
Predictive Value of the Mayo Adhesive Probability (MAP) Score in Laparoscopic Partial Nephrectomies: A Systematic Review from the EAU Section of Uro-Technology (ESUT)


 ,
,  , ,
, ,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Selection Criteria and Data Extraction
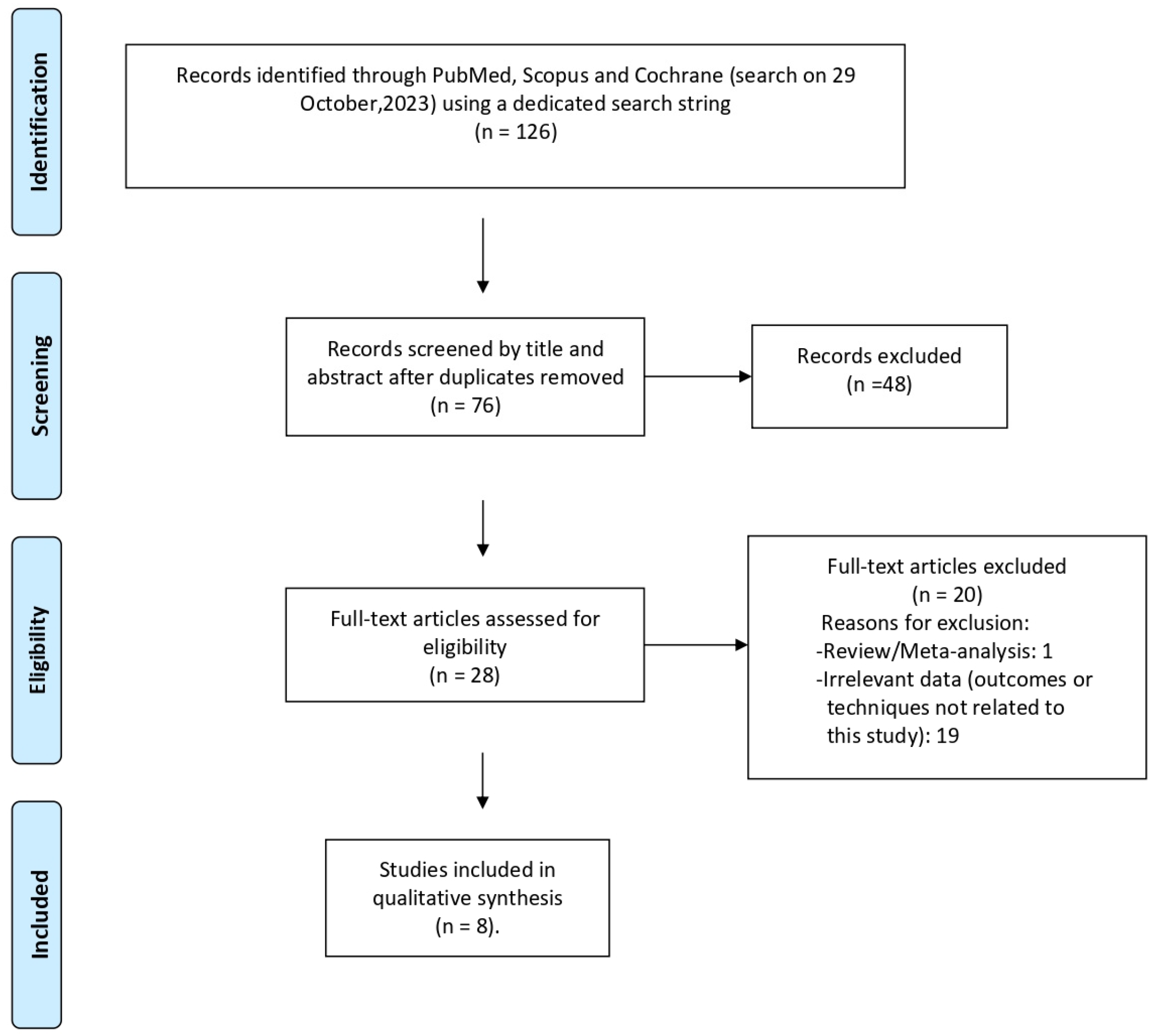
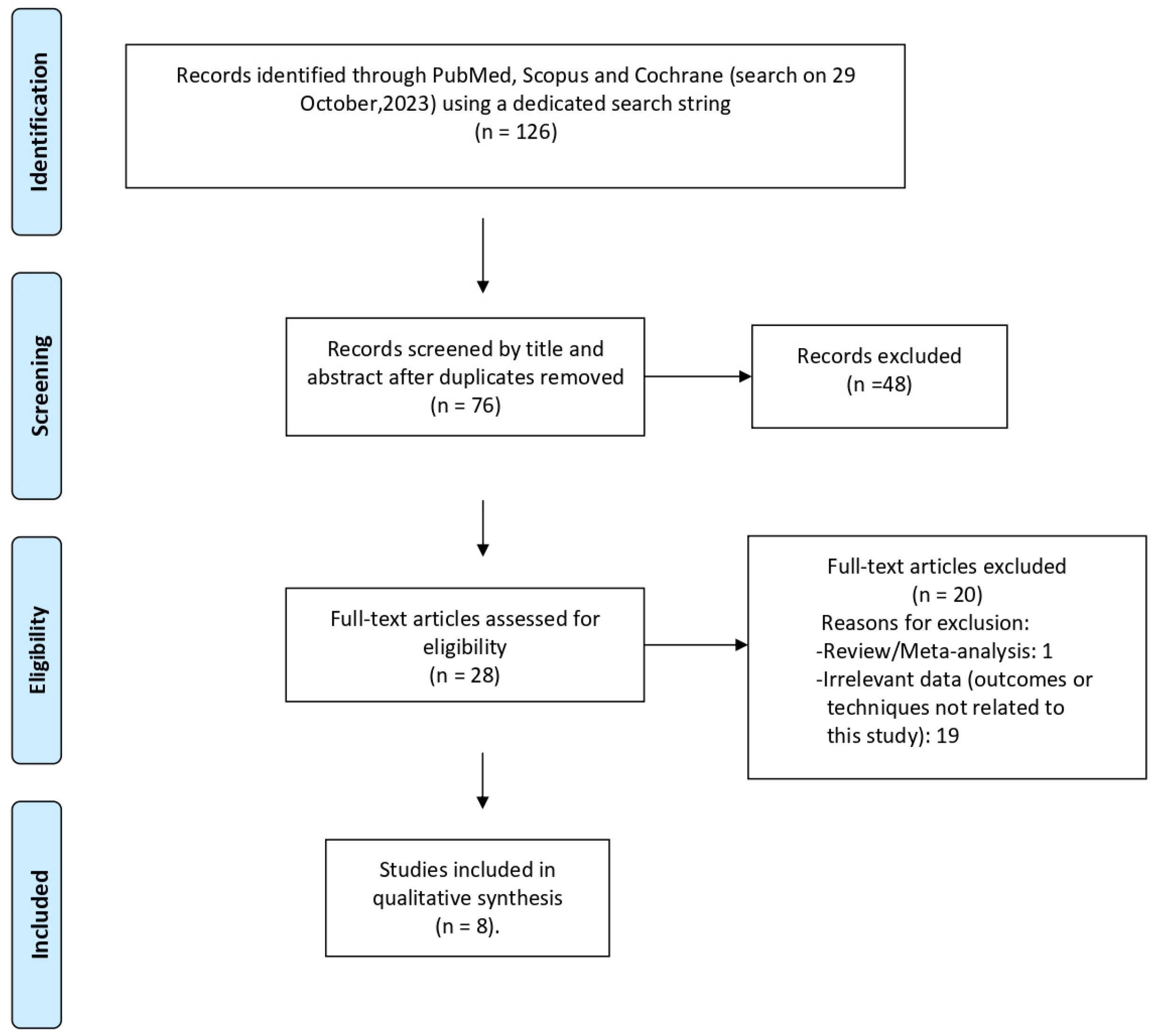
2.3. Article Selection
3. Results
3.1. Studies Characteristics
3.2. Patients’ Baseline Characteristics
3.3. Intraoperative and Postoperative Characteristics

{kind=link}
{kind=link}
{kind=link}
| Study Name | Gender | Age | BMI (kg/m2) | ASA | Tumor Size (cm) | Side | MAP | RNS | Pathol Ogical Stage | Fuhrman Grade |
|---|---|---|---|---|---|---|---|---|---|---|
| Yuanxin et al. (2019), [16] (median) | Male 58.7%, Female 41.3% (MAP ≤ 2), Male 88.4%, Female 11.6% (MAP ≥ 3) | 51 (43–60) (MAP ≤ 2), 54 (48–62) (MAP ≥ 3) | 25.0 (23.0–26.8) (MAP ≤ 2), 26.2 (24.7–29.4) (MAP ≥ 3) | ≤2 97.1%, >2 2.9% (MAP ≤ 2), ≤2 93.2%, >2 6.8% (MAP ≥ 3) | 2.5 (2–3) (MAP ≤ 2), 2.5 (2–3.2) (MAP ≥ 3) | Left 39.5%, right 60.5% (MAP ≤ 2), left 40.4%, right 59.6% (MAP ≥ 3) | 54.1% (MAP ≤ 2), 45.9% (MAP ≥ 3) | 6 (5–8) (MAP ≤ 2), 6 (6–8) (MAP ≥ 3) | T1a 93.0%, T1b 5.8%, ≥T2 1.2% (MAP ≤ 2), T1a 95.2%, T1b 2.1%, ≥T2 2.7% (MAP ≥ 3) | 1–2 95.6%, 3–4 (4.4%) (MAP ≤ 2), 1–2 90.6%, 3–4 (9.4%) (MAP ≥ 3) |
| Bier et al. (2017), [17] (mean) | Male 62%, Female 38% | 61.7± 12.7 | NA | NA | NA | Left 53.9%, right 46.1% | 66% (MAP ≤ 2), 34% (MAP ≥ 3) | 4–6 69%, 7–9 29%, >9 2% | pT1a 74.8%, pT1b 15.4%, pT2 0.5%, 9.1% pT3a (only RCCs) | NA |
| Fang et al. (2021), [18] (mean) | Male 64.7%, Female 35.3% | 57.1 ± 13.4 | 24.1 ± 3.7 | NA | 3.7 ± 1.5 | Left 48.8%, right 51.2% | 2.0 (0.0, 3.0) median | 6.0 (6.0, 8.0) median | pT1a 60.9%, pT1b 30.2%, pT2a 2.8%, ≥pT3 6.1% | I 7.5%, II 75.9%, III 16.6%, IV 0.0% |
| Yang et al. (2020), [19] (median) | Male 29.6%, Female 70.4% | 52 (45–61) | 25.1 (22.9–27.2) | Score 1 22.0%, Score 2 73.0%, Score 3 5.0% | 29.4 (21.5–36.0) mm | NA | 1 (0–3) | 8 (6–9) | T1a 83.6%, T1b 16.4% | NA |
| Jin et al. (2019), [20] (mean) | Male 64.1%, Female 35.9% | 54.8 ± 11.9 | 27.6 ± 5.2 | 1–2 61.4%, 3–4 48.6% | 3.4 ± 0.5 | Right 44.6%, left 55.4% | 2.08 (IQR 1–3) median | 7.06 (IQR 5–9) median | NA | NA |
| Tan et al. (2021), [21] (mean) | Female 36.3%, Male 63.7% | 55.1 ± 11.3 | 25.2 ± 4.4 | 1–2 65.9%, 3–4 34.1% | 3.4± 1.5 | Right 44.7%, left 55.3% | 2.04 (IQR, 0–3) median | 6.15 (IQR, 5–8) | pT1a 71.3%, pT1b 27.4%, pT2 1.3% | NA |
| Qian et al. (2019), [22] (mean) | Male 67.6%, Female 32.4% | 54.8 ± 12.7 | 23.0 ± 1.74 | NA | 3.52 ± 1.48 | NA | 2 (0–5) median | 6 (4–11) median | pT1a 70.7%, pT1B 29.3% | NA |
| Hata et al. (2021), [23] (mean) | Male 68.3%, Female 31.7% (non-deterioration), Male 73.0%, Female 27.0% (deterioration) | 65.5 ± 11.1 (non-deterioration), 66.8 ± 11.5 (deterioration) | 24.3 ± 3.81 (non-deterioration), 24.4 ± 2.69 (deterioration) | NA | 25.9 ± 11.5 (non-deterioration), 22.3 ± 9.06 (deterioration) mm | Right 58.5%, left 41.5% (non-deterioration), right 54.1%, left 32.4% (deterioration) | 2.0 ± 1.7 (non-deterioration), 2.0 ± 1.9 (deterioration) tumor side, 1.4 ± 1.7 (non-deterioration), 2.5 ± 1.8 (non-deterioration) unaffected side. | 5.7 ± 1.5 (non-deterioration), 5.6 ± 1.7 (deterioration) | NA | NA |
4. Discussion
4.1. Association of MAP Score with Intraoperative Characteristics
4.2. Association of MAP Score with Postoperative Characteristics
4.3. Combination of MAP Score with Other Scores
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Ljungberg, B.; Albiges, L.; Abu-Ghanem, Y.; Bedke, J.; Capitanio, U.; Dabestani, S.; Fernández-Pello, S.; Giles, R.H.; Hofmann, F.; Hora, M.; et al. European Association of Urology Guidelines on Renal Cell Carcinoma: The 2022 Update. Eur. Urol. 2022, 82, 399–410. [Google Scholar] [CrossRef] [PubMed]
- Gill, I.S.; Kavoussi, L.R.; Lane, B.R.; Blute, M.L.; Babineau, D.; Colombo, J.R., Jr.; Frank, I.; Permpongkosol, S.; Weight, C.J.; Kaouk, J.H.; et al. Comparison of 1800 laparoscopic and open partial nephrectomies for single renal tumors. J. Urol. 2007, 178, 41–46. [Google Scholar] [CrossRef] [PubMed]
- You, C.; Du, Y.; Wang, H.; Peng, L.; Wei, T.; Zhang, X.; Li, X.; Wang, A. Laparoscopic Versus Open Partial Nephrectomy: A Systemic Review and Meta-Analysis of Surgical, Oncological, and Functional Outcomes. Front. Oncol. 2020, 10, 583979. [Google Scholar] [CrossRef] [PubMed]
- Hou, W.; Yan, W.; Ji, Z. Anatomic features involved in technical complexity of partial nephrectomy. Urology 2015, 85, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Kutikov, A.; Uzzo, R.G. The RENAL nephrometry score: A comprehensive standardized system for quantitating renal tumor size, location and depth. J. Urol. 2009, 182, 844–853. [Google Scholar] [CrossRef]
- Borregales, L.D.; Adibi, M.; Thomas, A.Z.; Reis, R.B.; Chery, L.J.; Devine, C.E.; Wang, X.; Potretzke, A.M.; Potretzke, T.; Figenshau, R.S.; et al. Predicting Adherent Perinephric Fat Using Preoperative Clinical and Radiological Factors in Patients Undergoing Partial Nephrectomy. Eur. Urol. Focus 2021, 7, 397–403. [Google Scholar] [CrossRef] [PubMed]
- Gorin, M.A.; Mullins, J.K.; Pierorazio, P.M.; Jayram, G.; Allaf, M.E. Increased intra-abdominal fat predicts perioperative complications following minimally invasive partial nephrectomy. Urology 2013, 81, 1225–1230. [Google Scholar] [CrossRef] [PubMed]
- Bylund, J.R.; Qiong, H.; Crispen, P.L.; Venkatesh, R.; Strup, S.E. Association of clinical and radiographic features with perinephric “sticky” fat. J. Endourol. 2013, 27, 370–373. [Google Scholar] [CrossRef]
- Khene, Z.E.; Peyronnet, B.; Mathieu, R.; Fardoun, T.; Verhoest, G.; Bensalah, K. Analysis of the impact of adherent perirenal fat on peri-operative outcomes of robotic partial nephrectomy. World J. Urol. 2015, 33, 1801–1806. [Google Scholar] [CrossRef]
- Kocher, N.J.; Kunchala, S.; Reynolds, C.; Lehman, E.; Nie, S.; Raman, J.D. Adherent perinephric fat at minimally invasive partial nephrectomy is associated with adverse peri-operative outcomes and malignant renal histology. BJU Int. 2016, 117, 636–641. [Google Scholar] [CrossRef]
- Davidiuk, A.J.; Parker, A.S.; Thomas, C.S.; Leibovich, B.C.; Castle, E.P.; Heckman, M.G.; Custer, K.; Thiel, D.D. Mayo adhesive probability score: An accurate image-based scoring system to predict adherent perinephric fat in partial nephrectomy. Eur. Urol. 2014, 66, 1165–1171. [Google Scholar] [CrossRef]
- Dariane, C.; Le Guilchet, T.; Hurel, S.; Audenet, F.; Beaugerie, A.; Badoual, C.; Tordjman, J.; Clément, K.; Urien, S.; Pietak, M.; et al. Prospective assessment and histological analysis of adherent perinephric fat in partial nephrectomies. Urol. Oncol. 2017, 35, 39.e9–39.e17. [Google Scholar] [CrossRef]
- Martin, L.; Rouviere, O.; Bezza, R.; Bailleux, J.; Abbas, F.; Schott-Pethelaz, A.M.; Ruffion, A.; Paparel, P. Mayo Adhesive Probability Score Is an Independent Computed Tomography Scan Predictor of Adherent Perinephric Fat in Open Partial Nephrectomy. Urology 2017, 103, 124–128. [Google Scholar] [CrossRef] [PubMed]
- Tomaszewski, J.J.; Smaldone, M.C.; Cung, B.; Li, T.; Mehrazin, R.; Kutikov, A.; Canter, D.J.; Viterbo, R.; Chen, D.Y.; Greenberg, R.E.; et al. Internal validation of the renal pelvic score: A novel marker of renal pelvic anatomy that predicts urine leak after partial nephrectomy. Urology 2014, 84, 351–357. [Google Scholar] [CrossRef]
- Clavien, P.A.; Barkun, J.; de Oliveira, M.L.; Vauthey, J.N.; Dindo, D.; Schulick, R.D.; de Santibañes, E.; Pekolj, J.; Slankamenac, K.; Bassi, C.; et al. The Clavien-Dindo classification of surgical complications: Five-year experience. Ann. Surg. 2009, 250, 187–196. [Google Scholar] [CrossRef]
- Yao, Y.; Xu, Y.; Gu, L.; Liu, K.; Li, P.; Xuan, Y.; Gao, Y.; Zhang, X. The Mayo Adhesive Probability Score Predicts Longer Dissection Time During Laparoscopic Partial Nephrectomy. J. Endourol. 2020, 34, 594–599. [Google Scholar] [CrossRef]
- Bier, S.; Aufderklamm, S.; Todenhöfer, T.; Kruck, S.; Schuster, K.; Rausch, S.; Othman, A.; Notohamiprodjo, M.; Nikolaou, K.; Schwentner, C.; et al. Prediction of Postoperative Risks in Laparoscopic Partial Nephrectomy Using RENAL, Mayo Adhesive Probability and Renal Pelvic Score. Anticancer Res. 2017, 37, 1369–1373. [Google Scholar] [CrossRef] [PubMed]
- Fang, L.; Li, H.; Zhang, T.; Liu, R.; Zhang, T.; Bi, L.; Xie, D.; Wang, Y.; Yu, D. Analysis of predictors of adherent perinephric fat and its impact on perioperative outcomes in laparoscopic partial nephrectomy: A retrospective case-control study. World J. Surg. Oncol. 2021, 19, 319. [Google Scholar] [CrossRef] [PubMed]
- Yang, B.; Ma, L.L.; Qiu, M.; Xia, H.Z.; He, W.; Meng, T.Y.; Lu, M.; Lu, J. A novel nephrometry scoring system for predicting peri-operative outcomes of retroperitoneal laparoscopic partial nephrectomy. Chin. Med. J. 2020, 133, 577–582. [Google Scholar] [CrossRef]
- Jin, D.; Zhang, J.; Zhang, Y.; Ren, D.; Xu, G.; Ge, C.; Wang, D.; Zhang, W. A Combination of the Mayo Adhesive Probability Score and the RENAL Score to Predict Intraoperative Complications in Small Renal Masses. Urol. Int. 2020, 104, 142–147. [Google Scholar] [CrossRef]
- Tan, X.; Jin, D.; Hu, J.; Zhang, W.; Zhou, Y.; Li, Y.; Zhang, Y.; Wu, J. Development of a simple nomogram to estimate risk for intraoperative complications before partial nephrectomy based on the Mayo Adhesive Probability score combined with the RENAL nephrometry score. Investig. Clin. Urol. 2021, 62, 455–461. [Google Scholar] [CrossRef] [PubMed]
- Qian, J.; Jiang, J.; Li, P.; Zhang, S.; Bao, M.; Qin, C.; Meng, X.; Shao, P.; Wang, Z. Factors Influencing the Feasibility of Segmental Artery Clamping During Retroperitoneal Laparoscopic Partial Nephrectomy. Urology 2019, 129, 92–97. [Google Scholar] [CrossRef] [PubMed]
- Hata, J.; Matsuoka, Y.; Onagi, A.; Honda-Takinami, R.; Matsuoka, K.; Sato, Y.; Akaihata, H.; Ogawa, S.; Kataoka, M.; Hosoi, T.; et al. Usefulness of the mayo adhesive probability score as a predictive factor for renal function deterioration after partial nephrectomy: A retrospective case-control study. Int. Urol. Nephrol. 2021, 53, 2281–2288. [Google Scholar] [CrossRef] [PubMed]
- Hayden, J.A.; van der Windt, D.A.; Cartwright, J.L.; Côté, P.; Bombardier, C. Assessing bias in studies of prognostic factors. Ann. Intern. Med. 2013, 158, 280–286. [Google Scholar] [CrossRef] [PubMed]
- Grooten, W.J.A.; Tseli, E.; Äng, B.O.; Boersma, K.; Stålnacke, B.M.; Gerdle, B.; Enthoven, P. Elaborating on the assessment of the risk of bias in prognostic studies in pain rehabilitation using QUIPS-aspects of interrater agreement. Diagn. Progn. Res. 2019, 3, 5. [Google Scholar] [CrossRef] [PubMed]
- Kawamura, N.; Saito, K.; Inoue, M.; Ito, M.; Kijima, T.; Yoshida, S.; Yokoyama, M.; Ishioka, J.; Matsuoka, Y.; Kihara, K.; et al. Adherent Perinephric Fat in Asian Patients: Predictors and Impact on Perioperative Outcomes of Partial Nephrectomy. Urol. Int. 2018, 101, 437–442. [Google Scholar] [CrossRef]
- Ishiyama, R.; Kondo, T.; Takagi, T.; Iizuka, J.; Kobayashi, H.; Omae, K.; Fukuda, H.; Ishihara, H.; Tanabe, K. Impact of the Mayo Adhesive Probability Score on the Complexity of Robot-Assisted Partial Nephrectomy. J. Endourol. 2018, 32, 928–933. [Google Scholar] [CrossRef]
| Study Name | Journal/Year | Type of Study | Number of Patients | Surgical Technique | Comparison * | Outcomes | Risk of Bias *** |
|---|---|---|---|---|---|---|---|
| Yuanxin et al. (2019), [16] | Journal of Endourology, 2019 | Retrospective | n = 318 | Transperitoneal/Retroperitoneal | No | OT, dissection time, WIT, EBL. | Low |
| Bier et al. (2017), [17] | Anticancer Research, 2017 | Retrospective | n = 280 | Not defined | Renal Pelvic Score, RENAL nephrometry score | OT, WIT, complications ** | Low |
| Fang et al. (2021), [18] | World Journal of Surgical Oncology, 2021 | Retrospective | n = 215 | Transperitoneal/Retroperitoneal | RENAL nephrometry score | Surgical approach, OT, WIT, EBL, transfusion, length of postoperative stay, complications **, surgical margin, renal capsule rupture. | Low |
| Yang et al. (2020), [19] | Chinese Medical Journal, 2020 | Retrospective | n = 159 | Retroperitoneal | RENAL nephrometry score, novel nephrometry score (RNP score) | OT, EBL, WIT, margins and complications ** | Low |
| Jin et al. (2019), [20] | Urologia Internationalis, 2019 | Retrospective | n = 293 | Retroperitoneal | RENAL nephrometry score | OT, WIT, EBL, complications ** | Low |
| Tan et al. (2021), [21] | Investigate and Clinical Urology, 2021 | Retrospective | n = 637 | Retroperitoneal | RENAL nephrometry score | Complications ** | Low |
| Qian et al. (2019), [22] | Laparoscopy and Robotics, 2019 | Retrospective | n = 225 | Retroperitoneal | RENAL nephrometry score | Feasibility of segmental artery clamping | Low |
| Hata et al. (2021), [23] | International Urology and Nephrology, 2021 | Retrospective | n = 78 | Transperitoneal/Retroperitoneal | No | Postoperative renal function deterioration | Low |
| Study Name | OT (min) | Dissection Time (min) | EBL (mL) | WIT (min) | PSM | Conversion | Hospital Stay (Days) | Complications * | Blood Transfusion |
|---|---|---|---|---|---|---|---|---|---|
| Yuanxin et al. (2019), [16] (median) | 110 (90–141) MAP score ≤ 2, 131 (110–158) MAP score ≥ 3 | 54 (43–74) MAP score ≤ 2, 71 (58–93) MAP score ≥ 3 | 20 (20–50) MAP score ≤ 2, 50 (20–50) MAP score ≥ 3 | 20 (15–27) MAP score ≤ 2, 21 (15–26) MAP score ≥ 3 | 1.2% MAP score ≤ 2, 0% MAP score ≥ 3 | 0% (radical or open) MAP score ≤ 2, 0.7% MAP score ≥ 3 | 4 (3–5) MAP score ≤ 2, 4 (3–5) MAP score ≥ 3 | ≤II 2.3% MAP score ≤ 2, >II 0% MAP score ≥ 3, ≤II 3.4% MAP score ≤ 2, >II 0% MAP score ≥ 3, | 1.2% MAP score ≤ 2, 0.7% MAP score ≥ 3 |
| Bier et al. (2017), [17] (mean) | 132.9 ± 48 | NA | NA | 14.5 ± 11 | 1.79% | NA | 7 ± 4 | I 0%, II 3.6%, III 9.4%, IV and V 0% | NA |
| Fang et al. (2021), [18] (mean) | 130.7 ± 41.0 | NA | 50.0 (30.0, 100.0) median | 14.3 ± 7.3 | 2.3% | NA | 8.0 (7.0, 9.0) median | I–II 29.8%, III–IV 1.8% | 3.3% |
| Yang et al. (2020), [19] (median) | 149 (116–186) | NA | 20 (10–50) | 25 (18–30) | 6.3% | NA | NA | I 34.0%, II 3.9%, III/IV 0% | NA |
| Jin et al. (2019), [20] (mean) | 104.6 ± 43.4 | NA | 202 ± 156 | 18.7 ± 5.5 | 1.4% | 4.7% (radical), 1.0% (open) | 5.8 ± 2.6 | I 0%, II 3.4%, III 6.1%, IV 1.0% | 7.5% |
| Tan et al. (2021), [21] (mean) | 111.3 ± 38.7 | NA | 157.6 ± 63.2 | 15.3 ± 6.1 | NA | 5.0% (radical or open) | 5.1 ± 2.8 | Overall postoperative complications 9.6% | 6.6% |
| Qian et al. (2019), [22] (mean) | 87.16 ± 10.59 segmental artery clamping, 92.29 ± 15.92 main artery clamping | NA | 214.63 ± 120.19 segmental artery clamping, 170.29 ± 99.93 main artery clamping | 27.16 ± 6.01 Segmental artery clamping 29.03 ± 6.28 main artery clamping | 0% | 0% (open or radical), 15.6% (main renal artery clamping) | NA | I 7.11%, II 6.66%, IIIa 3.1% | 6.66% |
| Hata et al. (2021), [23] (mean) | NA | NA | NA | NA | NA | NA | NA | NA | NA |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kallidonis, P.; Spinos, T.; Zondervan, P.; Nyirády, P.; Backhaus, M.R.; Micali, S.; Hruby, S.; Alvarez-Maestro, M.; Tatanis, V.; Liatsikos, E.; et al. Predictive Value of the Mayo Adhesive Probability (MAP) Score in Laparoscopic Partial Nephrectomies: A Systematic Review from the EAU Section of Uro-Technology (ESUT). Cancers 2024, 16, 1455. https://doi.org/10.3390/cancers16081455
Kallidonis P, Spinos T, Zondervan P, Nyirády P, Backhaus MR, Micali S, Hruby S, Alvarez-Maestro M, Tatanis V, Liatsikos E, et al. Predictive Value of the Mayo Adhesive Probability (MAP) Score in Laparoscopic Partial Nephrectomies: A Systematic Review from the EAU Section of Uro-Technology (ESUT). Cancers. 2024; 16(8):1455. https://doi.org/10.3390/cancers16081455
Chicago/Turabian StyleKallidonis, Panagiotis, Theodoros Spinos, Patricia Zondervan, Peter Nyirády, Miguel Ramírez Backhaus, Salvatore Micali, Stephan Hruby, Mario Alvarez-Maestro, Vasileios Tatanis, Evangelos Liatsikos, and et al. 2024. "Predictive Value of the Mayo Adhesive Probability (MAP) Score in Laparoscopic Partial Nephrectomies: A Systematic Review from the EAU Section of Uro-Technology (ESUT)" Cancers 16, no. 8: 1455. https://doi.org/10.3390/cancers16081455
APA StyleKallidonis, P., Spinos, T., Zondervan, P., Nyirády, P., Backhaus, M. R., Micali, S., Hruby, S., Alvarez-Maestro, M., Tatanis, V., Liatsikos, E., & Gözen, A. S. (2024). Predictive Value of the Mayo Adhesive Probability (MAP) Score in Laparoscopic Partial Nephrectomies: A Systematic Review from the EAU Section of Uro-Technology (ESUT). Cancers, 16(8), 1455. https://doi.org/10.3390/cancers16081455