
The Emerging Role of Left Atrial Strain in Cardiovascular Risk Stratification for Multiple Myeloma Patients Undergoing Carfilzomib Therapy

 , , ,
, , ,  , and
, and 
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Clinical Assessment
2.2. Left Atrial Strain
2.3. Statistical Analysis
3. Results
3.1. General Characteristics and Cardiovascular Risk Factors
3.2. Cardiovascular Hypertensive Adverse Events
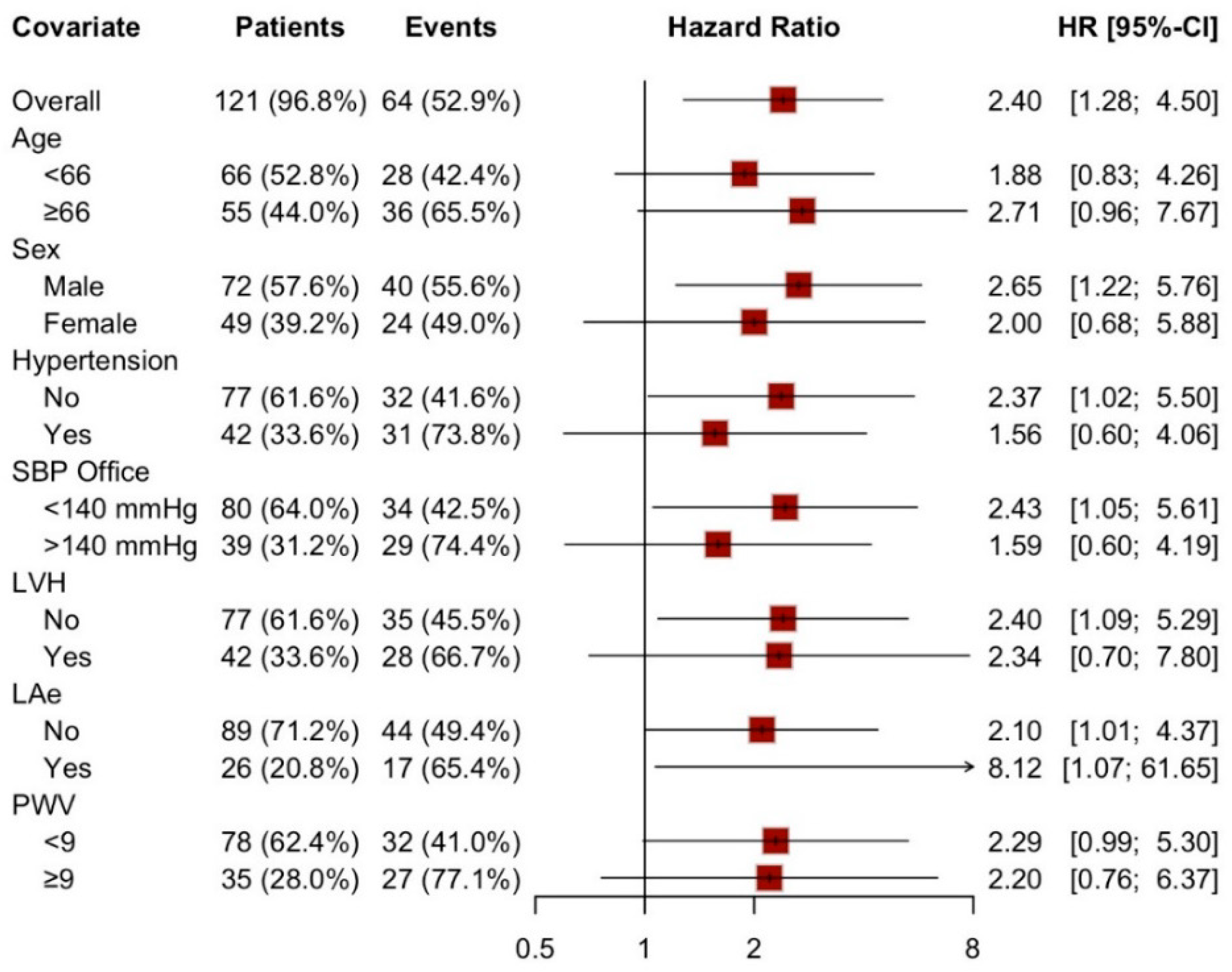
3.3. Predictive Variables of Hypertensive Events
4. Discussion
Study Limitation
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, D.; Martin, T.; Nooka, A.; Harvey, R.D.; Vij, R.; Niesvizky, R.; Badros, A.Z.; Jagannath, S.; McCulloch, L.; Rajangam, K.; et al. Integrated safety profile of single-agent carfilzomib: Experience from 526 patients enrolled in 4 phase II clinical studies. Haematologica 2013, 98, 1753–1761. [Google Scholar] [CrossRef]
- Röllig, C.; Knop, S.; Bornhäuser, M. Multiple myeloma. Lancet Lond. Engl. 2015, 385, 2197–2208. [Google Scholar] [CrossRef]
- Dimopoulos, M.A.; Goldschmidt, H.; Niesvizky, R.; Joshua, D.; Chng, W.J.; Oriol, A.; Orlowski, R.Z.; Ludwig, H.; Facon, T.; Hajek, R.; et al. Carfilzomib or bortezomib in relapsed or refractory multiple myeloma (ENDEAVOR): An interim overall survival analysis of an open-label, randomised, phase 3 trial. Lancet Oncol. 2017, 18, 1327–1337. [Google Scholar] [CrossRef]
- Waxman, A.J.; Clasen, S.; Hwang, W.-T.; Garfall, A.; Vogl, D.T.; Carver, J.; O’Quinn, R.; Cohen, A.D.; Stadtmauer, E.A.; Ky, B.; et al. Carfilzomib-Associated Cardiovascular Adverse Events: A Systematic Review and Meta-analysis. JAMA Oncol. 2018, 4, e174519. [Google Scholar] [CrossRef]
- Li, W.; Garcia, D.; RF, C.; Gailani, D.; Laubach, J.; ME, M.; PG, R.; Moslehi, J. Cardiovascular and Thrombotic Complications of Novel Multiple Myeloma Therapies: A Review. JAMA Oncol. 2017, 3, 980–988. [Google Scholar] [CrossRef]
- Milan, A.; Bruno, G.; Maffei, I.; Iannaccone, A.; Ravera, A.; Schiavone, D.; Veglio, F. Arterial Hypertension and Multiple Myeloma: Physiopathology and Cardiovascular Risk and “Practical” Indications in Patients Receiving Carfilzomib. Curr. Hypertens. Rev. 2019, 15, 47–53. [Google Scholar] [CrossRef]
- Bringhen, S.; De Wit, E.; Dimopoulos, M.-A. New Agents in Multiple Myeloma: An Examination of Safety Profiles. Clin. Lymphoma Myeloma Leuk. 2017, 17, 391–407.e5. [Google Scholar] [CrossRef] [PubMed]
- Lyon, A.R.; López-Fernández, T.; Couch, L.S.; Asteggiano, R.; Aznar, M.C.; Bergler-Klein, J.; Boriani, G.; Cardinale, D.; Cordoba, R.; Cosyns, B.; et al. 2022 ESC Guidelines on cardio-oncology developed in collaboration with the European Hematology Association (EHA), the European Society for Therapeutic Radiology and Oncology (ESTRO) and the International Cardio-Oncology Society (IC-OS). Eur. Heart J. 2022, 43, 4229–4361. [Google Scholar] [CrossRef]
- Smiseth, O.A.; Morris, D.A.; Cardim, N.; Cikes, M.; Delgado, V.; Donal, E.; Flachskampf, F.A.; Galderisi, M.; Gerber, B.L.; Gimelli, A.; et al. Multimodality imaging in patients with heart failure and preserved ejection fraction: An expert consensus document of the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2022, 23, e34–e61. [Google Scholar] [CrossRef] [PubMed]
- Thomas, L.; Marwick, T.H.; Popescu, B.A.; Donal, E.; Badano, L.P. Left Atrial Structure and Function, and Left Ventricular Diastolic Dysfunction: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2019, 73, 1961–1977. [Google Scholar] [CrossRef] [PubMed]
- Di Lisi, D.; Moreo, A.; Casavecchia, G.; Cadeddu Dessalvi, C.; Bergamini, C.; Zito, C.; Madaudo, C.; Madonna, R.; Cameli, M.; Novo, G. Atrial Strain Assessment for the Early Detection of Cancer Therapy-Related Cardiac Dysfunction in Breast Cancer Women (The STRANO STUDY: Atrial Strain in Cardio-Oncology). J. Clin. Med. 2023, 12, 7127. [Google Scholar] [CrossRef] [PubMed]
- Piña, P.; Lorenzatti, D.; Pellikka, P.A.; Shah, N.; Slipczuk, L. Prognostic value of left atrial strain in multiple myeloma. Eur. J. Intern. Med. 2023, 114, 150–153. [Google Scholar] [CrossRef]
- Mancia, G.; Kreutz, R.; Brunström, M.; Burnier, M.; Grassi, G.; Januszewicz, A.; Muiesan, M.L.; Tsioufis, K.; Agabiti-Rosei, E.; Algharably, E.A.E.; et al. 2023 ESH Guidelines for the management of arterial hypertension The Task Force for the management of arterial hypertension of the European Society of Hypertension: Endorsed by the International Society of Hypertension (ISH) and the European Renal Association (ERA). J. Hypertens. 2023, 41, 1874–2071. [Google Scholar] [CrossRef]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef]
- Terpos, E.; Kleber, M.; Engelhardt, M.; Zweegman, S.; Gay, F.; Kastritis, E.; van de Donk, N.W.C.J.; Bruno, B.; Sezer, O.; Broijl, A.; et al. European Myeloma Network guidelines for the management of multiple myeloma-related complications. Haematologica 2015, 100, 1254–1266. [Google Scholar] [CrossRef] [PubMed]
- Bringhen, S.; Milan, A.; D’Agostino, M.; Ferri, C.; Wäsch, R.; Gay, F.; Larocca, A.; Offidani, M.; Zweegman, S.; Terpos, E.; et al. Prevention, monitoring and treatment of cardiovascular adverse events in myeloma patients receiving carfilzomib A consensus paper by the European Myeloma Network and the Italian Society of Arterial Hypertension. J. Intern. Med. 2019, 286, 63–74. [Google Scholar] [CrossRef]
- Astarita, A.; Mingrone, G.; Airale, L.; Vallelonga, F.; Covella, M.; Catarinella, C.; Cesareo, M.; Bruno, G.; Leone, D.; Giordana, C.; et al. Multiple Myeloma Patients Undergoing Carfilzomib: Development and Validation of a Risk Score for Cardiovascular Adverse Events Prediction. Cancers 2021, 13, 1631. [Google Scholar] [CrossRef] [PubMed]
- Voigt, J.-U.; Pedrizzetti, G.; Lysyansky, P.; Marwick, T.H.; Houle, H.; Baumann, R.; Pedri, S.; Ito, Y.; Abe, Y.; Metz, S.; et al. Definitions for a Common Standard for 2D Speckle Tracking Echocardiography: Consensus Document of the EACVI/ASE/Industry Task Force to Standardize Deformation Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 183–193. [Google Scholar] [CrossRef]
- Colomba, A.; Astarita, A.; Mingrone, G.; Airale, L.; Catarinella, C.; Vallelonga, F.; Leone, D.; Cesareo, M.; Paladino, A.; Bringhen, S.; et al. Haemodynamic Forces: Emerging Markers of Ventricular Remodelling in Multiple Myeloma Cardiovascular Baseline Risk Assessment. Cancers 2024, 16, 3081. [Google Scholar] [CrossRef]
- Badano, L.P.; Kolias, T.J.; Muraru, D.; Abraham, T.P.; Aurigemma, G.; Edvardsen, T.; D’Hooge, J.; Donal, E.; Fraser, A.G.; Marwick, T.; et al. Standardization of left atrial, right ventricular, and right atrial deformation imaging using two-dimensional speckle tracking echocardiography: A consensus document of the EACVI/ASE/Industry Task Force to standardize deformation imaging. Eur. Heart J. Cardiovasc. Imaging 2018, 19, 591–600. [Google Scholar] [CrossRef]
- Rossi, A.; Carluccio, E.; Cameli, M.; Inciardi, R.M.; Mandoli, G.E.; D’Agostino, A.; Biagioli, P.; Maffeis, C.; Pugliese, N.R.; Pastore, M.C.; et al. Left atrial structural and mechanical remodelling in heart failure with reduced ejection fraction. ESC Heart Fail. 2021, 8, 4751–4759. [Google Scholar] [CrossRef] [PubMed]
- Patton, R.; Dragatakis, L.; Marpole, D.; Sniderman, A. The posterior left atrial echocardiogram of mitral regurgitation. Circulation 1978, 57, 1134–1139. [Google Scholar] [CrossRef] [PubMed]
- Inoue, K.; Khan, F.H.; Remme, E.W.; Ohte, N.; García-Izquierdo, E.; Chetrit, M.; Moñivas-Palomero, V.; Mingo-Santos, S.; Andersen, Ø.S.; Gude, E.; et al. Determinants of left atrial reservoir and pump strain and use of atrial strain for evaluation of left ventricular filling pressure. Eur. Heart J. Cardiovasc. Imaging 2022, 23, 61–70. [Google Scholar] [CrossRef] [PubMed]
- Nagueh, S.F.; Khan, S.U. Left Atrial Strain for Assessment of Left Ventricular Diastolic Function. JACC Cardiovasc. Imaging 2023, 16, 691–707. [Google Scholar] [CrossRef]
- Shinzato, M.H.; Santos, N.; Nishida, G.; Moriya, H.; Assef, J.; Feres, F.; Hortegal, R.A. Left ventricular and atrial myocardial strain in heart failure with preserved ejection fraction: The evidence so far and prospects for phenotyping strategy. Cardiovasc. Ultrasound 2024, 22, 4. [Google Scholar] [CrossRef]
- Nagueh, S.F.; Smiseth, O.A.; Appleton, C.P.; Byrd, B.F.; Dokainish, H.; Edvardsen, T.; Flachskampf, F.A.; Gillebert, T.C.; Klein, A.L.; Lancellotti, P.; et al. Recommendations for the Evaluation of Left Ventricular Diastolic Function by Echocardiography: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. Off. Publ. Am. Soc. Echocardiogr. 2016, 29, 277–314. [Google Scholar] [CrossRef]
- Park, H.; Kim, K.H.; Kim, H.Y.; Cho, J.Y.; Yoon, H.J.; Hong, Y.J.; Park, H.W.; Kim, J.H.; Ahn, Y.; Jeong, M.H.; et al. Left atrial longitudinal strain as a predictor of Cancer therapeutics-related cardiac dysfunction in patients with breast Cancer. Cardiovasc. Ultrasound 2020, 18, 28. [Google Scholar] [CrossRef]
- Raafs, A.G.; Vos, J.L.; Henkens, M.T.H.M.; Slurink, B.O.; Verdonschot, J.A.J.; Bossers, D.; Roes, K.; Gerretsen, S.; Knackstedt, C.; Hazebroek, M.R.; et al. Left Atrial Strain Has Superior Prognostic Value to Ventricular Function and Delayed-Enhancement in Dilated Cardiomyopathy. JACC Cardiovasc. Imaging 2022, 15, 1015–1026. [Google Scholar] [CrossRef]
- Yang, F.; Wang, L.; Wang, J.; Pu, L.; Xu, Y.; Li, W.; Wan, K.; Yang, D.; Sun, J.; Han, Y.; et al. Prognostic value of fast semi-automated left atrial long-axis strain analysis in hypertrophic cardiomyopathy. J. Cardiovasc. Magn. Reson. Off. J. Soc. Cardiovasc. Magn. Reson. 2021, 23, 36. [Google Scholar] [CrossRef]
- Chen, K.; Chang, L.; Huang, R.; Wang, Z.; Mu, D.; Wang, L. Left atrial conduit strain derived from cardiac magnetic resonance is an independent predictor of left ventricular reverse remodeling in patients with nonischemic cardiomyopathy. BMC Med. Imaging 2024, 24, 2. [Google Scholar] [CrossRef]
- Astarita, A.; Mingrone, G.; Airale, L.; Cesareo, M.; Colomba, A.; Catarinella, C.; Leone, D.; Gay, F.; Bringhen, S.; Veglio, F.; et al. Carfilzomib-Based Regimen and Cardiotoxicity in Multiple Myeloma: Incidence of Cardiovascular Events and Organ Damage in Carfilzomib-Dexamethasone versus Carfilzomib-Lenalidomide-Dexamethasone. A Real-Life Prospective Study. Cancers 2023, 15, 955. [Google Scholar] [CrossRef] [PubMed]
- Chen-Scarabelli, C.; Corsetti, G.; Pasini, E.; Dioguardi, F.S.; Sahni, G.; Narula, J.; Gavazzoni, M.; Patel, H.; Saravolatz, L.; Knight, R.; et al. Spasmogenic Effects of the Proteasome Inhibitor Carfilzomib on Coronary Resistance, Vascular Tone and Reactivity. EBioMedicine 2017, 21, 206–212. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| General Characteristics | Total Population (n: 125) | Event (n: 65) | No Event (n: 60) | p-Value (Event vs. No Event) |
|---|---|---|---|---|
| Age, years | 67.7 ± 8.71 | 68.8 ± 9.35 | 66.6 ± 7.87 | 0.145 |
| Female sex, n (%) | 52 (65) | 24 (36.9%) | 28 (46.7%) | 0.356 |
| BSA, m2 | 1.79 ± 0.21 | 1.81 ± 0.21 | 1.77 ± 0.21 | 0.254 |
| BMI, Kg/m2 | 27.3 ± 4.50 | 27.2 ± 4.95 | 27.3 ± 4.00 | 0.889 |
| SBP, mmHg | 129 ± 18.1 | 135 ± 16.1 | 122 ± 17.7 | <0.001 |
| DBP, mmHg | 76.3 ± 11.6 | 78.8 ± 11.2 | 73.6 ± 11.6 | 0.012 |
| Arterial Hypertension, n (%) | 42 (34.4) | 31 (48.4%) | 11 (19.0%) | 0.001 |
| Diabetes, n (%) | 10 (8.06) | 4 (6.15%) | 6 (10.2%) | 0.516 |
| Chronic Ischemic Heart Disease, n (%) | 3 (2.42) | 1 (1.92) | 2 (2.74) | 0.760 |
| Dyslipidemia, n (%) | 19 (15.3) | 7 (10.8%) | 12 (20.3%) | 0.219 |
| Atrial Fibrillation, n (%) | 3 (2.42) | 2 (3.08%) | 1 (1.69%) | 1.000 |
| Smoke status, n (%) | 65 (52.4) | 37 (56.9%) | 28 (47.5%) | 0.140 |
| SCORE-2, % | 8.50 [6.00; 14.1] | 13.0 [6.80; 17.6] | 7.95 [4.85; 11.0] | 0.029 |
| DS day, mmHg | 10.4 [8.76; 13.2] | 11.0 [9.59; 14.9] | 9.81 [7.66; 11.4] | 0.002 |
| BPV | 9.00 [7.00; 10.0] | 9.00 [7.00; 12.0] | 8.00 [6.00; 9.00] | 0.002 |
| PWV, m/s | 7.80 [6.82; 9.36] | 8.75 [7.31; 9.90] | 7.25 [6.42; 8.15] | 0.002 |
| PWV > 9, n (%) | 36 (31.3%) | 28 (46.7%) | 8 (14.5%) | <0.001 |
| AO ASC, mm | 33.6 ± 4.66 | 34.1 ± 3.55 | 33.1 ± 5.63 | 0.302 |
| LVM, g | 161 ± 48.3 | 173 ± 50.4 | 147 ± 42.5 | 0.003 |
| LVMi, g/m2 | 89.8 ± 24.3 | 96.1 ± 26.7 | 83.1 ± 19.4 | 0.002 |
| LVH, % | 42 (34.1%) | 28 (43.07) | 14 (23.33) | 0.018 |
| LVEDV, mL | 90.1 ± 28.0 | 90.3 ± 26.2 | 89.8 ± 30.0 | 0.909 |
| LVEDVi, mL/m2 | 50.4 ± 14.3 | 50.1 ± 13.4 | 50.7 ± 15.3 | 0.802 |
| LVEF, % | 62.3 ± 5.92 | 62.4 ± 6.15 | 62.2 ± 5.70 | 0.850 |
| GLS, % | −21.83 ± 2.51 | −21.39 ± 2.34 | −22.32 ± 2.62 | 0.053 |
| GLS < 20, n (%) | 24 (21.6%) | 16 (27.1%) | 8 (15.4%) | 0.205 |
| TAPSE, mm | 24.0 [21.1; 27.1] | 24.6 [21.1; 26.9] | 23.5 [21.0; 27.1] | 0.417 |
| Diastolic Disfunction, n (%) | 9 (8.26%) | 5 (6.85%) | 4 (5.48%) | 0.704 |
| LAS-r, % | 39.5 ± 11.7 | 37.8 ± 12.2 | 41.4 ± 11.0 | 0.092 |
| LAS-cd, % | −17.90 [−23.60; −13.50] | −16.20 [−20.75; −12.65] | −20.80 [−26.30; −15.40] | 0.006 |
| LAS-ct, % | −19.70 [−25.50; −15.70] | −19.45 [−25.30; −16.27] | −20.00 [−25.50; −15.20] | 0.975 |
| LAVi, mL/m2 | 29.0 ± 8.77 | 29.6 ± 8.95 | 28.4 ± 8.60 | 0.470 |
| LAe, n (%) | 29 (24.4%) | 18 (29.0%) | 11 (19.3%) | 0.307 |
| Hypertensive Adverse Events | Population, n. 125 |
|---|---|
| Total Hypertensive Events, n (%) | 65 (52) |
| Worsening of Chronic Hypertension, n (%) | 60 (48.38) |
| Non-target blood pressure before Carfilzomib infusion (followed by infusion), n (%) | 29 (23.2) |
| Non-target blood pressure before Carfilzomib infusion (not followed by infusion), n (%) | 12 (9.6) |
| Non-target blood pressure after Carfilzomib infusion, n (%) | 18 (14.4) |
| Hypertensive Urgency, n (%) | 5 (4) |
| Hypertensive Emergency, n (%) | 0 (0) |
| Covariate | Beta | HR (95% CI for HR) | p Value | Cox Assumption |
|---|---|---|---|---|
| Age | 0.02 | 1.02 (0.99–1.05) | 0.219 | 0.150 |
| Male sex | 0.23 | 1.26 (0.76–2.08) | 0.376 | 0.203 |
| SBP, (>122 mmHg) | 1.32 | 3.75 (2.04–6.92) | <0.001 | 0.440 |
| DS day (>8 mmHg) | 1.23 | 3.44 (1.37–8.60) | 0.008 | 0.857 |
| BPV (>9) | 0.74 | 2.11 (1.24–3.59) | 0.006 | <0.001 |
| PWV (>9 m/s) | 0.75 | 2.12 (1.26–3.54) | 0.004 | 0.046 |
| AO ASC (>35 mm) | 0.58 | 1.79 (1.01–3.18) | 0.046 | 0.080 |
| LVEDVi (>62 mL/m2) | −0.54 | 0.59 (0.28–1.23) | 0.158 | 0.398 |
| GLS (>23%) | 0.23 | 1.26 (0.70–2.27) | 0.441 | 0.382 |
| LAVi (>37 mL/m2) | 0.59 | 1.81 (1.01–3.23) | 0.047 | 0.086 |
| LAS-cd (>−22%) | 0.88 | 2.40 (1.28–4.51) | 0.006 | 0.582 |
| Covariate | Beta | HR (95% CI for HR) | p Value |
|---|---|---|---|
| SBP (>122 mmHg) | 0.70 | 2.01 (0.72–5.61) | 0.185 |
| DS day (>8 mmHg) | 0.81 | 2.24 (0.60–8.35) | 0.228 |
| BPV (>9) | 0.14 | 1.15 (0.54–2.46) | 0.710 |
| PWV (>9 m/s) | 0.08 | 1.08 (0.50–2.33) | 0.846 |
| AO_asc (>35 mm) | 0.14 | 1.15 (0.56–2.36) | 0.696 |
| LAVi (>37 mL/m2) | 0.06 | 1.06 (0.47–2.41) | 0.887 |
| LAS-cd (>−22%) | 1.97 | 7.16 (1.66–30.88) | 0.008 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Colomba, A.; Airale, L.; Lasagno, A.; Mingrone, G.; Astarita, A.; Vallelonga, F.; Leone, D.; Sanapo, M.; Paladino, A.; Novello, F.; et al. The Emerging Role of Left Atrial Strain in Cardiovascular Risk Stratification for Multiple Myeloma Patients Undergoing Carfilzomib Therapy. Cancers 2025, 17, 2375. https://doi.org/10.3390/cancers17142375
Colomba A, Airale L, Lasagno A, Mingrone G, Astarita A, Vallelonga F, Leone D, Sanapo M, Paladino A, Novello F, et al. The Emerging Role of Left Atrial Strain in Cardiovascular Risk Stratification for Multiple Myeloma Patients Undergoing Carfilzomib Therapy. Cancers. 2025; 17(14):2375. https://doi.org/10.3390/cancers17142375
Chicago/Turabian StyleColomba, Anna, Lorenzo Airale, Alice Lasagno, Giulia Mingrone, Anna Astarita, Fabrizio Vallelonga, Dario Leone, Martina Sanapo, Arianna Paladino, Francesca Novello, and et al. 2025. "The Emerging Role of Left Atrial Strain in Cardiovascular Risk Stratification for Multiple Myeloma Patients Undergoing Carfilzomib Therapy" Cancers 17, no. 14: 2375. https://doi.org/10.3390/cancers17142375
APA StyleColomba, A., Airale, L., Lasagno, A., Mingrone, G., Astarita, A., Vallelonga, F., Leone, D., Sanapo, M., Paladino, A., Novello, F., Bringhen, S., Gay, F., Veglio, F., & Milan, A. (2025). The Emerging Role of Left Atrial Strain in Cardiovascular Risk Stratification for Multiple Myeloma Patients Undergoing Carfilzomib Therapy. Cancers, 17(14), 2375. https://doi.org/10.3390/cancers17142375