Real-World Insights into the Impact of Durvalumab on Stage III Unresectable Non-Small Cell Lung Cancer—A Narrative Review

 , , , , , and
, , , , , and
Simple Summary
Abstract
1. Introduction
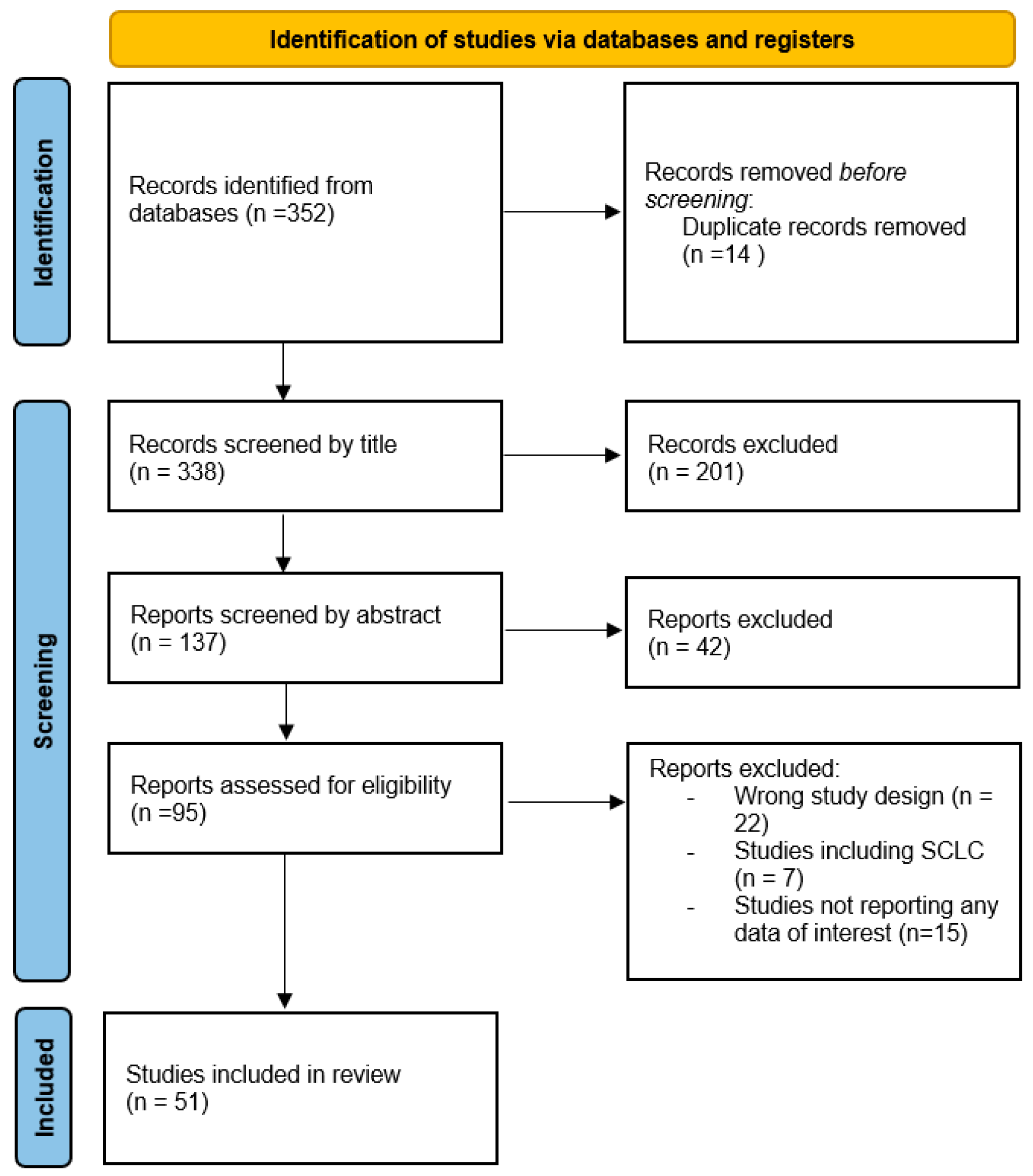
2. Materials and Methods
3. Results and Discussion
3.1. Patient Characteristics
3.2. Prognostic Factors
3.3. Chemo-Radiotherapy Regimen
3.4. Immune-Related Pneumonitis
3.5. PD-L1 and Driver Mutations
3.6. Treatment Beyond Progression
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Casal-Mouriño, A.; Ruano-Ravina, A.; Lorenzo-González, M.; Rodríguez-Martínez, Á.; Giraldo-Osorio, A.; Varela-Lema, L.; Pereiro-Brea, T.; Barros-Dios, J.M.; Valdés-Cuadrado, L.; Pérez-Ríos, M. Epidemiology of stage III lung cancer: Frequency, diagnostic characteristics, and survival. Transl. Lung Cancer Res. 2021, 10, 506–518. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Antonia, S.J.; Villegas, A.; Daniel, D.; Vicente, D.; Murakami, S.; Hui, R.; Yokoi, T.; Chiappori, A.; Lee, K.H.; De Wit, M.; et al. Durvalumab after Chemoradiotherapy in Stage III Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2017, 377, 1919–1929. [Google Scholar] [CrossRef] [PubMed]
- Hui, R.; Özgüroğlu, M.; Villegas, A.; Daniel, D.; Vicente, D.; Murakami, S.; Yokoi, T.; Chiappori, A.; Lee, K.H.; de Wit, M.; et al. Patient-reported outcomes with durvalumab after chemoradiotherapy in stage III, unresectable non-small-cell lung cancer (PACIFIC): A randomised, controlled, phase 3 study. Lancet Oncol. 2019, 20, 1670–1680. [Google Scholar] [CrossRef] [PubMed]
- Hsu, R.; Arter, Z.L.; Poei, D.; Benjamin, D.J. A narrative review on perioperative systemic therapy in non-small cell lung cancer. Explor. Target. Anti-tumor Ther. 2024, 5, 931–954. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Filippi, A.; Bar, J.; Chouaid, C.; Christoph, D.; Field, J.; Fietkau, R.; Garassino, M.; Garrido, P.; Haakensen, V.; Kao, S.; et al. Real-world outcomes with durvalumab after chemoradiotherapy in patients with unresectable stage III NSCLC: Interim analysis of overall survival from PACIFIC-R. ESMO Open 2024, 9, 103464. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Guberina, M.; Guberina, N.; Pöttgen, C.; Gauler, T.; Richlitzki, C.; Metzenmacher, M.; Wiesweg, M.; Plönes, T.; Forsting, M.; Wetter, A.; et al. Effectiveness of durvalumab consolidation in stage III non-small-cell lung cancer: Focus on treatment selection and prognostic factors. Immunotherapy 2022, 14, 927–944. [Google Scholar] [CrossRef] [PubMed]
- Moore, A.M.; Nooruddin, Z.; Reveles, K.R.; Datta, P.; Whitehead, J.M.; Franklin, K.; Alkadimi, M.; Williams, M.H.; Williams, R.A.; Smith, S.; et al. Durvalumab Treatment Patterns for Patients with Unresectable Stage III Non-Small Cell Lung Cancer in the Veterans Health Administration (VHA): A Nationwide, Real-World Study. Curr. Oncol. 2023, 30, 8411–8423. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Waterhouse, D.; Yong, C.; Frankart, A.; Brannman, L.; Mulrooney, T.; Robert, N.; Aguilar, K.M.; Ndukum, J.; Cotarla, I. Durvalumab real-world treatment patterns and outcomes in patients with stage III non-small-cell lung cancer treated in a US community setting. Futur. Oncol. 2023, 19, 1905–1916. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Zhao, J.J.; Soon, Y.Y.; Wong, A.; Aminkeng, F.; Ang, Y.; Asokumaran, Y.; Low, J.L.; Lee, M.; Choo, J.R.E.; et al. Real-world experience of consolidation durvalumab after concurrent chemoradiotherapy in stage III non-small cell lung cancer. Thorac. Cancer 2022, 13, 3152–3161. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Preti, B.T.B.; Sanatani, M.S.; Breadner, D.; Lakkunarajah, S.; Scott, C.; Esmonde-White, C.; McArthur, E.; Rodrigues, G.; Chaudhary, M.; Mutsaers, A.; et al. Real-World Analysis of Durvalumab after Chemoradiation in Stage III Non-Small-Cell Lung Cancer. Curr. Oncol. 2023, 30, 7713–7721. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sankar, K.; Bryant, A.K.; Strohbehn, G.W.; Zhao, L.; Elliott, D.; Moghanaki, D.; Kelley, M.J.; Ramnath, N.; Green, M.D. Real World Outcomes versus Clinical Trial Results of Durvalumab Maintenance in Veterans with Stage III Non-Small Cell Lung Cancer. Cancers 2022, 14, 614. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Verschueren, M.V.; Dijs, T.; Gulikers, J.L.; van Veelen, A.; Croes, S.; EL Hendriks, L.; Smit, A.A.; Bloem, L.T.; Egberts, A.C.; van de Garde, E.M.; et al. Durvalumab after chemoradiotherapy in patients with stage III non-small-cell lung cancer: Real-world outcomes versus clinical trial results. Immunotherapy 2023, 15, 839–851. [Google Scholar] [CrossRef] [PubMed]
- Saad, A.; Goldstein, J.; Appel, S.; Daher, S.; Urban, D.; Onn, A.; Gantz-Sorotsky, H.; Lobachov, A.; Gottfried, T.; Spieler, B.; et al. Chemoradiation followed by adjuvant durvalumab in stage III non-small cell lung cancer: Real-world comparison of treatment outcomes to historical controls treated with chemoradiation alone. Thorac. Cancer 2022, 13, 1763–1771. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Borghetti, P.; Volpi, G.; Facheris, G.; Cossali, G.; Mataj, E.; La Mattina, S.; Singh, N.; Imbrescia, J.; Bonù, M.L.; Tomasini, D.; et al. Unresectable stage III non-small cell lung cancer: Could durvalumab be safe and effective in real-life clinical scenarios? Results of a single-center experience. Front. Oncol. 2023, 13, 1208204. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Avrillon, V.; Daniel, C.; Boisselier, P.; Le Péchoux, C.; Chouaid, C. Nationwide Real-Life Safety and Treatment Exposure Data on Durvalumab After Concurrent Chemoradiotherapy in Unresectable Stage III, Locally Advanced, Non-small Cell Lung Cancer: Analysis of Patients Enrolled in the French Early Access Program. Lung 2022, 200, 95–105. [Google Scholar] [CrossRef] [PubMed]
- Denault, M.-H.; Feng, J.; Kuang, S.; Shokoohi, A.; Leung, B.; Liu, M.; Berthelet, E.; Laskin, J.; Sun, S.; Zhang, T.; et al. Beyond PACIFIC: Real-World Outcomes of Adjuvant Durvalumab According to Treatment Received and PD-L1 Expression. Curr. Oncol. 2023, 30, 7499–7507. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Girard, N.; Bar, J.; Garrido, P.; Garassino, M.C.; McDonald, F.; Mornex, F.; Filippi, A.R.; Smit, H.J.; Peters, S.; Field, J.K.; et al. Treatment Characteristics and Real-World Progression-Free Survival in Patients With Unresectable Stage III NSCLC Who Received Durvalumab After Chemoradiotherapy: Findings From the PACIFIC-R Study. J. Thorac. Oncol. 2022, 18, 181–193. [Google Scholar] [CrossRef] [PubMed]
- Park, C.-K.; Oh, H.-J.; Kim, Y.-C.; Kim, Y.-H.; Ahn, S.-J.; Jeong, W.G.; Lee, J.Y.; Lee, J.C.; Choi, C.M.; Ji, W.; et al. Korean Real-World Data on Patients With Unresectable Stage III NSCLC Treated With Durvalumab After Chemoradiotherapy: PACIFIC-KR. J. Thorac. Oncol. 2023, 18, 1042–1054. [Google Scholar] [CrossRef] [PubMed]
- Takeda, Y.; Kusaba, Y.; Tsukita, Y.; Uemura, Y.; Miyauchi, E.; Yamamoto, T.; Mayahara, H.; Hata, A.; Nakayama, H.; Tanaka, S.; et al. The efficacy profiles of concurrent chemoradiotherapy with intensity-modulated radiotherapy followed by durvalumab in patients with unresectable stage III non-small cell lung cancer: A multicenter retrospective cohort study. Clin. Transl. Radiat. Oncol. 2022, 37, 57–63. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Rueda, A.G.; Taus, Á.; Álvarez, R.Á.; Bernabé-Caro, R.; Chara, L.; López-Brea, M.; Vilà, L.; González, M.Á.S.; Aldagalán, A.d.B.D.; Herrera, B.E.; et al. Spanish Lung Cancer Group. The S-REAL study: Spanish real-world data on unresectable stage III NSCLC patients treated with durvalumab after chemoradiotherapy. Clin. Transl. Oncol. 2024, 26, 1779–1789. [Google Scholar] [CrossRef] [PubMed]
- Stevens, S.; Nindra, U.; Shahnam, A.; Wei, J.; Bray, V.; Pal, A.; Yip, P.Y.; Linton, A.; Blinman, P.; Nagrial, A.; et al. Real world efficacy and toxicity of consolidation durvalumab following chemoradiotherapy in older Australian patients with unresectable stage III non-small cell lung cancer. J. Geriatr. Oncol. 2024, 15, 101705. [Google Scholar] [CrossRef] [PubMed]
- Kakiuchi, Y.; Saruwatari, K.; Murotani, K.; Tokito, T.; Iriki, T.; Iwakawa, J.; Sakata, Y.; Shingu, N.; Saeki, S.; Inaba, M.; et al. Real-World Efficacy and Safety of Durvalumab Administration Following Chemoradiotherapy in Elderly Patients With Unresectable Locally Advanced Nonsmall Cell Lung Cancer: A Multicenter, Retrospective Study. Clin. Lung Cancer 2024, 25, 661–671.e7. [Google Scholar] [CrossRef] [PubMed]
- Trinh, J.Q.; Xiong, Y.; Smith, L.M.; Abughanimeh, O.; Marr, A.S.; Ganti, A.K. Durvalumab Outcomes in Stage III Non-small Cell Lung Cancer: A Single-institution Study. Anticancer. Res. 2024, 44, 605–612. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Tian, Y.; Zheng, L.; Sun, X.; Zhao, Z.; Zheng, Y.; Tian, J. Efficacy and safety of consolidation durvalumab after chemoradiation therapy for stage III non-small-cell lung cancer: A systematic review, meta-analysis, and meta-regression of real-world studies. Front. Pharmacol. 2023, 14, 1103927. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Bryant, A.K.; Sankar, K.; Strohbehn, G.W.; Zhao, L.; Daniel, V.; Elliott, D.; Ramnath, N.; Green, M.D. Prognostic and Predictive Role of PD-L1 Expression in Stage III Non-small Cell Lung Cancer Treated With Definitive Chemoradiation and Adjuvant Durvalumab. Int. J. Radiat. Oncol. 2022, 113, 752–758. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Aupérin, A.; Le Péchoux, C.; Rolland, E.; Curran, W.J.; Furuse, K.; Fournel, P.; Belderbos, J.; Clamon, G.; Ulutin, H.C.; Paulus, R.; et al. Meta-analysis of concomitant versus sequential radiochemotherapy in locally advanced non-small-cell lung cancer. J. Clin. Oncol. 2010, 28, 2181–2190. [Google Scholar] [CrossRef] [PubMed]
- Bradley, J.D.; Paulus, R.; Komaki, R.; Masters, G.; Blumenschein, G.; Schild, S.; Bogart, J.; Hu, C.; Forster, K.; Magliocco, A.; et al. Standard-dose versus high-dose conformal radiotherapy with concurrent and consolidation carboplatin plus paclitaxel with or without cetuximab for patients with stage IIIA or IIIB non-small-cell lung cancer (RTOG 0617): A randomised, two-by-two factorial phase 3 study. Lancet Oncol. 2015, 16, 187–199. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Stana, M.; Grambozov, B.; Karner, J.; Gollner, I.; Gaisberger, C.; Ruznic, E.; Zellinger, B.; Moosbrugger, R.; Studnicka, M.; Fastner, G.; et al. Chemo-Radio-Immunotherapy for NSCLC III: ESR/ATS Thresholds for DLCO Correlate with Radiation Dosimetry and Pneumonitis Rate. Cancers 2023, 15, 1966. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Wass, R.; Hochmair, M.; Kaiser, B.; Grambozov, B.; Feurstein, P.; Weiß, G.; Moosbrugger, R.; Sedlmayer, F.; Lamprecht, B.; Studnicka, M.; et al. Durvalumab after Sequential High Dose Chemoradiotherapy versus Standard of Care (SoC) for Stage III NSCLC: A Bi-Centric Trospective Comparison Focusing on Pulmonary Toxicity. Cancers 2022, 14, 3226. [Google Scholar] [CrossRef]
- Riudavets, M.; Auclin, E.; Mosteiro, M.; Dempsey, N.; Majem, M.; Lobefaro, R.; López-Castro, R.; Bosch-Barrera, J.; Pilotto, S.; Escalera, E.; et al. Durvalumab consolidation in patients with unresectable stage III non-small cell lung cancer with driver genomic alterations. Eur. J. Cancer 2022, 167, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Gao, R.W.; Day, C.N.; Yu, N.Y.; Bush, A.; Amundson, A.C.; Prodduturvar, P.; Majeed, U.; Butts, E.; Oliver, T.; Schwecke, A.J.; et al. Dosimetric predictors of pneumonitis in locally advanced non-small cell lung cancer patients treated with chemoradiation followed by durvalumab. Lung Cancer 2022, 170, 58–64. [Google Scholar] [CrossRef] [PubMed]
- Pennock, M.; Halmos, B.; Bodner, W.; Cheng, H.; Gucalp, R.; Ohri, N. Exploring causes and consequences of early discontinuation of durvalumab after chemoradiotherapy for non-small cell lung cancer. Clin. Transl. Radiat. Oncol. 2023, 41, 100643. [Google Scholar] [CrossRef]
- Edwards, D.M.; Sankar, K.; Alseri, A.; Jiang, R.; Schipper, M.; Miller, S.; Dess, K.; Strohbehn, G.W.; Elliott, D.A.; Moghanaki, D.; et al. Pneumonitis After Chemoradiotherapy and Adjuvant Durvalumab in Stage III Non-Small Cell Lung Cancer. Int. J. Radiat. Oncol. 2023, 118, 963–970. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Zhang, T.; Huang, Y.; Li, W.; Zhao, J.; Yang, Y.; Li, C.; Wang, L.; Bi, N. Real-World Safety and Efficacy of Consolidation Durvalumab After Chemoradiation Therapy for Stage III Non-small Cell Lung Cancer: A Systematic Review and Meta-analysis. Int. J. Radiat. Oncol. 2021, 112, 1154–1164. [Google Scholar] [CrossRef] [PubMed]
- LeClair, J.N.; Merl, M.Y.; Cohenuram, M.; Luon, D. Real-World Incidence of Pneumonitis in Patients Receiving Durvalumab. Clin. Lung Cancer 2021, 23, 34–42. [Google Scholar] [CrossRef] [PubMed]
- Shirasawa, M.; Yoshida, T.; Imabayashi, T.; Okuma, K.; Matsumoto, Y.; Masuda, K.; Shinno, Y.; Okuma, Y.; Goto, Y.; Horinouchi, H.; et al. Baseline PD-L1 expression and tumour-infiltrated lymphocyte status predict the efficacy of durvalumab consolidation therapy after chemoradiotherapy in unresectable locally advanced patients with non-small-cell lung cancer. Eur. J. Cancer 2021, 162, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Guo, M.Z.; Murray, J.C.; Ghanem, P.; Voong, K.R.; Hales, R.K.; Ettinger, D.; Lam, V.K.; Hann, C.L.; Forde, P.M.; Brahmer, J.R.; et al. Definitive Chemoradiation and Durvalumab Consolidation for Locally Advanced, Unresectable KRAS-mutated Non-Small Cell Lung Cancer. Clin. Lung Cancer 2022, 23, 620–629. [Google Scholar] [CrossRef] [PubMed]
- Abe, T.; Iino, M.; Saito, S.; Aoshika, T.; Ryuno, Y.; Ohta, T.; Igari, M.; Hirai, R.; Kumazaki, Y.; Miura, Y.; et al. Comparison of the Efficacy and Toxicity of Concurrent Chemoradiotherapy and Durvalumab and Concurrent Chemoradiotherapy Alone for Locally Advanced Non-small Cell Lung Cancer With N3 Lymph Node Metastasis. Anticancer. Res. 2023, 43, 675–682. [Google Scholar] [CrossRef] [PubMed]
- Storm, B.N.; Kalkhoran, H.A.; Wilms, E.B.; Brocken, P.; Codrington, H.; Houtsma, D.; Portielje, J.E.; de Glas, N.; van der Ziel, D.; Bos, F.v.D.; et al. Real-life safety of PD-1 and PD-L1 inhibitors in older patients with cancer: An observational study. J. Geriatr. Oncol. 2022, 13, 997–1002. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Deng, G.; Liang, N.; Hu, P.; Zhang, Y.; Qiao, L.; Zhang, Y.; Xie, J.; Luo, H.; Wang, F.; et al. Chemoradiotherapy Combined with Immunotherapy in Stage III Non-Small Cell Lung Cancer: A Systematic Review and Meta-Analysis of Efficacy and Safety Outcomes. Oncology 2023, 102, 382–398. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, T.; Tsukita, Y.; Katagiri, Y.; Matsushita, H.; Umezawa, R.; Ishikawa, Y.; Takahashi, N.; Suzuki, Y.; Takeda, K.; Miyauchi, E.; et al. Durvalumab after chemoradiotherapy for locally advanced non-small cell lung cancer prolonged distant metastasis-free survival, progression-free survival and overall survival in clinical practice. BMC Cancer 2022, 22, 364. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Taugner, J.; Käsmann, L.; Karin, M.; Eze, C.; Flörsch, B.; Guggenberger, J.; Li, M.; Tufman, A.; Reinmuth, N.; Duell, T.; et al. Planning target volume as a predictor of disease progression in inoperable stage III non-small cell lung cancer patients treated with chemoradiotherapy and concurrent and/or sequential immune checkpoint inhibition. Investig. New Drugs 2021, 40, 163–171. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Qiu, G.; Wang, F.; Xie, X.; Liu, T.; Zeng, C.; Chen, Z.; Zhou, M.; Deng, H.; Yang, Y.; Lin, X.; et al. A retrospective real-world experience of immunotherapy in patients with extensive stage small-cell lung cancer. Cancer Med. Cancer Med. 2023, 12, 14881–14891. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Park, C.-K.; Jeon, N.; Park, H.-K.; Oh, H.-J.; Kim, Y.-C.; Jeon, H.-L.; Kim, Y.-H.; Ahn, S.-J.; Oh, I.-J. A Propensity-Matched Retrospective Comparative Study with Historical Control to Determine the Real-World Effectiveness of Durvalumab after Concurrent Chemoradiotherapy in Unresectable Stage III Non-Small Cell Lung Cancer. Cancers 2023, 15, 1606. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Lebow, E.S.; Shepherd, A.; Eichholz, J.E.; Offin, M.; Gelblum, D.Y.; Wu, A.J.; Simone, C.B.; Schoenfeld, A.J.; Jones, D.R.; Rimner, A.; et al. Analysis of Tumor Mutational Burden, Progression-Free Survival, and Local-Regional Control in Patents with Locally Advanced Non-Small Cell Lung Cancer Treated With Chemoradiation and Durvalumab. JAMA Netw. Open 2023, 6, e2249591. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Spigel, D.R.; Faivre-Finn, C.; Gray, J.E.; Vicente, D.; Planchard, D.; Paz-Ares, L.; Vansteenkiste, J.F.; Garassino, M.C.; Hui, R.; Quantin, X.; et al. Five-Year Survival Outcomes From the PACIFIC Trial: Durvalumab After Chemoradiotherapy in Stage III Non-Small-Cell Lung Cancer. J. Clin. Oncol. 2022, 40, 1301–1311, Erratum in: J. Clin. Oncol. 2022, 40, 1965. https://doi.org/10.1200/JCO.22.01023. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Liu, Y.; Zhang, Z.; Rinsurongkawong, W.; Gay, C.M.; Le, X.; Ning, M.S.; Lewis, J.; Rinsurongkawong, V.; Lee, J.J.; Roth, J.; et al. Association of Driver Oncogene Variations With Outcomes in Patients With Locally Advanced Non-Small Cell Lung Cancer Treated With Chemoradiation and Consolidative Durvalumab. JAMA Netw. Open 2022, 5, e2215589. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Liu, J.; Bratton, E.; Yu, X.B.; Ladbury, C.; Wagner, J.B.; West, H.; Massarelli, E.; Salgia, R.; Pathak, R.; Villaflor, V.; et al. Patterns of Care in Maintenance Therapy in US Patients Undergoing Definitive Chemoradiation for Stage 3 Non-Small Cell Lung Cancer (NSCLC). Am. J. Clin. Oncol. 2022, 45, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Diamond, B.H.; Belani, N.; Masel, R.; DeCarli, K.; DiPetrillo, T.; Hepel, J.T.; Azzoli, C.G.; Khurshid, H.; Abbas, A.; Koffer, P.P. Predictors of Pneumonitis in Patients With Locally Advanced Non-Small Cell Lung Cancer Treated With Definitive Chemoradiation Followed by Consolidative Durvalumab. Adv. Radiat. Oncol. 2022, 8, 101130. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Hasegawa, T.; Ariyasu, R.; Tanaka, H.; Saito, R.; Kawashima, Y.; Horiike, A.; Sakatani, T.; Tozuka, T.; Shiihara, J.; Saiki, M.; et al. Subsequent treatment for locally advanced non-small-cell lung cancer that progressed after definitive chemoradiotherapy and consolidation therapy with durvalumab: A multicenter retrospective analysis (TOPGAN 2021-02). Cancer Chemother. Pharmacol. 2023, 92, 29–37. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.; Zhong, W.; Luo, Y.; Wu, C. The timing of durvalumab administration affects the risk of pneumonitis in patients with locally advanced non-small cell lung cancer: A systematic review and meta-analysis. BMC Cancer 2023, 23, 926. [Google Scholar] [CrossRef] [PubMed]
- Borghetti, P.; Imbrescia, J.; Volpi, G.; Scotti, V.; Aquilano, M.; Bruni, A.; Franceschini, D.; Ursino, S.; Ciammella, P.; Piperno, G.; et al. Chemo-radiotherapy plus durvalumab for loco-regional relapse of resected NSCLC. Radiat. Oncol. 2022, 17, 124. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Boys, E.; Gao, B.; Hui, R.; da Silva, I.; Hau, E.; Gee, H.; Nagrial, A. Use of durvalumab in stage III non-small-cell lung cancer based on eligibility for the PACIFIC study. Thorac. Cancer 2023, 14, 563–572. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- National Institute of Cancer. Common Terminology Criteria for Adverse Events (CTCAE); NIH Publication: Bethesda, MA, USA, 2010; Volume 2009, pp. 1–71. [Google Scholar] [CrossRef]
- Geng, Q.; Jiao, P.; Jin, P.; Su, G.; Dong, J.; Yan, B. PD-1/PD-L1 Inhibitors for Immuno-oncology: From Antibodies to Small Molecules. Curr. Pharm. Des. 2018, 23, 6033–6041. [Google Scholar] [CrossRef]
- Guo, X.; Chen, S.; Wang, X.; Liu, X. Immune-related pulmonary toxicities of checkpoint inhibitors in non-small cell lung cancer: Diagnosis, mechanism, and treatment strategies. Front. Immunol. 2023, 4, 14. [Google Scholar] [CrossRef]
- Miura, Y.; Mouri, A.; Kaira, K.; Yamaguchi, O.; Shiono, A.; Hashimoto, K.; Nishihara, F.; Shinomiya, S.; Akagami, T.; Murayama, Y.; et al. Chemoradiotherapy followed by durvalumab in patients with unresectable advanced non-small cell lung cancer: Management of adverse events. Thorac. Cancer 2020, 11, 1280–1287. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Inoue, H.; Ono, A.; Kawabata, T.; Mamesaya, N.; Kawamura, T.; Kobayashi, H.; Omori, S.; Wakuda, K.; Kenmotsu, H.; Naito, T.; et al. Clinical and radiation dose-volume factors related to pneumonitis after treatment with radiation and durvalumab in locally advanced non-small cell lung cancer. Investig. New Drugs 2020, 38, 1612–1617, Erratum in: Investig. New Drugs 2021, 39, 899. https://doi.org/10.1007/s10637-020-00969-4. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Saito, S.; Abe, T.; Kobayashi, N.; Aoshika, T.; Ryuno, Y.; Igari, M.; Hirai, R.; Kumazaki, Y.; Miura, Y.; Kaira, K.; et al. Incidence and dose-volume relationship of radiation pneumonitis after concurrent chemoradiotherapy followed by durvalumab for locally advanced non-small cell lung cancer. Clin. Transl. Radiat. Oncol. 2020, 23, 85–88. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Jung, H.A.; Noh, J.M.; Sun, J.-M.; Lee, S.-H.; Ahn, J.S.; Ahn, M.-J.; Pyo, H.; Ahn, Y.C.; Park, K. Real world data of durvalumab consolidation after chemoradiotherapy in stage III non-small-cell lung cancer. Lung Cancer 2020, 146, 23–29. [Google Scholar] [CrossRef] [PubMed]
- Mayahara, H.; Uehara, K.; Harada, A.; Kitatani, K.; Yabuuchi, T.; Miyazaki, S.; Ishihara, T.; Kawaguchi, H.; Kubota, H.; Okada, H.; et al. Predicting factors of symptomatic radiation pneumonitis induced by durvalumab following concurrent chemoradiotherapy in locally advanced non-small cell lung cancer. Radiat. Oncol. 2022, 17, 7. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Hellyer, J.A.; Aredo, J.V.; Das, M.; Ramchandran, K.; Padda, S.K.; Neal, J.W.; Wakelee, H.A. Role of Consolidation Durvalumab in Patients With EGFR- and HER2-Mutant Unresectable Stage III NSCLC. J. Thorac. Oncol. 2021, 16, 868–872. [Google Scholar] [CrossRef] [PubMed]
- Ruznic, E.; Klebermass, M.; Zellinger, B.; Langer, B.; Grambozov, B.; Purevdorj, A.; Karner, J.; Gruber, G.; Stana, M.; Minasch, D.; et al. Immunotherapy Improves Clinical Outcome in Kirsten Rat Sarcoma Virus-Mutated Patients with Unresectable Non-Small Cell Lung Cancer Stage III: A Subcohort Analysis of the Austrian Radio-Oncological Lung Cancer Study Association Registry (ALLSTAR). J. Clin. Med. 2025, 14, 945. [Google Scholar] [CrossRef] [PubMed]
- Aredo, J.V.; Wakelee, H.A.; Hui, A.B.-Y.; Padda, S.K.; Joshi, N.D.; Guo, H.H.; Chaudhuri, A.; Diehn, M.; Loo, B.W.; Neal, J.W. Induction EGFR tyrosine kinase inhibitors prior to definitive chemoradiotherapy in unresectable stage III EGFR-mutated non-small cell lung cancer. Cancer Treat. Res. Commun. 2022, 33, 100659. [Google Scholar] [CrossRef] [PubMed]
- Lu, S.; Kato, T.; Dong, X.; Ahn, M.-J.; Quang, L.-V.; Soparattanapaisarn, N.; Inoue, T.; Wang, C.-L.; Huang, M.; Yang, J.C.-H.; et al. Osimertinib after Chemoradiotherapy in Stage III EGFR-Mutated NSCLC. N. Engl. J. Med. 2024, 391, 585–597. [Google Scholar] [CrossRef] [PubMed]
- Bartolomeo, V.; Cortiula, F.; Hendriks, L.E.; De Ruysscher, D.; Filippi, A.R. A Glimpse Into the Future for Unresectable Stage III Non-Small Cell Lung Cancer. Int. J. Radiat. Oncol. 2023, 118, 1455–1460. [Google Scholar] [CrossRef] [PubMed]
- Raben, D.; Rimner, A.; Senan, S.; Broadhurst, H.; Pellas, T.; Dennis, P.; Faivre-Finn, C. Patterns of Disease Progression with Durvalumab in Stage III Non-small Cell Lung Cancer (PACIFIC). Int. J. Radiat. Oncol. 2019, 105, 683. [Google Scholar] [CrossRef]
- Palma, D.A.; Olson, R.; Harrow, S.; Gaede, S.; Louie, A.V.; Haasbeek, C.; Mulroy, L.; Lock, M.; Rodrigues, G.B.; Yaremko, B.P.; et al. Stereotactic Ablative Radiotherapy for the Comprehensive Treatment of Oligometastatic Cancers: Long-Term Results of the SABR-COMET Phase II Randomized Trial. J. Clin. Oncol. 2020, 38, 2830–2838. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Dickhoff, C.; Unal, S.; Heineman, D.; Winkelman, J.; Braun, J.; Bahce, I.; van Dorp, M.; Senan, S.; Dahele, M. Feasibility of salvage resection following locoregional failure after chemoradiotherapy and consolidation durvalumab for unresectable stage III non-small cell lung cancer. Lung Cancer 2023, 182, 107294. [Google Scholar] [CrossRef] [PubMed]
- Miyawaki, E.; Kenmotsu, H.; Shintani, Y.; Sekine, I.; Shukuya, T.; Takayama, K.; Inoue, A.; Okamoto, I.; Kiura, K.; Takahashi, K.; et al. Efficacy of platinum agents for stage III non-small-cell lung cancer following platinum-based chemoradiotherapy: A retrospective study. BMC Cancer 2022, 22, 342. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Imai, H.; Kaira, K.; Mori, K.; Ono, A.; Akamatsu, H.; Taira, T.; Yoshino, R.; Kenmotsu, H.; Saitoh, J.-I.; Harada, H.; et al. Comparison of platinum combination re-challenge therapy and docetaxel monotherapy in non-small cell lung cancer patients previously treated with platinum-based chemoradiotherapy. SpringerPlus 2015, 4, 152. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Leighl, N.B.; Redman, M.W.; Rizvi, N.; Hirsch, F.R.; Mack, P.C.; Schwartz, L.H.; Wade, J.L.; Irvin, W.J.; Reddy, S.C.; Crawford, J.; et al. Phase II study of durvalumab plus tremelimumab as therapy for patients with previously treated anti-PD-1/PD-L1 resistant stage IV squamous cell lung cancer (Lung-MAP substudy S1400F, NCT03373760). J. Immunother. Cancer 2021, 9, e002973. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Xu, S.; Shukuya, T.; Tamura, J.; Shimamura, S.; Kurokawa, K.; Miura, K.; Miyawaki, T.; Hayakawa, D.; Asao, T.; Yamamoto, K.; et al. Heterogeneous Outcomes of Immune Checkpoint Inhibitor Rechallenge in Patients With NSCLC: A Systematic Review and Meta-Analysis. JTO Clin. Res. Rep. 2022, 3, 100309. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Moliner, L.; Spurgeon, L.; Califano, R. Controversies in NSCLC: Which second-line strategy after chemo-immunotherapy? ESMO Open 2023, 8, 100879. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]

{kind=link}
| N° pts | Age, Median | Sex, Male (%) | Race | ECOG PS ≥ 2 (%) | Comorbidity | Smoking | Histology (%) | |
|---|---|---|---|---|---|---|---|---|
| Guberina et al. [6] | 39 | 62.3 | 67 | Missing | 8 | COPD G ≥ 3 5% | Ever smoker 95% | SCC 43.6 Non-SQ 56.4 |
| Moore et al. [7] | 935 | 60 | 95 | White 78% Black 21% | 16 | CCI median: 6 pt COPD: 70% | Current 46% | SCC 50 Non-SQ 43 Other 7 |
| Waterhouse et al. [8] | 528 | 70 | 51.5 | White 70.6% Black 5.5% Missing 23.9% | 9.1 | Missing | Current 23.5% Ever smoker79.6% | SCC 45.3 Non-SQ 44.7 Other 10 |
| Huang et al. [9] | 39 | 64 | 79.5 | 97.4% Asiatic | 5.1 | Missing | Current 30.8% Ever smoker 79.5% | SCC 28.8 Non-SQ 61.1 Other 10.1 |
| Preti et al. [10] | 118 | 66,3 | 51.7 | Missing | 0.7 | Missing | Current 24.7% Ever smoker 90.6% | SCC 32.2 Non-SQ 61.9 Other 5.9 |
| Sankar et al. [11] | 1006 | 69 | Missing | White 74.1% African American 22% Other/unknown 3.9% | Missing | CCI G ≥ 6 51.3% | Current 43.2% Ever smoker 83.2% | SCC 48.2 Non-SQ 48.7 Other 3.1 |
| Verschueren et al. [12] | 106 | 64.2 | 50.9 | Missing | 0.9 | Missing | Missing | SCC 30.8 Non-SQ 60.8 Other 8.4 |
| Saad et al. [13] | 71 | 67 | 63.7 | Missing | 5.6 | Missing | Ever smoker 90.1% | SCC 32.4 Non-SQ 54.9 Other 12.7 |
| Borghetti et al. [14] | 85 | 69 | 75 | Missing | 0 | COPD 57.1% COPD G ≥ 3 13.5% | Current 42.3% Ever smoker 92.3% | SCC 40.4 Non-SQ 55.8 Other 3.8 |
| Avrillon et al. [15] | 576 | 64 | 72.9 | Missing | Missing | COPD 3.7% | Missing | SCC 39.9 Non-SQ 52.1 Other 8 |
| Denault et al. [16] | 134 | 66 | 59.7 | Asian 8.2% Non Asian 91.8% | Missing | Missing | Missing | SCC 28.3 Non-SQ 70.1 Other 1.6 |
| Girard et al. [17] | 1399 | 66 | 67.5 | Missing | 2 | Missing | Current 32.6% Ever smoker 92.1% | SCC 36 Non-SQ 64 |
| Park et al. [18] | 157 | 65 | 85.4 | Missing | 10.8 | Comorbidity 72.6% COPD 31.8% | Current 32.5% Ever smoker 80.3% | SCC 52.2 Non-SQ 40.8 Other 7 |
| Takeda et al. [19] | 107 | 70 | 76 | Missing | 0 | Missing | Missing | SCC 50 Non-SQ 43.9 Other 6.1 |
| Gomez Rueda et al. [20] | 244 | 67 | 79.9 | Missing | 3.6 | COPD 23.8% Other Cancers 23.4% | Current 63.5% Former 33.2% | SCC 45.3 Non SQ 54.7 |
| Stevens et al. [21] | 152 | 67 | 63.2 | Missing | 4.6 | COPD 32.9% Cardiovascular disease 56.6% | Current 67.7% Former 28% | SCC 32.2 Non SQ 57.2 |
| Kakiuchi et al. [22] | 208 | 69.5 | 80.3 | Missing | 1 | Missing | Ever smoker 84.6% | SCC 40.9% Non-SQ 59.1 |
| Trinh et al. [23] | 79 | 63.5 | 43 | Missing | Missing | Missing | Current 26.6% Former 68.4% | SCC 45.6% Non-SQ 48.1% Other 6.3% |
| First Author | Year | Type of Article | Number of Patients | cCHT | sCHT | I Drug Carbo Platin | I Drug Cis Platin | II Drug Paclitaxel | II Drug Etoposide | II Drug Pemetrexed | II Drug Vinorelbina | Mono-CHT CBDCA | CHT 3-Week | CHT 1-Week | Dose < 54 Gy | Dose 54–66 Gy | Dose > 66 Gy | Dose 73.8 BIG | Dose 74 Gy | nFR | hFR | 3D | IMRT | VMAT | IMRT SS | Median OS | 1-Year OS | 2-Years OS | 3-Years OS |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| % | % | % | % | % | % | % | % | % | % | % | % | % | % | % | % | % | % | % | % | % | % | months | % | % | % | ||||
| Riudavets et al. [30] | 2022 | Retrospective | 323 | 81 | 19 | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | 47 | - | - | - |
| Gao et al. [31] | 2022 | Retrospective | 190 | 87.3 | 12.6 | 83.7 | 15.3 | 80 | 13.2 | 4.7 | 0 | 0 | - | - | - | 93.7 | 5.3 | - | - | - | - | - | - | - | - | - | 87 | - | 60.3 |
| Pennock et al. [32] | 2023 | Retrospective | 59 | 100 | 0 | 100 | 0 | 100 | 0 | 0 | 0 | 0 | 0 | 100 | 11.8 | - | - | - | - | 68 | 32 | - | - | - | - | 32 | - | - | - |
| Edwards et al. [33] | 2023 | Retrospective | 1994 | - | - | 71 | 0 | 71 | 0 | 0 | 0 | 0 | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - |
| Wang et al. [34] | 2022 | Review | 1677 | 83.7 | 16.4 | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | 90 | - | - |
| LeClair et al. [35] | 2021 | Retrospective | 83 | - | - | 78.4 | 17 | 70 | 9 | 14 | 0 | 0 | - | - | 85.5 | - | - | - | - | - | - | - | - | - | - | - | - | - | |
| Shirasawa et al. [36] | 2021 | Retrospective | 551 | - | - | - | - | - | - | - | - | 13 | - | - | - | 100 | 5 | - | - | - | - | - | - | - | - | 51.8 | - | - | - |
| Guo et al. [37] | 2022 | Retrospective | 134 | 100 | 0 | 78.4 | 21.5 | 54 | 10.9 | 35 | 0 | 0 | - | - | - | 100 | - | - | - | - | - | - | - | - | - | 32.4 | - | - | - |
| Takeda et al. [19] | 2022 | Retrospective | 107 | 100 | 0 | 38.3 | 54.2 | 38.3 | 0 | 9.3 | 44.9 | 0 | - | 35.5 | - | 100 | - | - | - | - | - | 0 | 100 | 72.9 | 27.1 | - | 88 | 80 | 75 |
| Abe et al. [38] | 2023 | Retrospective | 29 | 100 | 0 | - | - | - | - | - | - | - | - | - | - | 100 | - | - | - | - | - | 66 | - | 34.5 | 0 | - | 84 | - | - |
| Storm et al. [39] | 2022 | Retrospective | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - |
| Girard et al. [17] | 2022 | Retrospective | 1399 | 76.6 | 14.4 | 37.3 | 51.2 | 27.6 | 20.4 | 10.7 | 33.1 | 0.5 | - | - | - | 41.4 | 52.4 | - | - | - | - | - | - | - | - | - | - | 71.2 | - |
| Park et al. [18] | 2023 | Retrospective | 157 | 97.5 | 2.5 | 28 | 71.6 | 93 | 4.4 | - | 0.6 | - | 5.7 | 93 | 1.9 | 96.8 | 1.3 | - | - | - | - | 37 | 57.3 | - | - | - | 88 | 71 | 69.2 |
| Li et al. [40] | 2023 | Review | 4496 | 93.2 | 6.8 | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | 87 | 48.1 | - |
| Yamamoto et al. [41] | 2022 | Retrospective | 68 | - | - | 40 | 48 | 40 | - | - | 48 | - | - | - | - | 100 | - | - | - | 100 | 0 | 0 | 100 | 100 | 0 | - | 84 | - | - |
| Taugner et al. [42] | 2021 | Prospective | 33 | 51.5 | 33.3 | - | 82 | - | - | - | 82 | - | - | - | - | 100 | - | - | - | 100 | 0 | 0 | 100 | 100 | 0 | - | 87 | - | - |
| Qiu et al. [43] | 2023 | Retrospective | 353 | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - |
| Sankar et al. [11] | 2022 | Retrospective | 1006 | 100 | 0 | 70.8 | 7.7 | 70.8 | 7.7 | 5.6 | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | 77 | 61.9 | - |
| Wass et al. [29] | 2022 | Retrospective | 78 | 46.2 | 53.8 | 70.6 | 29.4 | 0 | 0 | 52.9 | 29.5 | 3.5 | - | - | - | 46.2 | - | 53.8 | - | - | - | 0 | 100 | 100 | 0 | - | - | - | - |
| Park, Jeon et al. [44] | 2023 | Retrospective | 386 | 100 | 0 | 10.1 | 89.9 | 100 | 0 | 0 | 0 | 0 | 0 | 100 | - | - | - | - | - | - | - | - | - | - | - | - | - | 74.4 | - |
| Moore et al. [7] | 2023 | Retrospective | 935 | 98 | 2 | 88 | 11 | - | - | - | - | - | - | - | 3 | 78 | 8 | - | 1 | - | - | - | - | - | - | - | - | - | - |
| Guberina et al. [6] | 2022 | Retrospective | 160 | 96.9 | 3,1 | 5 | 78,1 | - | - | - | 81.2 | - | - | - | 0,6 | - | 5.6 | - | - | - | - | 0 | 100 | - | - | - | - | 80 | - |
| Stana et al. [28] | 2023 | Retrospective | 112 | 0 | 100 | - | - | - | - | - | - | - | - | - | - | 50 | - | 50 | - | 50 | 50 | 0 | 100 | 54 | 46 | - | - | - | - |
| Preti et al. [10] | 2023 | Retrospective | 118 | 100 | 0 | 50 | 44 | 33.8 | 27.11 | - | 0.8 | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - |
| Lebow et al. [45] | 2023 | Retrospective | 81 | 100 | 0 | 69 | 29 | 38 | 7 | 53 | 0 | 0 | - | - | - | - | - | - | - | 100 | - | - | - | - | - | - | 93 | 72 | - |
| Zhang et al. [24] | 2023 | Review | 4056 | 92 | 8 | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | 85 | - | - |
| Denault et al. [16] | 2023 | Retrospective | 453 | - | - | 64.5 | 35.4 | - | - | - | - | - | - | - | - | 97.6 | - | - | - | - | - | - | - | - | - | 37.9 | - | 71.5 | - |
| Spigel et al. [46] | 2022 | Prospective | 713 | 100 | 0 | 42.2 | 55.4 | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | 47.5 | 83 | 66.3 | 56.7 |
| Borghetti, Volpi et al. [14] | 2023 | Retrospective | 85 | 87.1 | 12.9 | 82.3 | 3.5 | 82.3 | 3.5 | - | - | - | 52 | 48.2 | - | 100 | - | - | - | 100 | - | - | 100 | 94.1 | 5.9 | 52 | 83 | 69.4 | - |
| Liu, Zhang et al. [47] | 2022 | Retrospective | 104 | 100 | 0 | 91 | 9 | 85 | 3 | 10 | 0 | 1 | - | - | - | 85 | 12 | - | - | - | - | - | - | - | - | 36.2 | - | - | |
| Bryant et al. [25] | 2022 | Retrospective | 1306 | 100 | 0 | 71.6 | 8 | - | - | 2.9 | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - |
| Liu, Bratton et al. [48] | 2022 | Retrospective | 5802 | 100 | 0 | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - |
| Diamond et al. [49] | 2023 | Retrospective | 62 | 100 | 0 | 61 | - | 61 | - | - | - | - | - | - | - | 100 | - | - | - | - | - | 0 | 100 | - | - | - | 87 | - | - |
| Hasegawa et al. [50] | 2023 | Retrospective | 127 | 98.4 | 1.6 | 41.7 | 41 | 41.7 | - | - | 13.4 | - | - | - | - | - | - | - | - | - | - | - | - | - | - | 18.2 | - | - | - |
| Huang et al. [9] | 2022 | Retrospective | 84 | 100 | 0 | 28,6 | 63.1 | 26.2 | 38.1 | 27.4 | - | - | - | - | - | 100 | - | - | - | 100 | 0 | 0 | 100 | - | - | - | 94 | 75.2 | - |
| Yang et al. [51] | 2023 | Review | 2560 | - | - | - | - | - | - | - | - | - | - | - | - | 100 | - | - | - | - | - | - | - | - | - | - | - | - | - |
| Waterhouse et al. [8] | 2023 | Retrospective | 528 | 100 | 0 | 86.6 | 10.2 | 86.6 | 10.2 | - | - | - | - | - | 3,2 | 80.3 | - | - | - | - | - | - | - | - | - | - | 84 | 64 | - |
| Verschueren et al. [12] | 2023 | Retrospective | 383 | 69.7 | 30.3 | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | 84 | - | - |
| Saad et al. [13] | 2022 | Retrospective | 215 | 96 | 4 | 67.4 | 11.6 | 67.4 | 11.6 | - | - | - | - | - | - | 100 | - | - | - | - | - | 49 | 51.2 | - | - | - | 86 | - | - |
| Avrillon et al. [15] | 2022 | Retrospective | 576 | 100 | 0 | 42.9 | 52.9 | 27.9 | 2.1 | 15.9 | 45 | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - |
| Borghetti, Imbrescia et al. [52] | 2022 | Retrospective | 24 | 75 | 25 | 66.7 | 33 | 37.5 | 12.5 | 12.5 | 16.7 | 0 | 58 | 41.7 | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - |
| Boys et al. [53] | 2022 | Retrospective | 126 | 100 | 0 | 67 | 30 | 67 | 29 | 0.08 | - | - | - | - | 10 | 90 | - | - | - | 100 | 0 | 0 | 100 | - | - | 58.7 | - | - | - |
| RT Technique | RT Dose (Median) | RT Dose Range | Lung V20 Median (%) | Lung V20, <30% (%) | Lung V20 ≥30% (%) | MLD Median (Gy) | MLD ≤18 Gy | MLD | MHD (Median) | MHD <10 Gy | MHD ≥10 Gy | N. of Cycles of Durvalumab (Median) | N. of Cycles of Durvalumab (Range) | Time to Durvalumab (Median, Days) | Time to Durvalumab (Range, Days) | Pneumonitis | G2+ Pneumonitis | G2+ Pneumonitis RT | G2+ Pneumonitis DURVA | G2+ Pneumonitis EQUIVOCAL | Grade 3+ Pneumonitis | Discontinued Durva Due to Pneumonitis | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Diamond et al. [49] | - | - | 60–64.8 | 27 | 56% | 44 | 15.5 | 77 | 23 | 9.50 Gy (6.25–14) | 55 | 45 | 17 | 8–24 | - | - | 42 | 32.30 | 24 | 6.50 | 1.6 | 9.7 | 11 |
| Avrillon et al. [15] | - | - | 45–74 | - | - | - | - | - | - | - | - | - | 16 | 1–37 | 36 | 0–157 | - | - | - | - | - | - | - |
| Huang et al. [9] | VMAT/IMRT | - | 60–66 | - | - | - | - | - | - | - | - | - | 13 | - | 38 | 28.2 | - | - | - | - | 7.7 | - | |
| Waterhouse et al. [8] | - | - | 54–66 | - | - | - | - | - | - | - | - | - | - | - | 47 | 0–434 | - | - | - | 13.4 | - | - | - |
| Saad et al. [13] | VMAT/IMRT | - | 56–66 | - | - | - | - | - | - | - | - | - | - | - | - | - | 49.3 | - | - | - | - | 5.6 | - |
| Guberina et al. [6] | VMAT/IMRT | - | 53.5–74 | - | - | - | 15.2 | - | - | - | - | - | 18 | 1–27 | 25 | 7–80 | - | - | - | - | - | - | 10.25 |
| Borghetti et al. [14] | VMAT/IMRT | 60 | - | - | - | - | - | - | - | - | - | - | - | - | 47 | 2–105 | 30.8 | 23.1 | - | - | - | 5.8 | 3.85 |
| Preti et al. [10] | - | - | - | - | - | - | - | - | - | - | - | - | - | - | 40.5 | 7–238 | 39.8 | 38.9 | 0 | 38.9 | 0 | 16.9 | - |
| Stana et al. [28] | VMAT/IMRT | 72.3 | 39–88.2 | 20 | - | - | 12 | - | - | - | - | - | 15.6 | 15.6 | - | 2 | |||||||
| Park et al. [18] | - | - | 54–66 | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | 85.7 | - | - | - | - |
| Wass et al (high dose arm) [29,43] | VMAT | 72 | - | 20.5 | - | - | 13 | - | - | - | - | - | 14 | 1–26 | 18.5 | 4–127 | 28.6 | - | - | - | - | - | - |
| Wass et al (standard of care arm) [29] | VMAT | 59,4 | - | 16 | - | - | 16.7 | - | - | - | - | - | 8 | 1–21 | 22 | 2–114 | 27.8 | - | - | - | - | - | - |
| Taugner et al. [42] | - | 63,6 | - | - | - | - | - | - | - | - | - | - | 14 | 2–24 | 25 | 13–103 | - | - | - | - | - | 15.38 | - |
| Abe et al. [38] | VMAT/3D | 60 | - | 21.5 | - | - | 12.4 | - | - | 11.7 | - | - | 7 | - | - | - | 100 | 50 | - | - | - | 0 | 25 |
| Park et al. [44] | VMAT/3D/IMRT | - | 54–66 | - | - | - | - | - | - | - | - | - | 19 | 1–32 | 32 | 0–86 | 36.6 | - | 36.3 | 14.6 | - | 1.9 | - |
| LeClair et al. [35] | - | 60 | - | - | - | - | - | - | - | - | 13.9 | 1–47 | 57.3 | 8–226 | 25.3 | 22.9 | 2.4 | - | 6 | 22.9 | |||
| Edwards et al. [33] | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | 20.9 | - | 5.57 | 9 | 6.27 | - | - |
| Gao et al. [31] | IMRT/IMPT | 60 | - | - | - | - | - | - | - | - | 12 | 4–22 | 35.5 | 27–52 | 26.3 | - | 7.4 | ||||||
| Riudavets et al. [30] | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | 21 | - | 4.6 | - |
| Miura et al. [57] | - | 60 | 54–60 | 18.9 | - | - | - | - | - | - | - | - | - | - | 11 | 1–42 | 61 | 58.5 | - | - | - | 2.4 | 53.7 |
| Inoue et al. [58] | 3D/IMRT/PRB | - | 60–64 | 22 | - | - | - | - | - | - | - | - | - | - | - | - | 73.3 | 46.7 | - | - | - | 0 | - |
| Saito et al. [59] | 3D | - | - | - | - | - | - | - | - | - | - | - | - | 6.5 | 11 | 1–39 | - | - | - | - | - | - | 47.2 |
| Jung et al. [60] | 3D/IMRT/PRB | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | 81 | 42.9 | - | - | - | 14.3 | 42.9 |
| Mayahara et al. [61] | 3D/IMRT | 60 | 54–60 | - | - | - | - | - | - | - | - | - | - | - | - | - | 89.3 | 39.3 | - | - | - | 8.9 | 39.3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Facheris, G.; Cossali, G.; Imbrescia, J.; La Mattina, S.; Mataj, E.; Meli, N.; Volpi, G.; Triggiani, L.; Guerini, A.E.; Levi, G.; et al. Real-World Insights into the Impact of Durvalumab on Stage III Unresectable Non-Small Cell Lung Cancer—A Narrative Review. Cancers 2025, 17, 874. https://doi.org/10.3390/cancers17050874
Facheris G, Cossali G, Imbrescia J, La Mattina S, Mataj E, Meli N, Volpi G, Triggiani L, Guerini AE, Levi G, et al. Real-World Insights into the Impact of Durvalumab on Stage III Unresectable Non-Small Cell Lung Cancer—A Narrative Review. Cancers. 2025; 17(5):874. https://doi.org/10.3390/cancers17050874
Chicago/Turabian StyleFacheris, Giorgio, Gianluca Cossali, Jessica Imbrescia, Salvatore La Mattina, Eneida Mataj, Nicole Meli, Giulia Volpi, Luca Triggiani, Andrea Emanuele Guerini, Guido Levi, and et al. 2025. "Real-World Insights into the Impact of Durvalumab on Stage III Unresectable Non-Small Cell Lung Cancer—A Narrative Review" Cancers 17, no. 5: 874. https://doi.org/10.3390/cancers17050874
APA StyleFacheris, G., Cossali, G., Imbrescia, J., La Mattina, S., Mataj, E., Meli, N., Volpi, G., Triggiani, L., Guerini, A. E., Levi, G., Grisanti, S., Buglione di Monale e Bastia, M., & Borghetti, P. (2025). Real-World Insights into the Impact of Durvalumab on Stage III Unresectable Non-Small Cell Lung Cancer—A Narrative Review. Cancers, 17(5), 874. https://doi.org/10.3390/cancers17050874