Simple Summary
Diffuse midline glioma is a malignant brain tumor with no effective treatment. These tumors often harbor a Histone H3 K27M mutation, associated with a more aggressive clinical course and poorer response to treatment. Standard-of-care treatment is radiation therapy, but disease typically recurs or progresses despite treatment and there is a paucity of the literature specific to the features and outcomes of recurrent disease. Given this, our group sought to explore what factors may be associated with disease progression and clinical outcomes to guide disease management and prognosis. Through a multicenter retrospective analysis of clinical data from patients with recurrent midline glioma and H3 K27M-mutant diffuse glioma, we identified features associated with poorer overall survival following progression following frontline therapy. Taken together, these data provide insight into tumor biology and clinical outcomes, potentially informing future clinical trials.
Abstract
Background/Objectives: Midline glioma is a frequently morbid primary brain tumor often characterized by the histone mutation H3 K27M. The standard-of-care treatment is radiation therapy in the frontline setting, though effective treatment remains elusive and there is no established therapy in the second line or later setting. Here, we present the results of a multicenter, observational, retrospective study of the natural history of this disease in the recurrent setting when managed via standard-of-care interventions. Methods: Forty-four patients with recurrent H3 K27M-mutant and/or midline glioma after standard-of-care treatment were identified across 11 clinical centers in the United States who met inclusion criteria for evaluation. Data collected were analyzed by tumor radiographic appearance, age, anatomic location, and H3 K27M status, with factors contributing to overall survival (OS) identified. Results: Overall, median OS from time of first recurrence was 5.1 months (95% CI, 3.9 to 7.7%). In a subgroup analysis, survival was dismal across primary tumor locations, with a median OS of 3.7 months (95% CI: 0.7 to 9.8 months), 3.5 months (95% CI, 0.9 to not reached) for primary spinal, 5.1 months (95% CI to 0.2 not reached) for primary infratentorial, and 5.9 months (95% CI 4.4 to 14.7) for primary supratentorial tumors. In a multivariate analysis, DIPG and primary spinal tumor were associated with a higher risk of death. Conclusions: Taken together, these results shed light on prognostic factors and natural disease progression overtly related to recurrent midline and/or H3 K27M-mutant diffuse glioma, providing insight that can prove valuable for development of future clinical treatments for this recently defined disease.
1. Introduction
High-grade glial tumors represent the most morbid form of brain cancer [1]. Approximately 80% of midline gliomas and 5% of cerebral hemispheric gliomas harbor a K27M mutation in the genes encoding isoforms of the Histone proteins H3.1 or H3.3 [2,3,4,5,6,7,8,9]. This somatic missense mutation is known as H3 K27M, and is associated with loss of H3 K27 trimethylation, poorer response to standard therapy, and lower overall survival, especially in younger patients [10]. To date, radiotherapy is the standard therapeutic intervention for diffuse midline gliomas, but only provides a median six-month event-free survival, with little effect on overall survival [5,10]. As such, the presence of an H3 K27M mutation in a midline tumor now confers a WHO Grade 4 status [11,12,13,14,15]. Indeed, if untreated, patients suffering from H3 K27M-mutant diffuse intrinsic pontine glioma (DIPG) have a median survival of only 1–4.5 months from diagnosis [6,16,17,18]. Further research has since revealed additional molecular characteristics of H3 K27M-mutant tumors, including distinct protein, RNA, DNA methylation, and epigenetic profiles [15]. This recent work has shed some light on a few novel prognostic factors in H3 K27M DMG, such as FGFR1 mutations that are associated with a more favorable clinical prognosis. However, there remains limited published information about prognostic factors and disease progression overtly related to the H3 K27M mutation in glioma [19], particularly in the recurrent setting. Therefore, we conducted a clinical history study that aimed to define outcomes and prognostic factors in patients with recurrent H3 K27M-mutant and/or midline glioma.
2. Materials and Methods
We performed a multicenter, retrospective, descriptive, observational study in patients with recurrent midline and/or H3 K27M-mutant glioma, to describe outcomes and prognostic factors associated with survival. Data were collected via retrospective chart reviews from eleven clinical centers across the United States (Supplemental Table S1); the protocol was approved by participating sites prior to study initiation. The clinical investigative site primary investigator was responsible for reviewing the medical records of potential patients. This retrospective, observational study was conducted with only the available medical records and imaging scans. All patient data collected were pseudonymized in the database. The primary objective for this analysis was to determine prognostic factors for overall survival (OS). Of note, this study was terminated by the sponsor prior to activation of all planned sites/countries and prior to achievement of complete enrollment in both cohorts. The early termination was based on revised regulatory agency feedback related to the utility of data from this study in regulatory decision-making, and resulted in lower patient enrollment than initially planned.
A potential patient was required to have met all the following criteria to be eligible for inclusion in the study:
- Diagnosis of H3 K27M-mutant and/or midline glioma, initially diagnosed in 2012 or later.
- Known tissue-proven H3 K27 status (H3 K27M-mutant or wild-type).
- Medical records (including clinic notes and/or electronic databases) relating to glioma diagnosis and treatments received must be available for review. (Minimum information included demographics, disease characteristics, histology, disease history [diagnosis, tumor location, recurrences], radiation and other treatment history, survival status, and death date if applicable.)
- Presence of recurrent disease after standard-of-care therapy.
- No Prior Treatment with ONC201 or ONC 206.
2.1. Patients
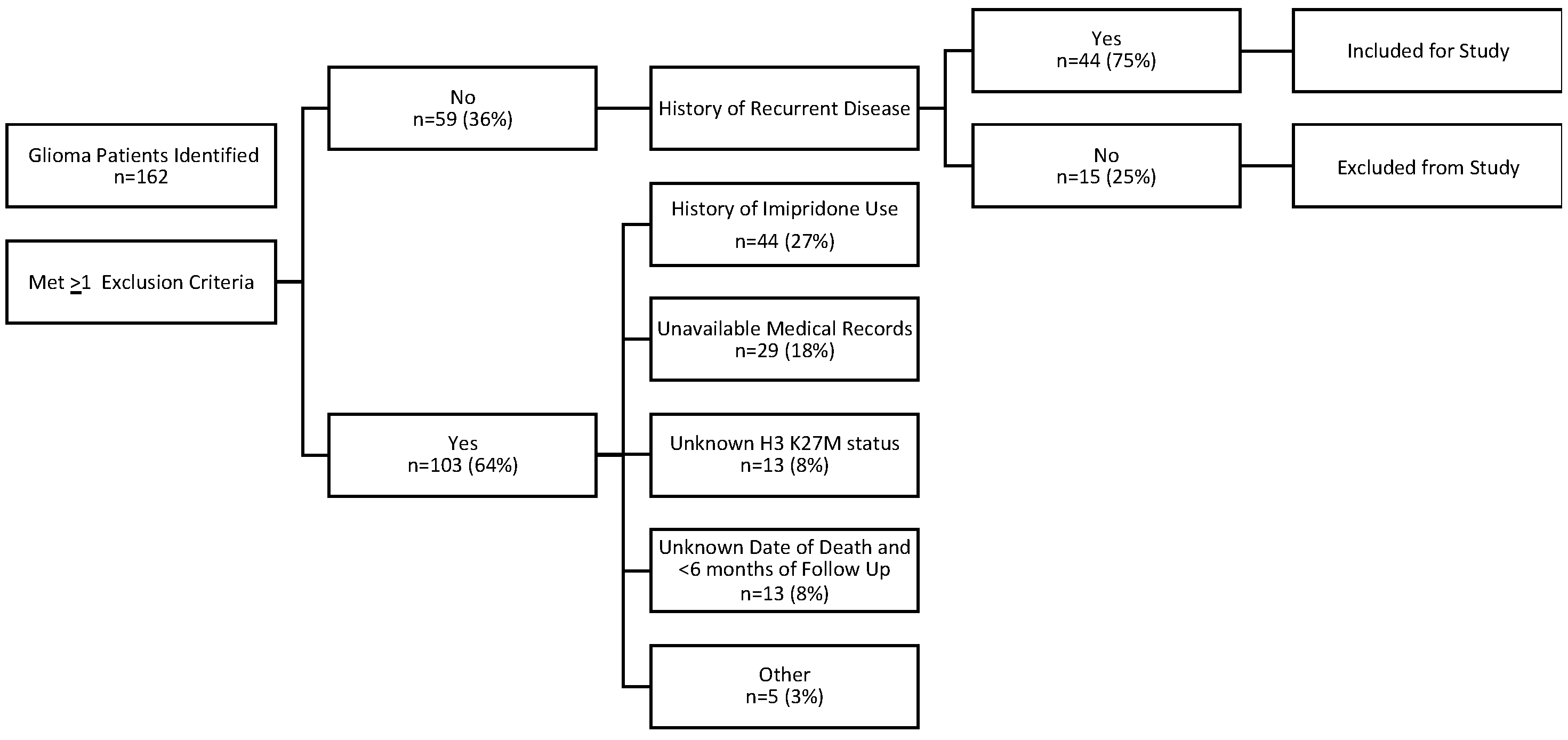
This study was intended to evaluate prognostic factors for survival in patients with biopsy-proven recurrent H3 K27M-mutant and/or midline glioma. A total of 162 potential patients were identified across participating institutions, with 44 patients with recurrent disease meeting the criteria for this analysis (Figure 1). Primary reasons for exclusion from analysis included treatment with ONC201 or ONC206 at any time (27.2%), insufficient medical records available (17.9%), unknown H3 K27M status (8%), and either an unknown date of death or <6 months survival follow-up from initial diagnosis (8%). One of the forty-four patients had no follow-up after first recurrence and therefore was censored as of first recurrence.
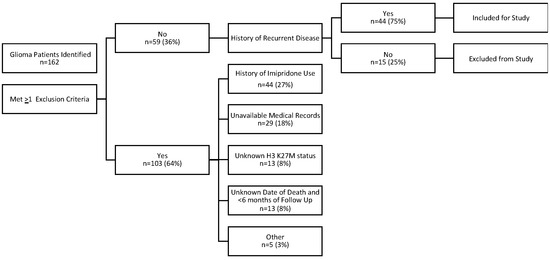
Figure 1.
Patient selection flowchart citing inclusion and exclusion criteria and numbers ultimately yielding n = 44 patient records analyzed in the present study.
2.2. Evaluation and Statistical Methods
OS was estimated from first recurrence using the Kaplan–Meier (KM) method with median survival times and corresponding 95% confidence intervals (CIs) presented. KM survival estimates are presented at 12 and 24 months with corresponding 95% CIs. Multivariate Cox proportional hazard models were used to assess the impact of factors on survival. Final models following backward selection are presented with p-values, hazard ratios, and 95% CIs for each factor. It should be noted for some comparisons, analysis is exploratory in nature due to small sample size and as reflected by wide confidence intervals.
3. Results
Of the 162 glioma patient records reviewed, a total of 44 patients met the specified criteria and had evidence of recurrent/progressive disease (Figure 1): 30 patients (50.8%) with one recurrence, 9 patients (15.3%) with two recurrences, and 5 patients (6.8%) with ≥three recurrences. H3 K27M mutation was present in 68.2% of patients with recurrent disease (n = 30), with the remainder lacking the H3 K27M mutation (Table 1). Among the patients with the H3 K27M mutation, four (9.1%) patients had non-midline primary tumor locations, and the remainder had midline primary tumor locations. The median age of patients analyzed was 28 years (range 4 to 68 years) with 16 (36.4%) being less than 18 years of age. An even number of patients were male (n = 22) and female (n = 22), while the majority were White (68.2%) and not Hispanic or Latino (79.5%, Table 1).

Table 1.
Patient demographic characteristics at first recurrence (N = 44) 1.
All 44 patients analyzed had a tissue-proven diagnosis of glioma and received frontline radiation therapy as required for study eligibility. A total of 21 (47.7%) of these patients underwent a surgical procedure (sub, near, or gross total resection) in lieu of or in addition to a diagnostic biopsy. In addition to frontline radiation therapy, a wide range of anticancer agents were used as second-line therapy at the time of recurrence. The most common of these included temozolomide in 25 patients (56.8%), and bevacizumab in 7 patients (15.9%, Supplemental Table S2). Seven patients (11.9%) received re-irradiation during their disease course.
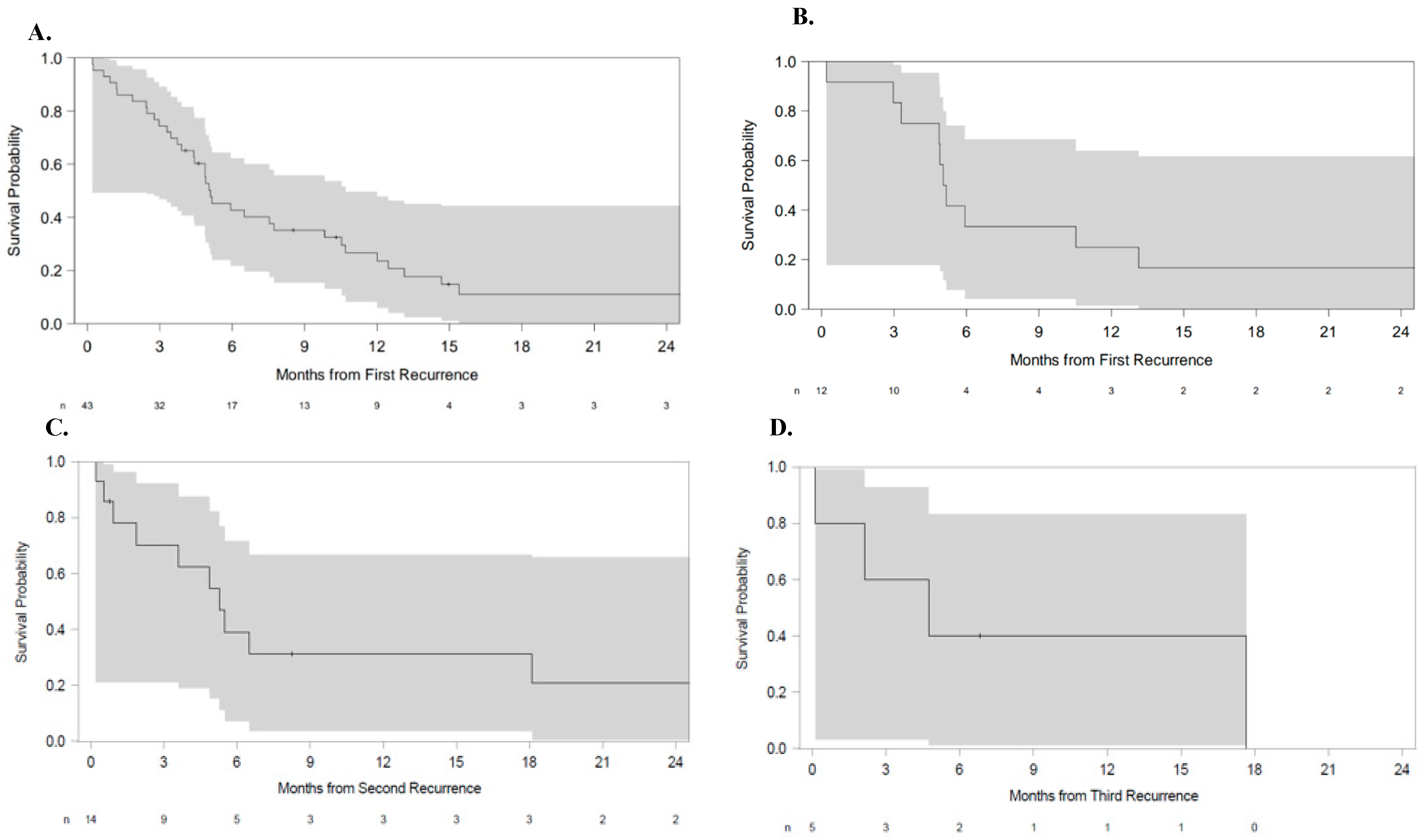
The median OS from the time of first recurrence was 5.1 months (95% CI: 3.9 to 7.7 months, Figure 2A). Excluding patients with DIPG, leptomeningeal spread, CSF dissemination, or primary spinal tumors (n = 12), the median OS was also 5.1 months (95% CI 3.0–13.1 months) (Figure 2B). Of the 14 patients reported to have two or more instances of recurrence, the median OS from second recurrence was 5.3 months (95% CI: 0.9 to 18.1 months) (Figure 2C). Of the remaining five patients with at least three instances of disease recurrence, the median OS from third recurrence was 4.7 months (95% CI: 0.1 to not reached) (Figure 2D).
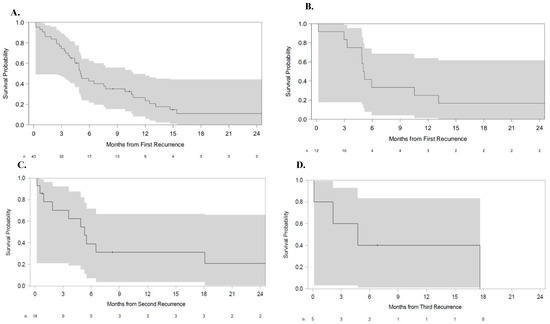
Figure 2.
Overall survival (A) from first recurrence in all patients, (B) from first recurrence in patients excluding DIPG, leptomeningeal spread, CSF dissemination, or primary spinal tumors, (C) from second recurrence, and (D) from third recurrence. In general, OS was identical (5.1 months) from first recurrence in all patients, and in the cohort of patients excluding DIPG, leptomeningeal spread, CSF dissemination, and spinal tumors (A and B, respectively). Survival at second recurrence (5.3 months) was slightly longer than that at third recurrence (4.7 months, C and D, respectively). Shaded areas represent the 95% CI.
Figure 2 shows patient survival after disease recurrence.
3.1. Analysis by H3 K27M Status
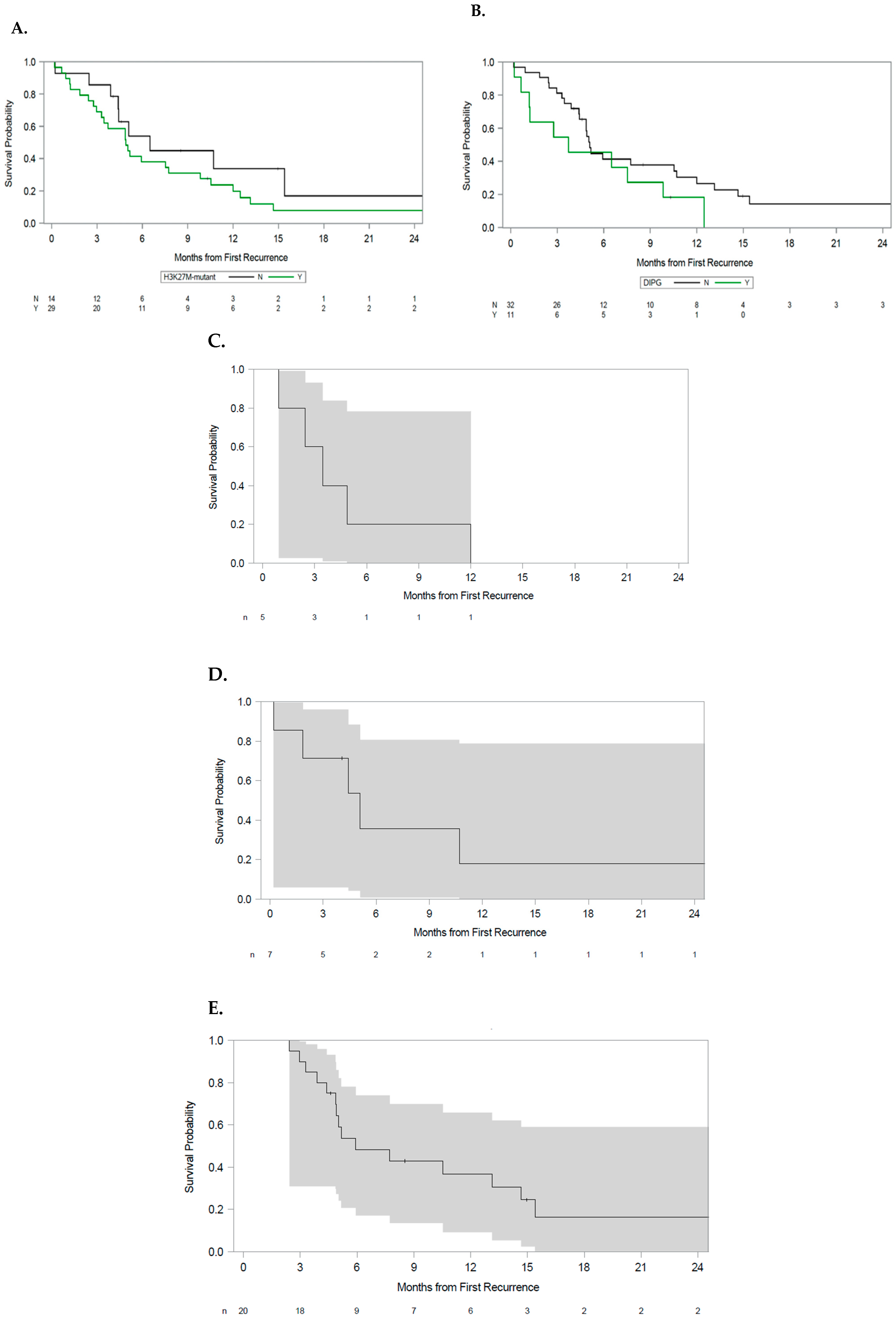
Patients with the H3 K27M mutation had a median overall survival of 4.9 months (95% CI: 3.0 to 7.7 months). We observed a potential association between the presence of H3 K27M mutation (n = 30) and shorter overall survival; however, this relationship was not statistically significant (HR 1.8, 95% CI 0.8 to 3.8, p = 0.14, Figure 3A).
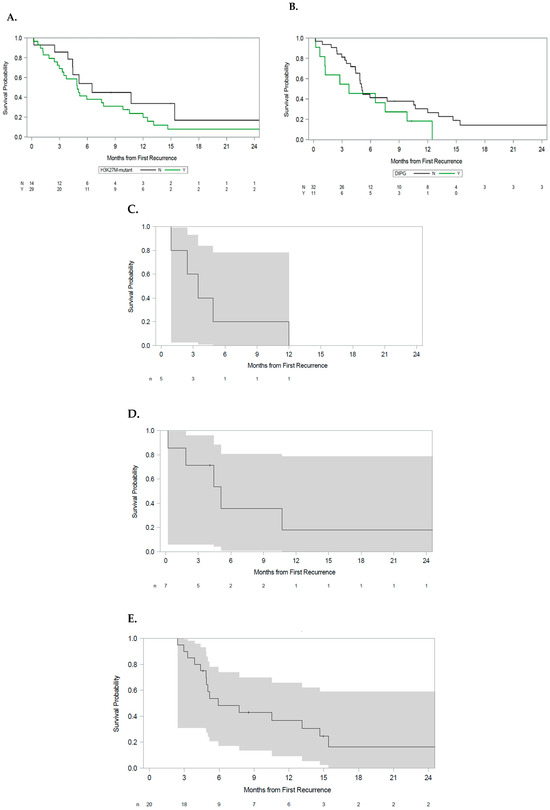
Figure 3.
Overall survival by (A) H3 K27M mutation status, (B) DIPG versus other patients, (C) primary spinal tumors, (D) infratentorial tumors excluding DIPG, and (E) supratentorial tumors. Shaded areas represent the 95% CI.
3.2. Analysis by Tumor Anatomic Origin
Patients with DIPG had a median OS from the time of first disease recurrence of 3.7 months (95% CI: 0.7 to 9.8 months). Patients with DIPG exhibited a trend toward worse survival compared to those patients without this diagnosis, although statistical significance was not reached (HR: 1.8, 95% CI 0.8 to 3.8, p = 0.14, Figure 3B).
Among patients with primary spinal tumors, overall survival for patients with primary spinal lesions from the time of first recurrence was 3.5 months (95% CI 0.9 to not reached, Figure 3C). Patients with infratentorial tumors had an OS of 5.1 months from the time of first recurrence (95% CI to 0.2 not reached Figure 3D). Patients with supratentorial lesions had an OS from the time of first disease recurrence of 5.9 months (95% CI 4.4 to 14.7, Figure 3E).
3.3. Multivariate Analysis
Multivariate Cox proportional hazard models conducted at first recurrence demonstrated that DIPG and primary spinal tumor were associated with a higher risk of death. HRs were 3.64 (95% CI: 1.41 to 9.45) and 4.69 (95% CI: 1.47 to 14.99), respectively (Table 2). Sub-total resections (n = 16) demonstrated a trend toward lowered risk of death (HR: 0.43; 95% CI: 0.19 to 1.01; p = 0.052). Due to the small sample size of patients with gross total resection (n = 2) and near gross resection (n = 3), the risk was inconclusive (Supplemental Figure S1).
Table 2.
Multivariate overall survival model, first recurrence final Cox model presented following backward selection, removing factors with p > 0.20. Improved overall survival HR < 1.0. Factors considered: sex, H3 K27M status, pediatric/adult, performance status, tumor size, resection, multifocal disease, DIPG/primary tumor location, contrast enhancement, steroid use, CSF dissemination, and leptomeningeal spread.
4. Discussion
Diffuse midline glioma is a highly morbid primary brain tumor, and despite recent advances in our understanding of tumor biology and the study of more targeted therapies, effective treatment remains elusive. While standard-of-care interventions, including radiation +/− adjuvant therapy, are still the mainstay for DMG treatment, studies of novel approaches are currently underway for both initial and recurrent disease, critical efforts given the likelihood of disease progression and/or recurrence despite standard treatment.
For example, the role of re-irradiation and bevacizumab in the setting of recurrent high-grade glioma has been studied, with some reports suggesting improved OS [20]. Re-irradiation alone for recurrent DMG is also reported to show some survival benefit and improvement in neurologic deficits [21], but more studies are still needed to determine which patients will benefit from these additional therapies. Recent studies have also focused on more advanced and nuanced epigenetic features, including histone post-translational modification patterns and 3D chromatin structure, as well as molecular subtyping and prognostic modeling in H3 K27M gliomas [22,23,24]. These studies suggest novel potential biomarkers for prediction of treatment response and disease recurrence, and therefore warrant further investigation. Indeed, a recent study of adult glioma highlights the prognostic and predictive impact of key molecular alterations, such as IDH mutation and MGMT promotor methylation status [25], suggesting using a molecular approach to guide therapy is clinically relevant and feasible.
Yet despite these multiple ongoing and promising efforts, there remains a continued need to better understand the factors that drive treatment response and disease recurrence in patients with diffuse midline glioma. Here, we performed a multicenter, observational, retrospective exploratory study of the natural history of recurrent disease after management with standard-of-care interventions (radiation +/− adjuvant therapy). A variety of useful observations were made through the analysis of these data, many substantiating prior study findings of this tumor population, and others pointing to important factors for consideration of clinical management of these patients.
Firstly, a tumor with a pontine epicenter and diffuse appearance on MRI, consistent with diagnosis of DIPG, was associated with worse prognosis at first recurrence compared to tumors arising primarily in other anatomic locations. These data are in line with other reports suggesting that, when compared to patients with brainstem tumors, patients with other lesions such as in the thalamus experience significantly better survival [26]. As with previous reports in the literature, the presence of H3 K27M mutation in patients with recurrent disease was found to be associated with a trend toward worse OS in our study, though these findings were not statistically significant. The validity of this result is likely undermined by our study being underpowered, secondary to issues with achieving intended sample size and enrollment due to premature closure of the study. These factors likely impacted the statistical significance of the detected effect of H3K27M-mutant status on OS. To this end, Vuong et al. performed an extensive literature review comprising 26 studies and over 600 patients harboring H3.1 (n = 102) or H3.3 mutations (n = 529), finding that the prognosis of H3 K27M mutation in DMG patients is modulated by patient age, with poorer survival in children with the H3.3 mutation relative to adults [27]. Zheng et al. also performed a retrospective review of a series of pediatric and adult patients with diffuse midline gliomas harboring the H3 K27M mutation (n = 164), and found prognosis was better for adult patients than the pediatric cohort [28]. The results of these studies and our data suggest that the presence of H3 K27M mutation may be a greater prognostic factor when patient age is considered.
One particularly unique dataset arising from this study is the measure of OS in the setting of tumor recurrence. The median OS measured from first recurrence was 5.1 months. Importantly, prognosis at disease recurrence differed by disease location, with DIPG and primary spinal tumor associated with a higher risk of death after first recurrence. Due to the small sample size in this study, our analysis was not able to adequately determine any survival benefit or the risk of death after gross total resection (n = 2) versus near gross resection (n = 3). Other studies have shown that there is no survival benefit to greater extent of resection with midline gliomas [29,30]. In contrast, in the same study, preoperative KPS and adjuvant radiotherapy have been found to be independent clinical parameters influencing OS [29]. Taken together, these studies suggest that multiple factors must be considered when guiding patients regarding prognosis of recurrent disease.
Our study is not without limitations. Due to the early termination of the study, as described above in the Methods section, we did not achieve the full enrollment, with only 11 centers enrolling and all within the United States. The large difference in anticipated versus actual accrual limits the size of available subgroups in our subgroup analyses, and some multivariate analyses resulted in wide confidence intervals due to low numbers in comparison groups.
Another important point is that additional molecular features important to DMG biology have recently been discovered. For example, the current WHO classification now subsumes midline gliomas with H3 K27M mutations together with gliomas showing aberrant EZHIP expression or with an EGFR mutation. However, the analyzed specimens reported here were from patients initially diagnosed from 2012 to 2021, and hence not tested for molecular features like EZHIP or EFGR, which have since been discovered to be important in DMG biology.
5. Conclusions
There are limited data describing natural disease history and progression, as well as prognostic factors, in H3 K27M-mutant glioma, particularly in the recurrent setting. The outcomes described here, while exploratory in nature, shed some light on clinical outcomes and prognostic factors in the recurrent setting. The small sample size reported here highlights the crucial nature of multicenter collaborative studies for rare diseases. Much work is left to be performed to identify treatment modalities that alter the natural course of disease progression in H3 K27M-mutant glioma.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/cancers17132107/s1, Supplemental Table S1: Second-line therapies received. Table S2: Second Line Therapies Received. Supplemental Figure S1: Overall Survival after Disease recurrence. Hazard ratio with 95% Confidence Interval (CI) depicted.
Author Contributions
Conceptualization, J.E.A., R.S.T., S.C.R., P.Y.W., I.A.-R., T.B., and T.C.; methodology, J.E.A., R.S.T., S.C.R., P.Y.W., I.A.-R., T.B., and T.C.; formal analysis, T.B., S.C.R., T.C., A.M.S., and D.Y.; investigation, S.J.B., Y.U., J.S.M., I.A.-R., K.J.B., N.B., K.H., X.-T.K., Y.O., A.S., L.W., C.K., P.Y.W., and T.K.; writing—original draft preparation, A.M.S.; writing—review and editing, A.M.S., T.B., S.C.R., J.E.A., and R.S.T. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Chimerix, Inc., a subsidiary of Jazz Pharmaceuticals.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Boards at participating medical centers as Appendix A.
Informed Consent Statement
Patient consent was waived due to retrospective, blinded data analysis study design.
Data Availability Statement
Patient-level data collected as part of this analysis are not available for analysis by independent researchers. For more information, please contact clinicaltrials@chimerix.com.
Conflicts of Interest
Patrick Wen, Isabel Arrillaga-Romany, Nick Butowski, Yazmin Odia, Akanksha Sharma, Yoshie Umemura, Lauren Weintraub, Timothy Cloughesy, and Stephen J. Bagley have received research and/or clinical trial support from Chimerix, Inc., a subsidiary of Jazz Pharmaceuticals. Amanda M. Saratsis is a paid consultant for Chimerix, Inc. Patrick Wen has served on an advisory board for Chimerix, Inc. Dewen Yang was an employee of Chimerix, Inc. at the time of the conduct of this study. Tom Brundage, Samuel C. Ramage, Rohinton Tarapore, and Joshua E. Allen are employees of and have stock ownership in Chimerix, Inc. Joshua E. Allen has royalties and licenses associated with ONC201 and related products, and has patents for ONC201 and related products. Truman Knowles, Joe S. Mendez, Kevin J. Bielamowicz, and Xiao-Tang Kong have no relevant conflicts of interest to declare.
Appendix A
| PI Name | Institution | IRB | IRB Study Code |
| Yazmin Odia | Miami Cancer Institute | Advarra IRB | SSU00180912 |
| Kevin Bielamowicz | Arkansas Children’s Hospital | University of Arkansas for Medical Sciences IRB | 274102 |
| Lauren Weinbtraub | Albany Medical Center | Advarra IRB | SSU00180912 |
| Xiao-Tang Kong | University of California, Irvine | University of California, Irvine Office of Research IRB | UCI IRB #769 |
| Joe Mendez | The University of Utah, Huntsman Cancer Institute | The University of Utah IRB | IRB_00124158 |
| Akanksha Sharma | Providence Saint John’s Health Center | Advarra IRB | SSU00180912 |
| Yoshie Umemura | University of Michigan Health System | University of Michigan Medical School IRB | HUM00188956 |
| Nicholas Butowski | University of California San Francisco | University of California San Francisco Human Research Protection Program IRB | 257857 |
| Isabel Arrillaga | Massachusetts General Hospital | Dana Farber Cancer Institute Office for Human Research Studies IRB | 20–639 |
| Stephen Bagley | University of Pennsylvania Pearlman Center for Advance Medicine | Office of the Institutional Review Board University of Pennsylvania | 850834 |
References
- Weller, M.; van den Bent, M.; Preusser, M.; Le Rhun, E.; Tonn, J.C.; Minniti, G.; Bendszus, M.; Balana, C.; Chinot, O.; Dirven, L.; et al. EANO guidelines on the diagnosis and treatment of diffuse gliomas of adulthood. Nat. Rev. Clin. Oncol. 2020, 18, 170–186. [Google Scholar] [CrossRef] [PubMed]
- Khuong-Quang, D.-A.; Buczkowicz, P.; Rakopoulos, P.; Liu, X.-Y.; Fontebasso, A.M.; Bouffet, E.; Bartels, U.; Albrecht, S.; Schwartzentruber, J.; Letourneau, L.; et al. K27M mutation in histone H3.3 defines clinically and biologically distinct subgroups of pediatric diffuse intrinsic pontine gliomas. Acta Neuropathol. 2012, 124, 439–447. [Google Scholar] [CrossRef] [PubMed]
- Schwartzentruber, J.; Korshunov, A.; Liu, X.-Y.; Jones, D.T.W.; Pfaff, E.; Jacob, K.; Sturm, D.; Fontebasso, A.M.; Khuong-Quang, D.-A.; Tönjes, M.; et al. Driver mutations in histone H3.3 and chromatin remodelling genes in paediatric glioblastoma. Nature 2012, 482, 226–231, Erratum in Nature 2012, 484, 130. [Google Scholar] [CrossRef]
- Saratsis, A.M.; Kambhampati, M.; Snyder, K.; Yadavilli, S.; Devaney, J.M.; Harmon, B.; Hall, J.; Raabe, E.H.; An, P.; Weingart, M.; et al. Comparative multidimensional molecular analyses of pediatric diffuse intrinsic pontine glioma reveals distinct molecular subtypes. Acta Neuropathol. 2013, 127, 881–895. [Google Scholar] [CrossRef] [PubMed]
- Karremann, M.; Gielen, G.H.; Hoffmann, M.; Wiese, M.; Colditz, N.; Warmuth-Metz, M.; Bison, B.; Claviez, A.; van Vuurden, D.G.; O von Bueren, A.; et al. Diffuse high-grade gliomas with H3 K27M mutations carry a dismal prognosis independent of tumor location. Neuro-Oncology 2017, 20, 123–131. [Google Scholar] [CrossRef]
- Erker, C.; Lane, A.; Chaney, B.; Leary, S.; E Minturn, J.; Bartels, U.; Packer, R.J.; Dorris, K.; Gottardo, N.G.; E Warren, K.; et al. Characteristics of patients ≥10 years of age with diffuse intrinsic pontine glioma: A report from the International DIPG/DMG Registry. Neuro-Oncology 2021, 24, 141–152. [Google Scholar] [CrossRef]
- Aihara, K.; Mukasa, A.; Gotoh, K.; Saito, K.; Nagae, G.; Tsuji, S.; Tatsuno, K.; Yamamoto, S.; Takayanagi, S.; Narita, Y.; et al. H3F3A K27M mutations in thalamic gliomas from young adult patients. Neuro-Oncology 2013, 16, 140–146. [Google Scholar] [CrossRef]
- Meyronet, D.; Esteban-Mader, M.; Bonnet, C.; Joly, M.-O.; Uro-Coste, E.; Amiel-Benouaich, A.; Forest, F.; Rousselot-Denis, C.; Burel-Vandenbos, F.; Bourg, V.; et al. Characteristics of H3 K27M-mutant gliomas in adults. Neuro-Oncology 2017, 19, 1127–1134. [Google Scholar] [CrossRef]
- Ebrahimi, A.; Skardelly, M.; Schuhmann, M.U.; Ebinger, M.; Reuss, D.; Neumann, M.; Tabatabai, G.; Kohlhof-Meinecke, P.; Schittenhelm, J. High frequency of H3 K27M mutations in adult midline gliomas. J. Cancer Res. Clin. Oncol. 2019, 145, 839–850. [Google Scholar] [CrossRef]
- Lu, V.M.; Alvi, M.A.; McDonald, K.L.; Daniels, D.J. Impact of the H3K27M mutation on survival in pediatric high-grade glioma: A systematic review and meta-analysis. J. Neurosurg. Pediatr. 2019, 23, 308–316. [Google Scholar] [CrossRef]
- Pagès, M.; Beccaria, K.; Boddaert, N.; Saffroy, R.; Besnard, A.; Castel, D.; Fina, F.; Barets, D.; Barret, E.; Lacroix, L.; et al. Co-occurrence of histone H3 K27M and BRAF V600E mutations in paediatric midline grade I ganglioglioma. Brain Pathol. 2016, 28, 103–111. [Google Scholar] [CrossRef]
- Joyon, N.; Tauziède-Espariat, A.; Alentorn, A.; Giry, M.; Castel, D.; Capelle, L.; Zanello, M.; Varlet, P.; Bielle, F. K27M mutation in H3F3A in ganglioglioma grade I with spontaneous malignant transformation extends the histopathological spectrum of the histone H3 oncogenic pathway. Neuropathol. Appl. Neurobiol. 2017, 43, 271–276. [Google Scholar] [CrossRef] [PubMed]
- Mosaab, A.; El-Ayadi, M.; Khorshed, E.N.; Amer, N.; Refaat, A.; El-Beltagy, M.; Hassan, Z.; Soror, S.H.; Zaghloul, M.S.; El-Naggar, S. Histone H3K27M Mutation Overrides Histological Grading in Pediatric Gliomas. Sci. Rep. 2020, 10, 8368. [Google Scholar] [CrossRef] [PubMed]
- Findlay, I.J.; De Iuliis, G.N.; Duchatel, R.J.; Jackson, E.R.; Vitanza, N.A.; Cain, J.E.; Waszak, S.M.; Dun, M.D. Pharmaco-proteogenomic profiling of pediatric diffuse midline glioma to inform future treatment strategies. Oncogene 2021, 41, 461–475. [Google Scholar] [CrossRef]
- Solomon, D.A.; Wood, M.D.; Tihan, T.; Bollen, A.W.; Gupta, N.; Phillips, J.J.J.; Perry, A. Diffuse Midline Gliomas with Histone H3-K27M Mutation: A Series of 47 Cases Assessing the Spectrum of Morphologic Variation and Associated Genetic Alterations. Brain Pathol. 2015, 26, 569–580. [Google Scholar] [CrossRef] [PubMed]
- Langmoen, I.A.; Lundar, T.; Storm-Mathisen, I.; Lie, S.O.; Hovind, K.H. Management of pediatric pontine gliomas. Child’s Nerv. Syst. 1991, 7, 13–15. [Google Scholar] [CrossRef]
- Hoffman, L.M.; van Zanten, S.E.V.; Colditz, N.; Baugh, J.; Chaney, B.; Lane, A.; Fuller, C.; Miles, L.; Hawkins, C.; Bartels, U.; et al. HG-75 Clinical, Radiological, and Histo-Genetic Characteristics of Long-Term Survivors of Diffuse Intrinsic Pontine Glioma: A Collaborative Report from the International and SIOP-E Dipg Registries. Neuro-Oncology 2016, 18, iii65–iii66. [Google Scholar] [CrossRef]
- Baugh, J.; Colditz, N.; Janssens, G.; Dietzsch, S.; Hargrave, D.; von Bueren, A.; Kortmann, R.-D.; Bison, B.; van Vuurden, D.; van Zanten, S.V.; et al. DIPG-77 Treatment Extent and the Effect on Survival in Diffuse Intrinsic Pontine Glioma. Neuro-Oncology 2020, 22, iii302. [Google Scholar] [CrossRef]
- Schüller, U.; Iglauer, P.; Dorostkar, M.M.; Mawrin, C.; Herms, J.; Giese, A.; Glatzel, M.; Neumann, J.E. Mutations within FGFR1 are associated with superior outcome in a series of 83 diffuse midline gliomas with H3F3A K27M mutations. Acta Neuropathol. 2021, 141, 323–325. [Google Scholar] [CrossRef]
- Kulinich, D.P.; Sheppard, J.P.; Nguyen, T.; Kondajji, A.M.; Unterberger, A.; Duong, C.; Enomoto, A.; Patel, K.; Yang, I. Radiotherapy versus combination radiotherapy-bevacizumab for the treatment of recurrent high-grade glioma: A systematic review. Acta Neurochir. 2021, 163, 1921–1934. [Google Scholar] [CrossRef]
- Shariff, N.; Moreno, A.S.; Bennett, J.; Ramaswamy, V.; Das, A.; Liu, A.P.; Huang, A.; Tabori, U.; Hawkins, C.; Dirks, P.; et al. Re-irradiation for children with diffuse intrinsic pontine glioma and diffuse midline glioma. Radiother. Oncol. 2025, 207, 110865. [Google Scholar] [CrossRef] [PubMed]
- Furth, N.; Algranati, D.; Dassa, B.; Beresh, O.; Fedyuk, V.; Morris, N.; Kasper, L.H.; Jones, D.; Monje, M.; Baker, S.J.; et al. H3-K27M-mutant nucleosomes interact with MLL1 to shape the glioma epigenetic landscape. Cell Rep. 2022, 39, 110836. [Google Scholar] [CrossRef]
- Wang, J.; Huang, T.Y.-T.; Hou, Y.; Bartom, E.; Lu, X.; Shilatifard, A.; Yue, F.; Saratsis, A. Epigenomic landscape and 3D genome structure in pediatric high-grade glioma. Sci. Adv. 2021, 7, eabg4126. [Google Scholar] [CrossRef] [PubMed]
- Bhattarai, S.; Hakkim, F.L.; Day, C.A.; Grigore, F.; Langfald, A.; Entin, I.; Hinchcliffe, E.H.; Robinson, J.P. H3F3A K27M mutations drive a repressive transcriptome by modulating chromatin accessibility independent of H3K27me3 in Diffuse Midline Glioma. Epigenet. Chromatin 2025, 18, 23. [Google Scholar] [CrossRef]
- Saaid, A.; Monticelli, M.; Ricci, A.A.; Orlando, G.; Botta, C.; Zeppa, P.; Bianconi, A.; Osella-Abate, S.; Bruno, F.; Pellerino, A.; et al. Prognostic Analysis of the IDH1 G105G (rs11554137) SNP in IDH-Wildtype Glioblastoma. Genes 2022, 13, 1439. [Google Scholar] [CrossRef]
- Vuong, H.G.; Le, H.T.; Jea, A.; McNall-Knapp, R.; Dunn, I.F. Risk stratification of H3 K27M–mutant diffuse midline gliomas based on anatomical locations: An integrated systematic review of individual participant data. J. Neurosurg. Pediatr. 2022, 30, 99–106. [Google Scholar] [CrossRef]
- Vuong, H.G.; Ngo, T.N.M.; Le, H.T.; Dunn, I.F. The prognostic significance of HIST1H3B/C and H3F3A K27M mutations in diffuse midline gliomas is influenced by patient age. J. Neuro-Oncol. 2022, 158, 405–412. [Google Scholar] [CrossRef] [PubMed]
- Zheng, L.; Gong, J.; Yu, T.; Zou, Y.; Zhang, M.; Nie, L.; Chen, X.; Yue, Q.; Liu, Y.; Mao, Q.; et al. Diffuse Midline Gliomas With Histone H3 K27M Mutation in Adults and Children. Am. J. Surg. Pathol. 2022, 46, 863–871. [Google Scholar] [CrossRef]
- Wang, Y.; Feng, L.-L.; Ji, P.-G.; Liu, J.-H.; Guo, S.-C.; Zhai, Y.-L.; Sankey, E.W.; Wang, Y.; Xue, Y.-R.; Wang, N.; et al. Clinical Features and Molecular Markers on Diffuse Midline Gliomas With H3K27M Mutations: A 43 Cases Retrospective Cohort Study. Front. Oncol. 2021, 10, 602553. [Google Scholar] [CrossRef]
- Manjunath, N.; Jha, P.; Singh, J.; Raheja, A.; Kaur, K.; Suri, A.; Garg, A.; Sharma, M.C.; Sarkar, C.; Mohan, M.; et al. Clinico-pathological and molecular characterization of diffuse midline gliomas: Is there a prognostic significance? Neurol. Sci. 2020, 42, 925–934. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).