
Ibrutinib in Combination with Lenalidomide Revlimid/Dexamethasone in Relapsed/Refractory Multiple Myeloma (AFT-15)

 ,
,  , ,
, , 
Simple Summary
Abstract
1. Introduction
2. Study Design and Treatment
2.1. Treatment
2.2. Study Procedures
2.3. Statistical Design and Methods
3. Results
3.1. Patient Characteristics
3.2. Dose Escalation
3.3. Treatment Course, Safety and Toxicity
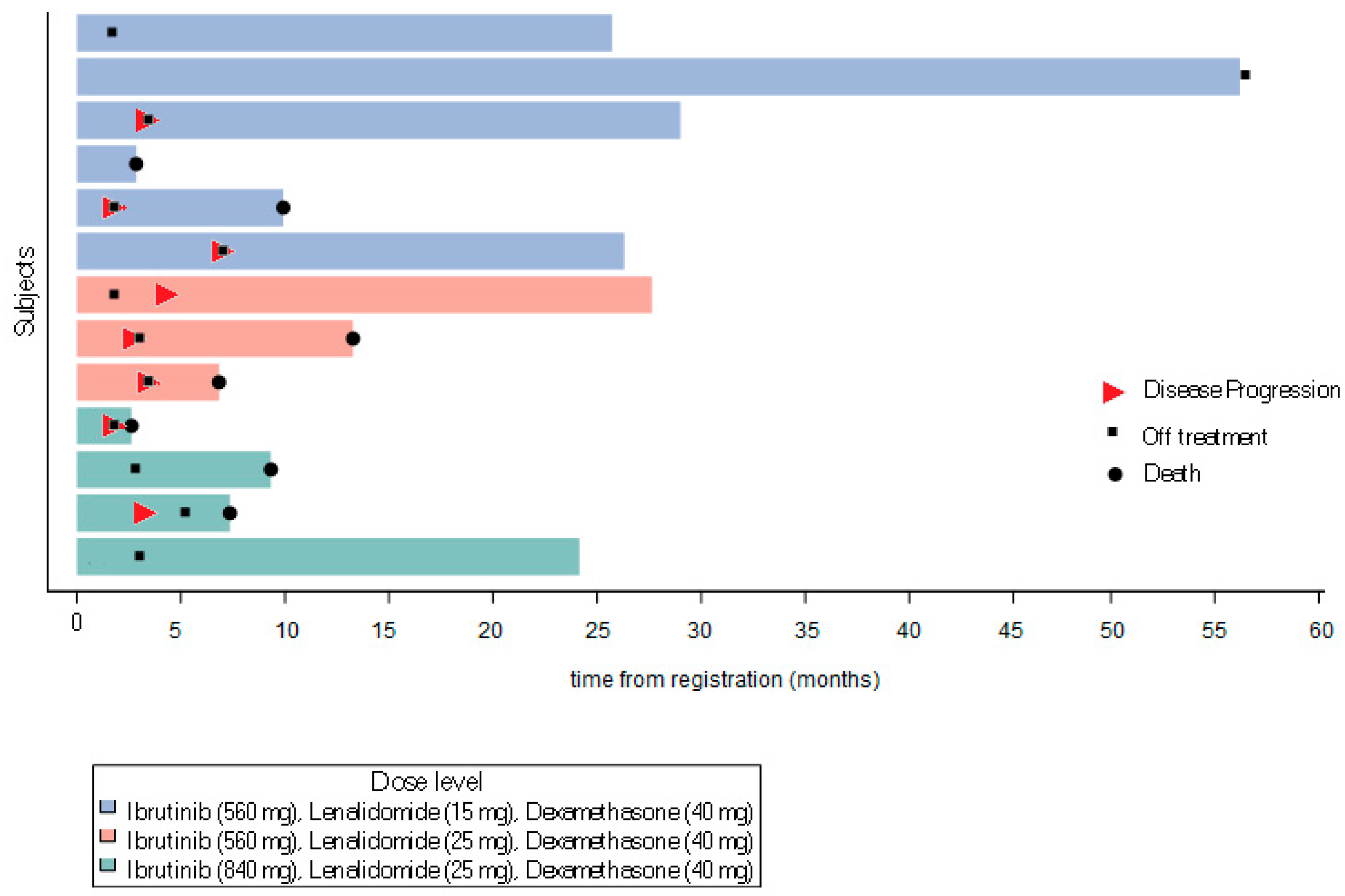
3.4. Clinical Outcome: Response and Survival
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Clinicaltrials.gov Identifier
References
- Kumar, S.K.; Lee, J.H.; Lahuerta, J.J.; Morgan, G.; Richardson, P.G.; Crowley, J.; Haessler, J.; Feather, J.; Hoering, A.; Moreau, P.; et al. Risk of progression and survival in multiple myeloma relapsing after therapy with IMiDs and bortezomib: A multicenter international myeloma working group study. Leukemia 2012, 26, 149–157. [Google Scholar] [CrossRef] [PubMed]
- Siegel, D.S.; Martin, T.; Wang, M.; Vij, R.; Jakubowiak, A.J.; Lonial, S.; Trudel, S.; Kukreti, V.; Bahlis, N.; Alsina, M.; et al. A phase 2 study of single-agent carfilzomib (PX-171-003-A1) in patients with relapsed and refractory multiple myeloma. Blood 2012, 120, 2817–2825. [Google Scholar] [CrossRef] [PubMed]
- Galustian, C.; Meyer, B.; Labarthe, M.C.; Dredge, K.; Klaschka, D.; Henry, J.; Todryk, S.; Chen, R.; Muller, G.; Stirling, D.; et al. The anti-cancer agents lenalidomide and pomalidomide inhibit the proliferation and function of T regulatory cells. Cancer Immunol. Immunother. 2009, 58, 1033–1045. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.K.; Callander, N.S.; Adekola, K.; Anderson, L.; Baljevic, M.; Campagnaro, E.; Castillo, J.J.; Chandler, J.C.; Costello, C.; Efebera, Y.; et al. Multiple Myeloma, Version 3.2021, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2020, 18, 1685–1717. [Google Scholar] [CrossRef] [PubMed]
- Murray, M.Y.; Zaitseva, L.; Auger, M.J.; Craig, J.I.; MacEwan, D.J.; Rushworth, S.A.; Bowles, K.M. Ibrutinib inhibits BTK-driven NF-kappaB p65 activity to overcome bortezomib-resistance in multiple myeloma. Cell Cycle 2015, 14, 2367–2375. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Shi, J.; Gu, Z.; Salama, M.E.; Das, S.; Wendlandt, E.; Xu, H.; Huang, J.; Tao, Y.; Hao, M.; et al. Bruton tyrosine kinase is a therapeutic target in stem-like cells from multiple myeloma. Cancer Res. 2015, 75, 594–604. [Google Scholar] [CrossRef] [PubMed]
- Bam, R.; Ling, W.; Khan, S.; Pennisi, A.; Venkateshaiah, S.U.; Li, X.; van Rhee, F.; Usmani, S.; Barlogie, B.; Shaughnessy, J.; et al. Role of Bruton’s tyrosine kinase in myeloma cell migration and induction of bone disease. Am. J. Hematol. 2013, 88, 463–471. [Google Scholar] [CrossRef] [PubMed]
- Rushworth, S.A.; Bowles, K.M.; Barrera, L.N.; Murray, M.Y.; Zaitseva, L.; MacEwan, D.J. BTK inhibitor ibrutinib is cytotoxic to myeloma and potently enhances bortezomib and lenalidomide activities through NF-kappaB. Cell Signal 2013, 25, 106–112. [Google Scholar] [CrossRef] [PubMed]
- Richardson, P.G.; Trudel, S.; Popat, R.; Mateos, M.V.; Vangsted, A.J.; Ramasamy, K.; Martinez-Lopez, J.; Quach, H.; Orlowski, R.Z.; Arnao, M.; et al. Mezigdomide plus Dexamethasone in Relapsed and Refractory Multiple Myeloma. N. Engl. J. Med. 2023, 389, 1009–1022. [Google Scholar] [CrossRef] [PubMed]
- Richardson, P.G.; Bensinger, W.I.; Huff, C.A.; Costello, C.L.; Lendvai, N.; Berdeja, J.G.; Anderson, L.D., Jr.; Siegel, D.S.; Lebovic, D.; Jagannath, S.; et al. Ibrutinib alone or with dexamethasone for relapsed or relapsed and refractory multiple myeloma: Phase 2 trial results. Br. J. Haematol. 2018, 180, 821–830. [Google Scholar] [CrossRef] [PubMed]
- Ailawadhi, S.; Parrondo, R.D.; Moustafa, M.A.; LaPlant, B.R.; Alegria, V.; Chapin, D.; Roy, V.; Sher, T.; Paulus, A.; Chanan-Khan, A.A. Ibrutinib, lenalidomide and dexamethasone in patients with relapsed and/or refractory multiple myeloma: Phase I trial results. Hematol. Oncol. 2022, 40, 695–703. [Google Scholar] [CrossRef] [PubMed]
- Hajek, R.; Pour, L.; Ozcan, M.; Martin Sanchez, J.; Garcia Sanz, R.; Anagnostopoulos, A.; Oriol, A.; Cascavilla, N.; Terjung, A.; Lee, Y.; et al. A phase 2 study of ibrutinib in combination with bortezomib and dexamethasone in patients with relapsed/refractory multiple myeloma. Eur. J. Haematol. 2020, 104, 435–442. [Google Scholar] [CrossRef] [PubMed]
- Chari, A.; Cornell, R.F.; Gasparetto, C.; Karanes, C.; Matous, J.V.; Niesvizky, R.; Lunning, M.; Usmani, S.Z.; Anderson, L.D., Jr.; Chhabra, S.; et al. Final analysis of a phase 1/2b study of ibrutinib combined with carfilzomib/dexamethasone in patients with relapsed/refractory multiple myeloma. Hematol. Oncol. 2020, 38, 353–362. [Google Scholar] [CrossRef] [PubMed]
- Gordon, M.J.; Feng, L.; Strati, P.; Lee, H.J.; Hagemeister, F.B.; Westin, J.R.; Samaniego, F.; Marques-Piubelli, M.L.; Vega Vazquez, F.; Parra Cuentas, E.R.; et al. Safety and efficacy of ibrutinib in combination with rituximab and lenalidomide in previously untreated follicular and marginal zone lymphoma: An open label, phase 2 study. Cancer 2024, 130, 876–885. [Google Scholar] [CrossRef] [PubMed]
- Ip, A.; Petrillo, A.; Della Pia, A.; Lee, G.G.; Gill, S.; Varughese, T.; Zenreich, J.; Gutierrez, M.; Zhang, J.; Ahn, J.; et al. Phase 1b dose-finding study of rituximab, lenalidomide, and ibrutinib (R2I) in patients with relapsed/refractory mantle cell lymphoma. Leuk. Lymphoma 2023, 64, 2225–2235. [Google Scholar] [CrossRef] [PubMed]
- Goy, A.; Ramchandren, R.; Ghosh, N.; Munoz, J.; Morgan, D.S.; Dang, N.H.; Knapp, M.; Delioukina, M.; Kingsley, E.; Ping, J.; et al. Ibrutinib plus lenalidomide and rituximab has promising activity in relapsed/refractory non-germinal center B-cell-like DLBCL. Blood 2019, 134, 1024–1036. [Google Scholar] [CrossRef] [PubMed]
- Jerkeman, M.; Eskelund, C.W.; Hutchings, M.; Raty, R.; Wader, K.F.; Laurell, A.; Toldbod, H.; Pedersen, L.B.; Niemann, C.U.; Dahl, C.; et al. Ibrutinib, lenalidomide, and rituximab in relapsed or refractory mantle cell lymphoma (PHILEMON): A multicentre, open-label, single-arm, phase 2 trial. Lancet Haematol. 2018, 5, e109–e116. [Google Scholar] [CrossRef] [PubMed]
- Hagner, P.R.; Chiu, H.; Ortiz, M.; Apollonio, B.; Wang, M.; Couto, S.; Waldman, M.F.; Flynt, E.; Ramsay, A.G.; Trotter, M.; et al. Activity of lenalidomide in mantle cell lymphoma can be explained by NK cell-mediated cytotoxicity. Br. J. Haematol. 2017, 179, 399–409. [Google Scholar] [CrossRef] [PubMed]
- Ujjani, C.; Wang, H.; Skarbnik, A.; Trivedi, N.; Ramzi, P.; Khan, N.; Cheson, B.D. A phase 1 study of lenalidomide and ibrutinib in combination with rituximab in relapsed and refractory CLL. Blood Adv. 2018, 2, 762–768. [Google Scholar] [CrossRef] [PubMed]
- Durie, B.G.; Harousseau, J.L.; Miguel, J.S.; Blade, J.; Barlogie, B.; Anderson, K.; Gertz, M.; Dimopoulos, M.; Westin, J.; Sonneveld, P.; et al. International uniform response criteria for multiple myeloma. Leukemia 2006, 20, 1467–1473. [Google Scholar] [CrossRef] [PubMed]
- Rajkumar, S.V.; Harousseau, J.L.; Durie, B.; Anderson, K.C.; Dimopoulos, M.; Kyle, R.; Blade, J.; Richardson, P.; Orlowski, R.; Siegel, D.; et al. Consensus recommendations for the uniform reporting of clinical trials: Report of the International Myeloma Workshop Consensus Panel 1. Blood 2011, 117, 4691–4695. [Google Scholar] [CrossRef] [PubMed]
- Richardson, P.G.; San Miguel, J.F.; Moreau, P.; Hajek, R.; Dimopoulos, M.A.; Laubach, J.P.; Palumbo, A.; Luptakova, K.; Romanus, D.; Skacel, T.; et al. Interpreting clinical trial data in multiple myeloma: Translating findings to the real-world setting. Blood Cancer J. 2018, 8, 109. [Google Scholar] [CrossRef] [PubMed]
- Lonial, S.; Popat, R.; Hulin, C.; Jagannath, S.; Oriol, A.; Richardson, P.G.; Facon, T.; Weisel, K.; Larsen, J.T.; Minnema, M.C.; et al. Iberdomide plus dexamethasone in heavily pretreated late-line relapsed or refractory multiple myeloma (CC-220-MM-001): A multicentre, multicohort, open-label, phase 1/2 trial. Lancet Haematol. 2022, 9, e822–e832. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Characteristic | No. Patients (%) (n = 13) |
|---|---|
| Median age, years (range) | 64 (45–84) |
| Sex | |
| Male | 5 (38.5%) |
| Female | 8 (61.5%) |
| Race | |
| Black or African American/African Heritage | 1 (7.7%) |
| White | 10 (76.9%) |
| Not provided | 2 (15.4%) |
| Ethnicity | |
| Hispanic/Latino | 1 (7.7%) |
| Non-Hispanic/Latino | 11 (84.6%) |
| Not provided | 1 (7.7%) |
| ECOG Performance Score | |
| 0 | 3 (23.1%) |
| 1 | 10 (76.9%) |
| Prior autologous transplant | 10 (76.9%) |
| Number of lines of prior systemic therapy | |
| 2 | 5 (38.5%) |
| 3 | 3 (23.1%) |
| 4–9 | 5 (38.5%) |
| Prior systemic therapy | |
| Bortezomib | 13 (100%) |
| Carfilzomib | 5 (38.5%) |
| CAR-T cell therapy | 1 (7.7%) |
| CB-839 HCI | 1 (7.7%) |
| Cyclophosphamide | 2 (15.4%) |
| Daratumumab | 7 (53.8%) |
| Iberdomide | 1 (7.7%) |
| Ixazomib | 2 (15.4%) |
| Lenalidomide | 12 (92.3%) |
| Pomalidomide | 4 (30.8%) |
| Thalidomide | 1 (7.7%) |
| No measurable soft tissue plasmacytomas or extramedullary disease present | 13 (100%) |
| FISH abnormalities | |
| No abnormal findings | 1 (7.7%) |
| Abnormal findings including: | 12 (92.3%) |
| del(13q) —3 pts | |
| del (17p)—3 pts | |
| t(4; 14)—1 pt | |
| t(11:14)—3 pts | |
| gain1q—4 pts | |
| loss1p—1 pt | |
| trisomy—2 pts | |
| MYC abnormality—1 pt |
| Toxicity | Grade (n = 13) | |||
|---|---|---|---|---|
| 2 | 3 | 4 | 5 | |
| Abdominal pain | 7.7% | |||
| Alanine aminotransferase increase | 7.7% | |||
| Alkaline phosphatase increase | 7.7% | |||
| Anemia | 7.7% | 15.4% | ||
| Anorexia | 7.7% | |||
| Aspartate aminotransferase increase | 7.7% | |||
| Back pain | 23.1% | |||
| Blood bilirubin increase | 7.7% | |||
| Cellulitis | 7.7% | |||
| Chest pain—cardiac | 7.7% | |||
| COVID-19 | 7.7% | 7.7% | ||
| Chronic kidney disease | 7.7% | |||
| Confusion | 7.7% | |||
| Conjunctivitis | 7.7% | |||
| Constipation | 7.7% | |||
| Creatinine increase | 7.7% | |||
| Cytopenia | 7.7% | |||
| Dehydration | 7.7% | |||
| Diarrhea | 23.1% | |||
| Dyspepsia | 15.4% | |||
| Dyspnea | 7.7% | |||
| E. coli (urine) | 7.7% | |||
| Edema (face) | 7.7% | |||
| Fatigue | 30.8% | 7.7% | ||
| Febrile neutropenia | 7.7% | |||
| Gastroesophageal reflux disease | 15.4% | |||
| Generalized muscle weakness | 7.7% | |||
| Hypoalbuminemia | 7.7% | |||
| Hypocalcemia | 7.7% | |||
| Hypokalemia | 7.7% | |||
| Hypophosphatemia | 7.7% | 7.7% | ||
| Hypotension | 7.7% | |||
| Insomnia | 7.7% | |||
| Lung infection | 7.7% | |||
| Lymphocyte count decrease | 30.8% | 7.7% | ||
| Myalgia | 7.7% | |||
| Nail infection | 7.7% | |||
| Nasal congestion | 7.7% | |||
| Non-viral hepatitis | 7.7% | |||
| Pain in extremity | 7.7% | |||
| Platelet count decrease | 15.4% | 7.7% | ||
| Pleural effusion | 7.7% | |||
| Rash, maculo-papular | 15.4% | |||
| Sepsis syndrome | 7.7% | |||
| Sinus tachycardia | 7.7% | |||
| Sinusitis | 7.7% | |||
| Skin infection | 7.7% | |||
| Soft tissue infection | 7.7% | |||
| Somnolence | 7.7% | |||
| Upper respiratory infection | 15.4% | |||
| Urinary tract infection | 7.7% | |||
| Weight loss | 15.4% | |||
| White blood cell decrease | 7.7% | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Efebera, Y.; Suman, V.; Dinner, S.; O’Donnell, T.; Rosko, A.; Mckay, J.; Barth, P.; Hagen, P.; Usmani, S.; Richardson, P.; et al. Ibrutinib in Combination with Lenalidomide Revlimid/Dexamethasone in Relapsed/Refractory Multiple Myeloma (AFT-15). Cancers 2025, 17, 2433. https://doi.org/10.3390/cancers17152433
Efebera Y, Suman V, Dinner S, O’Donnell T, Rosko A, Mckay J, Barth P, Hagen P, Usmani S, Richardson P, et al. Ibrutinib in Combination with Lenalidomide Revlimid/Dexamethasone in Relapsed/Refractory Multiple Myeloma (AFT-15). Cancers. 2025; 17(15):2433. https://doi.org/10.3390/cancers17152433
Chicago/Turabian StyleEfebera, Yvonne, Vera Suman, Shira Dinner, Taylor O’Donnell, Ashley Rosko, John Mckay, Peter Barth, Patrick Hagen, Saad Usmani, Paul Richardson, and et al. 2025. "Ibrutinib in Combination with Lenalidomide Revlimid/Dexamethasone in Relapsed/Refractory Multiple Myeloma (AFT-15)" Cancers 17, no. 15: 2433. https://doi.org/10.3390/cancers17152433
APA StyleEfebera, Y., Suman, V., Dinner, S., O’Donnell, T., Rosko, A., Mckay, J., Barth, P., Hagen, P., Usmani, S., Richardson, P., & Laubach, J. (2025). Ibrutinib in Combination with Lenalidomide Revlimid/Dexamethasone in Relapsed/Refractory Multiple Myeloma (AFT-15). Cancers, 17(15), 2433. https://doi.org/10.3390/cancers17152433