



Impact of Bowel Resection on Operative Mortality and Overall Survival in Advanced Epithelial Ovarian Cancer
 , ,
, ,
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Ethical Approval
2.2. Patient Selection
2.3. Surgical Evaluation and Procedures
2.4. Postoperative Management and Follow-Up
2.5. Data Collection
2.6. Outcome Definitions
2.7. Statistical Analysis
- Age (continuous).
- Histological subtype (categorical: low grade serous, mucinous, mixed, transitional, carcinoid; reference: high-grade serous).
- Timing of surgery (primary cytoreductive surgery vs. interval debulking surgery).
- Secondary cytoreduction (yes/no).
- Stoma formation (yes/no).
- Residual disease status (optimal vs suboptimal).
- Platinum resistance (yes/no).
- Lymph node resection (yes/no).
3. Results
3.1. Patients and Extent of Disease
3.2. Primary Outcomes
3.2.1. Clinical Outcomes
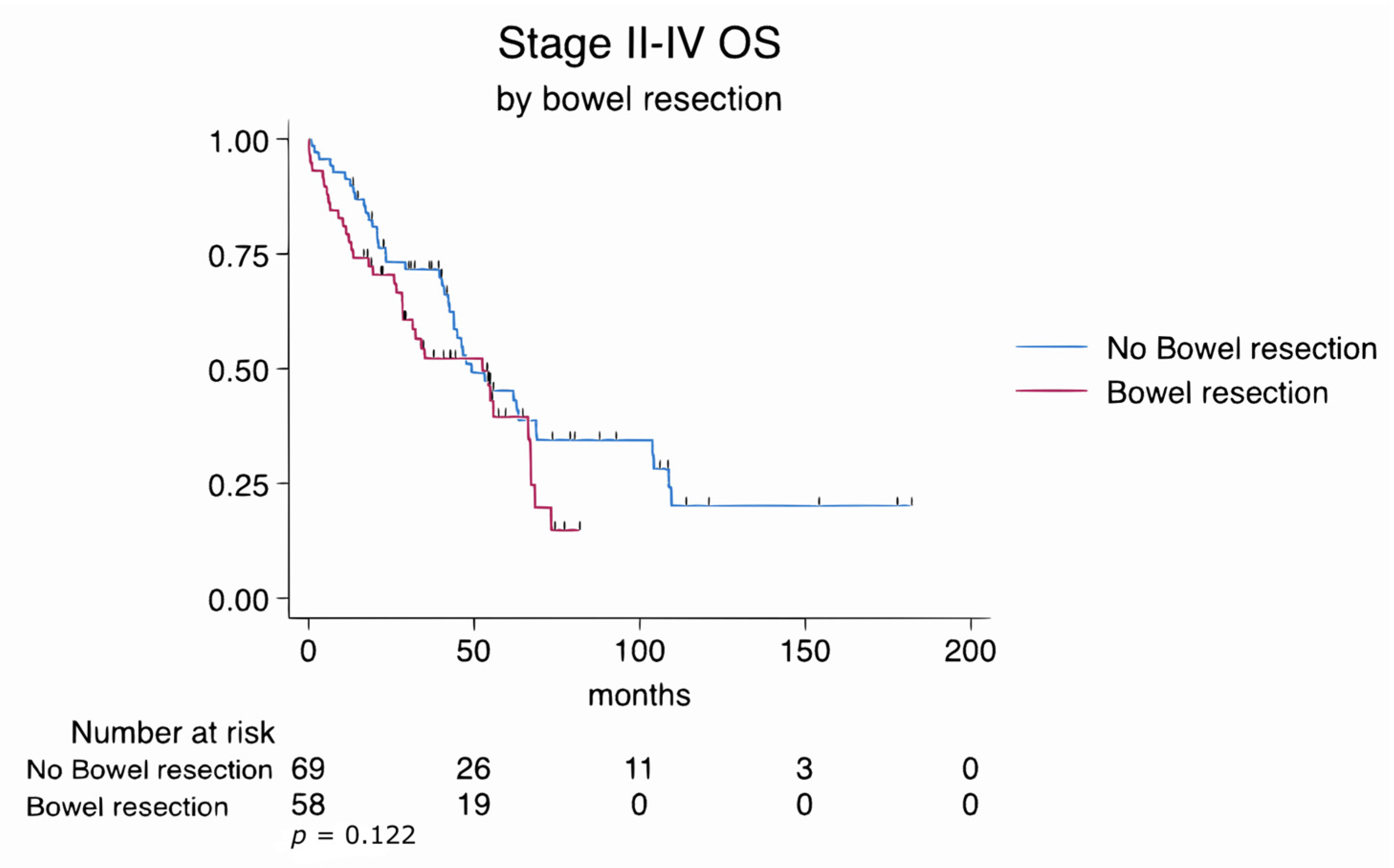
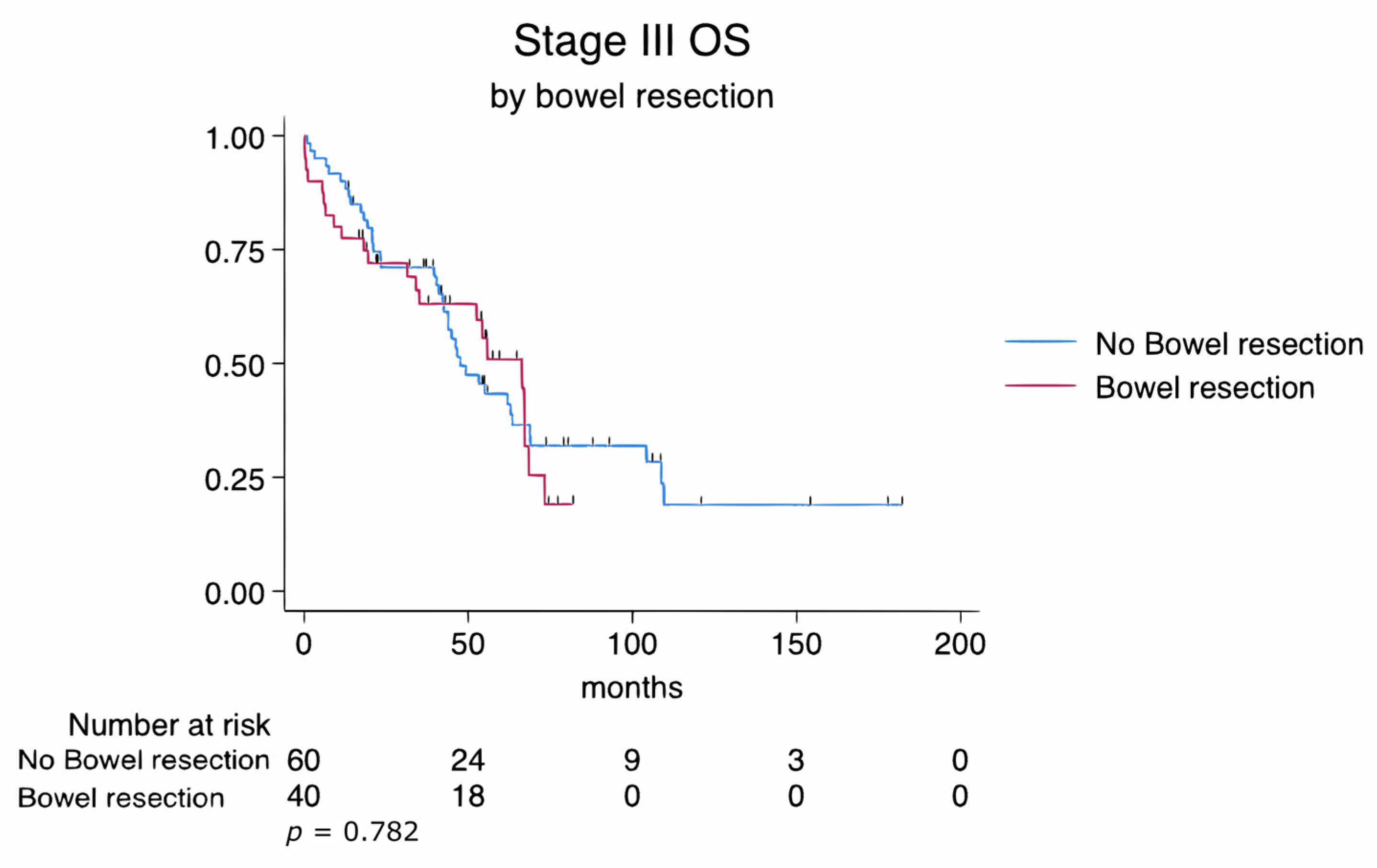
3.2.2. Overall Survival Analysis
3.3. Secondary Outcomes
3.4. Subgroup Analyses
3.4.1. Subgroup Analysis Stratified by Bowel Resection
Residual Disease Status and Bowel Resection (Optimal vs. Suboptimal Cytoreduction)
Primary vs. IDS with and Without Bowel Resection
4. Discussion
4.1. Summary of Study Results
4.2. Results in the Context of the Published Literature
4.3. Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CS | Cytoreductive surgery |
| IDS | Interval debulking surgery |
| OS | Overall survival |
| EOC | Epithelial ovarian cancer |
| FIGO | International Federation of Gynecology and Obstetrics |
| ECOG | Eastern Cooperative Oncology Group |
| NACT | Neoadjuvant chemotherapy |
| PDS | Primary debulking surgery |
| ICU | Intensive care unit |
| FFP | Fresh frozen plasma |
| R0 | No gross residual tumor |
| ASA | American Society of Anesthesiologists |
References
- Huang, J.; Chan, W.C.; Ngai, C.H.; Lok, V.; Zhang, L.; Lucero-Prisno, D.E., III; Xu, W.; Zheng, Z.-J.; Elcarte, E.; Withers, M. Worldwide burden, risk factors, and temporal trends of ovarian cancer: A global study. Cancers 2022, 14, 2230. [Google Scholar] [CrossRef] [PubMed]
- Torre, L.A.; Trabert, B.; DeSantis, C.E.; Miller, K.D.; Samimi, G.; Runowicz, C.D.; Gaudet, M.M.; Jemal, A.; Siegel, R.L. Ovarian cancer statistics, 2018. CA A Cancer J. Clin. 2018, 68, 284–296. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.-J.; Bristow, R.E.; Chi, D.S.; Cliby, W.A. Role of aggressive surgical cytoreduction in advanced ovarian cancer. J. Gynecol. Oncol. 2015, 26, 336. [Google Scholar] [CrossRef]
- Tozzi, R.; Casarin, J.; Baysal, A.; Pinelli, C.; Matak, L.; Ghanbarzadeh, N.; Alazzam, M.; Garruto-Campanile, R.; Majd, H.S.; Kilic, Y. Morbidity of multiple bowel resection compared to single bowel resection after debulking surgery for ovarian cancer. Eur. J. Obstet. Gynecol. Reprod. Biol. 2019, 240, 215–219. [Google Scholar] [CrossRef]
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology: Ovarian Cancer Including Fallopian Tube Cancer and Primary Peritoneal Cancer, Version 1.2017. Available online: https://www2.tri-kobe.org/nccn/guideline/gynecological/english/ovarian.pdf (accessed on 20 June 2025).
- Son, J.-H.; Chang, S.-J. Extrapelvic bowel resection and anastomosis in cytoreductive surgery for ovarian cancer. Gland Surg. 2021, 10, 1207. [Google Scholar] [CrossRef]
- Eisenkop, S.M.; Spirtos, N.M. Procedures required to accomplish complete cytoreduction of ovarian cancer: Is there a correlation with “biological aggressiveness” and survival? Gynecol. Oncol. 2001, 82, 435–441. [Google Scholar] [CrossRef]
- Le, T.; Krepart, G.; Lotocki, R.; Heywood, M. Does debulking surgery improve survival in biologically aggressive ovarian carcinoma? Gynecol. Oncol. 1997, 67, 208–214. [Google Scholar] [CrossRef] [PubMed]
- Derlatka, P.; Sienko, J.; Grabowska-Derlatka, L.; Palczewski, P.; Danska-Bidzinska, A.; Bidzinski, M.; Czajkowski, K. Results of optimal debulking surgery with bowel resection in patients with advanced ovarian cancer. World J. Surg. Oncol. 2016, 14, 58. [Google Scholar] [CrossRef]
- Estes, J.M.; Leath, C.A., III; Straughn, J.M., Jr.; Rocconi, R.P.; Kirby, T.O.; Huh, W.K.; Barnes, M.N., III. Bowel resection at the time of primary debulking for epithelial ovarian carcinoma: Outcomes in patients treated with platinum and taxane-based chemotherapy. J. Am. Coll. Surg. 2006, 203, 527–532. [Google Scholar] [CrossRef]
- Liu, J.; Berchuck, A.; Backes, F.J.; Cohen, J.; Grisham, R.; Leath, C.A.; Martin, L.; Matei, D.; Miller, D.S.; Robertson, S.; et al. NCCN Guidelines®® Insights: Ovarian Cancer/Fallopian Tube Cancer/Primary Peritoneal Cancer, Version 3.2024. J. Natl. Compr. Cancer Netw. 2024, 22, 512–519. [Google Scholar] [CrossRef]
- Vergote, I.; Tropé, C.G.; Amant, F.; Kristensen, G.B.; Ehlen, T.; Johnson, N.; Verheijen, R.H.; Van Der Burg, M.E.; Lacave, A.J.; Panici, P.B. Neoadjuvant chemotherapy or primary surgery in stage IIIC or IV ovarian cancer. N. Engl. J. Med. 2010, 363, 943–953. [Google Scholar] [CrossRef] [PubMed]
- Tozzi, R.; Noventa, M.; Saccardi, C.; Spagnol, G.; De Tommasi, O.; Coldebella, D.; Marchetti, M. Feasibility of laparoscopic Visceral-Peritoneal Debulking (L-VPD) in patients with stage III–IV ovarian cancer: The ULTRA-LAP trial pilot study. J. Gynecol. Oncol. 2023, 35, e14. [Google Scholar] [CrossRef] [PubMed]
- Hudson, C. A radical operation for fixed ovarian tumours. BJOG Int. J. Obstet. Gynaecol. 1968, 75, 1155–1160. [Google Scholar] [CrossRef]
- Clark, T.G.; Bradburn, M.J.; Love, S.B.; Altman, D.G. Survival analysis part I: Basic concepts and first analyses. Br. J. Cancer 2003, 89, 232–238. [Google Scholar] [CrossRef]
- Peduzzi, P.; Concato, J.; Kemper, E.; Holford, T.R.; Feinstein, A.R. A simulation study of the number of events per variable in logistic regression analysis. J. Clin. Epidemiol. 1996, 49, 1373–1379. [Google Scholar] [CrossRef]
- Bacalbasa, N.; Dima, S.; Balescu, I.; David, L.; Brasoveanu, V.; Popescu, I. Results of primary cytoreductive surgery in advanced-stage epithelial ovarian cancer: A single-center experience. Anticancer Res. 2015, 35, 4099–4104. [Google Scholar]
- Jaeger, W.; Ackermann, S.; Kessler, H.; Katalinic, A.; Lang, N. The effect of bowel resection on survival in advanced epithelial ovarian cancer. Gynecol. Oncol. 2001, 83, 286–291. [Google Scholar] [CrossRef] [PubMed]
- Harter, P.; Sehouli, J.; Lorusso, D.; Reuss, A.; Vergote, I.; Marth, C.; Kim, J.-W.; Raspagliesi, F.; Lampe, B.; Aletti, G. A randomized trial of lymphadenectomy in patients with advanced ovarian neoplasms. N. Engl. J. Med. 2019, 380, 822–832. [Google Scholar] [CrossRef]
- Armbrust, R.; Fotopoulou, C.; Zocholl, D.; Chekerov, R.; Muallem, M.Z.; Braicu, I.; Pietzner, K.; Harter, P.; Sehouli, J. Role of lymphadenectomy in advanced ovarian cancer—A subgroup analysis of the patients excluded from the LION trial (the Charité cohort). Int. J. Gynecol. Cancer 2025, 101683. [Google Scholar] [CrossRef]
- Kongkamsuan, W.; Boonyapipat, S. Epithelial ovarian cancer in younger age versus older age groups: Survival and clinicopathological features. J. Cancer Res. Ther. 2024, 20, 363–368. [Google Scholar] [CrossRef]
- Liontos, M.; Papatheodoridi, A.; Andrikopoulou, A.; Thomakos, N.; Haidopoulos, D.; Rodolakis, A.; Zagouri, F.; Bamias, A.; Dimopoulos, M.-A. Management of the Elderly patients with high-Grade Serous Ovarian Cancer in the REAL-WORLD setting. Curr. Oncol. 2021, 28, 1143–1152. [Google Scholar] [CrossRef] [PubMed]
- Chan, J.; Urban, R.; Cheung, M.; Osann, K.; Husain, A.; Teng, N.; Kapp, D.; Berek, J.; Leiserowitz, G. Ovarian cancer in younger vs older women: A population-based analysis. Br. J. Cancer 2006, 95, 1314–1320. [Google Scholar] [CrossRef] [PubMed]
- Trillsch, F.; Czogalla, B.; Mahner, S.; Loidl, V.; Reuss, A.; du Bois, A.; Sehouli, J.; Raspagliesi, F.; Meier, W.; Cibula, D. Risk factors for anastomotic leakage and its impact on survival outcomes in radical multivisceral surgery for advanced ovarian cancer: An AGO-OVAR. OP3/LION exploratory analysis. Int. J. Surg. 2025, 111, 2914–2922. [Google Scholar] [CrossRef]
- Tseng, J.H.; Suidan, R.S.; Zivanovic, O.; Gardner, G.J.; Sonoda, Y.; Levine, D.A.; Abu-Rustum, N.R.; Tew, W.P.; Chi, D.S.; Roche, K.L. Diverting ileostomy during primary debulking surgery for ovarian cancer: Associated factors and postoperative outcomes. Gynecol. Oncol. 2016, 142, 217–224. [Google Scholar] [CrossRef]
- Hogen, L.; Siriwardena, T.; Salman, L.; Bernardini, M.Q.; Ferguson, S.E.; Laframboise, S.; Bouchard-Fortier, G.; Atenafu, E.G.; May, T. Factors Influencing Surgeons’ Decision for Diverting Ileostomy and Associated Complications in Ovarian Cancer Cytoreductive Surgery. Int. J. Gynecol. Cancer 2025, 35, 101640. [Google Scholar] [CrossRef]
- McNamara, B.; Guerra, R.; Qin, J.; Craig, A.D.; Chen, L.-m.; Varma, M.G.; Chapman, J.S. Survival impact of bowel resection at the time of interval cytoreductive surgery for advanced ovarian cancer. Gynecol. Oncol. Rep. 2021, 38, 100870. [Google Scholar] [CrossRef] [PubMed]
- Aletti, G.D.; Santillan, A.; Eisenhauer, E.L.; Hu, J.; Aletti, G.; Podratz, K.C.; Bristow, R.E.; Chi, D.S.; Cliby, W.A. A new frontier for quality of care in gynecologic oncology surgery: Multi-institutional assessment of short-term outcomes for ovarian cancer using a risk-adjusted model. Gynecol. Oncol. 2007, 107, 99–106. [Google Scholar] [CrossRef]
- Cai, H.-B.; Zhou, Y.-F.; Chen, H.-Z.; Hou, H.-Y. The role of bowel surgery with cytoreduction for epithelial ovarian cancer. Clin. Oncol. 2007, 19, 757–762. [Google Scholar] [CrossRef]
- Kim, M.-S.; Lee, A.J.; Shim, S.-H.; Jang, E.B.; Kim, N.K.; Kim, M.K.; Suh, D.H.; Kim, J.; Son, J.-H.; Kong, T.-W. Comparison of Outcomes in Bowel Resections by Gynecologic Oncologists Versus General Surgeons During Maximal Cytoreductive Surgery for Advanced Ovarian Cancer: Gynecologic Oncology Research Investigators Collaboration Study (GORILLA-3006). Ann. Surg. Oncol. 2024, 31, 6040–6047. [Google Scholar] [CrossRef]
- Suidan, R.S.; Ramirez, P.T.; Sarasohn, D.M.; Teitcher, J.B.; Iyer, R.B.; Zhou, Q.; Iasonos, A.; Denesopolis, J.; Zivanovic, O.; Roche, K.C.L. A multicenter assessment of the ability of preoperative computed tomography scan and CA-125 to predict gross residual disease at primary debulking for advanced epithelial ovarian cancer. Gynecol. Oncol. 2017, 145, 27–31. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Bowel Resection (n = 58) | No Bowel Resection (n = 69) | p-Value |
|---|---|---|---|
| IDS/Primary CS | 10/48 (17.2%/82.8%) | 18/51 (26.1%/73.9%) | 0.231 |
| Optimal cytoreduction rate | 52/58 (89.1%) | 58/69 (83.3%) | 0.653 |
| Age (median, range) | 59 (35–88) | 60 (40–88) | 0.433 |
| BMI (median, range) | 27.9 (14.7–40.1) | 28 (16.2–44.8) | 0.924 |
| ECOG score | 0.005 | ||
| - 0 | 14/58 (24.1%) | 30/69 (43.5%) | 0.045 |
| - 1 | 26/58 (44.8%) | 33/69 (47.8%) | 0.930 |
| - 2 | 10/58 (17.2%) | 5/69 (7.2%) | 0.082 |
| - 3 | 8/58 (13.8%) | 1/69 (1.4%) | 0.014 |
| FIGO Stage | 0.020 | ||
| - II | 2/58 (3.4%) | 3/69 (4.3%) | 0.795 |
| - III | 40/58 (69.0%) | 60/69 (87.0%) | 0.014 |
| - IV | 16/58 (27.6%) | 6/69 (8.7%) | 0.005 |
| Histology | 0.602 | ||
| - High-grade serous | 55/58 (94.8%) | 59/69 (85.5%) | 0.084 |
| - Low-grade serous | 1/58 (1.7%) | 3/69 (4.3%) | 0.399 |
| - Clear cell | 1/58 (1.7%) | 2/69 (2.9%) | 0.664 |
| - Mucinous | 1/58 (1.7%) | 1/69 (1.4%) | 0.901 |
| - Transitional | 0/58 (0%) | 1/69 (1.4%) | 0.357 |
| - Mixed | 0/58 (0%) | 2/69 (2.9%) | 0.191 |
| - Other | 0/58 (0%) | 1/69 (1.4%) | 0.357 |
| Preoperative CA-125 (median, range) | 726.8 (9.2–11476) | 673.8 (4–7337) | 0.622 |
| Presence of ascites | 36/58 (62.1%) | 25/69 (36.2%) | 0.004 |
| Stoma rate | 20/58 (34.5%) | N.A. | — |
| Anastomosis rate | 46/58 (79.3%) | N.A. | — |
| Protective stoma rate | 13/46 (28.9%) | N.A. | — |
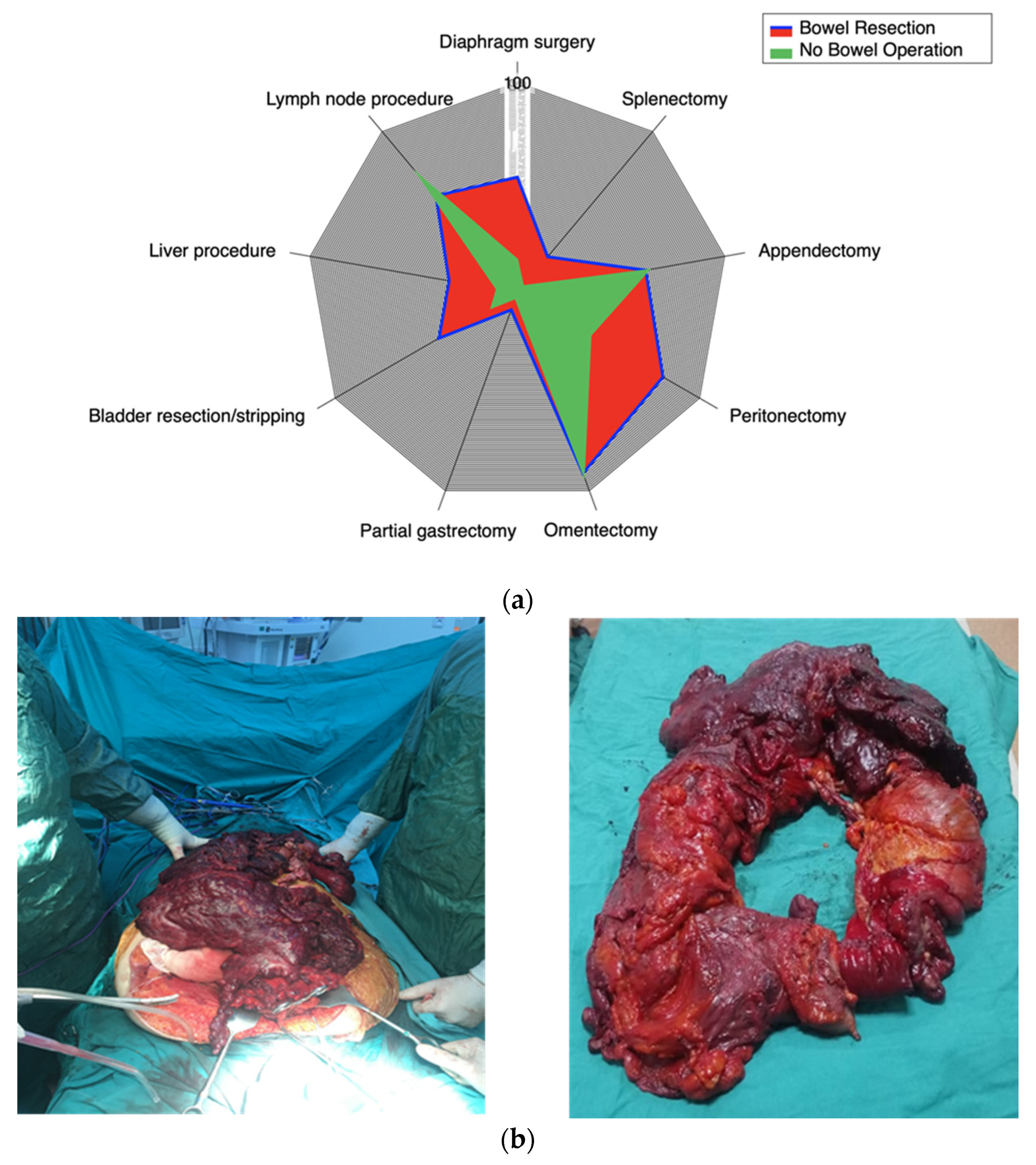
| Procedures During CS | Bowel Resection (n = 58) | No Bowel Resection (n = 69) | p-Value |
|---|---|---|---|
| Lymph node procedure | 35 (60.3%) | 51 (73.9%) | 0.103 |
| Diaphragm Stripping | 32 (55.2%) | 11 (15.9%) | <0.001 |
| Splenectomy | 13 (22.4%) | 3 (4.3%) | 0.002 |
| Appendectomy | 36 (62.1%) | 44 (63.8%) | 0.843 |
| Peritonectomy | 46 (79.3%) | 29 (42%) | <0.001 |
| Omentectomy | 53 (91.4%) | 64 (92.8%) | 0.775 |
| Partial Gastrectomy | 5 (8.6%) | 2 (2.9%) | 0.159 |
| Bladder Resection/Stripping | 25 (43.1%) | 10 (14.5%) | <0.001 |
| Liver Procedure | 19 (32.8%) | 7 (10.1%) | 0.002 |
| Short-Term Outcomes | Bowel Resection (n = 58) | No Bowel Resection (n = 69) | p-Value |
|---|---|---|---|
| Mortality in 90 days | 4 (6.9%) | 2 (2.9%) | 0.411 |
| Rate of FFP transfusion | 46 (78.6%) | 20 (28.8%) | <0.001 |
| Number of used intraoperative FFP (median, range) | 2 (1–5) | 1 (1–3) | 0.008 |
| Rate of red blood cell transfusion | 46 (80%) | 28 (40.9%) | <0.001 |
| Number of used red blood cell packages | 2 (1–4) | 1 (1–5) | 0.003 |
| Rate of ICU admission | 44 (75.9%) | 20 (29%) | <0.001 |
| ICU duration (day) (median, range) | 1 (1–18) | 1 (1–24) | 0.058 |
| Operation duration (minutes) | 424 ± 38.5 | 329.5 ± 34.6 | <0.001 |
| Long-term Outcomes | Bowel Resection (n = 58) | No Bowel Resection (n = 69) | p-value |
| Overall mortality during follow-up | 35 (60.3%) | 42 (60.9%) | 0.952 |
| Development of platinum resistance | 7 (12.1%) | 8 (11.6%) | 0.934 |
| Secondary CS during follow-up | 11 (19%) | 26 (37.7%) | 0.021 |
| Re-admission rate in 3 months | 23 (39.7%) | 9 (13%) | 0.001 |
| Number of hospital Re-admissions per patient in 3 months (median, range) | 0 (0–4) | 0 (0–6) | 0.001 |
| Re-admission rate in 3-6 months | 10 (17.2%) | 8 (11.6%) | 0.363 |
| Number of hospital Re-admissions per patient in 3–6 months | 0 (0–3) | 0 (0–7) | 0.462 |
| Variable | Hazard Ratio | 95% CI | p-Value |
|---|---|---|---|
| Age | 1.05 | 1.025–1.076 | <0.004 |
| Bowel Resection | 1.438 | 0.904–2.286 | 0.124 |
| Secondary cytoreduction | 0.602 | 0.365–0.992 | 0.047 |
| Histology mucinous | 23.01 | 2–265 | 0.012 |
| Stage III | 1.382 | 0.335–5.701 | 0.654 |
| Stage IV | 2.465 | 0.551–11.027 | 0.258 |
| Primary CS | 0.565 | 0.330–0.967 | 0.037 |
| Stoma | 1.739 | 0.932–3.243 | 0.080 |
| Lymph node dissection | 0.337 | 0.212–0.537 | <0.001 |
| Platinum Resistance | 2.06 | 1.12–3.79 | 0.020 |
| Diaphragm Stripping | 1.43 | 0.887–2.347 | 0.150 |
| Peritonectomy | 0.795 | 0.508–1.245 | 0.317 |
| Splenectomy | 1.082 | 0.538–2.176 | 0.824 |
| Bladder Stripping | 0.877 | 0.486–1.586 | 0.664 |
| Liver Excision | 1.064 | 0.881–1.948 | 0.840 |
| Residual Disease | 1.855 | 1.065–3.224 | 0.029 |
| Variable | Hazard Ratio | 95% CI | p-Value |
|---|---|---|---|
| Age | 1.042 | 1.01–1.07 | 0.005 |
| Lymph node dissection | 0.45 | 0.26–0.77 | 0.003 |
| Primary CS (vs IDS) | 0.54 | 0.30–0.99 | 0.047 |
| Mucinous histology | 8.65 | 0.68–110.43 | 0.097 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ceylan, Ö.O.; Turan, İ.; Erdemoglu, E.; González, M.S.; Magrina, J. Impact of Bowel Resection on Operative Mortality and Overall Survival in Advanced Epithelial Ovarian Cancer. Cancers 2025, 17, 2086. https://doi.org/10.3390/cancers17132086
Ceylan ÖO, Turan İ, Erdemoglu E, González MS, Magrina J. Impact of Bowel Resection on Operative Mortality and Overall Survival in Advanced Epithelial Ovarian Cancer. Cancers. 2025; 17(13):2086. https://doi.org/10.3390/cancers17132086
Chicago/Turabian StyleCeylan, Özgür Ozan, İlyas Turan, Evrim Erdemoglu, Marina Santos González, and Javier Magrina. 2025. "Impact of Bowel Resection on Operative Mortality and Overall Survival in Advanced Epithelial Ovarian Cancer" Cancers 17, no. 13: 2086. https://doi.org/10.3390/cancers17132086
APA StyleCeylan, Ö. O., Turan, İ., Erdemoglu, E., González, M. S., & Magrina, J. (2025). Impact of Bowel Resection on Operative Mortality and Overall Survival in Advanced Epithelial Ovarian Cancer. Cancers, 17(13), 2086. https://doi.org/10.3390/cancers17132086