



Contrast Agent Dynamics Determine Radiomics Profiles in Oncologic Imaging
 , , and
, , and
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethics
2.2. Inclusion and Exclusion Criteria
2.3. Dynamic Contrast-Enhanced CT Imaging Protocol
2.4. Dynamic Contrast-Enhanced MRI Imaging Protocol for pzPC Patients
2.5. Dynamic Contrast-Enhanced MRI Imaging Protocol for NSCLC Patients
2.6. Region-of-Interest Segmentation
2.7. Radiomics Feature Extraction
2.8. Statistical Analysis
- 1.
- 2.
3. Results
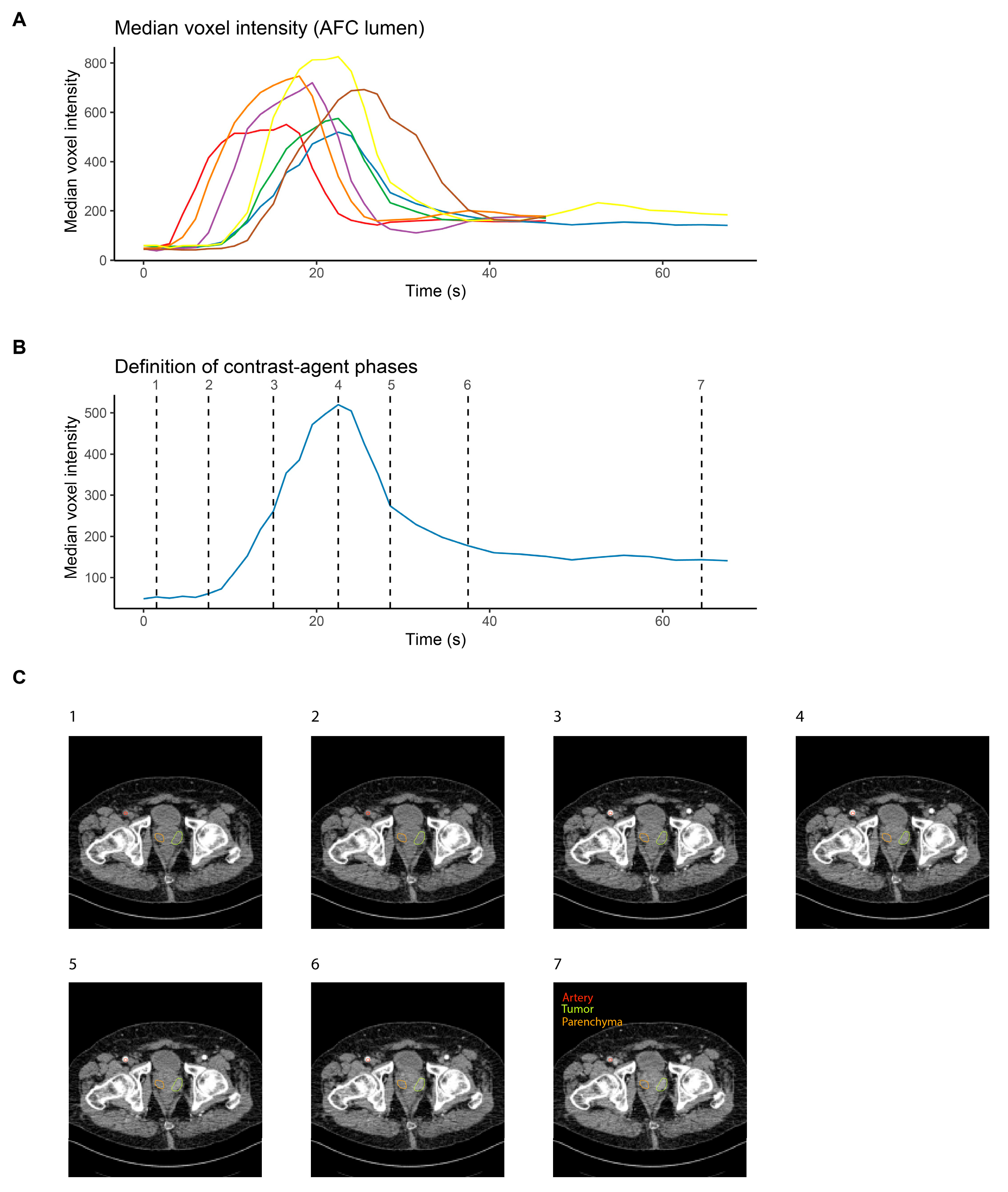
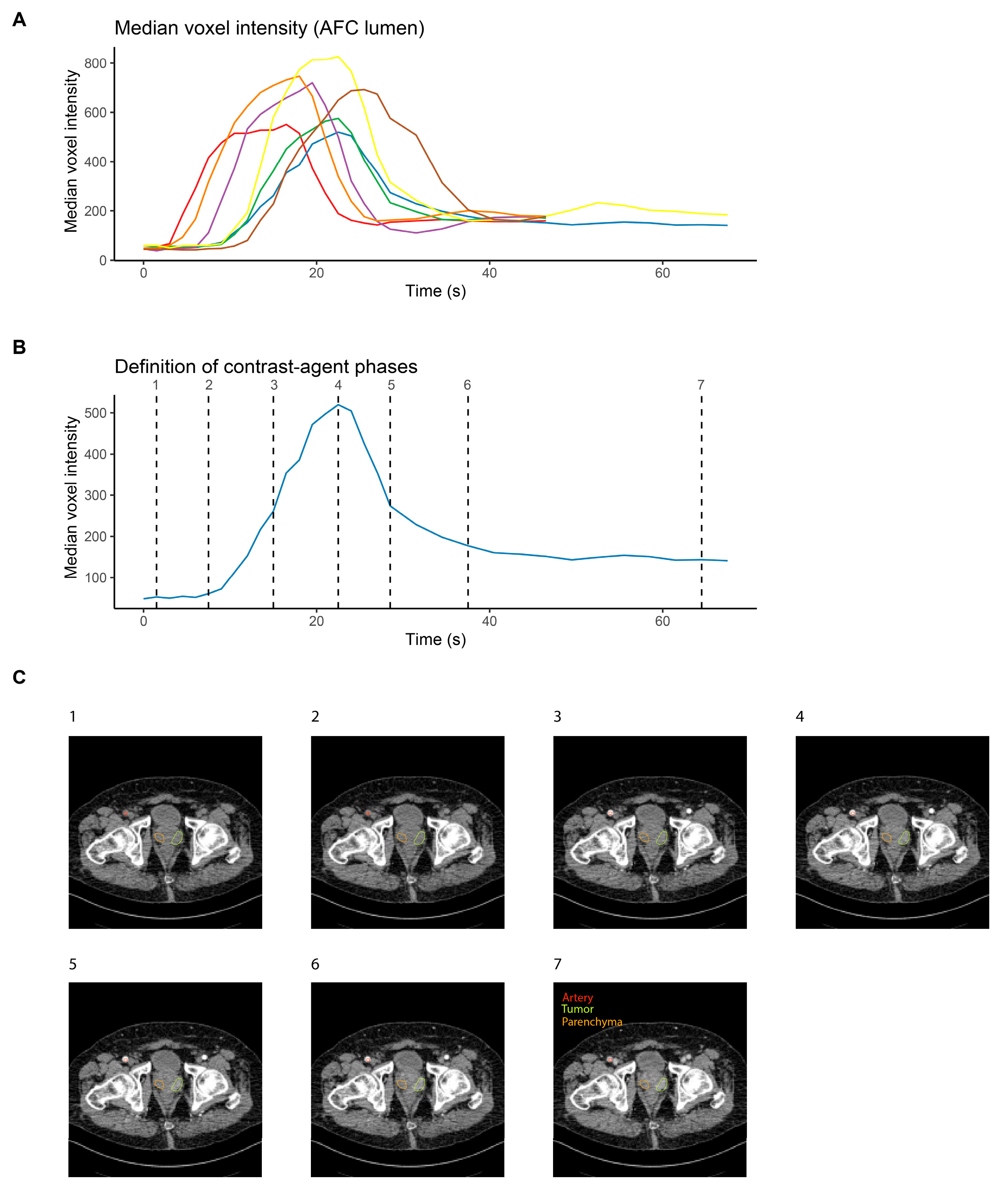
3.1. Contrast Agent Dynamics Vary between Patients and Require Standardization for Systematic Analysis
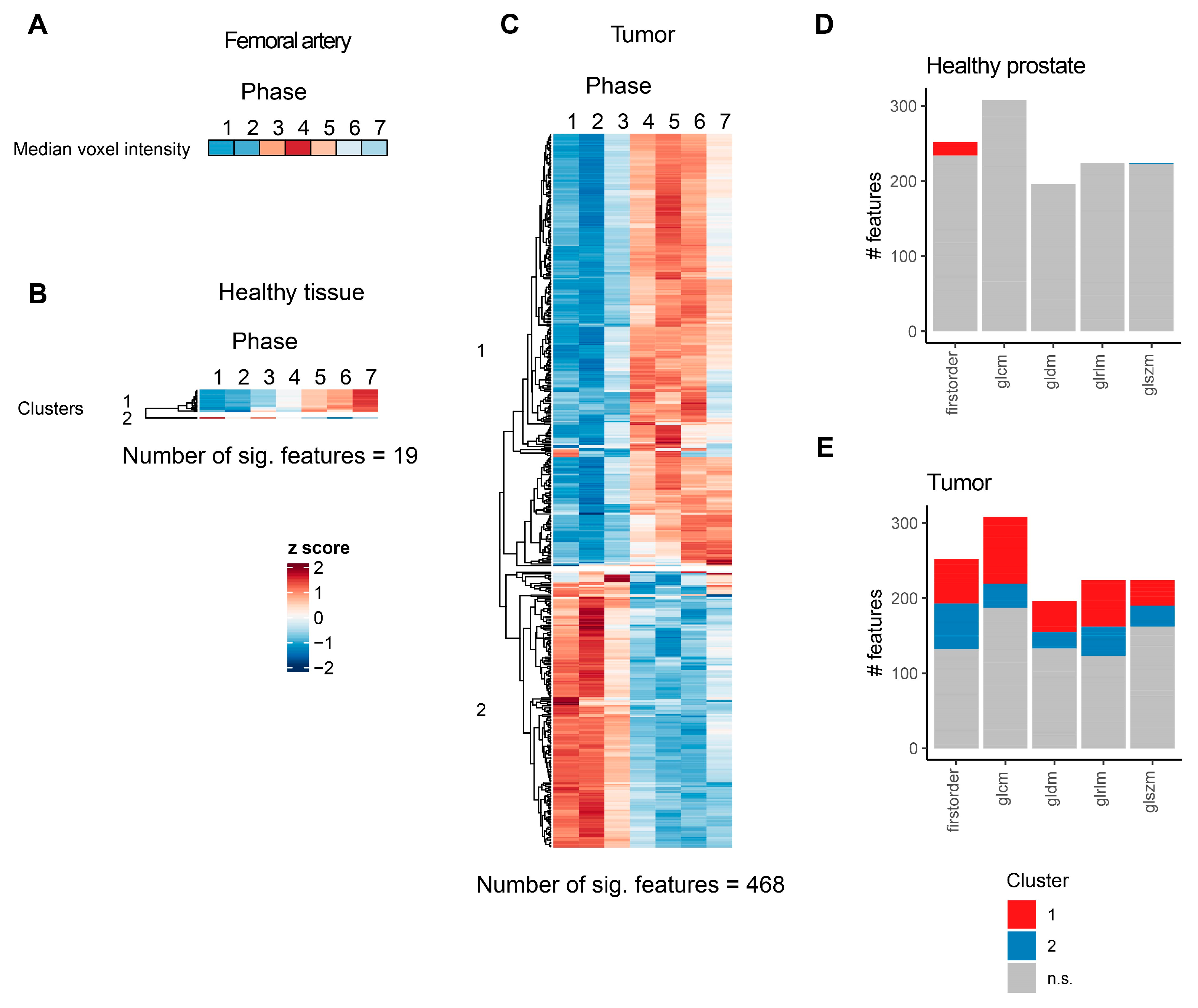
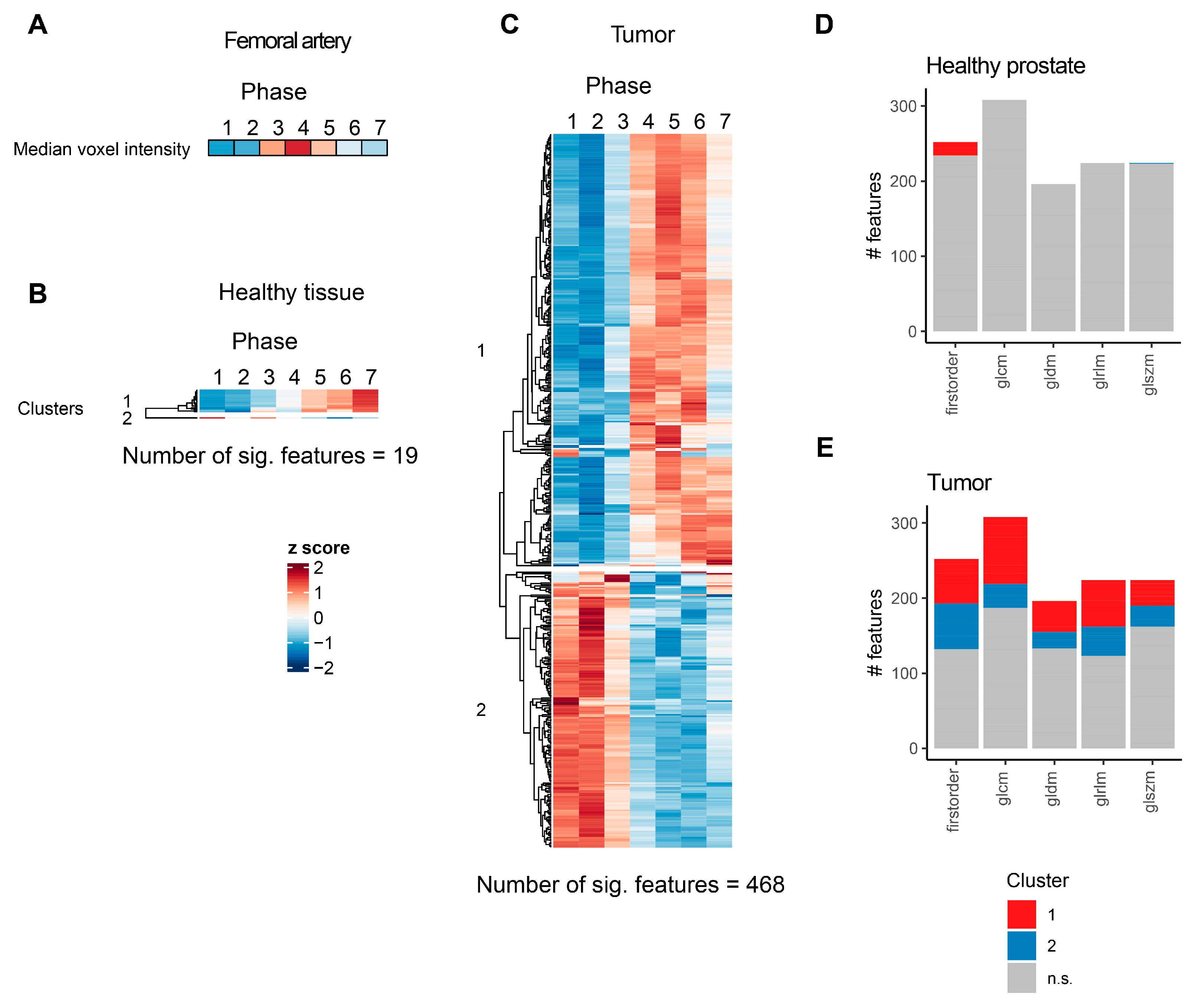
3.2. Contrast Agent Injection Induces Changes in CT Radiomics Features in Peripheral Zone Prostate Cancer and Healthy Prostate Parenchyma
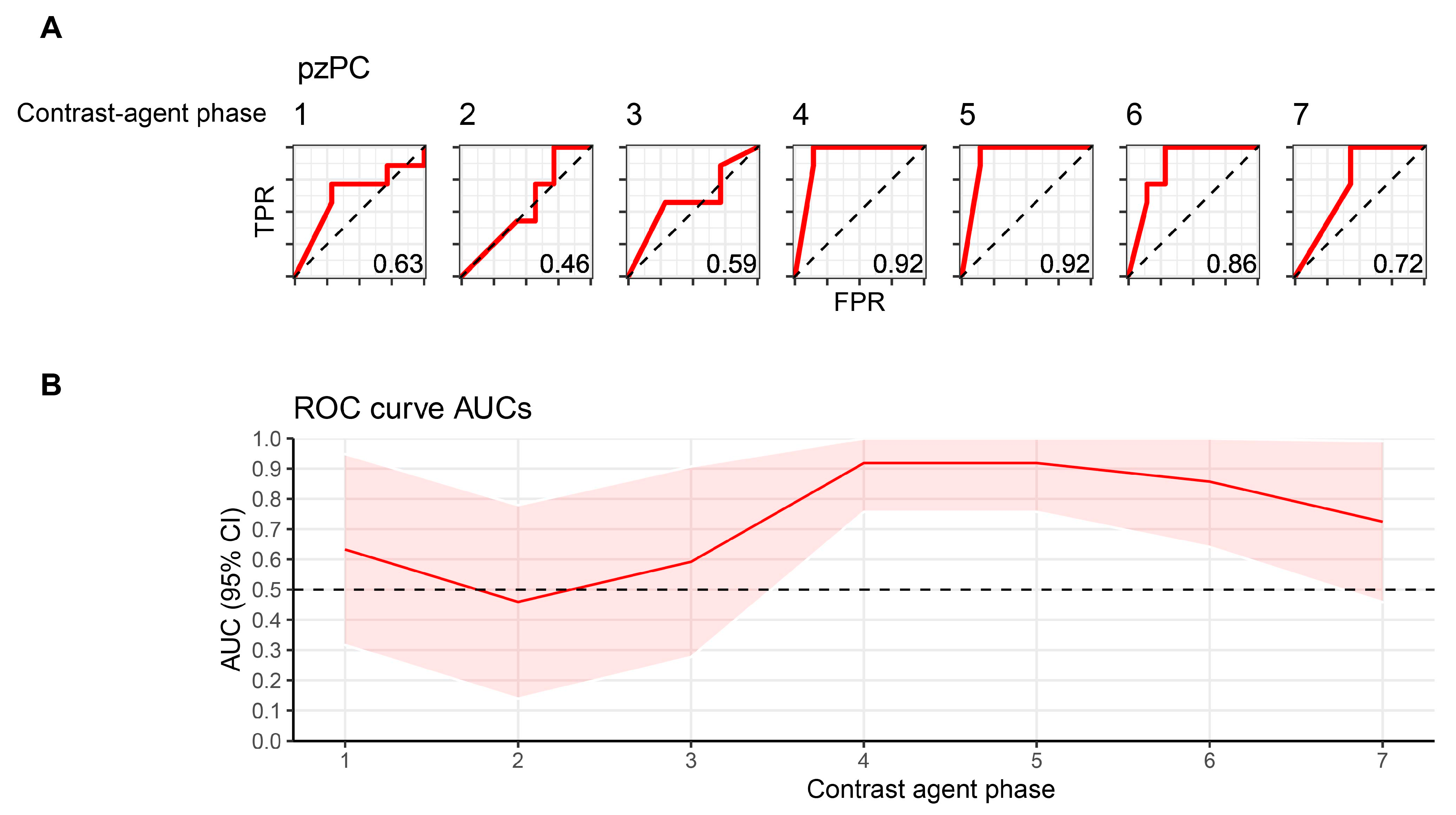
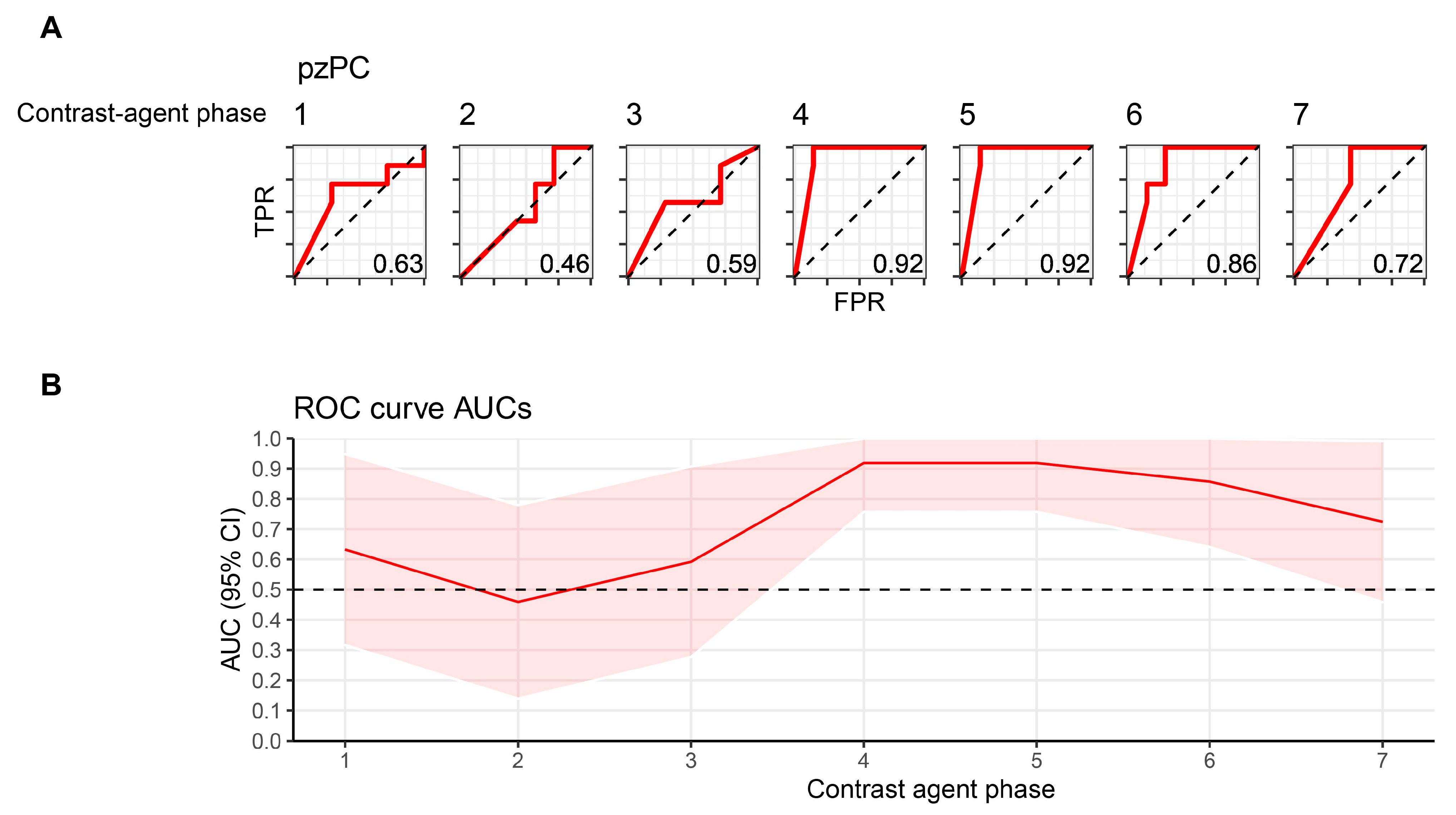
3.3. Machine-Learning-Based Classification of Healthy and Tumor ROIs Depends on Contrast Agent Phase
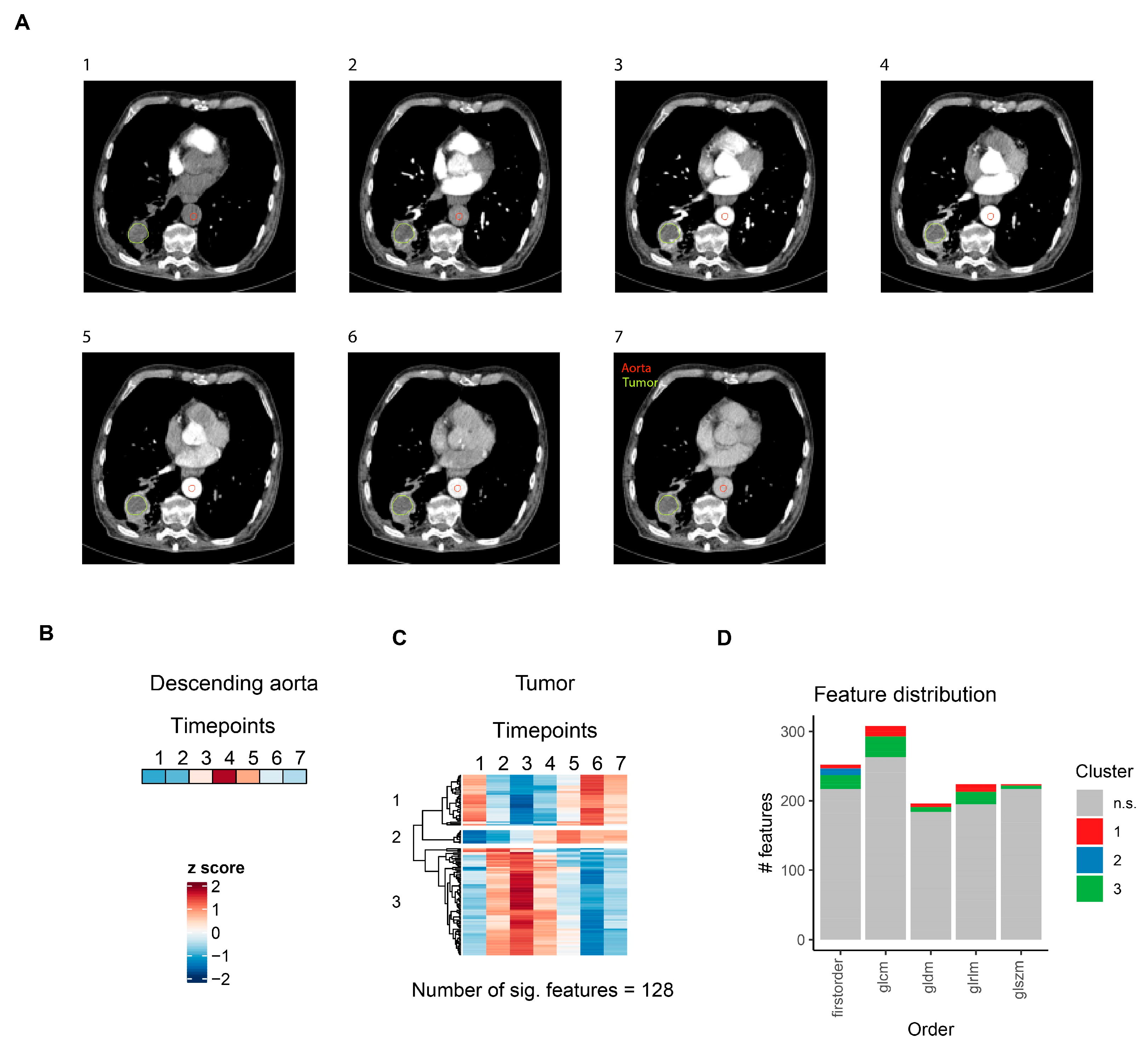
3.4. CT Radiomics Features Show Distinct Contrast Agent Dynamics in Lung Cancer
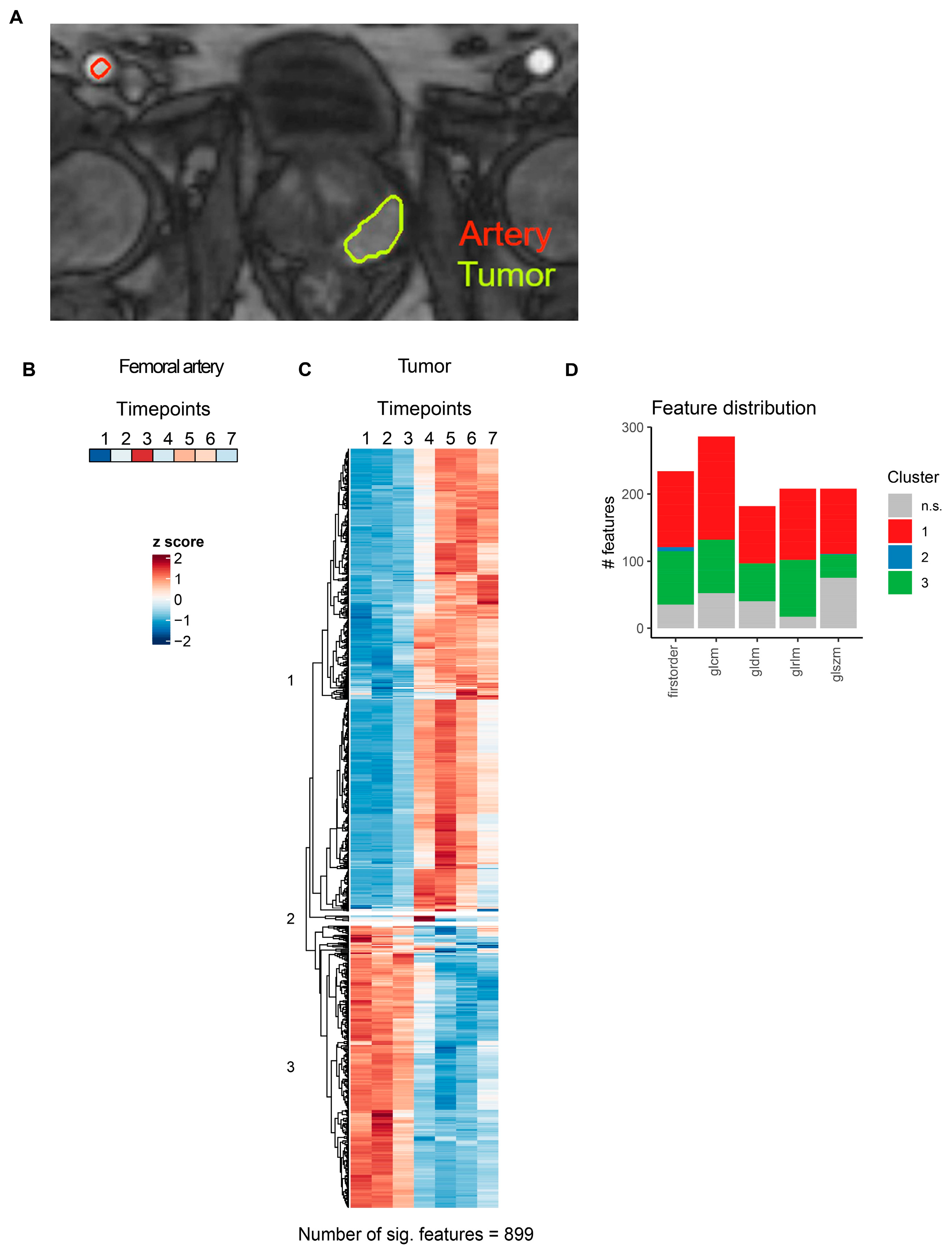
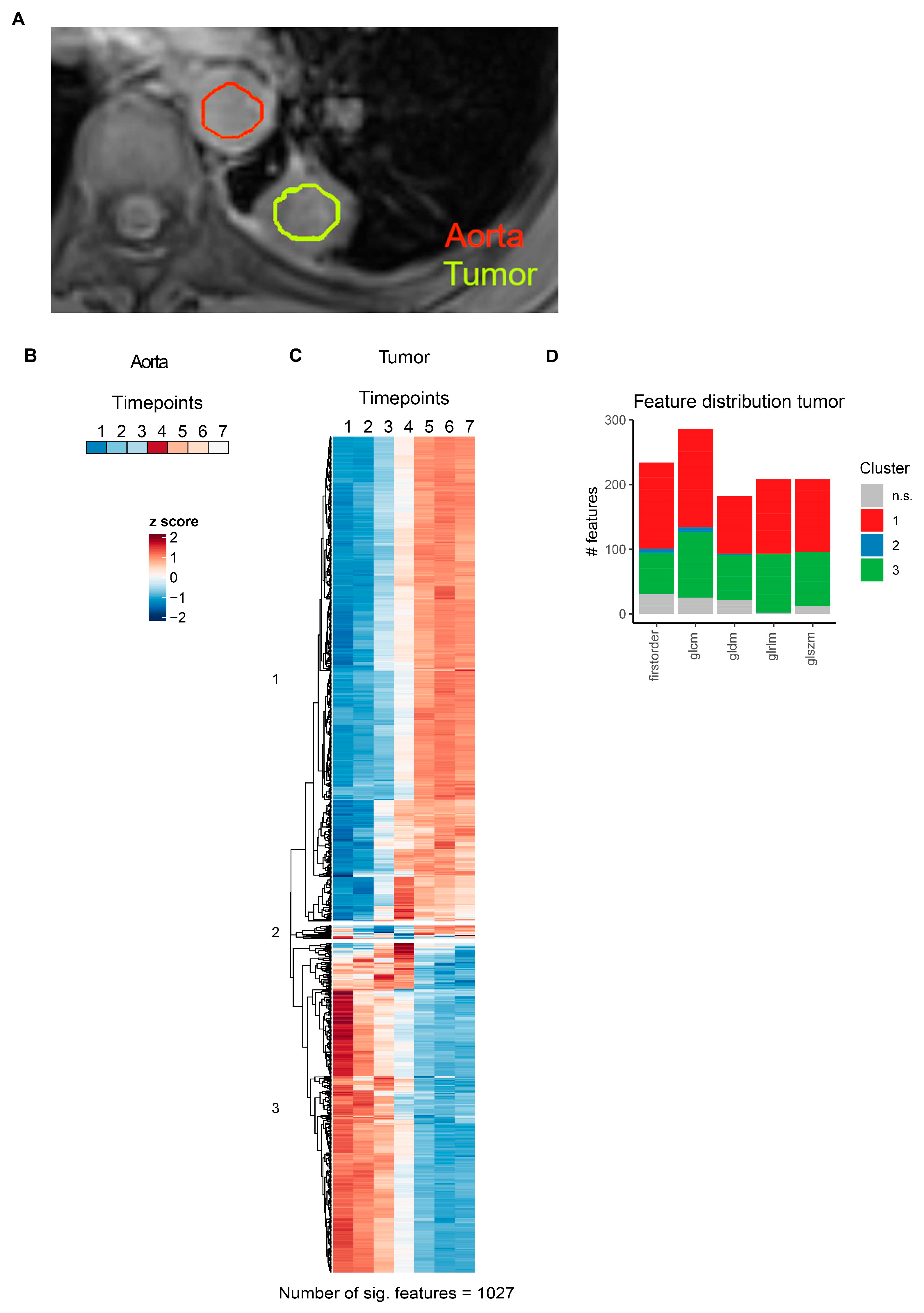
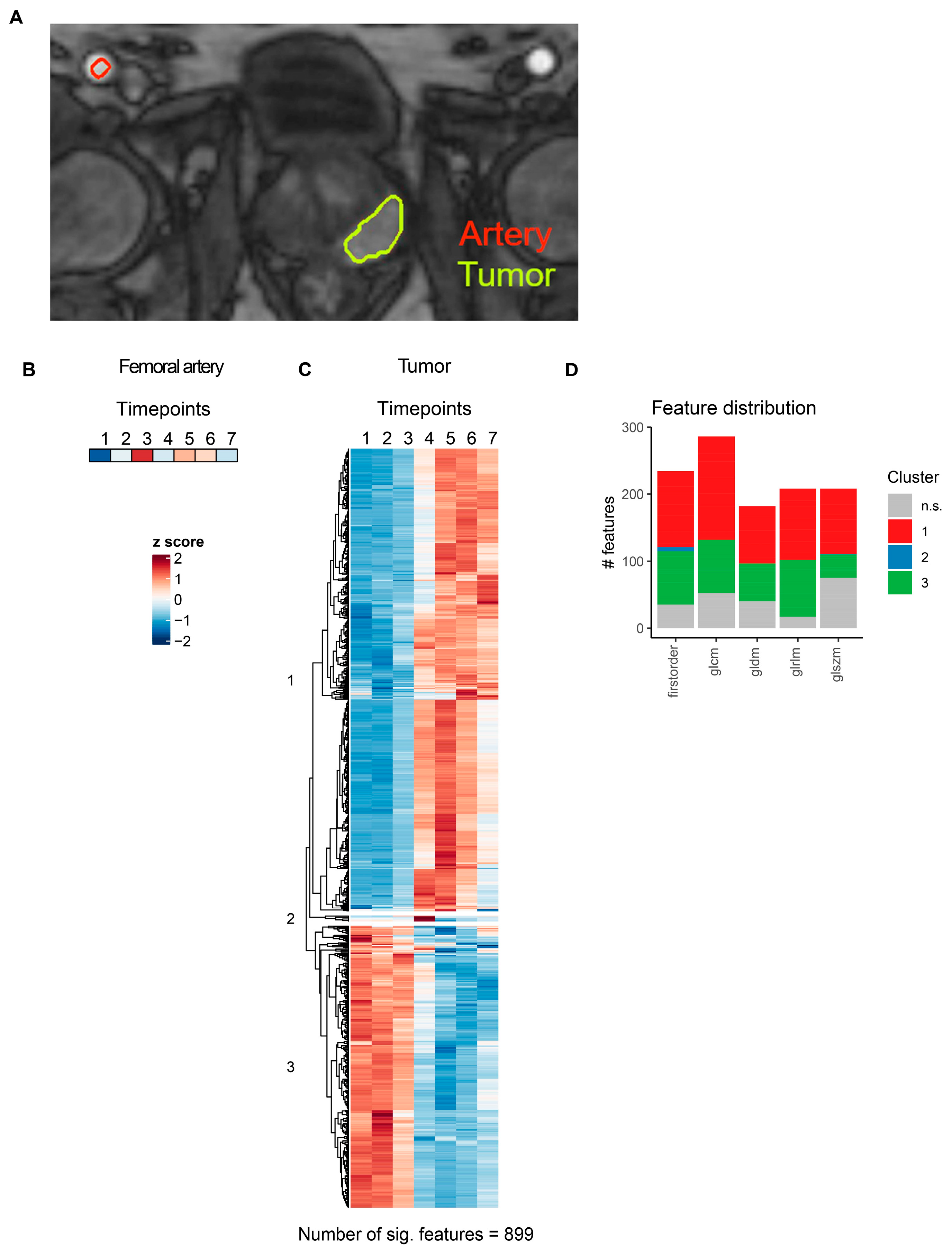
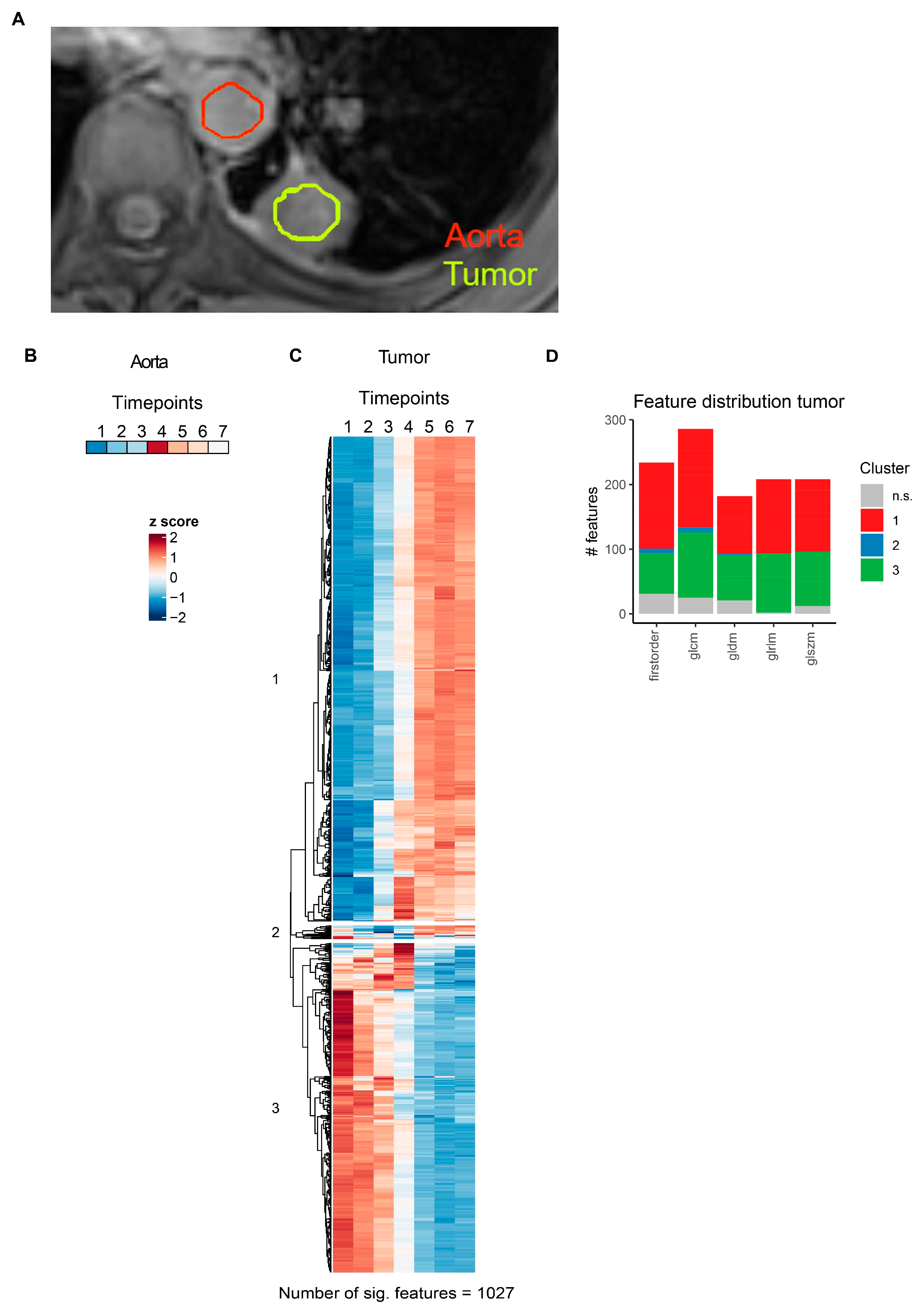
3.5. Contrast Agent Application Induces Drastic Changes in MRI Radiomics Features in pzPC and NSCLC Tumors
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CT | Computed tomography |
| dceCT | Dynamic contrast-enhanced CT |
| dceMRI | Dynamic contrast-enhanced MRI |
| FDR | False discovery rate |
| GLCM | Gray level co-occurrence matrix |
| GLDM | Gray level dependence matrix |
| GLRLM | Gray level run length matrix |
| GLSZM | Gray level size zone matrix |
| i.v. | Intravenous |
| kVp | Kilovolt pascal |
| LoG | Laplacian of Gaussian |
| mL | Mililiter |
| MRI | Magnetic resonance imaging |
| NSCLC | Non-small cell lung cancer |
| PI-RADS | Prostate Imaging-Reporting and Data System |
| pzPC | Peripheral zone prostate cancer |
| ROC | Receiver-operator-characteristics |
| ROI | Region-of-interest |
References
- Lambin, P.; Rios-Velazquez, E.; Leijenaar, R.; Carvalho, S.; van Stiphout, R.G.; Granton, P.; Zegers, C.M.; Gillies, R.; Boellard, R.; Dekker, A.; et al. Radiomics: Extracting more information from medical images using advanced feature analysis. Eur. J. Cancer 2012, 48, 441–446. [Google Scholar] [CrossRef] [PubMed]
- Dinis Fernandes, C.; Schaap, A.; Kant, J.; van Houdt, P.; Wijkstra, H.; Bekers, E.; Linder, S.; Bergman, A.M.; van der Heide, U.; Mischi, M.; et al. Radiogenomics Analysis Linking Multiparametric MRI and Transcriptomics in Prostate Cancer. Cancers 2023, 15, 3074. [Google Scholar] [CrossRef] [PubMed]
- Nicoletti, G.; Mazzetti, S.; Maimone, G.; Cignini, V.; Cuocolo, R.; Faletti, R.; Gatti, M.; Imbriaco, M.; Longo, N.; Ponsiglione, A.; et al. Development and Validation of an Explainable Radiomics Model to Predict High-Aggressive Prostate Cancer: A Multicenter Radiomics Study Based on Biparametric MRI. Cancers 2024, 16, 203. [Google Scholar] [CrossRef] [PubMed]
- Coroller, T.P.; Agrawal, V.; Huynh, E.; Narayan, V.; Lee, S.W.; Mak, R.H.; Aerts, H. Radiomic-Based Pathological Response Prediction from Primary Tumors and Lymph Nodes in NSCLC. J. Thorac. Oncol. 2017, 12, 467–476. [Google Scholar] [CrossRef] [PubMed]
- Ligero, M.; Garcia-Ruiz, A.; Viaplana, C.; Villacampa, G.; Raciti, M.V.; Landa, J.; Matos, I.; Martin-Liberal, J.; Ochoa-de-Olza, M.; Hierro, C.; et al. A CT-based Radiomics Signature Is Associated with Response to Immune Checkpoint Inhibitors in Advanced Solid Tumors. Radiology 2021, 299, 109–119. [Google Scholar] [CrossRef] [PubMed]
- Martin, A.; Marcelin, C.; Petitpierre, F.; Jambon, E.; Maaloum, R.; Grenier, N.; Le Bras, Y.; Crombe, A. Clinical, Technical, and MRI Features Associated with Patients’ Outcome at 3 Months and 2 Years following Prostate Artery Embolization: Is There an Added Value of Radiomics? J. Pers. Med. 2024, 14, 67. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.W.; Chao, H.S.; Chiu, H.Y.; Lin, Y.H.; Chen, H.C.; Lu, C.F.; Liao, C.Y.; Lee, Y.; Shiao, T.H.; Chen, Y.M.; et al. Evaluating the Potential of Delta Radiomics for Assessing Tyrosine Kinase Inhibitor Treatment Response in Non-Small Cell Lung Cancer Patients. Cancers 2023, 15, 5125. [Google Scholar] [CrossRef] [PubMed]
- Zhao, B. Understanding Sources of Variation to Improve the Reproducibility of Radiomics. Front. Oncol. 2021, 11, 633176. [Google Scholar] [CrossRef] [PubMed]
- Jha, A.K.; Mithun, S.; Jaiswar, V.; Sherkhane, U.B.; Purandare, N.C.; Prabhash, K.; Rangarajan, V.; Dekker, A.; Wee, L.; Traverso, A. Repeatability and reproducibility study of radiomic features on a phantom and human cohort. Sci. Rep. 2021, 11, 2055. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Lu, B.; Yang, X.; Lan, D.; Lin, S.; Zhou, Z.; Li, K.; Deng, D.; Peng, P.; Zeng, Z.; et al. Prognostic analysis and risk stratification of lung adenocarcinoma undergoing EGFR-TKI therapy with time-serial CT-based radiomics signature. Eur. Radiol. 2023, 33, 825–835. [Google Scholar] [CrossRef]
- Johnson, D.Y.; Farjat, A.E.; Vernuccio, F.; Hurwitz, L.M.; Nelson, R.C.; Marin, D. Evaluation of Intraindividual Contrast Enhancement Variability for Determining the Maximum Achievable Consistency in CT. AJR Am. J. Roentgenol. 2020, 214, 18–23. [Google Scholar] [CrossRef] [PubMed]
- Sakai, S.; Yabuuchi, H.; Chishaki, A.; Okafuji, T.; Matsuo, Y.; Kamitani, T.; Setoguchi, T.; Honda, H. Effect of cardiac function on aortic peak time and peak enhancement during coronary CT angiography. Eur. J. Radiol. 2010, 75, 173–177. [Google Scholar] [CrossRef] [PubMed]
- van Timmeren, J.E.; Cester, D.; Tanadini-Lang, S.; Alkadhi, H.; Baessler, B. Radiomics in medical imaging-“how-to” guide and critical reflection. Insights Into Imaging 2020, 11, 91. [Google Scholar] [CrossRef] [PubMed]
- Shur, J.D.; Doran, S.J.; Kumar, S.; Ap Dafydd, D.; Downey, K.; O‘Connor, J.P.B.; Papanikolaou, N.; Messiou, C.; Koh, D.M.; Orton, M.R. Radiomics in Oncology: A Practical Guide. Radiogr. A Rev. Publ. Radiol. Soc. N. Am. Inc. 2021, 41, 1717–1732. [Google Scholar] [CrossRef] [PubMed]
- Beer, L.; Polanec, S.H.; Baltzer, P.A.T.; Schatzl, G.; Georg, D.; Schestak, C.; Dutschke, A.; Herrmann, H.; Mazal, P.; Brendel, A.K.; et al. 4D perfusion CT of prostate cancer for image-guided radiotherapy planning: A proof of concept study. PLoS ONE 2019, 14, e0225673. [Google Scholar] [CrossRef] [PubMed]
- Ohno, Y.; Koyama, H.; Matsumoto, K.; Onishi, Y.; Takenaka, D.; Fujisawa, Y.; Yoshikawa, T.; Konishi, M.; Maniwa, Y.; Nishimura, Y.; et al. Differentiation of malignant and benign pulmonary nodules with quantitative first-pass 320-detector row perfusion CT versus FDG PET/CT. Radiology 2011, 258, 599–609. [Google Scholar] [CrossRef] [PubMed]
- van Griethuysen, J.J.M.; Fedorov, A.; Parmar, C.; Hosny, A.; Aucoin, N.; Narayan, V.; Beets-Tan, R.G.H.; Fillion-Robin, J.C.; Pieper, S.; Aerts, H. Computational Radiomics System to Decode the Radiographic Phenotype. Cancer Res. 2017, 77, e104–e107. [Google Scholar] [CrossRef] [PubMed]
- Benjamini, Y.; Hochberg, Y. Controlling the False Discovery Rate: A Practical and Powerful Approach to Multiple Testing. J. R. Stat. Soc. Ser. B Methodol. 1995, 57, 289–300. [Google Scholar]
- Polanec, S.H.; Bickel, H.; Wengert, G.J.; Arnoldner, M.; Clauser, P.; Susani, M.; Shariat, S.F.; Pinker, K.; Helbich, T.H.; Baltzer, P.A.T. Can the addition of clinical information improve the accuracy of PI-RADS version 2 for the diagnosis of clinically significant prostate cancer in positive MRI? Clin. Radiol. 2020, 75, 157.E1–157.E7. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Steinmann, A.; Ding, Y.; Lee, H.; Owens, C.; Wang, J.; Yang, J.; Followill, D.; Ger, R.; MacKin, D.; et al. Radiomics feature robustness as measured using an MRI phantom. Sci. Rep. 2021, 11, 3973. [Google Scholar] [CrossRef] [PubMed]
- Prayer, F.; Hofmanninger, J.; Weber, M.; Kifjak, D.; Willenpart, A.; Pan, J.; Rohrich, S.; Langs, G.; Prosch, H. Variability of computed tomography radiomics features of fibrosing interstitial lung disease: A test-retest study. Methods 2021, 188, 98–104. [Google Scholar] [CrossRef] [PubMed]
- van Timmeren, J.E.; Leijenaar, R.T.H.; van Elmpt, W.; Wang, J.; Zhang, Z.; Dekker, A.; Lambin, P. Test-Retest Data for Radiomics Feature Stability Analysis: Generalizable or Study-Specific? Tomography 2016, 2, 361–365. [Google Scholar] [CrossRef] [PubMed]
- Escudero Sanchez, L.; Rundo, L.; Gill, A.B.; Hoare, M.; Mendes Serrao, E.; Sala, E. Robustness of radiomic features in CT images with different slice thickness, comparing liver tumour and muscle. Sci. Rep. 2021, 11, 8262. [Google Scholar] [CrossRef] [PubMed]
- Zhao, B.; Tan, Y.; Tsai, W.Y.; Qi, J.; Xie, C.; Lu, L.; Schwartz, L.H. Reproducibility of radiomics for deciphering tumor phenotype with imaging. Sci. Rep. 2016, 6, 23428. [Google Scholar] [CrossRef] [PubMed]
- Guo, L.; Du, S.; Gao, S.; Zhao, R.; Huang, G.; Jin, F.; Teng, Y.; Zhang, L. Delta-Radiomics Based on Dynamic Contrast-Enhanced MRI Predicts Pathologic Complete Response in Breast Cancer Patients Treated with Neoadjuvant Chemotherapy. Cancers 2022, 14, 3515. [Google Scholar] [CrossRef] [PubMed]
- Pesapane, F.; Rotili, A.; Agazzi, G.M.; Botta, F.; Raimondi, S.; Penco, S.; Dominelli, V.; Cremonesi, M.; Jereczek-Fossa, B.A.; Carrafiello, G.; et al. Recent Radiomics Advancements in Breast Cancer: Lessons and Pitfalls for the Next Future. Curr. Oncol. 2021, 28, 2351–2372. [Google Scholar] [CrossRef] [PubMed]
- Miceli, V.; Gennarini, M.; Tomao, F.; Cupertino, A.; Lombardo, D.; Palaia, I.; Curti, F.; Riccardi, S.; Ninkova, R.; Maccioni, F.; et al. Imaging of Peritoneal Carcinomatosis in Advanced Ovarian Cancer: CT, MRI, Radiomic Features and Resectability Criteria. Cancers 2023, 15, 5827. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ID | Age (Years) | Tumor Location | PI-RADS | Gleason Score | Number of CT Scans | Number of MRI Scans |
|---|---|---|---|---|---|---|
| 1 | 78 | Left peripheral zone | 5 | 3 + 4 | 26 | 70 |
| 2 | 75 | Left peripheral zone | 4 | 3 + 3 | 33 | 70 |
| 3 | 64 | Left peripheral zone | 4 | 3 + 4 | 26 | 21 |
| 4 | 57 | Right peripheral zone | 4 | 3 + 3 | 26 | No MRI included |
| 5 | 76 | Left peripheral zone | 4 | 3 + 4 | 33 | 70 |
| 6 | 71 | Left peripheral zone | 4 | 4 + 3 | 26 | No MRI included |
| 7 | 57 | Left peripheral zone | 4 | 3 + 3 | 26 | No MRI included |
| 8 | 76 | Right peripheral zone | 4 | 3 + 4 | No CT included | 70 |
| 9 | 63 | Left peripheral zone | 4 | 3 + 3 | No CT included | 70 |
| 10 | 84 | Left peripheral zone | 4 | 3 + 3 | No CT included | 70 |
| 11 | 58 | Right peripheral zone | 4 | 3 + 3 | No CT included | 70 |
| 12 | 63 | Right peripheral zone | 4 | 4 + 3 | No CT included | 70 |
| ID | Age (Years) | Sex | Histology | Target Lesion | Stage | Number of CT Scans |
|---|---|---|---|---|---|---|
| 1 | 70 | Male | Squamous cell carcinoma | Primary tumor | IV | 20 |
| 2 | 77 | Male | Squamous cell carcinoma | Primary tumor | IV | 30 |
| 3 | 74 | Female | Adenocarcinoma | Primary tumor | IV | 20 |
| 4 | 61 | Male | Squamous cell carcinoma | Lymph node metastasis | IV | 30 |
| 5 | 60 | Male | Adenocarcinoma | Lymph node metastasis | IV | 20 |
| 6 | 67 | Male | Squamous cell carcinoma | Primary tumor | III | 30 |
| 7 | 81 | Male | Squamous cell carcinoma | Lymph node metastasis | IV | 30 |
| ID | Age (Years) | Sex | Histology | Target Lesion | Stage | Number of Visits | Number of Scans |
|---|---|---|---|---|---|---|---|
| 1 | 55 | Male | Squamous cell carcinoma | Primary tumor | IV | 5 | 60–78 per visit |
| 2 | 76 | Male | Squamous cell carcinoma | Primary tumor | IV | 2 | 76 per visit |
| 3 | 43 | Female | Adenocarcinoma | Primary tumor | IV | 2 | 76 per visit |
| 4 | 76 | Male | Adenocarcinoma | Primary tumor | IV | 2 | 76 per visit |
| 5 | 66 | Female | Squamous cell carcinoma | Primary tumor | IV | 1 | 76 |
| 6 | 64 | Male | Squamous cell carcinoma | Primary tumor | IV | 2 | 74–76 per visit |
| 7 | 70 | Male | Adenocarcinoma | Primary tumor | IV | 1 | 76 |
| 8 | 55 | Female | Squamous cell carcinoma | Primary tumor | IV | 2 | 76–78 per visit |
| 9 | 67 | Male | Squamous cell carcinoma | Primary tumor | IV | 1 | 16 |
| 10 | 54 | Male | Squamous cell carcinoma | Primary tumor | IV | 1 | 76 |
| 11 | 74 | Male | Adenocarcinoma | Primary tumor | IV | 3 | 70–76 per visit |
| 12 | 56 | Male | Adenocarcinoma | Primary tumor | IV | 2 | 76 per visit |
| 13 | 69 | Female | Adenocarcinoma | Primary tumor | IV | 2 | 76 per visit |
| 14 | 52 | Female | Squamous cell carcinoma | Primary tumor | IV | 3 | 76 per visit |
| 15 | 81 | Female | Adenocarcinoma | Primary tumor | IV | 1 | 76 |
| 16 | 54 | Male | Adenocarcinoma | Primary tumor | IV | 1 | 76 |
| 17 | 64 | Male | Squamous cell carcinoma | Primary tumor | IV | 1 | 76 |
| 18 | 68 | Female | Squamous cell carcinoma | Primary tumor | IV | 1 | 76 |
| 19 | 50 | Female | Adenocarcinoma | Primary tumor | IV | 1 | 70 |
| 20 | 74 | Male | Adenocarcinoma | Primary tumor | IV | 1 | 76 |
| 21 | 60 | Female | Squamous cell carcinoma | Primary tumor | IV | 1 | 76 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Watzenboeck, M.L.; Beer, L.; Kifjak, D.; Röhrich, S.; Heidinger, B.H.; Prayer, F.; Milos, R.-I.; Apfaltrer, P.; Langs, G.; Baltzer, P.A.T.; et al. Contrast Agent Dynamics Determine Radiomics Profiles in Oncologic Imaging. Cancers 2024, 16, 1519. https://doi.org/10.3390/cancers16081519
Watzenboeck ML, Beer L, Kifjak D, Röhrich S, Heidinger BH, Prayer F, Milos R-I, Apfaltrer P, Langs G, Baltzer PAT, et al. Contrast Agent Dynamics Determine Radiomics Profiles in Oncologic Imaging. Cancers. 2024; 16(8):1519. https://doi.org/10.3390/cancers16081519
Chicago/Turabian StyleWatzenboeck, Martin L., Lucian Beer, Daria Kifjak, Sebastian Röhrich, Benedikt H. Heidinger, Florian Prayer, Ruxandra-Iulia Milos, Paul Apfaltrer, Georg Langs, Pascal A. T. Baltzer, and et al. 2024. "Contrast Agent Dynamics Determine Radiomics Profiles in Oncologic Imaging" Cancers 16, no. 8: 1519. https://doi.org/10.3390/cancers16081519
APA StyleWatzenboeck, M. L., Beer, L., Kifjak, D., Röhrich, S., Heidinger, B. H., Prayer, F., Milos, R.-I., Apfaltrer, P., Langs, G., Baltzer, P. A. T., & Prosch, H. (2024). Contrast Agent Dynamics Determine Radiomics Profiles in Oncologic Imaging. Cancers, 16(8), 1519. https://doi.org/10.3390/cancers16081519