
Clinical [18F]FSPG Positron Emission Tomography Imaging Reveals Heterogeneity in Tumor-Associated System xc− Activity

 , ,
, ,  and
and
Abstract
Simple Summary
Abstract
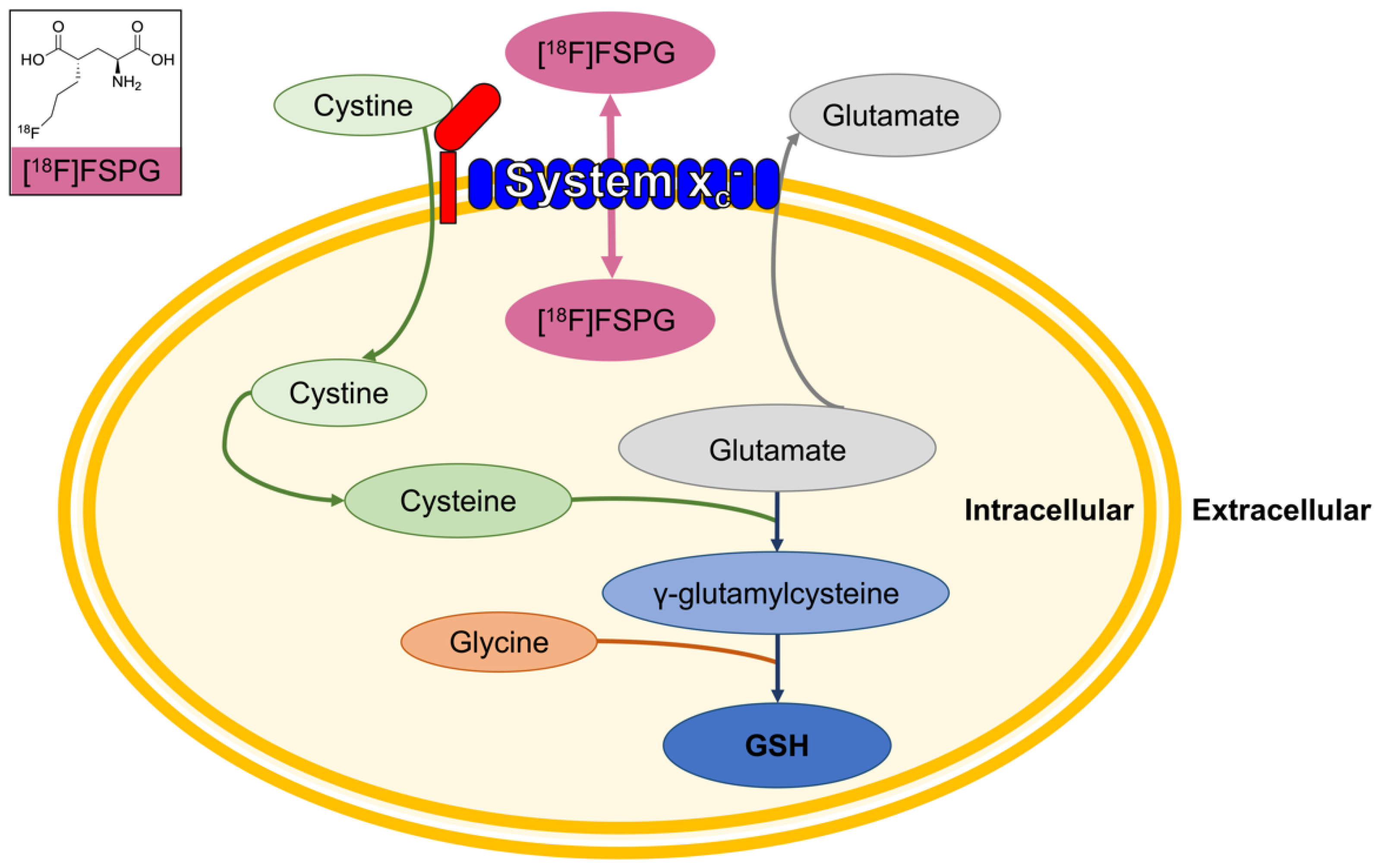
1. Background
2. Data and Methods
2.1. [18F]FSPG Acquisition
2.2. Image Analysis
2.3. Statistical Analysis
3. Results
3.1. Subject Demographics
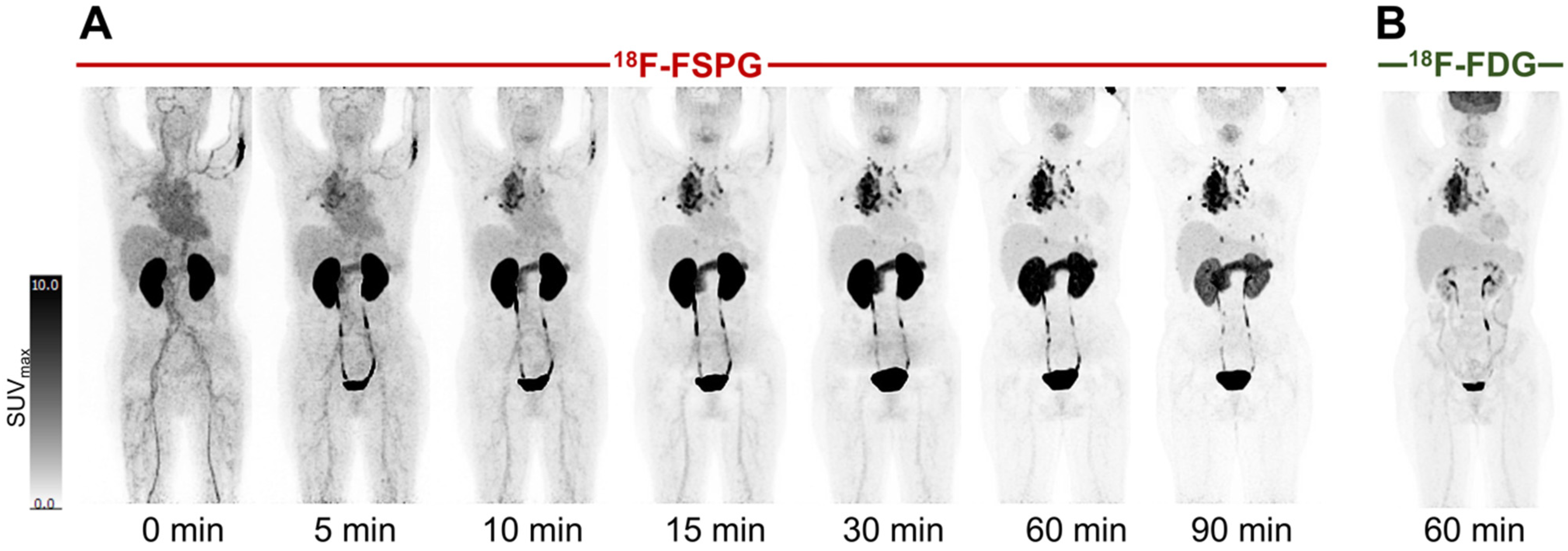
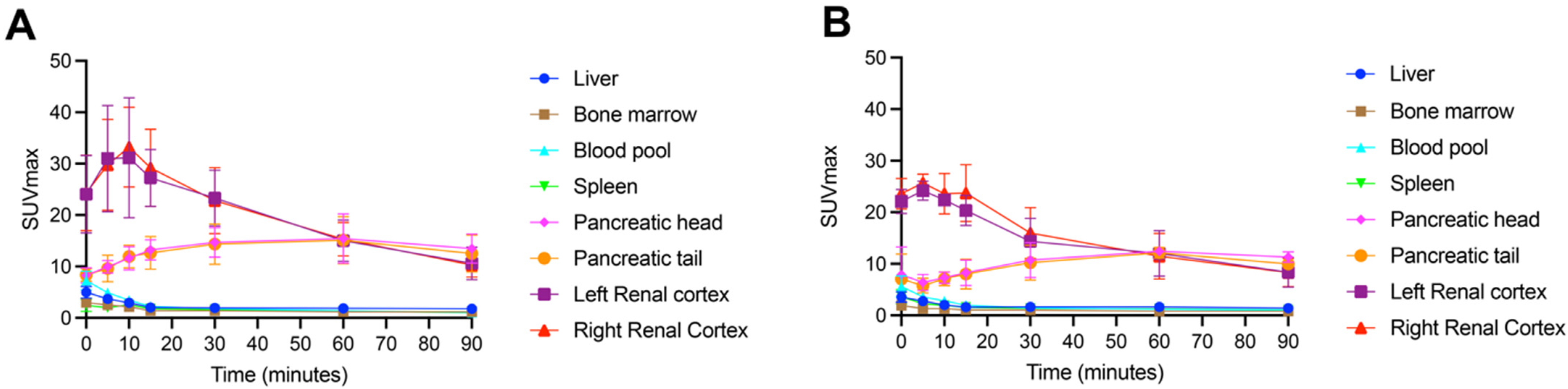
3.2. [18F]FSPG Has Consistent Biodistribution in Normal Organs
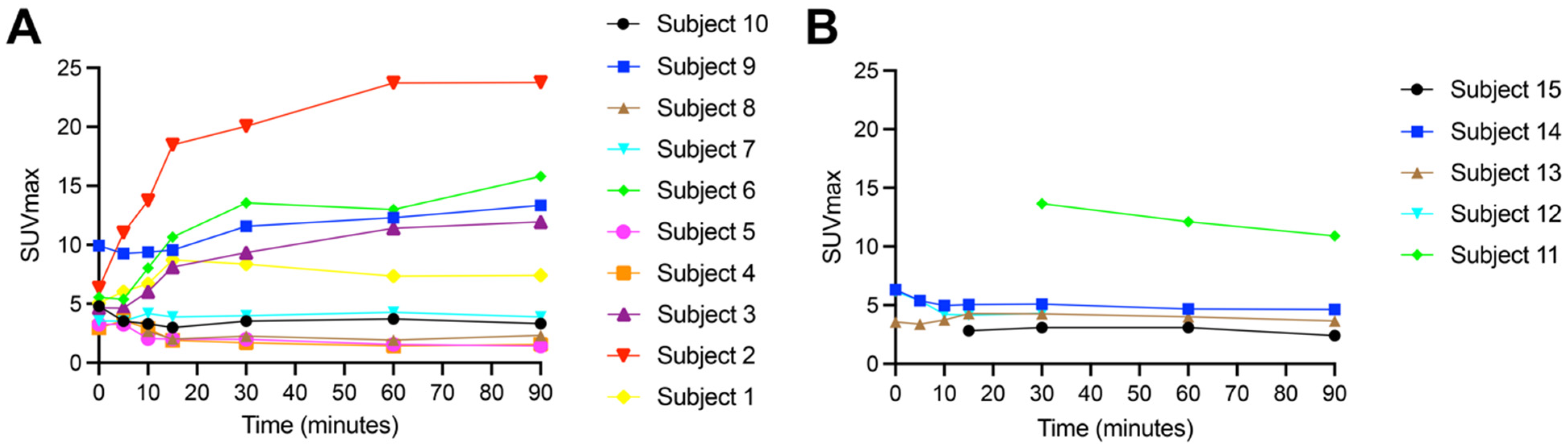
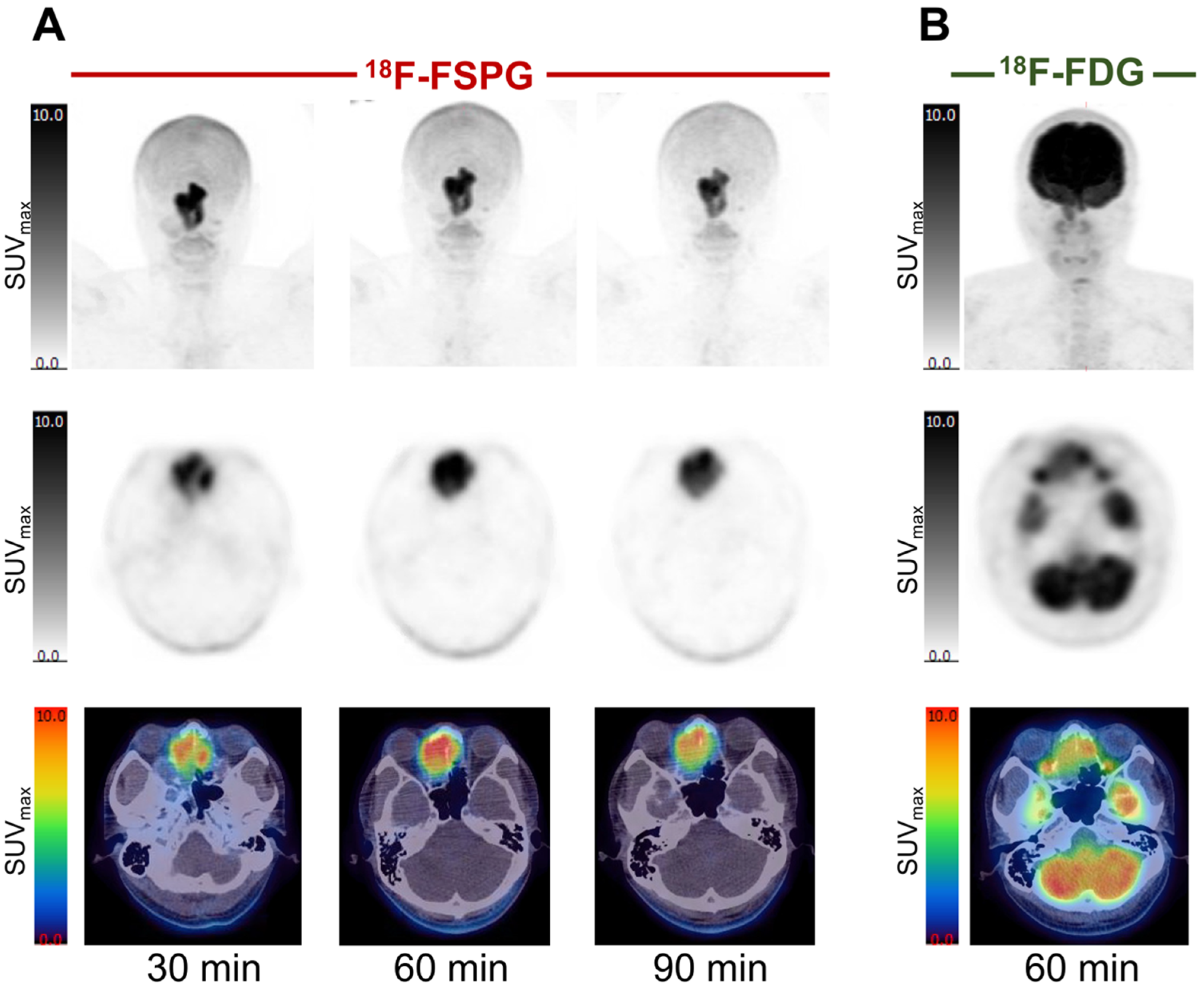
3.3. [18F]FSPG Retention Is Heterogeneous in Both NSCLC and HNSCC Primary Tumors
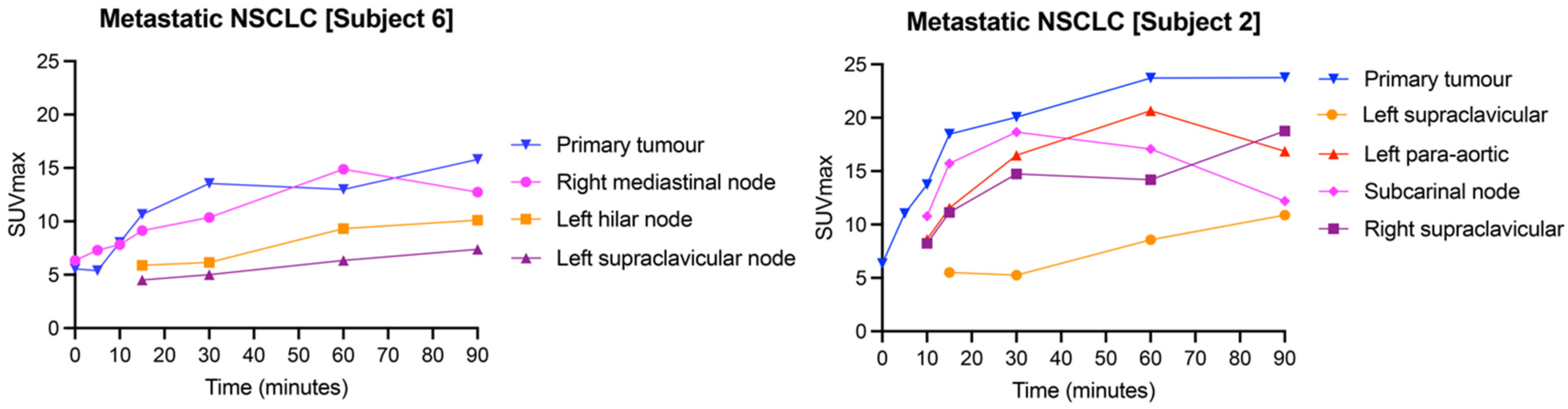
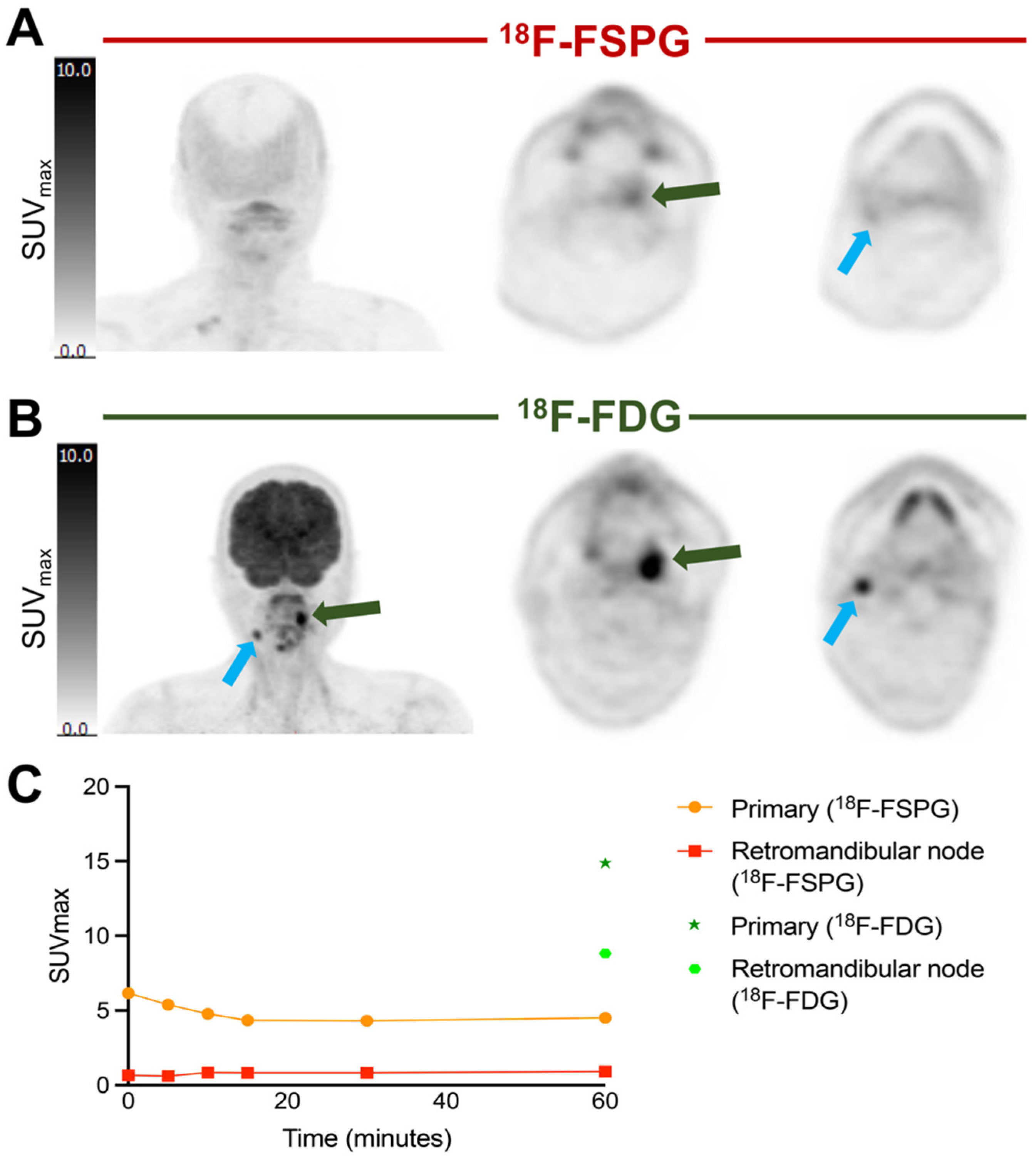
3.4. Inter-Lesion Variability across Metastases Is Apparent with [18F]FSPG
3.5. Image Analysis Results in High Inter-Observer Concordance
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| [18F]FDG | 18F-2-fluoro-2-deoxy-D-glucose |
| [18F]FSPG | (4S)-4-(3-[18F]fluoropropyl)-L-glutamic acid |
| GSH | glutathione |
| PET | positron emission tomography |
| CT | computed tomography |
| HNSCC | head and neck squamous cell cancer |
| NSCLC | non-small-cell lung cancer |
| SUV | standardized uptake value |
References
- Aboelella, N.S.; Brandle, C.; Kim, T.; Ding, Z.-C.; Zhou, G. Oxidative Stress in the Tumor Microenvironment and Its Relevance to Cancer Immunotherapy. Cancers 2021, 13, 986. [Google Scholar] [CrossRef]
- Mittra, E.S.; Koglin, N.; Mosci, C.; Kumar, M.; Hoehne, A.; Keu, K.V.; Iagaru, A.H.; Mueller, A.; Berndt, M.; Bullich, S.; et al. Pilot Preclinical and Clinical Evaluation of (4S)-4-(3-[18F]Fluoropropyl)-L-Glutamate (18F-FSPG) for PET/CT Imaging of Intracranial Malignancies. PLoS ONE 2016, 11, e0148628. [Google Scholar] [CrossRef]
- Kavanaugh, G.; Williams, J.; Morris, A.S.; Nickels, M.L.; Walker, R.; Koglin, N.; Stephens, A.W.; Washington, M.K.; Geevarghese, S.K.; Liu, Q.; et al. Utility of [18F]FSPG PET to Image Hepatocellular Carcinoma: First Clinical Evaluation in a US Population. Mol. Imaging Biol. 2016, 18, 924–934. [Google Scholar] [CrossRef]
- Li, Y.; Zhang, X.; Wang, Z.; Li, B.; Zhu, H. Modulation of Redox Homeostasis: A Strategy to Overcome Cancer Drug Resistance. Front. Pharmacol. 2023, 14, 1156538. [Google Scholar] [CrossRef]
- Daher, B.; Parks, S.K.; Durivault, J.; Cormerais, Y.; Baidarjad, H.; Tambutte, E.; Pouysségur, J.; Vučetić, M. Genetic Ablation of the Cystine Transporter XCT in PDAC Cells Inhibits MTORC1, Growth, Survival, and Tumor Formation via Nutrient and Oxidative Stresses. Cancer Res. 2019, 79, 3877–3890. [Google Scholar] [CrossRef]
- Smolarz, K.; Krause, B.J.; Graner, F.-P.; Wagner, F.M.; Hultsch, C.; Bacher-Stier, C.; Sparks, R.B.; Ramsay, S.; Fels, L.M.; Dinkelborg, L.M.; et al. (S)-4-(3-18F-Fluoropropyl)-l-Glutamic Acid: An 18F-Labeled Tumor-Specific Probe for PET/CT Imaging—Dosimetry. J. Nucl. Med. 2013, 54, 861–866. [Google Scholar] [CrossRef]
- Mosci, C.; Kumar, M.; Smolarz, K.; Koglin, N.; Stephens, A.W.; Schwaiger, M.; Gambhir, S.S.; Mittra, E.S. Characterization of Physiologic 18F FSPG Uptake in Healthy Volunteers. Radiology 2016, 279, 898–905. [Google Scholar] [CrossRef][Green Version]
- Park, S.Y.; Mosci, C.; Kumar, M.; Wardak, M.; Koglin, N.; Bullich, S.; Mueller, A.; Berndt, M.; Stephens, A.W.; Chin, F.T.; et al. Initial Evaluation of (4S)-4-(3-[18F]Fluoropropyl)-l-Glutamate (FSPG) PET/CT Imaging in Patients with Head and Neck Cancer, Colorectal Cancer, or Non-Hodgkin Lymphoma. EJNMMI Res. 2020, 10, 100. [Google Scholar] [CrossRef]
- Wardak, M.; Sonni, I.; Fan, A.P.; Minamimoto, R.; Jamali, M.; Hatami, N.; Zaharchuk, G.; Fischbein, N.; Nagpal, S.; Li, G.; et al. 18F-FSPG PET/CT Imaging of System xC− Transporter Activity in Patients with Primary and Metastatic Brain Tumors. Radiology 2022, 303, 620–631. [Google Scholar] [CrossRef]
- Baek, S.; Choi, C.-M.; Ahn, S.H.; Lee, J.W.; Gong, G.; Ryu, J.-S.; Oh, S.J.; Bacher-Stier, C.; Fels, L.; Koglin, N.; et al. Exploratory Clinical Trial of (4S)-4-(3-[18F]Fluoropropyl)-l-Glutamate for Imaging XC− Transporter Using Positron Emission Tomography in Patients with Non–Small Cell Lung or Breast Cancer. Clin. Cancer Res. 2012, 18, 5427–5437. [Google Scholar] [CrossRef]
- Paez, R.; Shah, C.; Cords, A.J.; Muterspaugh, A.; Helton, J.E.; Antic, S.; Eisenberg, R.; Chen, H.; Grogan, E.L.; Manning, H.C.; et al. 18F-FSPG PET Imaging for the Evaluation of Indeterminate Pulmonary Nodules. PLoS ONE 2022, 17, e0265427. [Google Scholar] [CrossRef]
- Baek, S.; Mueller, A.; Lim, Y.-S.; Lee, H.C.; Lee, Y.-J.; Gong, G.; Kim, J.S.; Ryu, J.-S.; Oh, S.J.; Lee, S.J.; et al. (4S)-4-(3-18F-Fluoropropyl)-l-Glutamate for Imaging of XC¯ Transporter Activity in Hepatocellular Carcinoma Using PET: Preclinical and Exploratory Clinical Studies. J. Nucl. Med. 2013, 54, 117–123. [Google Scholar] [CrossRef]
- Cheng, M.-F.; Huang, Y.-Y.; Ho, B.-Y.; Kuo, T.-C.; Hsin, L.-W.; Shiue, C.-Y.; Kuo, H.-C.; Jeng, Y.-M.; Yen, R.-F.; Tien, Y.-W. Prospective Comparison of (4S)-4-(3-18F-Fluoropropyl)-l-Glutamate versus 18F-Fluorodeoxyglucose PET/CT for Detecting Metastases from Pancreatic Ductal Adenocarcinoma: A Proof-of-Concept Study. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 810–820. [Google Scholar] [CrossRef]
- Park, S.Y.; Na, S.J.; Kumar, M.; Mosci, C.; Wardak, M.; Koglin, N.; Bullich, S.; Mueller, A.; Berndt, M.; Stephens, A.W.; et al. Clinical Evaluation of (4S)-4-(3-[18F]Fluoropropyl)-L-Glutamate (18F-FSPG) for PET/CT Imaging in Patients with Newly Diagnosed and Recurrent Prostate Cancer. Clin. Cancer Res. 2020, 26, 5380–5387. [Google Scholar] [CrossRef]
- Sharkey, A.R.; Witney, T.H.; Cook, G.J.R. Is System Xc− a Suitable Target for Tumour Detection and Response Assessment with Imaging? Cancers 2023, 15, 5573. [Google Scholar] [CrossRef]
- McCormick, P.N.; Greenwood, H.E.; Glaser, M.; Maddocks, O.D.K.; Gendron, T.; Sander, K.; Gowrishankar, G.; Hoehne, A.; Zhang, T.; Shuhendler, A.J.; et al. Assessment of Tumor Redox Status through (S)-4-(3-[18F]Fluoropropyl)-L-Glutamic Acid Positron Emission Tomography Imaging of System Xc− Activity. Cancer Res. 2018, 79, 853–863. [Google Scholar] [CrossRef]
- Greenwood, H.E.; McCormick, P.N.; Gendron, T.; Glaser, M.; Pereira, R.; Maddocks, O.D.K.; Sander, K.; Zhang, T.; Koglin, N.; Lythgoe, M.F.; et al. Measurement of Tumor Antioxidant Capacity and Prediction of Chemotherapy Resistance in Preclinical Models of Ovarian Cancer by Positron Emission Tomography. Clin. Cancer Res. 2019, 25, 2471–2482. [Google Scholar] [CrossRef]
- Koglin, N.; Mueller, A.; Berndt, M.; Schmitt-Willich, H.; Toschi, L.; Stephens, A.W.; Gekeler, V.; Friebe, M.; Dinkelborg, L.M. Specific PET Imaging of XC− Transporter Activity Using a 18F-Labeled Glutamate Derivative Reveals a Dominant Pathway in Tumor Metabolism. Clin. Cancer Res. 2011, 17, 6000–6011. [Google Scholar] [CrossRef]
- Greenwood, H.E.; Edwards, R.S.; Tyrrell, W.E.; Barber, A.R.; Baark, F.; Tanc, M.; Khalil, E.; Falzone, A.; Ward, N.P.; DeBlasi, J.M.; et al. Imaging the Master Regulator of the Antioxidant Response in Non-Small Cell Lung Cancer with Positron Emission Tomography. bioRxiv 2023. [Google Scholar] [CrossRef]
- Godwin, A.K.; Meister, A.; O’Dwyer, P.J.; Huang, C.S.; Hamilton, T.C.; Anderson, M.E. High Resistance to Cisplatin in Human Ovarian Cancer Cell Lines Is Associated with Marked Increase of Glutathione Synthesis. Proc. Natl. Acad. Sci. USA 1992, 89, 3070–3074. [Google Scholar] [CrossRef]
- Ballatori, N.; Krance, S.M.; Notenboom, S.; Shi, S.; Tieu, K.; Hammond, C.L. Glutathione Dysregulation and the Etiology and Progression of Human Diseases. Biol. Chem. 2009, 390, 191–214. [Google Scholar] [CrossRef]
- Borst, P. Cancer Drug Pan-Resistance: Pumps, Cancer Stem Cells, Quiescence, Epithelial to Mesenchymal Transition, Blocked Cell Death Pathways, Persisters or What? Open Biol. 2012, 2, 120066. [Google Scholar] [CrossRef]
- Holohan, C.; Schaeybroeck, S.V.; Longley, D.B.; Johnston, P.G. Cancer Drug Resistance: An Evolving Paradigm. Nat. Rev. Cancer 2013, 13, 714–726. [Google Scholar] [CrossRef]
- Housman, G.; Byler, S.; Heerboth, S.; Lapinska, K.; Longacre, M.; Snyder, N.; Sarkar, S. Drug Resistance in Cancer: An Overview. Cancers 2014, 6, 1769–1792. [Google Scholar] [CrossRef]
- Sheikhbahaei, S.; Taghipour, M.; Ahmad, R.; Fakhry, C.; Kiess, A.P.; Chung, C.H.; Subramaniam, R.M. Diagnostic Accuracy of Follow-Up FDG PET or PET/CT in Patients With Head and Neck Cancer After Definitive Treatment: A Systematic Review and Meta-Analysis. Am. J. Roentgenol. 2015, 205, 629–639. [Google Scholar] [CrossRef]
- Sheikhbahaei, S.; Mena, E.; Yanamadala, A.; Reddy, S.; Solnes, L.B.; Wachsmann, J.; Subramaniam, R.M. The Value of FDG PET/CT in Treatment Response Assessment, Follow-Up, and Surveillance of Lung Cancer. Am. J. Roentgenol. 2017, 208, 420–433. [Google Scholar] [CrossRef]
- Bae, S.-W.; Wang, J.; Georgiou, D.K.; Wen, X.; Cohen, A.S.; Geng, L.; Tantawy, M.N.; Manning, H.C. Feasibility of [18F]FSPG PET for Early Response Assessment to Combined Blockade of EGFR and Glutamine Metabolism in Wild-Type KRAS Colorectal Cancer. Tomography 2023, 9, 497–508. [Google Scholar] [CrossRef]
- Badawi, R.D.; Shi, H.; Hu, P.; Chen, S.; Xu, T.; Price, P.M.; Ding, Y.; Spencer, B.A.; Nardo, L.; Liu, W.; et al. First Human Imaging Studies with the EXPLORER Total-Body PET Scanner. J. Nucl. Med. 2019, 60, 299–303. [Google Scholar] [CrossRef]
- Levring, T.B.; Hansen, A.K.; Nielsen, B.L.; Kongsbak, M.; von Essen, M.R.; Woetmann, A.; Ødum, N.; Bonefeld, C.M.; Geisler, C. Activated Human CD4+ T Cells Express Transporters for Both Cysteine and Cystine. Sci. Rep. 2012, 2, 266. [Google Scholar] [CrossRef]
- Chae, S.Y.; Choi, C.-M.; Shim, T.S.; Park, Y.; Park, C.-S.; Lee, H.S.; Lee, S.J.; Oh, S.J.; Kim, S.-Y.; Baek, S.; et al. Exploratory Clinical Investigation of (4S)-4-(3-18F-Fluoropropyl)-l-Glutamate PET of Inflammatory and Infectious Lesions. J. Nucl. Med. 2016, 57, 67–69. [Google Scholar] [CrossRef]
- Martín, A.; Vázquez-Villoldo, N.; Gómez-Vallejo, V.; Padro, D.; Soria, F.N.; Szczupak, B.; Plaza-García, S.; Arrieta, A.; Reese, T.; Llop, J.; et al. In Vivo Imaging of System Xc− as a Novel Approach to Monitor Multiple Sclerosis. Eur. J. Nucl. Med. Mol. Imaging 2016, 43, 1124–1138. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subject | Gender | Age | Pathology | Location | Prior Treatment | |
|---|---|---|---|---|---|---|
| NSCLC subjects | 1 | Male | 68 | NSCLC, adenocarcinoma | Right lung | None |
| 2 | Female | 58 | NSCLC, adenocarcinoma | Right lung | None | |
| 3 | Male | 70 | NSCLC, squamous cell carcinoma | Right lung | None | |
| 4 | Female | 54 | NSCLC, adenocarcinoma | Right lung | None | |
| 5 | Male | 66 | NSCLC, adenocarcinoma | Right lung | None | |
| 6 | Male | 60 | NSCLC, squamous cell carcinoma | Left lung | None | |
| 7 | Female | 50 | NSCLC, adenocarcinoma | Right lung | None | |
| 8 | Male | 54 | NSCLC, adenocarcinoma | Bilateral | None | |
| 9 | Male | 62 | NSCLC, adenocarcinoma | Right lung | None | |
| 10 | Male | 55 | NSCLC, adenocarcinoma | Right lung | None | |
| HNSCC subjects | 11 | Male | 44 | HNSCC | Nasal cavity | None |
| 12 | Male | 73 | HNSCC | Oropharynx/oral cavity (recurrent) | Chemoradiation, laryngectomy | |
| 13 | Male | 71 | HNSCC | Left maxillary sinus | Chemoradiation | |
| 14 | Male | 74 | HNSCC | Larynx | None | |
| 15 | Male | 72 | HNSCC | Nasopharynx | None |
| Subject | Scan | SUV Max | SUV Mean | SUV SD | SUV Peak | MTV | SUV Max/Mean | |
|---|---|---|---|---|---|---|---|---|
| NSCLC | 1 | [18F]FDG 60 min p.i. | 11.8 | 7.1 | 1.7 | 8.8 | 3.1 | 1.7 |
| [18F]FSPG 60 min p.i. | 7.3 | 4.6 | 1.3 | 6.4 | 4.5 | 1.6 | ||
| 2 | [18F]FDG 60 min p.i. | 16.9 | 8.8 | 14.3 | 1.7 | 62.8 | 1.9 | |
| [18F]FSPG 60 min p.i. | 23.7 | 13.9 | 2.5 | 16.9 | 16.8 | 1.7 | ||
| 3 | [18F]FDG 60 min p.i. | 11.8 | 7.0 | 1.5 | 9.7 | 34.8 | 1.7 | |
| [18F]FSPG 60 min p.i. | 11.4 | 6.2 | 1.5 | 8.8 | 13.1 | 1.8 | ||
| 4 | [18F]FDG 60 min p.i. | 7.8 | 5.0 | 1.3 | 6.1 | 2.5 | 1.6 | |
| [18F]FSPG 60 min p.i. | 1.4 | 0.9 | 0.3 | / | / | 1.5 | ||
| 5 | [18F]FDG 60 min p.i. | 15.1 | 9.9 | 2.9 | 12.4 | 2.9 | 1.5 | |
| [18F]FSPG 60 min p.i. | 1.6 | 1.1 | 0.3 | / | / | 1.5 | ||
| 6 | [18F]FDG 60 min p.i. | 17.3 | 13.2 | 2.2 | 15.0 | 3.9 | 1.3 | |
| [18F]FSPG 60 min p.i. | 13.0 | 7.5 | 2.1 | 9.7 | 2.6 | 1.7 | ||
| 7 | [18F]FDG 60 min p.i. | 10.3 | 6.8 | 1.5 | 8.9 | 10.4 | 1.5 | |
| [18F]FSPG 60 min p.i. | 4.3 | 2.6 | 0.9 | / | / | 1.6 | ||
| 8 | [18F]FDG 60 min p.i. | 9.3 | 5.5 | 1.4 | 7.5 | 5.1 | 1.7 | |
| [18F]FSPG 60 min p.i. | 1.9 | 1.3 | 0.3 | / | / | 1.5 | ||
| 9 | [18F]FDG 60 min p.i. | 12.6 | 6.7 | 2.3 | 7.7 | 2.0 | 1.9 | |
| [18F]FSPG 60 min p.i. | 12.3 | 7.8 | 2.1 | / | 1.4 | 1.6 | ||
| 10 | [18F]FDG 60 min p.i. | 7.8 | 5.6 | 1.0 | 6.4 | 2.7 | 1.4 | |
| [18F]FSPG 60 min p.i. | 3.7 | 2.1 | 0.8 | / | / | 1.7 | ||
| HNSCC | 11 | [18F]FDG 60 min p.i. | 5.5 | 4.5 | 0.7 | / | / | 1.2 |
| [18F]FSPG 60 min p.i. | 12.1 | 7.4 | 10.8 | 1.8 | 38.5 | 1.6 | ||
| 12 | [18F]FDG 60 min p.i. | 14.9 | 8.5 | 2.2 | 10.8 | 3.7 | 0.6 | |
| [18F]FSPG 60 min p.i. | 4.5 | 4.1 | 0.5 | / | / | 0.9 | ||
| 13 | [18F]FDG 60 min p.i. | 11.4 | 6.7 | 1.6 | 9.1 | 10.3 | 1.7 | |
| [18F]FSPG 60 min p.i. | 4.0 | 2.7 | 0.8 | / | / | 1.5 | ||
| 14 | [18F]FDG 60 min p.i. | Primary tumor not detectable with [18F]FDG | ||||||
| [18F]FSPG 60 min p.i. | 6.3 | 4.1 | 1.1 | / | / | 1.5 | ||
| 15 | [18F]FDG 60 min p.i. | 6.4 | 4.1 | 1.2 | / | / | 1.6 | |
| [18F]FSPG 60 min p.i. | 3.1 | 1.6 | 0.8 | / | / | 1.9 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sharkey, A.R.; Koglin, N.; Mittra, E.S.; Han, S.; Cook, G.J.R.; Witney, T.H. Clinical [18F]FSPG Positron Emission Tomography Imaging Reveals Heterogeneity in Tumor-Associated System xc− Activity. Cancers 2024, 16, 1437. https://doi.org/10.3390/cancers16071437
Sharkey AR, Koglin N, Mittra ES, Han S, Cook GJR, Witney TH. Clinical [18F]FSPG Positron Emission Tomography Imaging Reveals Heterogeneity in Tumor-Associated System xc− Activity. Cancers. 2024; 16(7):1437. https://doi.org/10.3390/cancers16071437
Chicago/Turabian StyleSharkey, Amy R., Norman Koglin, Erik S. Mittra, Sangwon Han, Gary J. R. Cook, and Timothy H. Witney. 2024. "Clinical [18F]FSPG Positron Emission Tomography Imaging Reveals Heterogeneity in Tumor-Associated System xc− Activity" Cancers 16, no. 7: 1437. https://doi.org/10.3390/cancers16071437
APA StyleSharkey, A. R., Koglin, N., Mittra, E. S., Han, S., Cook, G. J. R., & Witney, T. H. (2024). Clinical [18F]FSPG Positron Emission Tomography Imaging Reveals Heterogeneity in Tumor-Associated System xc− Activity. Cancers, 16(7), 1437. https://doi.org/10.3390/cancers16071437