res. 2012, 15, 483–494. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Age (Years) | 63.3 (38–80) |
| Sex | |
| Male | 24 (61.5%) |
| Female | 15 (38.5%) |
| Tumor size (cm) | 4.3 (2–8.5) |
| T stage | |
| T1 | 0 (0%) |
| T2 | 2 (5.1%) |
| T3 | 31 (79.5%) |
| T4 | 6 (15.4%) |
| N stage | |
| N0 | 4 (10.3%) |
| N1 | 20 (51.3%) |
| N2 | 15 (38.5%) |
| SEPT9mr | 0.0317 (0.008–0.125) |
| cTR | cCR | 23 (59%) | |
| Non-cCR but cPR | 4 (10.3%) | 27 (69.2%) | |
| Non-cTR | Non-cCR nor cPR | 12 (30.8%) | 12 (30.8%) |
| cTR | p | OR (95% CI) | ||
|---|---|---|---|---|
| No | Yes | |||
| Age (years) | 62.0 ± 12.2 | 63.9 ± 10.5 | 0.624 | 1.02 (0.95, 1.08) |
| Sex | 0.580 | |||
| Male | 6 (50.0%) | 18 (66.7%) | ||
| Female | 6 (50.0%) | 9 (33.3%) | ||
| SEPT9mr | 0.032 (0.023–0.043) | 0.023 (0.018–0.029) | 0.033 | 0.97 (0.92, 1.00) |
| Tumor size (cm) | 4.9 (4.0–6.7) | 4.0 (2.9–4.5) | 0.026 | 0.55 (0.30, 0.88) |
| T | 0.748 | |||
| T2 | 1 (8.3%) | 1 (3.7%) | ||
| T3 | 8 (66.7%) | 23 (85.2%) | ||
| T4 | 3 (25.0%) | 3 (11.1%) | ||
| N | 0.368 | |||
| N0 | 0 (0.0%) | 4 (14.8%) | ||
| N1 | 6 (50.0%) | 14 (51.9%) | ||
| N2 | 6 (50.0%) | 9 (33.3%) | ||
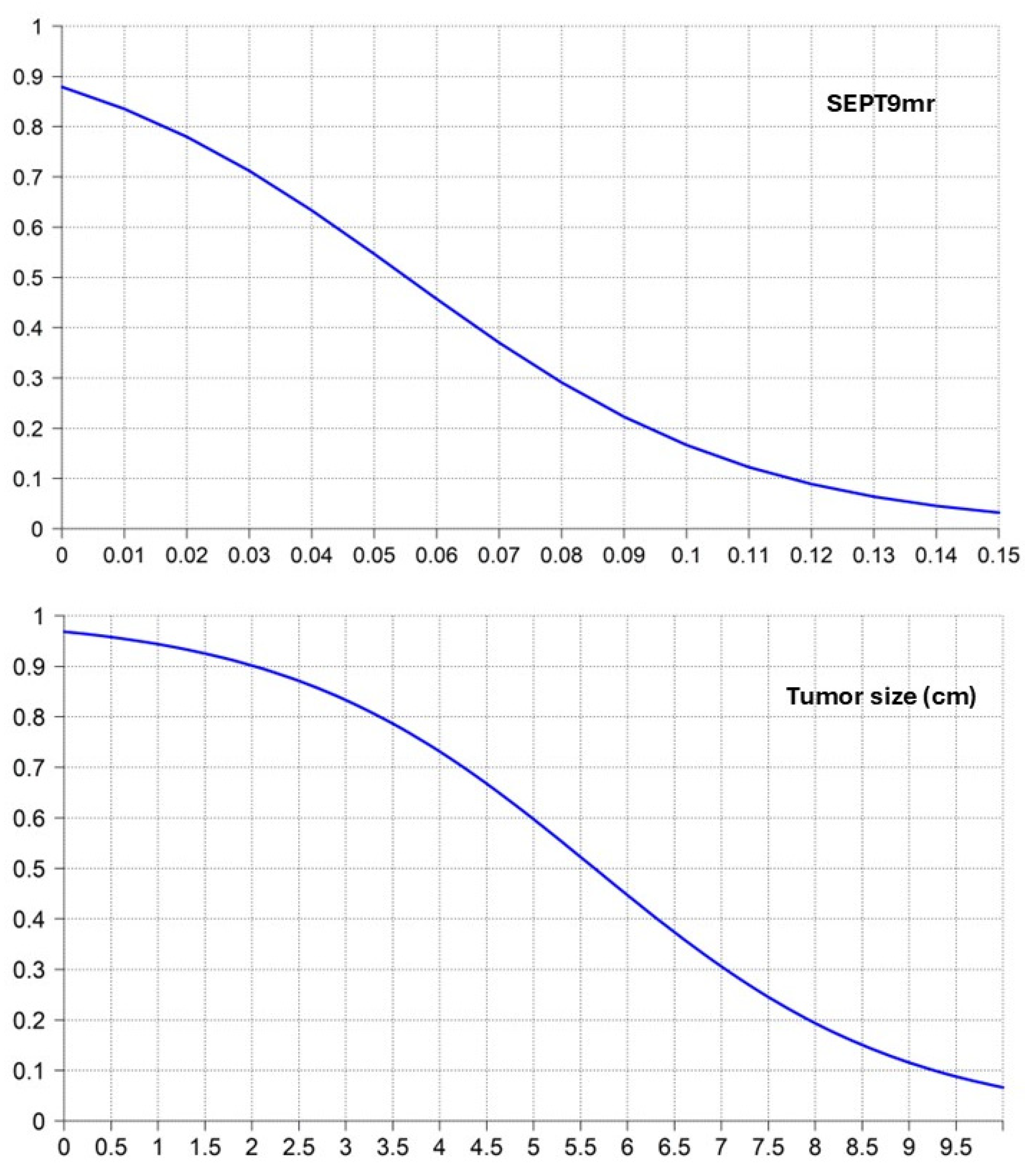
| SEPT9mr | Probability of cTR | Tumor Size (cm) | Probability of cTR |
|---|---|---|---|
| 0.00 | 0.879 | 0.0 | 0.969 |
| 0.01 | 0.835 | 0.5 | 0.958 |
| 0.02 | 0.780 | 1.0 | 0.944 |
| 0.03 | 0.712 | 1.5 | 0.925 |
| 0.04 | 0.633 | 2.0 | 0.902 |
| 0.05 | 0.547 | 2.5 | 0.871 |
| 0.06 | 0.457 | 3.0 | 0.833 |
| 0.07 | 0.370 | 3.5 | 0.787 |
| 0.08 | 0.291 | 4.0 | 0.731 |
| 0.09 | 0.223 | 4.5 | 0.668 |
| 0.10 | 0.167 | 5.0 | 0.597 |
| 0.11 | 0.122 | 5.5 | 0.523 |
| 0.12 | 0.089 | 6.0 | 0.447 |
| 0.13 | 0.064 | 6.5 | 0.374 |
| 0.14 | 0.045 | 7.0 | 0.306 |
| 0.15 | 0.032 | 7.5 | 0.245 |
| 8.0 | 0.194 | ||
| 8.5 | 0.151 | ||
| 9.0 | 0.116 | ||
| 9.5 | 0.088 | ||
| 10.0 | 0.067 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Domínguez-Prieto, V.; León-Arellano, M.; Olivera-Salazar, R.; Vega-Clemente, L.; Caramés, C.; Ruiz-Hispán, E.; Fuentes-Mateos, R.; Rosero-Rodríguez, D.; Guadalajara, H.; García-Arranz, M.; et al. Pre-Treatment SEPTIN9 Gene Methylation Ratio Predicts Tumor Response to Total Neoadjuvant Therapy in Patients with Locally Advanced Rectal Cancer. Cancers 2025, 17, 965. https://doi.org/10.3390/cancers17060965
Domínguez-Prieto V, León-Arellano M, Olivera-Salazar R, Vega-Clemente L, Caramés C, Ruiz-Hispán E, Fuentes-Mateos R, Rosero-Rodríguez D, Guadalajara H, García-Arranz M, et al. Pre-Treatment SEPTIN9 Gene Methylation Ratio Predicts Tumor Response to Total Neoadjuvant Therapy in Patients with Locally Advanced Rectal Cancer. Cancers. 2025; 17(6):965. https://doi.org/10.3390/cancers17060965
Chicago/Turabian StyleDomínguez-Prieto, Víctor, Miguel León-Arellano, Rocío Olivera-Salazar, Luz Vega-Clemente, Cristina Caramés, Eva Ruiz-Hispán, Raquel Fuentes-Mateos, Diana Rosero-Rodríguez, Héctor Guadalajara, Mariano García-Arranz, and et al. 2025. "Pre-Treatment SEPTIN9 Gene Methylation Ratio Predicts Tumor Response to Total Neoadjuvant Therapy in Patients with Locally Advanced Rectal Cancer" Cancers 17, no. 6: 965. https://doi.org/10.3390/cancers17060965
APA StyleDomínguez-Prieto, V., León-Arellano, M., Olivera-Salazar, R., Vega-Clemente, L., Caramés, C., Ruiz-Hispán, E., Fuentes-Mateos, R., Rosero-Rodríguez, D., Guadalajara, H., García-Arranz, M., & García-Olmo, D. (2025). Pre-Treatment SEPTIN9 Gene Methylation Ratio Predicts Tumor Response to Total Neoadjuvant Therapy in Patients with Locally Advanced Rectal Cancer. Cancers, 17(6), 965. https://doi.org/10.3390/cancers17060965