

Cryoablation and Intratumoral Immunotherapy for Breast Cancer: A Future Path to Cost-Effective De-Escalation for Larger Tumors, Lymph Nodes and Metastatic Disease

 , , , and
, , , and
Simple Summary
Abstract
1. Introduction
1.1. A Spectrum of De-Escalation and Acceptance of Surgical Lumpectomy
1.2. Breast Cancer Tumor Size and Metastatic Potential
2. Current Adjunctive Therapies to Reduce Recurrence and Metastatic Disease
3. Cryoablation
3.1. The Use of Cytotoxic Isotherms and the Potential for Treating Larger Breast Tumors
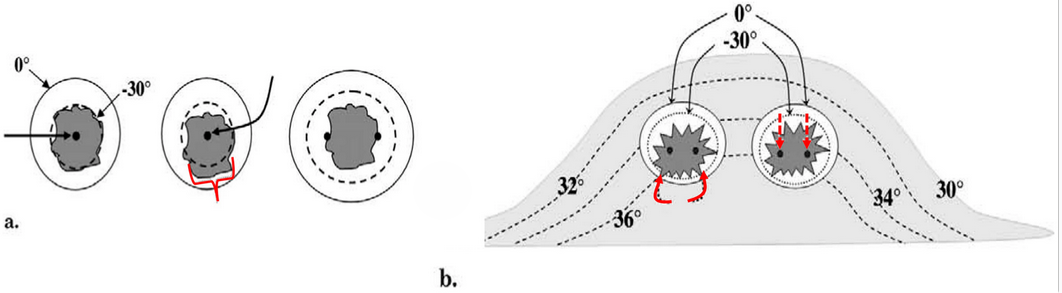
3.2. Cryoablation Techniques: Imaging Guidance and the “Knuckle Rule”
3.3. The Potential of Large-Volume Breast Cryoablation
4. Immunotherapy
4.1. Systemic Alone (Currently Intravenous)
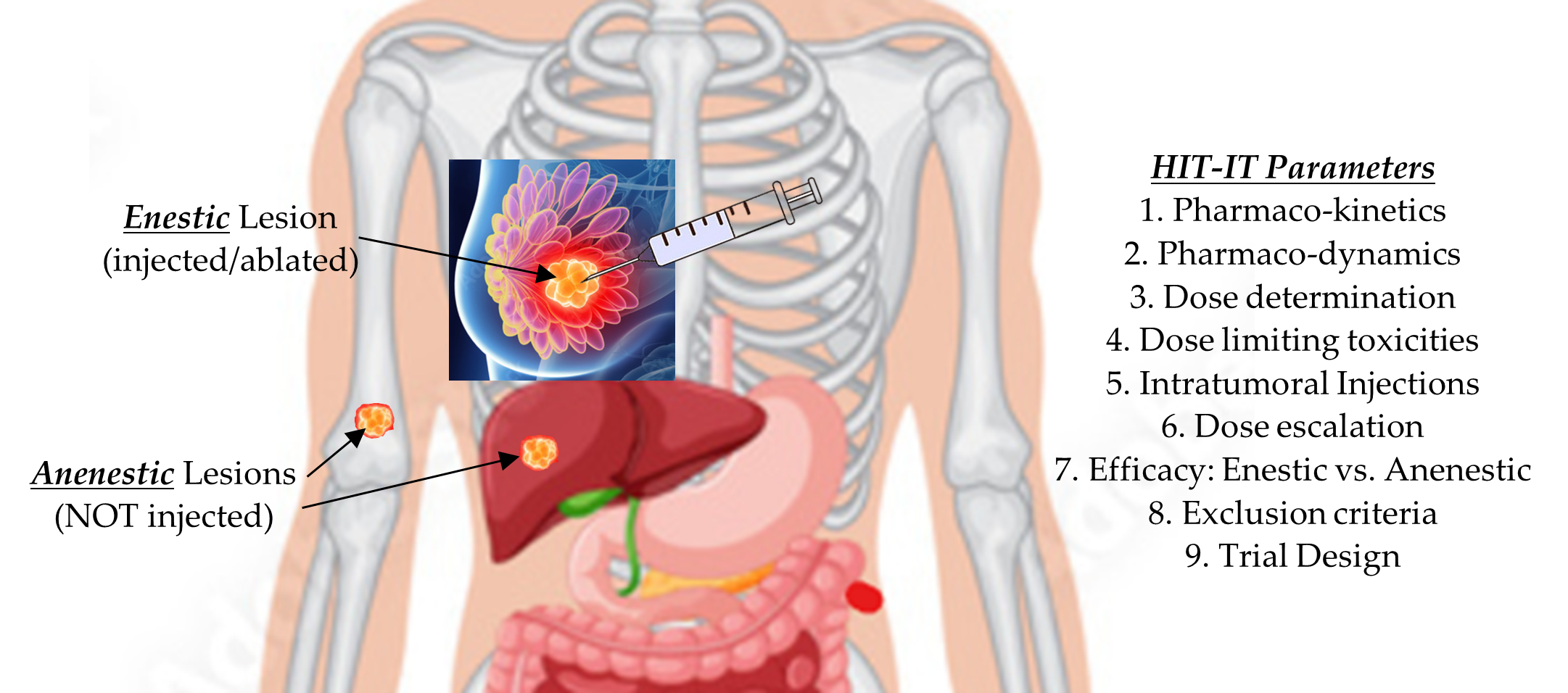
4.2. Human IntraTumoral ImmunoTherapy (HIT-IT; Drugs Alone)
4.3. The Potential of Activating Immune Responses
Combining Cryoablation + Immune Stimulating Adjuvants
5. Combined Cryoablation and HIT-IT-Type Ablation Immunotherapy (Current and Future)
6. Cost-Effectiveness and Patient-Reported Quality-of-Life Outcomes
7. Discussion/Future Directions
8. Conclusions
- Key Points:
- •
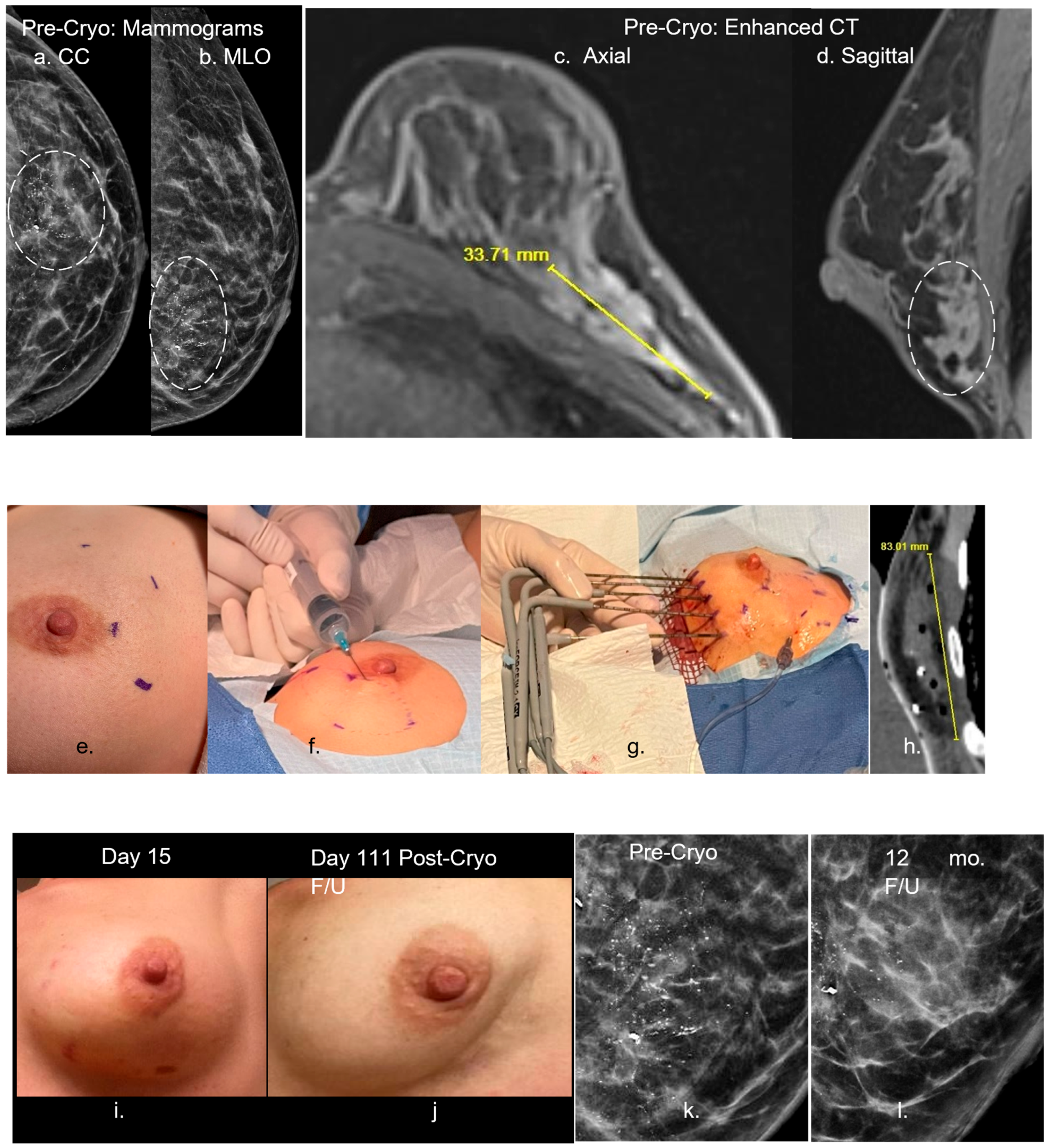
- Combined CT/US, image-guided cryoablation displays visible ice extending beyond tumor margins for improved local tumor control in patients with breast cancers > 1.5 cm.
- •
- Appropriate cytotoxic isotherms need to volumetrically extend beyond all apparent tumor margins, which favors multi-probe cryoablation for tumors > 1.5 cm, whereas even larger single cryoprobes appear to be limited to breast cancers < 1.5 cm.
- •
- Intratumoral injection of chemo- and immunotherapeutic drugs is a promising strategy for improving the effectiveness and reducing the morbidity of chemotherapy and immunotherapy.
- •
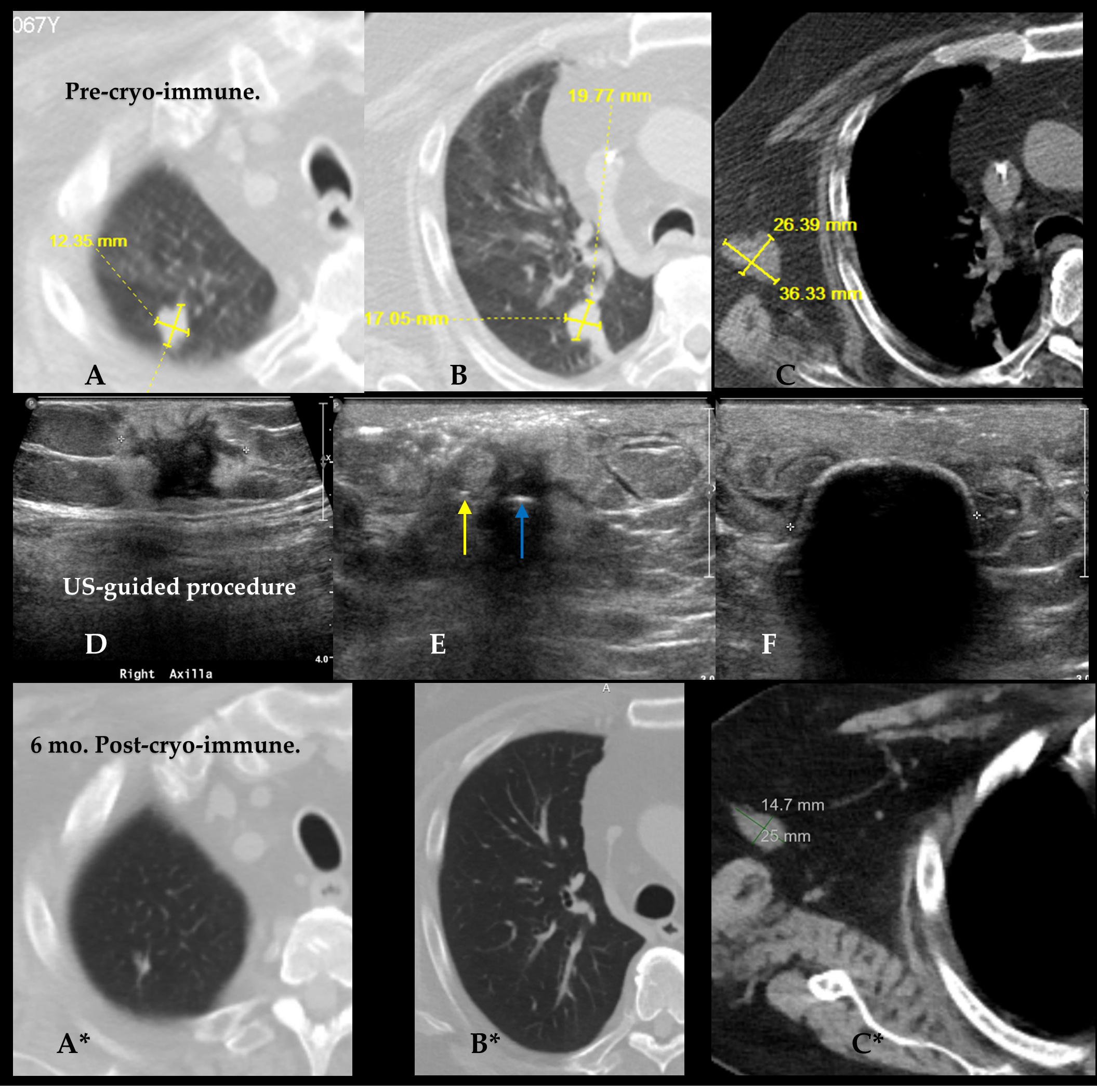
- Image-guided cryoablation combined with intratumoral immunochemotherapy provides a dual-modality approach that promotes systemic immune responses and may markedly decrease costs of future breast cancer therapies.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Surveillance, Epidemiology, and End Results (SEER) Program. Cancer Statistics for Breast Cancer. National Cancer Institute. Available online: https://seer.cancer.gov/statfacts/html/breast.html (accessed on 18 October 2024).
- Holmes, D.R. Breast cancer care during a pandemic: An opportune time for cryoablation? Breast Cancer Res. Treat. 2020, 182, 515–521. [Google Scholar] [CrossRef] [PubMed]
- Sacchini, V.; Norton, L. Escalating de-escalation in breast cancer treatment. Breast Cancer Res. Treat. 2022, 195, 85–90. [Google Scholar] [CrossRef]
- Khan, S.Y.; Cole, J.; Habrawi, Z.; Melkus, M.W.; Layeequr Rahman, R. Cryoablation Allows the Ultimate De-escalation of Surgical Therapy for Select Breast Cancer Patients. Ann. Surg. Oncol. 2023, 30, 8398–8403. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Huang, M.L.; Tomkovich, K.; Lane, D.L.; Katta, R.; Candelaria, R.P.; Santiago, L. Breast Cancer Cryoablation Fundamentals Past and Present: Technique Optimization and Imaging Pearls. Acad. Radiol. 2023, 30, 2383–2395. [Google Scholar] [CrossRef] [PubMed]
- Melkus, M.W.; Khan, S.Y.; Cole, J.; Layeequr Rahman, R. ASO Author Reflections: Achieving Surgical De-Escalation of Breast Cancer Through Cryoablation. Ann. Surg. Oncol. 2024, 31, 384–385. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Thai, J.N.; Sevrukov, A.B.; Ward, R.C.; Monticciolo, D.L. Cryoablation Therapy for Early-Stage Breast Cancer: Evidence and Rationale. J. Breast Imaging 2023, 305, 646–657. [Google Scholar] [CrossRef] [PubMed]
- Banys-Paluchowski, M.; Rubio, I.T.; Ditsch, N.; Krug, D.; Gentilini, O.D.; Kühn, T. Real de-escalation or escalation in disguise? Breast 2023, 69, 249–257. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Pederson, H.J.; Pratt, D.; Calhoun, B.C. Surgical de-escalation: Are we ready for ‘observation’ of benign high-risk breast lesions found on core needle biopsy? Clevel. Clin. J. Med. 2023, 90, 433–438. [Google Scholar] [CrossRef] [PubMed]
- Holmes, D.; Iyengar, G. Breast Cancer Cryoablation in the Multidisciplinary Setting: Practical Guidelines for Patients and Physicians. Life 2023, 13, 1756. [Google Scholar] [CrossRef]
- Cheng, O.; Postlewait, L.M. De-Escalation of Multidisciplinary Breast Cancer Care with Cryoablation Therapy: Navigating Novel Therapeutics, Ethics, and Outcomes. Ann. Surg. Oncol. 2024, 31, 1433–1435. [Google Scholar] [CrossRef] [PubMed]
- Hajar, R. The physician’s oath: Historical perspectives. Heart Views 2017, 18, 154–159. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Wood, G.E.; Chamberlain, F.; Tran, B.; Conduit, C.; Liow, E.; Nicol, D.L.; Shamash, J.; Alifrangis, C.; Rajan, P. Treatment de-escalation for stage II seminoma. Nat. Rev. Urol. 2023, 20, 502–512. [Google Scholar] [CrossRef] [PubMed]
- Piombino, C.; Tonni, E.; Oltrecolli, M.; Pirola, M.; Pipitone, S.; Piombino, C.; Dominici, M.; Sabbatini, R.; Vitale, M.G. Immunotherapy in urothelial cancer: Current status and future directions. Expert. Rev. Anticancer Ther. 2023, 23, 1141–1155. [Google Scholar] [CrossRef] [PubMed]
- Bland, C.S. The Halsted mastectomy: Present illness and past history. West. J. Med. 1981, 134, 549. [Google Scholar]
- Fisher, B.; Anderson, S.; Bryant, J.; Margolese, R.G.; Deutsch, M.; Fisher, E.R.; Jeong, J.H.; Wolmark, N. Twenty-year follow-up of a randomized trial comparing total mastectomy, lumpectomy, and lumpectomy plus irradiation for the treatment of invasive breast cancer. N. Engl. J. Med. 2002, 347, 1233–1241. [Google Scholar] [CrossRef]
- Veronesi, U.; Cascinelli, N.; Mariani, L.; Greco, M.; Saccozzi, R.; Luini, A.; Aguilar, M.; Marubini, E. Twenty-year follow-up of a randomized study comparing breast-conserving surgery with radical mastectomy for early breast cancer. N. Engl. J. Med. 2002, 347, 1227–1232. [Google Scholar] [CrossRef]
- Tadros, A.B.; Moo, T.A.; Stempel, M.; Zabor, E.C.; Khan, A.J.; Morrow, M. Axillary management for young women with breast cancer varies between patients electing breast-conservation therapy or mastectomy. Breast Cancer Res. Treat. 2020, 180, 197–205. [Google Scholar] [CrossRef]
- Cortina, C.S.; Bergom, C.; Craft, M.A.; Fields, B.; Brazauskas, R.; Currey, A.; Kong, A.L. A national survey of breast surgeons and radiation oncologists on contemporary axillary management in mastectomy patients. Ann. Surg. Oncol. 2021, 28, 5568–5579. [Google Scholar] [CrossRef] [PubMed]
- Kantor, O.; Means, J.; Grossmith, S.; Dey, T.; Bellon, J.R.; Mittendorf, E.A.; King, T.A. Optimizing axillary management in clinical T1–2N0 mastectomy patients with positive sentinel lymph nodes. Ann. Surg. Oncol. 2022, 29, 972–980. [Google Scholar] [CrossRef]
- Keshavarz, S.; Wall, J.R.; Keshavarz, S.; Vojoudi, E.; Jafari-Shakib, R. Breast cancer immunotherapy: A comprehensive review. Clin. Exp. Med. 2023, 23, 4431–4447. [Google Scholar] [CrossRef] [PubMed]
- Sopik, V.; Narod, S.A. The relationship between tumour size, nodal status and distant metastases: On the origins of breast cancer. Breast Cancer Res. Treat. 2018, 170, 647–656. [Google Scholar] [CrossRef] [PubMed]
- Covington, K.R.; Brusco, L.; Barone, I.; Tsimelzon, A.; Selever, J.; Corona-Rodriguez, A.; Brown, P.; Kumar, R.; Hilsenbeck, S.G.; Fuqua, S.A. Metastasis tumor-associated protein 2 enhances metastatic behavior and is associated with poor outcomes in estrogen receptor-negative breast cancer. Breast Cancer Res. Treat. 2013, 141, 375–384. [Google Scholar] [CrossRef] [PubMed]
- Burstein, H.J.; Griggs, J.J. Adjuvant hormonal therapy for early-stage breast cancer. Surg. Oncol. Clin. N. Am. 2010, 19, 639–647. [Google Scholar] [CrossRef] [PubMed]
- Cahir, C.; Dombrowski, S.U.; Kelly, C.M.; Kennedy, M.J.; Bennett, K.; Sharp, L. Women’s experiences of hormonal therapy for breast cancer: Exploring influences on medication-taking behaviour. Support. Care Cancer Off. J. Multinatl. Assoc. Support. Care Cancer 2015, 23, 3115–3130. [Google Scholar] [CrossRef]
- Stankowski-Drengler, T.J.; Livingston-Rosanoff, D.; Schumacher, J.R.; Hanlon, B.M.; Hitchcock, M.E.; Neuman, H.B. Breast Cancer Outcomes of Neoadjuvant Versus Adjuvant Chemotherapy by Receptor Subtype: A Scoping Review. J. Surg. Res. 2020, 254, 83–90. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kumar, T.; Dutta, R.R.; Thakre, S.; Singh, A.; Velagala, V.R.; Shinde, R.K. Resistance to Resilience: Understanding Post-surgical Hormone Therapy in Breast Cancer Care. Cureus 2023, 15, e47869. [Google Scholar] [CrossRef]
- Derouane, F.; van Marcke, C.; Berlière, M.; Gerday, A.; Fellah, L.; Leconte, I.; Van Bockstal, M.R.; Galant, C.; Corbet, C.; Duhoux, F.P. Predictive Biomarkers of Response to Neoadjuvant Chemotherapy in Breast Cancer: Current and Future Perspectives for Precision Medicine. Cancers 2022, 14, 3876. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Korde, L.A.; Somerfield, M.R.; Carey, L.A.; Crews, J.R.; Denduluri, N.; Hwang, E.S.; Khan, S.A.; Loibl, S.; Morris, E.A.; Perez, A.; et al. Neoadjuvant Chemotherapy, Endocrine Therapy, and Targeted Therapy for Breast Cancer: ASCO Guideline. J. Clin. Oncol. 2021, 39, 1485–1505. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Larsen, C.M.; Arango, M.G.; Dasari, H.; Calle, M.A.; Adjei, E.; Mesa, J.R.; Scott, C.G.; Thompson, C.A.; Cerhan, J.R.; Haddad, T.C.; et al. Association of anthracycline with heart failure in patients treated for breast cancer or lymphoma, 1985–2010. JAMA Netw. Open 2023, 6, e2254669. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ringborg, U.; Bergqvist, D.; Brorsson, B.; Cavallin-Ståhl, E.; Ceberg, J.; Einhorn, N.; Frödin, J.E.; Järhult, J.; Lamnevik, G.; Lindholm, C.; et al. The Swedish Council on Technology Assessment in Health Care (SBU) systematic overview of radiotherapy for cancer including a prospective survey of radiotherapy practice in Sweden 2001--Summary and Conclusions. Acta Oncol. 2003, 42, 357–365. [Google Scholar] [CrossRef]
- Moding, E.J.; Kastan, M.B.; Kirsch, D.G. Strategies for optimizing the response of cancer and normal tissues to radiation. Nat. Rev. Drug Discov. 2013, 12, 526–542. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Hufnagle, J.J.; Andersen, S.N.; Maani, E.V. Radiation-Induced Cardiac Toxicity. In StatPearls [Internet]; Updated 29 May 2023; StatPearls Publishing: Treasure Island, FL, USA, 2025. Available online: https://www.ncbi.nlm.nih.gov/books/NBK554453/ (accessed on 15 October 2024).
- Darby, S.C.; Ewertz, M.; McGale, P.; Bennet, A.M.; Blom-Goldman, U.; Brønnum, D.; Correa, C.; Cutter, D.; Gagliardi, G.; Gigante, B.; et al. Risk of ischemic heart disease in women after radiotherapy for breast cancer. N. Engl. J. Med. 2013, 368, 987–998. [Google Scholar] [CrossRef] [PubMed]
- van den Bogaard, V.A.; Ta, B.D.; van der Schaaf, A.; Bouma, A.B.; Middag, A.M.; Bantema-Joppe, E.J.; van Dijk, L.V.; van Dijk-Peters, F.B.; Marteijn, L.A.; de Bock, G.H.; et al. Validation and Modification of a Prediction Model for Acute Cardiac Events in Patients With Breast Cancer Treated With Radiotherapy Based on Three-Dimensional Dose Distributions to Cardiac Substructures. J. Clin. Oncol. 2017, 35, 1171–1178. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Taylor, C.; Correa, C.; Duane, F.K.; Aznar, M.C.; Anderson, S.J.; Bergh, J.; Dodwell, D.; Ewertz, M.; Gray, R.; Jagsi, R.; et al. Early Breast Cancer Trialists’ Collaborative Group. Estimating the Risks of Breast Cancer Radiotherapy: Evidence From Modern Radiation Doses to the Lungs and Heart and From Previous Randomized Trials. J. Clin. Oncol. 2017, 35, 1641–1649. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Bergom, C.; Bradley, J.A.; Ng, A.K.; Samson, P.; Robinson, C.; Lopez-Mattei, J.; Mitchell, J.D. Past, Present, and Future of Radiation-Induced Cardiotoxicity: Refinements in Targeting, Surveillance, and Risk Stratification. JACC CardioOncol. 2021, 3, 343–359. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Erinjeri, J.P.; Clark, T.W. Cryoablation: Mechanism of action and devices. J. Vasc. Interv. Radiol. 2010, 21 (Suppl. 8), S187–S191. [Google Scholar] [CrossRef]
- Ali Mohammad, S.; Hak, A.; Pogu, S.V.; Rengan, A.K. Radiotherapy, photodynamic therapy, and cryoablation-induced abscopal effect: Challenges and future prospects. Cancer Innov. 2023, 2, 323–345. [Google Scholar] [CrossRef]
- Pfleiderer, S.O.; Freesmeyer, M.G.; Marx, C.; Kühne-Heid, R.; Schneider, A.; Kaiser, W.A. Cryotherapy of breast cancer under ultrasound guidance: Initial results and limitations. Eur. Radiol. 2002, 12, 3009–3014. [Google Scholar] [CrossRef]
- Sabel, M.S.; Kaufman, C.S.; Whitworth, P.; Chang, H.; Stocks, L.H.; Simmons, R.; Schultz, M. Cryoablation of early-stage breast cancer: Work-in-progress report of a multi-institutional trial. Ann. Surg. Oncol. 2004, 11, 542–549. [Google Scholar] [CrossRef] [PubMed]
- Littrup, P.J.; Freeman-Gibb, L.; Andea, A.; White, M.; Amerikia, K.C.; Bouwman, D.; Harb, T.; Sakr, W. Cryotherapy for breast fibroadenomas. Radiology 2005, 234, 63–72. [Google Scholar] [CrossRef]
- Littrup, P.J.; Jallad, B.; Chandiwala-Mody, P.; D’Agostini, M.; Adam, B.A.; Bouwman, D. Cryotherapy for breast cancer: A feasibility study without excision. J. Vasc. Interv. Radiol. 2009, 20, 1329–1341. [Google Scholar] [CrossRef] [PubMed]
- Pusceddu, C.; Paliogiannis, P.; Nigri, G.; Fancellu, A. Cryoablation In The Management Of Breast Cancer: Evidence To Date. Breast cancer. Dove Med. 2019, 11, 283–292. [Google Scholar] [CrossRef]
- Kwong, A.; Co, M.; Fukuma, E. Prospective Clinical Trial on Expanding Indications for Cryosurgery for Early Breast Cancers. Clin. Breast Cancer 2023, 23, 363–368. [Google Scholar] [CrossRef]
- Khan, S.Y.; Snitman, A.; Habrawi, Z.; Crawford, S.; Melkus, M.W.; Layeequr Rahman, R. The Role of Cryoablation in Breast Cancer Beyond the Oncologic Control: COST and Breast-Q Patient-Reported Outcomes. Ann. Surg. Oncol. 2023, 30, 1029–1037. [Google Scholar] [CrossRef]
- Littrup, P.J.; Jallad, B.; Vorugu, V.; Littrup, G.; Currier, B.; George, M.; Herring, D. Lethal isotherms of cryoablation in a phantom study: Effects of heat load, probe size, and number. J. Vasc. Interv. Radiol. 2009, 20, 1343–1351. [Google Scholar] [CrossRef]
- Littrup, P.J.; Bang, H.J.; Currier, B.; Goodrich, D.; Aoun, H.D.; Heilbrun, L.; Adam, B. Soft tissue cryoablation in diffuse locations: Feasibility and intermediate outcomes. J. Vasc. Interv. Radiol. 2013, 24, 1817–1825. [Google Scholar] [CrossRef] [PubMed]
- Page 73. Available online: https://icecure-medical.com/wp-content/uploads/2021/01/DMS_7064_ProSense-User-Manual-European-Indications_C_3.pdf (accessed on 20 October 2024).
- Cryoablation Treatment Planning. Available online: https://www.bostonscientific.com/content/dam/bostonscientific/pi/portfolio-group/pdf-documents/PI-814202-AB%20Cryoablation%20Treatment%20Planning%20-%20FINAL%20CORRECTED.pdf (accessed on 10 May 2024).
- Wang, H.; Littrup, P.J.; Duan, Y.; Zhang, Y.; Feng, H.; Nie, Z. Thoracic masses treated with percutaneous cryotherapy: Initial experience with more than 200 procedures. Radiology 2005, 235, 289–298. [Google Scholar] [CrossRef]
- Littrup, P.J.; Ahmed, A.; Aoun, H.; Noujaim, D.; Harb, T.; Nakat, S.; Abdallah, K.; Adam, B.; Sakr, W.; Edson, P.; et al. CT-guided percutaneous cryotherapy of renal masses. J. Vasc. Interv. Radiol. 2007, 18, 383–392. [Google Scholar] [CrossRef] [PubMed]
- Littrup, P.J.; Aoun, H.D.; Adam, B.; Krycia, M.; Prus, M.; Shields, A. Percutaneous cryoablation of hepatic tumors: Long-term experience of a large U.S. series. Abdom. Radiol. 2016, 41, 767–780. [Google Scholar] [CrossRef] [PubMed]
- Pigg, N.; Gordillo, C.; Wang, Y.; Ward, R.C. Breast cancer cryoablation with radiologic-pathologic correlation. Br. J. Radiol. 2022, 95, 20220480. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Roca Navarro, M.J.; Oliver Goldaracena, J.M.; Garrido Alonso, D.; Navarro Monforte, Y.; Díaz de Bustamante Durbán, T.; Córdoba Chicote, M.V.; García Martínez, F.; Martí Álvarez, C.; Yébenes Gregorio, L.; Montes Botella, J.L.; et al. Pre-surgical cryoablation in ≤2 cm ER + /HER2-tumors. Prognostic factors for the presence of residual invasive carcinoma. Breast Cancer Res. Treat. 2024, 206, 561–573. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Fine, R.E.; Gilmore, R.C.; Dietz, J.R.; Boolbol, S.K.; Berry, M.P.; Han, L.K.; Kenler, A.S.; Sabel, M.; Tomkovich, K.R.; VanderWalde, N.A.; et al. Cryoablation Without Excision for Low-Risk Early-Stage Breast Cancer: 3-Year Interim Analysis of Ipsilateral Breast Tumor Recurrence in the ICE3 Trial. Ann. Surg. Oncol. 2021, 28, 5525–5534. [Google Scholar] [CrossRef]
- Fine, R.E.; Gilmore, R.C.; Tomkovich, K.R.; Dietz, J.R.; Berry, M.P.; Hernandez, L.E.; Columbus, K.S.; Seedman, S.A.; Fisher, C.S.; Han, L.K.; et al. Cryoablation Without Excision for Early-Stage Breast Cancer: ICE3 Trial 5-Year Follow-Up on Ipsilateral Breast Tumor Recurrence. Ann. Surg. Oncol. 2024, 31, 7273–7283. [Google Scholar] [CrossRef] [PubMed]
- Seidel, J.A.; Otsuka, A.; Kabashima, K. Anti-PD-1 and Anti-CTLA-4 Therapies in Cancer: Mechanisms of Action, Efficacy, and Limitations. Front. Oncol. 2018, 8, 86. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- de la Cruz-Merino, L.; Palazón-Carrión, N.; Henao-Carrasco, F.; Nogales-Fernández, E.; Álamo-de la Gala, M.; Vallejo-Benítez, A.; Chiesa, M.; Sánchez-Margalet, V. GEICAM (Spanish Breast Cancer Research Group) and GÉTICA (Spanish Group for Cancer Immuno-Biotherapy). New horizons in breast cancer: The promise of immunotherapy. Clin. Transl. Oncol. 2019, 21, 117–125. [Google Scholar] [CrossRef] [PubMed]
- Wojtukiewicz, M.Z.; Rek, M.M.; Karpowicz, K.; Górska, M.; Polityńska, B.; Wojtukiewicz, A.M.; Moniuszko, M.; Radziwon, P.; Tucker, S.C.; Honn, K.V. Inhibitors of immune checkpoints-PD-1, PD-L1, CTLA-4-new opportunities for cancer patients and a new challenge for internists and general practitioners. Cancer Metastasis Rev. 2021, 40, 949–982. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Marabelle, A.; Andtbacka, R.; Harrington, K.; Melero, I.; Leidner, R.; de Baere, T.; Robert, C.; Ascierto, P.A.; Baurain, J.F.; Imperiale, M.; et al. Starting the fight in the tumor: Expert recommendations for the development of human intratumoral immunotherapy (HIT-IT). Ann. Oncol. 2018, 29, 2163–2174. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Luke, J.J.; Davar, D.; Andtbacka, R.H.; Bhardwaj, N.; Brody, J.D.; Chesney, J.; Coffin, R.; de Baere, T.; de Gruijl, T.D.; Fury, M.; et al. Society for Immunotherapy of Cancer (SITC) recommendations on intratumoral immunotherapy clinical trials (IICT): From premalignant to metastatic disease. J. Immunother. Cancer 2024, 12, e008378. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ott, P.A. Intralesional Cancer Immunotherapies. Hematol. Oncol. Clin. N. Am. 2019, 33, 249–260. [Google Scholar] [CrossRef] [PubMed]
- Xu, W.; Atkinson, V.G.; Menzies, A.M. Intratumoural immunotherapies in oncology. Eur. J. Cancer 2020, 127, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Yuan, J.; Khilnani, A.; Brody, J.; Andtbacka, R.H.; Hu-Lieskovan, S.; Luke, J.J.; Diab, A.; Marabelle, A.; Snyder, A.; Cao, Z.A.; et al. Current strategies for intratumoural immunotherapy–Beyond immune checkpoint inhibition. Eur. J. Cancer 2021, 157, 493–510. [Google Scholar] [CrossRef] [PubMed]
- Champiat, S.; Tselikas, L.; Farhane, S.; Raoult, T.; Texier, M.; Lanoy, E.; Massard, C.; Robert, C.; Ammari, S.; De Baère, T.; et al. Intratumoral Immunotherapy: From Trial Design to Clinical Practice. Clin. Cancer Res. 2021, 27, 665–679. [Google Scholar] [CrossRef] [PubMed]
- Ghosn, M.; Tselikas, L.; Champiat, S.; Deschamps, F.; Bonnet, B.; Carre, É.; Testan, M.; Danlos, F.X.; Farhane, S.; Susini, S.; et al. Intratumoral Immunotherapy: Is It Ready for Prime Time? Curr. Oncol. Rep. 2023, 25, 857–867. [Google Scholar] [CrossRef] [PubMed]
- Sheth, R.A.; Murthy, R.; Hong, D.S.; Patel, S.; Overman, M.J.; Diab, A.; Hwu, P.; Tam, A. Assessment of image-guided intratumoral delivery of immunotherapeutics in patients with cancer. JAMA Netw. Open 2020, 3, e207911. [Google Scholar] [CrossRef] [PubMed]
- Seymour, L.; Bogaerts, J.; Perrone, A.; Ford, R.; Schwartz, L.H.; Mandrekar, S.; Lin, N.U.; Litière, S.; Dancey, J.; Chen, A.; et al. RECIST working group. iRECIST: Guidelines for response criteria for use in trials testing immunotherapeutics. Lancet Oncol. 2017, 18, e143–e152. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Munoz, N.M.; Williams, M.; Dixon, K.; Dupuis, C.; McWatters, A.; Avritscher, R.; Manrique, S.Z.; McHugh, K.; Murthy, R.; Tam, A.; et al. Influence of injection technique, drug formulation and tumor microenvironment on intratumoral immunotherapy delivery and efficacy. J. Immunother. Cancer 2021, 9, e001800. [Google Scholar] [CrossRef]
- den Brok, M.H.; Sutmuller, R.P.; van der Voort, R.; Bennink, E.J.; Figdor, C.G.; Ruers, T.J.; Adema, G.J. In situ tumor ablation creates an antigen source for the generation of antitumor immunity. Cancer Res. 2004, 64, 4024–4029. [Google Scholar] [CrossRef] [PubMed]
- den Brok, M.H.; Sutmuller, R.P.; Nierkens, S.; Bennink, E.J.; Frielink, C.; Toonen, L.W.; Boerman, O.C.; Figdor, C.G.; Ruers, T.J.; Adema, G.J. Efficient loading of dendritic cells following cryo and radiofrequency ablation in combination with immune modulation induces anti-tumour immunity. Br. J. Cancer 2006, 95, 896–905. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Mauda-Havakuk, M.; Hawken, N.M.; Owen, J.W.; Mikhail, A.S.; Saxena, A.; Karim, B.; Wakim, P.G.; Pritchard, W.F.; Karanian, J.W.; Wood, B.J. Comparative analysis of the immune response to RFA and cryoablation in a colon cancer mouse model. Sci. Rep. 2022, 12, 18229. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- den Brok, M.H.; Sutmuller, R.P.; Nierkens, S.; Bennink, E.J.; Toonen, L.W.; Figdor, C.G.; Ruers, T.J.; Adema, G.J. Synergy between in situ cryoablation and TLR9 stimulation results in a highly effective in vivo dendritic cell vaccine. Cancer Res. 2006, 66, 7285–7292. [Google Scholar] [CrossRef] [PubMed]
- Nierkens, S.; den Brok, M.H.; Roelofsen, T.; Wagenaars, J.A.; Figdor, C.G.; Ruers, T.J.; Adema, G.J. Route of administration of the TLR9 agonist CpG critically determines the efficacy of cancer immunotherapy in mice. PLoS ONE 2009, 4, e8368. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Slovak, R.; Ludwig, J.M.; Gettinger, S.N.; Herbst, R.S.; Kim, H.S. Immuno-thermal ablations—Boosting the anticancer immune response. J. Immunother. Cancer 2017, 5, 78. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zhang, Z.; Kuo, J.C.; Yao, S.; Zhang, C.; Khan, H.; Lee, R.J. CpG Oligodeoxynucleotides for Anticancer Monotherapy from Preclinical Stages to Clinical Trials. Pharmaceutics 2021, 14, 73. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Wu, Y.; Cao, F.; Zhou, D.; Chen, S.; Qi, H.; Huang, T.; Tan, H.; Shen, L.; Fan, W. Cryoablation reshapes the immune microenvironment in the distal tumor and enhances the anti-tumor immunity. Front. Immunol. 2022, 13, 930461. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- McArthur, H.L.; Diab, A.; Page, D.B.; Yuan, J.; Solomon, S.B.; Sacchini, V.; Comstock, C.; Durack, J.C.; Maybody, M.; Sung, J.; et al. A Pilot Study of Preoperative Single-Dose Ipilimumab and/or Cryoablation in Women with Early-Stage Breast Cancer with Comprehensive Immune Profiling. Clin. Cancer Res. 2016, 22, 5729–5737. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Bostwick, D.G.; Wilk, M.M.; Cribbs, M.; Linton, J.; Ellis, E.E.; Bostwick, B.R.; Rajaratnam, E.C.; Galeazzi, L.M.; Qian, J.; Rydesky, P.M.; et al. Abstract 706: First-in-Human Phase 2 Clinical Trial of Multiplex Combination Intratumoral Immunotherapy (MCII) in Patients with Metastatic Solid Cancer (Abscopal 5001 Trial); SITC: Singapore, 2023. [Google Scholar] [CrossRef]
- Wang, Y.; Jiang, T.; Xie, L.; Wang, H.; Zhao, J.; Xu, L.; Fang, C. Effect of pulsed field ablation on solid tumor cells and microenvironment. Front. Oncol. 2022, 12, 899722. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- National Cancer Institute, NIH, DHHS, Bethesda, MD. Cancer Trends Progress Report. Financial Burden of Cancer Care. Available online: https://progressreport.cancer.gov. (accessed on 16 October 2024).
- Guy, G.P., Jr.; Ekwueme, D.U.; Yabroff, K.R.; Dowling, E.C.; Li, C.; Rodriguez, J.L.; de Moor, J.S.; Virgo, K.S. Economic burden of cancer survivorship among adults in the United States. J. Clin. Oncol. 2013, 31, 3749–3757. [Google Scholar] [CrossRef] [PubMed]
- Mokbel, K.; Kodresko, A.; Ghazal, H.; Mokbel, R.; Trembley, J.; Jouhara, H. The Evolving Role of Cryosurgery in Breast Cancer Management: A Comprehensive Review. Cancers 2023, 15, 4272. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Medicare.gov. Procedure Price Lookup for Outpatient Services: Cryoablation. Available online: https://www.medicare.gov/procedure-price-lookup/cost/0581t (accessed on 8 August 2024).
- Medicare.gov. Procedure Price Lookup for Outpatient Services: Partial Mastectomy Including Lumpectomy. Available online: https://www.medicare.gov/procedure-price-lookup/cost/19301/ (accessed on 8 August 2024).
- Medicare.gov. Procedure Price Lookup for Outpatient Services: Mastectomy, Complete. Available online: https://medicare.gov/procedure-price-lookup/cost/19303/ (accessed on 8 August 2024).
- CostHelper: Cost of a Lumpectomy—2024 Healthcare Costs. Available online: https://health.costhelper.com/lumpectomy.html (accessed on 8 August 2024).
- CostHelper: Mastectomy Cost—2024 Healthcare Costs. Available online: https://health.costhelper.com/mastectomy.html (accessed on 8 August 2024).
- CostHelper: Cost of Breast Cancer Treatment—2024 Healthcare Costs. Available online: https://health.costhelper.com/breast-cancer.html (accessed on 9 August 2024).
- CostHelper: Cost of Radiation Therapy—2024 Healthcare Costs. Available online: https://health.costhelper.com/radiation-therapy.html (accessed on 9 August 2024).
- How Much Does Immunotherapy Cost? Available online: https://www.goodrx.com/drugs/biologics/resources-for-affording-immunotherapy (accessed on 9 August 2024).
- Goldstein, D.A. Adjuvant Ipilimumab for Melanoma-The $1.8 Million per Patient Regimen. JAMA Oncol. 2017, 3, 1628–1629. [Google Scholar] [CrossRef] [PubMed]
- Keytruda Prices. Available online: https://www.drugs.com/price-guide/keytruda (accessed on 8 August 2024).
- Yervoy Prices. Available online: https://www.drugs.com/price-guide/yervoy (accessed on 8 August 2024).
- Yun, J.H.; Fang, A.; Khorshidi, F.; Habibollahi, P.; Kutsenko, O.; Etezadi, V.; Hunt, S.; Nezami, N. New Developments in Image-Guided Percutaneous Irreversible Electroporation of Solid Tumors. Curr. Oncol. Rep. 2023, 25, 1213–1226. [Google Scholar] [CrossRef] [PubMed]
- Neal, R.E., 2nd; Singh, R.; Hatcher, H.C.; Kock, N.D.; Torti, S.V.; Davalos, R.V. Treatment of breast cancer through the application of irreversible electroporation using a novel minimally invasive single needle electrode. Breast Cancer Res. Treat. 2010, 123, 295–301. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Xu, Z.; Pan, C.; Chen, L.; Qian, J.; Chen, X.; Zhou, L.; Zheng, S. Nanosecond Pulsed Electric Field Induces an Antitumor Effect in Triple-Negative Breast Cancer via CXCL9 Axis Dependence in Mice. Cancers 2023, 15, 2076. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Pastori, C.; Nafie, E.H.O.; Wagh, M.S.; Mammarappallil, J.G.; Neal, R.E., 2nd. Pulsed Electric Field Ablation versus Radiofrequency Thermal Ablation in Murine Breast Cancer Models: Anticancer Immune Stimulation, Tumor Response, and Abscopal Effects. J. Vasc. Interv. Radiol. 2024, 35, 442–451.e7. [Google Scholar] [CrossRef] [PubMed]
- Jimenez, M.; Fernandez, J.M.; Krimsky, W.S. Pulsed Electric Field (PEF) treatment of progressive non-small cell lung cancer concurrently treated with immune checkpoint blockade: A case report. Respir. Med. Case Rep. 2024, 49, 102018. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kim, D.H.; Suh, R.D.; Chiang, J.; Abtin, F.; Genshaft, S.J.; Hao, F.; Lu, D.S.K.; Raman, S.S. Technical Feasibility and Safety of Image-Guided Biphasic Monopolar Pulsed Electric Field Ablation of Metastatic and Primary Malignancies. J. Vasc. Interv. Radiol. 2024, 35, 1644–1654. [Google Scholar] [CrossRef] [PubMed]
- Qu, S.; Worlikar, T.; Felsted, A.E.; Ganguly, A.; Beems, M.V.; Hubbard, R.; Pepple, A.L.; Kevelin, A.A.; Garavaglia, H.; Dib, J.; et al. Non-thermal histotripsy tumor ablation promotes abscopal immune responses that enhance cancer immunotherapy. J. Immunother. Cancer 2020, 8, e000200. [Google Scholar] [CrossRef]
- Osada, T.; Jiang, X.; Zhao, Y.; Chen, M.; Kreager, B.C.; Wu, H.; Kim, H.; Ren, J.; Snyder, J.; Zhong, P.; et al. The use of histotripsy as intratumoral immunotherapy beyond tissue ablation- the rationale for exploring the immune effects of histotripsy. Int. J. Hyperther. 2023, 40, 2263672. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| pT | pTNM-Stage | Clinical Treatments | Metastasis |
|---|---|---|---|
| Stage 0 | |||
| Tis: DCIS, LCIS, Paget’s (no tumor) | 0/Tis | Surgery, Radiation | No distant metastasis |
| Stage I | |||
| T1 mic ≤ 0.1 cm | IA/T1N0 | Surgery, Radiation | No distant metastasis |
| T1a ≤ 0.5 cm | IA/T1N0 | Surgery, Radiation | No distant metastasis |
| T1b > 0.5–1.0 cm | IB/T0-1N1 or T0-1N1mi | Surgery, Radiation, Chemotherapy | No distant metastasis |
| Stage II | |||
| T1c > 1–2 cm | IIA/T1N0-1, T2N0 | Surgery, Chemotherapy, Radiation | No distant metastasis |
| T2 > 2–5 cm | IIA/T2N0-1 | Surgery, Chemotherapy, Radiation | No distant metastasis |
| T3 > 5 cm (no chest wall/skin invasion) | IIB/T3N0-1 | Surgery, Radiation, Chemotherapy | No distant metastasis |
| Stage III | |||
| T4a (chest wall extension) | IIIA/T0-2N2, T3N1-2 | Surgery, Radiation, Chemotherapy | Metastasis |
| T4b (ulceration, skin nodules, peau d’orange) | IIIA/T4N0-3, T3N1-2 | Surgery, Chemotherapy | Metastasis |
| T4c (T4a + T4b) | IIIC/any TN3 | Chemotherapy, Radiation | Metastasis |
| Stage IV | |||
| T4d (inflammatory cancer) | IV | Systemic | Metastasis |
| De-escalation Opportunities | Estimated Costs |
|---|---|
| Cryotherapy–Small Tumor | Hospital Outpatient Facility Fee: USD 3631; Medicare pays up to USD 2905 [85] |
| Cryotherapy–Large Tumors (7 probes) | Outpatient Cost: USD 8226 [46] |
| Lumpectomy | Total Cost: USD 16,896.50 [46]; Expected Range: USD 10,000–USD 20,000 [86,88] |
| Mastectomy | Medicare Pays: USD 5726; Expected Range: USD 15,000–USD 55,000 [89] |
| Hormonal Therapy | Tamoxifen: ~USD 14/month or ~USD 168/year; Arimidex: ~USD 19/month or ~USD 228/year [90] |
| Chemotherapy | USD 10,000–USD 100,000 [90] |
| Radiation Therapy (Whole Breast) | USD 4500–USD 14,500 (specifically reported for breast cancer) [91] |
| Immunotherapy–Intravenous (IV) | USD 100,000–USD 500,000 (varies); Pembrolizumab: USD 22,674.72 every six weeks (~USD 191,000/year); Yervoy (3-year full regimen): ~USD 1.77 million [USD 145/mg] [92,93,94,95] |
| Immunotherapy–Intratumoral + Sub-Q | Keytruda: ~USD 6098 per 4 mL dose [92,94]; Yervoy: ~USD 9174 per 10 mL dose [92,93,95]; Leukine (GM-CSF): ~USD 4255 for 14 vials (4-week post-ablation course) |
| Cellular-Based Treatments (e.g., CAR-T) | ~USD 373,000 per infusion [92] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fermanian, J.; Ward, R.C.; Holmes, D.R.; Fisher, A.C.; Harvey, J.; Marples, B.; Littrup, P.J. Cryoablation and Intratumoral Immunotherapy for Breast Cancer: A Future Path to Cost-Effective De-Escalation for Larger Tumors, Lymph Nodes and Metastatic Disease. Cancers 2025, 17, 1915. https://doi.org/10.3390/cancers17121915
Fermanian J, Ward RC, Holmes DR, Fisher AC, Harvey J, Marples B, Littrup PJ. Cryoablation and Intratumoral Immunotherapy for Breast Cancer: A Future Path to Cost-Effective De-Escalation for Larger Tumors, Lymph Nodes and Metastatic Disease. Cancers. 2025; 17(12):1915. https://doi.org/10.3390/cancers17121915
Chicago/Turabian StyleFermanian, Josephine, Robert C. Ward, Dennis R. Holmes, Ariel C. Fisher, Jennifer Harvey, Brian Marples, and Peter J. Littrup. 2025. "Cryoablation and Intratumoral Immunotherapy for Breast Cancer: A Future Path to Cost-Effective De-Escalation for Larger Tumors, Lymph Nodes and Metastatic Disease" Cancers 17, no. 12: 1915. https://doi.org/10.3390/cancers17121915
APA StyleFermanian, J., Ward, R. C., Holmes, D. R., Fisher, A. C., Harvey, J., Marples, B., & Littrup, P. J. (2025). Cryoablation and Intratumoral Immunotherapy for Breast Cancer: A Future Path to Cost-Effective De-Escalation for Larger Tumors, Lymph Nodes and Metastatic Disease. Cancers, 17(12), 1915. https://doi.org/10.3390/cancers17121915