
HepatoPredict Accurately Selects Hepatocellular Carcinoma Patients for Liver Transplantation Regardless of Tumor Heterogeneity

 , , , , , , ,
, , , , , , ,  ,
,  and
and
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Sample Collection
2.3. Sample Analysis and Selection
2.4. HepatoPredict Assay
2.5. Performance Metrics
2.6. HepatoPredict Algorithm Retraining and Performance Assessment
2.7. Intra-Nodule and Intra-Patient (Inter-Nodule) Heterogeneity
2.8. Data Analysis and Visualization
3. Results
3.1. Demographic and Clinical Data Are Comparable Between Datasets
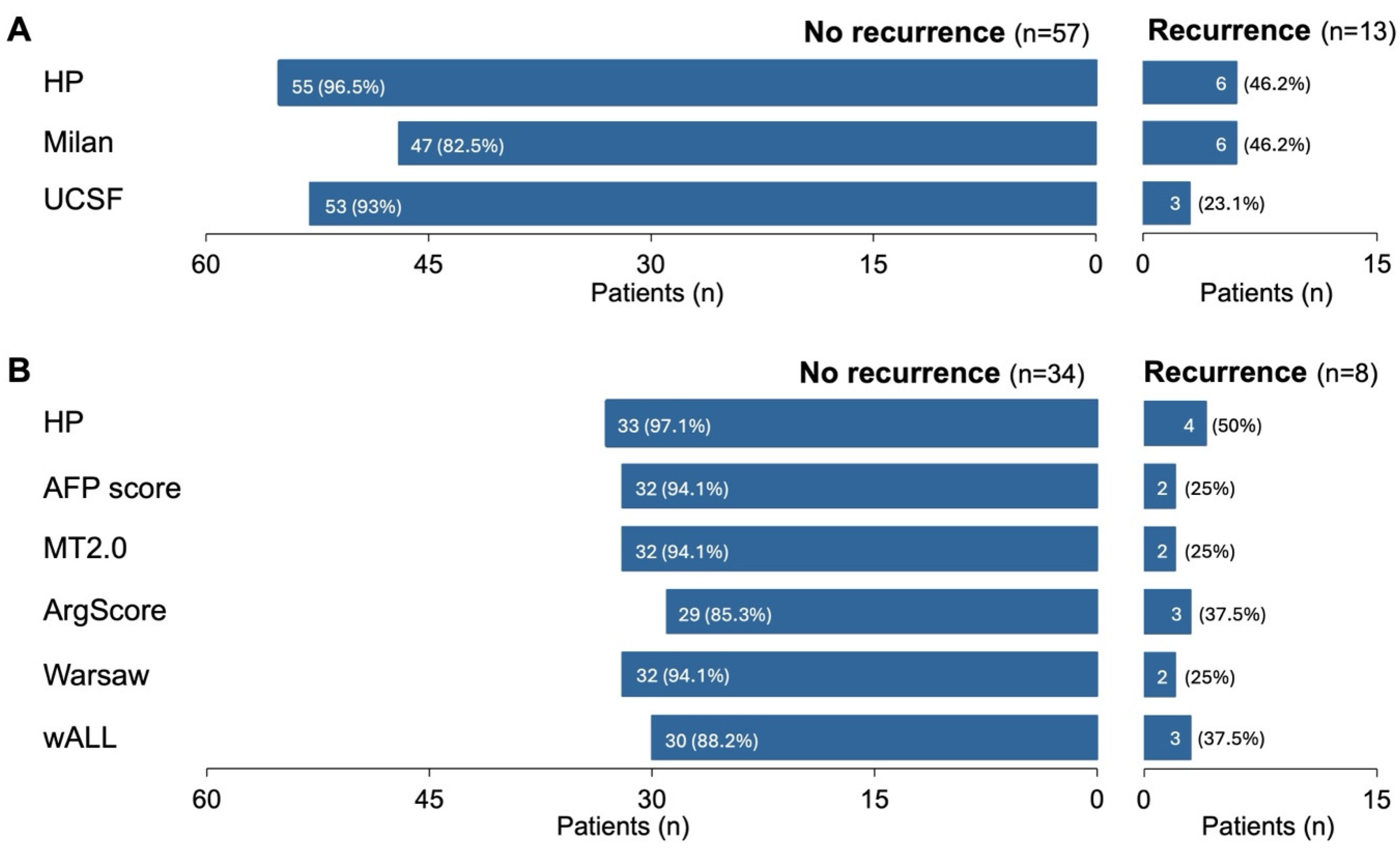
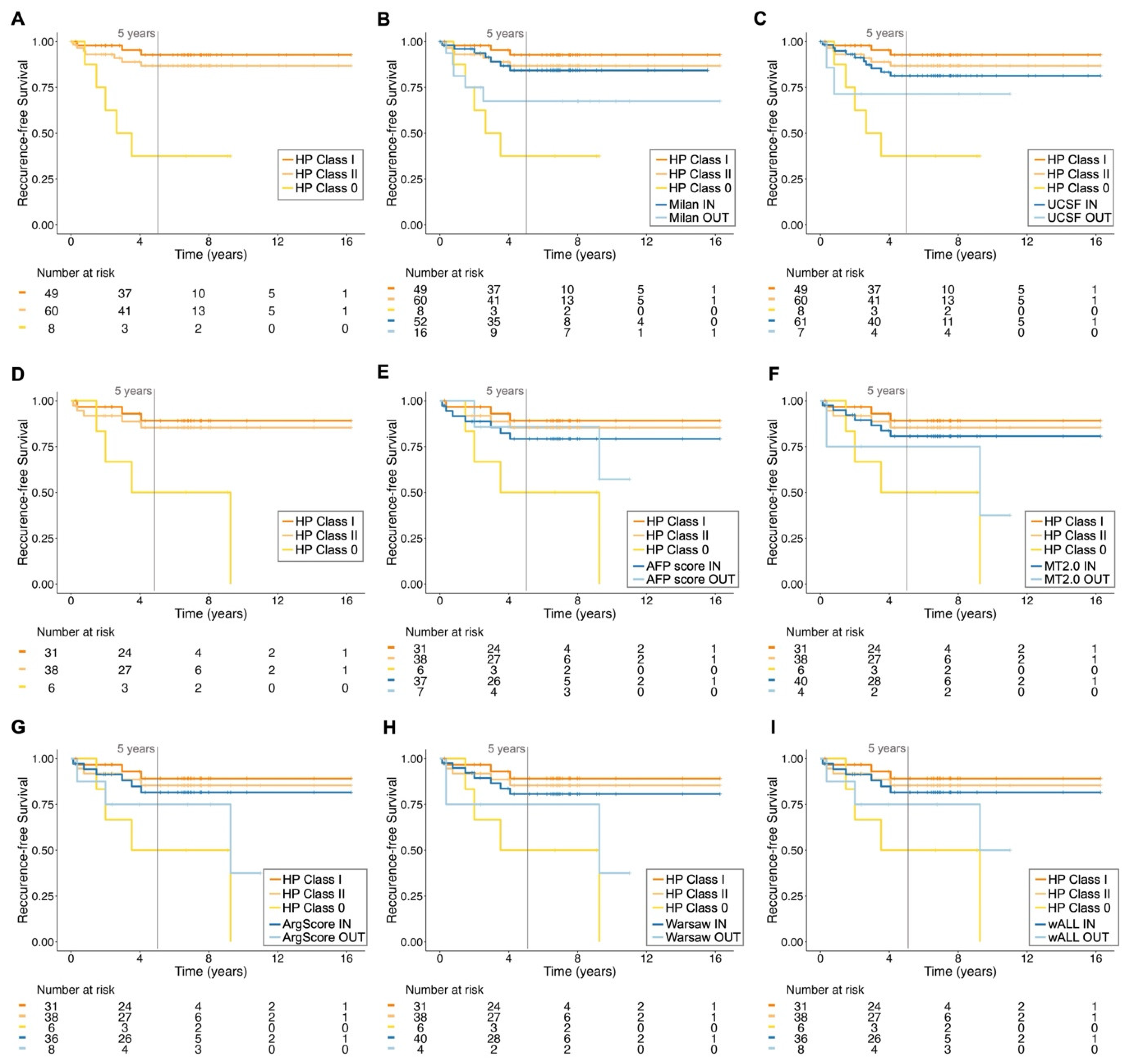
3.2. The Retrained HP Algorithm Outperforms the Current Clinically Used Criteria

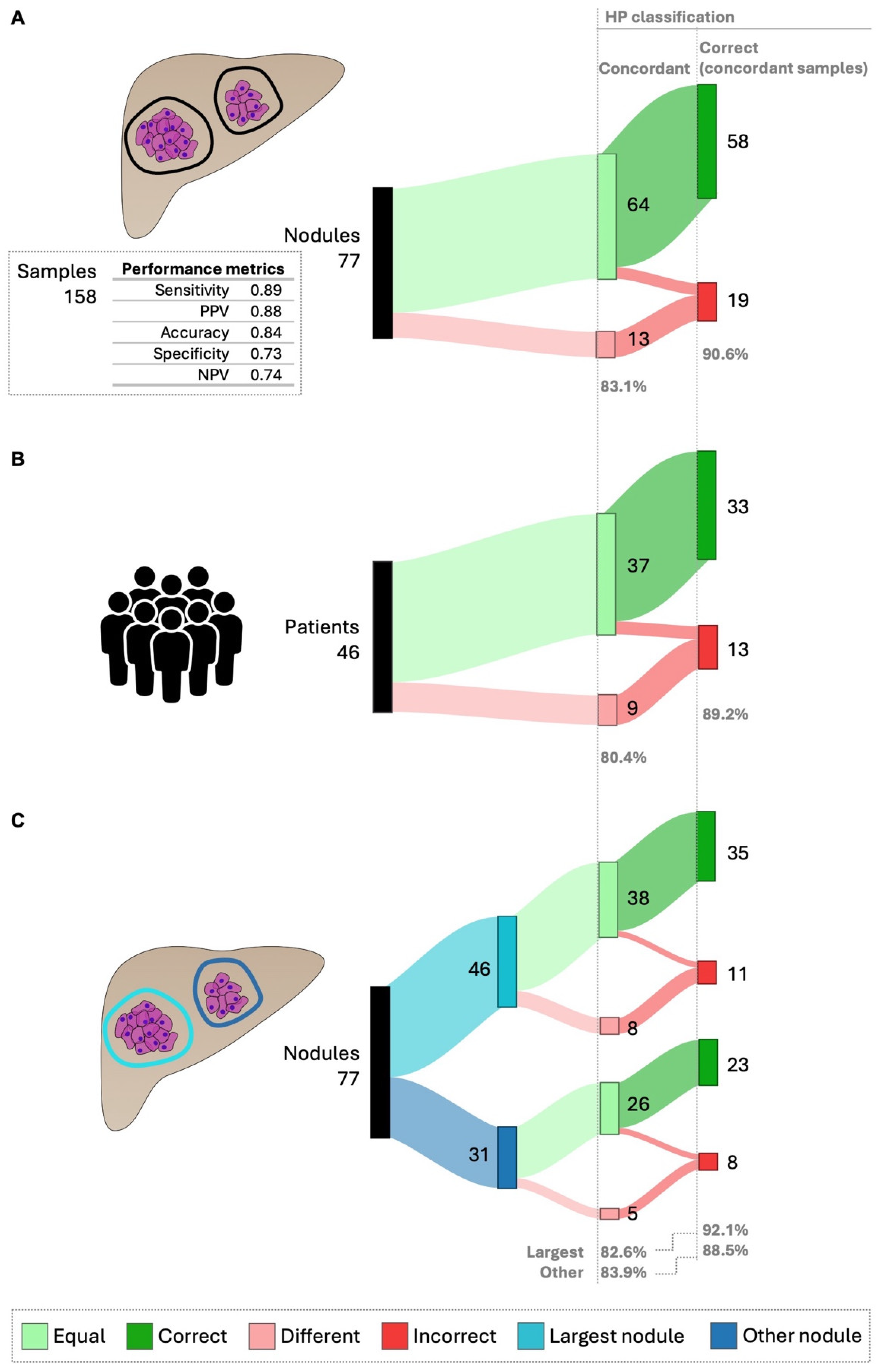
3.3. The HepatoPredict Tool Demonstrates Strong Performance Despite Intra-Nodule and Intra-Patient Heterogeneity
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AFP | alpha-fetoprotein |
| ArgScore | Argentinian score |
| DCP | des-gamma carboxyprothrombin |
| FFPE | formalin-fixed paraffin-embedded |
| HCC | hepatocellular carcinoma |
| HE | hematoxylin-eosin |
| HP | HepatoPredict |
| IQR | inter-quartile range |
| LT | liver transplantation |
| Max | maximum |
| MELD | model for end-stage liver disease |
| MT2.0 | Metroticket 2.0 |
| N | number |
| NPV | negative predictive value |
| OS | overall survival |
| PPV | positive predictive value |
| RFS | recurrence-free survival |
| RNA | ribonucleic acid |
| RT-qPCR | reverse transcriptase real-time polymerase chain reaction |
| SD | standard deviation |
| UCSF | University of California, San Francisco |
| wALL | within all criteria |
| WHO | World Health Organization |
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Philips, C.A.; Rajesh, S.; Nair, D.C.; Ahamed, R.; Abduljaleel, J.K.; Augustine, P. Hepatocellular Carcinoma in 2021: An Exhaustive Update. Cureus 2021, 13, e19274. [Google Scholar] [CrossRef]
- Amini, M.; Looha, M.A.; Zarean, E.; Pourhoseingholi, M.A. Global pattern of trends in incidence, mortality, and mortality-to-incidence ratio rates related to liver cancer, 1990–2019: A longitudinal analysis based on the global burden of disease study. BMC Public Health 2022, 22, 604. [Google Scholar] [CrossRef] [PubMed]
- Rumgay, H.; Arnold, M.; Ferlay, J.; Lesi, O.; Cabasag, C.J.; Vignat, J.; Laversanne, M.; McGlynn, K.A.; Soerjomataram, I. Global burden of primary liver cancer in 2020 and predictions to 2040. J. Hepatol. 2022, 77, 1598–1606. [Google Scholar] [CrossRef]
- Sayiner, M.; Golabi, P.; Younossi, Z.M. Disease Burden of Hepatocellular Carcinoma: A Global Perspective. Dig. Dis. Sci. 2019, 64, 910–917. [Google Scholar] [CrossRef]
- Reig, M.; Forner, A.; Rimola, J.; Ferrer-Fàbrega, J.; Burrel, M.; Garcia-Criado, Á.; Kelley, R.K.; Galle, P.R.; Mazzaferro, V.; Salem, R.; et al. BCLC strategy for prognosis prediction and treatment recommendation: The 2022 update. J. Hepatol. 2022, 76, 681–693. [Google Scholar] [CrossRef] [PubMed]
- Golabi, P.; Fazel, S.; Otgonsuren, M.; Sayiner, M.; Locklear, C.T.; Younossi, Z.M. Mortality assessment of patients with hepatocellular carcinoma according to underlying disease and treatment modalities. Medicine 2017, 96, e5904. [Google Scholar] [CrossRef]
- Mazzaferro, V.; Regalia, E.; Doci, R.; Andreola, S.; Pulvirenti, A.; Bozzetti, F.; Montalto, F.; Ammatuna, M.; Morabito, A.; Gennari, L. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. N. Engl. J. Med. 1996, 334, 693–702. [Google Scholar] [CrossRef] [PubMed]
- Mazzaferro, V.; Sposito, C.; Zhou, J.; Pinna, A.D.; de Carlis, L.; Fan, J.; Cescon, M.; Di Sandro, S.; Yi-Feng, H.; Lauterio, A.; et al. Metroticket 2.0 Model for Analysis of Competing Risks of Death After Liver Transplantation for Hepatocellular Carcinoma. Gastroenterology 2018, 154, 128–139. [Google Scholar] [CrossRef]
- Yao, F.Y.; Ferrell, L.; Bass, N.M.; Watson, J.J.; Bacchetti, P.; Venook, A.; Ascher, N.L.; Roberts, J.P. Liver transplantation for hepatocellular carcinoma: Expansion of the tumor size limits does not adversely impact survival. Hepatology 2001, 33, 1394–1403. [Google Scholar] [CrossRef]
- Notarpaolo, A.; Layese, R.; Magistri, P.; Gambato, M.; Colledan, M.; Magini, G.; Miglioresi, L.; Vitale, A.; Vennarecci, G.; Ambrosio, C.D.; et al. Validation of the AFP model as a predictor of HCC recurrence in patients with viral hepatitis-related cirrhosis who had received a liver transplant for HCC. J. Hepatol. 2017, 66, 552–559. [Google Scholar] [CrossRef] [PubMed]
- Halazun, K.J.; Najjar, M.; Abdelmessih, R.M.; Samstein, B.; Griesemer, A.D.; Guarrera, J.v.; Kato, T.; Verna, E.C.; Emond, J.C.; Brown, R.S., Jr. Recurrence after liver transplantation for hepatocellular carcinoma. Ann. Surg. 2017, 265, 557–564. [Google Scholar] [CrossRef]
- Sasaki, K.; Morioka, D.; Conci, S.; Margonis, G.A.; Sawada, Y.; Ruzzenente, A.; Kumamoto, T.; Iacono, C.; Andreatos, N.; Guglielmi, A.; et al. The Tumor Burden Score: A New “metro-ticket” Prognostic Tool for Colorectal Liver Metastases Based on Tumor Size and Number of Tumors. Ann. Surg. 2018, 267, 132–141. [Google Scholar] [CrossRef] [PubMed]
- Kaido, T.; Ogawa, K.; Mori, A.; Fujimoto, Y.; Ito, T.; Tomiyama, K.; Takada, Y.; Uemoto, S. Usefulness of the Kyoto criteria as expanded selection criteria for liver transplantation for hepatocellular carcinoma. Surgery 2013, 154, 1053–1060. [Google Scholar] [CrossRef] [PubMed]
- Lei, J.Y.; Wang, W.T.; Yan, L.N. Up-to-seven criteria for hepatocellular carcinoma liver transplantation: A single center analysis. World J. Gastroenterol. 2013, 19, 6077–6083. [Google Scholar] [CrossRef] [PubMed]
- Toso, C.; Meeberg, G.; Hernandez-Alejandro, R.; Dufour, J.F.; Marotta, P.; Majno, P.; Kneteman, N.M. Total Tumor Volume and Alpha-Fetoprotein for Selection of Transplant Candidates With Hepatocellular Carcinoma: A Prospective Validation. Hepatology 2015, 62, 158–165. [Google Scholar] [CrossRef] [PubMed]
- Macaron, C.; Hanouneh, I.A.; Lopez, R.; Aucejo, F.; Zein, N.N. Total tumor volume predicts recurrence of hepatocellular carcinoma after liver transplantation in patients beyond Milan or UCSF criteria. Transplant. Proc. 2010, 42, 4585–4592. [Google Scholar] [CrossRef] [PubMed]
- Hanif, H.; Ali, M.J.; Susheela, A.T.; Khan, I.W.; Luna-Cuadros, M.A.; Khan, M.M.; Lau, D.T.Y. Update on the applications and limitations of alpha-fetoprotein for hepatocellular carcinoma. World J. Gastroenterol. 2022, 28, 216–229. [Google Scholar] [CrossRef] [PubMed]
- Volk, M.L.; Hernandez, J.C.; Su, G.L.; Lok, A.S.; Marrero, J.A. Risk factors for hepatocellular carcinoma may impair the performance of biomarkers: A comparison of AFP, DCP, and AFP-L31. Cancer Biomark. 2007, 3, 79–87. [Google Scholar] [CrossRef] [PubMed]
- Saffroy, R.; Pham, P.; Reffas, M.; Takka, M.; Lemoine, A.; Debuire, B. New perspectives and strategy research biomarkers for hepatocellular carcinoma. Clin. Chem. Lab. Med. 2007, 45, 1169–1179. [Google Scholar] [CrossRef]
- Llovet, J.M.; Kelley, R.K.; Villanueva, A.; Singal, A.G.; Pikarsky, E.; Roayaie, S.; Lencioni, R.; Koike, K.; Zucman-Rossi, J.; Finn, R.S. Hepatocellular carcinoma. Nat. Rev. Dis. Primers 2021, 7, 6. [Google Scholar] [CrossRef]
- Wen, N.; Cai, Y.; Li, F.; Ye, H.; Tang, W.; Song, P.; Cheng, N. The clinical management of hepatocellular carcinoma worldwide: A concise review and comparison of current guidelines: 2022 update. Biosci. Trends. 2022, 16, 20–30. [Google Scholar] [CrossRef] [PubMed]
- Frazao, L.P.; Pereira-Leal, J.B.; Duvoux, C.; Cardoso, J. Role of accuracy measures in selecting hepatocellular carcinoma patients for liver transplantation A systematic review and meta-analysis. medRxiv 2024. [Google Scholar] [CrossRef]
- Lozanovski, V.J.; Ramouz, A.; Aminizadeh, E.; Al-Saegh, S.A.H.; Khajeh, E.; Probst, H.; Picardi, S.; Rupp, C.; Chang, D.H.; Probst, P.; et al. Prognostic role of selection criteria for liver transplantation in patients with hepatocellular carcinoma: A network meta-analysis. BJS Open 2022, 6, zrab130. [Google Scholar] [CrossRef]
- Mehta, N. Liver Transplantation Criteria for Hepatocellular Carcinoma, including Posttransplant Management. Clin. Liver Dis. 2021, 17, 332–336. [Google Scholar] [CrossRef] [PubMed]
- Santopaolo, F.; Lenci, I.; Milana, M.; Manzia, T.M.; Baiocchi, L. Liver transplantation for hepatocellular carcinoma: Where do we stand? World J. Gastroenterol. 2019, 25, 2591–2602. [Google Scholar] [CrossRef]
- Pinto-Marques, H.; Cardoso, J.; Silva, S.; Neto, J.L.; Gonçalves-Reis, M.; Proença, D.; Mesquita, M.; Manso, A.; Carapeta, S.; Sobral, M.; et al. A gene expression signature to select hepatocellular carcinoma patients for liver transplantation. Ann. Surg. 2022, 276, 868–874. [Google Scholar] [CrossRef]
- Gonçalves-Reis, M.; Proença, D.; Frazão, L.P.; Neto, J.L.; Silva, S.; Pinto-Marques, H.; Pereira-Leal, J.B.; Cardoso, J. Analytical validation and algorithm improvement of HepatoPredict kit to assess hepatocellular carcinoma prognosis before a liver transplantation. Pract. Lab. Med. 2024, 39, e00365. [Google Scholar] [CrossRef] [PubMed]
- Barcena-Varela, M.; Lujambio, A. The endless sources of hepatocellular carcinoma heterogeneity. Cancers 2021, 13, 2621. [Google Scholar] [CrossRef]
- Marusyk, A.; Almendro, V.; Polyak, K. Intra-tumour heterogeneity: A looking glass for cancer? Nat. Rev. Cancer 2012, 12, 323–334. [Google Scholar] [CrossRef] [PubMed]
- Alizadeh, A.A.; Aranda, V.; Bardelli, A.; Blanpain, C.; Bock, C.; Borowski, C.; Caldas, C.; Califano, A.; Doherty, M.; Elsner, M.; et al. Toward understanding and exploiting tumor heterogeneity. Nat. Med. 2015, 21, 846–853. [Google Scholar] [CrossRef]
- Kalasekar, S.M.; Vansant-Webb, C.H.; Evason, K.J. Intratumor heterogeneity in hepatocellular carcinoma: Challenges and opportunities. Cancers 2021, 13, 5524. [Google Scholar] [CrossRef]
- Lu, L.C.; Hsu, C.H.; Hsu, C.; Cheng, A.L. Tumor heterogeneity in hepatocellular carcinoma: Facing the challenges. Liver Cancer 2016, 5, 128–138. [Google Scholar] [CrossRef] [PubMed]
- Gisder, D.M.; Tannapfel, A.; Tischoff, I. Histopathology of hepatocellular carcinoma—When and what. Hepatoma Res. 2022, 8, 4. [Google Scholar] [CrossRef]
- He, H.; Bai, Y.; Garcia, E.A.; Li, S. ADASYN: Adaptive synthetic sampling approach for imbalanced learning. In Proceedings of the 2008 IEEE International Joint Conference on Neural Networks (IEEE World Congress on Computational Intelligence), Hong Kong, China, 1–8 June 2008; pp. 1322–1328. [Google Scholar]
- Yao, F.Y.; Xiao, L.; Bass, N.M.; Kerlan, R.; Ascher, N.L.; Roberts, J.P. Liver transplantation for hepatocellular carcinoma: Validation of the UCSF-expanded criteria based on preoperative imaging. Am. J. Transplant. 2007, 7, 2587–2596. [Google Scholar] [CrossRef] [PubMed]
- Duvoux, C.; Roudot-Thoraval, F.; Decaens, T.; Pessione, F.; Badran, H.; Piardi, T.; Francoz, C.; Compagnon, P.; Vanlemmens, C.; Dumortier, J.; et al. Liver transplantation for hepatocellular carcinoma: A model including α-fetoprotein improves the performance of milan criteria. Gastroenterology 2012, 143, 986–994. [Google Scholar] [CrossRef] [PubMed]
- Piñero, F.; Marciano, S.; Anders, M.; Ganem, F.O.; Zerega, A.; Cagliani, J.; Andriani, O.; de Santibañes, E.; Gil, O.; Podestá, L.G.; et al. Identifying patients at higher risk of hepatocellular carcinoma recurrence after liver transplantation in a multicenter cohort study from Argentina. Eur. J. Gastroenterol. Hepatol. 2016, 28, 421–427. [Google Scholar] [CrossRef] [PubMed]
- Grąt, M.; Wronka, K.M.; Stypułkowski, J.; Bik, E.; Krasnodębski, M.; Masior, Ł.; Lewandowski, Z.; Grąt, K.; Patkowski, W.; Krawczyk, M. The Warsaw Proposal for the Use of Extended Selection Criteria in Liver Transplantation for Hepatocellular Cancer. Ann. Surg. Oncol. 2017, 24, 526–534. [Google Scholar] [CrossRef]
- Piñero, F.; Costentin, C.; Degroote, H.; Notarpaolo, A.; Boin, I.F.; Boudjema, K.; Baccaro, C.; Chagas, A.; Bachellier, P.; Ettorre, G.M.; et al. AFP score and metroticket 2.0 perform similarly and could be used in a “within-ALL” clinical decision tool. JHEP Rep. 2023, 5, 100644. [Google Scholar] [CrossRef] [PubMed]
- Ho, C.M.; Lee, C.H.; Lee, M.C.; Zhang, J.F.; Chen, C.H.; Wang, J.Y.; Hu, R.H.; Lee, P.H. Survival After Treatable Hepatocellular Carcinoma Recurrence in Liver Recipients: A Nationwide Cohort Analysis. Front. Oncol. 2021, 10, 616094. [Google Scholar] [CrossRef]
- Alshahrani, A.A.; Ha, S.M.; Hwang, S.; Ahn, C.S.; Kim, K.H.; Moon, D.B.; Ha, T.Y.; Song, G.W.; Jung, D.H.; Park, G.C.; et al. Clinical Features and Surveillance of Very Late Hepatocellular Carcinoma Recurrence After Liver Transplantation. Ann. Transplant. 2018, 23, 659–665. [Google Scholar] [CrossRef]
- Clavien, P.A.; Lesurtel, M.; Bossuyt, P.M.M.; Gores, G.J.; Langer, B.; Perrier, A. Recommendations for liver transplantation for hepatocellular carcinoma: An international consensus conference report. Lancet Oncol. 2012, 13, e11–e22. [Google Scholar] [CrossRef]
- Lai, Q.; Lesari, S.; Lerut, J.P. The impact of biological features for a better prediction of posttransplant hepatocellular cancer recurrence. Curr. Opin. Organ Transplant. 2022, 27, 305–311. [Google Scholar] [CrossRef]
- Di Tommaso, L.; Spadaccini, M.; Donadon, M.; Personeni, N.; Elamin, A.; Aghemo, A.; Lleo, A. Role of liver biopsy in hepatocellular carcinoma. World J. Gastroenterol. 2019, 25, 6041–6052. [Google Scholar] [CrossRef]
- Friemel, J.; Rechsteiner, M.; Frick, L.; Böhm, F.; Struckmann, K.; Egger, M.; Moch, H.; Heikenwalder, M.; Weber, A. Intratumor Heterogeneity in Hepatocellular Carcinoma. Clin. Cancer Res. 2015, 21, 1951–1961. [Google Scholar] [CrossRef] [PubMed]
- Rastogi, A.; Maiwall, R.; Ramakrishna, G.; Modi, S.; Taneja, K.; Bihari, C.; Kumar, G.; Patil, N.; Thapar, S.; Choudhury, A.K.; et al. Hepatocellular carcinoma: Clinicopathologic associations amidst marked phenotypic heterogeneity. Pathol. Res. Pract. 2021, 217, 153290. [Google Scholar] [CrossRef]
- Liu, J.; Dang, H.; Wang, X.W. The significance of intertumor and intratumor heterogeneity in liver cancer. Exp. Mol. Med. 2018, 50, e416. [Google Scholar] [CrossRef]
- Galle, P.R.; Forner, A.; Llovet, J.M.; Mazzaferro, V.; Piscaglia, F.; Raoul, J.L.; Schirmacher, P.; Vilgrain, V. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef]
- Torbenson, M.S. Hepatocellular carcinoma: Making sense of morphological heterogeneity, growth patterns, and subtypes. Hum. Pathol. 2021, 112, 86–101. [Google Scholar] [CrossRef]
- Calderaro, J.; Ziol, M.; Paradis, V.; Zucman-Rossi, J. Molecular and histological correlations in liver cancer. J. Hepatol. 2019, 71, 616–630. [Google Scholar] [CrossRef]
- Calderaro, J.; Couchy, G.; Imbeaud, S.; Amaddeo, G.; Letouzé, E.; Blanc, J.-F.; Laurent, C.; Hajji, Y.; Azoulay, D.; Bioulac-Sage, P.; et al. Histological subtypes of hepatocellular carcinoma are related to gene mutations and molecular tumour classification. J. Hepatol. 2017, 67, 727–738. [Google Scholar] [CrossRef] [PubMed]
- Tan, P.S.; Nakagawa, S.; Goossens, N.; Venkatesh, A.; Huang, T.; Ward, S.C.; Sun, X.; Song, W.M.; Koh, A.; Canasto-Chibuque, C.; et al. Clinicopathological indices to predict hepatocellular carcinoma molecular classification. Liver Int. 2016, 36, 108–118. [Google Scholar] [CrossRef] [PubMed]
- Neuberger, J.; Patel, J.; Caldwell, H.; Davies, S.; Hebditch, V.; Hollywood, C.; Hubscher, S.; Karkhanis, S.; Lester, W.; Roslund, N.; et al. Guidelines on the use of liver biopsy in clinical practice from the British Society of Gastroenterology, the Royal College of Radiologists and the Royal College of Pathology. Gut 2020, 69, 1382–1403. [Google Scholar] [CrossRef]
- Samuel, D.; Coilly, A. Management of patients with liver diseases on the waiting list for transplantation: A major impact to the success of liver transplantation. BMC Med. 2018, 16, 113. [Google Scholar] [CrossRef]
- Chan, L.K.; Tsui, Y.M.; Ho, D.W.H.; Ng, I.O.L. Cellular heterogeneity and plasticity in liver cancer. Semin. Cancer Biol. 2022, 82, 134–149. [Google Scholar] [CrossRef]
- Beumer, B.R.; Polak, W.G.; de Man, R.A.; Metselaar, H.J.; van Klaveren, D.; Labrecque, J.; IJzermans, J.N. Impact of waiting time on post-transplant survival for recipients with hepatocellular carcinoma: A natural experiment randomized by blood group. JHEP Rep. 2023, 5, 100629. [Google Scholar] [CrossRef]
- Straś, W.A.; Wasiak, D.; Łągiewska, B.; Tronina, O.; Hreńczuk, M.; Gotlib, J.; Lisik, W.; Małkowski, P. Recurrence of Hepatocellular Carcinoma After Liver Transplantation: Risk Factors and Predictive Models. Ann. Transplant. 2022, 27, e934924-1–e934924-11. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Dataset 1 (n = 232) | Dataset 2 (n = 46) | |
|---|---|---|
| Recipient characteristics | ||
| Male gender, N (%) | 203 (87.5%) | 44 (95.7) |
| Age, years, median (IQR) | 57 (13) | 58 (14) |
| Obesity, N (%) | 61 (26.3) | 12 (26.1) |
| MELD score, median (IQR) | 11 (5.5) | 12.4 (5) |
| Waiting list, months, median (IQR) | 2.2 (4.1) | 1.8 (2) |
| Tumor-related factors | ||
| Nº of nodules, median (IQR), range | 1 (1), 1–4 | 2 (1), 1–6 |
| Size of largest nodule, median (IQR), range | 2.9 (1.8), 0.7–8.7 | 3.0 (1.6), 1.0–8.2 |
| Total tumor diameter (cm), median (IQR), range | 3.4 (2.5), 0.7–12.5 | 4.45 (2.3), 1–12.5 |
| Total tumor volume (cm3), median (IQR), range | 14.1 (28.3), 0.2–344.8 | 19.5 (28.9), 0.5–291.4 |
| Within Milan criteria, N (%) | 179 (77.2) | 31 (67.4) |
| Total tumor volume ≤ 115 cm3, N (%) | 219 (94.4) | 42 (91.3) |
| Survival data | ||
| Patients alive at 5 years, N (%) | 151 (65.1) | 29 (63.0) |
| Recurrence at 5 years, N (%) | 43 (18.5) | 9 (19.6) |
| Follow-up (years) | ||
| Follow-up, median (IQR), max. range | 6.6 (5.9), 16.3 | 5.0 (4.3), 15.9 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Andrade, R.; Perez-Rojas, J.; da Silva, S.G.; Miskinyte, M.; Quaresma, M.C.; Frazão, L.P.; Peixoto, C.; Cubells, A.; Montalvá, E.M.; Figueiredo, A.; et al. HepatoPredict Accurately Selects Hepatocellular Carcinoma Patients for Liver Transplantation Regardless of Tumor Heterogeneity. Cancers 2025, 17, 500. https://doi.org/10.3390/cancers17030500
Andrade R, Perez-Rojas J, da Silva SG, Miskinyte M, Quaresma MC, Frazão LP, Peixoto C, Cubells A, Montalvá EM, Figueiredo A, et al. HepatoPredict Accurately Selects Hepatocellular Carcinoma Patients for Liver Transplantation Regardless of Tumor Heterogeneity. Cancers. 2025; 17(3):500. https://doi.org/10.3390/cancers17030500
Chicago/Turabian StyleAndrade, Rita, Judith Perez-Rojas, Sílvia Gomes da Silva, Migla Miskinyte, Margarida C. Quaresma, Laura P. Frazão, Carolina Peixoto, Almudena Cubells, Eva M. Montalvá, António Figueiredo, and et al. 2025. "HepatoPredict Accurately Selects Hepatocellular Carcinoma Patients for Liver Transplantation Regardless of Tumor Heterogeneity" Cancers 17, no. 3: 500. https://doi.org/10.3390/cancers17030500
APA StyleAndrade, R., Perez-Rojas, J., da Silva, S. G., Miskinyte, M., Quaresma, M. C., Frazão, L. P., Peixoto, C., Cubells, A., Montalvá, E. M., Figueiredo, A., Cipriano, A., Gonçalves-Reis, M., Proença, D., Folgado, A., Pereira-Leal, J. B., Oliveira, R. C., Pinto-Marques, H., Tralhão, J. G., Berenguer, M., & Cardoso, J. (2025). HepatoPredict Accurately Selects Hepatocellular Carcinoma Patients for Liver Transplantation Regardless of Tumor Heterogeneity. Cancers, 17(3), 500. https://doi.org/10.3390/cancers17030500