
Long-Term Results of a Prospective Multicenter Trial of APBI with Photon IORT

 and
and
Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Study Design and Participants
2.2. Follow-Up
2.3. Outcomes
2.4. Statistical Analysis
3. Results
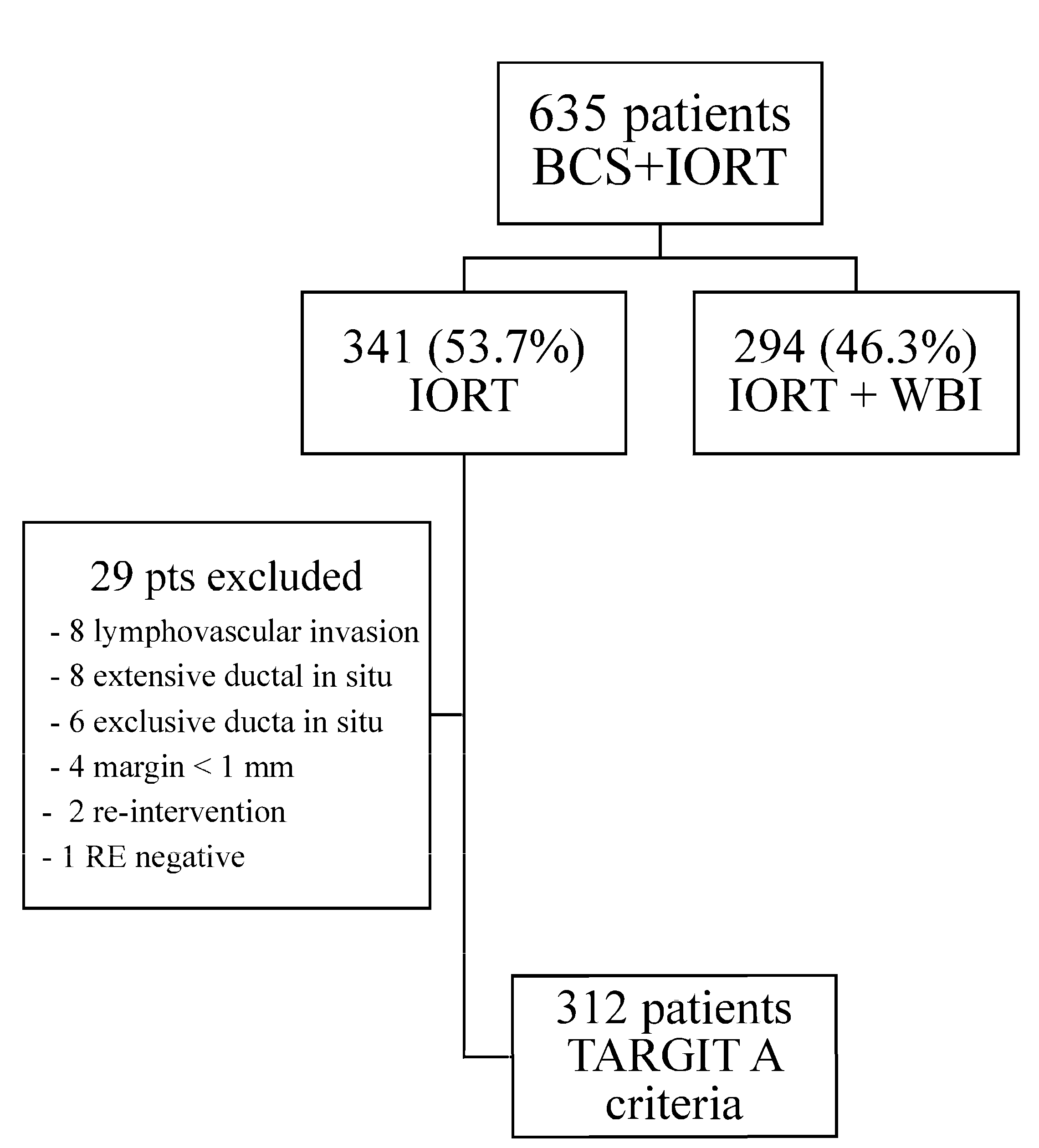
3.1. Patients and Treatment
3.2. Toxicity
4. Discussion
- (a)
- Strict adherence to patient selection characteristics outlined by the TARGIT A criteria for exclusive IORT, which also align with the GEC-ESTRO low-risk criteria (good candidates) for partial breast irradiation, was maintained. Our inclusion criteria followed those proposed in the TARGIT A trial: age over 45 years, no preoperative systemic therapy administered, invasive carcinoma of any grade, unifocal tumor with a diameter ≤ 3 cm, cN0, M0, and no lobular histology. Patients with risk factors necessitating complementary external radiotherapy, such as surgical margin < 1 mm, any resection after IORT, lymphovascular invasion, lobular histology, extensive ductal in situ component, and nodal involvement (pN1), were excluded from the study.
- (b)
- We also included only luminal cases. Luminal B (Her2+ and highly proliferating tumors) were also included if they were not considered candidates for primary systemic therapy. Patients with high-risk molecular factors (Her2+/triple negative) and/or advanced tumors (node positive, T > 3 cm) were referred for primary systemic therapy (if necessary).
- (c)
- Our study was carried out in 3 academic hospitals in the Las Palmas province with immediate access to conservative surgery and intraoperative radiotherapy. Furthermore, after the TARGIT A publications, it was shown that the post-pathology cohort had poorer results for local control within the breast compared to those receiving immediate intraoperative radiotherapy. Therefore, no post-pathology patients were included in our study.
- (d)
- As per protocol, our patients were not candidates for adjuvant WBI according to the TARGIT A guidelines. Furthermore, our patients were GEC-ESTRO candidates for partial breast irradiation, so no indication for whole-breast irradiation was acknowledged.
- (e)
- All patients in our study had luminal profiles; therefore, all of them were recommended to receive hormonal adjuvant treatment, either alone or in combination with chemotherapy or anti-Her2treatment according to guidelines. Unfortunately, 15 cases (4.8%) had medical contraindications or refused hormonal treatment.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Early Breast Cancer Trialists’ Collaborative Group (EBCTCG); Darby, S.; McGale, P.; Correa, C.; Taylor, C.; Arriagada, R.; Clarke, M.; Cutter, D.; Davies, C.; Ewertz, M.; et al. Effect of radiotherapy after breast-conserving surgery on 10-year recurrence and 15-year breast cancer death: Meta-analysis of individual patient data for 10,801 women in 17 randomised trials. Lancet 2011, 378, 1707–1716. [Google Scholar] [CrossRef] [PubMed]
- Baum, M.; Vaidya, J.S.; Mittra, I. Multicentricity and recurrence of breast cancer. Lancet 1997, 349, 208. [Google Scholar] [CrossRef] [PubMed]
- Livi, L.; Meattini, I.; Marrazzo, L.; Simontacchi, G.; Pallotta, S.; Saieva, C.; Paiar, F.; Scotti, V.; De Luca Cardillo, C.; Bastiani, P.; et al. Accelerated partial breast irradiation using intensity-modulated radiotherapy versus whole breast irradiation: 5-year survival analysis of a phase 3 randomised controlled trial. Eur. J. Cancer 2015, 51, 451–463. [Google Scholar] [CrossRef] [PubMed]
- Coles, C.E.; Griffin, C.L.; Kirby, A.M.; Titley, J.; Agrawal, R.K.; Alhasso, A.; Bhattacharya, I.S.; Brunt, A.M.; Ciurlionis, L.; Chan, C.; et al. IMPORT Trialists. Partial-breast radiotherapy after breast conservation surgery for patients withearly breast cancer (UK IMPORT LOW trial): 5-year results from a multicentre, randomised, controlled, phase 3, non-inferiority trial. Lancet 2017, 390, 1048–1060. [Google Scholar] [CrossRef]
- Strnad, V.; Ott, O.J.; Hildebrandt, G.; Kauer-Dorner, D.; Knauerhase, H.; Major, T.; Lyczek, J.; Guinot, J.L.; Dunst, J.; Gutierrez Miguelez, C.; et al. Groupe Européen de Curiethérapie of European Society for Radiotherapy and Oncology (GEC-ESTRO). 5-year results of accelerated partial breast irradiation using sole interstitial multicatheter brachytherapy versus whole-breast irradiation with boost after breast-conserving surgery for low-risk invasive and in-situ carcinoma of the female breast: A randomised, phase 3, non-inferiority trial. Lancet 2016, 387, 229–238. [Google Scholar] [CrossRef] [PubMed]
- Shaitelman, S.F.; Anderson, B.M.; Arthur, D.W.; Bazan, J.G.; Bellon, J.R.; Bradfield, L.; Coles, C.E.; Gerber, N.K.; Kathpal, M.; Kim, L. Partial Breast Irradiation for Patients With Early-Stage Invasive Breast Cancer or Ductal Carcinoma In Situ: An ASTRO Clinical Practice Guideline. Pract. Radiat. Oncol. 2024, 14, 112–132. [Google Scholar] [CrossRef] [PubMed]
- Strnad, V.; Major, T.; Polgar, C.; Lotter, M.; Guinot, J.L.; Gutierrez-Miguelez, C.; Galalae, R.; Van Limbergen, E.; Guix, B.; Niehoff, P.; et al. ESTRO-ACROP guideline: Interstitial multi-catheter breast brachytherapy as Accelerated Partial Breast Irradiation alone or as boost—GEC-ESTRO Breast Cancer Working Group practical recommendations. Radiother. Oncol. 2018, 128, 411–420. [Google Scholar] [CrossRef]
- Veronesi, U.; Orecchia, R.; Maisonneuve, P.; Viale, G.; Rotmensz, N.; Sangalli, C.; Luini, A.; Veronesi, P.; Galimberti, V.; Zurrida, S.; et al. Intraoperative radiotherapy versus external radiotherapy for early breast cancer (ELIOT): A randomised controlled equivalence trial. Lancet Oncol. 2013, 14, 1269–1277. [Google Scholar] [CrossRef] [PubMed]
- Vaidya, J.S.; Wenz, F.; Bulsara, M.; Tobias, J.S.; Joseph, D.J.; Keshtgar, M.; Flyger, H.L.; Massarut, S.; Alvarado, M.; Saunders, C.; et al. TARGIT trialists’ group Risk-adapted targeted intraoperative radiotherapy versus whole-breast radiotherapy for breast cancer: 5-year results for local control and overall survival from the TARGIT-A randomised trial. Lancet 2014, 383, 603–613. [Google Scholar] [CrossRef] [PubMed]
- Fastner, G.; Gaisberger, C.; Kaiser, J.; Scherer, P.; Ciabattoni, A.; Petoukhova, A.; Sperk, E.; Poortmans, P.; Calvo, F.A.; Sedlmayer, F.; et al. ESTRO IORT Task Force/ACROP recommendations for intraoperative radiation therapy with electrons (IOERT) in breast cancer. Radiother. Oncol. 2020, 149, 150–157. [Google Scholar] [CrossRef] [PubMed]
- Cuzick, J. Radiotherapy for breast cancer, the TARGIT-A trial. Lancet 2014, 383, 1716. [Google Scholar] [CrossRef] [PubMed]
- Vaidya, J.S.; Bulsara, M.; Saunders, C.; Flyger, H.; Tobias, J.S.; Corica, T.; Massarut, S.; Wenz, F.; Pigorsch, S.; Alvarado, M.; et al. Effect of Delayed Targeted Intraoperative Radiotherapy vs. Whole-Breast Radiotherapy on Local Recurrence and Survival: Long-term Results From the TARGIT-A Randomized Clinical Trial in Early Breast Cancer. JAMA Oncol. 2020, 6, e200249. [Google Scholar] [CrossRef]
- Vaidya, J.S.; Bulsara, M.; Baum, M.; Wenz, F.; Massarut, S.; Pigorsch, S.; Alvarado, M.; Douek, M.; Saunders, C.; Flyger, H.L.; et al. Long term survival and local control outcomes from single dose targeted intraoperative radiotherapy during lumpectomy (TARGIT-IORT) for early breast cancer: TARGITA randomised clinical trial. BMJ 2020, 370, m2836. [Google Scholar] [CrossRef] [PubMed]
- Piroth, M.D.; Strnad, V.; Krug, D.; Fastner, G.; Baumann, R.; Combs, S.E.; Duma, M.N.; Dunst, J.; Feyer, P.; Fietkau, R.; et al. Long-Term Results of the TARGIT-A Trial: More Questions than Answers. Breast Care 2022, 17, 81–84. [Google Scholar] [CrossRef] [PubMed]
- Vaidya, J.S.; Bulsara, M.; Wenz, F.; Coombs, N.; Singer, J.; Ebbs, S.; Massarut, S.; Saunders, C.; Douek, M.; Williams, N.R.; et al. Reduced Mortality With Partial-Breast Irradiation for Early Breast Cancer: A Meta-Analysis of Randomized Trials. Int. J. Radiat. Oncol. Biol. Phys. 2016, 96, 259–265. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.boe.es/eli/es/rd/1998/07/17/1566 (accessed on 14 March 2025).
- Brierley, J.D.; Gospodarowicz, M.K.; Wittekind, C. (Eds.) TNM Classification of Malignant Tumours, 8th ed.; Wiley-Blackwell: Hoboken, NJ, USA, 2016; ISBN 978-1-119-26357-9. [Google Scholar]
- Available online: https://www.nccn.org/professionals/physician_gls/pdf/breast.pdf (accessed on 14 March 2025).
- Available online: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/ctc.htm#ctc_50 (accessed on 14 March 2025).
- Ravani, L.V.; Calomeni, P.; Wang, M.; Deng, D.; Speers, C.; Zaorsky, N.G.; Shah, C. Comparison of partial-breast irradiation and intraoperative radiation to whole-breast irradiation in early-stage breast cancer patients: A Kaplan-Meier-derived patient data meta-analysis. Breast Cancer Res. Treat. 2024, 203, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Viani, G.A.; Arruda, C.V.; Faustino, A.C.; De Fendi, L.I. Partial-breast irradiation versus whole-breast radiotherapy for early breast cancer: A systematic review and update meta-analysis. Brachytherapy 2020, 19, 491–498. [Google Scholar] [CrossRef] [PubMed]
- Vaidya, J.S.; Vaidya, U.J.; Baum, M.; Bulsara, M.K.; Joseph, D.; Tobias, J.S. Global adoption of single-shot targeted intraoperative radiotherapy (TARGIT-IORT) for breast cancer-better for patients, better for healthcare systems. Front. Oncol. 2022, 12, 786515. [Google Scholar] [CrossRef]
- Laplana, M.; García-Marqueta, M.; Sánchez-Fernández, J.J.; Martínez-Pérez, E.; Pérez-Montero, H.; Martínez-Montesinos, I.; Eraso, A.; Saldaña, P.; Martín, R.; Martín, M.I.; et al. Effectiveness and safety of intraoperative radiotherapy (IORT) with low-energy X-rays (INTRABEAM()) for accelerated partial breast irradiation (APBI). Clin. Transl. Oncol. 2022, 24, 1732–1743. [Google Scholar] [CrossRef] [PubMed]
- Tallet, A.; Racadot, S.; Boher, J.M.; Cohen, M.; Barrou, J.; Houvenaeghel, G.; Gutowski, M.; Delmond, L.; Lemanski, C. The actual benefit of intraoperative radiation therapy using 50 kV x-rays in early breast cancer: A retrospective study of 676 patients. Breast J. 2020, 26, 2145–2150. [Google Scholar] [CrossRef] [PubMed]
- Valente, S.A.; Tendulkar, R.D.; Cherian, S.; Shah, C.; Ross, D.L.; Lottich, S.C.; Laronga, C.; Broman, K.K.; Donnelly, E.D.; Bethke, K.P.; et al. TARGIT-R (Retrospective): 5-Year Follow-Up Evaluation of Intraoperative Radiation Therapy (IORT) for Breast Cancer Performed in North America. Ann. Surg. Oncol. 2021, 28, 2512–2521. [Google Scholar] [CrossRef] [PubMed]
- Guillerm, S.O.; Bourstyn, E.; Itti, R.; Cahen-Doidy, L.; Quéro, L.; Labidi, M.; Marchand, E.; Lorphelin, H.; Giacchetti, S.; Cuvier, C.; et al. Intraoperative Radiotherapy for Breast Cancer in Elderly Women. Clin. Breast Cancer 2022, 22, e109–e113. [Google Scholar] [CrossRef] [PubMed]
- Vinante, L.; Vaidya, J.S.; Caroli, A.; Mileto, M.; Piccoli, E.; Avanzo, M.; Barresi, L.; Marson, M.; Montico, M.; Baboci, L.; et al. Real world clinical outcomes from targeted intraoperative radiotherapy (TARGIT-IORT) during lumpectomy for breast cancer: Data from a large cohort at a national cancer institute. Front. Oncol. 2024, 14, 1424630. [Google Scholar] [CrossRef] [PubMed]
- Takanen, S.; Gambirasio, A.; Gritti, G.; Källi, M.; Andreoli, S.; Fortunato, M.; Feltre, L.; Filippone, F.R.; Iannacone, E.; Maffioletti, L.; et al. Breast cancer electron intraoperative radiotherapy: Assessment of preoperative selection factors from a retrospective analysis of 758 patients and review of literature. Breast Cancer Res. Treat. 2017, 165, 261–271. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Ibarria, N.G.; Pinar, B.; García, L.; Cabezón, A.; Rey-Baltar, D.; Rodríguez-Melcón, J.I.; Lloret, M.; Lara, P.C. Ten-Year Results of Accelerated Partial-Breast Irradiation with Interstitial Multicatheter Brachytherapy after Breast-Conserving Surgery for Low-Risk Early Breast Cancer. Cancers 2024, 16, 1138. [Google Scholar] [CrossRef]
- Kunkler, I.H.; Williams, L.J.; Jack, W.J.L.; Cameron, D.A.; Dixon, J.M. Breast-Conserving Surgery with or without Irradiation in Early Breast Cancer. N. Engl. J. Med. 2023, 388, 585–594. [Google Scholar] [CrossRef] [PubMed]
- Taha, A.M.; Kamel, H.A.; Khlidj, Y.; Salem, D.S.; Saed, S.A.A.; Abouelmagd, K.; Nguyen, D.; Shash, E.; Chapagain, S.; Kassem, L. Adjuvant radiotherapy in postmenopausal women with early-stage ER-positive breast cancer: A systematic review and meta-analysis. Medicine 2025, 104, e41632. [Google Scholar] [CrossRef] [PubMed]
- Haussmann, J.; Budach, W.; Corradini, S.; Krug, D.; Bölke, E.; Tamaskovics, B.; Jazmati, D.; Haussmann, A.; Matuschek, C. Whole Breast Irradiation in Comparison to EndocrineTherapy in Early Stage Breast Cancer-A Direct and Network Meta-Analysis of Published Randomized Trials. Cancers 2023, 15, 4343. [Google Scholar] [CrossRef]
- Hannoun-Levi, J.M.; Chamorey, E.; Boulahssass, R.; Polgar, C.; Strnad, V.; Breast Cancer Working Group of the GEC-ESTRO. Endocrine therapy with accelerated partial breast irradiation or exclusive ultra-accelerated partial breast irradiation for women aged >60 years with early-stage breast cancer (EPOPE): The rationale for a GEC-ESTRO randomized phase III-controlled trial. Clin. Transl. Radiat. Oncol. 2021, 29, 1–8. [Google Scholar] [CrossRef]
- Meattini, I.; De Santis, M.C.; Visani, L.; Scorsetti, M.; Fozza, A.; Meduri, B.; De Rose, F.; Bonzano, E.; Prisco, A.; Masiello, V.; et al. Single-modality endocrine therapy versus radiotherapy after breast-conserving surgery in women aged 70 years and older with luminal A-like early breast cancer (EUROPA): A preplanned interim analysis of a phase 3, non-inferiority, randomised trial. Lancet Oncol. 2025, 26, 37–50. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Patients | |
|---|---|
| Age (years) Mean 62 (46–88) | |
| <70 | 257 (82.4%) |
| ≥70 | 55 (17.6%) |
| Menopausal status | |
| Premenopausal | 36 (11.5%) |
| Postmenopausal | 276 (88.5%) |
| T stage | |
| pT1mi | 1 (0.3%) |
| pT1a | 10 (3.2%) |
| pT1b | 143 (45.8%) |
| pT1c | 147 (47.2%) |
| pT2 | 11 (3.5%) |
| Grade | |
| 1 | 200 (64.1%) |
| 2 | 104 (33.3%) |
| 3 | 8 (2.6%) |
| ER status | |
| Positive | 312 (100%) |
| PR status | |
| Positive | 280 (89.7%) |
| Negative | 32 (10.3%) |
| Ki67 status | |
| Positive | 85 (27.2%) |
| Negative | 180 (57.7%) |
| Unknown | 47 (15.1%) |
| Her2 status | |
| Positive | 10 (3.2%) |
| Negative | 301 (96.5%) |
| Unknown | 1 (0.3%) |
| Molecular subtype | |
| Luminal A | 183 (58.7%) |
| Luminal B | 93 (29.8%) |
| Luminal | 36 (11.5%) |
| Chemotherapy | |
| Yes | 44 (14.1%) |
| No | 268 (85.9%) |
| Endocrine therapy | |
| Yes | 297 (95.2%) |
| No | 15 (4.8%) |
| Anti HER2 therapy | |
| Yes | 8 (2.6%) |
| No | 304 (97.4%) |
| Patients | 5 y IBTR (95%CI) | p Value | |
|---|---|---|---|
| Age at diagnosis | |||
| <70 y | 257 (82.4%) | 0.5% (0–1%) | 0.084 |
| ≥70 y | 55 (17.6%) | 3.9% (1.2–6.6%) | |
| Menopausal status | |||
| Premenopausal | 36 (11.5%) | 0% | 0.425 |
| Postmenopausal | 276 (88.5%) | 1.2% (0.5–1.9%) | |
| Surgical margins distance | |||
| ≤1 mm | 33 (10.6%) | 3.1% (0–6.2%) | 0.667 |
| >1 & ≤10 mm | 202 (64.7%) | 0.5% (0–1%) | |
| >10 mm | 77 (24.7%) | 2.2% (0–4.4%) | |
| Tumor status | |||
| pT1 | 301 (96.5%) | 1.1% (0.4–1.8%) | 0.705 |
| pT2 | 11 (3.5%) | 0% | |
| Tumor grade | |||
| 1 | 200 (64.1%) | 0% | 0.021 |
| 2 | 104 (33.3%) | 3.2% (1.4–5%) | |
| 3 | 8 (2.6%) | 0% | |
| PR status | |||
| Positive | 280 (89.7%) | 0.8% (0.3–1.3%) | 0.279 |
| Negative | 32 (10.3%) | 4.3% (0–8.6%) | |
| Her2 status | |||
| Positive | 10 (3.2%) | 0% | 0.924 |
| Negative | 301 (96.5%) | 1.1% (0.4–1.8%) | |
| Ki67 status | |||
| Positive | 85 (57.7%) | 4% (1.7–6.3%) | 0.004 |
| Negative | 180 (57.7%) | 0% | |
| Unknown | 47 (15.1%) | 0% | |
| ESTRO risk | |||
| Low | 253 (81.1%) | 0.5% (0–1%) | 0.147 |
| Intermediate | 59 (18.9%) | 3.5% (1–6%) | |
| (A) PBI vs. WBI Studies | Type of Study | Centers | PBI Patients | PBI Technique | IBTR (5 y) |
|---|---|---|---|---|---|
| FLORENCE (2015) [3] | Randomized | Multicenter | 260 | EBRT | 1.5% |
| IMPORT LOW (2017) [4] | Randomized | Multicenter | 669 | EBRT | 0.5% |
| GEC-ESTRO (2016) [5] | Randomized | Multicenter | 633 | Brachy | 1.44% |
| ELLIOT (2013) [8] | Randomized | Multicenter | 651 | IOERT | 4,2% |
| TARGIT A (2014) [9] | Randomized | Multicenter | 1721 * | Ph-IORT | 3.3% |
| (B) Exclusive phIORT | Type of study | Centers | PBI Patients | PBI technique | IBTR (5 y) |
| Tallet A (2020) [24] | Retrospective | Multicenter | 406 # | phIORT | 1.5% |
| TARGIT R(2021) [25] | Retrospective | Multicenter | 477 # | phIORT | 8% |
| Guillerm (2022) [26] | Retrospective | Unicenter | 191 # | phIORT | 1.7% |
| Laplana M, (2022) [23] | Prospective | Unicenter | 50 | phIORT | 2.9% |
| Vinante et al (2024) [27] | Prospective | Unicenter | 491 # | phIORT | 2,5% |
| Present study (2025) | Prospective | Multicenter | 312 | phIORT | 1,1% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
García-Cabrera, L.; Pinar-Sedeño, B.; Cabezón-Pons, M.A.; Rodriguez-Ibarria, N.; Dominguez-Dominguez, A.; Aguiar-Santana, D.; Martín-Barrientos, P.; Rey-López, I.; Lara, P.C.; Lloret-Saez-Bravo, M. Long-Term Results of a Prospective Multicenter Trial of APBI with Photon IORT. Cancers 2025, 17, 1762. https://doi.org/10.3390/cancers17111762
García-Cabrera L, Pinar-Sedeño B, Cabezón-Pons MA, Rodriguez-Ibarria N, Dominguez-Dominguez A, Aguiar-Santana D, Martín-Barrientos P, Rey-López I, Lara PC, Lloret-Saez-Bravo M. Long-Term Results of a Prospective Multicenter Trial of APBI with Photon IORT. Cancers. 2025; 17(11):1762. https://doi.org/10.3390/cancers17111762
Chicago/Turabian StyleGarcía-Cabrera, Laura, Beatriz Pinar-Sedeño, María Auxiliadora Cabezón-Pons, Nieves Rodriguez-Ibarria, Alba Dominguez-Dominguez, Daniel Aguiar-Santana, Paula Martín-Barrientos, Irene Rey-López, Pedro C. Lara, and Marta Lloret-Saez-Bravo. 2025. "Long-Term Results of a Prospective Multicenter Trial of APBI with Photon IORT" Cancers 17, no. 11: 1762. https://doi.org/10.3390/cancers17111762
APA StyleGarcía-Cabrera, L., Pinar-Sedeño, B., Cabezón-Pons, M. A., Rodriguez-Ibarria, N., Dominguez-Dominguez, A., Aguiar-Santana, D., Martín-Barrientos, P., Rey-López, I., Lara, P. C., & Lloret-Saez-Bravo, M. (2025). Long-Term Results of a Prospective Multicenter Trial of APBI with Photon IORT. Cancers, 17(11), 1762. https://doi.org/10.3390/cancers17111762