Aggressive Angiomyxoma of the Lower Female Genital Tract: A Review of the MITO Rare Tumors Group

 , ,
, ,  and
and
Abstract
Simple Summary
Abstract
1. Introduction
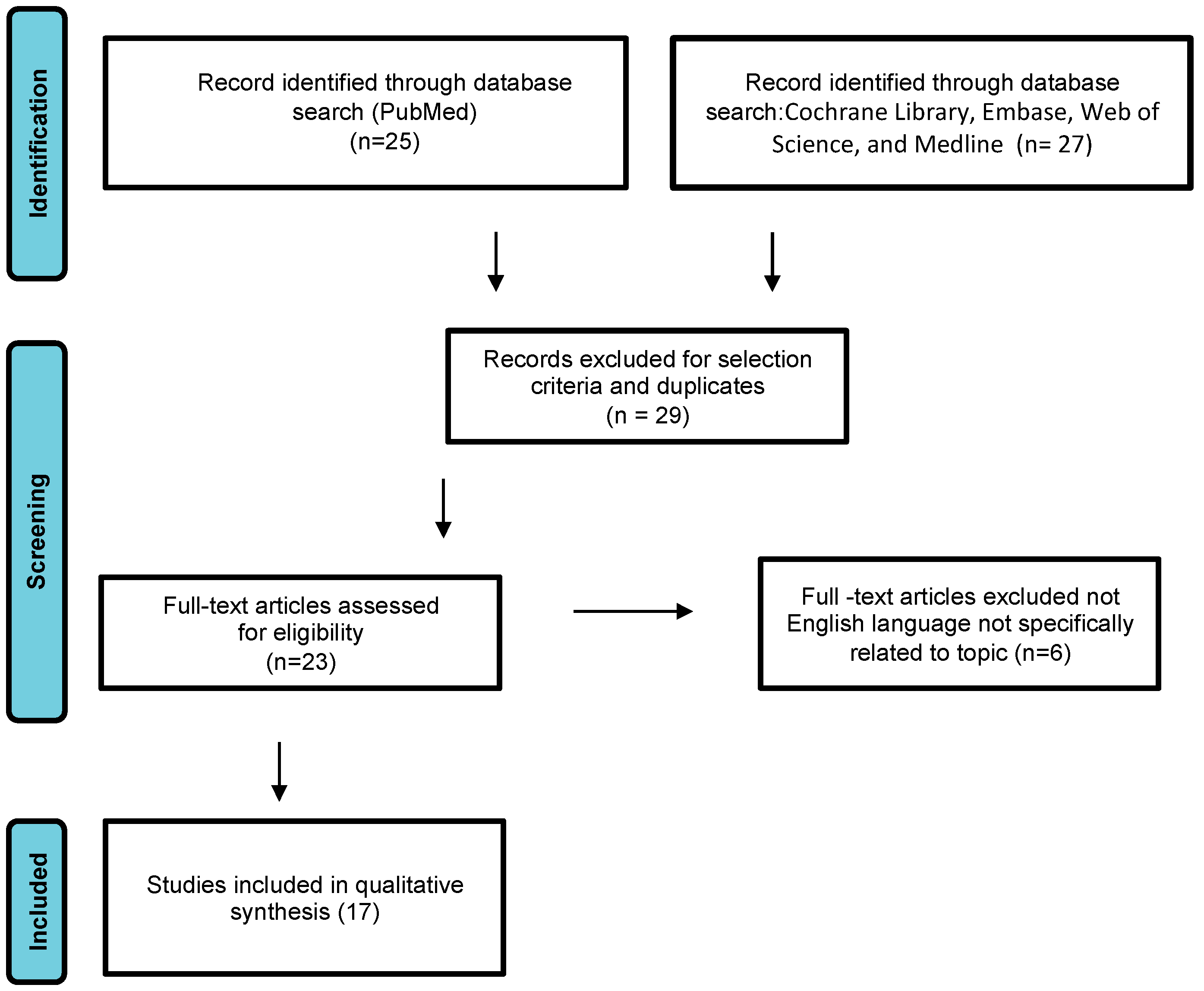
2. Materials and Methods
3. Pathological Examination
4. Clinical Features
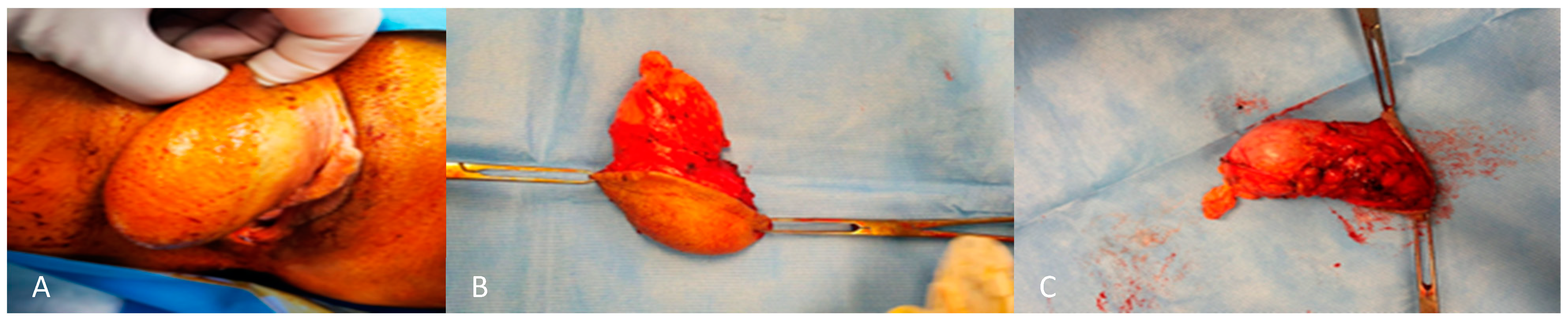
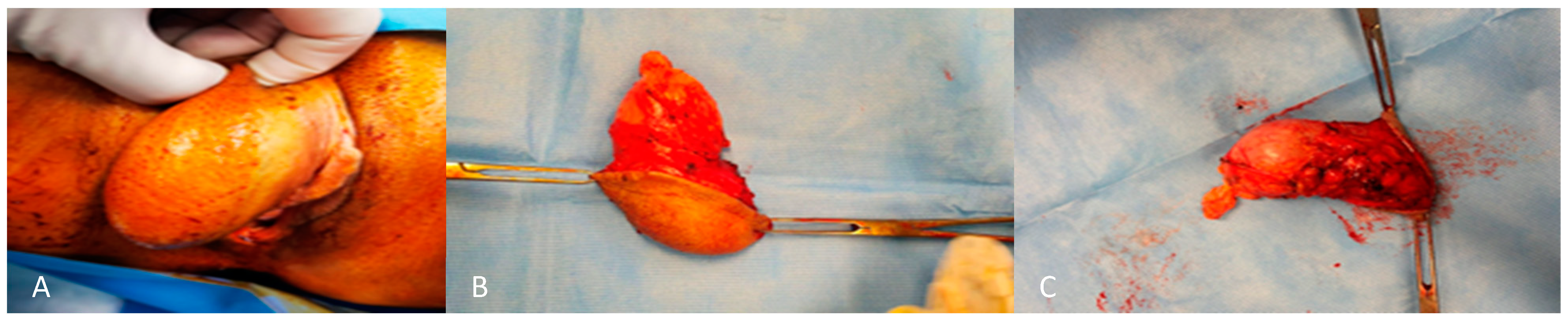
5. Management: Treatment of Aggressive Angiomyxoma of the Vulva
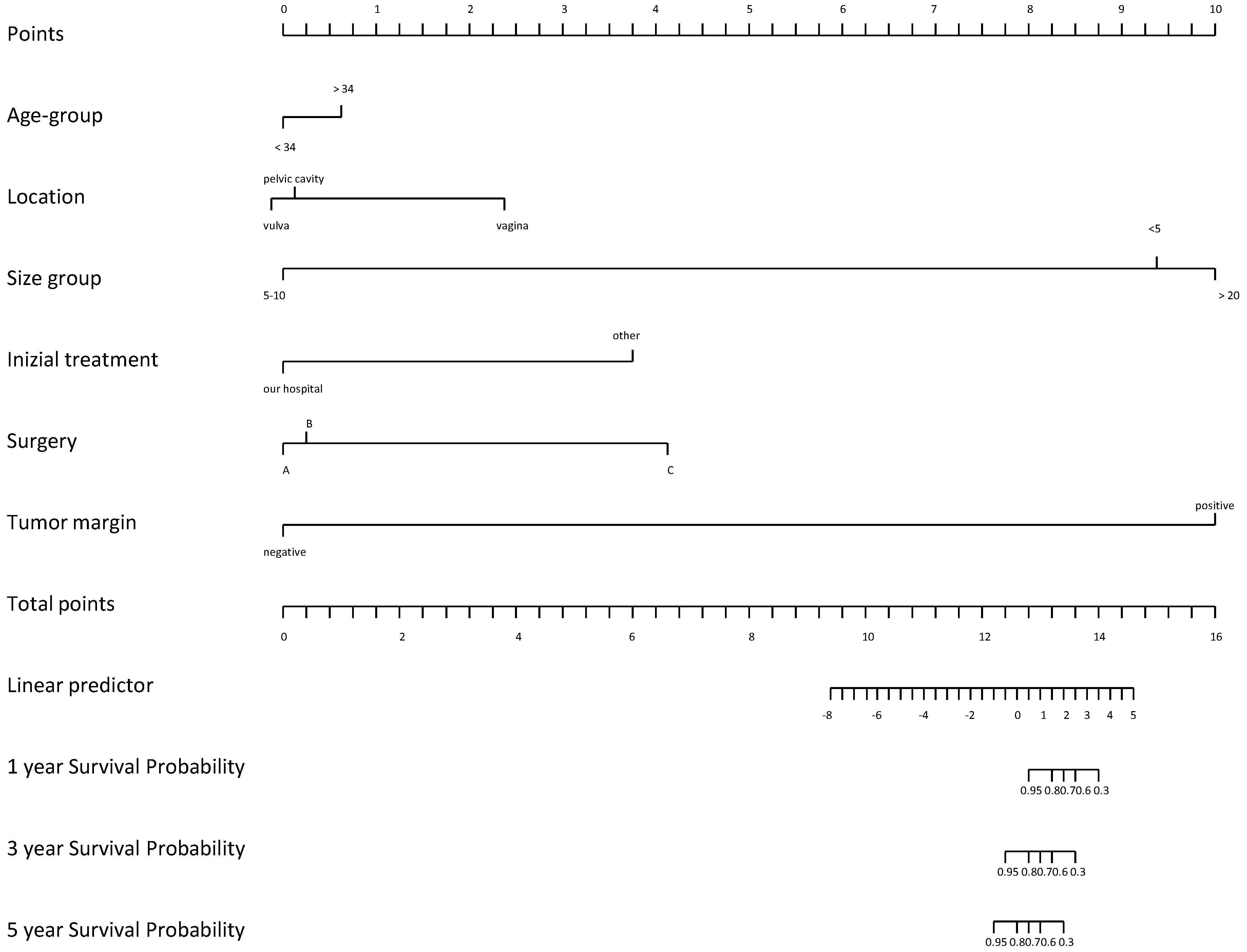
6. Prognostic Factors
- -
- a case of an aggressive angiomyxoma of the pelvis, with massive bilateral pulmonary, mediastinal, iliac, and aortic lymph node and peritoneal metastases ending in death described by Siassi et al. in 1999 [14].
- -
- another case, a 34-year-old woman developed several local recurrences after primary resection of an AAM and subsequently died from multiple lung metastases [17].
7. Results
8. Discussion
9. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Steeper, T.A.; Rosai, J. Aggressive angiomyxoma of the female pelvis and perineum. Report of nine cases of a distinctive type of gynecologic soft-tissue neoplasm. Am. J. Surg. Pathol. 1983, 7, 463–475. [Google Scholar] [CrossRef] [PubMed]
- Graadt van Roggen, J.F.; Hogendoorn, P.C.; Fletcher, C.D. Myxoid tumours of soft tissue. Histopathology 1999, 35, 291–312. [Google Scholar] [CrossRef] [PubMed]
- Preti, M.; Bucchi, L.; Micheletti, L.; Privitera, S.; Corazza, M.; Cosma, S.; Gallio, N.; Borghi, A.; Bevilacqua, F.; Benedetto, C. Four-decade trends in lymph node status of patients with vulvar squamous cell carcinoma in northern Italy. Sci. Rep. 2021, 11, 5661. [Google Scholar] [CrossRef] [PubMed]
- Dellino, M.; Cicogna, S.; Falcone, F.; Mitidieri, M.; Mazzeo, R.; Pignata, S.; Mangili, G.; Cormio, G. “Intestinal-Type” Vulvar Adenocarcinoma: A Review of the MITO Rare Tumors Group. Cancers 2022, 14, 5171. [Google Scholar] [CrossRef] [PubMed]
- Cicogna, S.; Dellino, M.; Miano, S.T.; Magazzino, F.; Domenici, L.; Pignata, S.; Mangili, G.; Cormio, G. Aggressive Angiomyxoma of the Lower Female Genital Tract in Pregnancy: A Review of the MITO Rare Tumors Group. Cancers 2023, 15, 3403. [Google Scholar] [CrossRef] [PubMed]
- Carney, J.A.; Headington, J.T.; Su, W.P. Cutaneous myxomas. A major component of the complex of myxomas, spotty pigmentation, and endocrine overactivity. Arch. Dermatol. 1986, 122, 790–798. [Google Scholar] [CrossRef]
- Behranwala, K.A.; Latifaj, B.; Blake, P.; Barton, D.P.; Shepherd, J.H.; Thomas, J.M. Vulvar soft tissue tumors. Int. J. Gynecol. Cancer 2004, 14, 94–99. [Google Scholar] [CrossRef] [PubMed]
- Chan, Y.M.; Hon, E.; Ngai, S.W.; Ng, T.Y.; Wong, L.C. Aggressive angiomyxoma in females: Is radical resection the only option? Acta Obstet. Gynecol. Scand. 2000, 79, 216–220. [Google Scholar] [CrossRef] [PubMed]
- Zizi-Sermpetzoglou, A.; Myoteri, D.; Koulia, K.; Kontostolis, V.; Moschouris, H.; Dellaportas, D. Aggressive angiomyxoma of the vulva: A bizarre perineal lesion. Case Rep. Oncol. Med. 2015, 2015, 292304. [Google Scholar] [CrossRef]
- van Roggen, J.F.; van Unnik, J.A.; Briaire-de Bruijn, I.H.; Hogendoorn, P.C. Aggressive angiomyxoma: A clinicopathological and immunohistochemical study of 11 cases with long-term follow-up. Virchows Arch. 2005, 446, 157–163. [Google Scholar] [CrossRef]
- Micci, F.; Panagopoulos, I.; Bjerkehagen, B.; Heim, S. Deregulation of HMGA2 in an aggressive angiomyxoma with t(11;12)(q23;q15). Virchows Arch. 2006, 448, 838–842. [Google Scholar] [CrossRef] [PubMed]
- Nucci, M.R.; Weremowicz, S.; Neskey, D.M.; Sornberger, K.; Tallini, G.; Morton, C.C.; Quade, B.J. Chromosomal translocation t(8;12) induces aberrant HMGIC expression in aggressive angiomyxoma of the vulva. Genes Chromosomes Cancer 2001, 32, 172–176. [Google Scholar] [CrossRef] [PubMed]
- Pisacane, A.; Cascardi, E.; Berrino, E.; Polidori, A.; Sarotto, I.; Casorzo, L.; Panero, M.; Boccaccio, C.; Verginelli, F.; Benvenuti, S. Real-world histopathological approach to malignancy of undefined primary origin (MUO) to diagnose cancers of unknown primary (CUPs). Virchows Arch. 2023, 482, 463–475. [Google Scholar] [CrossRef] [PubMed]
- Siassi, R.M.; Papadopoulos, T.; Matzel, K.E. Metastasizing aggressive angiomyxoma. N. Engl. J. Med. 1999, 341, 1772. [Google Scholar] [CrossRef] [PubMed]
- Wei, H.Q.; Liu, J.; Feng, J.J. Clinicopathological analysis of aggressive angiomyxoma. Zhonghua Yi Xue Za Zhi 2012, 92, 1553–1555. [Google Scholar] [PubMed]
- Pinto, V.; Dellino, M.; Cicinelli, R.; Micheletti, L.; Ingravallo, G.; Cazzato, G.; Cascardi, E.; Cicinelli, E. Multiple Vulvar Polyps in Pregnancy: A Benign Disease With a Challenging Diagnosis. J. Low. Genit. Tract Dis. 2023, 27, 302–305. [Google Scholar] [CrossRef] [PubMed]
- Gulino, F.A.; Gulisano, M.; Ettore, C.; Giorlandino, A.; Russo, E.; Ettore, G. Aggressive Angiomyxoma of the Vulva: Which Is the Best Management Strategy? Description of a Case Report and Review of Literature of the Last Ten Years. J. Clin. Med. 2023, 12, 1726. [Google Scholar] [CrossRef]
- Xu, H.; Sun, P.; Xu, R.; Wang, L.; Shi, Y. Aggressive angiomyxoma in pregnancy: A case report and literature review. J. Int. Med. Res. 2020, 48, 0300060520936414. [Google Scholar] [CrossRef]
- Dellino, M.; Gargano, G.; Tinelli, R.; Carriero, C.; Minoia, C.; Tetania, S.; Silvestris, E.; Loizzi, V.; Paradiso, A.; Casamassima, P.; et al. A strengthening the reporting of observational studies in epidemiology (STROBE): Are HE4 and CA 125 suitable to detect a Paget disease of the vulva? Medicine 2021, 100, e24485. [Google Scholar] [CrossRef]
- Faraj, W.; Houjeij, M.; Haydar, A.; Nassar, H.; Nounou, G.; Khalife, M. Aggressive angiomyxoma presenting with back and perineal bulge; a complex surgical approach: A case report. Int. J. Surg. Case Rep. 2016, 24, 211–214. [Google Scholar] [CrossRef]
- Cohen-Cole, S.A. Training outcome in liaison psychiatry. Literature review and methodological proposals. Gen. Hosp. Psychiatry 1980, 2, 282–288. [Google Scholar] [CrossRef]
- Choi, H.; Park, C.; Ji, Y.-I. Alternative surgical approaches for aggressive angiomyxoma at different sites in the pelvic cavity. Obstet. Gynecol. Sci. 2015, 58, 525–529. [Google Scholar] [CrossRef]
- Salman, M.C.; Kuzey, G.M.; Dogan, N.U.; Yuce, K. Aggressive angiomyxoma of vulva recurring 8 years after initial diagnosis. Arch. Gynecol. Obstet. 2009, 280, 485–487. [Google Scholar] [CrossRef]
- McCluggage, W.; Jamieson, T.; Dobbs, S.; Grey, A. Aggressive angiomyxoma of the vulva: Dramatic response to gonadotropin-releasing hormone agonist therapy. Gynecol. Oncol. 2006, 100, 623–625. [Google Scholar] [CrossRef]
- Yuan, R.; Zhuo, R.; Xiao, T.; Dai, X.; Wang, Z.; Le, A. Five cases’ female aggressive angiomyxoma experience. Eur. J. Gynaecol. Oncol. 2017, 38, 715–719. [Google Scholar]
- Schwartz, P.E.; Hui, P.; McCarthy, S. Hormonal therapy for aggressive angiomyxoma: A case report and proposed management algorithm. J. Low. Genit. Tract Dis. 2014, 18, E55–E61. [Google Scholar] [CrossRef]
- Dahiya, K.; Jain, S.; Duhan, N.; Nanda, S.; Kundu, P. Aggressive angiomyxoma of vulva and vagina: A series of three cases and review of literature. Arch. Gynecol. Obstet. 2011, 283, 1145–1148. [Google Scholar] [CrossRef]
- Raptin, C.; Lucot, J.-P.; Bassil, A.; Poncelet, E.; Prolongeau, J.-F.; Phalippou, J. Aggressive angiomyxoma of the perineal region. SAGE Open Med. Case Rep. 2019, 7, 2050313X19843391. [Google Scholar] [CrossRef]
- Blandamura, S.; Cruz, J.; Vergara, L.F.; Puerto, I.M.; Ninfo, V. Aggressive angiomyxoma: A second case of metastasis with patient’s death. Hum. Pathol. 2003, 34, 1072–1074. [Google Scholar] [CrossRef]
- Zamani, M.; Mollabashi, M.; Mehrabi, N.; Alizadeh, S. Aggressive angiomyxoma of vulva in 28-years old patient: A case report of second recurrence. Ann. Med. Surg. 2021, 69, 102706. [Google Scholar] [CrossRef]
- Wiser, A.; Korach, J.; Gotlieb, W.; Fridman, E.; Apter, S.; Ben-Baruch, G. Importance of accurate preoperative diagnosis in the management of aggressive angiomyxoma: Report of three cases and review of the literature. Abdom. Imaging 2006, 31, 383–386. [Google Scholar] [CrossRef]
- Shinohara, N.; Nonomura, K.; Ishikawa, S.; Seki, H.; Koyanagi, T. Medical management of recurrent aggressive angiomyxoma with gonadotropin-releasing hormone agonist. Int. J. Urol. 2004, 11, 432–435. [Google Scholar] [CrossRef]
- Bhandari, R.N.; Dragun, A.E.; Aguero, E.G.; Sharma, A.K. External beam radiotherapy for perirectal angiomyxoma results in a dramatic clinical response and allows a patient to avoid abdominoperineal resection. Am. J. Clin. Oncol. 2006, 29, 318–319. [Google Scholar] [CrossRef]
- Begin, L.R.; Clement, P.B.; Kirk, M.E.; Jothy, S.; McCaughey, W.T.; Ferenczy, A. Aggressive angiomyxoma of pelvic soft parts: A clinicopathologic study of nine cases. Hum. Pathol. 1985, 16, 621–628. [Google Scholar] [CrossRef]
- Fetsch, J.F.; Laskin, W.B.; Tavassoli, F.A. Superficial angiomyxoma (cutaneous myxoma): A clinicopathologic study of 17 cases arising in the genital region. Int. J. Gynecol. Pathol. 1997, 16, 325–334. [Google Scholar] [CrossRef]
- Granter, S.R.; Nucci, M.R.; Fletcher, C.D. Aggressive angiomyxoma: Reappraisal of its relationship to angiomyofibroblastoma in a series of 16 cases. Histopathology 1997, 30, 3–10. [Google Scholar] [CrossRef]
- York, D.; Saikumar, S.; Patel, P.; Edwards, C.; Garcia, G.; Naqvi, H. A Paraurethral Aggressive (Deep) Angiomyxoma. Case Rep. Obstet. Gynecol. 2022, 2022, 5604460. [Google Scholar] [CrossRef]
- Han-Geurts, I.J.; van Geel, A.N.; van Doorn, L.; Bakker, M.d.; Eggermont, A.M.; Verhoef, C. Aggressive angiomyxoma: Multimodality treatments can avoid mutilating surgery. Eur. J. Surg. Oncol. 2006, 32, 1217–1221. [Google Scholar] [CrossRef]
- Foust-Wright, C.; Allen, A.; Shobeiri, S.A. Periurethral aggressive angiomyxoma: A case report. Int. Urogynecol. J. 2013, 24, 877–880. [Google Scholar] [CrossRef]
- Srivastava, V.; Jha, P.K.; Verma, A.K.; Ansari, M.A. Vulvar aggressive angiomyxoma: A surgical challenge. BMJ Case Rep. 2021, 14, e240687. [Google Scholar] [CrossRef]
- Wahid, A.; Hakeem, A.; Khan, S. Aggressive angiomyxoma in the ischiorectal fossa. J. Pak. Med. Assoc. 2020, 70, 1304–1306. [Google Scholar] [CrossRef]
- Ayati, E.; Pesikhani, M.D.; Karamali, M.; Borhan, A.; Pourali, L. A deep giant aggressive angiomyxoma of the labia majora: A case report. Int. J. Surg. Case Rep. 2022, 96, 107313. [Google Scholar] [CrossRef]
- Padmavathy, L.; Rao, L.L.; Lakshmi, M.D.; Sylvester, N. Aggressive angiomyxoma. Indian Dermatol. Online J. 2014, 5, 151–153. [Google Scholar] [CrossRef]
- Li, J.; You, L.; Wang, C.; Zhao, H.; Guo, W.; Yu, J.; Yuan, Z.; Qi, S.; Huang, Y. Clinicopathological characteristics and prognosis analysis of Aggressive angiomyxoma: A Retrospective Study. Res. Sq. 2022. [Google Scholar] [CrossRef]
- Siddiqui, S.F. Rare case of metastatic aggressive angiomyxoma-first case of renal metastasis. Gynecol. Obstet. Case Rep. 2020, 6, 27. [Google Scholar]
- Goyal, L.D.; Garg, P.; Badyal, R.; Bhalla, S. Aggressive (deep) angiomyxoma of the vulva: A case report. J. Med. Case Rep. 2022, 16, 71. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| References | Sample Size n° / Age | Symptoms / Clinical Aspects | Dimensions/ Site | Primary (P) / Relapse (R) | Treatment | Margins | Histological Features | Immuno-Histochemical Analysis | Follow-Up/ Treatment |
|---|---|---|---|---|---|---|---|---|---|
| Salman MC, 2009 [23] | 1 28 yrs | Non-tender mass | 3.5 cm × 3 cm RLM | R 8 yrs later | Surgical excision | + | Myxoid stroma/ spindle-shaped cells/ arterioles with thick walls | N.A. | Alive-NED |
| McCluggage WG, 2006 [24] | 1 35 yrs | Menorrhagia, swelling, fluctuant mass | 8 cm × 6 cm × 6 cm vulva right side, RLM, centre of the pelvis | P | Surgical excision with TAH+MSO+ GnRHa | + | Myxoid stroma/ spindle-shaped cells/ thick-thin walled blood vessels | ER+ PR− | Alive-NED/GnRHa |
| Sun NX, 2010 [18] | 1 31 yrs | Soft mass | 3.2 cm × 1.8 cm RLM (2 cm anterior to the anus) | P | Surgical excision + GnRHa | - | Myxoid stroma/ spindle-shaped cells/ thick-thin walled blood vessels | Vimentin+ SMA + Desmin− S100− ER+ PR+ | Alive-NED/GnRHa |
| Yuan R, 2017 [25] | 5 32 yrs (median age 20–52) 1 2 3 4 5 | Cystic mass Low abdominal pain Vaginal prolapse Vaginal bleeding after sexual Vaginal mass | 3 solid masses (75%) and 1 cystic mass (25%) 18 cm × 10 cm × 9 cm pelvis 23 cm × 20 cm × 10 cm abdomen-pelvis Vagina Vagina Vagina | R (20 months after) P P P P | Surgical excision Surgical excision Surgical excision Surgical excision Surgical excision | + 2/5 - 3/5 | Myxoid stroma/spindle cells-stellate cells/ thick-thin walled blood vessels | SMA + (60%) S100− | Alive (the patients were followed up for 6 to 43 months): 1 RD |
| Choi H, 2015 [22] | 3 49 yrs 31 yrs 36 yrs | Soft mass Mixed echogenic mass, abdominal distension and lower abdominal swelling Soft mass | 27 cm LLM 18 cm × 15 cm × 8 cm Pelvis 15 cm × 10 cm × 6 cm left buttock and left perineum, extending to the left retroperitoneum | P P P | Surgical excision Surgical excision Surgical excision | - - - | N.A. Capillaries and cavernous vascular spaces filled with blood and stellate spindle cell proliferation in interstitial tissue Capillaries and cavernous vascular spaces filled with blood and stellate spindle cell proliferation in the interstitial tissue | ER+ Desmin+ CD24+ S100+ CD10+ SMA+ Desmin+ CD34+ CD10+ SMA+ Desmin+ CD34+ | Alive-NED Alive-NED Alive-NED |
| Schwartz PE, 2014 [26] | 1 32 yrs | Soft mass | 4 cm × 2.5 cm LLM- pelvis- presacral region/ left sciatic nerve | P/R 7 recurrences during 16 yrs, latest in November 2006 | Surgical excision + GnRHa | + | Myxoid stroma/ spindle-shape cells/ thick-thin walled blood vessels | ER+ PR+ | Alive-NED with GnRHa (free of disease for more than 2 years after discontinuing the leuprolide acetate) |
| Dahiya K, 2010 [27] | 3 27 yrs 30 yrs 32 yrs | Non-tender cyst discharge, dispareunia Tumor mass Cystic mass, swelling and discomfort | 5 cm × 4 cm/ right posterior-lateral wall of vagina 10 × 12 × 8 cm/ vulva and paravaginal tissue 3 cm × 4 cm/ vulva | P P P | Surgical excision Surgical excision Surgical excision | - + - | Myxoid tissue & jelly-like material/vascular structure Myxoid-collagenous stroma/thick-walled vessels/spindle-stellate shaped cells Myxoid stroma/ spindle-shaped cells/ thick-thin walled blood vessels | NA NA ND | Alive-NED Lost to F.U. Alive-NED |
| Raptin C, 2019 [28] | 1 24 yrs | Rectocele, perineal swelling | 7 cm/ mass of the rectovaginal septum | P | Surgical excision | - | Myxoid stroma/ spindle-shaped cells/ thick-thin walled blood vessels | ER+ PR+ Desmin+ SMA+ CD34+ S100− | R.D. at 1 year: second surgery |
| Faraj W, 2016 [20] | 1 36 yrs | Non-tender mass Pelvic heaviness, urinary urgency | 20 cm/ lower back- perineal right area/ right ischiorectal fossa and inferior right perineum/ lung metastasis | R 1 yrs later | Surgical excision | - | Fibro-collagenous and myxoid stroma/ spindled and stellate bland cells | Desmin+ SMA+ S100− | N.A. |
| Blandamura S, 2003 [29] | 1 27 yrs | Mass | 20 cm vulva/ lung metastasis | P | Surgical excision | NA | Myxoid stroma spindle and stellate cells/ some vessels | Desmin+ SMA+ S100− Mib1− p53− PR+ ER+ (lung) ER− (vulva) | R.D.-DEAD |
| Zamani M, 2021 [30] | 1 28 yrs | Pedunculated polypoidal mass, soft, spongy painless, | 20 × 15 × 10 cm supra and pre pubic/labium majora and minora/invasive lesions in anal canal | R 2 yrs after the first recurrence | Surgical excision/ Decapeptide | - | Stroma without atypia/obvious mitotic activity/variably sized vessels | ER+ PR+ | Alive-NED |
| Wiser A, 2006 [31] | 3 25 yrs 40 yrs 48 yrs | Soft mass/ swelling/ Mass Asymptomatic- pedunculated mass | 7.6 cm LLM 10 cm right buttock/perineal and intrapelvic 2 cm posterior vaginal fornix | P R P | Surgical excision Surgical excision Surgical excision | - - - | Spindle cells/lack of mitotic activity/ interdigitation protrusion myxoid matrix | NA NA NA | RD: surgical excision/ Alive-NED Alive-NED Alive-NED |
| Shinohara N, 2004 [32] | 1 34 yrs | Gelatinous soft mass | 50 × 49 × 19 cm perineum/ pelvic cavity | R 4 yrs later | Surgical excision/GnRHa | + | Myxoid stroma/ spindle-stellate tumor cells/blood vessels | ER+ PR+ | R.D.: GnRHa/Alive-NED |
| Bhandari RN, 2006 [33] | 1 74 yrs | Soft, nontender, well mass | 8 × 10 cm left gluteus/pelvic floor to within 0.4 cm of the rectum | P | BPS/ RT | N.A. | N.A. | Desmin+ Cytokeratin+ S100− CD34− | Alive-NED 1 year after |
| Steeper TA, 1983 [1] | 9 21 yrs 33 25 26 38 34 32 28 32 | Tumor mass Soft mass Lobulated mass NA Painful/“hernia-like” mass Soft mass Swelling/ Soft mass Irregularly rounded mass Soft mass | 14 cm × 10 cm × 8 cm vulva 11 cm × 6 cm pelvis/perineum 18 cm × 12 cm vulva/ischiorectal fossa 14 cm × 9 cm × 5 cm vulva 5 cm × 5 cm × 3 cm vulva 60 cm × 20 cm pelvis/gluteal region/retroperitoneum 25 cm × 6 cm vulva/obturator fossa 3 cm × 3 cm vulva 10 cm × 7 cm × 3 cm pelvis/perineum | P R 14–15 yrs later R 3 yrs later P P P R 1 yrs later P P | Surgical excision Surgical excision Surgical excision Surgical excision Surgical excision Incomplete surgical excision Surgical excision Surgical excision Surgical excision | N.A. | Partially or completely encapsulated mass/finger-like tumor projections/ lobulated appearance/ spindled cells in stellate configuration/myxoid background/ prominent vascular pattern | N.A. | R.D. 2 yrs later: surgical excision/ lost to FU Alive-NED Alive-NED Alive-NED Local recurrence-21 months later: Surgical excision-Alive-NED RD 2 months later: surgical excision-NED Alive-NED Alive-NED N.A. |
| Bégin LR, 1985 [34] | 7 63 yrs 21 yrs 36 yrs 47 yrs 30 yrs 36 yrs 32 yrs | Cyst-like lesion Swelling after delivery N.A. Swelling Incidental mass at episiotomy Mass Polypoid lesion | 4.3 × 2 × 1.5 cm vagina 14 × 9 × 5 cm vagina/pelvic floor 10 cm vagina 3 × 2 × 1 cm pelvic floor/ vagina/LLM 5.5 cm rectum/LLM perineum/left ischiorectal space 8 × 5 × 5 cm vulva 5 × 3 × 1.5 cm vulva | P P P P P P P | Surgical excision Surgical excision Surgical excision Surgical excision Surgical excision Surgical excision Surgical excision | 4/7 + | Myxoid stroma/stellate and spindled-shaped cells/ vascular channels of small or medium-sized arteries and veins. | Actin + CEA− Keratin− FVIII− Prot.S100− | R.D. 16 months later: surgical excision N.A. R.D. (interval NA) 2 R.D. (48,144 months later)-DEAD R.D. 84 months after N.A. R.D. 24 months |
| Fetsch JF, 1996 [35] | 29 (16–70 yrs, median age 34) | Mass/ pain/pressure and pulsating sensations/dyspareunia/increased mass effect with heavy lifting or during menstruation/ pelvic and vague lower abdominal pain/sensation of fullness in the vulva/ urinary frequency | 210 cm pelvis/perirectal region/perineum/vulva/buttock/ Bartholin gland region/ retroperitoneum/ inguinal region/LM | P | Surgical excision/ TAH/BSO/ RT | N.A. | Mesenchymal cells/ matrix with collagen/scattered vessels of varying caliber/arborizing vascular pattern absent | Desmin+ (22 pt/22) SMA+ (19 pt/20) MSA+ (16 pt/19) Vimentin+ (17 pt/17) CD34/QBEND-10 + (8 pt/16) ER+ (13 pt/14) PR+ (9 pt/10) S100− (0 pt/20) Ki67 < 1% | 8 R.D. 21 NED |
Granter SR, 1997 [36] | 16 (19–53 yrs, median age 39.5) | Soft mass/pain/Bartholin cyst/inguinal hernia/ abscess | 5–23 cm (range) perineal mass/anus/vagina/bladder/rectum/mons pubis/inguinal region/para-urethral | N.A. | Surgical excision | 14/16 + 2/16 − | Myxoid stroma/spindled cells/ variable sized vessels | Desmin+ (13/14) SMA+ (10/11) S100− | 6 NED 3 N.A. 4 R.D. 1 Alive with symptoms 2 N.A. |
| York D, 2022 [37] | 1 31 yrs | Vaginal itching/pelvic pressure/discomfort | 3.5 × 2 × 1.5 cm para-urethral/anterior vaginal wall mass | P | Surgical excision | N.A. | Myxoid stroma/abundant vasculature/ focally infiltrating fibroadipose tissue | N.A. | N.A. |
| Siassi RM, 1999 [14] | 1 63 yrs | Abdominal discomfort/ | up to 9.5 by 7 cm pelvis/chest (metastasis) | P | Surgical excision | - | Stellate and spindled cells/ myxo-collagenous matrix | CD34+ ER+ PR+ S100− SMA+ Desmin+ Vimentin+ | DEAD |
| Han-Geurts IJ, 2006 [38] | 7 (23–39 yrs, median age 32) | Swelling | left gluteal area/ pelvis/vagina/ LLM/RLM/pubic bone/ischiorectal fossa/perineal area | 4P 3R | Surgical excision/embolization/RT | 5 − 2 + | Stellate and spindled cells/ myxo-collagenous matrix | ER+ PR+ | 6 NED 1 RD: NED after treatment |
| Foust-Wright C, 2012 [39] | 1 19 yrs | Asymmetric soft tissue mass/pelvic pain-vaginal protrusion-mild dysuria- occasional urinary stress incontinence | 5. × 2.5 × 1 cm/periurethral | P | Surgical excision | - | Spindle-stellate cells/vessels and occasional thick-walled blood vessels | ND | Alive-NED |
| Srivastava V, 2021 [40] | 1 37 yrs | Swelling | 10 × 15 cm right vulvar region/perineum/ right ischiorectal fossa | R 3 yrs after | Surgical excision/ Tamoxifen | - | Spindle- stellate cells/myxoid/thin to medium caliber blood vessel/ no atypical mitosis | ER+ PR+ t12q13–15 leading to HMGA2 | Alive-NED |
| Wahid A, 2020 [41] | 1 17 yrs | Pain, burning, numbness | 7 × 4.5 × 2 cm/ right ischiorectal fossa | P | Surgical excision | - | Spindle shaped cells/myxoid background/ vessels with adventitial thickening and perivascular lymphocytic cuffing with presence of smooth muscle cells | Desmin+ CD34+ S100− SMA− | Alive-NED |
| Ayati E, 2022 [42] | 1 31 yrs | Swelling | 13.7 × 6 × 19 cm RLM/ right lateral wall of the vagina and the anal canal | P | Surgical excision | - | Spindle cell/variable-sized blood vessels/ myxoid areas | N.A. | NED |
| Padmavathy L, 2014 [43] | 1 55 yrs | 8 cm peduncolate tumor/ 0.5 × 0.5 cm peduncolate tumor | Anterior vaginal wall/ posterior vaginal wall | P | Surgical excision | - | Fibromyxoid stroma/proliferating vascular channels of varying size ulcerated stratified squamous epithelium | Desmin+ CD34+ S100− | N.A. |
| Li JunHu, 2022 [44] | 14 34 yrs (median age 19–58) | 11 painless masses (78.6%)/ 2 abdominal pain (14.3%)/ 1 dysuria (7.1%) | 5 pelvis (35.7%)/ 5 vulva (35.7%)/ 4 vagina (28.6%) | N.A. | Surgical excision | 8− (51.7%) 6+ (42.9%) | N.A. | Desmin+ SMA+ Vimentin+ CD34+ ER+ PR+ S100− (+1/12) | 7 RD: 2° surgery+ADJ TRP(GnRHa/CHT/AE)-Alive-NED 7 Alive-NED |
| Siddiqui SF, 2020 [45] | 1 45 yrs | Large mass | 13 × 12 × 10 cm vagina/ abdomen/pelvis/ chest (metastasis) | P | BPS/ neoadjuvant GnRH therapy | N.A. | N.A. | Desmin+ CD34+ S100− SMA− | DEAD after therapy |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dellino, M.; Magazzino, F.; Domenici, L.; Cicogna, S.; Miano, S.T.; Pignata, S.; Mangili, G.; Cormio, G. Aggressive Angiomyxoma of the Lower Female Genital Tract: A Review of the MITO Rare Tumors Group. Cancers 2024, 16, 1375. https://doi.org/10.3390/cancers16071375
Dellino M, Magazzino F, Domenici L, Cicogna S, Miano ST, Pignata S, Mangili G, Cormio G. Aggressive Angiomyxoma of the Lower Female Genital Tract: A Review of the MITO Rare Tumors Group. Cancers. 2024; 16(7):1375. https://doi.org/10.3390/cancers16071375
Chicago/Turabian StyleDellino, Miriam, Francescapaola Magazzino, Lavinia Domenici, Stefania Cicogna, Salvatora Tindara Miano, Sandro Pignata, Giorgia Mangili, and Gennaro Cormio. 2024. "Aggressive Angiomyxoma of the Lower Female Genital Tract: A Review of the MITO Rare Tumors Group" Cancers 16, no. 7: 1375. https://doi.org/10.3390/cancers16071375
APA StyleDellino, M., Magazzino, F., Domenici, L., Cicogna, S., Miano, S. T., Pignata, S., Mangili, G., & Cormio, G. (2024). Aggressive Angiomyxoma of the Lower Female Genital Tract: A Review of the MITO Rare Tumors Group. Cancers, 16(7), 1375. https://doi.org/10.3390/cancers16071375