
The Prognostic Impact of the Surgical Margin in Renal Cell Carcinoma Treated with Partial Nephrectomy: A Multi-Center Study


Abstract
Simple Summary
Abstract
1. Introduction
2. Method
2.1. Data Collection and Database Description
2.2. Preoperative Patient Characteristics
2.3. Tumor Characteristics and Surgical Aspects
2.4. Follow-Up Protocol and Recurrence Assessment
2.5. Ethical Approvals
3. Results
3.1. Patient Demographics and Baseline Characteristics
3.2. Positive Surgical Margin
3.3. Recurrences
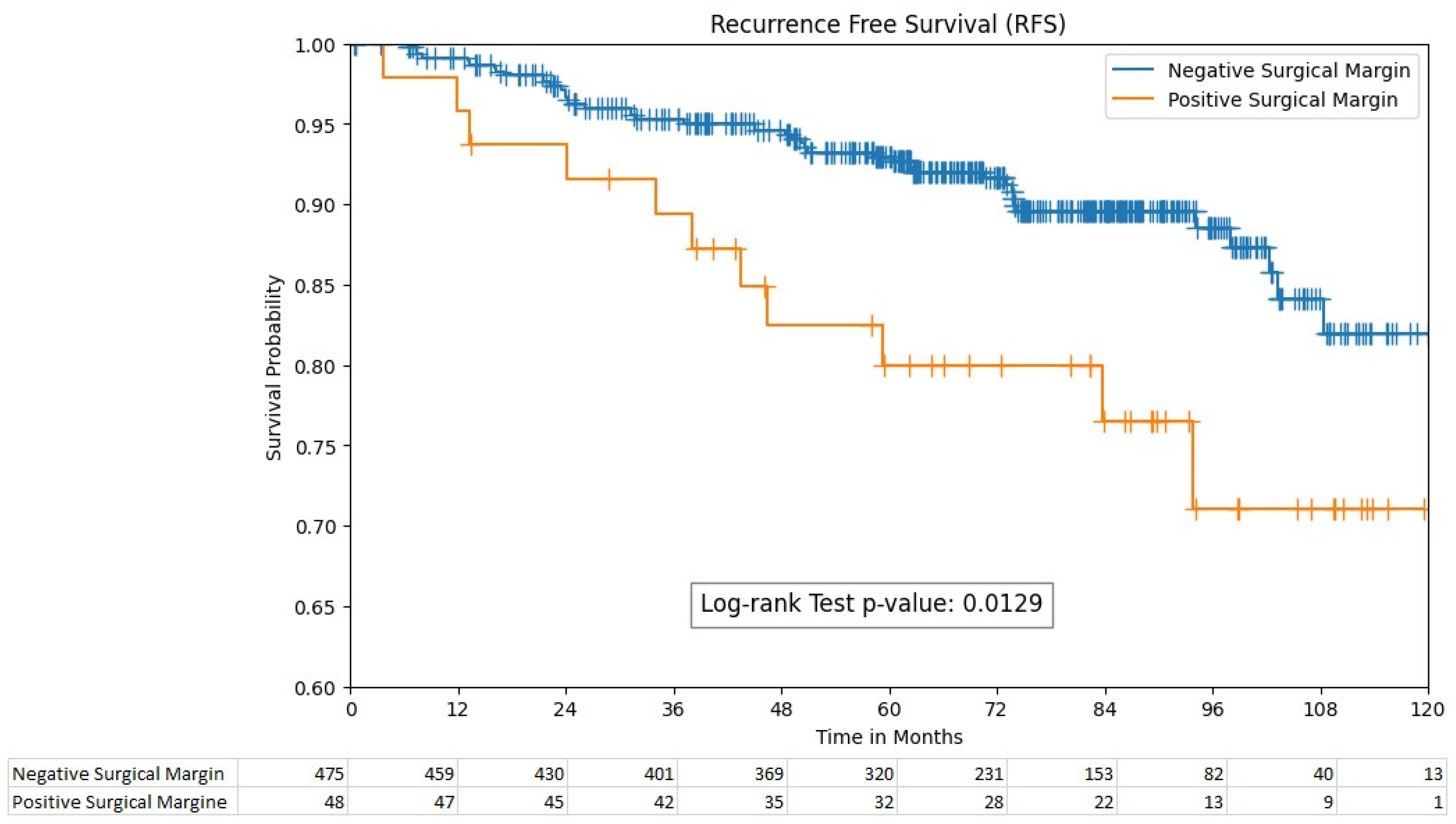
3.4. Survival Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Laganosky, D.D.; Filson, C.P.; Master, V.A. Surgical Margins in Nephron-Sparing Surgery for Renal Cell Carcinoma. Curr. Urol. Rep. 2017, 18, 8. [Google Scholar] [CrossRef]
- Morrone, A.; Bentellis, I.; Bernhard, J.-C.; Bensalah, K.; Champy, C.; Bruyere, F.; Doumerc, N.; Olivier, J.; Audenet, F.; Parier, B.; et al. Positive surgical margin’s impact on short-term oncological prognosis after robot-assisted partial nephrectomy (MARGINS study: UroCCR no 96). Sci. Rep. 2022, 12, 18342. [Google Scholar] [CrossRef]
- Shah, P.H.; Moreira, D.M.; Okhunov, Z.; Patel, V.R.; Chopra, S.; Razmaria, A.A.; Alom, M.; George, A.K.; Yaskiv, O.; Schwartz, M.J.; et al. Positive Surgical Margins Increase Risk of Recurrence after Partial Nephrectomy for High Risk Renal Tumors. J. Urol. 2016, 196, 327–334. [Google Scholar] [CrossRef]
- Yossepowitch, O.; Thompson, R.H.; Leibovich, B.C.; Eggener, S.E.; Pettus, J.A.; Kwon, E.D.; Herr, H.W.; Blute, M.L.; Russo, P. Positive surgical margins at partial nephrectomy: Predictors and oncological outcomes. J. Urol. 2008, 179, 2158–2163. [Google Scholar] [CrossRef]
- Ljungberg, B.; Albiges, L.; Abu-Ghanem, Y.; Bensalah, K.; Dabestani, S.; Fernández-Pello, S.; Giles, R.H.; Hofmann, F.; Hora, M.; Kuczyk, M.A.; et al. European Association of Urology Guidelines on Renal Cell Carcinoma: The 2019 Update. Eur. Urol. 2019, 75, 799–810. [Google Scholar] [CrossRef]
- Li, T.; Badre, A.; Alambeigi, F.; Tavakoli, M. Robotic Systems and Navigation Techniques in Orthopedics: A Historical Review. Appl. Sci. 2023, 13, 9768. [Google Scholar] [CrossRef]
- Gadus, L.; Kocarek, J.; Chmelik, F.; Matejkova, M.; Heracek, J. Robotic Partial Nephrectomy with Indocyanine Green Fluorescence Navigation. Contrast Media Mol. Imaging 2020, 2020, 1287530. [Google Scholar] [CrossRef]
- Calpin, G.G.; Ryan, F.R.; McHugh, F.T.; McGuire, B.B. Comparing the outcomes of open, laparoscopic and robot-assisted partial nephrectomy: A network meta-analysis. BJU Int. 2023, 132, 353–364. [Google Scholar] [CrossRef]
- Kim, H.; Kim, J.K.; Ye, C.; Choi, J.H.; Lee, H.; Oh, J.J.; Lee, S.; Hong, S.K.; Byun, S.-S. Recurrence after radical and partial nephrectomy in high complex renal tumor using propensity score matched analysis. Sci. Rep. 2021, 11, 2919. [Google Scholar] [CrossRef]
- Abu-Ghanem, Y.; Ramon, J.; Berger, R.; Kaver, I.; Fridman, E.; Leibowitz-Amit, R.; Dotan, Z.A. Positive surgical margin following radical nephrectomy is an independent predictor of local recurrence and disease-specific survival. World J. Surg. Oncol. 2017, 15, 193. [Google Scholar] [CrossRef]
- Demirel, H.C.; Çakmak, S.; Yavuzsan, A.H.; Yeşildal, C.; Türk, S.; Dalkılınç, A.; Kireççi, S.L.; Tokuç, E.; Horasanlı, K. Prognostic factors for surgical margin status and recurrence in partial nephrectomy. Int. J. Clin. Pract. 2020, 74, e13587. [Google Scholar] [CrossRef]
- Hakam, N.; Abou Heidar, N.; Khabsa, J.; Hneiny, L.; Akl, E.A.; Khauli, R. Does a Positive Surgical Margin after Nephron Sparing Surgery Affect Oncological Outcome in Renal Cell Carcinoma? A Systematic Review and Meta-analysis. Urology 2021, 156, e30–e39. [Google Scholar] [CrossRef]
- Grivas, N.; Kafarakis, V.; Tsimaris, I.; Raptis, P.; Hastazeris, K.; Stavropoulos, N.E. Clinico-pathological prognostic factors of renal cell carcinoma: A 15-year review from a single center in Greece. Urol. Ann. 2014, 6, 116–121. [Google Scholar] [CrossRef]
- López-Costea, M.Á.; Bonet, X.; Pérez-Reggeti, J.; Etcheverry, B.; Vigués, F. Oncological outcomes and prognostic factors after nephron-sparing surgery in renal cell carcinoma. Int. Urol. Nephrol. 2016, 48, 681–686. [Google Scholar] [CrossRef]
- Petros, F.G.; Metcalfe, M.J.; Yu, K.-J.; Keskin, S.K.; Fellman, B.M.; Chang, C.M.; Gu, C.; Tamboli, P.; Matin, S.F.; Karam, J.A.; et al. Oncologic outcomes of patients with positive surgical margin after partial nephrectomy: A 25-year single institution experience. World J. Urol. 2018, 36, 1093–1101. [Google Scholar] [CrossRef]
- Khalifeh, A.; Kaouk, J.H.; Bhayani, S.; Rogers, C.; Stifelman, M.; Tanagho, Y.S.; Kumar, R.; Gorin, M.A.; Sivarajan, G.; Samarasekera, D.; et al. Positive surgical margins in robot-assisted partial nephrectomy: A multi-institutional analysis of oncologic outcomes (leave no tumor behind). J. Urol. 2013, 190, 1674–1679. [Google Scholar] [CrossRef]
- Takagi, T.; Yoshida, K.; Wada, A.; Kondo, T.; Fukuda, H.; Ishihara, H.; Kobayashi, H.; Iizuka, J.; Okumi, M.; Ishida, H.; et al. Predictive factors for recurrence after partial nephrectomy for clinical T1 renal cell carcinoma: A retrospective study of 1227 cases from a single institution. Int. J. Clin. Oncol. 2020, 25, 892–898. [Google Scholar] [CrossRef]
- Henderickx, M.M.E.L.; Baldew, S.V.; Marconi, L.; van Dijk, M.D.; van Etten-Jamaludin, F.S.; Lagerveld, B.W.; Bex, A.; Zondervan, P.J. Surgical margins after partial nephrectomy as prognostic factor for the risk of local recurrence in pT1 RCC: A systematic review and narrative synthesis. World J. Urol. 2022, 40, 2169–2179. [Google Scholar] [CrossRef]
- Bai, R.; Gao, L.; Wang, J.; Jiang, Q. Positive surgical margins may not affect the survival of patients with renal cell carcinoma after partial nephrectomy: A meta-analysis based on 39 studies. Front. Oncol. 2022, 12, 945166. [Google Scholar] [CrossRef]
- García-Perdomo, H.A.; Ribal Caparrós, M.J.; Alcaraz Asensio, A.; Vilaseca Cabo, A. Effect of Positive Surgical Margins in Patients Who Undergo a Partial Nephrectomy Regarding Recurrence, Overall Survival, Recurrence/Progression-Free Survival, and Metastasis-Free Survival. A Systematic Review and Meta-Analysis. Clin. Genitourin. Cancer 2022, 20, 459–472. [Google Scholar] [CrossRef]
- Comparative Analysis of Salvage Partial Nephrectomy Versus Radical Nephrectomy after the Failure of Initial Partial Nephrectomy—ScienceDirect n.d. Available online: https://www.sciencedirect.com/science/article/abs/pii/S1078143923002582 (accessed on 19 January 2024).
- Shah, P.H.; George, A.K.; Moreira, D.M.; Alom, M.; Okhunov, Z.; Salami, S.; Waingankar, N.; Schwartz, M.J.; Vira, M.A.; Richstone, L.; et al. To clamp or not to clamp? Long-term functional outcomes for elective off-clamp laparoscopic partial nephrectomy. BJU Int. 2016, 117, 293–299. [Google Scholar] [CrossRef] [PubMed]
- Every Minute Counts When the Renal Hilum Is Clamped During Partial Nephrectomy—ClinicalKey n.d. Available online: https://www.clinicalkey.com/#!/content/playContent/1-s2.0-S0302283810005312?returnurl=https:%2F%2Flinkinghub.elsevier.com%2Fretrieve%2Fpii%2FS0302283810005312%3Fshowall%3Dtrue&referrer=https:%2F%2Fbjui-journals.onlinelibrary.wiley.com%2F (accessed on 19 January 2024).
- Thompson, R.H.; Lane, B.R.; Lohse, C.M.; Leibovich, B.C.; Fergany, A.; Frank, I.; Gill, I.S.; Campbell, S.C.; Blute, M.L. Comparison of warm ischemia versus no ischemia during partial nephrectomy on a solitary kidney. Eur. Urol. 2010, 58, 331–336. [Google Scholar] [CrossRef] [PubMed]
- Positive Surgical Margin Appears to Have Negligible Impact on Survival of Renal Cell Carcinomas Treated by Nephron-Sparing Surgery—PubMed n.d. Available online: https://pubmed.ncbi.nlm.nih.gov/19359089/ (accessed on 30 March 2023).
- Current Strategies to Diagnose and Manage Positive Surgical Margins and Local Recurrence after Partial Nephrectomy—ScienceDirect n.d. Available online: https://www.sciencedirect.com/science/article/pii/S2214388222000406 (accessed on 19 January 2024).
- Carini, M.; Minervini, A.; Lapini, A.; Masieri, L.; Serni, S. Simple enucleation for the treatment of renal cell carcinoma between 4 and 7 cm in greatest dimension: Progression and long-term survival. J. Urol. 2006, 175, 2022–2026, discussion 2026. [Google Scholar] [CrossRef]


{kind=link}
| Characteristic | PSM (n = ) N (%) | NSM (n = ) N (%) | p-Value |
|---|---|---|---|
| Age (median, IQR) | 61.2 (54.4–69.1) | 64.1 (55.3–69.7) | 0.57 |
| Gender | 0.24 | ||
| Male | 36 (75%) | 317 (66.7%) | |
| Female | 12 (25%) | 158 (33.3%) | |
| Performance score | 0.93 | ||
| 0 | 38 | 355 | |
| 1 | 8 | 77 | |
| 2 | 2 | 27 | |
| 3 | 0 | 2 | |
| Body Max Index (median, IQR) | 26.5 (23.1–31.6) | 26.8 (24.1–30.1) | 0.84 |
| Charlson score index | 0.37 | ||
| 0 | 132 | 9 | |
| 1 | 169 | 23 | |
| 2 | 108 | 12 | |
| 3 | 45 | 4 | |
| 4 | 16 | 0 | |
| 5 | 5 | 0 | |
| Hypertension | 28 (58.3%) | 239 (51.2%) | 0.35 |
| Symptoms | 13 (27.7%) | 167 (36.9%) | 0.21 |
| PADUA score (median, IQR) | 9 (7–11) | 8 (7–10) | 0.26 |
| Smoking | N = 45 | N = 442 | 0.24 |
| Current | 18 (40%) | 129 (29.2%) | |
| Previous | 11 (24.4%) | 153 (34.6%) | |
| Never | 16 (35.6%) | 160 (36.2%) | |
| Tumor localization | 0.63 | ||
| Right kidney | 23 (47.9%) | 236 (50.1%) | |
| Left kidney | 23 (47.9%) | 224 (47.6%) | |
| Bilateral | 2 (4.2%) | 11 (2.3%) | |
| Tumor size (mm) (median, IQR) | 30 (23–40) | 30 (21–41) | 0.35 |
| Surgical technique | |||
| Laparoscopic | 16 (34%) | 110 (23.8) | |
| Open | 18 (38.3%) | 130 (28.1%) | |
| Robotic | 13 (27.7%) | 222 (48.1%) | 0.03 |
| Clamping technique | N = 47 | N = 433 | 0.47 |
| Yes | 39 (86.7%) | 390 (90.1%) | |
| No | 6 (13.3%) | 43 (9.9%) | |
| Resection technique | N = 45 | N = 439 | 0.11 |
| Excision | 42 (93.3%) | 428 (97.5%) | |
| Enucleation | 3 (6.7%) | 11 (2.5%) | |
| Histology | N = 46 | N = 467 | 0.49 |
| Clear cell | 27 (58.7%) | 323 (69.2%) | |
| Non-clear cell | 19 (41.3%) | 144 (30.8%) | |
| T-category | 0.06 | ||
| T1a | 32 (68.1%) | 344 (72.9%) | |
| T1b | 7 (14.9%) | 94 (19.9%) | |
| T2 | 4 (8.5%) | 22 (4.7%) | |
| T3a/b | 4 (8.5%) | 12 (2.5%) | |
| Nuclear Grade | N = 42 | N = 459 | 0.29 |
| Fuhrmann 1 | 5 (11.9%) | 111 (24.2%) | |
| Fuhrmann 2 | 29 (69%) | 272 (59.3%) | |
| Fuhrmann 3 and 4 | 8 (19.1%) | 76 (16.5%) | |
| Recurrences | |||
| No | 37 (77%) | 431 (91%) | 0.01 |
| Yes | 11 (23%) | 44 (9%) | |
| Site of recurrence | 11 | 44 | 0.007 |
| Local | 9 | 24 | |
| Lunge + | 1 | 9 | |
| Bone + | 0 | 3 | |
| Other + | 1 | 8 | |
| Died | 6 | 103 | 0.14 |
| Risk Factors | Categories | Number (%) | p-Value |
|---|---|---|---|
| Surgical approach | Laparoscopic | 16 (12.7%) | 0.01 |
| Open | 18 (12.2%) | ||
| Robot | 13 (5.5%) | ||
| pT-category | T1 | 1 (33.3%) | 0.45 |
| T1a | 31 (8.3%) | ||
| T1b | 7 (6.9%) | ||
| T2a | 4 (20%) | ||
| T3a | 3 (23%) | ||
| T3b | 1 (50%) | ||
| Resection technique | Enucleation | 3 (21.4%) | 0.28 |
| Excision | 42 (8.9%) | ||
| Histologic subtype | clear cell adenocarcinoma | 27 (7.7%) | 0.21 |
| chromofobe renal cell carcinoma | 7 (14.9%) | ||
| papillary adenocarcinoma type 1 | 8 (14.5%) | ||
| papillary adenocarcinoma type 2 | 4 (8.9%) | ||
| Leibovich score | 0 | 21 (7.6%) | 0.19 |
| 1 | 8 (10.1%) | ||
| 2 | 1 (1.5%) | ||
| 3 | 4 (10.8%) | ||
| 4 | 7 (21.2%) | ||
| 5 | 3 (23.1%) | ||
| 6 | 0 (0) | ||
| 7 | 0 (0) | ||
| Tumor size | <4 cm | 36 (9.3%) | 0.91 |
| 4–7 cm | 9 (8.3%) | ||
| >7 cm | 3 (10.7%) | ||
| Ischemia technique | Clamping | 39 (9.1%) | 0.52 |
| Off clamping | 6 (12.2%) |
| Variable | Hazard Ratio | 95% CI | p-Value |
|---|---|---|---|
| Resection technique | 0.71 | 0.17 to 2.93 | 0.64 |
| Necrosis | 1.58 | 0.89 to 2.79 | 0.12 |
| T-category | 1.13 | 0.64 to 2.02 | 0.67 |
| Fuhrman Grade | 1.80 | 1.21 to 2.68 | <0.005 |
| PADUA score | 1.12 | 0.97 to 1.30 | 0.13 |
| Tumor size | 1.02 | 1.01 to 1.03 | <0.005 |
| Leibovich score | 1.48 | 1.20 to 1.82 | <0.005 |
| Age | 1.24 | 0.93 to 1.65 | 0.14 |
| Positive surgical margin | 2.27 | 1.17 to 4.40 | 0.02 |
| Variable | Coefficient | Hazard Ratio | 95% CI | p-Value |
|---|---|---|---|---|
| PSM | 0.72 | 2.05 | 0.04 to 1.40 | 0.04 |
| Gender | 0.31 | 1.37 | −0.32 to 0.94 | 0.33 |
| Leibovich score | 0.26 | 1.3 | 0.11 to 0.42 | <0.005 |
| Age | 0.02 | 1.02 | −0.01 to 0.05 | 0.16 |
| Surgical technique: Open | −0.2 | 0.82 | −0.92 to 0.51 | 0.57 |
| Surgical technique: Robot | −0.04 | 0.96 | −0.71 to 0.63 | 0.91 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mosholt, K.S.S.; Aagaard, M.; Røder, A.; Azawi, N. The Prognostic Impact of the Surgical Margin in Renal Cell Carcinoma Treated with Partial Nephrectomy: A Multi-Center Study. Cancers 2024, 16, 1449. https://doi.org/10.3390/cancers16081449
Mosholt KSS, Aagaard M, Røder A, Azawi N. The Prognostic Impact of the Surgical Margin in Renal Cell Carcinoma Treated with Partial Nephrectomy: A Multi-Center Study. Cancers. 2024; 16(8):1449. https://doi.org/10.3390/cancers16081449
Chicago/Turabian StyleMosholt, Karina Sif Søndergaard, Mark Aagaard, Andreas Røder, and Nessn Azawi. 2024. "The Prognostic Impact of the Surgical Margin in Renal Cell Carcinoma Treated with Partial Nephrectomy: A Multi-Center Study" Cancers 16, no. 8: 1449. https://doi.org/10.3390/cancers16081449
APA StyleMosholt, K. S. S., Aagaard, M., Røder, A., & Azawi, N. (2024). The Prognostic Impact of the Surgical Margin in Renal Cell Carcinoma Treated with Partial Nephrectomy: A Multi-Center Study. Cancers, 16(8), 1449. https://doi.org/10.3390/cancers16081449